Back to Journals » Infection and Drug Resistance » Volume 19
Associations Between Systemic Immunity Inflammation Index, Aggregate Index of Systemic Inflammation, and Hospital Acquired Otitis Media in Children Aged ≤12 years with Bacterial Pneumonia
Authors Han L ![]() , Li Y, Gao C, Liu J, Wu J
, Li Y, Gao C, Liu J, Wu J ![]()
Received 20 November 2025
Accepted for publication 4 March 2026
Published 13 March 2026 Volume 2026:19 582992
DOI https://doi.org/10.2147/IDR.S582992
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chi H. Lee
Liyuan Han,1,2 Yanhua Li,1,2 Chunyan Gao,1,2 Jie Liu,3 Jinghua Wu1,2
1Clinical Laboratory, Tangshan Maternal and Child Health Care Hospital, Tangshan, Hebei, People’s Republic of China; 2Key Laboratory of Molecular Medicine for Abnormal Development and Related Diseases, Tangshan Maternal and Child Health Care Hospital, Tangshan, Hebei, People’s Republic of China; 3Otorhinolaryngology Head and Neck Surgery, Tangshan Maternal and Child Health Care Hospital, Tangshan, Hebei, People’s Republic of China
Correspondence: Jinghua Wu, Clinical Laboratory, Tangshan Maternal and Child Health Care Hospital, Tangshan, Hebei, People’s Republic of China, Email [email protected]
Purpose: Hospital-acquired otitis media (OM) is a common complication in children with bacterial pneumonia, associated with prolonged morbidity. Systemic inflammation indices (SII and AISI) may serve as biomarkers for OM risk. This study aimed to evaluate the association of SII and AISI with hospital-acquired OM risk in children (≤ 12 years) with bacterial pneumonia.
Patients and Methods: A total of 388 children (aged ≤ 12 years) diagnosed with bacterial pneumonia were enrolled in this study from January 2024 to June 2025.. Data included demographic characteristics, birth history, feeding history, and laboratory tests. Logistic regression analysis was used to analyze the relationship between SII, AISI, and the risk of OM. This study constructed a nomogram prediction model, and the performance of the model was assessed by the area under the receiver operating characteristic curve (AUC), calibration curves, and decision curve analysis (DCA).
Results: The majority of patients were male (54.90%) and aged ≤ 3 years (55.93%). Based on OM status, children were divided into No-OM group (n = 289) and OM group (n = 99). The OM group showed significantly elevated levels of inflammatory markers (WBC, NEU, MON, PLT, CRP, SII and AISI), alongside lower levels of RBC, HGB, and TP, compared to the No-OM group (all p< 0.05). Multivariate analysis found log2-SII (OR = 1.38, 95% CI: 1.05– 1.82, p = 0.021) and log2-AISI (OR = 1.37, 95% CI: 1.07– 1.78, p < 0.001) were risk factors of hospital acquired OM. Compared to log2-SII model (0.827, 95% CI: 0.780– 0.875), log2-AISI model (0.834, 95% CI: 0.788– 0.881) demonstrated superior discriminatory ability. Both models exhibited a favorable clinical benefit rate. Additionally, restricted cubic spline (RCS) analysis showed a significant linear relationship between log2-SII, log2-AISI and OM risk (all P for nonlinear > 0.05), with inflection points at 9.71 (log2-SII) and 8.16 (log2-AISI).
Conclusion: This study established the predictive value of SII and AISI for hospital acquired OM in children aged ≤ 12 years with bacterial pneumonia. Integrating them into clinical practice can guide targeted prevention and thereby improve prognosis.
Keywords: systemic immunity inflammation index, aggregate index of systemic inflammation, bacterial pneumonia, otitis media, inflammation
Introduction
Pneumonia is a pulmonary disease caused by pathogens, such as bacteria, mycoplasma and viruses.1–3 The global annual number of deaths from pneumonia was about 2.5 million between 1990 and 2019.4 Bacterial pneumonia, as an acute inflammation of the lung parenchyma (including alveoli, terminal airways, and pulmonary interstitium) is caused by bacterial infection, and it is one of the most common types of pneumonia clinically. Streptococcus pneumoniae and Haemophilus influenzae are the most common bacterial pathogen.5,6 Studies had shown that Streptococcus pneumoniae alone causes over 1 million deaths annually in susceptible populations (children and the elderly.5 Hospitalization for bacterial pneumonia in children can lead to many complications, such as pleural effusion, empyema, respiratory failure, sepsis, and otitis media (OM).7–11 Among these, OM is the most common,12 which can affect children’s hearing, language and quality of life.13
The pathogenesis of OM secondary to bacterial pneumonia is closely linked to the anatomical connectivity and inflammatory spillover between the upper and lower respiratory tracts. The pediatric Eustachian tube is shorter, more horizontal, and functionally immature compared to adults, facilitating the reflux or aspiration of nasopharyngeal secretions containing pathogens into the middle ear.14,15 Furthermore, the systemic inflammatory response triggered by bacterial pneumonia can lead to mucosal swelling and dysfunction of the Eustachian tube, disrupting middle ear ventilation and clearance.16 This creates a conducive environment for secondary bacterial infection and effusion, characterizing the course of hospital-acquired OM.17 In additional, studies had indicated that factors influencing the OM during hospitalization in children with bacterial pneumonia include non-exclusive breastfeeding, inflammation, and decreased serum vitamin D levels.18–20 Among these, inflammation is of significant importance, as it can influence the occurrence of otitis media.
Systemic immunity inflammation index (SII) and the aggregate index of systemic inflammation (AISI) are novel inflammatory markers, which are calculated by neutrophils, monocytes and lymphocytes. These values can be easily obtained through routine complete blood cell count test, it is an economical, rapid and widely used clinical test. Previous research had found associations between these indices and various diseases, such as breast cancer, esophageal cancer, cardiovascular diseases, and diabetes.21–24 However, the relationship between SII, AISI and the hospital acquired OM in bacterial pneumonia children remains unclear. Therefore, we planned to explore the relationship between SII, AISI and OM risk during hospitalization in pediatric patients with bacterial pneumonia.
Materials and Methods
Data Sources and Population Selection
This study retrospectively collected 388 children with bacterial pneumonia who were admitted to Tangshan Maternal and Child Health Care Hospital between January 2024 and June 2025. Based on the occurrence of OM after admission, the children were divided into bacterial pneumonia with OM group (OM group) and bacterial pneumonia without OM group (No-OM group). Inclusion criteria were as follows: (1) Children ≤12 years old; (2) Complete demographic information, clinical records, and laboratory test results; (3) Pathogenic bacteria confirmed as positive through sputum culture or bronchoalveolar lavage fluid bacterial culture; (4) Absence of clinical manifestations related to otitis media upon admission. Exclusion criteria: (1) Presence of hepatic or renal dysfunction, or cardiac impairment; (2) Presence of chronic underlying diseases such as connective tissue diseases, neurological disorders, endocrine system diseases, or developmental delays; (3) Diagnosis of malignancy. All finally included cases strictly met the above criteria. To ensure the reliability of the results, this study adopted rigorous methods, excluded hepatic dysfunction (26), renal dysfunction (32), cardiac impairment (21); presence of chronic underlying diseases such as connective tissuediseases (15), neurologicaldisorders (4), endocrine systemdiseases (6), or developmental delays (2); diagnosis of malignancy (3). This retrospective study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved by the Tangshan Maternal and Child Health Care Hospital Ethics Review Committee (Approval No.: 2023–080-01). All data were anonymized and handled exclusively by the research team in a secure environment, used solely for this study without disclosure for any other purpose. The flowchart was shown in Figure 1.
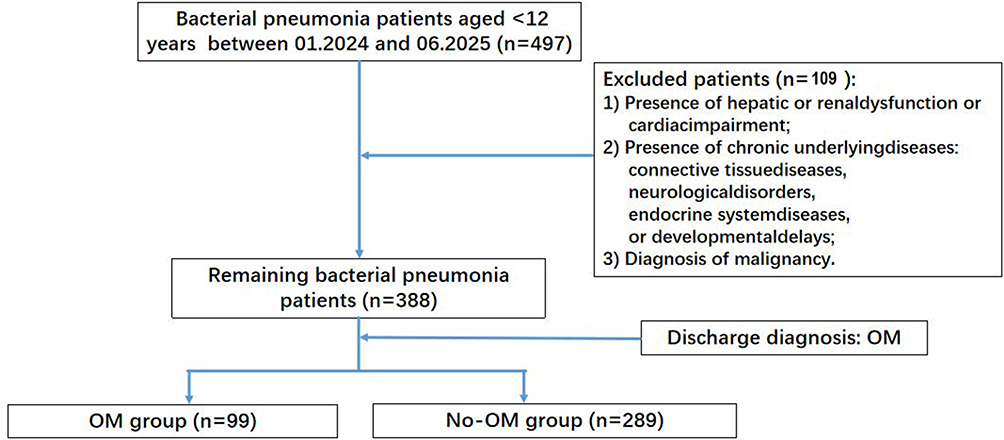 |
Figure 1 Patient Selection Flowchart. |
Data Collection
All data for this study were collected from the electronic medical record system of Tangshan Maternal and Child Health Care Hospital. We collected data on the following: demographic characteristics (sex, age); birth history (delivery mode, maternal gravidity, preterm birth); feeding practices (breastfeeding, formula, or mixed); clinical manifestations; and laboratory parameters (hematological, biochemical, and pathogen detection results).
The peripheral blood indices included WBC, NEU, MON, LYM, PLT, RBC, and HGB; the biochemical parameters included CRP, ALT, AST, TP, CK, and LDH. A 3mL fasting venous blood sample was collected from children aged ≤ 12 years with bacterial pneumonia on admission day. The complete blood count was analyzed using an automated hematology analyzer (Mindray BC-6800). Blood samples were centrifuged by centrifugal force (3000 r/min, 15 minutes). Biochemical indices were measured using a Beckman biochemical analyzer.
In bacteriological analysis, we focused on the four most frequently detected pathogens in sputum culture or bronchoalveolar lavage fluid culture: Haemophilus influenzae (HI), Streptococcus pneumoniae (SP), Staphylococcus aureus (SA), and Moraxella catarrhalis (MC).
All laboratory tests were performed in strict accordance with standardized operating procedures.
Definition of Dependent Variables: Hospital Acquired OM with Bacterial Pneumonia
Bacterial pneumonia refers to parenchymal inflammation of the lungs caused by bacterial pathogens, primarily involving the alveoli and pulmonary interstitium.25
OM was defined by moderate to severe tympanic membrane bulging, new otorrhea (excluding external otitis) or mild bulging with ear pain or erythema.26 In this study, bacterial pneumonia complicated by OM in hospitalized children refers to cases where children were admitted for bacterial pneumonia without symptoms of OM at the time of admission but developed OM during their hospital stay.
Definition of Independent Variables: SII and AISI
SII and AISI are composite biomarkers based on counts of inflammatory cells in peripheral blood. Fasting venous blood (3 mL) was collected from patients on the day of hospitalization. Monocytes, lymphocytes, neutrophils, and PLT counts were measured using an automated hematology analyzer (Mindray BC-6800). The formula for SII is platelet count × neutrophil count / lymphocyte count, while the formula for AISI is monocyte count × platelet count × neutrophil count / lymphocyte count.27 Since the SII and AISI values in this study exhibited a skewed distribution, SII and AISI were log2-transformed before data analysis.
Definition of Other Variables
Preterm infants were defined as a gestational age of less than 37 weeks with a birth weight of less than 2500 grams.28 Gravidity is defined as the total number of pregnancies a woman has experienced, including all singleton and multiple gestations (eg, twins count as one pregnancy), ectopic pregnancies, miscarriages (both spontaneous and induced abortions), and live births from normal deliveries. Any confirmed pregnancy is counted as one gravidity event.
Antibiotic use was defined as the administration of β-lactam or macrolide antibiotics before admission.
Statistical Analysis
Data management was performed using Excel 2020, and statistical analyses were conducted in R 4.4.3. Continuous variables were presented as mean ± standard deviation or median with interquartile range, as appropriate based on their distribution. Categorical variables were expressed as frequencies and percentages. To compare baseline characteristics, continuous variables were analyzed using independent t-tests (for normally distributed data) or Mann–Whitney U-tests (for non-normally distributed data). Categorical variables were compared using χ2-tests. To identify independent risk factors for hospital-acquired OM, a multivariable logistic regression model was developed. Variables with P-values < 0.05 in univariate analyses were included in a backward stepwise selection process. For the purpose of providing a visual and practical tool for individualized risk prediction, a nomogram was constructed based on the final regression model. To comprehensively evaluate the predictive performance of the nomogram, we assessed its discrimination using the area under the receiver operating characteristic curve (AUC), its calibration using calibration curves with 1000 bootstrap resamples, and its clinical utility using decision curve analysis (DCA). Results were reported as odds ratios (OR) with their 95% confidence intervals (CI). Statistical significance for all tests was defined as a two-sided P-value < 0.05.
Results
Baseline Characteristics
388 bacterial pneumonia children were included in this study, 213 (54.90%) was male, 175 (45.10%) was female. Among these patients, most were aged ≤ 3 years (55.93%), born at term (94.85%) and via Caesarean section (57.47%). Concerning bacterial infections, SP was detected in 31.70%, SA was 14.95% and MC was 18.04%. HI was found in 30.41% of the patients. The majority of children (75.26%) had taken antibiotics before being hospitalized.
The children were divided into two groups: non-OM group (n=289) and OM group (n=99). Compared to the non-OM group, the OM group had a significantly higher proportion aged ≤3 years and a higher rate of HI infection. Laboratory findings revealed significantly elevated levels of WBC, log2‑transformed SII and AISI, CRP, ALT, AST, CK, and LDH, alongside lower levels of RBC, HGB, and TP (all p < 0.05). Detailed information was presented in Table 1. Furthermore, among male patients aged ≤3 years, the incidence of OM was 34.15%, compared with 40.43% among their female counterparts (Table S1). No statistically significant difference in OM incidence was observed between sexes across any age group (Table S2).
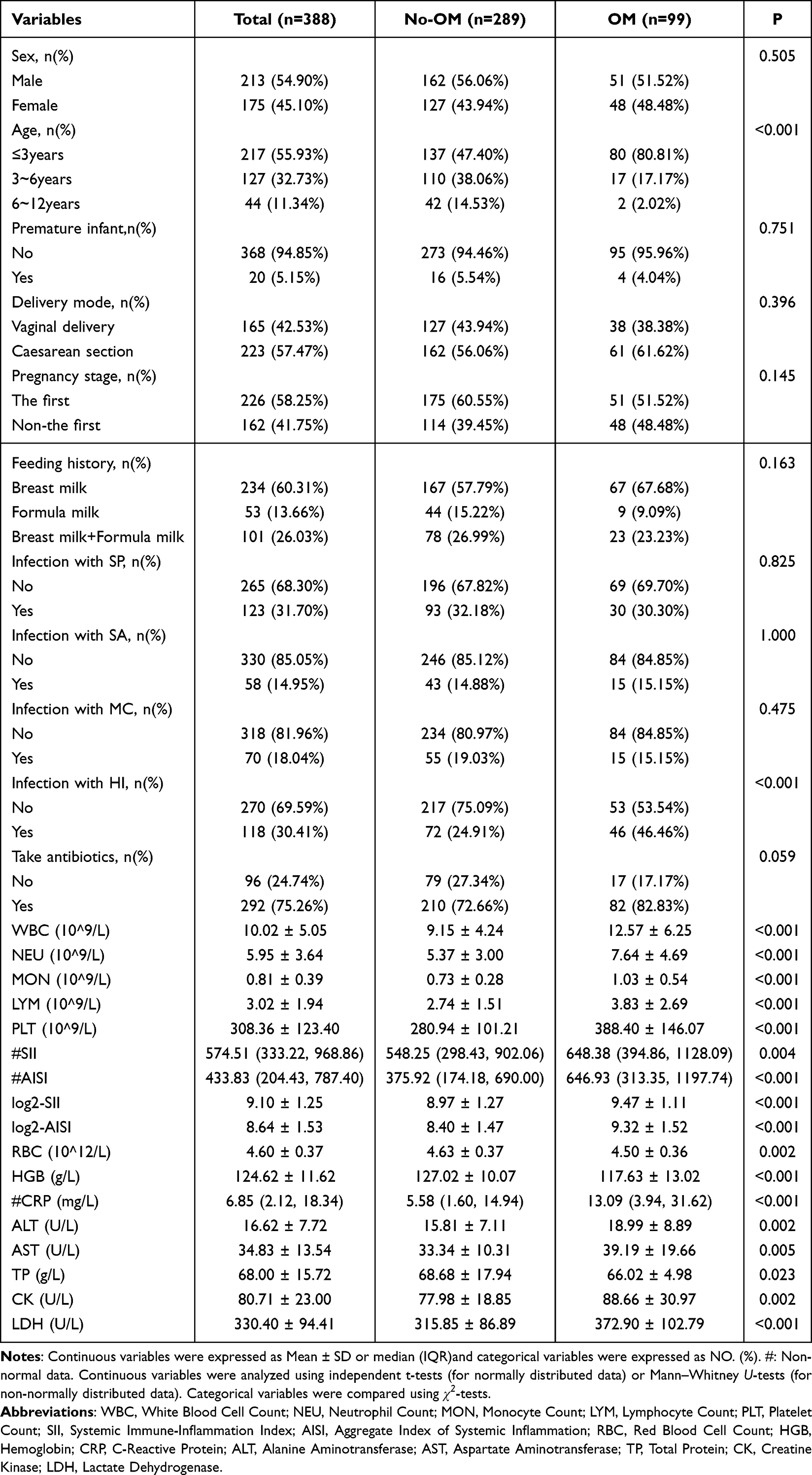 |
Table 1 Comparison of Baseline Characteristics |
Univariate Logistic Regression Analysis of OM Risk
As shown in Table 2, the results showed age (3~6 years: OR = 0.27, 95% CI: 0.15–0.47, p < 0.001; 6~12 years: OR = 0.09, 95% CI: 0.01–0.30, p = 0.001), infection with HI (OR = 2.61, 95% CI: 1.62–4.21, p < 0.001), take antibiotics (OR = 1.80, 95% CI: 1.02–3.32, p = 0.041), log2-SII (OR = 1.42, 95% CI: 1.16–1.73, p = 0.001), log2-AISI (OR = 1.54, 95% CI: 1.30–1.84, p < 0.001), WBC (OR = 1.14, 95% CI: 1.08–1.20, p < 0.001), RBC (OR = 0.37, 95% CI: 0.19–0.73, p = 0.004), HGB (OR = 0.93, 95% CI: 0.90–0.95, p < 0.001), CRP (OR = 1.02, 95% CI: 1.01–1.04, p < 0.001), ALT (OR = 1.05, 95% CI: 1.02–1.08, p = 0.001), AST (OR = 1.03, 95% CI: 1.01–1.05, p = 0.001), TP (OR = 0.92, 95% CI: 0.87–0.97, p = 0.002), CK (OR = 1.02, 95% CI: 1.01–1.03, p < 0.001) and LDH (OR = 1.01, 95% CI: 1.00–1.01, p < 0.001) were influencing factors of OM.
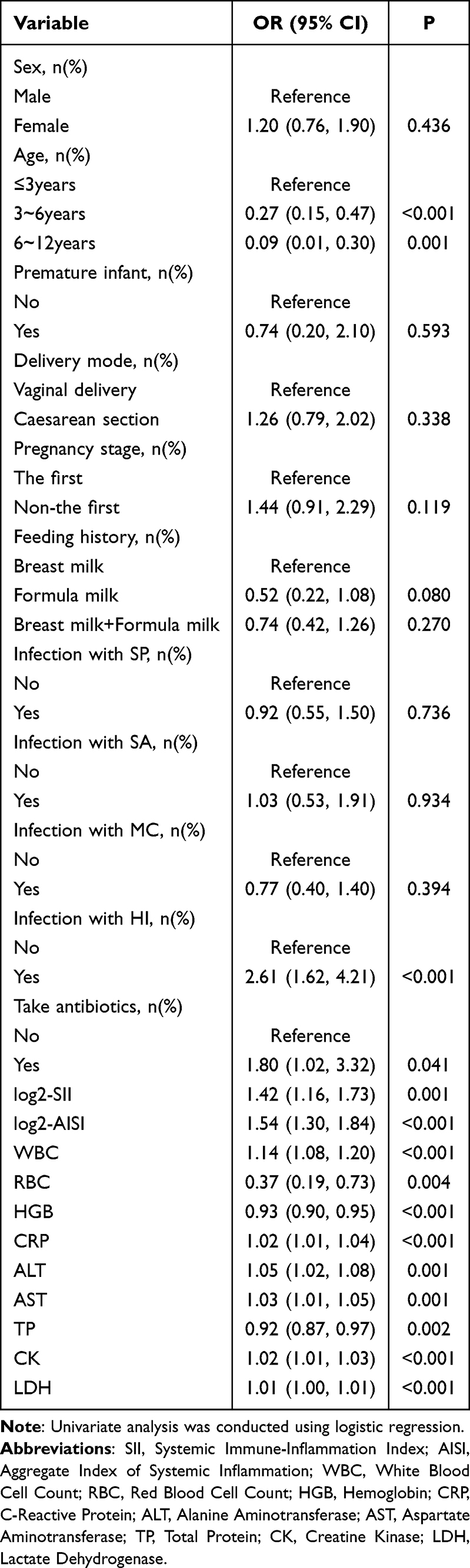 |
Table 2 Univariate Logistic Regression Analysis |
Multivariate Logistic Regression Analysis of OM Risk
Two multiple logistic regression models were constructed, incorporating log2-SII and log2-AISI. Table 3 summarized the results of log2-SII model. Model 1 showed log2-SII was a OM risk factor (OR = 1.39, 95% CI: 1.06–1.85, p = 0.022). To enhance predictive performance, we employed a backward stepwise logistic regression approach. Model 2 also showed log2-SII (OR = 1.38, 95% CI: 1.05–1.82, p = 0.021) was influencing factors.
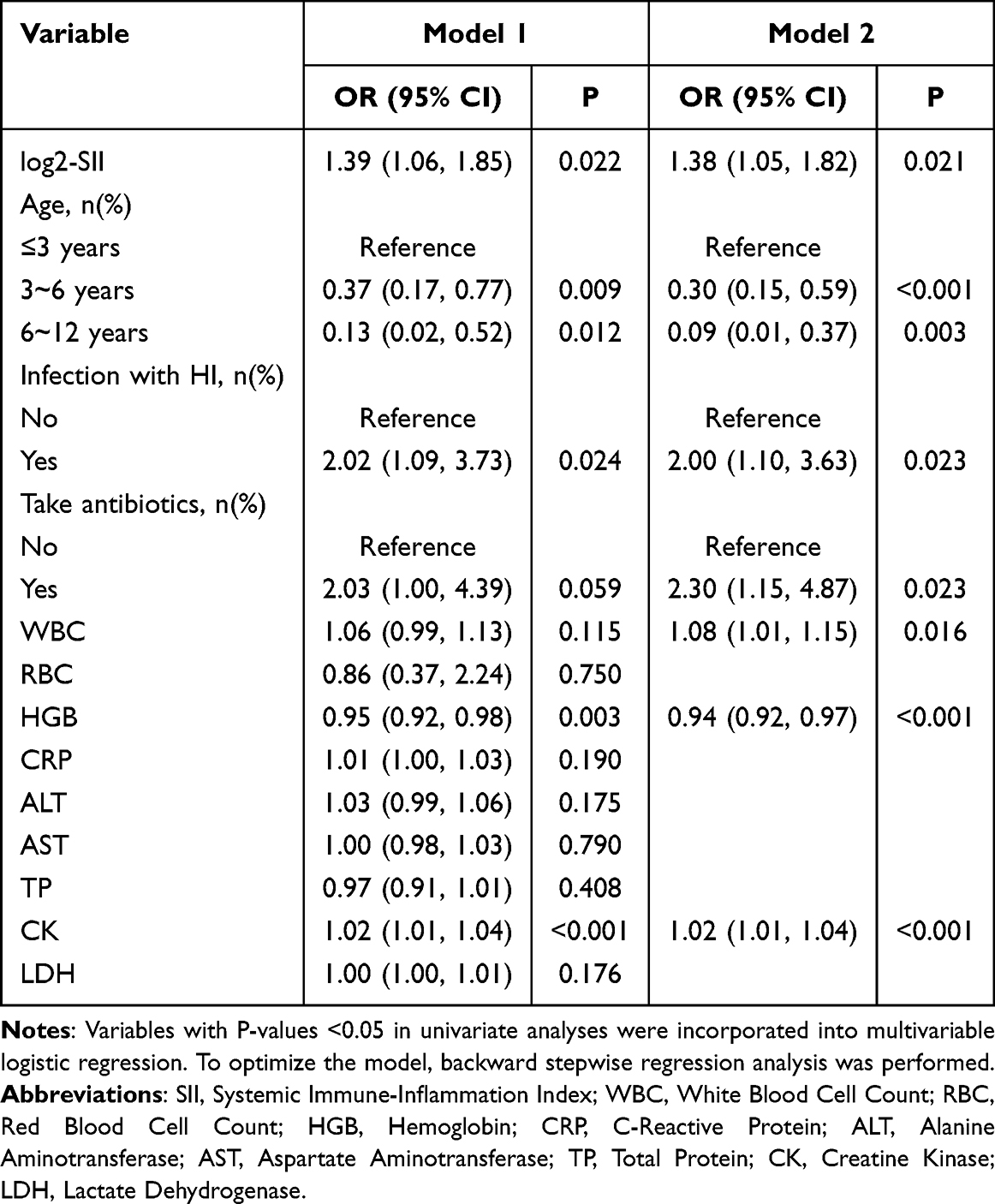 |
Table 3 Log2-SII Multivariate Logistic Regression Model |
Table 4 summarized the results of log2-AISI model. Model 1 showed log2-AISI was a OM risk factor (OR = 1.37, 95% CI: 1.07–1.79, p = 0.015). Model 2 also showed log2-AISI was a OM risk factor (OR = 1.37, 95% CI: 1.07–1.78, p < 0.001).
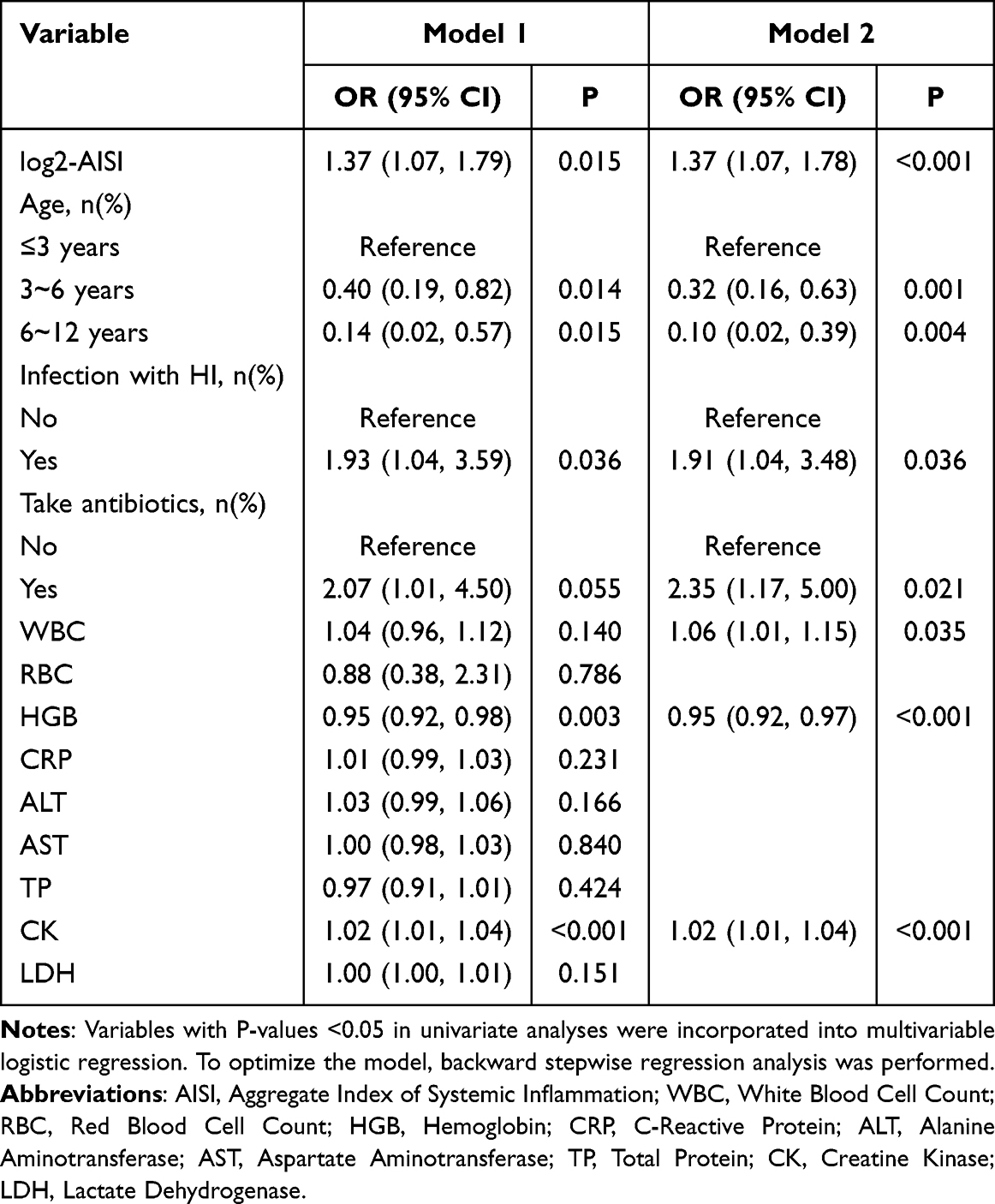 |
Table 4 Log2-AISI Multivariate Logistic Regression Model |
Nomogram for Predicting OM Risk
Based on Model 2, we built two nomograms (Figure 2). The nomograms showed higher log2-SII, higher log2-AISI, age 3–12 years, infection with HI, take antibiotics, higher WBC, lower HGB and higher CK were risk factors for OM. When using the nomogram to predict OM risk, doctors can place on the corresponding axes based on the patient’s risk factors. The assigned scores from each factor were summed to obtain a total score. A higher total score indicated a greater risk of OM. Using the bootstrap method (1000 times), a calibration curve was plotted to evaluate the model. Predictive accuracy is visually assessed by the proximity of the solid line (the predictions) to the dashed diagonal (the ideal line). Greater alignment between the two signifies a more accurate model (Figure 3). The mean absolute error of log2-SII nomogram model was 0.024 (Figure 3A), and log2-AISI nomogram model was 0.023 (Figure 3B), which showed that the predicted values were in good agreement with the actual values. AUC of log2-SII nomogram was 0.827 (95% CI: 0.780–0.875), with a sensitivity of 0.768 and a specificity of 0.737 (Figure 4A); AUC of log2-AISI nomogram was 0.834 (95% CI: 0.788–0.881), with a sensitivity of 0.758 and a specificity of 0.747 (Figure 4B). In addition, the log2-AISI nomogram had a higher AUC than the log2-SII nomogram, indicating that the models had good discrimination ability. DCA showed the nomogram provided superior net benefit compared to the “treat-all” and “treat-none” strategies across the entire threshold probability range (10–90%), supporting its clinical utility (Figure 5).
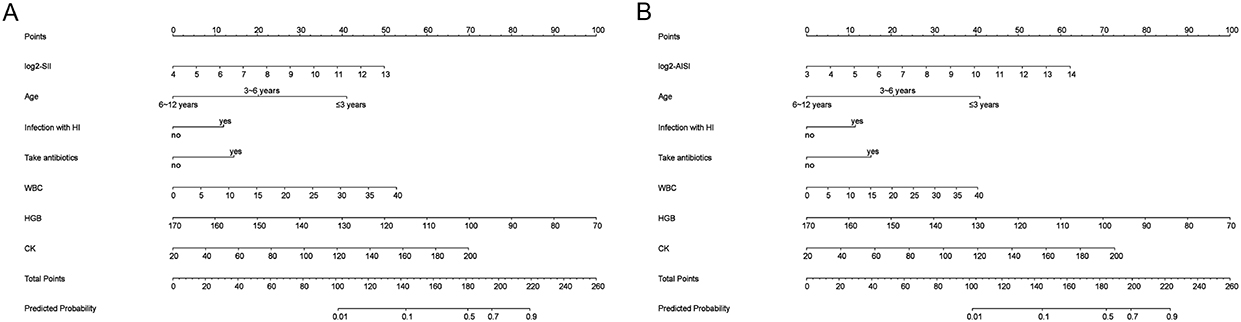 |
Figure 2 Nomogram models (A) log2-SII; (B) log2-AISI. (Scores were obtained from each scale according to patient-specific indicators, with total scores corresponding to predicted probabilities after summation. Higher total scores indicated greater OM risk). |
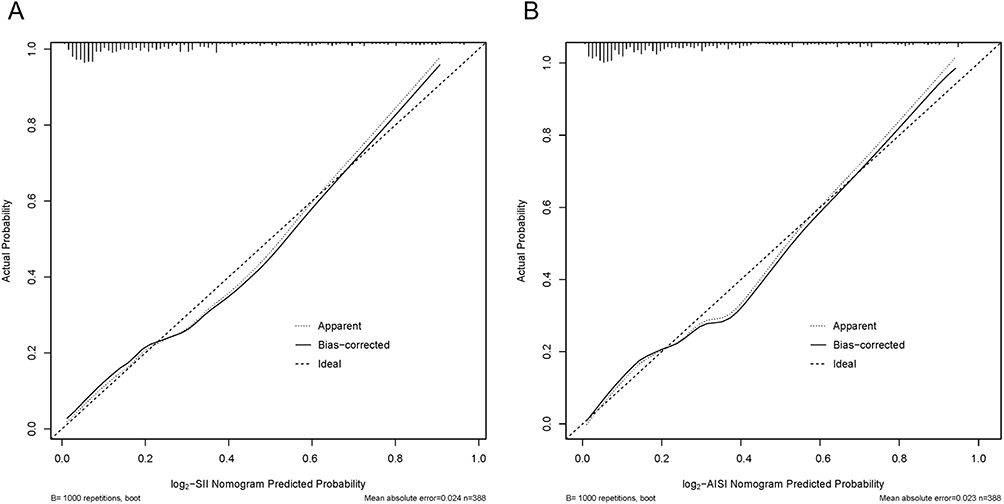 |
Figure 3 Calibration curves of nomogram model (A) log2-SII; (B) log2-AISI. (The calibration curve was generated using 1000 bootstrap repetitions. The diagonal dashed line represents the ideal case of perfect prediction, while the solid line indicates the actual performance of our model. Closer agreement between the two lines signifies better predictive accuracy). |
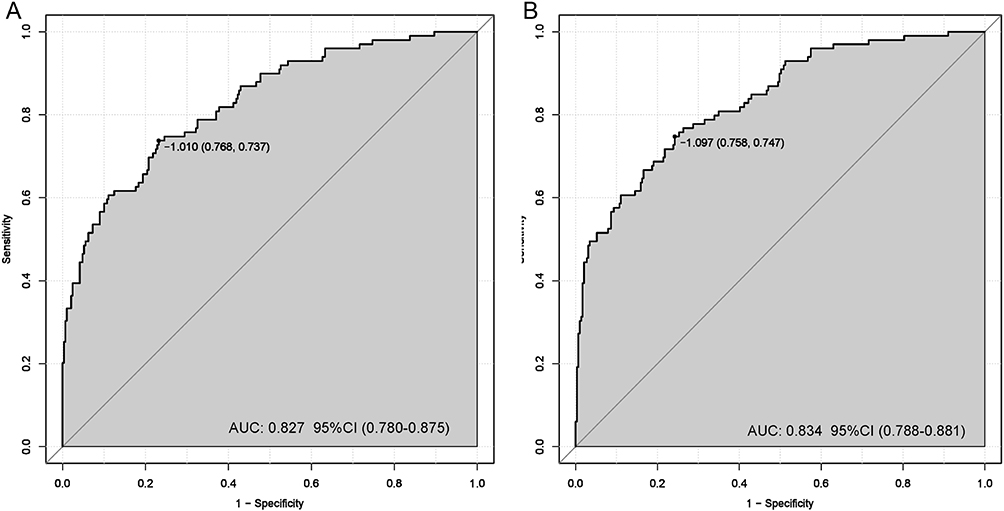 |
Figure 4 ROC curves of nomogram model (A) log2-SII; (B) log2-AISI. (AUC > 0.7 indicateing that the model possesses a relatively good discriminatory ability and accuracy). |
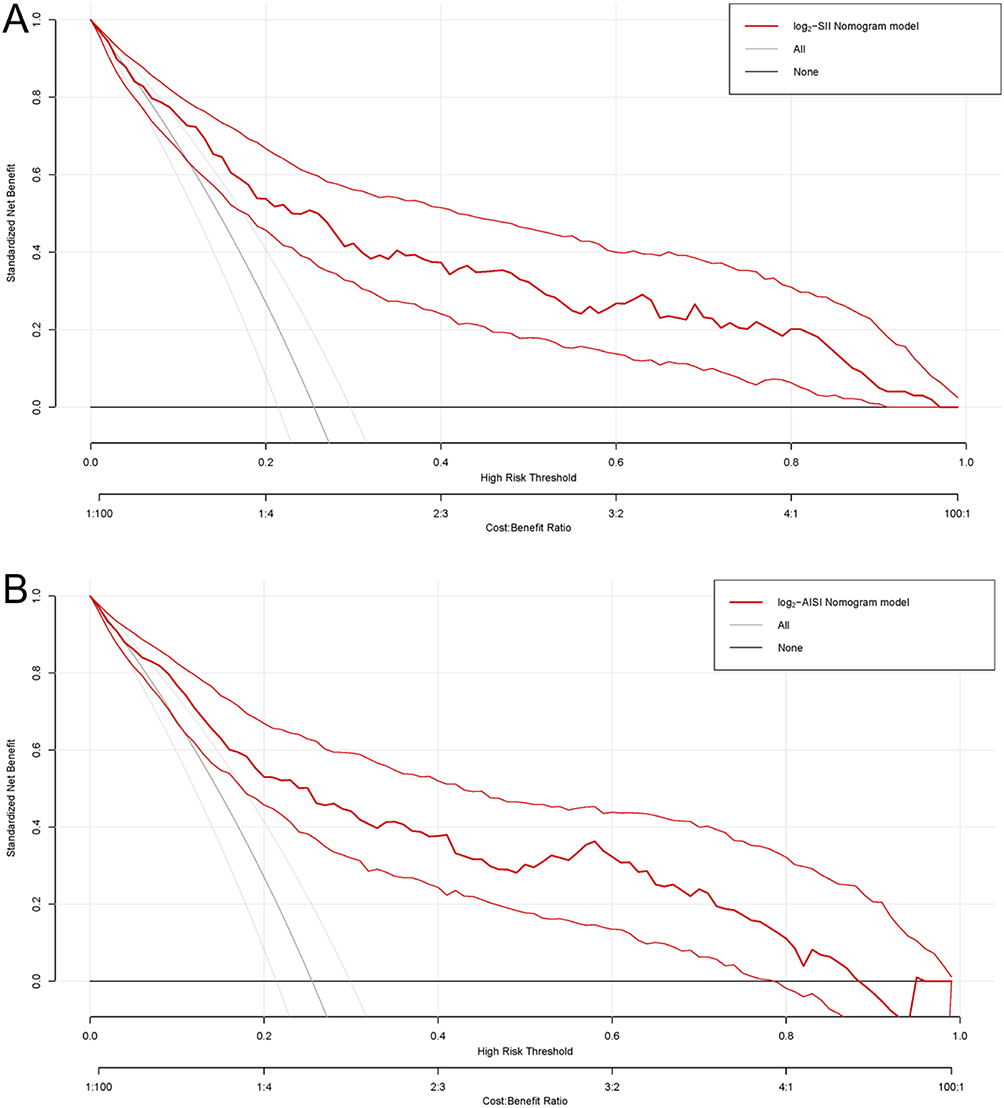 |
Figure 5 Decision curve analysis of nomogram model (A) log2-SII; (B) log2-AISI. (Nomograms offered a greater net benefit compared to both the “treat-all” and “treat-none” approaches over a threshold probability range from 10% to 90%, confirming its clinical utility in routine practice). |
Relationship Between SII, AISI and OM in Children with Bacterial Pneumonia
In the overall population, univariate logistic regression results (Model 1) showed a positive association between log2-SII (OR: 1.42, 95% CI: 1.16–1.73, p < 0.001), log2-AISI (OR: 1.54, 95% CI: 1.30–1.84, p < 0.001) and OM. After adjusting for age, infection with HI and take antibiotics, Model 2 showed log2-SII (OR: 1.60, 95% CI: 1.28–2.02, p < 0.001) and log2-AISI (OR: 1.54, 95% CI: 1.27–1.86, p < 0.001). After full covariate adjustment, Model 3 showed log2-SII (OR: 1.51, 95% CI: 1.18–1.94, p = 0.001) and log2-AISI (OR: 1.45, 95% CI: 1.18–1.80, p < 0.001). Detailed results were shown in Table 5.
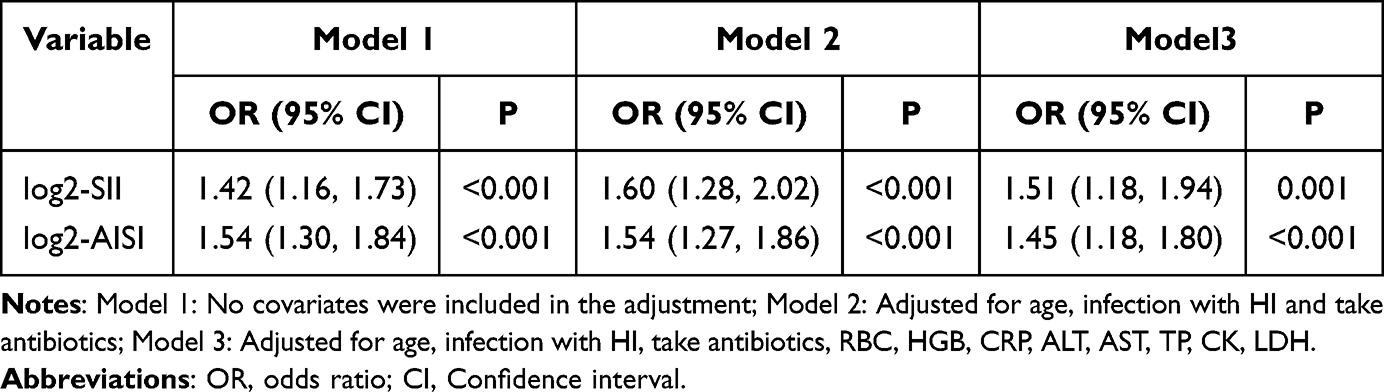 |
Table 5 The Relationship Between SII, AISI and OM Risk Used Logistic Regression Analysis |
A significant linear association between log2-SII, log2-AISI and OM risk was revealed by restricted cubic spline (RCS) analysis (Figure 6). In the fully adjusted Model 3, the inflection point for log2-SII was identified at 9.71 (Figure 6A), the inflection point for log2-AISI was identified at 8.16 (Figure 6B), respectively. The results indicated that OM risk remained low when log2-SII and log2-AISIwere below their threshold points, but increased rapidly once these indices exceeded their respective thresholds.
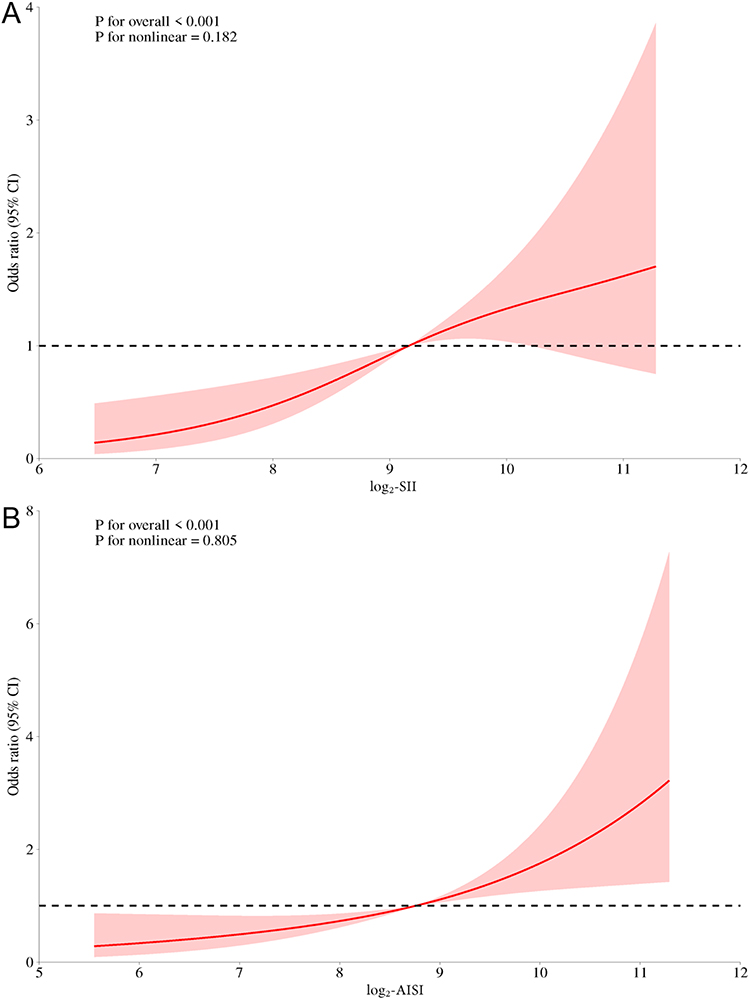 |
Figure 6 Relationship between SII, AISI and OMrisk (A) log2-SII; (B) log2-AISI. (RCS shows a linear relationship between log2-SII, log2-AISI and OM risk. The fitted regression line is a solid red line; the black dashed line indicates the position where the OR is equal to 1; the red shaded area indicates the 95% CI). |
Discussion
Our study identified both SII and AISI were associated with hospital-acquired OM in children with bacterial pneumonia. This finding extended the known clinical utility of these hematological indices from chronic and oncologic diseases to acute infectious complications. The primary mechanistic link lies in their capacity to quantify a pro-inflammatory, yet immunologically dysregulated, host state that predisposes the middle ear to secondary infection.
This imbalance is critical in the etiopathogenesis of secondary OM through the following interconnected pathways: (1) Systemic inflammation and middle ear Immune activation. During bacterial pneumonia, the systemic inflammatory response can exacerbate OM.29,30 Elevated neutrophils and platelets indicate myeloid activation, this immune environment facilitates the dissemination of pathogens and the formation of localized infections.31 In pediatric bacterial pneumonia, increased SII and AISI correlate with higher circulating pro-inflammatory mediators (eg, TNF-α, IL-1β, IL-6).32 These cytokines enhance vascular permeability, enabling immune cell infiltration into sites such as the middle ear and triggering local inflammation.33 They may also impair Eustachian tube function and reduce mucociliary clearance, promoting pathogen colonization. (2) Immune dysfunction and regulatory imbalance. Severe bacterial pneumonia is associated with reduced CD8⁺ T-cell subsets, suggesting impaired adaptive immunity.22 Severe infection leads to T-cell exhaustion and diminished effector responses.34 This exhaustion is particularly evident in children with hospital-acquired OM. Compensatory immune mobilization against new infections may further deplete systemic immune resources. (3) Complexity of interactions between microbes and hosts. Pathogen dominance in the respiratory tract can facilitate bacterial migration to the middle ear via mechanisms such as molecular mimicry and immune evasion.35,36 Dysbiosis and systemic inflammation exhibit a bidirectional relationship: respiratory microbiota imbalance can exacerbate inflammation (elevating SII/AISI), while systemic inflammation alters the respiratory and Eustachian tube microenvironment, further disrupting microbial balance.37
Previous studies had found that SII and AISI were risk factors of various diseases, such as tumors and cardiovascular diseases.38,39 This association is largely driven by a sustained systemic inflammatory response, which releases proinflammatory cytokines (eg, TNF-α, IL-1β, IL-6) that damage vascular endothelial and tissue cells, thereby fostering a disease-promoting microenvironment.40 In the context of middle ear infection, pathogen recognition by mucosal epithelial cells and resident macrophages triggers rapid chemokine release. These signals guide neutrophils across the vascular endothelium into the infected cavity. Systemic immune indices such as the SII and AISI are derived from peripheral counts of neutrophils, monocytes, lymphocytes, and platelets. Alterations in these indices reflect not only the magnitude of systemic inflammation but also specific changes in the functional contributions of these cellular components to middle ear pathology. (1) Neutrophils. An elevated neutrophil count, a key driver of high SII/AISI, signifies a robust but potentially damaging innate immune surge. Upon infiltrating the middle ear, neutrophils combat pathogens through phagocytosis, ROS release, and NET formation. However, this intense activity directly contributes to mucosal barrier disruption, tissue edema, and pus formation, manifesting clinically as acute otalgia and fever.41 (2) Monocytes. Circulating monocytes differentiate into tissue macrophages. An increase in monocyte count contributes to systemic inflammation. In the middle ear, M1-phenotype macrophages dominate early inflammation, while a transition to the M2 phenotype is vital for tissue repair.42 They clear debris and present antigens, bridging innate and adaptive immunity.43 Dysregulation in this population can skew the inflammatory response towards chronicity. (3) Lymphocytes. B lymphocytes, with T cell help, differentiate into antibody-secreting plasma cells. These pathogen-specific antibodies neutralize toxins and promote opsonophagocytosis, a key clearance mechanism evidenced by their abundance in middle ear effusions during secretory OM.44 Helper T cells orchestrate the immune response by releasing cytokines that direct macrophages, neutrophils, and B cells. Cytotoxic T cells directly eliminate infected host cells, while regulatory T cells modulate inflammation and limit tissue damage through inhibitory cytokines such as IL-10 and TGF-β.45 (4) Platelets. An elevated platelet count elevates both SII and AISI. Platelets are active inflammatory mediators. By adhering to leukocytes, they enhance chemotaxis and ROS production, amplifying inflammation.46 Furthermore, platelet aggregation can induce microthrombi, compromising middle ear mucosal microcirculation. This exacerbates local hypoxia and effusion accumulation, and in severe cases, may facilitate the spread of inflammation to the mastoid, increasing the risk of acute mastoiditis.47
Furthermore, this study identified several independent risk factors for hospital-acquired OM, which can be contextualized within three overarching pathogenic themes linking them to the core disease process. (1) Anatomy and Physiology. The Eustachian tube in children (age ≤ 3 years) is structurally and functionally underdeveloped. Its short, horizontal orientation, weak cartilage, and inefficient tensor veli palatini muscle impair ventilation and drainage.47 This dysfunction permits the reflux of pathogens and secretions into the middle ear, initiating OM.48 (2) Microbiome Ecology. Specific microbiological factors further increase vulnerability. Haemophilus influenzae (HI) employs robust biofilm formation and adhesins (eg, pili) to enhance its colonization and persistence in the nasopharynx and middle ear.49,50 Prior antibiotic use exacerbates this risk by disrupting the commensal nasopharyngeal microbiome, diminishing colonization resistance, and selecting for resistant HI strains. (3) Systemic Vulnerability and Metabolic Imbalance. Several hematological and biochemical markers point to a systemically compromised host state conducive to OM. (a) Anemia (reflected by lower RBC and HGB), often indicative of nutritional iron deficiency, can impair T-cell function and phagocytic activity, weakening mucosal immunity.51,52 (b) Hepatic Dysfunction (suggested by elevated ALT/AST with decreased TP) may compromise systemic protein synthesis and immune capacity, hindering effective infection resolution.53 (c) Tissue Injury and Hypoxia (indicated by elevated CK and LDH) intensify local inflammation and nasopharyngeal edema, which can obstruct eustachian tube drainage. Local hypoxia may further elevate LDH via anaerobic metabolism, impeding mucosal repair and fostering pathogen proliferation.54,55
However, this study had several limitations. First, as a single center study, external validation was not possible. Second, as a retrospective study, it cannot establish a causal relationship between SII, AISI, and OM. Third, the small sample size may affect the stability of results. Fourth, the factors included in this study were limited, other inflammatory markers (such as IL-6 and TNF-α) were not analyzed. Fifth, this study focused on hematological and biochemical indices of inflammation. While we adjusted for key clinical confounders (eg, age, prior antibiotic use) in the analysis, other potentially relevant demographic and lifestyle factors (such as detailed dietary history, family size, or birth order) were not examined. These factors may influence host susceptibility or the microenvironment in the nasopharynx and middle ear independently of systemic inflammation. Based on limitations, future research can be pursued in the following areas. (1) Incorporating Multidimensional Data: Prospective, large-scale studies should systematically collect and integrate the systemic inflammatory indices (SII, AISI) with detailed demographic (eg, age, sex), socioeconomic, and lifestyle data (such as dietary patterns, household size, and birth order). This approach would allow for the dissection of independent and interactive effects between a pro-inflammatory host state and broader environmental or host-constitutional risk factors. (2) Refining the Biomarker Panel: Expanding the biochemical profile to include a wider array of specific inflammatory mediators (eg, IL-6, TNF-α) and nutritional markers would enhance the granularity of risk prediction. This could help determine whether the composite indices SII, AISI act as surrogates for specific cytokine milieus or distinct biological pathways. (3) Elucidating Causal Pathways: To move beyond association, mechanistic studies are needed. These should investigate how the systemic inflammation captured by SII, AISI directly modulates the local microenvironment of the nasopharynx and middle ear, and how this interaction may be modified by the factors mentioned above.
Conclusion
This study established a significant association between elevated SII, elevated AISI and an increased risk of hospital-acquired OM in children with bacterial pneumonia, thereby achieving our primary objective of elucidating the role of systemic inflammation in secondary complications. These indices function as integrative biomarkers, reflecting the specific pro-inflammatory and immune-dysregulated host state that predisposes patients to middle ear infection. Consequently, monitoring SII and AISI levels may aid clinicians in identifying high-risk patients who would benefit from heightened vigilance and supportive management to mitigate OM risk.
Abbreviations
SII, Systemic immune-inflammation index; AISI, Systemic Inflammatory Response Syndrome Index; SP, Streptococcus pneumoniae; SA, Staphylococcus aureus; MC, Moraxella catarrhalis; HI, Haemophilus influenzae; WBC, White blood cell; PLT, Platelet; RBC, Red blood cell; HGB, Hemoglobin; CRP, C-reactive protein; SAA, Serum amyloid protein A; ALT, Alanine aminotransferase; AST, Aspartate aminotransferase; TP, Total protein; CK, Creatine kinase; LDH, Lactate dehydrogenase; PCT, Procalcitonin; ESR, Erythrocyte sedimentation rate; IL-1β, Interleukin-1β; IL-6, Interleukin 6; TNF-α, Tumor Necrosis Factor-α; IL-10, Interleukin 10; TGF-β, Transforming growth factor β; OM, Otitis media; IQR, Interquartile range; ORs, Odds ratios; CI, Confidence intervals; ROC, Receiver operating characteristic; AUC, Area under the curve; DCA, Decision curve analysis; RCS, Restricted cubic spline; ROS, Reactive oxygen species; NETs, Neutrophil extracellular traps.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This retrospective investigation was conducted in accordance with the Helsinki Declaration. Ethical approval was granted by the Ethical Committee of Tangshan Maternal and Child Health Care Hospital (Approval Number: 2023-080-01), which also waived the need for informed consent due to the study’s retrospective design. All data were anonymized and handled exclusively by the research team in a secure environment, used solely for this study without disclosure for any other purpose.
Consent for Publication
Written informed consent for publication was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Supported by Key Laboratory of Molecular Medicine for Abnormal Development and Related Diseases in Tangshan City (NO.2022TS008b).
Disclosure
No conflicts of interest were disclosed by the authors.
References
1. Liu J, Bao B, Zhang T, Jia W, Guo C, Song C. Comparative analysis of the clinical characteristics of severe mycoplasma pneumoniae pneumonia and severe bacterial pneumonia in children. BMC Pediatr. 2025;25(1):439. doi:10.1186/s12887-025-05804-4
2. Mao Z, Liu C, Ni J, et al. Gut derived (S)-equol mitigates influenza viral pneumonia by modulating macrophage polarization via Nrf2 mediated AKT/ERK/NF-κb signaling pathways. Free Radic Biol Med. 2025;239:457–17. doi:10.1016/j.freeradbiomed.2025.08.004
3. Xie S, Wu M, Shang Y, et al. Development and validation of an early diagnosis model for severe mycoplasma pneumonia in children based on interpretable machine learning. Respir Res. 2025;26(1):182. doi:10.1186/s12931-025-03262-1
4. Kyu HH, Vongpradith A, Sirota SB, Novotney A, Troeger CE, Doxey MC. Age-sex differences in the global burden of lower respiratory infections and risk factors, 1990-2019: results from the global burden of disease study 2019. Lancet Infect Dis. 2022;22(11):1626–1647. doi:10.1016/S1473-3099(22)00510-2
5. Troeger C, Blacker B, Khalil IA, Rao PC, Cao J, Zimsen SRM. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Infect Dis. 2018;18(11):1191–1210. doi:10.1016/S1473-3099(18)30310-4
6. Moleleki M, Reddy C, Ndlangisa K, et al. Respiratory pathogens detected in children aged <5 years hospitalized with severe respiratory illness, South Africa, 2017. Front Pediatr. 2025;13:1498197. doi:10.3389/fped.2025.1498197
7. Li J, Si J, Yang Y, et al. The value of CT-based radiomics for differentiation of pleural effusions in bacterial pneumonia and mycoplasma pneumoniae pneumonia in children. Transl Pediatr. 2025;14(1):70–79. doi:10.21037/tp-24-364
8. Mokhaberi N, Vasileiadis V, Ambs JM, Reinshagen K. Pneumothorax after VATS for pleural empyema in pediatric patients. Child Basel Switz. 2025;12(2):154. doi:10.3390/children12020154
9. Islam N, Mohsin ASM, Choudhury SH, et al. COVID-19 and pneumonia detection and web deployment from CT scan and X-ray images using deep learning. PLoS One. 2024;19(7):e0302413. doi:10.1371/journal.pone.0302413
10. Tian Z, Zhang Y, Yun J, Kuang W, Li J. Advances in nanotechnology for the therapy of bacterial pneumonia. Front Cell Infect Microbiol. 2025;15:1639783. doi:10.3389/fcimb.2025.1639783
11. Gaudin J, Thayalakulasingam T. Invasive pneumococcal disease and COVID-19 with acute otitis media and a tegmen tympani defect. Cureus. 2023;15(9):e44869. doi:10.7759/cureus.44869
12. Mina MJ, Klugman KP, Rosch JW, McCullers JA. Live attenuated influenza virus increases pneumococcal translocation and persistence within the middle ear. J Infect Dis. 2015;212(2):195–201. doi:10.1093/infdis/jiu804
13. Rich JR, Dymock M, Seppanen EJ, et al. Evaluating the impact of the “blow, breathe, cough” health promotion intervention in resolving otitis media with effusion in children: an adaptive randomized-controlled trial protocol. Contemp Clin Trials Commun. 2025;47:101531. doi:10.1016/j.conctc.2025.101531
14. Pagano AS, Márquez S, Smith CM, et al. Identification of critical windows in early development of human upper respiratory tract and middle ear disease. Anat Rec. 2021;304(9):1953–1973. doi:10.1002/ar.24600
15. Mauthner R, Marom T, Klein A, et al. Pediatric acute mastoiditis severity - Can inflammatory biomarkers help us? Int J Pediatr Otorhinolaryngol. 2025;195:112405. doi:10.1016/j.ijporl.2025.112405
16. Vanneste P, Page C. Otitis media with effusion in children: pathophysiology, diagnosis, and treatment. A review. J Otol. 2019;14(2):33–39. doi:10.1016/j.joto.2019.01.005
17. Jotic A, Cirkovic I, Jovicic N, et al. Biofilm formation and its relationship with the microbiome in pediatric otitis media. Microorganisms. 2025;13(12):2760. doi:10.3390/microorganisms13122760
18. Brennan-Jones CG, Head K, Chong LY, et al. Topical antibiotics for chronic suppurative otitis media. Cochrane Database Syst Rev. 2025;6(6):CD013051. doi:10.1002/14651858.CD013051.pub3
19. Manole A, Mărcuț LF, Cârciumaru R, Manole F. Preventing recurrent otitis media in children aged 2-7 years: a cross-sectional evaluation of serum vitamin D as a modifiable factor. Diagnostics. 2025;15(5):519. doi:10.3390/diagnostics15050519
20. Higuchi N, Sawane K, Tanaka T, et al. Association of cytokines in breast milk with otitis media infection and fever frequency in infants: a case-control study. Breastfeed Med. 2025;20(10):729–736. doi:10.1177/15568253251363255
21. Xiong J, Zhang D, Yuan Y, Quan C, Xie N. Association between systemic immune-inflammation index and female breast cancer based on NHANES data (2001-2018): a cross-sectional study. PLoS One. 2025;20(9):e0330571. doi:10.1371/journal.pone.0330571
22. Xiao K, Cao Y, Yan P, et al. A large-scale single-cell atlas reveals the peripheral immune panorama of bacterial pneumonia. Am J Respir Crit Care Med. 2025;211(12):2363–2381. doi:10.1164/rccm.202501-0217OC
23. Wang R, Chen R, Tao W, Cheng X. Nonlinear associations between the aggregate index of systemic inflammation and cardiovascular disease in adults: evidence from NHANES 2011-2020. BMC Public Health. 2025;25(1):3031. doi:10.1186/s12889-025-24320-9
24. Zhang Z, Li C, Xiao Y, et al. Integrated machine learning and population attributable fraction analysis of systemic inflammatory indices for mortality risk prediction in diabetes and prediabetes. Ann Med. 2025;57(1):2536204. doi:10.1080/07853890.2025.2536204
25. Shorr AF, Jones ME, Friedmann S, et al. Ceftobiprole versus ceftriaxone ± linezolid in community-acquired bacterial pneumonia (CABP): re-analysis of a randomized, Phase 3 study using 2020 FDA guidance. PLoS One. 2025;20(6):e0326758. doi:10.1371/journal.pone.0326758
26. Agarwal M, Juliano AF, Hagiwara M, et al. ACR appropriateness criteria® inflammatory ear disease. J Am Coll Radiol. 2025;22(5S):S300–S318. doi:10.1016/j.jacr.2025.02.026
27. Li R, Atawula A, Li H, et al. Association between novel immune-inflammatory markers and hypertension patients with coronary heart disease: a cross-sectional study based on NHANES (2005-2016). BMC Cardiovasc Disord. 2025;25(1):467. doi:10.1186/s12872-025-04906-2
28. Chen Y, Cai SL. Effect of early micro-breastfeeding on growth rate and postpartum depression in preterm infants with low-birth-weight. World J Psychiatry. 2025;15(8):108919. doi:10.5498/wjp.v15.i8.108919
29. Zheng B, Jin H. Exploring the role of gut probiotic metabolites in the prevention and treatment of otitis media. Front Cell Infect Microbiol. 2025;15:1661871. doi:10.3389/fcimb.2025.1661871
30. Chen Y, Zhang X, Liu Y, et al. Deciphering cytokine dynamics: staged immune responses in acute otitis media. Microbiol Pathogen. 2025;207:107884. doi:10.1016/j.micpath.2025.107884
31. Loupy A, Preka E, Chen X, Wang H, He J, Zhang K. Reshaping transplantation with AI, emerging technologies and xenotransplantation. Nat Med. 2025;31(7):2161–2173. doi:10.1038/s41591-025-03801-9
32. Iordache MP, Buliman A, Costea-Firan C, et al. Immunological and inflammatory biomarkers in the prognosis, prevention, and treatment of ischemic stroke: a review of a decade of advancement. Int J Mol Sci. 2025;26(16):7928. doi:10.3390/ijms26167928
33. Heo KW, Pak K, Kurabi A, Ryan AF. Leukotriene B4 is a major determinant of leukocyte recruitment during otitis media. Front Cell Infect Microbiol. 2021;11:768815. doi:10.3389/fcimb.2021.768815
34. Bian LQ, Bi Y, Zhou SW, et al. T cell responses in senior patients with community-acquired pneumonia related to disease severity. Exp Cell Res. 2017;361(1):56–62. doi:10.1016/j.yexcr.2017.09.041
35. Aldakheel FM, Alduraywish SA. Discovery of novel DdlA inhibitors in multidrug-resistant pseudomonas aeruginosa using virtual screening, molecular docking, and dynamics simulations. Sci Rep. 2025;15(1):15290. doi:10.1038/s41598-025-97698-6
36. Guerra FE, Karlinsey JE, Libby SJ, Fang FC. Evasion of serum antibodies and complement by salmonella typhi and paratyphi a. PLOS Pathog. 2025;21(5):e1012917. doi:10.1371/journal.ppat.1012917
37. Duff AF, Jurcisek JA, Kurbatfinski N, et al. Oral and middle ear delivery of otitis media standard of care antibiotics, but not biofilm-targeted antibodies, alter chinchilla nasopharyngeal and fecal microbiomes. npj Biofilms Microbiomes. 2024;10(1):10. doi:10.1038/s41522-024-00481-0
38. Zhou J, Tan B, Gao F. Prognostic values of combined ratios of white blood cells in glioma: a systematic review and meta-analysis. Neurosurg Rev. 2024;47(1):831. doi:10.1007/s10143-024-03064-x
39. Tang J, Li TX, Deng L, Huang XC, He PY, Zhao H. Inflammatory indices AISI and SIRI in atherosclerosis risk stratification: validation across community and intensive care populations. Ann Med. 2025;57(1):2530792. doi:10.1080/07853890.2025.2530792
40. Poredos P, Poredos P. Inflammation-a link between arterial atherosclerotic and venous thromboembolic diseases. Cells. 2025;14(17):1319. doi:10.3390/cells14171319
41. Wang C, Zhang S, Zeng F, et al. Neutrophil extracellular traps-inspired hydrogen-bonded organic framework-based bio-orthogonal nanozymes for enhanced bacterial capture and sterilization. ACS Appl Mater Interfaces. 2025;17(33):47396–47411. doi:10.1021/acsami.5c11332
42. Mantovani A, Biswas SK, Galdiero MR, Sica A, Locati M. Macrophage plasticity and polarization in tissue repair and remodelling. J Pathol. 2013;229(2):176–185. doi:10.1002/path.4133
43. Slarve M, Nielsen T, Yu D, VanOrman J, Luna B, Spellberg B. Evaluating antibody mediated opsonophagocytosis of bacteria via lab protocol: RAW 264.7 cell phagocytosis assay. PLoS One. 2025;20(9):e0331445. doi:10.1371/journal.pone.0331445
44. Phad GE, Pinto D, Foglierini M, et al. Clonal structure, stability and dynamics of human memory B cells and circulating plasmablasts. Nat Immunol. 2022;23(7):1076–1085. doi:10.1038/s41590-022-01230-1
45. Guo H, Wang B, Wu Z, et al. CD8+HLA-DR+CD27+ T cells define a population of naturally occurring regulatory precursors in humans. Sci Adv. 2025;11(37):eadw1702. doi:10.1126/sciadv.adw1702
46. Kaiser R, Anjum A, Nicolai L. Platelet heterogeneity in disease: the many and the diverse? Blood. 2025;
47. Duygu E, Şevik Eliçora S. Our experience on the management of acute mastoiditis in pediatric acute otitis media patients. Int J Pediatr Otorhinolaryngol. 2020;138:110372. doi:10.1016/j.ijporl.2020.110372
48. Fricano EE, Gremba AP, Teixeira MS, Swarts JD, Alper CM. Using geometric morphometric analysis of magnetic resonance imaging to assess the anatomy of the eustachian tube in children with and without otitis media. Bioengineering. 2023;10(10):1115. doi:10.3390/bioengineering10101115
49. Seppanen EJ, Bayliss J, Clark SL, et al. Haemophilus influenzae remains the predominant otitis media pathogen in australian children undergoing ventilation tube insertion in the PCV13 era. J Infect. 2025;90(4):106478. doi:10.1016/j.jinf.2025.106478
50. Principi N, Esposito S. Biofilm production and its implications in pediatrics. Microorganisms. 2024;12(8):1522. doi:10.3390/microorganisms12081522
51. Cao J, Yang Z, Liu W, Chen S, Qu G, Zhong C. Association of iron deficiency with chronic suppurative otitis media in adults. Acta Otolaryngol. 2024;144(1):19–22. doi:10.1080/00016489.2024.2310013
52. Kolarš B, Mijatović Jovin V, Živanović N, et al. Iron deficiency and iron deficiency anemia: a comprehensive overview of established and emerging concepts. Pharm Basel Switz. 2025;18(8):1104. doi:10.3390/ph18081104
53. Wang X, Lai C, Li R, et al. High HBsAg clearance rate and viral dynamics in HBeAg-positive, ALT-normal children and adolescents with chronic HBV infection: results from the prospective sprout project. Emerg Microbes Infect. 2025;14(1):2516173. doi:10.1080/22221751.2025.2516173
54. Netala VR, Hou T, Wang Y, Zhang Z, Teertam SK. Cardiovascular biomarkers: tools for precision diagnosis and prognosis. Int J Mol Sci. 2025;26(7):3218. doi:10.3390/ijms26073218
55. Ede LC, O’Brien J, Chonmaitree T, Han Y, Patel JA. Lactate dehydrogenase as a marker of nasopharyngeal inflammatory injury during viral upper respiratory infection: implications for acute otitis media. Pediatr Res. 2013;73(3):349–354. doi:10.1038/pr.2012.179
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of Ambroxol Combined with Loquat Syrup on Bacterial Pneumonia in Mice
Li C, Chen Z, Shi J, Zheng X
Journal of Inflammation Research 2024, 17:10107-10117
Published Date: 30 November 2024