")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 17
Associations of LRP5 and MTHFR Gene Variants with Osteoarthritis Prevalence in Elderly Women: A Japanese Cohort Survey Randomly Sampled from a Basic Resident Registry
Authors Nakano M, Yui H, Kikugawa S , Tokida R, Sakai N, Kondo N, Endo N, Haro H, Shimodaira H, Suzuki T, Kato H, Takahashi J , Nakamura Y
Received 21 July 2021
Accepted for publication 5 September 2021
Published 29 September 2021 Volume 2021:17 Pages 1065—1073
DOI https://doi.org/10.2147/TCRM.S330530
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Masaki Nakano,1,* Haruka Yui,1,* Shingo Kikugawa,2 Ryosuke Tokida,3 Noriko Sakai,4 Naoki Kondo,5 Naoto Endo,5 Hirotaka Haro,6 Hiroki Shimodaira,1 Takako Suzuki,1,7 Hiroyuki Kato,1 Jun Takahashi,1 Yukio Nakamura1
1Department of Orthopaedic Surgery, Shinshu University School of Medicine, Matsumoto, Nagano, 390-8621, Japan; 2DNA Chip Research Inc., Minato-ku, Tokyo, 105-0022, Japan; 3Rehabilitation Center, Shinshu University Hospital, Matsumoto, Nagano, 390-8621, Japan; 4Department of Orthopaedic Surgery, New Life Hospital, Obuse, Nagano, 381-0295, Japan; 5Division of Orthopedic Surgery, Department of Regenerative and Transplant Medicine, Niigata University Graduate School of Medical and Dental Sciences, Chuo-ku, Niigata, 951-8510, Japan; 6Department of Orthopaedic Surgery, University of Yamanashi Graduate School of Medicine, Chuo, Yamanashi, 409-3898, Japan; 7Department of Human Nutrition, Faculty of Human Nutrition, Tokyo Kasei Gakuin University, Chiyoda-ku, Tokyo, 102-8341, Japan
*These authors contributed equally to this work
Correspondence: Yukio Nakamura
Department of Orthopaedic Surgery, Shinshu University School of Medicine, 3-1-1 Asahi, Matsumoto, Nagano, 390-8621, Japan
Tel +81-263-37-2659
Fax +81-263-35-8844
Email [email protected]
Objective: Osteoarthritis (OA) is a common and degenerative joint disorder in the elderly. A greater importance of understanding the relationship between genetic factors and OA prevalence has emerged with population aging. We therefore investigated the associations of several bone disease-related genetic variants with the prevalence of OA and osteoporosis in Japanese elderly women from the Obuse study cohort, which was randomly sampled from a basic town resident registry.
Methods and Results: In total, 206 female participants (mean ± standard deviation age: 69.7 ± 11.0 years) who completed OA, bone mineral density, and genotype assessments were included. The number of patients diagnosed as having knee/hip OA and osteoporosis was 59 (28.6%) and 30 (14.6%), respectively. Fisher’s exact testing revealed significant relationships between the minor T allele of LDL receptor related protein 5 (LRP5) rs3736228 and the prevalence of knee/hip OA and osteoporosis. The respective odds ratios (ORs) of the TT genotype for knee/hip OA and osteoporosis were 7.28 (95% confidence interval [CI] 2.22– 28.08) and 5.24 (95% CI 0.95– 26.98). An additional subgroup analysis for knee OA revealed that the frequency of the common C allele of methylenetetrahydrofolate reductase (MTHFR) rs1801133 had a statistically significant protective association with the prevalence of knee OA (OR 0.58, 95% CI 0.35– 0.97).
Conclusion: In sum, the present study demonstrated significant associations of LRP5 rs3736228 and MTHFR rs1801133 with knee/hip OA and osteoporosis prevalences and knee OA prevalence, respectively, in Japanese elderly women. These results will help further the understanding of OA pathogenesis and related genetic risk factors.
Keywords: genetic variant, LRP5, MTHFR, osteoarthritis, osteoporosis
Introduction
Osteoarthritis (OA) is a common degenerative joint disorder occurring with age whose pathophysiology remains incompletely understood. At present, almost all non-surgical treatment options for OA are limited to analgesis and improving joint movement, with no fundamental cures.1 Osteoporosis is a widespread metabolic skeletal disease characterized by diminished bone mineral density (BMD) or bone strength, both of which increase the risk of fractures. Although several effective medications exist,2 both osteoporosis and OA are becoming major worldwide health concerns with population aging and rising health-care costs. Therefore, understanding the genetic risk factors for these disorders has emerged as an important issue for disease prevention and therapeutic management.
Many studies on the association of genetic factors with OA and osteoporosis have been reported to date. In the present day, the relationships among genetic variants and related disorders are generally investigated by genome-wide association studies (GWAS). Regarding the prevalence of OA and osteoporosis, 256 and 22 records, respectively, were found in the GWAS catalog (https://www.ebi.ac.uk/gwas/).3 Several gene polymorphisms appear to affect OA as well as osteoporosis. Indeed, associations of gene variants in LDL receptor related protein 5 (LRP5),4,5 growth differentiation factor 5 (GDF5),6,7 and SMAD family member 3 (SMAD3)8,9 with OA prevalence have been reported. In addition, we very recently uncovered a novel association between a homocysteine metabolism-related methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism (rs1801133), which was reportedly related to osteoporosis, and the progression of spinal OA.10
We have recently established a new population-based epidemiological study of Japanese people that employs random sampling from the basic resident registry of Obuse, a rural town in Japan.11,12 The Obuse study contains detailed medical information on the community-dwelling elderly population with minimized selection bias, which allows for examination of a cohort representative of the general population. The present study aimed to investigate the associations of several reported bone disease-related genetic variants, including MTHFR rs1801133, with the prevalence of OA and osteoporosis in elderly women sampled from the Obuse study cohort. Significant associations were seen for LRP5 rs3736228 with the prevalence of knee/hip OA and osteoporosis, and for MTHFR rs1801133 with knee OA prevalence in Japanese elderly women.
Methods
The study protocol of this investigation for human research was approved by the investigational ethics review board of Shinshu University Hospital, Japan (approval number: 2792). The research procedure was carried out in accordance with the ethical guidelines of the 2013 Declaration of Helsinki. Written informed consent for research and publication was provided by all participants prior to the initiation of the study.
Study Subjects
The Obuse study was launched in October 2014 for epidemiological data collection until June 2017. The study randomly sampled 1297 male and female individuals from 5352 members of the resident population between 50–89 years of age in the basic resident registry of Obuse town (Nagano Prefecture, Japan) as a joint collaboration with the cooperating town office. In total, 203 male and 212 female participants provided written informed consent and were enrolled in the Obuse study. The current investigation included 206 female subjects who completed assessments of knee and hip OA, BMD measurements of the total hips and lumbar spine, and genotype determination of the gene variants of interest. Due to budget constraints, we analyzed only female subjects who were susceptible to systemic skeletal disorders including OA and osteoporosis compared to males.
Assessment of OA and Osteoporosis
OA of the knee and hip was assessed by radiographic examination. The degree of degeneration was evaluated in accordance with the Kellgren–Lawrence (KL) grading system.13 Radiographs were examined by 2 experienced orthopaedic surgeons (H.S. and Y.N.). The subjects with the worst KL grading of ≥ 3 in either side of the knees or hips, or who had undergone arthroplasty for OA were judged as OA patients. The subjects with persistent joint pain and tenderness were also radiologically assessed as having OA. BMD at the lumbar spine and hips was measured using dual-energy X-ray absorptiometry (DXA; PRODIGY, GE Healthcare, Chicago, IL). The regions of interest for lumbar and hip BMD were the L2–4 spinal and bilateral total hip regions, respectively. Subjects with BMD values of ≤ 70% of the young adult mean (YAM) for either the lumbar region or total hips were diagnosed as having osteoporosis.14
Determination of Genetic Variants
Cell-free DNA (cfDNA) was extracted from plasma samples of study subjects using a QIAamp Circulating Nucleic Acid Kit (Qiagen, Venlo, Netherlands) according to the manufacturer’s instructions. Genotyping assays were performed by a droplet digital polymerase chain reaction (ddPCR) QX200 system (Bio-Rad, Hercules, CA). Reaction mixture aliquots of 20 µL containing 10 µL 2 × ddPCR Supermix, 5 µL cfDNA sample, and 0.5 µL 40 × TaqMan SNP Genotyping Assay for each variant (Applied Biosystems, Waltham, MA) were prepared. The droplets were generated with a QX200 droplet generator and carefully transferred to 96-well PCR plates. After PCR cycling (40 cycles of 94°C for 30 s and 60°C for 1 min), the fluorescence of each droplet was determined using a QX200 droplet reader followed by analysis with QuantaSoft version 1.7.4 software (Bio-Rad). The present study examined the following genetic variants: LRP5 rs312009 and rs3736228, GDF5 rs143383, SMAD3 rs12901499, and MTHFR rs1801133.
Statistical Analysis
The background characteristic data of each study group (healthy control, OA, osteoporosis, and comorbid with OA and osteoporosis) are presented as the mean ± standard deviation (SD) together with the median value. Fisher’s exact test was performed to calculate the odds ratio (OR) and 95% confidence interval (CI) of variant genotypes and alleles for the prevalence of OA and osteoporosis versus healthy controls. To examine the population homogeneity of the study participants, Haldane’s exact test for Hardy–Weinberg equilibrium (HWE) was calculated. All statistical tests were carried out by using R version 3.4 software.15 A two-tailed P-value of < 0.05 was considered statistically significant in this study.
Results
Background Characteristics of Study Subjects
The average ± SD age of the 206 female subjects at enrollment was 69.7 ± 11.0 years. The number of patients diagnosed as having OA and osteoporosis was 51 (24.8%; knee: 40, hip: 3, knee and hip: 8) and 22 (10.7%), respectively. Eight patients (3.9%) suffered from both osteoporosis and OA (knee: 6, hip: 1, knee and hip: 1) and were classified into the comorbid group. One hundred and twenty-five subjects having neither OA nor osteoporosis were defined as healthy controls in this study. The background characteristics of the study groups are summarized in Table 1.
 |
Table 1 Background Characteristics of the Study Groups |
Associations of Genotype and Allele Frequencies with OA and Osteoporosis
In the present cohort, we observed no remarkable associations for LRP5 rs312009, GDF5 rs143383, or SMAD3 rs12901499 with both OA and osteoporosis prevalence (Tables 2 and 3 and Figures 1 and 2). In contrast, the minor T allele of LRP5 rs3736228 and its homozygotic genotype showed significant relationships with the prevalence rate of knee/hip OA. The ORs of the TT genotype and T allele for OA compared with healthy controls were 7.28 (95% CI 2.22–28.08; P < 0.001) and 1.80 (95% CI 1.07–3.00; P < 0.05), respectively (Table 2 and Figure 1). Although not significantly, the common C allele of MTHFR rs1801133 tended to protect against knee/hip OA prevalence. The respective ORs of the CC genotype and C allele for OA were 0.55 (95% CI 0.23–1.22; P = 0.15) and 0.70 (95% CI 0.43–1.14; P = 0.13) versus the healthy control group (Table 2 and Figure 1). The prevalence rate of osteoporosis was significantly correlated with the TT genotype of LRP5 rs3736228 (OR 5.24, 95% CI 0.95–26.98; P < 0.05) (Table 3 and Figure 2). The distributions of genotype frequencies were in Hardy–Weinberg equilibrium (HWE P-value > 0.05).
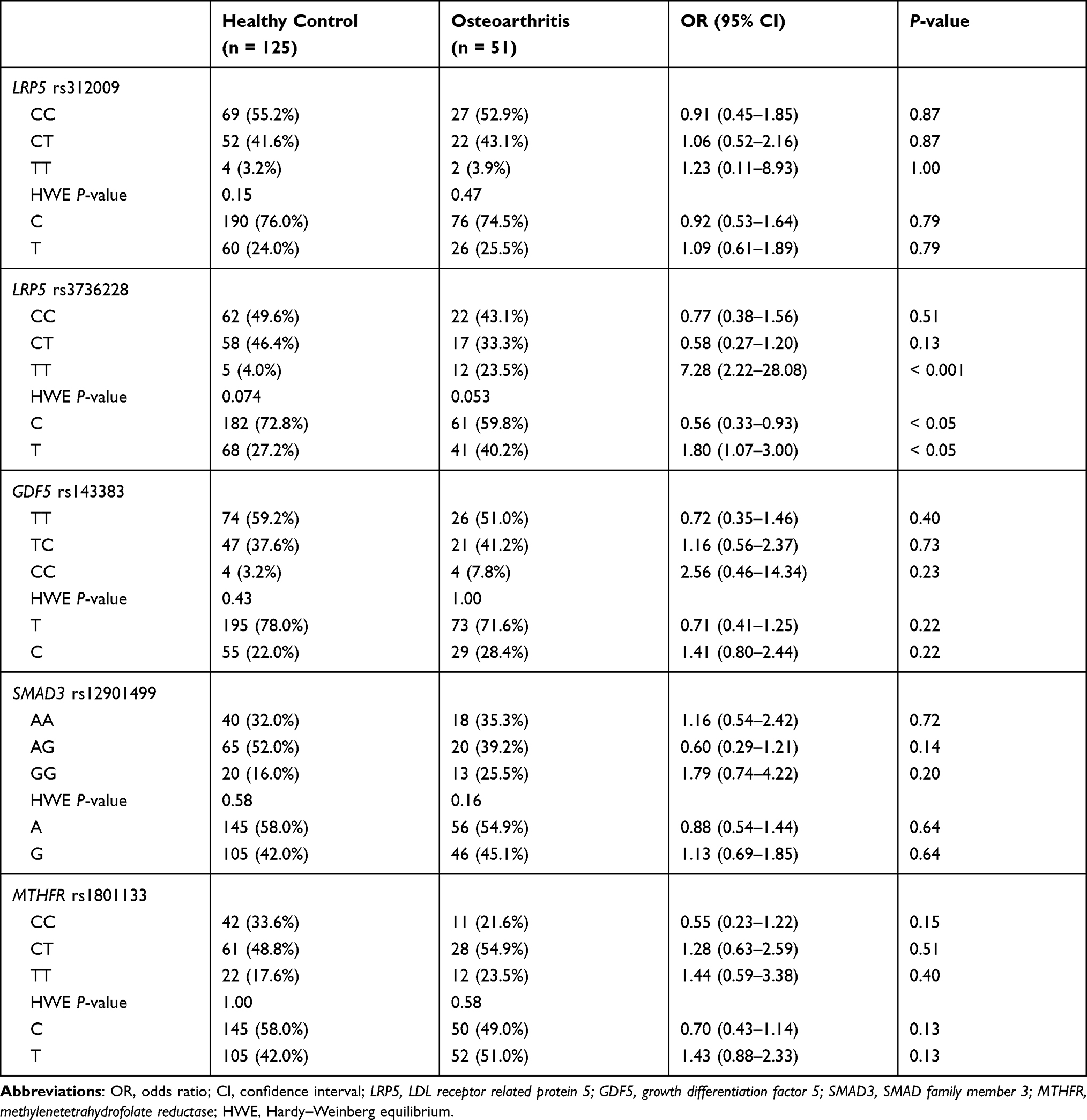 |
Table 2 Genotype and Allele Frequencies in Patients with Osteoarthritis |
 |
Table 3 Genotype and Allele Frequencies in Patients with Osteoporosis |
 |
Figure 1 Odds ratios for osteoarthritis by each variant genotype. Fisher’s exact test was employed to calculate the odds ratio and 95% confidence interval of variant genotypes for the prevalence of osteoarthritis versus the healthy control group. Abbreviations: LRP5, LDL receptor related protein 5; GDF5, growth differentiation factor 5; SMAD3, SMAD family member 3; MTHFR, methylenetetrahydrofolate reductase. |
 |
Figure 2 Odds ratios for osteoporosis by each variant genotype. Fisher’s exact test was employed to calculate the odds ratio and 95% confidence interval of variant genotypes for the prevalence of osteoporosis versus the healthy control group. Abbreviations: LRP5, LDL receptor related protein 5; GDF5, growth differentiation factor 5; SMAD3, SMAD family member 3; MTHFR, methylenetetrahydrofolate reductase. |
Subgroup Analysis for Knee OA Prevalence
In a subgroup analysis, we focused on the prevalence of knee OA, which was the most common disorder witnessed in this study. In knee OA only or knee OA + comorbid osteoporosis patients, both the TT genotype (P < 0.001) and T allele (P < 0.05) of LRP5 rs3736228 associated significantly with knee OA prevalence as compared with healthy controls (Table 4). Moreover, the C allele of MTHFR rs1801133 demonstrated a statistically significant protective association with the prevalence rate of knee OA (OR 0.58, 95% CI 0.35–0.97; P < 0.05) in the knee OA + comorbid osteoporosis subgroup (Table 4).
 |
Table 4 Subgroup Analysis of Patients with Knee Osteoarthritis |
Discussion
This study demonstrated a significant relationship between LRP5 rs3736228 and the skeletal disorders of OA and osteoporosis in elderly community-dwelling female residents randomly sampled from a Japanese town resident registry. A statistically significant protective association of the common allele of MTHFR rs1801133 with knee OA prevalence was also observed. As the population sampling of our cohort minimized selection bias, our results might be considered reflective of the Japanese general population.
LRP5 and 6 (LRP5/6) are required as co-receptors for canonical Wnt signaling16,17 and play important roles in skeletal development and metabolism. A number of LRP5 gene variants have been reported. Of those, associations of the missense variants LRP5 rs3736228 (Ala1330Val) and rs4988321 (Val667Met) with decreased BMD and the risk of osteoporotic fracture are well described.18,19 In particular, a relationship between LRP5 A1330V and diminished BMD has been identified in the Japanese population as well.20,21 A loss of function in LRP5 increased cartilage degradation in a mouse model22 and was also suggested to be associated with OA. However, little is known on the precise connection between OA and LRP5 gene variants. Although associations of LRP5 rs41494349 (Gln89Arg) with spinal OA4 and LRP5 rs3736228 with knee OA5 have been reported, no information has been recorded in the GWAS catalog to date (https://www.ebi.ac.uk/gwas/).3 Therefore, the findings of this study demonstrating a relationship between the T allele of LRP5 rs3736228 and knee/hip OA prevalence in a randomly sampled population cohort will be of value for further understanding the relationship between OA development and the pathophysiological role of LRP5 dysfunction.
In the subgroup analysis for knee OA, there was a protective association for the common C allele of MTHFR rs1801133 (Ala222Val) rather than a risk association of the minor T allele with the prevalence rate of knee OA. MTHFR is known to act within the methionine cycle and plays an essential role in homocysteine clearance. A functional deficiency of the MTHFR enzyme leads to mild elevation of circulating homocysteine levels.23 The A222V missense variant is a common mutation in the MTHFR gene that causes dysfunctional enzymatic activity. Notably, the T allele of MTHFR rs1801133 has been implicated in decreased BMD and the occurrence of osteoporotic fractures,24,25 and we very recently uncovered a relationship among homocysteine, MTHFR rs1801133, and spinal OA in Japanese postmenopausal women.10 The results of the present study imply a correlation between diminished homocysteine levels and a lowered risk of knee OA prevalence. Since circulating homocysteine levels can be decreased by vitamin B group supplementation,26 the significance of B-vitamins intervention in individuals bearing the T allele of MTHFR rs1801133 for preventing OA development may warrant further investigation.
An intron variant of LRP5 gene rs312009 as well as GDF5 rs143383 and SMAD3 rs12901499 showed no remarkable correlations with OA or osteoporosis prevalence in this study. The rs143383 is located in the 5′-untranslated region core promotor of GDF5, which encodes a chondrogenic protein. A relationship of rs143383 with OA has been demonstrated in various racial groups, including a Japanese cohort.6,7 On the other hand, SMAD3 is a member of the SMAD family of proteins and plays an essential role in mediating the transforming growth factor-beta signaling pathway. A genetic variant, rs12901499, within the intron 1 of SMAD3 is reportedly associated with OA in Caucasian and Asian populations.8,9 However, other studies have shown no relationship for either GDF5 rs143383 or SMAD3 rs12901499 with OA prevalence.27,28 Relatively small number of samples limited to female subjects is a limitation of the current study. Besides, although the subjects were randomly sampled from a resident registry, there was a potential for selection bias due to the low participation rate (32.0%) as a result of the noncompulsory survey design. Furthermore, since it sampled from a single town in Japan, this study might contain local features that should be considered when interpreting the data. Future studies with larger sample size and male subjects that include multiple regions in Japan and/or other Asian countries will overcome the controversial issues. Further investigations including experimental study on the mechanisms and/or pathways will be required as well.
Conclusion
We observed significant associations of LRP5 rs3736228 and MTHFR rs1801133 with knee/hip OA and osteoporosis prevalences and knee OA prevalence, respectively, in Japanese elderly women from the randomly sampled Obuse study cohort. The results of the present study will help further the understanding of OA pathogenesis and related genetic risk factors, which will contribute to improved disease prevention and therapeutic management.
Acknowledgments
This work was supported by a grant from the JOA-Subsidized Science Project Research 2018–2020 to Y.N. We would like to thank Dr. Takashi Igarashi of the Center for Clinical Research at Shinshu University Hospital, Dr. Hironobu Sato of the Obuse Town Institute for Community Health Promotion, and the Obuse Town Office for sample selection in this study. Our gratitude extends to Mr. Trevor Ralph for English language editing as well as all participants in the present study.
Disclosure
All of the authors have declared that there were no conflicts of interest in this study.
References
1. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745–1759. doi:10.1016/S0140-6736(19)30417-9
2. Ensrud KE, Crandall CJ. Osteoporosis. Ann Intern Med. 2017;167(3):ITC17–ITC32. doi:10.7326/AITC201708010
3. Welter D, MacArthur J, Morales J, et al. The NHGRI GWAS catalog, a curated resource of SNP-trait associations. Nucleic Acids Res. 2014;42(Database issue):D1001–D1006. doi:10.1093/nar/gkt1229
4. Urano T, Shiraki M, Narusawa K, et al. Q89R polymorphism in the LDL receptor-related protein 5 gene is associated with spinal osteoarthritis in postmenopausal Japanese women. Spine. 2007;32:25–29. doi:10.1097/01.brs.0000251003.62212.5b
5. Yerges-Armstrong LM, Yau MS, Liu Y, et al. Association analysis of BMD-associated SNPs with knee osteoarthritis. J Bone Miner Res. 2014;29(6):1373–1379. doi:10.1002/jbmr.2160
6. Miyamoto Y, Mabuchi A, Shi D, et al. A functional polymorphism in the 5’ UTR of GDF5 is associated with susceptibility to osteoarthritis. Nat Genet. 2007;39(4):529–533. doi:10.1038/2005
7. Chapman K, Takahashi A, Meulenbelt I, et al. A meta-analysis of European and Asian cohorts reveals a global role of a functional SNP in the 5’ UTR of GDF5 with osteoarthritis susceptibility. Hum Mol Genet. 2008;17(10):1497–1504. doi:10.1093/hmg/ddn038
8. Valdes AM, Spector TD, Tamm A, et al. Genetic variation in the SMAD3 gene is associated with hip and knee osteoarthritis. Arthritis Rheum. 2010;62(8):2347–2352. doi:10.1002/art.27530
9. Yang HY, Hu WH, Jiang T, Zhao H. SMAD3 gene rs12901499 polymorphism increased the risk of osteoarthritis. Biosci Rep. 2018;38(3):BSR20180380. doi:10.1042/BSR20180380
10. Nakano M, Nakamura Y, Urano T, et al. Associations of homocysteine metabolism with the risk of spinal osteoarthritis progression in postmenopausal women. J Clin Endocrinol Metab. 2021;dgab591. doi:10.1210/clinem/dgab591
11. Uehara M, Takahashi J, Ikegami S, et al. Sagittal spinal alignment deviation in the general elderly population: a Japanese cohort survey randomly sampled from a basic resident registry. Spine J. 2019;19(2):349–356. doi:10.1016/j.spinee.2018.06.346
12. Tokida R, Ikegami S, Takahashi J, et al. Association between musculoskeletal function deterioration and locomotive syndrome in the general elderly population: a Japanese cohort survey randomly sampled from a basic resident registry. BMC Musculoskelet Disord. 2020;21(1):431. doi:10.1186/s12891-020-03469-x
13. Ball J, Jeffrey MR, Kellgren JH, Editors. The Epidemiology of Chronic Rheumatism: Atlas of Standard Radiographs of Arthritis. Oxford, UK: Blackwell Scientific Publications; 1963.
14. Soen S, Fukunaga M, Sugimoto T, et al. Japanese society for bone and mineral research and japan osteoporosis society joint review committee for the revision of the diagnostic criteria for primary osteoporosis. Diagnostic criteria for primary osteoporosis: year 2012 revision. J Bone Miner Metab. 2013;31(3):247–257. doi:10.1007/s00774-013-0447-8
15. R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2017. Available from: https://www.r-project.org/.
16. Tamai K, Semenov M, Kato Y, et al. LDL-receptor-related proteins in Wnt signal transduction. Nature. 2000;407(6803):530–535. doi:10.1038/35035117
17. Pinson KI, Brennan J, Monkley S, Avery BJ, Skarnes WC. An LDL-receptor-related protein mediates Wnt signalling in mice. Nature. 2000;407(6803):535–538. doi:10.1038/35035124
18. van Meurs JB, Trikalinos TA, Ralston SH, et al; GENOMOS Study. Large-scale analysis of association between LRP5 and LRP6 variants and osteoporosis. JAMA. 2008;299(11):1277–1290. doi:10.1001/jama.299.11.1277
19. Richards JB, Rivadeneira F, Inouye M, et al. Bone mineral density, osteoporosis, and osteoporotic fractures: a genome-wide association study. Lancet. 2008;371(9623):1505–1512. doi:10.1016/S0140-6736(08)60599-1
20. Ezura Y, Nakajima T, Urano T, et al. Association of a single-nucleotide variation (A1330V) in the low-density lipoprotein receptor-related protein 5 gene (LRP5) with bone mineral density in adult Japanese women. Bone. 2007;40(4):997–1005. doi:10.1016/j.bone.2005.06.025
21. Urano T, Shiraki M, Usui T, Sasaki N, Ouchi Y, Inoue S. A1330V variant of the low-density lipoprotein receptor-related protein 5 (LRP5) gene decreases Wnt signaling and affects the total body bone mineral density in Japanese women. Endocr J. 2009;56(4):625–631. doi:10.1507/endocrj.K09E-133
22. Lodewyckx L, Luyten FP, Lories RJ. Genetic deletion of low-density lipoprotein receptor-related protein 5 increases cartilage degradation in instability-induced osteoarthritis. Rheumatology. 2012;51(11):1973–1978. doi:10.1093/rheumatology/kes178
23. Moll S, Varga EA. Homocysteine and MTHFR mutations. Circulation. 2015;132(1):e6–e9. doi:10.1161/CIRCULATIONAHA.114.013311
24. Bathum L, von Bornemann Hjelmborg J, Christiansen L, Madsen JS, Skytthe A, Christensen K. Evidence for an association of methylene tetrahydrofolate reductase polymorphism C677T and an increased risk of fractures: results from a population-based Danish twin study. Osteoporos Int. 2004;15(8):659–664. doi:10.1007/s00198-003-1584-z
25. Shiraki M, Urano T, Kuroda T, et al. The synergistic effect of bone mineral density and methylenetetrahydrofolate reductase (MTHFR) polymorphism (C677T) on fractures. J Bone Miner Metab. 2008;26(6):595–602. doi:10.1007/s00774-008-0878-9
26. Homocysteine lowering trialists’ Collaboration. Lowering blood homocysteine with folic acid based supplements: meta-analysis of randomised trials. BMJ. 1998;316(7135):894–898. doi:10.1136/bmj.316.7135.894
27. Tsezou A, Satra M, Oikonomou P, Bargiotas K, Malizos KN. The growth differentiation factor 5 (GDF5) core promoter polymorphism is not associated with knee osteoarthritis in the Greek population. J Orthop Res. 2008;26(1):136–140. doi:10.1002/jor.20464
28. Hong JQ, Wang YX, Li SH, et al. Association between SMAD3 gene polymorphisms and osteoarthritis risk: a systematic review and meta-analysis. J Orthop Surg Res. 2018;13(1):232. doi:10.1186/s13018-018-0939-2
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.