")
Back to Journals » International Journal of General Medicine » Volume 16
Associations of Serum Clara Cell Protein 16 with Severity and Prognosis in Adults with Community-Acquired Pneumonia
Authors Li JF, Zou Q, Li X, Liu Y, He QY, Fu L , Zhao H
Received 8 July 2023
Accepted for publication 25 October 2023
Published 31 October 2023 Volume 2023:16 Pages 4907—4917
DOI https://doi.org/10.2147/IJGM.S429665
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Jia-Fei Li,1– 3 Qian Zou,2 Xun Li,2 Ying Liu,1,3 Qi-Yuan He,1,3 Lin Fu,1,3 Hui Zhao1,3
1Department of Respiratory and Critical Care Medicine, Second Affiliated Hospital of Anhui Medical University, Hefei, Anhui, 230601, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, First People’s Hospital of Chuzhou, Chuzhou, Anhui, 239001, People’s Republic of China; 3Institute of Respiratory Diseases, Second Affiliated Hospital of Anhui Medical University, Hefei, Anhui, 230601, People’s Republic of China
Correspondence: Lin Fu; Hui Zhao, Department of Respiratory and Critical Care Medicine, Second Affiliated Hospital of Anhui Medical University, Furong Road 678, Hefei, Anhui, 230601, People’s Republic of China, Tel/Fax +86 551 63869400, Email [email protected]; [email protected]
Background: Clara cell protein 16 (CC16) has multiple functions, including antioxidant, anti-inflammatory, and immune regulation properties. Nevertheless, the concrete function of CC16 in adult patients with community-acquired pneumonia (CAP) remained blurred.
Methods: A total of 541 adult patients with CAP were recruited on admission. Peripheral blood specimens, clinical parameters, and demographic characteristics were collected. The concentration of serum CC16 was evaluated through ELISA. The relationships between serum CC16 and clinical parameters were appraised by Spearman or Pearson correlative analyses. The correlations of serum CC16 with severity and prognosis were assessed using linear or logistic regression models.
Results: The level of CC16 was gradually decreased across with the elevated severity scores system of CAP. After treatment, the level of serum CC16 was upregulated. Correlative analyses found that serum CC16 was negatively related to inflammatory cytokines. Additionally, multivariate linear and logistic regression models revealed that serum CC16 was inversely associated with severity scores system. In addition, reduced serum CC16 on admission elevated the risks of vasoactive agent usage, ICU admission, and death during hospitalization. We observed an almost discriminatory ability for severity and death between serum CC16 and severity scores system, and were all obviously elevated compared to routine inflammatory and infectious markers.
Conclusion: There are substantially inverse correlations between serum CC16 level on admission with severity scores and poorly prognostic outcomes, indicating that CC16 is involved in the pathophysiological process of CAP. This study is helpful for establishing the potential application of serum CC16 in risk evaluation and targeted treatment.
Keywords: Clara cell protein 16, community-acquired pneumonia, severity, prognosis, inflammation, cohort study
Background
Community-acquired pneumonia (CAP) is a significant reason for morbidity and mortality, which has posed a huge threat to human health all over the world. Because of regular complications and a long hospitalization period, mortality is still high among CAP patients.1–3 CAP is a popular infectious disease. At present, more than 5 million CAP patients emerge in America, with 1 million hospitalizations and 60,000 deaths from pneumonia every year.4 As many countries have faced an aging society, immune system is decreased, as well as changing characteristics of pathogens and rising antibiotic resistance are incrementally occurring, CAP therapy is presently encountering lots of new challenge in today’s complex world.5–7 Several more effective biomarkers may offer assistance to estimate the illness condition and reduce the death risk in CAP patients. Previous studies have found that levels of serum annexin A1, procalcitonin, D-Dimer, and miR-181b can predict the severity and prognosis in CAP patients.8–11 In addition, a series of studies from our team indicated that the concentrations of several serum biomarkers, such as S100A9, survivin, interleukin-27 (IL-27), and IL-37 are strongly associated with the severity and prognosis among CAP patients.12–14 Therefore, we speculate that serum biomarkers exert vital roles in early illness estimation and prognostic prediction in CAP patients.
Clara cell protein 16 (CC16) is a small protein primarily produced by Clara cells and arranges on the respiratory epithelium, distal respiratory, terminal bronchioles, and the mucosa of the respiratory tract, which accounts for the majority of its contents in blood.15–17 An emerging body of evidences indicates that CC16 has multiple physiological functions, such as anti-inflammatory, antioxidant, antifibrosis, immune regulation, anti-tumoral properties, and so on.18–21 Previous investigations have hinted that CC16 is implicated in the progression of many pulmonary diseases, consisting of acute lung injury, chronic obstructive pulmonary disease (COPD), asthma, silicosis, and idiopathic pulmonary fibrosis.22–27 Additionally, serum CC16 is also obviously reduced in smokers.28 Consequently, CC16 has been a topic of general interest for its potential biomarker in pulmonary diseases.
So far, there is no exact evidence of CC16 in CAP. The correlation of CC16 and CAP severity has not been elucidated. Not only that, the relationships between CC16 and prognostic outcomes remain indistinct among CAP cases. Previous animal studies have revealed that the level of CC16 is reduced in bronchoalveolar lavage fluid (BALF) of mouse model of human influenza infection.29 Moreover, CC16 deficiency mouse increases the secretion of bacterial invasion proteins during Mycoplasma pneumoniae infection.30 Therefore, we think that CC16 may exert vital roles in the process of CAP. Hence, when the content of serum CC16 was detected, the associations between serum CC16 with the severity scores system and poor prognostic outcomes were assessed in CAP cases. Our study may provide a useful reference for the value of serum CC16 in the disease assessment and prognosis discrimination for CAP cases.
Materials and Methods
Study Population
The entire 541 participators were recruited in the Second Affiliated Hospital of Anhui Medical University in Hefei city, Anhui Province, China, from September 2020 to June 2022 through systematic sampling. All participants were diagnosed in accordance with CAP diagnostic standard.31,32 The inclusion criteria: (I) All CAP patients were newly diagnosed; (II) All patients were infected in the community, not hospital; (III) All subjects participated in the follow-up research and blood fasting samples were collected; (IV) All participators did not receive treatment or intervention before the hospitalization. Moreover, the follows were the exclusion criteria: (I) Under the age of 18; (II) Pregnant women; (III) Antibiotics, antiviral drugs, and glucocorticoids were taken in the past week; (IV) Subjects who accompanied by autoimmune diseases, tumor, COPD, infectious diseases, asthma, and other chronic pulmonary diseases were excluded; (V) Patients were in hospital over the past 6 months; (VI) Nucleic acid testing was conducted, Corona Virus Disease 2019 (COVID-19) patients were excluded.33,34 Patients who presented with symptoms of CAP should be admitted immediately. Blood draw was conducted by professional nurses at 7 am on admission. In addition, clinical characteristics, demographic information, as well as laboratory data were collected. The severity was estimated using CAP severity scores system, including CRB-65, CURB-65, CURXO, PSI, SMART-COP, and APACHE II.35,36 The higher the scores were, the severer the severity was.37,38 Moreover, CAP patients were divided into mild and severe cases on the basis of the American Thoracic Society criterion.39
Enzyme-Linked Immunosorbent Assay (ELISA)
Blood specimens were centrifuged at 3000 RPM, then collected and kept in the −80°C refrigerator until use.40,41 Human CC16 commercial ELISA kits (CSB-E08680h) were provided by Cusabio, Wuhan, China. The concentration of serum CC16 was determined using ELISA in accordance with the standard methods with simple alterations.42–44 Dilution of samples, reaction time of antibodies, and color-developing time were different and moderately altered in this experiment. Moreover, CAP patients were divided into three groups on the basis of the tertiles of serum CC16: Tertile 1, the concentration of serum CC16 was lower than 63.8 pg/mL; Tertile 2, the concentration of serum CC16 was from 63.8 pg/mL to 153.1 pg/mL; Tertile 3, the concentration of serum CC16 was higher than 153.1 pg/mL.
Statistical Analysis
All statistical analyses were conducted in SPSS 19.0. The continuous variables were presented as mean (standard error) or median (P25, P75). The categorical variables are expressed in terms of frequency (percentage). One-way ANOVA and non-parametric test were used to compare the differences between continuous variables. The differences in categorical variables were compared with χ2 test. The value of serum CC16 was log-transformed. The relationships between serum CC16 level and clinical parameters were appraised by Spearman or Pearson correlation analyses. In addition, confounding factors, including age, smoker, hypertension, diabetes mellitus, cerebral infarction, coronary heart disease, and bronchitis, were adjusted in the multivariate linear and logistic regression models. The relationships between serum CC16 level with severity scores system and poorly prognostic outcomes were estimated in the multivariate regression models. Paired Student’s t-test was conducted to compare serum CC16 of CAP patients in onset and convalescent phases. Predictive capacity was analyzed using receiver operating characteristic (ROC). Thirty-day mortality was compared with Kaplan–Meier methods and Log rank test. P value less than 0.05 was defined as statistically significant.
Results
Demographic Characteristics and Clinical Information
Demographic information, clinical parameters, and laboratory data were evaluated. As shown in Table 1, 541 eligible CAP patients were finally enrolled. The average age was 59.1 years. Female patients accounted for 41.2% and there were 20.0% smokers. Moreover, the comorbidities were evaluated. The results indicated that there were 146 (27.0%) hypertension, 59 (10.6%) diabetes mellitus, 50 (9.2%) cerebral infarction, 28 (5.2%) coronary heart disease, and 6 (1.1%) bronchitis in all CAP patients (Table 1). Several inflammatory cytokines, such as D-dimer, tumor necrosis factor-α (TNF-α), C-reactive protein (CRP), and interleukin 6 (IL-6) were simultaneously detected. According to CURXO score, there were 113 (20.9%) severe patients in the whole CAP cases. The average scores of CURB-65, CRB-65, PSI, SMART-COP, and APACHE II were 1.1, 0.9, 66.5, 1.7, and 7.6, respectively. Finally, demographic information, clinical and laboratory data were further estimated in cases with different concentrations of serum CC16. As shown in Table 1, age was decreased with elevating CC16 concentration among CAP patients. Moreover, we found that TNF-α concentration was lower in subjects with a higher CC16 content. Finally, severity scores system was gradually downregulated across the elevated CC16 (Table 1).
 |
Table 1 Demographic Characteristics of Participants at Baseline |
The Content of Serum CC16 in CAP Cases
The contents of serum CC16 were compared in CAP cases. Figure 1A indicates no difference of serum CC16 level in cases with different CRB-65 scores. Based on CURB-65 score system, the content of serum CC16 was higher in cases with 0~1 score than those in 3~5 scores (Figure 1B). According to SMART-COP score system, serum CC16 was lowest in 7~8 scores compared with other scores in CAP cases (Figure 1C). Additionally, serum CC16 level was downregulated in severe cases (CURXO score system) (Figure 1D). Serum CC16 concentration was gradually reduced in line with PSI score (Figure 1E). Simultaneously, on the basis of APACHE II score, serum CC16 concentration was higher in <4 scores compared with 6~9 and >9 scores (Figure 1F). After treatment, serum CC16 was significantly upregulated in CAP cases (Figure 1G). Lastly, serum CC16 was compared in CAP cases with different etiologies. No obvious difference of serum CC16 content was observed in cases with bacterial infection or viral infection (data not shown).
 |
Figure 1 The contents of serum CC16 in CAP patients with different severity. (A–G) The concentration of serum CC16 was evaluated using ELISA. (A) The concentrations of CC16 were compared in cases with different CRB-65 scores. (B) The concentrations of CC16 were compared in cases with different CURB-65 scores. (C) The concentrations of CC16 were compared in cases with different SMART-COP scores. (D) The concentrations of CC16 were compared in cases with different CURXO scores. (E) The concentrations of CC16 were compared in cases with different PSI scores. (F) The concentrations of CC16 were compared in cases with different APACHE II scores. (G) The concentrations of serum CC16 were compared in CAP cases before and after treatment. *P<0.05, **P<0.01. |
Correlations Between Serum CC16 Content and Clinical Parameters
Pearson correlation analysis revealed that serum CC16 content was positively linked with the count of lymphocyte (r=0.56; P=0.004) (Figure 2). Although no dominant correlation was found between serum CC16 with the indexes of liver function and renal function, Pearson correlation analysis found that the content of serum CC16 was inversely correlated with creatine kinase MB (CKMB) (r=−0.82; P<0.05). Moreover, Spearman correlation analysis indicated that serum CC16 was negatively related with many inflammatory cytokines, including D-dimer (r=−0.33; P<0.05), TNF-α (r=−0.47; P<0.05), CRP (r=−0.46; P<0.01) and IL-6 (r=−0.60; P<0.01) in CAP patients (Figure 2).
 |
Figure 2 The associations between serum CC16 and clinical parameters in CAP patients. The associations between serum CC16 and many clinical parameters were estimated by Spearman correlation coefficient or Pearson rank correlation analyses. The correlations between serum CC16 with white blood cell (WBC), neutrophil, lymphocyte, monocyte, eosinophil, basophil, uric acid, urea nitrogen, creatinine, alanine aminotransferase (ALT), aspartate aminotransferase (AST), creatine kinase (CK), and creatine kinase MB (CKMB) were analyzed by Spearman correlation analysis. In addition, the relationships between serum CC16 with lactate dehydrogenase (LDH), procalcitonin (PCT), tumor necrosis factor alpha (TNF-α), D-Dimer, interleukin 6 (IL-6), and C-reactive protein (CRP) were assessed through Spearman correlation analysis. Red color indicated the positive associations and blue color meant the inverse relationship between serum CC16 and clinical characteristics. The sizes of the circles hinted the strength of the correlations. The larger sizes were, the higher correlations strengths were. |
Associations Between Serum CC16 and Severity Scores System
In the model 1, age and smoker were adjusted. Multivariate linear regression model found that serum CC16 content was negatively linked with CRB-65 (β=−0.637; 95% CI: −0.939~-0.335), CURB-65 (β=−0.769; 95% CI: −1.129~-0.409), SMART-COP (β=−1.489; 95% CI: −2.179~-0.800), CURXO (β=−0.289; 95% CI: −0.433~-0.145), PSI (β=−37.885; 95% CI: −50.008~-25.762), and APACHE II (β=−4.180; 95% CI: −6.196~-2.165) (Table 2). Additionally, multivariate logistic regression analyses found that CURB-65 (OR=0.353; 95% CI: 0.172~0.727), CURXO (Severe) (OR=0.351; 95% CI: 0.166~0.740), APACHE II (OR=0.494; 95% CI: 0.227~0.976), and APACHE II (OR=0.262; 95% CI: 0.126~0.543) scores were all gradually elevated across with reduced CC16 levels (All P trend <0.05) (Table 2). In the model 2, age, smoker, hypertension, diabetes mellitus, cerebral infarction, coronary heart disease, and bronchitis were further adjusted. As shown in Supplementary Figure 1, multivariate logistic regression analyses also found that serum CC16 was negatively associated with severity scores system.
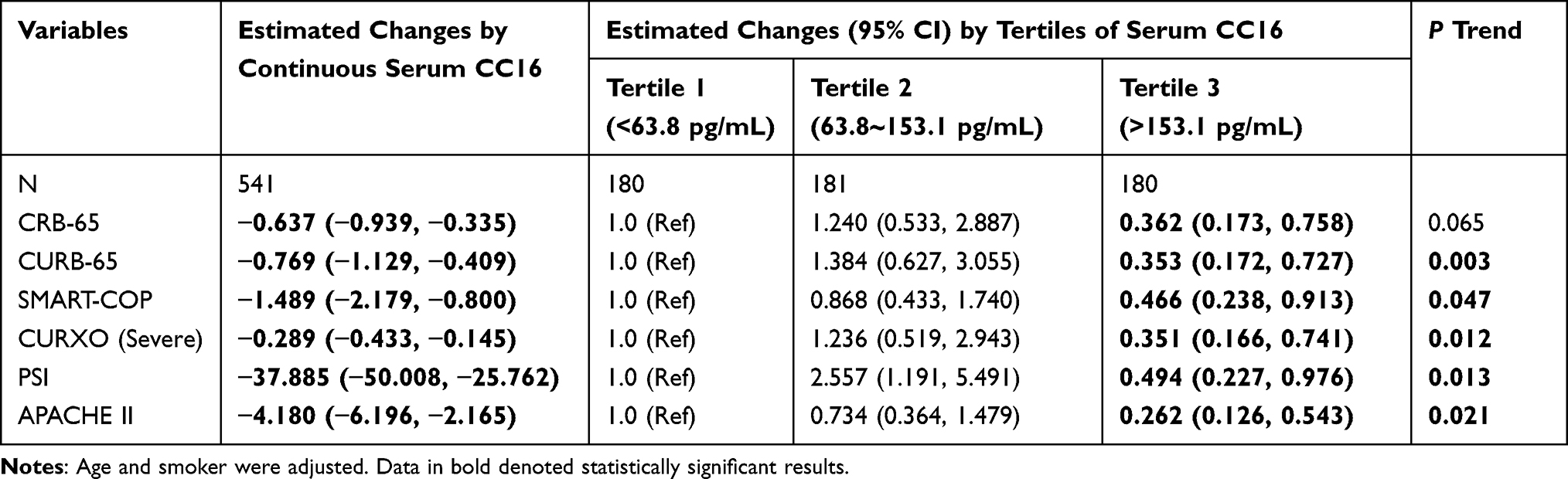 |
Table 2 Associations Between Serum CC16 and CAP Severity Scores |
Associations Between Serum CC16 and Prognostic Outcomes
According to the contents of serum CC16, the prognostic outcomes were compared in different groups. As presented in Table 3, the counts of cases with mechanical ventilation (P trend=0.015), vasoactive agent usage (P trend=0.007), ICU admission (P trend=0.006), and death (P trend=0.002) were gradually elevated in line with serum CC16 decline during hospitalization. Age, smoker, hypertension, diabetes mellitus, cerebral infarction, coronary heart disease, and bronchitis were adjusted. Logistic regression analyses demonstrated that lower serum CC16 on admission upregulated the relative risk (RR) of vasoactive agent usage, ICU admission, and death (all P trend<0.05) among CAP patients during hospitalization (Table 3).
 |
Table 3 Associations Between Serum CC16 and Prognostic Outcomes |
The Predictive Capacities for Severity and Death in Different Clinical Characteristics
The predictive capacities for severity were estimated through ROC in different parameters. As presented in Figure 3A, the area under the curve (AUC) was as follows: SMART-COP, 0.959; CRB-65, 0.944; CURB-65, 0.941; APACHE II, 0.875; CURXO, 0.876; serum CC16, 0.886; PSI, 0.789; D-dimer, 0.780; PCT, 0.759; TNF-α, 0.722; IL-6, 0.612; CRP, 0.518. Serum CC16 had a cutoff value of 85.6 pg/mL to distinguish severe cases. Serum CC16 had a sensitivity of 86.3% and a specificity of 84.2%. Additionally, the predictive power for death was estimated. As presented in Figure 3B, the area AUC was as follows: SMART-COP, 0.944; CURB-65, 0.865; CRB-65, 0.858; PSI, 0.828; APACHE II, 0.750; CURXO, 0.726; serum CC16, 0.886; PCT, 0.754; IL-6, 0.579; TNF-α, 0.612; D-dimer, 0.772; CRP, 0.589. The cutoff concentration of serum CC16 to identify death was 50.9 pg/mL, with a sensitivity of 80.6% and a specificity of 82.3%. Additionally, CAP patients were separated into two subgroups: Lower group, the level of CC16 was lower than median value (73.9 pg/mL); Higher group, the level of CC16 was higher than 73.9 pg/mL. Kaplan–Meier analysis indicated that 30-day mortality was obviously elevated in cases with lower serum CC16 level (Figure 3C).
 |
Figure 3 The predictive abilities for severity and death among CAP patients. The predictive abilities for severity and death were analyzed with ROC curve. (A) The predictive ability for severity was assessed. (B) The predictive ability for death was evaluated. (C) 30-day mortality was estimated by Kaplan–Meier analysis in patients with CAP. |
Discussion
The current research assessed the associations between serum CC16 level with severity scores system and poorly prognostic outcomes of CAP cases. The main results included Serum CC16 content was gradually declined across with elevated severity scores system; Serum CC16 content was strongly linked with many clinical parameters; Serum CC16 level was significantly and negatively associated with severity scores system; Reduced serum CC16 on admission elevated the risks of poorly prognostic outcomes during hospitalization; There was similar predictive capacities for severity and death between serum CC16 and severity scores system.
Mounting investigations have demonstrated that CC16 is a secreted protein and can exert lots of physiological functions, mainly including anti-inflammatory, antioxidant, antifibrosis, immune regulation, and anti-tumoral properties.18–21 Previous researches have confirmed that CC16 is tightly related to many pulmonary diseases. A report from a case-control study indicated that serum CC16 concentration is decreased in stable COPD patients.21 The level of pulmonary CC16 is reduced in lipopolysaccharide (LPS)-induced acute lung inflammation.45 Serum CC16 is downregulated in patients with silicosis compared to those in healthy population and is negatively associated with grades of lung damage.46 Nevertheless, the association of serum CC16 level and CAP has been obscure in the past. Our results suggest that serum CC16 concentration was reduced with elevated severity scores system. Extensive previous research has hinted that pulmonary inflammation is involved in the pathophysiology of coronavirus disease 2019 (COVID-19) and other pneumonias.47–49 Our results indicated that serum CC16 content was inversely associated with several inflammatory cytokines. Statistical analyses found that the decline of serum CC16 content was related to elevated severity scores system. Not only that, serum CC16 level was upregulated in CAP patients that received therapy. Therefore, these data first provided evidence that serum CC16 content is negatively associated with the severity of CAP cases.
A growing body of evidence suggests that serum CC16 concentration is associated with prognosis in many diseases. A previous study has revealed that serum CC16 level is higher in survivors with ventilator-associated pneumonia compared with dead elderly cases.50 Serum CC16 decrease is correlated with the elevated mortality risk of cancer patients.51 Moreover, serum CC16 reduction is positively associated with the disease progression among COPD patients.21 In addition, lower serum CC16 elevates the risks of neurotoxicity in human beings with occupational aluminium exposure.52 We speculated that there was a certain association between serum CC16 content and prognostic outcomes of CAP cases. The lower level of serum CC16 on admission increased the risks of bad prognostic outcomes during hospitalization. Additionally, exposure to cigarette smoke extract can evoke bronchial epithelial damage and CC16 decline in bronchial epithelial cells.20 In our investigation, there were 20% CAP patients with smoking habit. But no smoking was conducted in smoking patients during hospitalization. So, we thought that previously smoking habit did not affect the level of serum CC16 among CAP patients on admission. In order to further eliminate the effect of smoking status on the content of serum CC, smoking status was adjusted in the regression models. Our results suggest that serum CC16 content was inversely associated with CAP severity scores and poor prognostic outcomes whether adjusted to smoking status or not. These data hinted that CAP was the most important factor for CC16 decline, not smoking status. In order to evaluate the diagnostic accuracy for severity and death among serum CC16 content, severity scores system, and routine markers of inflammation and infection, ROC curve was analyzed. These results found that the predictive capacities of SMART-COP for severity and death were highest and that there was similar diagnostic efficiency for severity and death between serum CC16 level and other severity scores in CAP patients. The predictive powers of these severity scores were all higher than routine inflammatory and infectious indicators. Consequently, these findings suggest that serum CC16 level on admission is inversely correlated with adverse prognoses during hospitalization among CAP patients. Serum CC16 level on admission may help in predicting the severity and death risk in CAP patients early.
This study indicated that CC16 was implicated in the pathophysiology of CAP, but the exact mechanism was not elucidated. As we all known, CC16 is involved in immune function regulation and inflammation repression.25,53 In addition, CC16 has been explored as a biomarker for indicating pulmonary epithelial injury of lung diseases.54,55 CC16 not only is produced by Clara cells but also leaks across the disrupted epithelial barrier into the blood circulation. Clara cells can attenuate airway mucus production and hypersecretion. The typical characteristics of epithelial and endothelial injury are Clara cells loss and CC16 expression reduction.56,57 Clara cells are obviously reduced in COVID-19 patients.58,59 Moreover, SARS-CoV-2 infection evokes airway epithelial cell homeostasis dysfunction and mucus overproduction, finally leading to bronchiole obstruction. Injured Clara cells further reduce the production of CC16. In addition, the levels of CC16 are downregulated in lung tissues and serum specimens of COVID-19 patients.58,59 CAP is primarily evoked by bacterial infection or viral infection, which harms pulmonary epithelial and endothelial cells in CAP patients. An in vitro study indicated that Klebsiella pneumoniae (G-bacterial infection) decreases the expression of CC16 in bronchial epithelial cells. Overexpression of CC16 attenuates Klebsiella pneumoniae infection-induced inflammation and apoptosis in bronchial epithelial cells.60 Besides, it was reported that Streptococcus pneumoniae infection causes mucus overproduction and bronchiole obstruction in mice.61 Therefore, we think that bacterial infection or viral infection may damage pulmonary epithelial or endothelial homeostasis, then injure Clara cells and ultimately restrict the secretion of CC16 in CAP patients.
The current study has elevated our knowledge about CC16 in CAP patients, but there are still some shortages. Firstly, this project was only a single-institution study. More samples from different centers are required in the following work. Secondly, the level of CC16 was only measured in blood specimen. Nevertheless, CC16 expressions were not detected in lung tissues and BALF in CAP patients. Thirdly, this was an epidemiological study, the exact molecular mechanism of CC16 decrease was unclear. Only animal and cellular experiments may help to resolve this doubt. Fourthly, the validated and replicated cohorts cannot be conducted in a short time. Further validation and replication in independent studies would strengthen the robustness and generalizability of the results in the future.
Conclusion
To summarize, this project mostly analyzed the associations between serum CC16 on admission with severity and prognosis in CAP patients through a hospital-based, prospective cohort study. These data revealed that the level of serum CC16 on admission is gradually decreased in parallel with increased CAP severity scores. There are obvious and inverse dose–response associations between serum CC16 content on admission with severity and poor prognosis. Consequently, these results firstly provide evidences that CC16 is involved in the pathophysiology process of CAP. Therefore, serum CC16 content may help to predict the severity and poor prognosis in CAP patients. Our study has helped to establish the potential application of this biomarker in risk evaluation and targeted treatment of CAP patients.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was supported by the Ethics Committee of Second Affiliated Hospital of Anhui Medical University (YX2021-146) and reached the principles expressed in the Declaration of Helsinki. Informed consent was obtained from all subjects or their legal guardian(s).
Acknowledgments
We thank all patients and their families involved in this research. We also thank all members in Department of Respiratory and Critical Care Medicine in the Second Affiliated Hospital of Anhui Medical University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Natural Science Foundation of China (82100078 and 82270071).
Disclosure
All authors have declared that no competing interest existed.
References
1. Yu Y, Fei A. Atypical pathogen infection in community-acquired pneumonia. Biosci Trends. 2016;10(1):7–13. doi:10.5582/bst.2016.01021
2. Niederman MS, Mandell LA, Anzueto A, et al. Guidelines for the management of adults with community-acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med. 2001;163(7):1730–1754. doi:10.1164/ajrccm.163.7.at1010
3. Arnold FW, Summersgill JT, Lajoie AS, et al. A worldwide perspective of atypical pathogens in community-acquired pneumonia. Am J Respir Crit Care Med. 2007;175(10):1086–1093. doi:10.1164/rccm.200603-350OC
4. File TJ, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgrad Med. 2010;122(2):130–141. doi:10.3810/pgm.2010.03.2130
5. Mandell LA. Community-acquired pneumonia: an overview. Postgrad Med. 2015;127(6):607–615. doi:10.1080/00325481.2015.1074030
6. Le Roux DM, Zar HJ. Community-acquired pneumonia in children - a changing spectrum of disease. Pediatr Radiol. 2017;47(11):1392–1398. doi:10.1007/s00247-017-3827-8
7. Bartlett JG. Diagnostic tests for agents of community-acquired pneumonia. Clin Infect Dis. 2011;52(Suppl 4):S296–S304. doi:10.1093/cid/cir045
8. Karakioulaki M, Stolz D. Biomarkers in pneumonia-beyond procalcitonin. Int J Mol Sci. 2019;20(8):2004. doi:10.3390/ijms20082004
9. Gu M, Han X, Liu X, Sui F, Zhang Q, Pan S. Predictive value of annexin A1 for disease severity and prognosis in patients with community-acquired pneumonia. Diagnostics. 2023;13(3):396. doi:10.3390/diagnostics13030396
10. Cerda-Mancillas MC, Santiago-Germán D, Andrade-Bravo B, et al. D-dimer as A biomarker of severity and adverse outcomes in patients with community acquired pneumonia. Arch Med Res. 2020;51(5):429–435. doi:10.1016/j.arcmed.2020.04.014
11. Li Q, Wu T, Li S. MiR-181b serves as diagnosis and prognosis biomarker in severe community-acquired pneumonia. Genet Mol Biol. 2021;44(3):e20200431. doi:10.1590/1678-4685-GMB-2020-0431
12. Liu H-Y, Xiang H-X, Xiang Y, et al. The associations of serum S100A9 with the severity and prognosis in patients with community-acquired pneumonia: a prospective cohort study. BMC Infect Dis. 2021;21(1):327. doi:10.1186/s12879-021-06020-y
13. Cheng J-Y, Tang M-M, Fang P, et al. Longitudinal associations of serum survivin with the severity and prognosis of community-acquired pneumonia patients. Respir Investig. 2023;61(1):84–94. doi:10.1016/j.resinv.2022.09.007
14. Xu Z, Wang X-M, Cao P, et al. Serum IL-27 predicts the severity and prognosis in patients with community-acquired pneumonia: a prospective cohort study. Int J Med Sci. 2022;19(1):74–81. doi:10.7150/ijms.67028
15. Broeckaert F, Clippe A, Knoops B, Hermans C, Bernard A. Clara cell secretory protein (CC16): features as a peripheral lung biomarker. Ann N Y Acad Sci. 2000;923:68–77. doi:10.1111/j.1749-6632.2000.tb05520.x
16. Broeckaert F, Bernard A. Clara cell secretory protein (CC16): characteristics and perspectives as lung peripheral biomarker. Clin Exp Allergy. 2000;30(4):469–475. doi:10.1046/j.1365-2222.2000.00760.x
17. Manning CM, Johnston CJ, Hernady E, et al. Exacerbation of lung radiation injury by viral infection: the role of Clara cells and Clara cell secretory protein. Radiat Res. 2013;179(6):617–629. doi:10.1667/RR3279.1
18. Mukherjee AB, Zhang Z, Chilton BS. Uteroglobin: a steroid-inducible immunomodulatory protein that founded the Secretoglobin superfamily. Endocr Rev. 2007;28(7):707–725. doi:10.1210/er.2007-0018
19. Lakind JS, Holgate ST, Ownby DR, et al. A critical review of the use of Clara cell secretory protein (CC16) as a biomarker of acute or chronic pulmonary effects. Biomarkers. 2007;12(5):445–467. doi:10.1080/13547500701359327
20. Briana DD, Gourgiotis D, Boutsikou M, et al. Clara cell protein in full-term pregnancies: the influence of intrauterine growth restriction. Pediatr Pulmonol. 2010;45(12):1186–1191. doi:10.1002/ppul.21305
21. Rong B, Fu T, Gao W, et al. Reduced serum concentration of CC16 is associated with severity of chronic obstructive pulmonary disease and contributes to the diagnosis and assessment of the disease. Int J Chron Obstruct Pulmon Dis. 2020;15:461–470. doi:10.2147/COPD.S230323
22. Kropski JA, Fremont RD, Calfee CS, Ware LB. Clara cell protein (CC16), a marker of lung epithelial injury, is decreased in plasma and pulmonary edema fluid from patients with acute lung injury. Chest. 2009;135(6):1440–1447. doi:10.1378/chest.08-2465
23. Zhang S, Jia Q, Song J, et al. Clinical significance of CC16 and IL-12 in bronchoalveolar lavage fluid of various stages of silicosis. Ann Palliat Med. 2020;9(6):3848–3856. doi:10.21037/apm-20-1838
24. Laucho-Contreras ME, Polverino F, Tesfaigzi Y, Pilon A, Celli BR, Owen CA. Club cell protein 16 (CC16) augmentation: a potential disease-modifying approach for Chronic Obstructive Pulmonary Disease (COPD). Expert Opin Ther Targets. 2016;20(7):869–883. doi:10.1517/14728222.2016.1139084
25. Tsoumakidou M, Bouloukaki I, Thimaki K, Tzanakis N, Siafakas NM. Innate immunity proteins in chronic obstructive pulmonary disease and idiopathic pulmonary fibrosis. Exp Lung Res. 2010;36(6):373–380. doi:10.3109/01902141003690389
26. Janssen R, Sato H, Grutters JC, et al. Study of Clara cell 16, KL-6, and surfactant protein-D in serum as disease markers in pulmonary sarcoidosis. Chest. 2003;124(6):2119–2125. doi:10.1378/chest.124.6.2119
27. Martin AC, Laing IA, Khoo SK, et al. Acute asthma in children: relationships among CD14 and CC16 genotypes, plasma levels, and severity. Am J Respir Crit Care Med. 2006;173(6):617–622. doi:10.1164/rccm.200509-1367OC
28. Lam DC, Kwok HH, Yu WC, et al. CC16 levels correlate with cigarette smoke exposure in bronchial epithelial cells and with lung function decline in smokers. BMC Pulm Med. 2018;18(1):47. doi:10.1186/s12890-018-0607-7
29. Chakrabarti A, Nguyen A, Newhams MM, et al. Surfactant protein D is a biomarker of influenza-related pediatric lung injury. Pediatr Pulmonol. 2022;57(2):519–528. doi:10.1002/ppul.25776
30. Iannuzo N, Dy ABC, Guerra S, Langlais PR, Ledford JG. The impact of CC16 on pulmonary epithelial-driven host responses during mycoplasma pneumoniae infection in mouse tracheal epithelial cells. Cells. 2023;12(15):1984. doi:10.3390/cells12151984
31. Feng CM, Cheng JY, Xu Z, et al. Associations of serum resistin with the severity and prognosis in patients with community-acquired pneumonia. Front Immunol. 2021;12:703515. doi:10.3389/fimmu.2021.703515
32. Cao B, Huang Y, She DY, et al. Diagnosis and treatment of community-acquired pneumonia in adults: 2016 Clinical Practice Guidelines by the Chinese Thoracic Society, Chinese Medical Association. Clin Respir J. 2018;12:1320–1360. doi:10.1111/crj.12674
33. Cao LF, Cheng JY, Xu Z, et al. Serum 8-Hydroxydeoxyguanosine is a potential indicator for the severity and prognosis in patients with community-acquired pneumonia: a prospective cohort study. J Immunol. 2022;208(2):321–327. doi:10.4049/jimmunol.2100711
34. Jiang X, Huang CM, Feng CM, Xu Z, Fu L, Wang XM. Associations of serum S100A12 with severity and prognosis in patients with community-acquired pneumonia: a prospective cohort study. Front Immunol. 2021;12:714026. doi:10.3389/fimmu.2021.714026
35. Marti C, Garin N, Grosgurin O, et al. Prediction of severe community-acquired pneumonia: a systematic review and meta-analysis. Crit Care. 2012;16(4):R141. doi:10.1186/cc11447
36. Kollef KE, Reichley RM, Micek ST, Kollef MH. The modified APACHE II score outperforms Curb65 pneumonia severity score as a predictor of 30-day mortality in patients with methicillin-resistant Staphylococcus aureus pneumonia. Chest. 2008;133(2):363–369. doi:10.1378/chest.07-1825
37. Feng CM, Wang XM, Li MD, et al. Serum interleukin-17 predicts severity and prognosis in patients with community acquired pneumonia: a prospective cohort study. BMC Pulm Med. 2021;21(1):393. doi:10.1186/s12890-021-01770-6
38. Zheng L, Fei J, Feng CM, Xu Z, Fu L, Zhao H. Serum 8-iso-PGF2α predicts the severity and prognosis in patients with community-acquired pneumonia: a retrospective cohort study. Front Med. 2021;8:633442. doi:10.3389/fmed.2021.633442
39. Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019;200(7):e45–e67. doi:10.1164/rccm.201908-1581ST
40. Fu L, Zhao H, Xiang Y, et al. Reactive oxygen species-evoked endoplasmic reticulum stress mediates 1-nitropyrene-induced epithelial-mesenchymal transition and pulmonary fibrosis. Environ Pollut. 2021;283:117134. doi:10.1016/j.envpol.2021.117134
41. Zheng L, Jiang YL, Fei J, et al. Circulatory cadmium positively correlates with epithelial-mesenchymal transition in patients with chronic obstructive pulmonary disease. Ecotoxicol Environ Saf. 2021;215:112164. doi:10.1016/j.ecoenv.2021.112164
42. Jiang YL, Fei J, Cao P, et al. Serum cadmium positively correlates with inflammatory cytokines in patients with chronic obstructive pulmonary disease. Environ Toxicol. 2022;37(1):151–160. doi:10.1002/tox.23386
43. Fei J, Fu L, Cao W, Hu B, Zhao H, Li JB. Low vitamin D status is associated with epithelial-mesenchymal transition in patients with chronic obstructive pulmonary disease. J Immunol. 2019;203(6):1428–1435. doi:10.4049/jimmunol.1900229
44. Fu L, Fei J, Tan ZX, et al. Low vitamin D status is associated with inflammation in patients with chronic obstructive pulmonary disease. J Immunol. 2021;206(3):515–523. doi:10.4049/jimmunol.2000964
45. Arsalane K, Broeckaert F, Knoops B, Wiedig M, Toubeau G, Bernard A. Clara cell specific protein (CC16) expression after acute lung inflammation induced by intratracheal lipopolysaccharide administration. Am J Respir Crit Care Med. 2000;161(5):1624–1630. doi:10.1164/ajrccm.161.5.9812157
46. Sarkar K, Dhatrak S, Sarkar B, Ojha UC, Raghav P, Pagdhune A. Secondary prevention of silicosis and silico-tuberculosis by periodic screening of silica dust exposed workers using serum club cell protein 16 as a proxy marker. Health Sci Rep. 2021;4(3):e373. doi:10.1002/hsr2.373
47. Fu L, Li XY, Fei J, et al. Myocardial injury at early stage and its association with the risk of death in COVID-19 patients: a hospital-based retrospective cohort study. Front Cardiovasc Med. 2020;7:590688. doi:10.3389/fcvm.2020.590688
48. Fu L, Fei J, Xu S, et al. Liver dysfunction and its association with the risk of death in COVID-19 patients: a prospective cohort study. J Clin Transl Hepatol. 2020;8(3):246–254. doi:10.14218/JCTH.2020.00043
49. Xiang HX, Fei J, Xiang Y, et al. Renal dysfunction and prognosis of COVID-19 patients: a hospital-based retrospective cohort study. BMC Infect Dis. 2021;21(1):158. doi:10.1186/s12879-021-05861-x
50. Wang J, Zhao Y, Pan L, He X, Zhang X. The relationship between the expression of serum IL-18 mRNA, CC16, and sTREM-1 and the severity and prognosis of ventilator-associated pneumonia in elderly patients. Ann Palliat Med. 2021;10(12):12767–12774. doi:10.21037/apm-21-3511
51. Guerra S, Vasquez MM, Spangenberg A, Halonen M, Martinez FD. Serum concentrations of club cell secretory protein (Clara) and cancer mortality in adults: a population-based, prospective cohort study. Lancet Respir Med. 2013;1(10):779–785. doi:10.1016/S2213-2600(13)70220-0
52. Halatek T, Sinczuk-Walczak H, Rydzynski K. Prognostic significance of low serum levels of Clara cell phospholipid-binding protein in occupational aluminium neurotoxicity. J Inorg Biochem. 2005;99(9):1904–1911. doi:10.1016/j.jinorgbio.2005.06.027
53. Johnson MDL, Younis US, Menghani SV, et al. CC16 binding to α4β1 integrin protects against mycoplasma pneumoniae infection. Am J Respir Crit Care Med. 2021;203(11):1410–1418. doi:10.1164/rccm.202006-2576OC
54. Park HY, Churg A, Wright JL, et al. Club cell protein 16 and disease progression in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;188(12):1413–1419. doi:10.1164/rccm.201305-0892OC
55. Guerra S, Halonen M, Vasquez MM, et al. Relation between circulating CC16 concentrations, lung function, and development of chronic obstructive pulmonary disease across the lifespan: a prospective study. Lancet Respir Med. 2015;3(8):613–620. doi:10.1016/S2213-2600(15)00196-4
56. Hsu HS, Liu CC, Lin JH, Hsu TW, Su K, Hung SC. Repair of naphthalene-induced acute tracheal injury by basal cells depends on β-catenin. J Thorac Cardiovasc Surg. 2014;148(1):322–332. doi:10.1016/j.jtcvs.2013.10.039
57. Sarker RSJ, Conlon TM, Morrone C, et al. CARM1 regulates senescence during airway epithelial cell injury in COPD pathogenesis. Am J Physiol Lung Cell Mol Physiol. 2019;317(5):L602–L614. doi:10.1152/ajplung.00441.2018
58. Yin W, Cao W, Zhou G, et al. Analysis of pathological changes in the epithelium in COVID-19 patient airways. ERJ Open Res. 2021;7(2):00690–02020. doi:10.1183/23120541.00690-2020
59. Almuntashiri S, James C, Wang X, Siddiqui B, Zhang D. The potential of lung epithelium specific proteins as biomarkers for COVID-19-associated lung injury. Diagnostics. 2021;11(9):1643. doi:10.3390/diagnostics11091643
60. Almuntashiri S, Han Y, Zhu Y, et al. CC16 regulates inflammation, ROS generation and apoptosis in bronchial epithelial cells during Klebsiella pneumoniae infection. Int J Mol Sci. 2021;22(21):11459. doi:10.3390/ijms222111459
61. Lee J, Komatsu K, Lee BC, et al. Phosphodiesterase 4B mediates extracellular signal-regulated kinase-dependent up-regulation of mucin MUC5AC protein by Streptococcus pneumoniae by inhibiting cAMP-protein kinase A-dependent MKP-1 phosphatase pathway. J Biol Chem. 2012;287(27):22799–22811. doi:10.1074/jbc.M111.337378
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.