")
Back to Journals » Clinical Interventions in Aging » Volume 18
Associations Between Dysphagia and Adverse Health Outcomes in Older Adults with Dementia in Intensive Care Units: A Retrospective Cohort Study
Authors Cheng H , Deng X, Li J, Tang Y, Yuan S , Huang X , Wang Z , Zhou F, Lyu J
Received 23 February 2023
Accepted for publication 17 June 2023
Published 3 August 2023 Volume 2023:18 Pages 1233—1248
DOI https://doi.org/10.2147/CIA.S409828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Nandu Goswami
Hongtao Cheng,1,2,* Xingwen Deng,3,* Jieyao Li,4,* Yonglan Tang,1,2 Shiqi Yuan,5 Xiaxuan Huang,5 Zichen Wang,1 Fuling Zhou,6 Jun Lyu1,7
1Department of Clinical Research, The First Affiliated Hospital of Jinan University, Guangzhou, People’s Republic of China; 2School of Nursing, Jinan University, Guangzhou, People’s Republic of China; 3Department of Medical Information, The First Affiliated Hospital of Jinan University, Guangzhou, People’s Republic of China; 4Department of Intensive Care Unit, The First Affiliated Hospital of Jinan University, Guangzhou, People’s Republic of China; 5Department of Neurology, The First Affiliated Hospital of Jinan University, Guangzhou, People’s Republic of China; 6Department of Hematology, Zhongnan Hospital of Wuhan University, Wuhan, People’s Republic of China; 7Guangdong Provincial Key Laboratory of Traditional Chinese Medicine Informatization, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jun Lyu, Department of Clinical Research, The First Affiliated Hospital of Jinan University, Guangzhou, 510630, People’s Republic of China, Email [email protected] Fuling Zhou, Department of Hematology, Zhongnan Hospital of Wuhan University, No. 169 Donghu Road, Wuhan, 430071, People’s Republic of China, Email [email protected]
Background: Dysphagia is common in elderly patients with dementia and is one of the common clinical geriatric syndromes. It imposes a heavy burden on patients and their caregivers and is becoming an important public health problem. This study examined the association between dysphagia in older dementia patients in the ICU and the subsequent adverse health outcomes they experience.
Patients and Methods: A retrospective analysis of adults (≥ 65 years) with dementia in ICUs of a Boston tertiary academic medical center was conducted. Using the International Classification of Diseases’ Ninth and Tenth Revisions, dementia patients were identified. The study cohort comprised 1009 patients, median age 84.82 years, 56.6% female, predominantly White (72.9%). Patients were grouped based on swallowing function: dysphagia (n=282) and no-dysphagia (n=727). Dysphagia was identified via positive bedside swallowing screening. Primary outcomes were 90- and 180-day mortality, secondary outcomes included aspiration pneumonia, pressure injury, and delirium. Cohort characteristics were compared using the Wilcoxon rank-sum and chi-square tests. Dysphagia and outcomes correlations were examined via Kaplan-Meier survival analysis, Cox proportional-hazards regression models, logistic regression models, and subgroup analysis.
Results: After adjusting for covariates, the results from multivariate Cox proportional-hazards regression indicated that dysphagia was significantly associated with increased 90-day (HR=1.36, 95% CI=1.07– 1.73, E-value=1.78) and 180-day (HR=1.47, 95% CI=1.18– 1.82, E-value=1.94) mortality; the multifactorial logistic regression results indicated that dysphagia was associated with significant increases in pressure injury (OR=1.58, 95% CI=1.11– 2.23, E-value=1.83) and aspiration pneumonia occurrence (OR=4.04, 95% CI=2.72– 6.01, E-value=7.54), but was not significantly associated with delirium prevalence (OR=1.27, 95% CI=0.93– 1.74).
Conclusion: Dysphagia is likely to increase the risk of adverse health outcomes in older adults with dementia in ICU, and these adverse outcomes mostly include 90- and 180-day mortality, aspiration pneumonia, and pressure injury.
Keywords: dysphagia, dementia, older adults, mortality, intensive care unit, delirium
Introduction
Dementia, often manifesting in late adulthood, is characterized by progressive and irreversible cognitive dysfunction and behavioral impairment, typically resulting from degenerative lesions of the central nervous system.1–4 Alzheimer’s disease (AD), the most prevalent form of dementia, afflicted an estimated 6.5 million Americans aged 65 or older in 2022, a number projected to rise to 13.8 million by 2060 without significant advances in prevention and treatment.5–7 AD remains the fifth-most-common cause of death among Americans aged 65 years or older, with uncompensated dementia care reportedly costing US$ 271.6 billion in 2021.7,8
In older adults with dementia, dysphagia, particularly oropharyngeal dysphagia, is a common and detrimental complication.9 This disorder hinders the normal progression of food or liquid from the mouth into the esophagus, characterized by strained and time-consuming swallowing, and food and fluid accumulation in the mouth.10–12 The risks of dysphagia include malnutrition, aspiration, dehydration, weight loss, increased healthcare costs, and death.13 Estimates of dysphagia prevalence vary widely among older patients due to differences in assessment methods and healthcare settings; the average prevalence is approximately 15% among community-dwelling older adults,14 and approximately 47.4% among patients admitted to acute geriatric care.15 The prevalence among patients with dementia varies depending on their stage, and may be 80% or even higher in patients with eating problems in the late stages.16,17 Despite the high prevalence, dysphagia may be underreported clinically.18 Adding to the complexity, dementia, a significant public health issue, imposes substantial disease and economic burdens, which are amplified when compounded with dysphagia.19,20 This interplay warrants early preventive care strategies to alleviate these dual health and economic impacts.
With the global aging population on the rise, there is a corresponding increase in the number of individuals affected by both dementia and dysphagia. However, little attention has been given to the specific subset of these patients who necessitate intensive care unit (ICU) treatment. This study aims to address this knowledge gap, focusing on this unique population due to their heightened vulnerability. These individuals face an elevated risk of complications due to a combination of factors, including advanced age, cognitive impairment stemming from dementia, and the presence of severe physical health conditions requiring ICU intervention.21 Considering the established link between intubation, a common ICU procedure, and exacerbated dysphagia, our focus primarily lies on dysphagia that was present prior to ICU admission or intubation.22 By exploring the impact of dysphagia on this high-risk group, our objective is to enhance ICU management practices and mitigate the risk of adverse health outcomes.
The primary aim of this study was to determine the associations between older patients with dementia in the ICU and specific adverse health outcomes, particularly focusing on dysphagia and complications related to dysphagia, aiming to provide insight that could guide preventive and interventional strategies. Based on previous studies4,23 and neurologist experiences, we proposed an underlying hypothesis that the incidence rates of adverse health outcomes (death, aspiration pneumonia, pressure injury, and delirium) are higher in older patients with dementia and dysphagia than in those patients without dysphagia.
Methods
Data Source
The information and data used in this study were from the Medical Information Mart for Intensive Care IV (MIMIC-IV) version 2.0. MIMIC-IV is a large, free, publicly available critical-care database that includes electronic health records (EHRs) from the internationally renowned Beth Israel Deaconess Medical Center in Boston, Massachusetts, USA.24 The MIMIC-IV database covers tens of thousands of patients admitted to the ICU from 2008 to 2019. The database includes comprehensive medical and nursing information, which are recorded periodically from the MetaVision bedside monitoring system.25 One of our authors (Hongtao Cheng) received a certificate to access the database after completing the training (record ID: 45369280).
Study Setting, Design, and Population
This was a retrospective cohort study involving patients from a tertiary academic medical center in Boston, Massachusetts, USA (one of the teaching hospitals affiliated with Harvard Medical School). Under the Health Insurance Portability and Accountability Act,26 once suitable patients in the MIMIC-IV had been identified, sensitive information was removed and their true years of admission were concealed, and so informed consent did not need to be obtained from the patients.27 The study was approved by the Ethics Committee and Institutional Review Board of the First Affiliated Hospital of Jinan University, and it followed the regulations of the Declaration of Helsinki.
The inclusion criteria for the patients in this cohort study were as follows: (1) dementia diagnosis, (2) first hospitalization and ICU admission, and (3) assessed and documented patients with swallowing function (“itemid” =225118). The term “first hospitalization” refers to the patient’s initial stay in the hospital, while “ICU admission” refers to the patient’s first admission to the Intensive Care Unit during that initial hospitalization. This selection was made to minimize potential confounding factors, such as the effects of multiple hospitalizations or ICU admissions on the outcome. The exclusion criteria were being younger than 65 years (n=122) and having stayed in the ICU for less than 1 day (n=346) (Figure 1). Dementia was determined according to the Ninth and Tenth Revisions of the International Classification of Diseases (ICD-9 and ICD-10, respectively), and the corresponding codes are listed in eTable 1 including all types of dementia.28,29
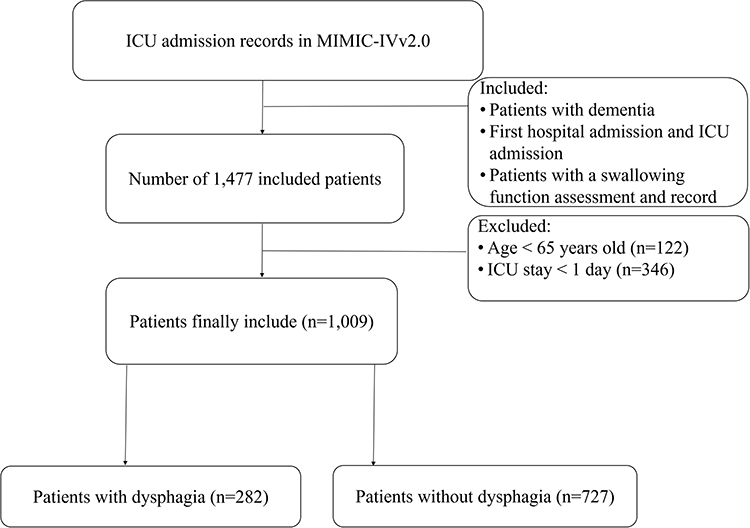 |
Figure 1 Inclusion and exclusion flowchart of the study. Abbreviations: MIMIC-IV, Medical Information Mart for Intensive Care IV; ICU, Intensive Care Units. |
Data Extraction
The study used Structured Query Language to extract data, and all the data and information that were obtained from the EHRs were preprocessed by healthcare professionals.30 The extracted data included (1) General patient information (age, sex, race, and weight); (2) Relevant scores [Sequential Organ Failure Assessment (SOFA)31 score, Glasgow Coma Scale (GCS) score,32 Charlson Comorbidity Index (CCI),33 and Braden Scale score34]; (3) Laboratory tests (albumin, hemoglobin, and red blood cells); (4) Comorbidities (congestive heart failure, cerebrovascular disease, gastric ulcer disease, mild and severe liver disease, diabetes, renal disease, malignant cancer, sepsis, hypertension, depression, and malnutrition); (5) Treatments and medications (donepezil, enteral nutrition, renal replacement therapy, vasopressors, invasive mechanical ventilation, and antibiotics); and (6) Adverse health outcomes (time to death, pressure injuries, aspiration pneumonia, and delirium). Measurements for laboratory tests and critical illness scores were taken on the first day of ICU admission for all patients. Sepsis was defined as life-threatening organ dysfunction caused by a dysregulated host response to infection and was diagnosed according to the Sepsis-3 criteria.35 The proportion of missing values for all extracted variables in this study did not exceed 25%, and we used the multiple interpolation method for addressing missing data.36
Exposure
Exposure was defined as the presence or absence of dysphagia (yes/no) in patients with dementia prior to ICU admission in our study. As the ICD-9 or ICD-10 codes for dysphagia are rather sparse,28 we turned to EHRs for identification. Specifically, we employed bedside swallowing screening data from the “chartevents” table (itemid=225118) in the MIMIC-IV database, an approach validated for its utility in numerous scientific studies.23,37,38 The “chartevents” table comprises a variety of patient measurements and observations recorded during their ICU stay, and the specific itemid “225118” corresponds to the dysphagia (difficulty swallowing) assessment, situated under the “Adm History/FHPA” (Admission History/Family History, Physical Assessment) category. The process of dysphagia assessment by the nursing team included:
- Completing a swallowing screening
- Completing an O-cat score
- Assessing the patient's alertness, ability to remain upright, and presence of oropharyngeal secretions
- Evaluating whether the patient's breathing was stable - Checking if the patient's medical history included a history of dysphagia or a diet of thickened liquids.
If a patient answered yes to any of these questions, an NPO (nihil per os, nothing by mouth) order was obtained and the patient was not allowed to eat or drink until a consultation was scheduled. If a patient answered no to all of these questions, a water swallow screening was performed. For more details on the dysphagia assessment procedure, please see the discussion at https://github.com/MIT-LCP/mimic-code/discussions/1538.
Outcomes and Definitions
The primary health outcome in this study was 90-day and 180-day all-cause mortality. The survival times of patients were calculated by subtracting the time of ICU admission from the time of death, with a minimum follow-up of 1 year per patient in the MIMIC-IV database. Secondary adverse health outcomes included aspiration pneumonia, pressure injury, and delirium. Aspiration pneumonia was diagnosed using ICD-9 code 507.X and ICD-10 code J69.X.39,40 Pressure injury was assessed directly by critical-care nurses.41 Delirium was assessed and screened for by healthcare professionals using the Confusion Assessment Method for the ICU (CAM-ICU).42,43 The scale included four features: (1) acute alteration or fluctuation in the state of consciousness, (2) inattention, (3) alteration in level of consciousness, and (4) disorganized thinking. A recent systematic review and meta-analysis demonstrated that CAM-ICU exhibits elevated sensitivity (85%) and exceptional specificity (95%).44 Patients were diagnosed as positive for delirium if they exhibited features 1, 2, and either 3 or 4. We also used a method based on a review of nursing notes to identify and accurately measure people with delirium in the ICU.45,46 We used this method to search for records47 related to (1) delirium, (2) confusion, (3) agitation, and (4) altered mental status, which were obtained from the “chartevents” table (itemid=220001).
Covariates
The following covariates were used for the analysis: age, sex, race, weight, SOFA score, GCS score, CCI, Braden Scale, albumin, malnutrition, cerebrovascular disease, chronic pulmonary disease, sepsis, donepezil, enteral nutrition, vasopressin, invasive mechanical ventilation, and antibiotics. The selection of covariates in our study was based on a comprehensive approach that took into account prior literature, clinical expertise, and the availability of data within the database.23,28 We identified variables that have previously been linked to dysphagia and dementia, as well as those with recognized clinical significance in these conditions. The variables considered in our study primarily included a wide range of factors, such as age, sex, comorbidities, medications, and disease severity scores, among others. This study adjusted covariates according to the characteristics of adverse health outcomes.
Statistical Analysis
This retrospective cohort study was performed in accordance with the recommendations of the statements in the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) initiative.48 Baseline characteristics of all patients were grouped according to swallowing status (dysphagia or no-dysphagia). The normality of continuous variables was evaluated through the Shapiro–Wilk test, revealing that the majority of these variables deviate from a normal distribution. Descriptive statistics were calculated, with continuous variables expressed as medians (interquartile ranges), and categorical variables expressed as numbers (percentages). We used the Wilcoxon rank-sum and chi-square tests for univariate comparisons of the demographic and clinical characteristics of patients and adverse health outcomes.
We performed Kaplan-Meier (KM) survival analysis to calculate survival rates at 90 and 180 days and cumulative mortality in both cohorts. The Log rank test was used to compare the differences between the survival distributions of the two cohorts. Cox proportional-hazards regression models were used to analyze the associations between dysphagia and primary adverse health outcomes, and logistic regression models were used to analyze that between dysphagia and secondary adverse health outcomes. Multifactor Cox proportional-hazards regression and multifactor logistic regression were used to adjust for covariates that could affect the study results. A subgroup analysis was performed in this study to verify the robustness of the primary findings. To enhance our comprehension of the post-discharge outcomes among older adults with dementia in the ICU, both with and without dysphagia, and to provide valuable insights for ongoing care, an extensive analysis of the discharge locations for surviving subjects was conducted. The outcomes are effectively depicted using visually informative pie charts, facilitating a clear and intuitive visualization of the distributions. Additionally, Chi-square tests were employed to evaluate the differences between groups.
In addition, despite the inclusion of potential confounders in our model, it is important to consider the presence of unmeasured confounding factors that could impact the results. Therefore, we have employed the E-value as a measure to evaluate the possibility of omitting a variable in an outcome. This metric aids in assessing whether an observed association may be influenced by an unmeasured underlying factor. Generally, a larger E-value indicates greater robustness of the research conclusion and makes it more difficult for confounding factors to explain or overturn the results.
A probability value of p<0.05 was considered significant. All data were processed using R software (version 4.2.0, https://www.r-project.org/). The E-values in our study were calculated using an online calculator available at (https://www.evalue-calculator.com/evalue/).
Results
Characteristics of the Study Cohort
This study included 1009 patients aged 65 years or older with dementia (Table 1) who were divided into two groups based on their swallowing function: dysphagia (n=282) and no-dysphagia (n=727) groups. The 1009 included patients had a median age of 84.82 years (interquartile range: 78.83–89.86 years), 571 (56.6%) were female, and most were White (72.9%). In the demographic data, the median age of patients in the no-dysphagia group was 84.75 years (interquartile range: 78.50–89.65 years) and that in the dysphagia group was 85.24 years (interquartile range: 80.45–91.03 years), with no significant difference between them (p=0.071). There were also no significant differences in sex or race between the two groups (both p>0.05). Patients with dementia and dysphagia had a lower weight, lower albumin levels, lower GCS and Braden Scale scores, and higher SOFA scores compared with the no-dysphagia group; these differences were all significant (all p<0.05). In terms of comorbidities, the dysphagia group had higher incidence rates of sepsis and malnutrition than the no-dysphagia group. In the comparison of treatment and medication use, enteral nutrition and antibiotics were used more in the dysphagia group. The differences in these comparisons were significant (all p<0.05).
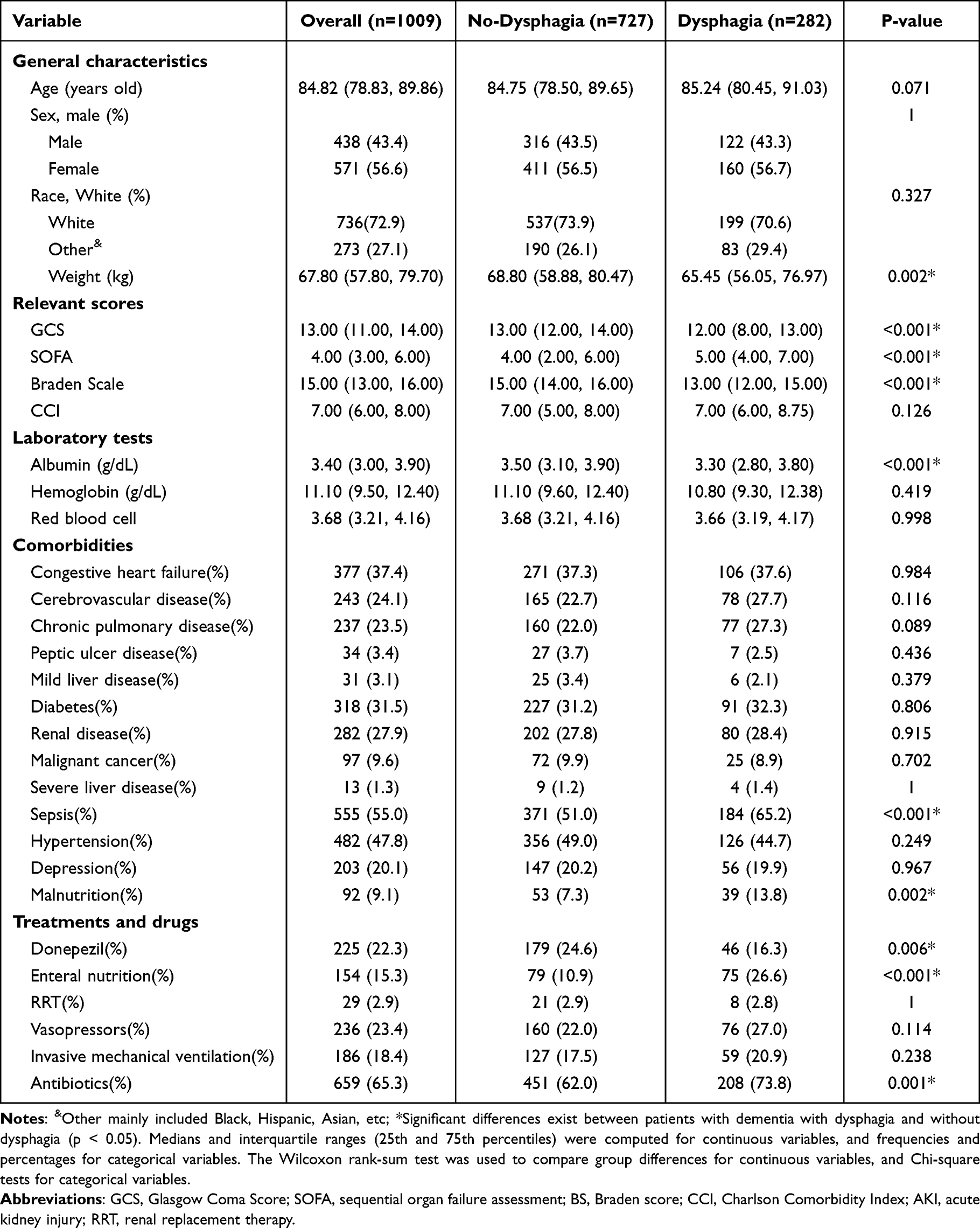 |
Table 1 Univariate Comparison of Patient Characteristics with and without Dysphagia in Older Adults with Dementia in Intensive Care Units |
Primary Outcome
The total population of this study had 90- and 180-day all-cause mortality rates of 32.6% and 40.4%, respectively (Table 2). Both 90-day (46.8% vs 27.1%, p<0.001) and 180-day (56.7% vs 34.1%, p<0.001) mortality were significantly higher in the dysphagia group with dementia than in the no-dysphagia group. KM survival curves indicated a difference in survival probability between patients with dementia in the dysphagia group and those in the no-dysphagia group (p<0.001). The survival probability was lower in the dysphagia than the no-dysphagia group (p<0.001) at 90 days (Figure 2a) and 180 days (Figure 2b). Figure 2c and d show the cumulative mortality curves for the study population at 90 and 180 days, respectively. The cumulative mortality curves also indicate that patients with dementia in the dysphagia group had a higher mortality rate than did those in the no-dysphagia group (p<0.001).
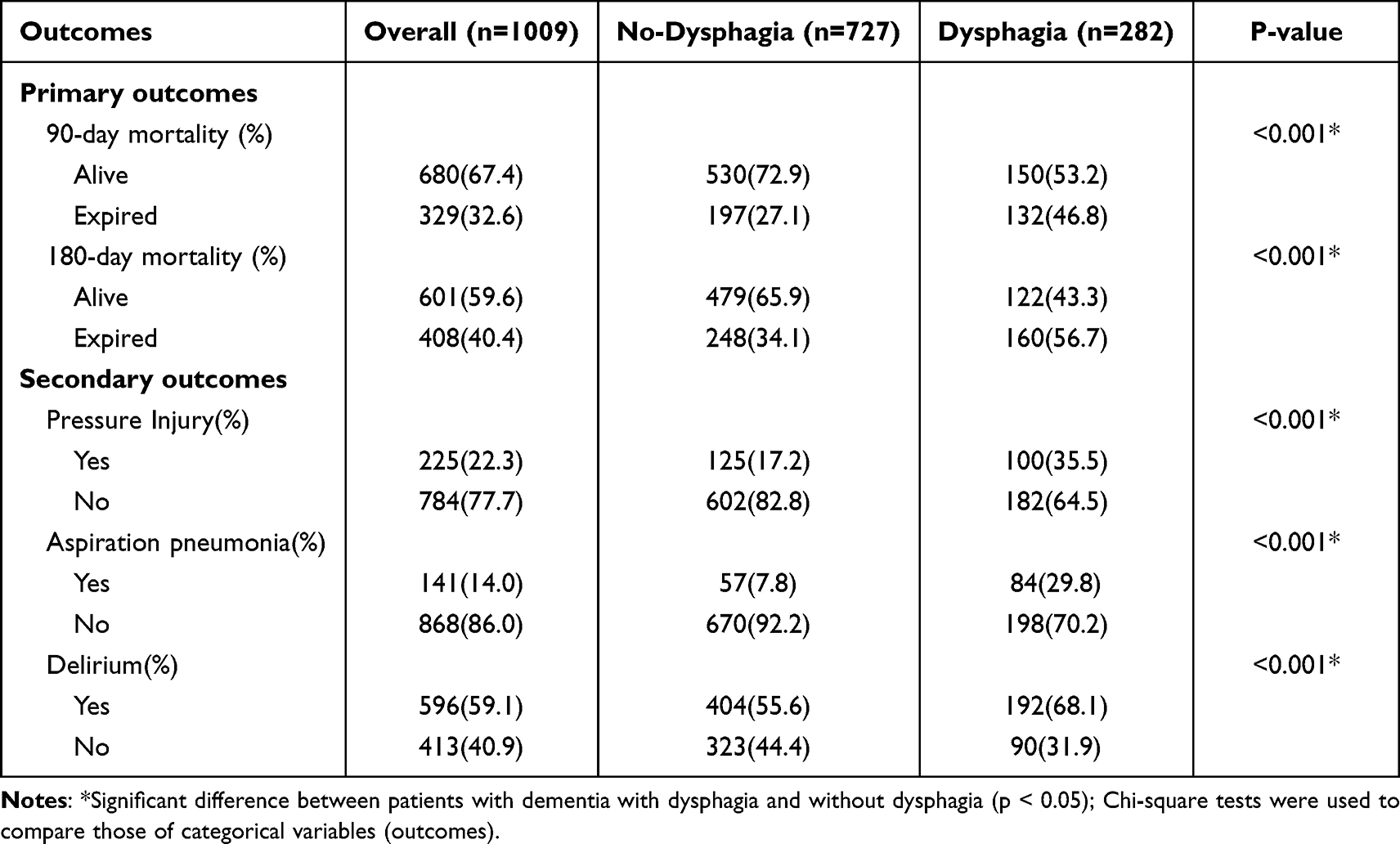 |
Table 2 Univariate Comparison of Study Outcomes with and without Dysphagia in Older Adults with Dementia in Intensive Care Units |
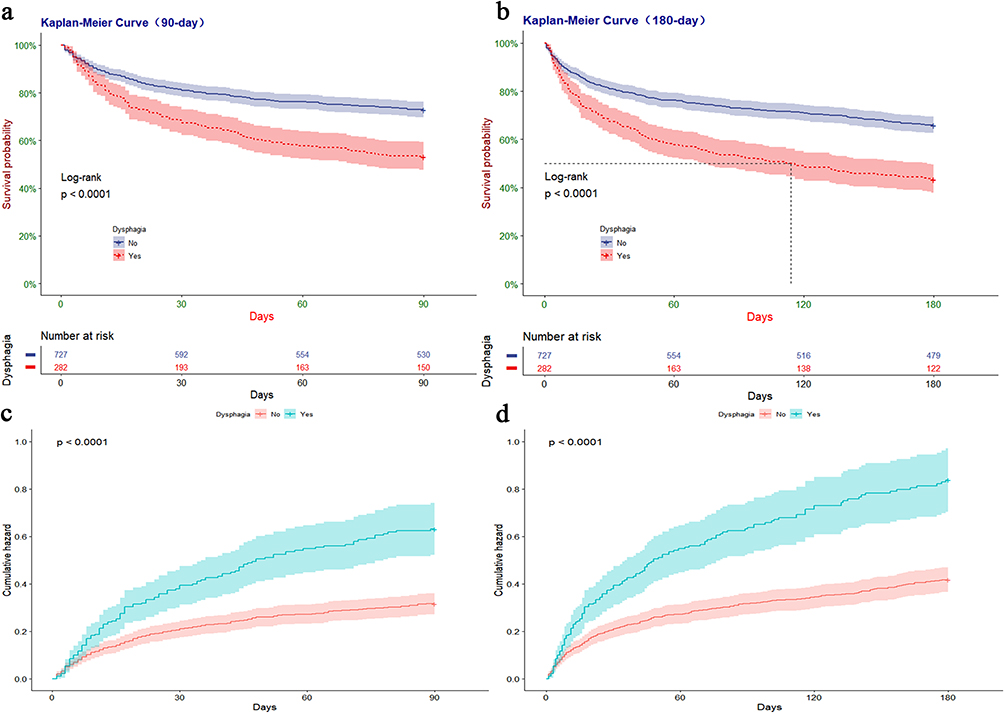 |
Figure 2 Kaplan-Meier survival curves between groups. P-value calculated by Log rank test<0.001 showed dysphagia group had lower survival probability or higher mortality than no-dysphagia group. Notes: (a) Represented the survival probability in 90-day. (b) Represented the survival probability in 180-day. (c) Represented the cumulative death curves in 90-day. (d) Represented the cumulative death curves in 180-day. |
Secondary Outcomes
The prevalence rates of pressure injury, aspiration pneumonia, and delirium in the total study population were 22.3%, 14.0%, and 59.1%, respectively (Table 2). Univariate comparisons of adverse health outcomes indicated that patients with dementia in the dysphagia group had significantly higher incidence rates of pressure injury (35.5% vs 17.2%), aspiration pneumonia (29.8% vs 7.8%), and delirium (68.1% vs 55.6%) compared with those in the no-dysphagia group (all p<0.001).
Dysphagia is Associated with Increased Adverse Health Outcomes
To test our study hypothesis, we used univariate and multifactorial models to analyze the associations between dysphagia and adverse health outcomes. Univariate Cox proportional-hazards regression (Table 3) indicated that 90- and 180-day mortality in patients with dementia were significantly associated with the presence of dysphagia (both p<0.001). We developed models to adjust for covariates such as age, sex, race, weight, and albumin, disease severity scores (eg, GCS score, SOFA score, and CCI), comorbidities (malnutrition, cerebrovascular disease, chronic pulmonary disease, and sepsis), and treatments and medications that may affect the prognosis (enteral nutrition, vasopressin, invasive mechanical ventilation, and antibiotics). After adjusting for covariates, dysphagia was associated with a significant increase in 90-day (HR=1.36, 95% CI=1.07–1.73, p=0.012) and 180-day (HR=1.47, 95% CI=1.18–1.82, p<0.001) mortality. Furthermore, we performed an E-value calculation to assess the potential impact of unaccounted confounders on the study findings. In our investigation of the relationship between dysphagia and patient mortality at 180 days, our sensitivity analysis yielded an E-value of 1.94, with a lower bound of the 95% confidence interval at 1.49. This suggests the existence of unmeasured confounding variables that could potentially explain the association between dysphagia and 180-day mortality. These confounding factors, both related to the exposure and outcome, would need to have a hazard ratio of at least 1.94 to account for the observed association.
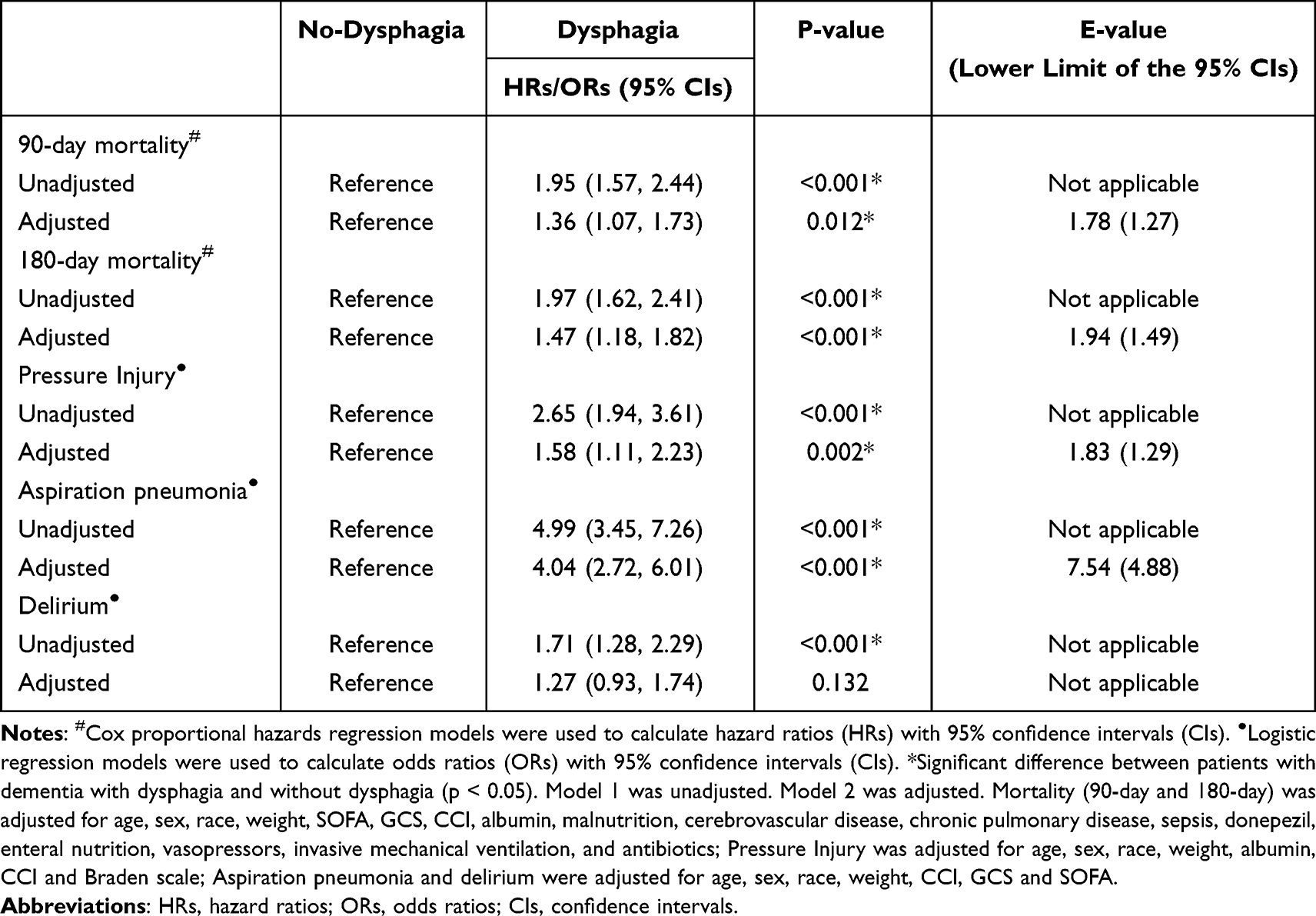 |
Table 3 Cox Proportional Hazards /Logistic Regression: Association Between Dysphagia and Primary/Secondary Study Outcomes |
This study used a binary logistic regression analysis model to calculate the associations of dysphagia with pressure injury, aspiration pneumonia, and delirium in patients with dementia. Univariate logistic regression analysis (Table 3) indicated that compared with patients with dementia without swallowing difficulties, the predominance ratios of pressure injury, aspiration pneumonia, and delirium in those with swallowing difficulties were 2.65 (95% CI=1.94–3.61), 4.99 (95% CI=3.45–7.26), and 1.71 (95% CI=1.28–2.29), with significant differences (all p<0.001). We developed multifactorial logistic regression models to adjust for covariates. Possible confounders included basic patient characteristics (sex, age, race, weight, and albumin) and disease severity scores (CCI and scores on the GCS, SOFA, and Braden Scale), and covariates were adjusted according to the characteristics of adverse health outcomes for inclusion in the multifactorial logistic regression model. After adjusting for covariates, dysphagia was significantly associated with increased occurrences of pressure injury (OR=1.58, 95% CI=1.11–2.23, p=0.002) and aspiration pneumonia (OR=4.04, 95% CI=2.72–6.01, p<0.001). However, there was no significant association between dysphagia and delirium prevalence after adjusting for confounders (OR=1.27, 95% CI=0.93–1.74, p=0.123).
Subgroup Analysis of the 180-Day Survival Rates of Patients with Dementia with and without Dysphagia
This study compared the 180-day survival rates of patients with dementia with and without dysphagia in a subgroup analysis; the results are presented as forest plots in Figure 3. Since we transformed the two continuous variables of age and GCS score into categorical variables to perform the analysis, we characterized the two variables using numbers (percentages) and compared the differences in the two variables among the patients using chi-square tests (eTable 2). Figure 3 displays the 180-day survival for subgroups of dementia patients with and without dysphagia. We observed no significant differences in 180-day survival between the two groups of patients with dementia for those aged less than 75 years and when malnutrition was present (both p>0.05). Additionally, we performed a univariate Cox proportional-hazards regression analysis to evaluate the differences among the subgroups of the two patient groups. The results of this analysis can be found in eFigure 1.
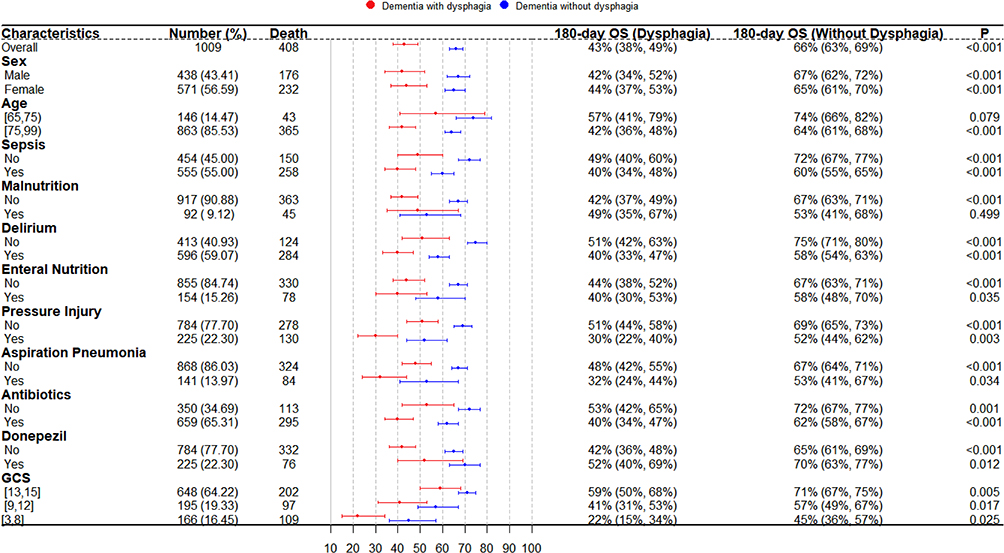 |
Figure 3 Forest plot for subgroup analysis in 180-day survival rates. P-value calculated by Log rank test <0.001 showed dysphagia group had lower survival probability than no-dysphagia group. Abbreviation: GCS, Glasgow Coma Score. |
Discharge Location
The number of patients who survived to discharge and had detailed records of their discharge locations amounted to 887. These patients were categorized into four groups based on their discharge destinations: home/family health care, nursing facility, rehabilitation facility, and other, where “other” mainly comprised psychological institutions and hospices. Figure 4a illustrates the discharge sites for older dementia patients with dysphagia, while Figure 4b shows the discharge sites for dementia patients without dysphagia. In the dysphagia group (Figure 4a), 156 individuals (65%) were discharged to nursing institutions, 32 individuals (13.33%) were discharged home, 16 individuals (6.67%) were discharged to rehabilitation facilities, and 36 individuals (15%) were transferred to other institutions. Conversely, in the group without dysphagia, 382 individuals (59.04%) were discharged to nursing facilities, 169 individuals (26.12%) were discharged home, 58 individuals (8.97%) were discharged to rehabilitation facilities, and 38 individuals (5.87%) were transferred to other institutions. Statistical analysis using a chi-square test indicated a significant difference in discharge locations between the two groups (p<0.001). This information is valuable for preparation, transitional care, and continuity of care planning for individuals with dementia who have undergone intensive care.
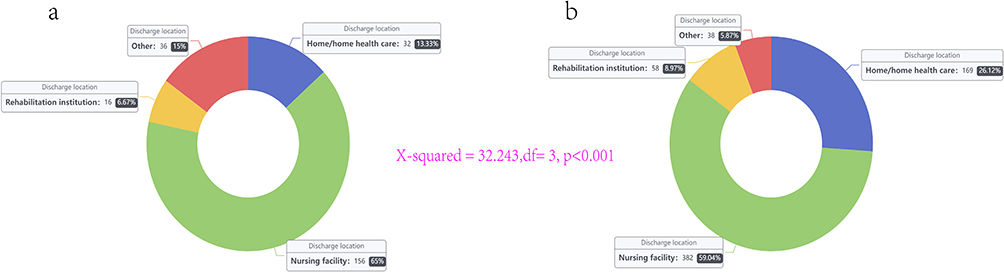 |
Figure 4 Discharge locations of dementia older patients with and without dysphagia. Notes: (a) Represented the group with dysphagia; (b) Represented the group without dysphagia; p<0.001 indicated a statistically significant difference in discharge locations between the two groups; “Other” mainly comprised psychological institutions and hospices. |
Discussion
Despite the high prevalence of dysphagia in patients with dementia who present at ICUs, assessments of their adverse outcomes have been lacking.18 Considering that dysphagia is strongly associated with adverse health outcomes in patients with severe dementia, this study selected 1009 patients from a large intensive care medicine database based on an EHR information system, including 282 with dysphagia. KM survival curves indicated that both 90- and 180-day survival rates were significantly lower in the patients with dementia and dysphagia than in those without dysphagia (both p<0.001). After adjusting for potential confounding factors, our multivariate analyses revealed a significant association between dysphagia and increased 90-day and 180-day mortality risk, pressure injuries, and aspiration pneumonia. However, no significant association was observed with delirium. These findings are further explained and discussed below.
Similar to previous findings, dysphagia was associated with increased mortality in patients with dementia.15,16,49 One possible reason for this phenomenon is that dysphagia is closely related to sarcopenia in older adults, which can affect feeding ability and nutrient absorption, and can lead to aspiration of food or liquid into the trachea, which results in aspiration pneumonia or even death from asphyxiation in severe cases.11,50 In light of these findings, dysphagia in dementia patients represents a substantial challenge post-discharge. The complex interplay of cognitive decline and impaired swallowing often leads to a significant understatement of symptoms, hindering effective management of dysphagia. Additionally, nursing partners frequently confront substantial communication gaps regarding dysphagia management, adding to their stress and potentially compromising the patient’s health outcomes.51,52 These unique challenges underscore the pressing need for healthcare managers to develop specialized care strategies aimed at improving the survival and quality of life in post-discharge dementia patients with dysphagia, considering the adverse effects of dysphagia on older adults with dementia.
Pressure injuries, also known as pressure ulcers, have a high incidence in high-risk settings such as the ICU, and are considered one of the most important indicators for evaluating nursing quality.53,54 Schott et al found that the risk of pressure injury was higher in inpatients with stroke.55 We reached the same conclusion: dysphagia was associated with a significant increase in the occurrence of pressure-related injuries. Patients with dysphagia are vulnerable to pressure injuries due to inadequate nutritional intake, hypoalbuminemia, and weight loss,56 which highlights the importance of intensive care nurses enhancing skin care for older patients with dementia and swallowing difficulties.
Makhnevich et al found a significant association between dysphagia and delirium onset in hospitalized patients with dementia (OR=1.53, 95% CI=1.40–1.68).23 However, our study found no significant association between dysphagia and delirium occurrence (OR=1.27, 95% CI=0.93–1.74, p=0.123). A reason for this may be differences in the study population, as Makhnevich et al focused on inpatients while we focused on the critical care population, where unlike in general wards, delirium is one of the common complications in patients admitted to the ICU.57 Another possible reason was that we used a combined CAM-ICU and nursing notes review approach to detect delirium. This combined approach may have high predictive validity for all clinical outcomes.45 The different methods used to identify delirium may therefore lead to differences in the study results. Furthermore, the challenges of differentiating between dementia and delirium due to their clinical similarity present additional complexity.58 This inherent difficulty, especially prevalent among clinicians and nurses outside the field of psychiatry, could have impacted the accurate identification and consequent documentation of delirium in our study population. Delirium is a complex topic for patients with dementia, and the relationship between dysphagia and delirium therefore still needs to be further explored.
Notably, the subgroup analysis indicated that there was no significant difference in 180-day survival between the dysphagia and no-dysphagia groups when the age was <75 years (p=0.079), whereas there was a significant difference when the patients were older than 75 years (p<0.001). One possible explanation is that nutrition in the elderly will change alongside physiological changes with age.59 In general, but specifically in the elderly, reduced energy intake, lower metabolic rate, inhibited mastication and digestion, and slower visual, olfactory, and gustatory responses with age may increase the risks of malnutrition and dehydration, which undoubtedly affect the prognosis of patients.60–63 This finding suggests that physicians and nurses in the ICU need to pay more attention to the prognosis of adult patients with dementia aged ≥75 years.
In the ICU management of older adults afflicted with both dementia and dysphagia, maintaining appropriate nutritional status emerges as a critical imperative. Existing studies reveal that the presence of appetite and weight loss symptoms during episodes of late-life depression can serve as predictive indicators for dementia outcomes, underscoring the significance of nutritional factors in this particular population.64 However, ensuring sufficient nutritional intake in patients with dementia and dysphagia poses a substantial challenge due to the presence of swallowing difficulties and potential eating disorders. Additionally, the decision-making process concerning the transition from oral feeding to alternative approaches, such as enteral nutrition, becomes crucial when managing complications like aspiration pneumonia or sepsis, as it can profoundly impact both the quality of life and disease progression of these patients. Notably, research has indicated that while percutaneous endoscopic gastrostomy (PEG) tube placement may initially appear as a logical intervention, patients with dementia have exhibited higher mortality rates subsequent to PEG placement, underscoring the need for cautious deliberation.65 The complexities associated with the nutritional management of ICU patients with dementia and dysphagia highlight the importance of adopting personalized, patient-centric approaches. Such approaches involve carefully weighing the benefits and risks associated with different feeding methods to optimize patient outcomes.
Indeed, there is still a lack of effective clinical management strategies for dysphagia and its associated symptoms for patients with dementia.13 Modifying food texture and liquid consistency is a popular nutritional management strategy and is one of the most common forms of clinical intervention for patients with swallowing difficulties.66 Patients will swallow more easily and safely when the properties of the food and liquids that they ingest are modified appropriately.67 However, several systematic evaluations and meta-analyses have found that there is insufficient evidence that changing food properties and fluid consistency improves patient morbidity, mortality, and adverse conditions such as aspiration pneumonia, which may lead to malnutrition and even affect the quality of life of patients with dysphagia.68–71 Patients with dysphagia must therefore be provided with information about potential risks before clinicians and dietitians can make the decision to prescribe a modified diet. This highlights the current clinical complexity of managing patients with dysphagia, especially in the critical population. Given the potential harm that dysphagia poses to older adults with dementia during critical illness, effective intervention strategies should be a focus of future research.
Limitations
Several limitations in this study necessitate emphasis. Firstly, the lack of detailed data regarding the severity and types of both dementia and dysphagia might have influenced the results. Despite noting the presence or absence of these conditions, the extent of their manifestation, which could have significantly impacted our findings, remained unidentified. A particular challenge was differentiating delirium from dementia; delirium, assessed through the CAM-ICU and nursing notes, was often conflated with dementia due to overlapping keywords such as “confusion”, potentially leading to misclassification. Furthermore, the dataset lacked comprehensive information pertaining to patients’ baseline cognitive functions. While cognitive assessments72 such as the Montreal Cognitive Assessment or Mini Mental State Examination are vital, their scores were not universally available in the electronic health records, thereby limiting our ability to interpret patients’ functional status upon ICU admission. Compounding these issues, the retrospective, single-center design of our study, conducted within a tertiary academic medical center, may restrict the broader applicability of our findings. Lastly, the timeframe of our study, spanning from 2008 to 2019, could have introduced additional confounding factors due to shifts in medical and nursing practices over this period.
Considering these limitations, the way forward necessitates undertaking comprehensive, prospective multi-center studies. These future investigations should strive to collect comprehensive data on the severity of dementia and dysphagia and baseline cognitive function. By addressing these gaps, we can augment our comprehension and clinical management of dysphagia in critically ill dementia patients, ultimately striving to enhance their quality of life and outcomes.
Conclusion
This retrospective population-based study explored the association of dysphagia with adverse health outcomes in ICU patients with dementia. Our findings, after adjusting for potential confounding factors, revealed that the presence of dysphagia significantly increased the risk of adverse outcomes, including mortality within 90 and 180 days. Moreover, dysphagia was linked to a heightened incidence of pressure injuries and aspiration pneumonia, but was not significantly associated with the prevalence of delirium. These results contributed to a growing body of evidence highlighting the clinical importance of identifying and managing dysphagia in the complex care of dementia patients within ICU settings. Our findings underscored the necessity of incorporating routine dysphagia screening and effective intervention strategies as part of the comprehensive care plan for this vulnerable population.
Abbreviations
AD, Alzheimer’s disease; CAM-ICU, the Confusion Assessment Method for the ICU; CCI, Charlson Comorbidity Index; CI, Confidence Intervals; EHRs, Electronic Health Records; GCS, Glasgow Coma Scale; HR, Hazard Ratios; ICD, International Classification of Diseases; ICU, Intensive Care Unit; KM, Kaplan-Meier; MIMIC-IV, Medical Information Mart for Intensive Care IV; OR, Odds Ratios; PEG, Percutaneous Endoscopic Gastrostomy; SOFA, Sequential Organ Failure Assessment; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; USA, the United States of America.
Data Sharing Statement
The data were available on the MIMIC-IV website at https://mimic.physionet.org/. The data in this article can be reasonably applied to the corresponding author.
Ethics Approval and Consent to Participate
The Medical Information Mart for Intensive Care IV (MIMIC-IV) database was supported by grants from the National Institute of Biomedical Imaging and Bioengineering (NIBIB) of the National Institutes of Health (NIH) under award numbers R01-EB001659 (2003–2013) and R01-EB017205 (2014–2018) and approved by the Institutional Review Boards of Beth Israel Deaconess Medical Center (Boston, MA) and the Massachusetts Institute of Technology (Cambridge, MA).
Informed Consent
Data extracted from the MIMIC-IV database do not require individual informed consent because the research data is publicly available, and all patient data are de-identified.
Acknowledgment
Thanks for all authors’ contribution(s) to the research and manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was supported by Guangdong Provincial Key Laboratory of Traditional Chinese Medicine Informatization (2021B1212040007).
Disclosure
The authors declare that they have no competing interests.
References
1. Gale SA, Acar D, Daffner KR. Dementia. Am J Med. 2018;131(10):1161–1169. doi:10.1016/j.amjmed.2018.01.022
2. Raz L, Knoefel J, Bhaskar K. The neuropathology and cerebrovascular mechanisms of dementia. J Cereb Blood Flow Metab. 2016;36(1):172–186. doi:10.1038/jcbfm.2015.164
3. Jia L, Quan M, Fu Y, et al. Dementia in China: epidemiology, clinical management, and research advances. Lancet Neurol. 2020;19(1):81–92. doi:10.1016/S1474-4422(19)30290-X
4. Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care. Lancet. 2017;390(10113):2673–2734. doi:10.1016/S0140-6736(17)31363-6
5. Ferri CP, Prince M, Brayne C, et al. Global prevalence of dementia: a delphi consensus study. Lancet. 2005;366(9503):2112–2117. doi:10.1016/S0140-6736(05)67889-0
6. Rajan KB, Weuve J, Barnes LL, McAninch EA, Wilson RS, Evans DA. Population estimate of people with clinical Alzheimer’s disease and mildcognitive impairment in the United States (2020–2060). Alzheimers Dement. 2021;17(12):1966–1975. doi:10.1002/alz.12362
7. 2022 Alzheimer’s disease facts and figures. Alzheimers Dement. 2022;18(4):700–789.
8. 2021 Alzheimer’s disease facts and figures. Alzheimers Dement. 2021;17(3):327–406.
9. Wirth R, Dziewas R, Beck AM, et al. Oropharyngeal dysphagia in older persons - from pathophysiology to adequateintervention: a review and summary of an international expert meeting. Clin Interv Aging. 2016;11:189–208. doi:10.2147/CIA.S97481
10. Thiyagalingam S, Kulinski AE, Thorsteinsdottir B, Shindelar KL, Takahashi PY. Dysphagia in older adults. Mayo Clin Proc. 2021;96(2):488–497. doi:10.1016/j.mayocp.2020.08.001
11. Rommel N, Hamdy S. Oropharyngeal dysphagia: manifestations and diagnosis. Nat Rev Gastroenterol Hepatol. 2016;13(1):49–59. doi:10.1038/nrgastro.2015.199
12. Carucci LR, Turner MA. Dysphagia revisited: common and unusual causes. Radiographics. 2015;35(1):105–122. doi:10.1148/rg.351130150
13. Flynn E, Smith CH, Walsh CD, Walshe M. Modifying the consistency of food and fluids for swallowing difficulties in dementia. Cochrane Database Syst Rev. 2018;9(9):D11077.
14. Madhavan A, LaGorio LA, Crary MA, Dahl WJ, Carnaby GD. Prevalence of and risk factors for dysphagia in the community dwelling elderly: asystematic review. J Nutr Health Aging. 2016;20(8):806–815. doi:10.1007/s12603-016-0712-3
15. Carrion S, Cabre M, Monteis R, et al. Oropharyngeal dysphagia is a prevalent risk factor for malnutrition in a cohortof older patients admitted with an acute disease to a general hospital. Clin Nutr. 2015;34(3):436–442. doi:10.1016/j.clnu.2014.04.014
16. Espinosa-Val MC, Martin-Martinez A, Graupera M, et al. Prevalence, risk factors, and complications of oropharyngeal dysphagia in older patients with dementia. Nutrients. 2020;12(3). doi:10.3390/nu12030863
17. Baijens LW, Clave P, Cras P, et al. European society for swallowing disorders - European Union geriatric medicine society white paper: oropharyngeal dysphagia as a geriatric syndrome. Clin Interv Aging. 2016;11:1403–1428. doi:10.2147/CIA.S107750
18. Wilkinson JM, Codipilly DC, Wilfahrt RP. Dysphagia: evaluation and collaborative management. Am Fam Physician. 2021;103(2):97–106.
19. Adkins C, Takakura W, Spiegel B, et al. Prevalence and characteristics of dysphagia based on a population-based survey. Clin Gastroenterol Hepatol. 2020;18(9):1970–1979. doi:10.1016/j.cgh.2019.10.029
20. Cheng ST. Dementia caregiver burden: a research update and critical analysis. Curr Psychiatry Rep. 2017;19(9):64. doi:10.1007/s11920-017-0818-2
21. Bloomer MJ, Woszczeiko C, Hutchinson AM. Older age, delirium, dementia, frailty, and critical care: care priorities. Intensive Crit Care Nurs. 2022;73:103297. doi:10.1016/j.iccn.2022.103297
22. Brodsky MB, Pandian V, Needham DM. Post-extubation dysphagia: a problem needing multidisciplinary efforts. Intensive Care Med. 2020;46(1):93–96. doi:10.1007/s00134-019-05865-x
23. Makhnevich A, Marziliano A, Ahmad SE, et al. Factors and outcomes associated with dysphagia in hospitalized persons with dementia. J Am Med Dir Assoc. 2022;23(8):1354–1359. doi:10.1016/j.jamda.2021.12.027
24. Johnson A, Bulgarelli L, Shen L, et al. MIMIC-IV, a freely accessible electronic health record dataset. Sci Data. 2023;10(1):1. doi:10.1038/s41597-022-01899-x
25. Yang J, Li Y, Liu Q, et al. Brief introduction of medical database and data mining technology in big dataera. J Evid Based Med. 2020;13(1):57–69. doi:10.1111/jebm.12373
26. Rosenbloom ST, Smith J, Bowen R, Burns J, Riplinger L, Payne TH. Updating HIPAA for the electronic medical record era. J Am Med Inform Assoc. 2019;26(10):1115–1119. doi:10.1093/jamia/ocz090
27. Zhang Z, Ho KM, Hong Y. Machine learning for the prediction of volume responsiveness in patients witholiguric acute kidney injury in critical care. Crit Care. 2019;23(1):112. doi:10.1186/s13054-019-2411-z
28. Lieberman OJ, Lee S, Zabinski J. Donepezil treatment is associated with improved outcomes in critically illdementia patients via a reduction in delirium. Alzheimers Dement. 2023;19(5):1742–1751. doi:10.1002/alz.12807
29. Knopman DS, Gottesman RF, Sharrett AR, et al. Mild cognitive impairment and dementia prevalence: the atherosclerosis risk in communities neurocognitive study (ARIC-NCS). Alzheimers Dement. 2016;2:1–11.
30. Wu WT, Li YJ, Feng AZ, et al. Data mining in clinical big data: the frequently used databases, steps, and methodological models. Mil Med Res. 2021;8(1):44. doi:10.1186/s40779-021-00338-z
31. Lambden S, Laterre PF, Levy MM, Francois B. The SOFA score-development, utility and challenges of accurate assessment in clinical trials. Crit Care. 2019;23(1):374. doi:10.1186/s13054-019-2663-7
32. Teasdale G, Maas A, Lecky F, Manley G, Stocchetti N, Murray G. The glasgow coma scale at 40 years: standing the test of time. Lancet Neurol. 2014;13(8):844–854. doi:10.1016/S1474-4422(14)70120-6
33. Charlson ME, Carrozzino D, Guidi J, Patierno C. Charlson comorbidity index: a critical review of clinimetric properties. Psychother Psychosom. 2022;91(1):8–35. doi:10.1159/000521288
34. Bergstrom N, Braden BJ, Laguzza A, Holman V. The braden scale for predicting pressure sore risk. Nurs Res. 1987;36(4):205–210. doi:10.1097/00006199-198707000-00002
35. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
36. Morris TP, White IR, Royston P. Tuning multiple imputation by predictive mean matching and local residual draws. Bmc Med Res Methodol. 2014;14:75. doi:10.1186/1471-2288-14-75
37. Hollinghurst J, Smithard DG. Identifying dysphagia and demographic associations in older adults using electronic health records: a national longitudinal observational study in Wales (United Kingdom) 2008-2018. Dysphagia. 2022;37(6):1612–1622. doi:10.1007/s00455-022-10425-5
38. Martin-Martinez A, Miro J, Amado C, et al. A systematic and universal artificial intelligence screening method for oropharyngeal dysphagia: improving diagnosis through risk management. Dysphagia. 2022. doi:10.1007/s00455-022-10547-w
39. Palacios-Cena D, Hernandez-Barrera V, Lopez-de-andres A, et al. Time trends in incidence and outcomes of hospitalizations for aspiration pneumonia among elderly people in Spain (2003–2013). Eur J Intern Med. 2017;38:61–67. doi:10.1016/j.ejim.2016.12.022
40. Bosch G, Comas M, Domingo L, et al. Dysphagia in hospitalized patients: prevalence, related factors and impact on aspiration pneumonia and mortality. Eur J Clin Invest. 2023;53(4):e13930. doi:10.1111/eci.13930
41. Martin-Loeches I, Rose L, Afonso E, et al. Epidemiology and outcome of pressure injuries in critically ill patients with chronic obstructive pulmonary disease: a propensity score adjusted analysis. Int J Nurs Stud. 2022;129:104222. doi:10.1016/j.ijnurstu.2022.104222
42. Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286(21):2703–2710. doi:10.1001/jama.286.21.2703
43. Stollings JL, Kotfis K, Chanques G, Pun BT, Pandharipande PP, Ely EW. Delirium in critical illness: clinical manifestations, outcomes, and management. Intensive Care Med. 2021;47(10):1089–1103. doi:10.1007/s00134-021-06503-1
44. Chen TJ, Chung YW, Chang HR, et al. Diagnostic accuracy of the CAM-ICU and ICDSC in detecting intensive care unit delirium: a bivariate meta-analysis. Int J Nurs Stud. 2021;113:103782. doi:10.1016/j.ijnurstu.2020.103782
45. Saczynski JS, Kosar CM, Xu G, et al. A tale of two methods: chart and interview methods for identifying delirium. J Am Geriatr Soc. 2014;62(3):518–524. doi:10.1111/jgs.12684
46. Inouye SK, Leo-Summers L, Zhang Y, Bogardus SJ, Leslie DL, Agostini JV. A chart-based method for identification of delirium: validation compared with interviewer ratings using the confusion assessment method. J Am Geriatr Soc. 2005;53(2):312–318. doi:10.1111/j.1532-5415.2005.53120.x
47. Puelle MR, Kosar CM, Xu G, et al. The language of delirium: keywords for identifying delirium from medical records. J Gerontol Nurs. 2015;41(8):34–42. doi:10.3928/00989134-20150723-01
48. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
49. Lindroos E, Saarela RK, Soini H, Muurinen S, Suominen MH, Pitkala KH. Caregiver-reported swallowing difficulties, malnutrition, and mortality among older people in assisted living facilities. J Nutr Health Aging. 2014;18(7):718–722. doi:10.1007/s12603-014-0506-4
50. Wieseke A, Bantz D, Siktberg L, Dillard N. Assessment and early diagnosis of dysphagia. Geriatr Nurs. 2008;29(6):376–383. doi:10.1016/j.gerinurse.2007.12.001
51. De Stefano A, Di Giovanni P, Kulamarva G, et al. Oropharyngeal dysphagia in elderly population suffering from mild cognitive impairment and mild dementia: understanding the link. Am J Otolaryngol. 2020;41(4):102501. doi:10.1016/j.amjoto.2020.102501
52. Makhnevich A, Marziliano A, Porreca K, Gromova V, Diefenbach MA, Sinvani L. Oropharyngeal dysphagia in hospitalized older adults with dementia: a mixed-methods study of care partners. Am J Speech Lang Pathol. 2023;32(1):234–245. doi:10.1044/2022_AJSLP-22-00126
53. Tayyib N, Coyer F. Effectiveness of pressure ulcer prevention strategies for adult patients in intensive care units: a systematic review. Worldviews Evid Based Nurs. 2016;13(6):432–444. doi:10.1111/wvn.12177
54. Wei M, Wu L, Chen Y, Fu Q, Chen W, Yang D. Predictive validity of the braden scale for pressure ulcer risk in critical care: a meta-analysis. Nurs Crit Care. 2020;25(3):165–170. doi:10.1111/nicc.12500
55. Schott M, Golin A, de Jesus SR, et al. Dysphagia, immobility, and diet acceptance: main factors associated with increased risk of pressure injury in patients hospitalized after stroke. Adv Skin Wound Care. 2020;33(10):527–532. doi:10.1097/01.ASW.0000694140.54146.75
56. Mervis JS, Phillips TJ. Pressure ulcers: pathophysiology, epidemiology, risk factors, and presentation. J Am Acad Dermatol. 2019;81(4):881–890. doi:10.1016/j.jaad.2018.12.069
57. Cortes-Beringola A, Vicent L, Martin-Asenjo R, et al. Diagnosis, prevention, and management of delirium in the intensive cardiac care unit. Am Heart J. 2021;232:164–176. doi:10.1016/j.ahj.2020.11.011
58. Fong TG, Hshieh TT, Tabloski PA, et al. Identifying delirium in persons with moderate or severe dementia: review of challenges and an illustrative approach. Am J Geriatr Psychiatry. 2022;30(10):1067–1078. doi:10.1016/j.jagp.2022.04.003
59. Shea MK, Korat A, Jacques PF, et al. Leveraging observational cohorts to study diet and nutrition in older adults: opportunities and obstacles. Adv Nutr. 2022;13(5):1652–1668. doi:10.1093/advances/nmac031
60. Norman K, Hass U, Pirlich M. Malnutrition in older adults-recent advances and remaining challenges. Nutrients. 2021;13(8):2764. doi:10.3390/nu13082764
61. Mathieu ME, Reid R, King NA. Sensory profile of adults with reduced food intake and the potential roles of nutrition and physical activity interventions. Adv Nutr. 2019;10(6):1120–1125. doi:10.1093/advances/nmz044
62. Roberts SB, Rosenberg I. Nutrition and aging: changes in the regulation of energy metabolism with aging. Physiol Rev. 2006;86(2):651–667. doi:10.1152/physrev.00019.2005
63. Roberts SB, Silver RE, Das SK, et al. Healthy aging-nutrition matters: start early and screen often. Adv Nutr. 2021;12(4):1438–1448. doi:10.1093/advances/nmab032
64. Saha S, Hatch DJ, Hayden KM, Steffens DC, Potter GG. Appetite and weight loss symptoms in late-life depression predict dementia outcomes. Am J Geriatr Psychiatry. 2016;24(10):870–878. doi:10.1016/j.jagp.2016.05.004
65. van Bruchem-Visser RL, Mattace-Raso F, de Beaufort ID, Kuipers EJ. Percutaneous endoscopic gastrostomy in older patients with and without dementia: survival and ethical considerations. J Gastroenterol Hepatol. 2019;34(4):736–741. doi:10.1111/jgh.14573
66. Hadde EK, Chen J. Texture and texture assessment of thickened fluids and texture-modified food for dysphagia management. J Texture Stud. 2021;52(1):4–15. doi:10.1111/jtxs.12567
67. Clave P, de Kraa M, Arreola V, et al. The effect of bolus viscosity on swallowing function in neurogenic dysphagia. Aliment Pharmacol Ther. 2006;24(9):1385–1394. doi:10.1111/j.1365-2036.2006.03118.x
68. O’Keeffe ST. Use of modified diets to prevent aspiration in oropharyngeal dysphagia: is current practice justified? Bmc Geriatr. 2018;18(1):167. doi:10.1186/s12877-018-0839-7
69. Duncan S, McAuley DF, Walshe M, et al. Interventions for oropharyngeal dysphagia in acute and critical care: asystematic review and meta-analysis. Intensive Care Med. 2020;46(7):1326–1338. doi:10.1007/s00134-020-06126-y
70. Alagiakrishnan K, Bhanji RA, Kurian M. Evaluation and management of oropharyngeal dysphagia in different types of dementia: a systematic review. Arch Gerontol Geriatr. 2013;56(1):1–9. doi:10.1016/j.archger.2012.04.011
71. Painter V, Le Couteur DG, Waite LM. Texture-modified food and fluids in dementia and residential aged care facilities. Clin Interv Aging. 2017;12:1193–1203. doi:10.2147/CIA.S140581
72. Pinto T, Machado L, Bulgacov TM, et al. Is the Montreal Cognitive Assessment (MoCA) screening superior to the Mini-MentalState Examination (MMSE) in the detection of mild cognitive impairment (MCI) and Alzheimer’s Disease (AD) in the elderly? Int Psychogeriatr. 2019;31(4):491–504. doi:10.1017/S1041610218001370
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.