Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Associations Between Gestational Diabetes Mellitus and Neonatal Acyl Metabolic Profiles: An Empirical Study Based on a Birth Cohort
Authors Yang Y, Peng Y, Guo F, Jia C, Yu B ![]()
Received 22 August 2025
Accepted for publication 28 December 2025
Published 28 January 2026 Volume 2026:19 561443
DOI https://doi.org/10.2147/DMSO.S561443
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Pablo Corral
Yuqi Yang,1,* Yue Peng,2,* Fang Guo,1 Chenbo Jia,1 Bin Yu1
1Department of Medical Genetics, Changzhou Maternal and Child Health Care Hospital, Changzhou Medical Center, Nanjing Medical University, Changzhou, Jiangsu, People’s Republic of China; 2Department of Obstetrics, Changzhou Maternal and Child Health Care Hospital, Changzhou Medical Center, Nanjing Medical University, Changzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Yu, Email [email protected]
Aim: This study aimed to identify gestational diabetes mellitus (GDM)-associated neonatal acylcarnitines (ACs), assess maternal glycemic control’s impact on these ACs, and evaluate maternal lipids’ mediating role, supporting early metabolic risk stratification in offspring.
Methods: Tandem mass spectrometry (TMS) measured AC levels in 4,974 newborns (836 GDMs,4,138 controls). Generalized linear models assessed GDM-neonatal AC associations. Non-parametric tests assessed differences among no-GDM (2769), well-controlled GDM (129), and suboptimally controlled GDM groups (425). Mediation analysis identified factors affecting neonatal ACs. Maternal clinical data were extracted from the electronic medical record (EMR) system.
Results: Of the 31 acylcarnitine species, 19 were significantly associated with GDM. Relative to the control group, 18 ACs exhibited significantly elevated levels, specifically malonylcarnitine+3-hydroxybutyrylcarnitine (C3DC+C4OH), isovalerylcarnitine+methylbutyrylcarnitine (C5), glutarylcarnitine+3-hydroxyhexanoylcarnitine (C5DC+C6OH), hexanoylcarnitine (C6), methylglutarylcarnitine (C6DC), decanoylcarnitine (C10), decenoylcarnitine (C10:1), dodecanoylcarnitine (C12), dodecenoylcarnitine (C12:1), tetradecanoylcarnitine (C14), tetradecenoylcarnitine (C14:1), palmitoylcarnitine (C16), palmitoleylcarnitine (C16:1), 3-hydroxypalmitoleylcarnitine (C16:1OH), 3-hydroxypalmitoylcarnitine (C16OH), stearoylcarnitine (C18), 3-hydroxyoleoylcarnitine (C18:1-OH),and 3-hydroxystearoylcarnitine (C18OH); only linoleoylcarnitine (C18:2) showed a significant decrease. In groups with progressively impaired glycemic control, triglyceride (TG) levels (P < 0.001) and propionylcarnitine (C3) levels (P = 0.02) exhibited a significant increasing trend, whereas high-density lipoprotein cholesterol (HDL-C) (P = 0.01) and C18:2 levels (P = 0.02) showed a consistent decreasing trend. Mediation analysis further demonstrated that maternal TG levels exerted a significant positive mediating effect on the elevation of neonatal C3 levels (10.7%, 95% CI: 0.0016, 0.0182, P = 0.006), whereas a significant masking effect was observed on C10:1 levels (− 14.27%, 95% CI: − 0.0006, − 0.0001, P < 0.001). Additionally, maternal HDL-C levels exhibited significant masking effects on most acylcarnitine indicators, with the only exception being a significant positive mediating effect on C18:2 levels (2.94%,95% CI: − 0.0018, − 0.0001, P = 0.0186).
Conclusion: GDM correlates with offspring AC levels, with TG and HDL-C partially mediating this relationship. Newborn fat oxidation metabolism is influenced by maternal factors from birth.
Keywords: gestational diabetes mellitus, fatty acid metabolism, acylcarnitine, β-oxidation
Introduction
GDM constitutes one of the prevalent metabolic complications during gestation. As the global obesity rate keeps escalating, the incidence of GDM demonstrates a year-on-year ascending trend.1 Additionally, GDM poses substantial immediate and long-term risks to the health of both mothers and infants. A considerable number of epidemiological studies have indicated that the risk of cardiovascular diseases and obesity among the offspring of GDM individuals is significantly higher than that in the general population.2 However, systematic investigations into the association between GDM and offspring diseases, as well as their underlying mechanisms, remain relatively limited in the current literature. Consequently, an in-depth exploration of the mechanism by which GDM affects the metabolic levels of the offspring holds significant scientific significance and clinical value.
ACs play a crucial role in human fatty acid oxidation metabolism and energy balance regulation and can serve as important biomarkers for complex metabolic syndromes.3,4 ACs levels have been linked to metabolic syndrome, obesity, and cardiovascular disease.5 For example, accumulating evidence supports a potential causal association between C18:2 and deep vein thrombosis (DVT),6 Plasma levels of short-chain acylcarnitines (SCAC) are positively associated with DPN risk.7 However, current evidence remains limited to clinical observational findings. Based on the theoretical framework of the Developmental Origins of Health and Disease (DOHaD), this study conducted a retrospective case-control study of acylcarnitine profiles in neonates born to mothers with GDM. The core objectives were to address two interrelated scientific questions: (1) whether GDM correlates with aberrant neonatal acylcarnitine profiles; and (2) whether maternal dyslipidemia mediates the association between GDM and alterations in neonatal acylcarnitine levels. By addressing these questions, this study not only uncovers potential links between maternal GDM and offspring fatty acid metabolic dysfunction but also provides critical scientific evidence to elucidate the mechanisms underlying the intergenerational transmission of maternal metabolic disorders.
Methods
Objects and Selection of Study Population
The present study recruited pregnant women who attended prenatal examinations at our hospital between November 2022 and June 2023. All participants underwent an oral glucose tolerance test (OGTT) during the second trimester of pregnancy. Based on the diagnostic criteria of the American Diabetes Association (ADA), they were stratified into a normal control group (n=4138) and a GDM group (n=865) (The inclusion criteria are presented in the supplementary materials). Among the GDM cohort, 836 participants ultimately underwent late-pregnancy glycemic profile screening. In accordance with the ADA guidelines, these participants were categorized into a well-controlled glycemia group (n=194) and suboptimally controlled glycemia group (n=642). Among them, 3,323 pregnant women underwent lipid level tests in the third trimester of pregnancy, and acylcarnitine levels of the newborns delivered by 4,974 pregnant women were tested three days after birth. (Figure 1). The study design and protocol were reviewed and approved by the ethics committee of Changzhou Maternity and Child Health care Hospital.
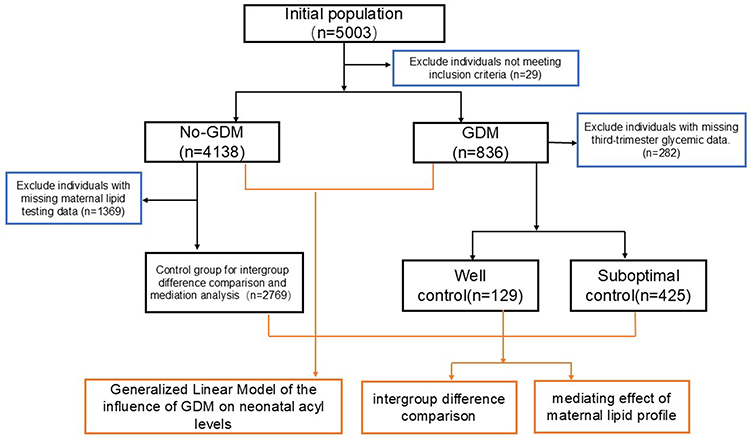 |
Figure 1 Study Design. |
Detection of Acylcarnitine
Three days after the birth of the newborn and after sufficient breastfeeding, heel blood samples were collected from the newborn for the detection of 31 acylcarnitines, including free carnitine (C0), acetylcarnitine (C2), C3, C3DC+C4OH, butyrylcarnitine+isobutyrylcarnitine (C4), methylmalonylcarnitine+ 3-hydroxyisovalerylcarnitine (C4DC+C5OH), isovalerylcarnitine+MetC5, tiglylcarnitine (C5:1), C5DC+C6OH, C6, C6DC, octanoylcarnitine (C8), octenoylcarnitine (C8:1), C10, C10:1, decadienoylcarnitine (C10:2), C12, C12:1, C14, C14:1, tetradecadienoylcarnitine (C14:2), 3-hydroxytetradecanoylcarnitine (C14OH), C16, C16:1, C16:1OH, C16OH, C18, oleoylcarnitine (C18:1), C18:1OH, C18:2, C18OH were evaluated by TMS detection methods as described in our previous study.8
Determination of Serum Lipids
Serum lipid levels were examined using Wet Chemistry via an automated analyzer (AU5800, Beckman Coulter Inc, USA). The normal reference ranges of serum lipid indices for the local population are as follows: total cholesterol (TC) ≤ 5.17 mmol/L, TG ≤ 1.6 mmol/L, HDL-C: 1.03–1.55 mmol/L, low-density lipoprotein cholesterol (LDL-C) ≤ 3.36 mmol/L, apolipoprotein A (ApoA): 1.0–1.6 g/L, apolipoprotein B (ApoB):0.6–1.1 g/L, lipoprotein (a) (Lpa) ≤ 300 mg/L, and free fatty acids (FFAs): 0.1–0.77 mmol/L.
Statistical Analysis
Qualitative data were analyzed with the chi-square test, while quantitative data were assessed using the Student’s t-test for normally distributed data and the Mann–Whitney U-test for non-normally distributed data. GDM was treated as the exposure factor for analysis, and a generalized linear model was employed to evaluate its association with neonatal acylcarnitine levels. Concurrently, maternal age at delivery, gestational age (GA), and pre-pregnancy body mass index (BMI) were incorporated as covariates in the model to adjust for potential confounding effects. We conducted mediation analyses using the Process SPSS macro (Process 4.1 for SPSS) to explore the relationships between variables. Specifically, we applied Macro Model 4,9 a widely used analytical framework designed to test simple mediation effects of a single mediator (TG or HDL-C). Statistical significance was set at a two-tailed p-value of 0.05. The Benjamini-Hochberg (BH) procedure computes adjusted significance levels by sorting p-values in ascending order. The Jonckheere-Terpstra (J-T) test is employed to assess whether relevant indicators exhibit a consistent upward or downward trend across categories of blood glucose control status. The statistical analysis software employed was IBM SPSS Statistics Version 20.
Results
Characteristics of the Study Population
This study included a total of 5003 pregnant women, with 4,138 serving as normal controls and 865 in the GDM group. In the GDM group, 194 patients had their blood glucose levels effectively controlled, while 642 patients had poor control, according to the ADA (fasting blood glucose<5.3mmol/L and 2-hour postprandial blood glucose<6.7mmol/L). Third-trimester blood glucose data were missing for 29 GDM patients. Significant differences were observed between the two groups of pregnant women in aspects such as weight at admission, weight gain during pregnancy, pre-pregnancy weight, age, gestational weeks, and mode of delivery (P < 0.05). Although no significant difference in the neonatal weight was found between the two groups (P=0.391), it was conspicuously observed that the proportion of large-for-gestational-age infants in the GDM group (In reference to the standards of the Chinese population10) significantly rose (15.954% VS 11.382%) after re-grouping in combination with gestational age factors and according to specific gestational age curves (P < 0.001). In addition, significant differences were observed across fetal weight subgroups (P = 0.031); the incidence of macrosomia in the GDM group was higher than that in the normal control group, and this difference became more pronounced after adjusting for gestational age (Table 1).
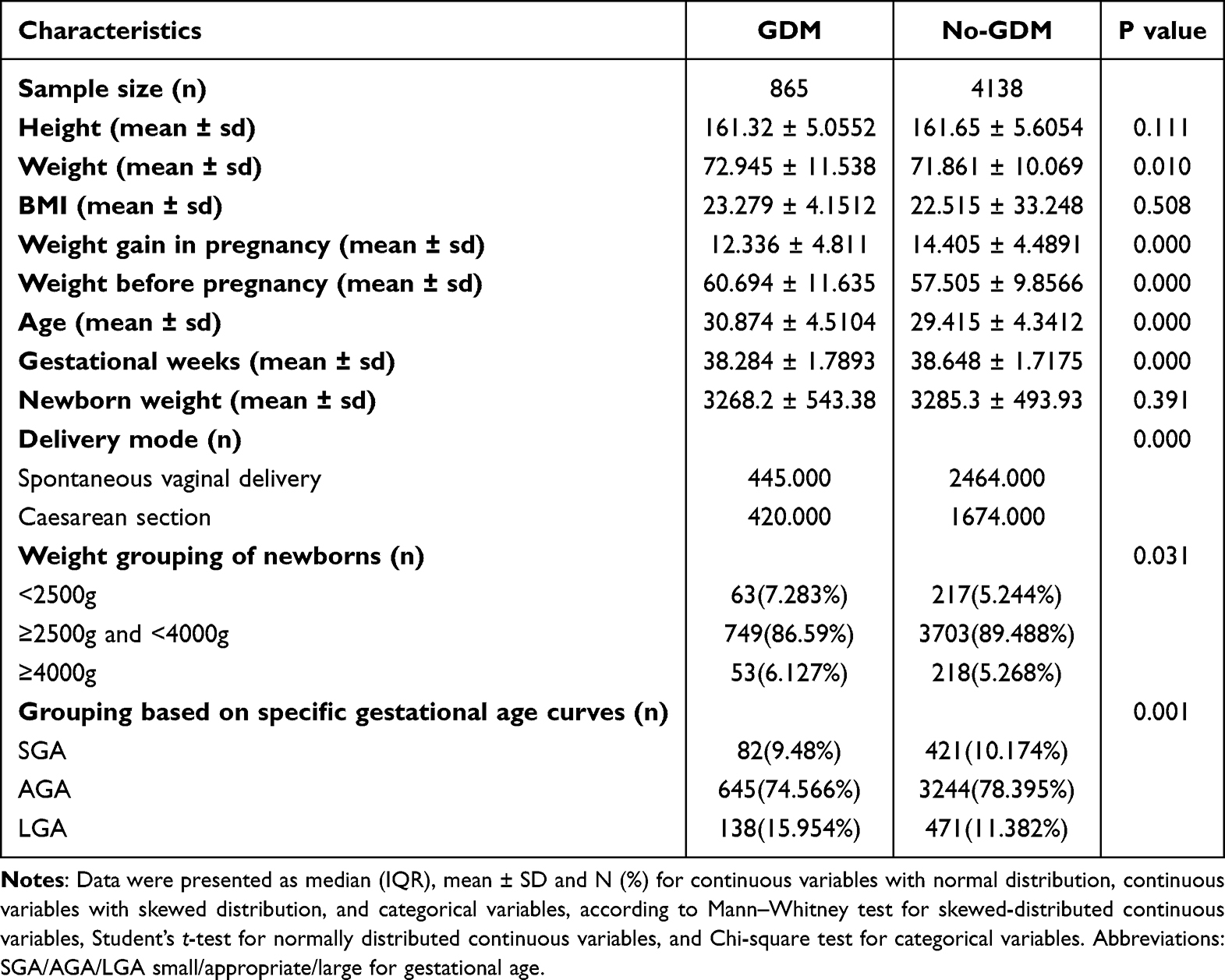 |
Table 1 Clinical Baseline of the Recruitment Cohort |
Association of GDM with Neonatal Acylcarnitine Profiles
The analysis results of the generalized linear model revealed that the differences of C3DC+C4OH (P=0.003), C5(P=0.028), C5DC + C6OH(P=0.003), C6(P=0.014), C6DC(P=0.003), C10(P=0.009), C10:1(P=0.003), C12(P=0.003), C12:1(P=0.003), C14(P=0.003). C14:1(P=0.009), C16(P=0.003), C16:1(P=0.003), C16:1OH(P=0.003), C16:OH(P=0.003), C18(P=0.02),C18:1(P=0.017), C18:2(P=0.003) and C18:OH(P=0.044) were statistically significant. Compared with the normal control group, all the aforementioned differential indices were significantly elevated, except for C18:2 (Table 2).
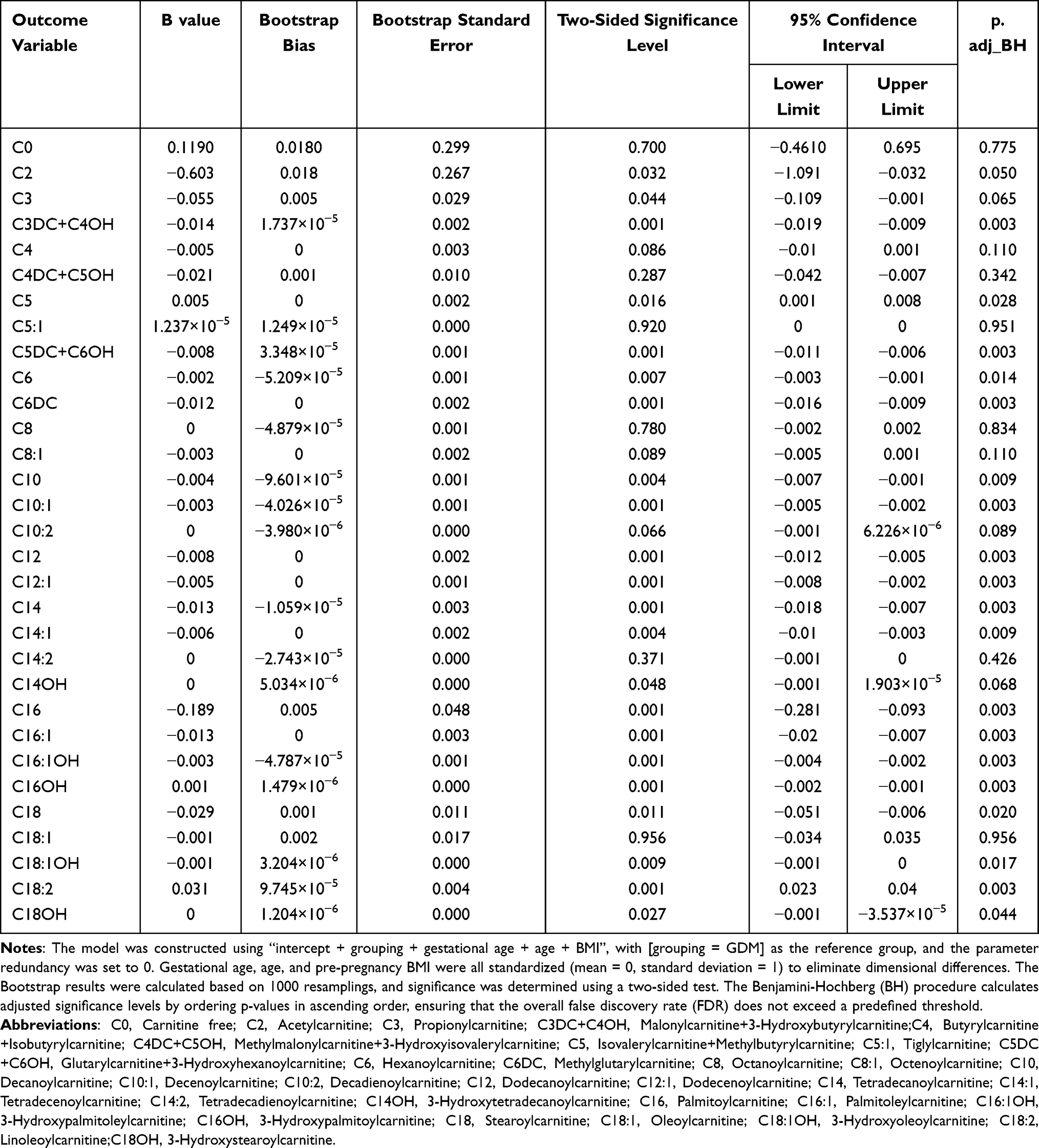 |
Table 2 Generalized Linear Model of the Influence of GDM on Neonatal Acyl Levels |
The results demonstrated a highly significant statistical difference in neonatal C18:2 levels across the three groups (p.adj (BH) < 0.001). Further validation via Jonckheere-Terpstra test revealed a significant linear decrease in C18:2 levels with worsening glycemic control in GDM patients (p (J-T) = 0.02), with the lowest levels observed in the poor glycemic control group and the highest in the normal control group, indicating a clear intergroup trend effect. For C3 levels, intergroup differences did not reach statistical significance following B-H correction (p.adj (BH) = 0.06); however, Jonckheere-Terpstra test showed a significant increase in C3 levels with worsening glycemic control (p (J-T) = 0.02), suggesting a potential trend association that warrants further validation with an expanded sample size. Additionally, while indicators including C4DC+C5OH, C5DC+C6OH, C6, C6DC, C12, C12:1, C14, C14:1, C14OH, C16:1, C16:1OH, and C16OH exhibited intergroup differences and non-monotonic trends, they lacked a consistent directional pattern of increase or decrease. This inconsistency may be attributed to random within-group variability or the masking effect of confounding factors.
In addition, maternal TG, HDL-C, and FFAs levels differed significantly among the three groups (P < 0.05). TG was highest in the suboptimal glycemic control group, while HDL-C and FFAs were lowest in this group. No significant differences were found in maternal TC, LDL-C, APO-A, APO-B, or Lpa levels across groups (P > 0.05) (Table 3).
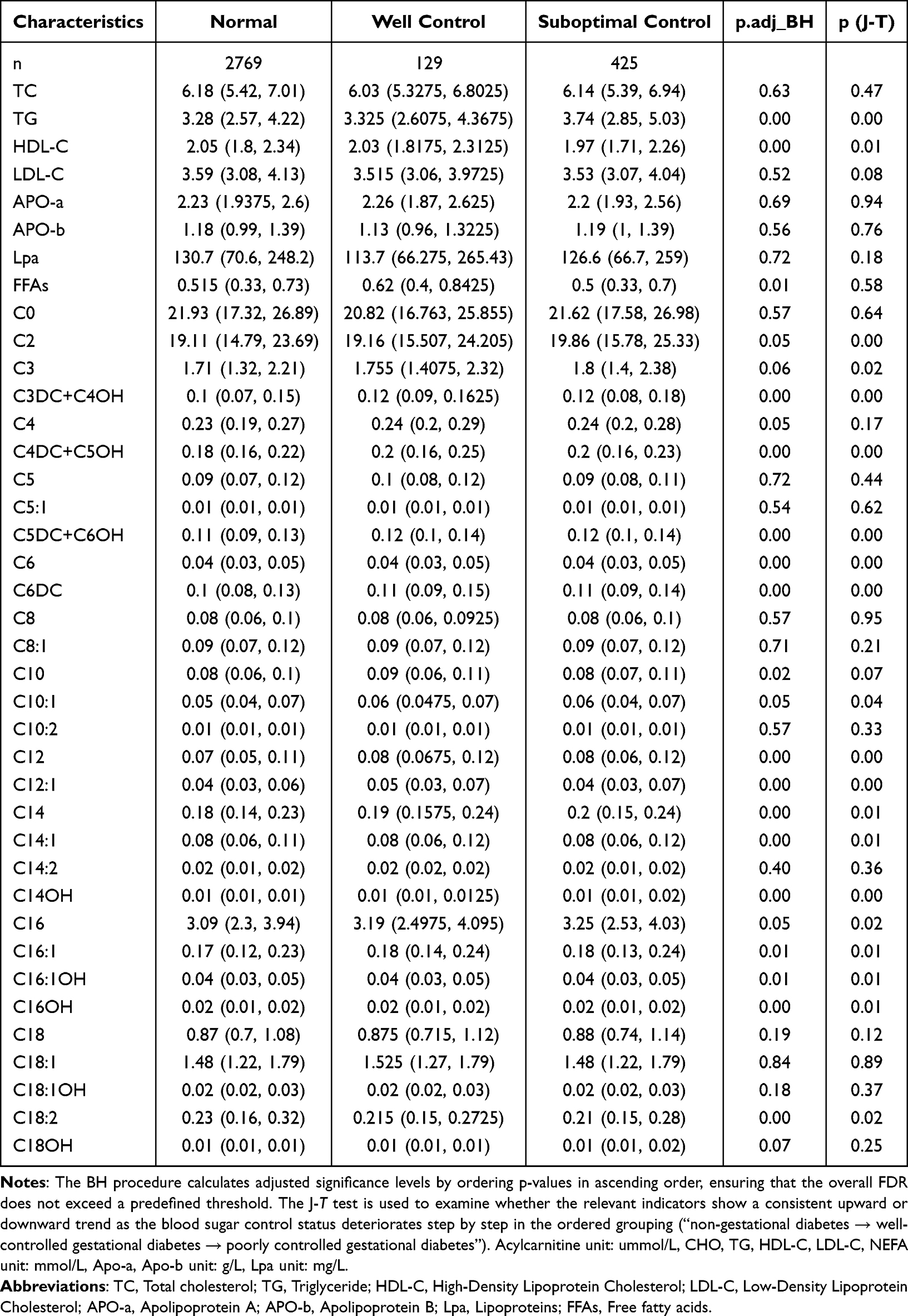 |
Table 3 Comparative Analysis of the Intergroup Differences |
Mediation Analyses
A model with TG as the mediating variable
Specifically, the total effect of C3 exhibited a significant positive association (effect size = 0.0840, 95% CI: 0.0112, 0.1568, P = 0.024), with both its direct effect (0.0750, 95% CI: 0.0066, 0.1434, P = 0.0317) and TG-mediated indirect effect (0.0090, 95% CI: 0.0016, 0.0182, P = 0.006) reaching statistical significance. The mediating proportion of TG in this association was 10.7%, indicating that TG served as a partial mediator in the relationship between GDM and C3. For C10:1, the total effect was also significant (0.0021, 95% CI: 0.0001, 0.0041, P = 0.036), and the direct effect showed a significant positive association (0.0024, 95% CI: 0.0005, 0.0043, P = 0.012). However, the TG-mediated indirect effect was significantly negative (−0.0003, SE = 0.0001, 95% CI: −0.0006, −0.0001, P < 0.001), with a mediating proportion of −14.27%, suggesting the presence of a suppression effect of TG in the GDM-C10:1 association. Regarding C14:2, neither the total effect nor the direct effect was statistically significant, whereas the TG-mediated indirect effect was significantly negative (−0.0001, 95% CI:-0.0002, 0.0000, P = 0.007), with a mediating proportion of −33.0%. These findings imply that the influence of GDM on C14:2 may be primarily exerted via the TG pathway, though further validation is warranted.
A model with HDL-C as the mediating variable
In the model with HDL-C as the mediator, the mediating effects of distinct acylcarnitine species fell into two categories. The first category comprised species with significant total effects. For instance, C2 exhibited a significant positive total effect (0.8254, 95% CI: 0.1872, 1.4636, P = 0.0113), with its direct effect also being significantly positive (0.8800, 95% CI: 0.2354, 1.5245, P = 0.0075). However, the HDL-C-mediated indirect effect was significantly negative (−0.0613, 95% CI:-0.1153, −0.0114, P = 0.0037), yielding a mediation proportion of −6.62%, indicative of a suppression effect of HDL-C in this association. Species including C6, C6DC, C12:1, C14, C14:1, C16, and C16:1OH shared a consistent pattern: both total and direct effects were significant, with the indirect effect being significantly negative and mediation proportions ranging from −4.17% to −9.09%, all consistent with the characteristics of a suppression effect. C18:2 exerts a predominant direct negative effect (−0.0272,0.0060,95% CI:-0.0389, −0.0155, P <0.001) on the outcome, while also inducing a statistically significant but relatively minor indirect negative effect (−0.0008,-0,0004,95% CI:-0.0018, −0.0001, P =0.0186) mediated by HDL-C. The second category included species with non-significant total effects (C8:1, C18, and C14:2), where neither total nor direct effects reached statistical significance, but the HDL-C-mediated indirect effect was significantly negative. These findings suggest that the influence of GDM on these Acs is primarily exerted via the negative HDL-C pathway, yet the absence of a significant total effect indicates that HDL-C may act as an independent mediator rather than a component of the overall association (Table 4).
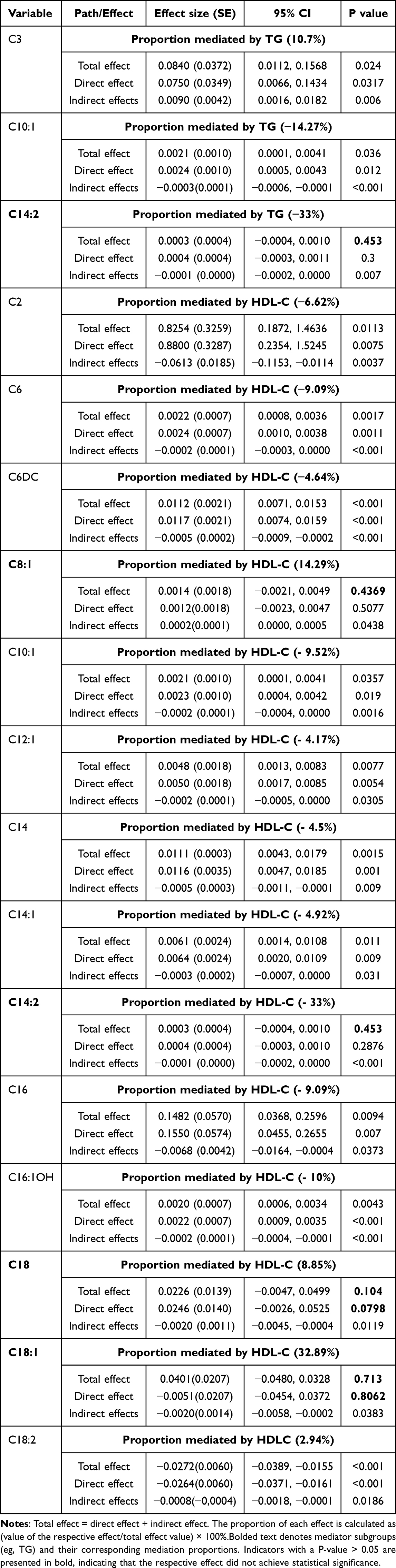 |
Table 4 Mediated Effects by TG and HDL-C on the Associations of Acylcarnitine Levels with GDM |
Discussion
GDM refers to the diabetes that is diagnosed for the first time during pregnancy. Its pathogenesis is rather complex, involving genetic factors, environmental influences, and lifestyle, among other aspects. In recent years, GDM has risen due to obesity, advanced age, and excessive pregnancy weight gain and this trend is expected to continue.11,12 GDM can lead to various adverse outcomes. For example, maternal complications include preeclampsia, gestational hypertension, postpartum hemorrhage, and lactation issues. From a long-term perspective, the probability of GDM patients evolving into type 2 diabetes in the later period is approximately ten times higher than that of the normal population.13 Additionally, the blood glucose level of the mother during pregnancy may have an impact on the long-term glucose tolerance and pancreatic islet cell sensitivity of the offspring, thereby increasing the risk of obesity and impaired metabolic function in the offspring.14 However, the relevant mechanisms by how GDM influences the metabolism of the offspring remain largely undefined. Many related mechanisms are still hypothetical and require further verification through scientific evidence. Clinically, robust systematic evidence in metabolomics is urgently needed to define the long-term effects of GDM on offspring and to uncover its underlying mechanistic pathways.
Acylcarnitine (AC), as an important metabolic intermediate product, plays a crucial role in energy metabolism and fatty acid oxidation. It is a conjugate of fatty acids and carnitine, promoting the entry of fatty acids into mitochondria to complete the β-oxidation process15 (Figure 2). As the research on metabolic regulatory mechanisms proceeds in depth, the biological functions of ACs have gradually come into focus, particularly their potential roles in metabolic disorders such as diabetes, obesity and cardiovascular diseases13,16 Currently, mass spectrometry serves as the gold standard for the detection of ACs. In this study, this technique was employed to quantify AC levels in neonates born to mothers with GDM. A total of 19 ACs are associated with GDM, among which 18 exhibit a positive correlation and one demonstrates a negative correlation. The 19 ACs with significant differences between the two groups cover three categories: short-chain, medium-chain, and long-chain. Medium- and long-chain acylcarnitines have been reported to be associated with insulin resistance and mitochondrial dysfunction.17,18 SCACs are metabolites formed by the conjugation of acyl groups containing 2–6 carbon atoms with carnitine, which play crucial roles in energy metabolism, metabolic regulation, and disease screening. For instance, Luo et al19 reported that elevated levels of maternal SCACs are associated with an increased risk of GDM.
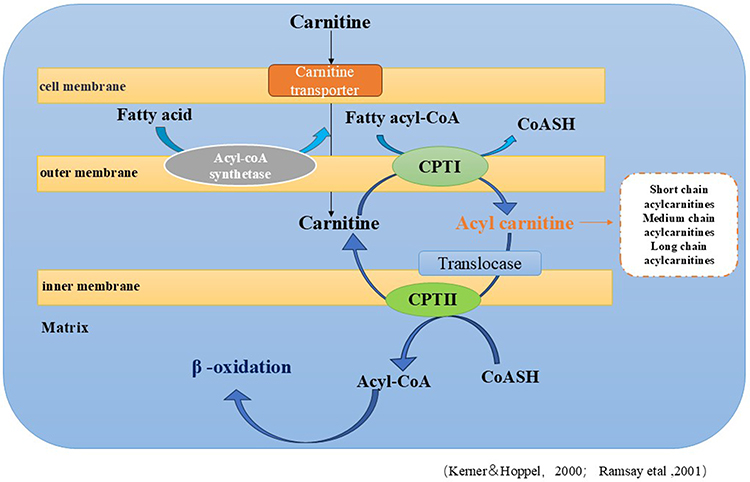 |
Figure 2 Working Mechanism of Acylcarnitine. |
In this study, the level of C18:2 (a conjugate of linoleic acid and carnitine) in neonates was significantly reduced in the GDM group and was correlated to some extent with the blood glucose control status. Previous research indicates that an elevation in C18:2 levels contributes to improving energy metabolism.20 Based on the findings of our study, it is hypothesized that GDM affects the energy metabolism of neonates, and this impact may be adverse. Yong-Hwa Lee et al5 have evidenced that the C3 levels in middle-aged and elderly individuals exhibit a positive correlation with the components related to metabolic syndrome, insulin resistance, and cardiovascular risk factors. After BH correction in this study, the statistical difference in C3 levels was marginally significant; however, the J-T test revealed that neonatal C3 levels exhibited a significant upward trend with increasing severity of maternal glycemic abnormality. As the sample size increases, the statistical significance of this difference may be further strengthened. We also found that offspring of mothers with GDM had significantly higher C3 levels than those in the normal population during the early postnatal period, with the difference increasing under suboptimal maternal glycemic control. This finding is in accordance with the phenomenon that the offspring of GDM patients are more susceptible to metabolic syndrome, cardiovascular diseases, and an increased risk of obesity.21–23 C6DC has been reported as a potential biomarker for the prediction of cardiovascular diseases among the diabetic population,24 while C16:1OH has been reported as a predictor for diabetic cardiomyopathy.25 All the aforementioned indicators demonstrated significant differences in the present study. The findings of this study indicate that these predictive indicators have already exhibited differential characteristics during the neonatal period.
A multitude of studies have indicated that lipid metabolism assumes a crucial role in the genesis and progression of GDM.26–28 There exist significant disparities in lipid metabolism levels in the serum of GDM patients compared with the normal population. Particularly, TG level and HDL-C level might serve as a predictive target for GDM.27,29,30 Through mediation analysis, we discovered that 10.7% of the influence of GDM on the C3 level of neonates was mediated by the TG level. HDL-C mediates the effect of GDM on the levels of multiple ACs (including C2, C6, and C14 and so on) in neonates, with a predominant masking effect. These suggest that the true direct association between GDM and ACs may be stronger than that indicated by the total effect. The findings from the mediation analysis confirm that lipid metabolism plays a critical role in the onset and progression of GDM, suggesting that lipid profile testing may be integrated into the clinical management of GDM. Nevertheless, its widespread implementation requires validation and support from additional high-quality prospective studies.
Limitations
This study has several limitations. First, as a single-center study, its findings may lack generalizability. Second, while the results suggest that GDM affects neonatal acylcarnitine levels early on, the absence of long-term growth data limits conclusions about the persistence of this effect. Finally, some neonatal data were sourced from the neonatal disease screening database, which has limited capacity to reflect overall neonatal metabolic status. Furthermore, the missing maternal lipid data compromised the completeness and comprehensiveness of the baseline lipid profile characterization for the entire cohort. It also hindered the full elucidation of maternal lipid profile distribution differences across distinct glycemic control states, which may further interfere with the assessment of intergroup baseline characteristic balance and the accurate interpretation of lipid-related mediating effects. Future studies should accumulate additional data to further validate these findings.
Conclusion
This study measured acylcarnitine levels, identifying distinct early metabolic profiles in offspring of mothers with GDM compared to those from the general population. Moreover, our findings indicate that the impact of GDM on offspring begins in the neonatal period, potentially providing a new direction for early screening of metabolic syndrome, cardiovascular diseases, and diabetes.
Furthermore, our mediation analysis uncovered a critical mechanistic insight: maternal lipid parameters play dual roles in the association between GDM and neonatal AC levels. These findings highlight that neonatal fat oxidation metabolism is intricately programmed by maternal GDM and lipid status from birth, revealing the intergenerational transmission pathway of metabolic risk.
Data Sharing Statement
The datasets used and analysed in this study are available upon contact with the corresponding author.
Ethics Approval and Consent to Participate
This study followed the principles of the Declaration of Helsinki. The study design and protocol were approved by the ethics committee of Changzhou Maternity and Child Health Care Hospital (Approval No.: 2022015). Neonatal acylcarnitine data were obtained from the neonatal disease screening database. Ethical approval for the study was also obtained from the same committee (Approval No.: 201608). All participants with gestational diabetes mellitus provided informed consent. Guardians of the neonates were informed prior to screening that the data would be used for future research and signed the relevant consent forms.
Acknowledgments
We thank all of the project participants for their contributions.
Author Contributions
Yuqi Yang: Conceptualization, Writing–Original Draft, Funding Acquisition.
Yue Peng: Data Curation, Investigation, Formal Analysis, Writing–Review & Editing.
Fang Guo: Investigation, Formal Analysis, Writing–Review & Editing.
Chenbo Jia: Investigation, Formal Analysis, Writing–Review & Editing.
Bin Yu: Conceptualization, Writing–Review & Editing, Supervision.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by a project supported by ChangZhou high-level healthcare professionals (2024CZBJ023), Major science and technology project of Changzhou Health Commission (ZD202326).
Disclosure
All authors have no conflicts of interest to disclose. This study was not supported by any industry, grant, or organization that could pose a potential conflict. No author has any financial, professional, or personal relationships that might inappropriately influence the presented results.
References
1. Zehravi M, Maqbool M, Ara I. Correlation between obesity, gestational diabetes mellitus, and pregnancy outcomes: an overview. Int J Adolescent Med Health. 2021;33(6):339–13. doi:10.1515/ijamh-2021-0058
2. Bianco ME, Josefson JL. Hyperglycemia during pregnancy and long-term offspring outcomes. Curr Diab Rep. 2019;19(12):143. doi:10.1007/s11892-019-1267-6
3. Li S, Gao D, Function JY. Detection and alteration of acylcarnitine metabolism in hepatocellular carcinoma. Metabolites. 2019;9(2):36. doi:10.3390/metabo9020036
4. Houten SM, Wanders RJA, Ranea-Robles P. Metabolic interactions between peroxisomes and mitochondria with a special focus on acylcarnitine metabolism. Biochim Biophys Acta Mol Basis Dis. 2020;1866(5):165720. doi:10.1016/j.bbadis.2020.165720
5. Lee YH, Park S. Genetic and lifestyle-related factors influencing serum hyper-propionylcarnitine concentrations and their association with metabolic syndrome and cardiovascular disease risk. Int J Mol Sci. 2023;24(21).
6. Liu Z, Ma H, Zhang L, et al. Exploring metabolite-mediated links between lipidome and deep vein thrombosis: insights from Mendelian randomization analysis. Medicine. 2025;104(10):e41783. doi:10.1097/MD.0000000000041783
7. An Z, Zheng D, Wei D, et al. Correlation between acylcarnitine and peripheral neuropathy in type 2 diabetes mellitus. J Diabet Res. 2022;2022(8115173):1–9. doi:10.1155/2022/8115173
8. Yang Y, Wang L, Wang B, et al. Application of next-generation sequencing following tandem mass spectrometry to expand newborn screening for inborn errors of metabolism: a multicenter study. Front Genetics. 2019;10(86).
9. Hayes AF, Rockwood NJ. Regression-based statistical mediation and moderation analysis in clinical research: observations, recommendations, and implementation. Behav Res Therap. 2017;98:39–57. doi:10.1016/j.brat.2016.11.001
10. Yuan X, Hu H, Zhang M, et al. Iron deficiency in late pregnancy and its associations with birth outcomes in Chinese pregnant women: a retrospective cohort study. Nutr Metab. 2019;16(30). doi:10.1186/s12986-019-0360-9
11. Najafi F, Hasani J, Izadi N, et al. The effect of prepregnancy body mass index on the risk of gestational diabetes mellitus: a systematic review and dose-response meta-analysis. Obesity Rev. 2019;20(3):472–486. doi:10.1111/obr.12803
12. Garmendia ML, Mondschein S, Montiel B, et al. Trends and predictors of gestational diabetes mellitus in Chile. Int J Obstetrics Gynaecology. 2020;148(2):210–218. doi:10.1002/ijgo.13023
13. Vounzoulaki E, Khunti K, Abner SC, et al. Progression to type 2 diabetes in women with a known history of gestational diabetes: systematic review and meta-analysis. BMJ. 2020;369. doi:10.1136/bmj.m1361
14. Lowe WL, Lowe LP, Kuang A, et al. Maternal glucose levels during pregnancy and childhood adiposity in the hyperglycemia and adverse pregnancy outcome follow-up study. Diabetologia. 2019;62(4):598–610. doi:10.1007/s00125-018-4809-6
15. Kerner J, Hoppel C. Fatty acid import into mitochondria. BBA. 2000;1486(1):1–17. doi:10.1016/S1388-1981(00)00044-5
16. Xu ZR, Zhu XY, Lu W, et al. Altered serum amino acid and acylcarnitine profiles in hyperinsulinemic hypoglycemia and ketotic hypoglycemia. Front Endocrinol. 2020;11(577373). doi:10.3389/fendo.2020.577373
17. Batchuluun B, Al Rijjal D, Prentice KJ, et al. Elevated medium-chain acylcarnitines are associated with gestational diabetes mellitus and early progression to type 2 diabetes and induce pancreatic β-cell dysfunction. Diabetes. 2018;67(5):885–897. doi:10.2337/db17-1150
18. Panov AV, Mayorov VI, Dikalova AE, et al. Long-Chain and medium-chain fatty acids in energy metabolism of murine kidney mitochondria. Int J Mol Sci. 2022;24(1). doi:10.3390/ijms24010379
19. Luo H, Zhu Z. Serum acylcarnitines levels as a potential predictor for gestational diabetes: a systematic review and meta-analysis. Front Public Health. 2023;11(1217237). doi:10.3389/fpubh.2023.1217237
20. Sánchez MC, Herráiz A, Ciudad MJ, et al. Metabolomics and biochemical benefits of multivitamin and multimineral supplementation in healthy individuals: a pilot study. Foods. 2024;13(14):2207. doi:10.3390/foods13142207
21. Hammoud NM, Visser GHA, Van Rossem L, et al. Long-term BMI and growth profiles in offspring of women with gestational diabetes. Diabetologia. 2018;61(5):1037–1045. doi:10.1007/s00125-018-4584-4
22. Gomes D, Von Kries R, Delius M, et al. Late-pregnancy dysglycemia in obese pregnancies after negative testing for gestational diabetes and risk of future childhood overweight: an interim analysis from a longitudinal mother-child cohort study. PLoS Med. 2018;15(10):e1002681. doi:10.1371/journal.pmed.1002681
23. Tam WH, Ma RCW, Ozaki R, et al. In utero exposure to maternal hyperglycemia increases childhood cardiometabolic risk in offspring. Diabetes Care. 2017;40(5):679–686. doi:10.2337/dc16-2397
24. Shen M, Xie Q, Zhang R, et al. Metabolite-assisted models improve risk prediction of coronary heart disease in patients with diabetes. Front Pharmacol. 2023;14(1175021). doi:10.3389/fphar.2023.1175021
25. Zheng DM, An ZN, Ge MH, et al. Medium & long-chain acylcarnitine’s relation to lipid metabolism as potential predictors for diabetic cardiomyopathy: a metabolomic study. Lipids Health Dis. 2021;20(1):151. doi:10.1186/s12944-021-01576-9
26. Wu P, Wang Y, Ye Y, et al. Liver biomarkers, lipid metabolites, and risk of gestational diabetes mellitus in a prospective study among Chinese pregnant women. BMC Med. 2023;21(1):150. doi:10.1186/s12916-023-02818-6
27. Dong Y, Hu AQ, Han BX, et al. Mendelian randomization analysis reveals causal effects of blood lipidome on gestational diabetes mellitus. Cardiovascul Diabetol. 2024;23(1):335. doi:10.1186/s12933-024-02429-2
28. Zhang Z, Zhou Z, Li H. The role of lipid dysregulation in gestational diabetes mellitus: early prediction and postpartum prognosis. J Diabetes Invest. 2024;15(1):15–25. doi:10.1111/jdi.14119
29. Ma N, Bai L, Lu Q. First-Trimester triglyceride-glucose index and triglyceride/high-density lipoprotein cholesterol are predictors of gestational diabetes mellitus among the four surrogate biomarkers of insulin resistance. Diabetes Metabol Syndr Obesity. 2024;17:1575–1583. doi:10.2147/DMSO.S454826
30. You Y, Hu H, Cao C, et al. Association between the triglyceride to high-density lipoprotein cholesterol ratio and the risk of gestational diabetes mellitus: a second analysis based on data from a prospective cohort study. Front Endocrinol. 2023;14(1153072). doi:10.3389/fendo.2023.1153072
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.