Back to Journals » Psychology Research and Behavior Management » Volume 16
Associations Between Workplace Violence and Mental Health Among Chinese Health Technicians: A Moderated Mediation Analysis of Sleep Quality and Physical Activity
Authors Li Q ![]() , Jing W, Wei Z, Wang Y, Sun L
, Jing W, Wei Z, Wang Y, Sun L ![]()
Received 4 March 2023
Accepted for publication 31 May 2023
Published 5 June 2023 Volume 2023:16 Pages 2045—2057
DOI https://doi.org/10.2147/PRBM.S411098
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Qixiu Li,1,2 Wenhua Jing,3 Zhen Wei,1,2 Yifan Wang,1,2 Long Sun1,2
1Centre for Health Management and Policy Research, School of Public Health, Cheeloo College of Medicine, Shandong University, Jinan, Shandong, People’s Republic of China; 2National Health Commission of China (NHC) Key Laboratory of Health Economics and Policy Research (Shandong University), Jinan, Shandong, People’s Republic of China; 3Hospital Service Department, Qilu Hospital of Shandong University, Jinan, Shandong, People’s Republic of China
Correspondence: Long Sun, Centre for Health Management and Policy Research, School of Public Health, Cheeloo College of Medicine, Shandong University, 44 Wenhuaxi Road, Jinan, Shandong, 250012, People’s Republic of China, Email [email protected]
Background: Workplace violence (WPV) had always been the focus of attention in all walks of lives, especially in the health fields. Previous studies had shown it adversely affected mental health for healthcare workers. In addition, both sleep quality and physical activity were supported to have impact on mental health. However, the mechanism of sleep quality and physical activity influence the association between WPV and mental health had not been explored, so the purpose of this paper was to explore this mechanistic link among workplace violence, sleep quality, physical activity, and mental health in Chinese health technicians.
Methods: Cross-sectional study was conducted in 3 cities of China, totally 3426 valid questionnaires were collected. WPV, physical activity, and social-demographic variables were evaluated. The Pittsburgh Sleep Quality Index and the Kessler Psychological Distress Scale were used to measure sleep quality and mental health. Descriptive analysis, univariate analysis, Pearson correlation, and moderated mediation analysis were used to estimate prevalence of WPV, association between WPV and mental health, and the role of sleep quality and physical activity on association between WPV and mental health.
Results: The prevalence of WPV was 52.2% among Chinese health technicians. After controlling social-demographic and work-related variables, sleep quality partially mediated the effect of WPV on mental health (indirect effect=0.829). Physical activity moderated the relationship between WPV and sleep quality (β=0.235, p=0.013), but not find the moderating role between WPV and mental health (β=0.140, p=0.474), and between sleep quality and mental health (β=0.018, p=0.550).
Conclusion: The rate of WPV among health technicians remained at an alarming level. Sleep quality and physical activity could mitigate the adverse effect of WPV on mental health. In the future, we could improve sleep quality and encourage health technicians to engage physical activity to decrease the negative effect of WPV on mental health.
Keywords: workplace violence, mental health, sleep quality, physical activity
Background
Workplace violence (WPV) was gradually becoming a widespread public health problem, since WPV presented in almost every industry.1 WPV had been shown to have a significant impact on workers’ safety, production efficiency, physical and psychological health.2,3 It had always been the focus of attention in all walks of life, especially in the field of health care.4 As a special occupational group, medical personnels beard the social responsibility of treating the sick, saving lives, helping the wounded, and the most important was to promote health, so compared with other occupational groups, healthcare workers who experienced WPV might face greater occupational impact.5 Ferris had confirmed that WPV in healthcare settings constituted almost a quarter of total violence in all workplaces, and it was estimated that two thirds of medical staffs experienced WPV during their careers.6 The negative impact of WPV could not be underestimated. First, experience of workplace violence had a negative impact on physical and mental health of health personnels. In addition, it can affect the work of health personnels, such as poor performance, low organizational commitment, etc. It also had adverse impact on the quality of patient care and even the health system.7–9
World Health Organization defined WPV as followed in 2002, workplace violence was a behavior of an explicit or implicit challenge to the safety, well-being, or health of a person who was being abused, threatened, or attacked in their workplace.10 But in the field of health care, WPV was defined as the psychological and physical harm that doctors and nurses confronted with when providing medical service.4 The prevalence of WPV varied greatly from country to country, 95.3% nurses in Canada had suffered direct or indirect workplace violence,11 overall prevalence estimate for psychological WPV in South Korean was 11%,12 83% participants reported exposure to at least one of five forms of violence in Victorian,13 75.4% nurses in eight provinces of China had experienced some form of workplace violence,14 nearly 90% staff in psychiatric wards had experience mild physical violence,15 and the prevalence of WPV experienced by physicians was 66.19% in four provinces of China.16 However, medical staff in China might face more serious occupational hazards because of the large number of medical personnels, the large Chinese population, and the uneven distribution of medical resources, so it was of great significance to study WPV in China.
Focusing on the mental health of health technicians was necessary for their wellbeing and for healthcare quality. Therefore, several systematic reviews had described the mental health of health technicians during the COVID-19 pandemic. A pooled analysis suggested that pooled prevalence of anxiety, depression and distress among healthcare workers were 40%, 37%, and 37% respectively.17 Another review cited different results from studies of health workers in different countries. The incidence of depression in the two studies was 9.4 and 77.6, respectively, the lowest and highest incidence in this meta-analysis.18,19 Two studies on nurse anxiety in China had the lowest and highest incidence rates of 8.1 and 77.3,18,19 respectively. The reason for the different incidence rates was that different studies of depression and anxiety chose different scales, and the choice of research objects and cut-off points were also different. It could be seen that the mental health problems of medical staff couldnot be ignored.
How to prevent WPV was an important topic to improve mental health all over the world, so far, researchers in many countries had carried out a large number of topics, among which physical activity and sleep quality were crucial tools to measure mental health. WHO recommended regular physical activity for individuals of all age groups, because its positive impacts on several relevant health outcomes, including physical health and various dimensions of mental health and well-being.20 Individuals who were physically active in the past years were found to adapt adverse events quickly and improved their mental health.21 Poor sleep quality had a negative impact on psychological aspects of life.22 The benefits conferred by physical activity, quality sleep to youth physical well-being had been accepted.23 But whether physical activity and sleep quality help mitigate WPV´s effect on mental health had not been proven.
Sleep quality was a person´s assessment of his or her sleep-related characteristics, and whether these qualities were satisfactory or not.14 The relationship between WPV and sleep quality had been demonstrated in previous studies. Some researches demonstrated that WPV was negatively correlated with sleep quality, WPV and its influences led to negatively effect on sleep quality.14,24–26 A study conducted in Korean workforce found workers who experienced WPV were 3.32 times more likely to suffer sleep disturbance.27 A systematic review and meta-analysis found workers exposed to violence manifested problems related to sleep (difficulty in falling asleep, frequent interruption, early awakening, insomnia, nightmares).28 Some studies showed that sleep quality had a positive correlation with mental health. Poor sleep quality could negatively affected anxiety, depression and other mental symptoms.29–33 A meta-analysis of randomized controlled trials reported that improving sleep quality had a medium-sized effect on mental health, with clear evidence that improving sleep quality alleviated depression, stress and anxiety.34 Studies also demonstrated that sleep quality could be a mediating variable between family violence and mental health in Finnish health care professionals, unhealthy movements behaviors and mental health in Brazilian adults.35 Based on these researches, our study hypothesized WPV could influence mental health through people´s sleep quality.
Numerous researches had testified the association of physical activity between sleep quality and mental health. Physical activity could provide distraction through cognitive attention, it also provided people with pleasant experiences. People interacted with people during exercise, which promoted people´s mental health and sleep quality.21 Besides, other studies also demonstrated the modulating role of physical activity. Physical activity played a moderated role between sleep quality and health related quality of life among the elderly.36 In a study by Swedish municipal workers, physical activity was found to play a marginal moderating role in the relationship between work stress, self-rated health, and sleep quality.37 Among the officers who were insufficient active or inactive, sleep quality was associated with cortisol awakening response, but among officers who were active, sleep quality was not associated with cortisol awakening response, suggesting that physical activity could expose a potential protective effect.38 Frailty affected physical disability more strongly in rural older adults with low physical activity levels than in older adults with high levels of physical activity, suggesting that physical activity appeared to moderate the relationship between frailty and disability.39 As physical activity levels changed, so did this impact of social isolation and satisfaction on depression symptoms.40 However, so far there had no studies demonstrated the role of physical activity in regulating the relationship between WPV, sleep quality and mental health, and most studies had focused on older adults and general population, rarely focused on the specific group of healthcare workers.
Based on the above results, our study further verified the impact of WPV on mental health among healthcare workers, whether sleep quality could be used as a mediator between WPV and mental health, and whether physical activity could regulate the impact of WPV on sleep quality and mental health of healthcare workers. Therefore, through the research, the study established links between the four to deepen understanding of the mechanisms WPV on mental health. The study established model (Figure 1) that prompted us to understand the impact of physical activity, sleep quality on prevention of workplace violence and provide evidence for controlling the adverse effects of WPV.
 |
Figure 1 The conceptual framework of the moderated mediation model. Abbreviation: WPV, denotes workplace violence. |
Method
Participants and Survey Procedure
A cross-sectional survey was performed in Shandong Province, China. In the current study, 3426 valid questionnaires were successfully filled (a response rate of 98.22%, 3426/3488). Based on the level of gross domestic product per capita in 2017, a multiple stratified random cluster sampling method was conducted to select health technicians. First, 3 cities (Qingdao, Zaozhuang, Dezhou) were chosen in the current study. Second, the study random chosen three counties or districts in each city. Third, one city-level hospital was randomly selected in every city and three county-level hospitals were randomly selected in chosen county or district. Finally, 12 hospitals in three cities (3 city-level hospitals and 9 county-level hospitals) were chosen. Next, three inpatient areas from each department were randomly selected in city-level hospitals and two inpatient areas from each department was randomly selected in county-level hospitals. All the health technicians in the survey data were invested to participate our study. The questionnaires were sent to every chosen health technician and participants could fill out it in their free time anonymously. In order to make sure every question could be understood clearly, two postgraduates who were trained rigorously were stationed in every hospital to answer the question and collected the questionnaires after health technicians completed the survey.
Measures
Social-Demographic Variables
In this study, gender, age, marriage, religious belief, professional positions, administration, education, hospital level, physical disease, and year of service for the subjects were interviewed. Gender was measured by male and female. Married status was evaluated by single, married, divorced, widowed, and others. Since few subjects were single, divorced, widowed and others, so this study divided married status into married and others. Religious brief was encoded into “yes” or “no”. Professional positions were measured by senior, vice-senior, middle, primary, scholar level and no professional, the study subsequently encoded it into senior, intermediate, and primary title. Administrative positions in our study were divided into “director of the hospital”, “director of the center”, “vice president of the hospital”, “deputy director of the center”, “head of department”, “deputy director of the department”, “matron” and “had no administrative position”. The study encoded it to “had administrative positions” and “had not administrative positions”. Education was evaluated by the academic degree that participants had been awarded, the original classification included 7 schooling stages ranging from “junior high school and below” to “doctor”. To simplify, the study collapsed them into 3 categories: “master’s degree or above”, “undergraduate” and “college degree and below”. Hospital level was assessed by “the level of your hospital”, our study coded hospital level into 2 categories: “tertiary hospital” and “secondary hospital.” Physical disease was evaluated by asking a question whether the health technicians had been diagnosed with any physical disease (“cardiovascular and cerebrovascular diseases”, “metabolic diseases”, “mental abnormalities”, “hereditary disorders”, “chronic occupational diseases”, “chronic tracheitis and emphysema” and other diseases), if participants had one of these diseases, the study coded this participant had physical disease. If participant had none of this disease, the study coded the participant had not physical disease. Year of service was measured by the years the participants worked in this specialty.
Mental Health
The Kessler Psychological Distress Scale was used to assess mental health of health technicians in our study.41 It was a widely used, simple self-report measure of psychological distress. It was a 10-item scale, and answers used a five-point scale (which 5 = all the time, and 1 = none of the time). Participants should answer the question based the truths in the past four weeks. The total score range 10–50, which higher score meant poor mental health. The scale, compiled in 1994 by Kessler and Mroczek of Michigan University, had shown good reliability and validity in previous studies.42 The Chinese version was verified by Zhou scholars among college students to have good reliability and validity.43 The Cronbach’s alpha was 0.932 in this study.
Sleep Quality
The Pittsburgh Sleep Quality Index was used to assess sleep quality in the current study.44 It was a seven dimensions scale which contains the sleep quality, namely subjective sleep quality, sleep duration, sleep disturbances, sleep latency, habitual sleep efficiency, daytime disfunction, and use of sleep medication. Each dimension was scored 0–3 points, which generated a total score ranging from 0–21. Higher scores indicated poor sleep quality. The scale was rated based on how the respondents had felt over the past one month. PSQI was an extremely popular scale with good reliability and validity for evaluating sleep quality in Chinese populations.45–47
Workplace Violence
WPV was estimated by the question: “Have your patients or their family members behaved in the following ways for you?” and participants could choose answers from “verbal violence”, “physical violence”, “both” and “none”. Our study divided workplace violence into 2 categories: “yes” and “no”, which the former contained “verbal violence”, “physical violence” and “both”. This study evaluated WPV using a commonly used international item, it had been widely used in previous studies.48–50
Physical Activity
Physical activity was evaluated by the question: “How many times a week do you participate in physical activity on average?” and participants could choose answers from “Never exercise”, “Exercise not once”, “Exercise once or twice”, “Exercise three to five times”, “Exercise six times or more”. This question was widely used in previous studies.51,52
Statistical Analysis
IBM SPSS Statistics 21 was used for data analysis. The study calculated the mean and standard errors for continuous variables, frequencies and percentages for categorical variables. Independent t-test and one-way analysis of variance (ANOVA) were calculated for comparing the distribution of mental health. The correlations of study variables (WPV, physical activity, sleep quality, mental health) were analyzed by Pearson correlation analyses. Linear regression was conducted to verify if mediation and moderation were present in our study. The meditation and moderated mediation model were analyzed by the PROCESS macro for SPSS. The bias-corrected 95% confidence interval (CI) was calculated with 5000 bootstrapping re-samples. First, testing whether sleep quality played a moderated role between WPV and mental health in model 4 (Figure 1). Secondly, Model 59 was used to examine the moderated mediation effect, if physical activity moderated the direct effect of WPV on mental health and indirect effect of WPV on mental health including effect of WPV on sleep quality, and effect of sleep quality on mental health (Figure 2). If the 95% CI of the interaction did not contain 0, a significant moderated mediation effect could be established. Statistical significance was defined as a two-tailed p-value < 0.05. In addition, all models were controlled for covariates (gender, marriage, religious belief, professional positions, administration, education, hospital level, physical disease, and year of service) and the study variables were standardized.
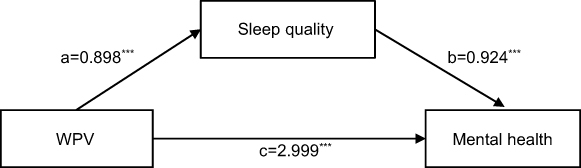 |
Figure 2 Output model of sleep quality mediation. Abbreviation: WPV, denotes workplace violence. Note: ***p<0.001. |
Results
Participants and Single Factor Analysis for the Samples
In this cross-sectional study, 3426 health technicians were successfully filled out the questioners. Table 1 describes the sample distribution regarding social-demographic and working characteristics. The average age was 35.14 (SD=8.42). Among these respondents, the majority of them were females (73.2%), married (81.8%), did not have religious belief (96.9%), in primary professional positions (53.8%), did not have administration (80.8%), undergraduate (69.1%), in third-class hospitals (56.7%), <1 time/week (32.6%), year of service less than 5 years (29.3%), experienced WPV (52.2%). The mean for Mental health and PSQI were 22.18 (SD=7.45) and 6.22 (SD=3.31), respectively.
 |
Table 1 Socio-Demographic Characteristics and the Distribution of Mental Health Among Health Technicians (n=3426) |
Table 1 also shows the result of differences in mental health among these social-demographic and working characteristics. Results show that marital status (t=2.58, p=0.010), professional positions (t=4.96, p=0.007), administration (t=−2.89, p=0.004), education (t=6.39, p=0.002), hospital level (t=4.69, p<0.001), physical activity (t=26.06, p<0.001), year of service (t=0.86, p<0.001), sleep quality (t=0.46, p<0.001) were positively associated with mental health, whereas religious belief (t=−2.22, p=0.030), physical disease (t=−10.18, p<0.001), WPV (t=−16.36, p<0.001) were negatively associated with mental health.
Bivariate Correlations Among WPV, Physical Activity, PSQI and Mental Health
Results of Pearson correlation among variables were displayed in Table 2. The results showed that WPV was positively related to PSQI and mental health (r=0.14, p<0.001; r=0.27, p<0.001). Physical activity was negatively associated with PSQI (r=−0.18, p<0.001). PSQI was positively correlated with mental health (r=0.46, p<0.001). Physical activity was negatively correlated with mental health (r=−0.17, p<0.001). In addition, WPV has a significantly negative relation to physical activity (r=−0.05, p=0.003).
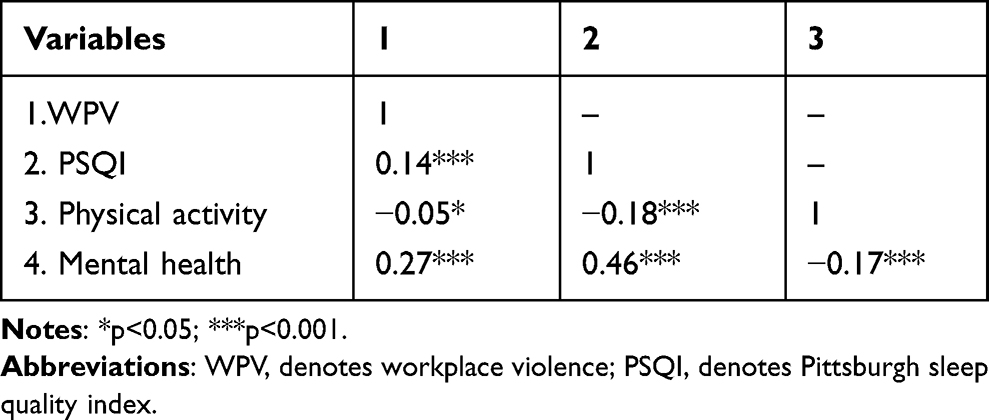 |
Table 2 Bivariate Correlation Among Workplace Violence, Sleeping Quality, Physical Activity, and Mental Health |
Regression Analysis of Sleep Quality Between WPV and Mental Health
Regression results are shown in Table 3. In the regression, firstly the study took WPV as the predictor variable and mental health as the dependent variable, the regression analysis was carried out, and the result showed that the regression effect was significant (β=3.83, p<0.001). Secondly, the study took WPV as the independent variable and sleep quality as the outcome variable, and conducted the regression analysis, the result presented the regression coefficient was statistically significant (β=0.90, p<0.001). Finally, taking WPV and sleep quality as independent variable and mental health as the dependent variable, a comprehensive regression of three variables was established, and the result indicated that the regression coefficient reached a significant level (β=0.92, p<0.001), indicating sleep quality played a mediating role. At the same time, after adding the mediating variable, WPV still had a significant effect on mental health (β=3.00, p<0.001), meaning that sleep quality played a partial mediating role between WPV and mental health.
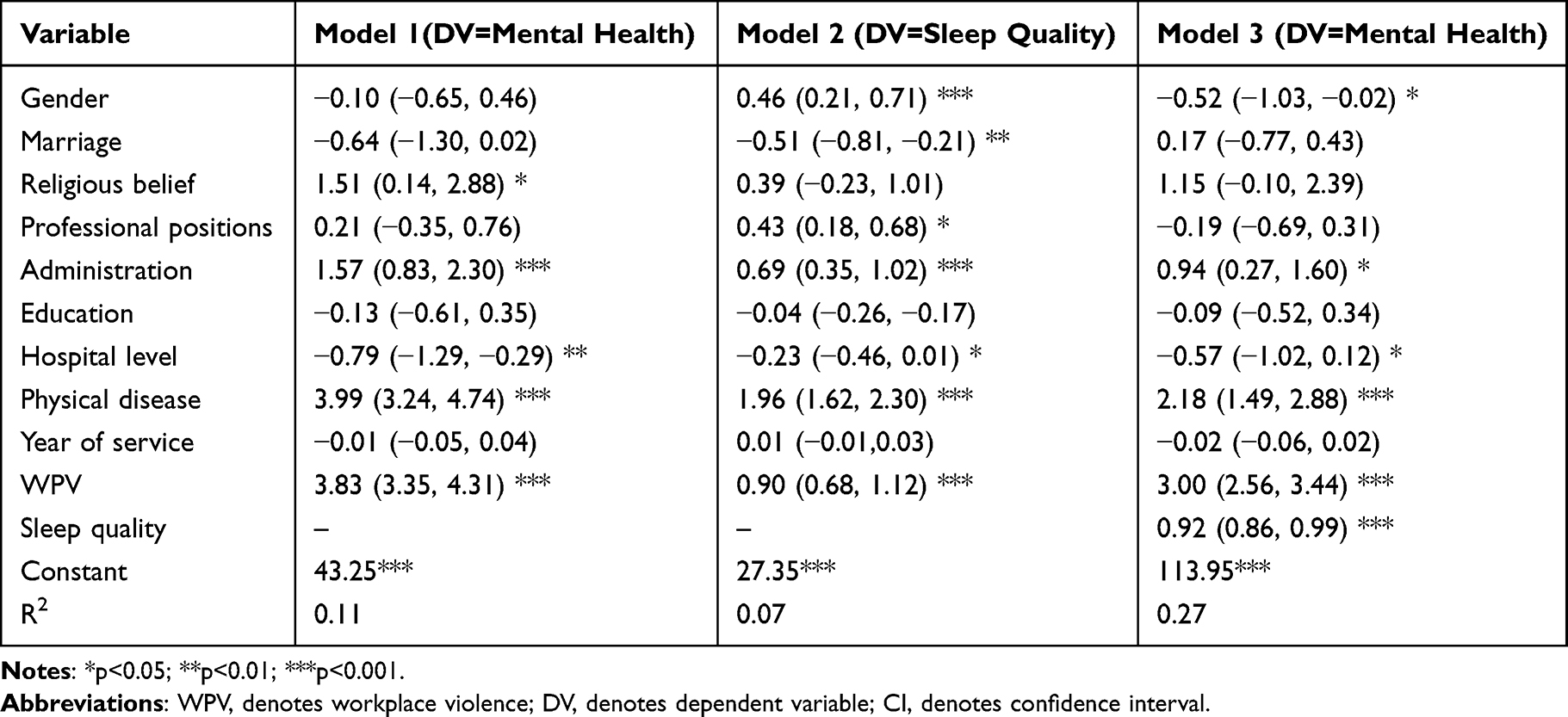 |
Table 3 Linear Regression Analysis for the Factors Associated with Sleep Quality and Mental Health [β (95% CI)] |
Mediation Analysis
As shown in Figure 2, the results of mediation analysis showed that the total effect (path c) of WPV on mental health was significant (β=3.828, p<0.001). The significant coefficient of path a (β=0.898, p<0.001) and path b (β=0.924, p<0.001) indicated the positive association of WPV on sleep quality, and sleep quality on mental health. Besides, the point estimates of indirect effect (path a*b) between WPV and mental health through sleep quality was 0.829 (SE=0.107), and the 95% bias-corrected bootstrap confidence interval was 0.621 to 1.026, which indicated that the indirect effect of WPV on mental health was statistically significantly. In addition, the direct effect of WPV on mental health (path c´=2.999, p<0.001) was also significant, indicating that sleep quality partially mediated the relationship between WPV and mental health.
Moderated Mediation Analyses
According to our hypothesis, physical activity might function as a moderator between WPV and mental health separately, or both in the direct (WPV-mental health) and indirect effect (path a: WPV-sleep quality and path b: sleep quality-mental health). However, physical activity did not play a moderating role in the direct effect (WPV-mental health) of the mediation model (WPV*physical activity: β=0.140, p=0.474, 95% CI: −0.239, 0.519). At the same, physical activity did not play a moderating role in the indirect effect (sleep quality-mental health) of the moderated model (sleep quality*physical activity: β=0.018, p=0.550, 95% CI: −0.038,0.074). The result showed that physical activity only moderated the effect of WPV on sleep quality (WPV*physical activity: β=0.235, p=0.013, 95% CI: 0.049, 0.422), signifying that the effect of WPV on sleep quality was moderated by physical activity among the health technicians. The final moderated mediation model was displayed in Figure 3.
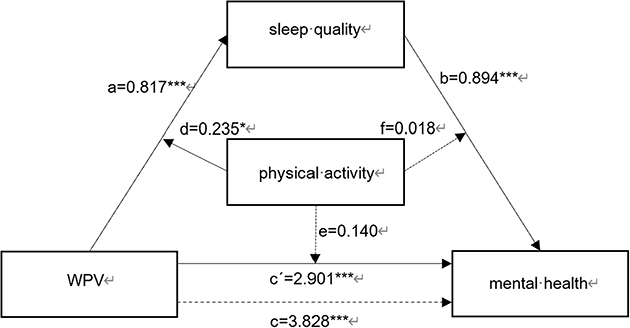 |
Figure 3 Mediation diagram with moderating effect. Abbreviation: WPV, denotes workplace violence. Notes: *p<0.05; ***p<0.001. |
Discussion
A cross-sectional study was conducted to reveal the situation of WPV experienced by technicians of hospitals in Shandong, China. To our knowledge, several studies explored the association between WPV, sleep quality, physical activity and mental health. In the present study, approximately, 52.2% participants had experienced WPV during the past year. This study not only confirmed negative impact of experience of WPV on participants´ sleep quality and mental health, but also used a moderated mediation analysis to elucidate the mediating role of sleep quality between WPV and mental health, and the moderating role of physical activity among them. This reminded us sleep quality and actively physical activity could mitigate the adverse effects of workplace violence and provide good support for improving the physical and mental health of health care workers.
This study was based on hospital physicians in Shandong, China. The results supported that the prevalence of WPV experienced by health technicians in the past year was 52.2%, which was lower than the result of a large cross-sectional study across 30 provinces in China among doctors (83.4%),26 it also lowered than the research which was based on a study by WeChat in Chinese mainland provinces, and the incidence of WPV was 56.4%.53 A study conducted in 4 provinces based on the geographical locations in the eastern, central and western regions of China, the rate of WPV during the past year was 66.19%,16 which included verbal violence, physical violence and sexual harassment. It was higher than ours. A meta-analysis concluded the overall prevalence of WPV from 44 studies in China with available data was 62.4%, that was higher than ours.1 Some studies that included Chinese nurses and psychiatric ward healthcare workers also had higher rates of WPV than our study,2,10,14,54 possibly because nurses had more contact with patients and their families than other health personnels, so they were more likely to experience violence, and unsupported work environment also made nurses experience higher rate of WPV.55 Mentally ill people had a poor mental state and more likely to commit violent acts against healthcare workers.55 However, compared with foreign studies, the experience of WPV in this study was lower than that of Syrian health care workers,56 Victorian health care workers,13 Brazilian health workers,25 but higher than that of Italian health professionals6 and higher than that of Korean nurses.6,12,13,25,56 The reason to suppose differences in the prevalence of WPV across the global and China, possibly due to the measurement construct of WPV and variation in normative behavior across culture and ethic contexts.57 Besides, the different geographical location might also explain the discrepancy between studies.56 Our results suggested WPV was less prevalent than previously estimated, though still at alarming level, in the future, governments and hospital officers should facilitate the design of prevention strategies.
In consistent with previous studies, the result revealed that the experience of WPV had a significantly negative effect on health technicians´ sleep quality and mental health.2,4,10,14,24 Health technicians who were experienced WPV were prone to suffer difficulty falling asleep, frequent disturbances, insomnia, nightmares, which affected the quality of their sleep. The feeling of vulnerability, emotional exhaustion and psychological discomfort resulted from the experience of WPV would reflect on sleep quality disorders.25 A possible explanation was that WPV, as a stress event, was associated with activation of the “sympathy-adreno-medullary”, which affected sleep quality.24 Previous studies revealed that WPV was a threat and violence to health workers, which in turn was a risk factor and a trigger for depression.49 As in most research, main consequences resulted from the experience of WPV, such as fear, anger, irritation, anxiety, depression, humiliation, guilt, fear of helplessness, and disappointment, all of these feelings could cause stress and burnout, eventually led to bad mental health.4,6 Therefore, health technicians needed some resources to cope with bad emotion. WPV was a pervasive phenomenon in the healthcare industry, in order to avoid WPV, health technicians tended to devote more resources, such as extra time and energy, to deal with negative emotions, but the consumption of resources was closely related to stress, burnout, depression, leading to poor health outcomes.26 WPV as a predictor of sleep quality and mental health, our study further validated that the experience of WPV of health care workers could impact sleep quality and mental health.
Moreover, mediation analysis of this study suggested that the relationship between WPV and mental health was mediated by sleep quality. This result supported the mediating effect of sleep quality among health technicians. More specifically, apart from the direct of WPV on mental health, the indirect effect from WPV should also be emphasized. As an internal component of health, sleep quality was an important psychological process with retrospective function, and poor sleep quality was considered as a secondary symptom of mental illness.45 WPV as a stressor, exposed to workplace violence could lead to heavy stress and burnout, mood swing that seriously affected their sleep quality. At the same time, short sleep at night, and poor sleep quality could lead to daytime fatigue, which increased bad mood.58 Moreover, poor sleep quality and lack of sleep amplified the negative effects of negative emotions and attenuated the beneficial effects of positive practices, which were not conductive to good mental health.34 Sleep disturbances led to a range of adverse outcomes, such as poor concentration, impaired glucose tolerance, sympathetic paranervous system activation, etc. They were strongly associated with adverse outcomes.24 Our study showed sleep quality played an important role between WPV and mental health, and WPV exacerbated psychological problems by reducing sleep quality, so suggesting that high quality of sleep could reduce the effect of WPV on mental health.
In the present study, the study also found that physical activity was not only associated with sleep quality and mental health, but also moderated the effect of WPV on sleep quality. Previous studies had reported the association between physical activity and sleep quality.38,59 In a survey of college students, increased physical activity was associated with a significant improvement of sleep quality.60 A study in young adults showed that moderated-intensity physical activity, higher sleep efficiency and poor-sleep wake rates were associated with fewer wake-ups, leading to better sleep quality.59 The underlying psychological mechanism might be that thermoregulation was the basis of sleep, physical activity had the effect of producing heat, raising body temperature, and then activating the hypothalamic controlled cooling process and sleep induction mechanism, energy consumption could also increase sleep.36,61 Health technicians who had experienced WPV can improve sleep efficacy and length of sleep, if they practiced physical activity regularly, which in turn improved sleep quality.
However, our study did not find physical activity could moderate the association between WPV and mental health or between sleep quality and mental health. Previous studies had not studied the relationship between WPV, physical activity, and mental health, but WPV as a negative life event could cause people´s stress response, tension, anxiety and other negative emotions, reduce mental health. People who regularly participated in physical activity adapt to adverse events more quickly and act as a buffer against adverse life events.21 Compared with other studies, our result found no association between physical activity in WPV and mental health might because participating in physical activity only helped improve less severe mental health measures, such as life satisfaction and subjective well-being.62 A study showed there was a curved relationship between physical activity and depression, and individuals with physical activity 2–3 times the recommended minimum amount of exercise were most strongly associated with a reduction in depression.63 Strenuous physical activity may also negatively affect the immune system, leading to depression through increasing oxidative stress and cortisol levels.63 As a special group, healthcare workers may face a variety of negative life events every day, and although studies had proven that physical activity helped improve depression, health technicians still faced stress, anxiety psychological confusion and other bad emotions, which had a negative influence on mental health. At the same time, although physical activity and sleep quality were significant factors influencing mental health, the result did not find the moderating role of sleep quality on mental health. Sleep disorders usually characterized by abnormal sleep duration and decreased sleep quality, resulting in fatigue, weakness. Sleep disturbances might reduce maximum oxygen consumption, increase the change of exercise-related injuries, and lead to daytime fatigue, which reduced the frequency and events of exercise, increased the chance of adverse health outcomes.36 And another explanation was that health technicians often on night shifts, it led to poor sleep quality, lacked of energy during the day, and difficulty in regular physical activity. Research proposed 45–60 minutes of moderate to vigorous exercise 3–5 days a week was good for adolescent physical and mental health.23 Health technicians may not be physically active at sufficient intensity to regulate the relationship between sleep quality and mental health.
Strategies are needed to reduce and prevent the incidence of WPV, hospitals must provide a safety system, sound policies, and preventive procedures. The incidence of WPV among health technicians in China still at an alarming level, due to the tremendous negative impact of WPV, we further advice hospitals to strength the management and training of physicians to reduce the harm of WPV. The effects of WPV on workers’ sleep quality and mental health must be emphasized. For victims of WPV, hospital management should intervene in a timely manner and provide assistance and supported environment, while encourage all health technicians to take physical activity actively, and ensure sleep quality in order to maintain good mental health.
The current study had some limitations. Firstly, a cross-sectional study was not helpful in establishing a causal relationship between WPV, sleep quality, physical activity and mental health. In the future, longitudinal studies were needed to explore the causal relations. Secondly, the data study collected were self-reported by the health technicians, might have resulted in a response bias, and to some extent, overestimated or underestimated the association between study variables. Third, the influencing factors of sleep quality, mental health were complex, our study only focus on sociodemographic factors, working characteristics, psychological condition, and not pay attention to all factors.
Conclusion
Our study showed that WPV was related to health technicians´ mental health, and sleep quality appeared to partially mediated the relationship between WPV and mental health. Additionally, physical activity appeared to moderate the association of WPV on sleep quality. WPV was an adverse life event that negatively affected the mental health of healthcare workers, and sleep quality and physical activity could weaken, alleviate the negative effects of WPV. This provided support for elucidate the underlying mechanism of the relationship between WPV and mental health and formed an effective way to improve the mental health of health technicians in China. It could provide relevant government departments with interventions to improve the health of health technicians.
Abbreviations
WPV, Workplace Violence; PSQI, The Pittsburgh Sleep Quality Index; ANOVA, Analysis of Variance; CI, Confidence Interval; SD, Standard Deviation.
Data Sharing Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Approval and Consent to Participate
The studies involving human participants were reviewed and approved by the Ethics Committee of School of Public Health, Shandong University (ref: 20181219), it had been approved in 2018. The participants provided their written informed consent to participate in this study. The principles set forth in the Helsinki Declaration were also observed.
Acknowledgments
We expressed gratitude to the subjects for their participation and cooperation. Furthermore, our study also thanked all interviewers for their efforts and help in this investigation. We were also grateful to the many contributors who had supported the development of this research.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The research was supported by the National Natural Science Foundation of China (71974114), and Humanities and Social Science in Shandong Province (2022-YYGL-51).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Lu L, Dong M, Wang SB, et al. Prevalence of Workplace Violence Against Health-Care Professionals in China: a Comprehensive Meta-Analysis of Observational Surveys. Trauma Violence Abuse. 2020;21(3):498–509. doi:10.1177/1524838018774429
2. Lu L, Lok KI, Zhang L, et al. Prevalence of verbal and physical workplace violence against nurses in psychiatric hospitals in China. Arch Psychiatr Nurs. 2019;33(5):68–72. doi:10.1016/j.apnu.2019.07.002
3. Magnavita N. Workplace violence and occupational stress in healthcare workers: a chicken-and-egg situation-results of a 6-year follow-up study. J Nurs Scholarsh. 2014;46(5):366–376. doi:10.1111/jnu.12088
4. Li X, Wu H. Does psychological capital mediate between workplace violence and depressive symptoms among doctors and nurses in Chinese general hospitals? Psychol Res Behav Manag. 2021;14:199–206. doi:10.2147/PRBM.S293843
5. Tong C, Cui C, Li Y, Wang L. The effect of workplace violence on depressive symptoms and the mediating role of psychological capital in Chinese township general practitioners and nurses: a cross-sectional study. Psychiatry Investig. 2019;16(12):896–903. doi:10.30773/pi.2019.0095
6. Ferri P, Silvestri M, Artoni C, Di Lorenzo R. Workplace violence in different settings and among various health professionals in an Italian general hospital: a cross-sectional study. Psychol Res Behav Manag. 2016;9:263–275. doi:10.2147/PRBM.S114870
7. Wang H, Zhang Y, Sun L. The effect of workplace violence on depression among medical staff in China: the mediating role of interpersonal distrust. Int Arch Occup Environ Health. 2021;94(3):557–564. doi:10.1007/s00420-020-01607-5
8. Caruso R, Toffanin T, Folesani F, et al. Violence against physicians in the workplace: trends, causes, consequences, and strategies for intervention. Curr Psychiatry Rep. 2022;24(12):911–924. doi:10.1007/s11920-022-01398-1
9. Kafle S, Paudel S, Thapaliya A, Acharya R. Workplace violence against nurses: a narrative review. J Clin Transl Res. 2022;8(5):421–424.
10. Zhao S, Xie F, Wang J, et al. Prevalence of workplace violence against Chinese nurses and its association with mental health: a cross-sectional survey. Arch Psychiatr Nurs. 2018;32(2):242–247. doi:10.1016/j.apnu.2017.11.009
11. Havaei F. Does the type of exposure to workplace violence matter to nurses’ mental health? Healthcare. 2021;9(1):564.
12. Lee J, Lee B. Psychological Workplace Violence and Health Outcomes in South Korean Nurses. Workplace Health Saf. 2022;70(5):228–234. doi:10.1177/21650799211025997
13. Tonso MA, Prematunga RK, Norris SJ, Williams L, Sands N, Elsom SJ. Workplace Violence in Mental Health: a Victorian Mental Health Workforce Survey. Int J Ment Health Nurs. 2016;25(5):444–451. doi:10.1111/inm.12232
14. Zhang SE, Liu W, Wang J, et al. Impact of workplace violence and compassionate behaviour in hospitals on stress, sleep quality and subjective health status among Chinese nurses: a cross-sectional survey. BMJ Open. 2018;8(10):e019373. doi:10.1136/bmjopen-2017-019373
15. Renwick L, Lavelle M, James K, Stewart D, Richardson M, Bowers L. The physical and mental health of acute psychiatric ward staff, and its relationship to experience of physical violence. Int J Ment Health Nurs. 2019;28(1):268–277. doi:10.1111/inm.12530
16. Duan X, Ni X, Shi L, et al. The impact of workplace violence on job satisfaction, job burnout, and turnover intention: the mediating role of social support. Health Qual Life Outcomes. 2019;17(1):93. doi:10.1186/s12955-019-1164-3
17. Saragih ID, Tonapa SI, Saragih IS, et al. Global prevalence of mental health problems among healthcare workers during the Covid-19 pandemic: a systematic review and meta-analysis. Int J Nurs Stud. 2021;121:104002. doi:10.1016/j.ijnurstu.2021.104002
18. Hong S, Ai M, Xu X, et al. Immediate psychological impact on nurses working at 42 government-designated hospitals during COVID-19 outbreak in China: a cross-sectional study. Nurs Outlook. 2021;69(1):6–12. doi:10.1016/j.outlook.2020.07.007
19. Marvaldi M, Mallet J, Dubertret C, Moro MR, Guessoum SB. Anxiety, depression, trauma-related, and sleep disorders among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2021;126:252–264. doi:10.1016/j.neubiorev.2021.03.024
20. WHO Guidelines Approved by the Guidelines Review Committee. Global Recommendations on Physical Activity for Health. World Health Organization; 2010.
21. Wicker P, Orlowski J. Coping with adversity: physical activity as a moderator in adaption to bereavement. J Public Health. 2021;43(2):e196–e203. doi:10.1093/pubmed/fdaa059
22. Yuan Y, Li J, Jing Z, et al. The role of mental health and physical activity in the association between sleep quality and quality of life among rural elderly in China: a moderated mediation model. J Affect Disord. 2020;273:462–467. doi:10.1016/j.jad.2020.05.093
23. Hosker DK, Elkins RM, Potter MP. Promoting Mental Health and Wellness in Youth Through Physical Activity, Nutrition, and Sleep. Child Adolesc Psychiatr Clin N Am. 2019;28(2):171–193. doi:10.1016/j.chc.2018.11.010
24. El-Zoghby SM, Ibrahim ME, Zaghloul NM, Shehata SA, Farghaly RM. Impact of workplace violence on anxiety and sleep disturbances among Egyptian medical residents: a cross-sectional study. Hum Resour Health. 2022;20(1):84. doi:10.1186/s12960-022-00786-1
25. Silveira F, Lira Neto JCG, Weiss C, Araújo MFM. Association between community-based and workplace violence and the sleep quality of health professionals: a cross-sectional study. Cien Saude Colet. 2021;26(5):1647–1656. doi:10.1590/1413-81232021265.04522021
26. Sun T, Gao L, Li F, et al. Workplace violence, psychological stress, sleep quality and subjective health in Chinese doctors: a large cross-sectional study. BMJ Open. 2017;7(12):e017182. doi:10.1136/bmjopen-2017-017182
27. Hwang WJ, Yang HK, Kim JH. What Are the Experiences of Emotional Labor and Workplace Violence that Are More Harmful to Health in Korean Workforce? Int J Environ Res Public Health. 2020;17(21). doi:10.3390/ijerph17218019
28. Magnavita N, Di Stasio E, Capitanelli I, Lops EA, Chirico F, Garbarino S. Sleep problems and workplace violence: a systematic review and meta-analysis. Front Neurosci. 2019;13:997. doi:10.3389/fnins.2019.00997
29. Aschbrenner KA, Naslund JA, Salwen-Deremer JK, et al. Sleep quality and its relationship to mental health, physical health and health behaviours among young adults with serious mental illness enrolled in a lifestyle intervention trial. Early Interv Psychiatry. 2022;16(1):106–110. doi:10.1111/eip.13129
30. Ghrouz AK, Noohu MM, Dilshad Manzar M, Warren Spence D, BaHammam AS, Pandi-Perumal SR. Physical activity and sleep quality in relation to mental health among college students. Sleep Breath. 2019;23(2):627–634. doi:10.1007/s11325-019-01780-z
31. Murray K, Godbole S, Natarajan L, et al. The relations between sleep, time of physical activity, and time outdoors among adult women. PLoS One. 2017;12(9):e0182013. doi:10.1371/journal.pone.0182013
32. Vaingankar JA, Muller-Riemenschneider F, Chu AHY, et al. Sleep duration, sleep quality and physical activity, but not sedentary behaviour, are associated with positive mental health in a multi-ethnic asian population: a cross-sectional evaluation. Int J Environ Res Public Health. 2020;17(22). doi:10.3390/ijerph17228489
33. Zhao Y, Song J, Brytek-Matera A, Zhang H, He J. The Relationships between Sleep and Mental and Physical Health of Chinese Elderly: exploring the Mediating Roles of Diet and Physical Activity. Nutrients. 2021;13(4). doi:10.3390/nu13041316
34. Scott AJ, Webb TL, Martyn-St James M, Rowse G, Weich S. Improving sleep quality leads to better mental health: a meta-analysis of randomised controlled trials. Sleep Med Rev. 2021;60:101556. doi:10.1016/j.smrv.2021.101556
35. Siltala HP, Holma JM, Hallman M. Family violence and mental health in a sample of Finnish health care professionals: the mediating role of perceived sleep quality. Scand J Caring Sci. 2019;33(1):231–243. doi:10.1111/scs.12629
36. Hu W, Chu J, Chen X, et al. The role of depression and physical activity in the association of between sleep quality, and duration with and health-related quality of life among the elderly: a UK Biobank cross-sectional study. BMC Geriatr. 2022;22(1):338. doi:10.1186/s12877-022-03047-x
37. Leitaru N, Kremers S, Hagberg J, Bjorklund C. Associations between job-strain, physical activity, health status, and sleep quality among Swedish municipality workers. J Occup Environ Med. 2019;61(2):e56–e60. doi:10.1097/JOM.0000000000001516
38. Fekedulegn D, Innes K, Andrew ME, et al. Sleep quality and the cortisol awakening response (CAR) among law enforcement officers: the moderating role of leisure time physical activity. Psychoneuroendocrinology. 2018;95:158–169. doi:10.1016/j.psyneuen.2018.05.034
39. Hao W, Li J, Fu P, et al. Physical frailty and health-related quality of life among Chinese rural older adults: a moderated mediation analysis of physical disability and physical activity. BMJ Open. 2021;11(1):e042496. doi:10.1136/bmjopen-2020-042496
40. Vargas I, Howie EK, Muench A, Perlis ML. Measuring the Effects of Social Isolation and Dissatisfaction on Depressive Symptoms during the COVID-19 Pandemic: the Moderating Role of Sleep and Physical Activity. Brain Sci. 2021;11(11). doi:10.3390/brainsci11111449
41. Kessler R, Mroczek D. Final Versions of our Non-Specific Psychological Distress Scale. University of Michigan; 1994.
42. Kessler RC, Andrews G, Colpe LJ, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002;32(6):959–976. doi:10.1017/s0033291702006074
43. Cheng-chao Z, Jie C, Ting W. Reliability and Validity of 10-item Kessler Scale (K10) Chinese Version in Evaluation of Mental Health Status of Chinese Population. Chine J Clin Psychol. 2008;16(06):627–629.
44. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
45. Wang Q, Zhang J, Wang R, et al. Sleep quality as a mediator of the association between coping styles and mental health: a population-based ten-year comparative study in a Chinese population. J Affect Disord. 2021;283:147–155. doi:10.1016/j.jad.2021.01.045
46. Zhai X, Wu N, Koriyama S, et al. Mediating effect of perceived stress on the association between physical activity and sleep quality among Chinese college students. Int J Environ Res Public Health. 2021;18(1):54.
47. Xianchen L, Maoqin T, Lei H. Reliability and validity of the Pittsburgh Sleep Quality Index. Chin J Psychiatry. 1996;2:103–107.
48. Arnetz JE, Hamblin L, Ager J, et al. Underreporting of Workplace Violence: comparison of Self-Report and Actual Documentation of Hospital Incidents. Workplace Health Saf. 2015;63(5):200–210. doi:10.1177/2165079915574684
49. Sun L, Zhang W, Qi F, Wang Y. Gender Differences for the Prevalence and Risk Factors of Workplace Violence Among Healthcare Professionals in Shandong, China. Front Public Health. 2022;10:873936. doi:10.3389/fpubh.2022.873936
50. Torok E, Rod NH, Ersboll AK, Jensen JH, Rugulies R, Clark AJ. Can work-unit social capital buffer the association between workplace violence and long-term sickness absence? A prospective cohort study of healthcare employees. Int Arch Occup Environ Health. 2020;93(3):355–364. doi:10.1007/s00420-019-01484-7
51. Chen X, Ms H, Yamagami T, Kagamimori S. Associations of lifestyle factors with quality of life (QOL) in Japanese children: a 3-year follow-up of the Toyama Birth Cohort Study. Original Article. 2016.
52. Finne E, Bucksch J, Lampert T, Kolip P. Physical activity and screen-based media use: cross-sectional associations with health-related quality of life and the role of body satisfaction in a representative sample of German adolescents. Health Psychol Behav Med. 2013;1(1):15–30. doi:10.1080/21642850.2013.809313
53. Tian Y, Yue Y, Wang J, Luo T, Li Y, Zhou J. Workplace violence against hospital healthcare workers in China: a national WeChat-based survey. BMC Public Health. 2020;20(1):582. doi:10.1186/s12889-020-08708-3
54. Chen Y, Wang P, Zhao L, et al. Workplace Violence and Turnover Intention Among Psychiatrists in a National Sample in China: the Mediating Effects of Mental Health. Front Psychiatry. 2022;13:855584. doi:10.3389/fpsyt.2022.855584
55. Yang BX, Stone TE, Petrini MA, Morris DL. Incidence, Type, Related Factors, and Effect of Workplace Violence on Mental Health Nurses: a Cross-sectional Survey. Arch Psychiatr Nurs. 2018;32(1):31–38. doi:10.1016/j.apnu.2017.09.013
56. Mohamad O, AlKhoury N, Abdul-Baki MN, Alsalkini M, Shaaban R. Workplace violence toward resident doctors in public hospitals of Syria: prevalence, psychological impact, and prevention strategies: a cross-sectional study. Hum Resour Health. 2021;19(1):8. doi:10.1186/s12960-020-00548-x
57. Cheung T, Lee PH, Yip PSF. Workplace Violence toward Physicians and Nurses: prevalence and Correlates in Macau. Int J Environ Res Public Health. 2017;14(8):554.
58. Banerjee S, Boro B. Analysing the role of sleep quality, functional limitation and depressive symptoms in determining life satisfaction among the older Population in India: a moderated mediation approach. BMC Public Health. 2022;22(1):1933. doi:10.1186/s12889-022-14329-9
59. Carneiro-Barrera A, Amaro-Gahete FJ, Acosta FM, Ruiz JR. Body Composition Impact on Sleep in Young Adults: the Mediating Role of Sedentariness, Physical Activity, and Diet. J Clin Med. 2020;9(5):76.
60. Wu X, Tao S, Zhang Y, Zhang S, Tao F. Low physical activity and high screen time can increase the risks of mental health problems and poor sleep quality among Chinese college students. PLoS One. 2015;10(3):e0119607. doi:10.1371/journal.pone.0119607
61. Su Y, Wang SB, Zheng H, et al. The role of anxiety and depression in the relationship between physical activity and sleep quality: a serial multiple mediation model. J Affect Disord. 2021;290:219–226. doi:10.1016/j.jad.2021.04.047
62. Cunningham GB, Wicker P. Pollution, health, and the moderating role of physical activity opportunities. Int J Environ Res Public Health. 2020;17(17). doi:10.3390/ijerph17176272
63. Kim SY, Jeon SW, Shin DW, Oh KS, Shin YC, Lim SW. Association between physical activity and depressive symptoms in general adult populations: an analysis of the dose-response relationship. Psychiatry Res. 2018;269:258–263. doi:10.1016/j.psychres.2018.08.076
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Emotional Eating, Sociodemographic Characteristics, Physical Activity, Sleep Duration, and Mental and Physical Health in Young Adults
Calderón-Asenjo RE, Jalk-Muñoz MC, Calizaya-Milla YE, Calizaya-Milla SE, Ramos-Vera C, Saintila J
Journal of Multidisciplinary Healthcare 2022, 15:2845-2859
Published Date: 13 December 2022
Characteristics and Influencing Factors of Post-Traumatic Growth: A Cross-Sectional Study of Psychiatric Nurses Suffering from Workplace Violence in Guangdong China

Wang W, Ye J, Wei Y, Yuan L, Wu J, Xia Z, Huang J, Wang H, Li Z, Guo J, Xiao A
Journal of Multidisciplinary Healthcare 2024, 17:1291-1302
Published Date: 20 March 2024
Acupressure for Sleep, Mental Health, and Quality of Life in Hemodialysis Patients: A Systematic Review and Meta-Analysis
Wang Y, Zhang X, Lan L, Qu Y, Wang Y, Chen J, Chou LW, Zeng F
Nature and Science of Sleep 2026, 18:566303
Published Date: 8 January 2026
Mental Health, Sleep, and Physical Activity Among Young Saudi Women During Ramadan: A Comparative Cohort Study
Balasubramanian K, Sanjeevi RR, Alshehri MM, Alothman SA
Nature and Science of Sleep 2026, 18:583610
Published Date: 11 June 2026