Back to Journals » Nature and Science of Sleep » Volume 17

Associations Among Obstructive Sleep Apnea, Thyroid Function and Morphology Changes
Authors Xie Y, Zhang H, Cao Z, Zhou Y, Lu C, Yin L, Zhu S ![]() , Su Y, Niu X, Ma L, Yuan Y, Zhang Y
, Su Y, Niu X, Ma L, Yuan Y, Zhang Y ![]() , Wang Z, Liu H, Ren X, Shi Y
, Wang Z, Liu H, Ren X, Shi Y ![]()
Received 19 November 2024
Accepted for publication 21 June 2025
Published 29 July 2025 Volume 2025:17 Pages 1727—1741
DOI https://doi.org/10.2147/NSS.S507318
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Valentina Alfonsi
Yushan Xie,1,2,* Hongli Zhang,3,* Zine Cao,1,* Yanuo Zhou,1,2 Chendi Lu,1,2 Libo Yin,4 Simin Zhu,1,2 Yonglong Su,1,2 Xiaoxin Niu,1,2 Lina Ma,1,2 Yuqi Yuan,1,2 Yitong Zhang,1,2 Zitong Wang,1,2 Haiqin Liu,1,2 Xiaoyong Ren,1,2 Yewen Shi1,2
1Department of Otorhinolaryngology—Head and Neck Surgery, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China; 2Shaanxi Provincial Key Laboratory for Precision Diagnosis and Treatment of Otorhinolaryngology, Xi’an, People’s Republic of China; 3Department of Ultrasound, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China; 4Otolaryngology Head and Neck Surgery Department, Xi’an Central Hospital, Xi’an, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoyong Ren, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China, Email [email protected] Yewen Shi, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China, Email [email protected]
Purpose: This study unveils the complex interplay among obstructive sleep apnea (OSA), thyroid function, and morphological changes.
Methods: Data from 1,102 patients were collected retrospectively from the Department of Otorhinolaryngology—Head and Neck Surgery of the Second Affiliated Hospital of Xi’an Jiaotong University from 2012 to 2023. The patients were divided into severe and non-severe OSA groups according to their polysomnography results. The data were analyzed by sex and age stratification.
Results: Serum free triiodothyronine (FT3), total triiodothyronine (TT3), and reverse triiodothyronine (RT3) were higher in severe OSA group in the total population (p < 0.05). Similar trends were observed in male but not in female. FT3 and TT3 are higher in the severe group in the nonelderly population (age < 60) (p < 0.05), and RT3 is higher in the severe group in the elderly population (age ≥ 60) (p < 0.05). In addition, we first reveal that RT3 is associated with the diameter of the left inferior thyroid artery (L-ITA) (r=0.394, p < 0.05) and lowest transcutaneous oxygen saturation at night (lowest SpO2) (r=− 0.269, p < 0.05). The severe OSA group showed larger thyroid volume and isthmus length, as well as the thicker ITA diameter and lower left thyroid lobe resistance index (RI) (all p < 0.05).
Conclusion: Our study demonstrates a significant association between thyroid function/morphology and OSA, with distinct sex- and age-related differences. Reduced RI in severe OSA suggests its clinical utility in assessing vascular health. Increased thyroid volume and isthmus length in severe OSA may reflect ITA-related changes. These findings support our prior observations of rising thyroid hormone levels with OSA progression and highlight the need for sex- and age-stratified analyses. Integrated evaluation of thyroid function and morphology is essential for understanding OSA-thyroid pathophysiology.
Keywords: obstructive sleep apnea, thyroid function, thyroid morphology, inferior thyroid artery
Background
Obstructive sleep apnea (OSA) is a prevalent sleep disorder characterized by recurrent episodes of upper airway obstruction during sleep, leading to partial or complete cessation of airflow. These repetitive breathing pauses result in intermittent hypoxia, sleep fragmentation, and increased sympathetic activity, contributing to numerous adverse health outcomes, including hypertension, coronary heart disease, and stroke.1 Moreover, OSA is closely associated with the endocrine system. The relationship between OSA and endocrine system diseases has recently become a research focus.
The thyroid gland, the largest endocrine gland in the human body, secretes total thyroxine (TT4) and serum total triiodothyronine (TT3), which significantly influence various physiological processes, including thermoregulation, digestion, and vital functions. The coexistence of OSA and thyroid disorders presents a complex interplay between two distinct physiological systems. Studies have suggested a bidirectional relationship between OSA and thyroid dysfunction, with each condition potentially influencing the pathogenesis and clinical course of the other. Chronic intermittent hypoxia (CIH) in OSA can disrupt the hypothalamic–pituitary–thyroid axis, leading to alterations in thyroid hormone (TH) levels and thyroid function.2 The precise mechanisms underlying this process remain incompletely understood. However, the characteristic CIH associated with OSA may promote the accumulation of reactive oxygen species (ROS), subsequently activating inflammatory pathways such as NF-κB.3 This cascade contributes to vascular endothelial dysfunction, leading to alterations in arterial morphology and function. Consistent with this hypothesis, a clinical study has shown a positive correlation between carotid intima-media thickness (IMT) and the apnea-hypopnea index (AHI).4 Notably, whether similar vascular changes occur in thyroid arteries remains an open question. Furthermore, CIH may contribute to the development of non-thyroidal illness syndrome (NTIS) by downregulating deiodinase 1 (DIO1) and upregulating deiodinase 3 (DIO3), thereby accelerating the conversion of T4 to RT3.5 Conversely, thyroid dysfunction may contribute to obesity, which is a common risk factor for OSA, through its impact on metabolism and energy regulation.6
Thyroid hormone levels exhibit physiological circadian rhythm variations.7 Beyond this regulation, thyroid function demonstrates sex-specific differences, potentially mediated by estrogen. Animal studies have shown that both estrogen and tamoxifen elevate T3 and T4 levels while promoting thyroid follicular cell proliferation.6 Additionally, the HPT axis undergoes adaptive changes with aging to counteract various stressors, including chronic inflammation, malnutrition, and circadian rhythm disruption.8 In aged mouse models, decreased DIO2 expression and increased Tshb (encoding TSH β-subunit) levels were observed,9 consistent with an age-related decline in thyroid follicular cell sensitivity to thyroid hormone (TH) negative feedback.
Previous studies have shown that OSA is closely associated with hypothyroidism. However, other studies have demonstrated that the occurrence and severity of OSA are unrelated to thyroid function.10 Since previous studies on the relationship between OSA and the thyroid gland have been inconclusive, we expanded the sample size across 10 years and conducted age stratification. Our study revealed that OSA progression may promote an increase in thyroid hormone levels, especially serum free triiodothyronine (FT3); however, this effect was not observed in the elderly population. In the whole population, average transcutaneous oxygen saturation at night (mean SpO2) was associated with thyroid nodules. Based on previous studies and the exploratory work conducted by our research group, we propose that thyroid function may be affected by not only age but also sex.11–13 Moreover, the volume of the thyroid gland is related to the occurrence of OSA. Previous studies have suggested that large goiters present in some patients with hypothyroidism alone can cause pharynx occlusion and lead to OSA.14 However, previous studies have primarily focused on the impact of massive goiter on OSA, without addressing physiological thyroid hypertrophy or including the thyroid isthmus in comparative analyses. In addition, CIH caused by OSA may be related to the increased occurrence rate of lung nodules, thyroid nodules, and carotid plaques.15 This finding reveals a previously understudied association between OSA and thyroid morphological changes. To address limitations in prior work, we expanded our cohort with age- and sex-stratification and comprehensive thyroid morphology assessments, enabling deeper exploration of OSA-thyroid relationships.
Methods
Study Design and Subjects
The present study enrolled 3,767 patients diagnosed with OSA and admitted to the Department of Otorhinolaryngology—Head and Neck Surgery of the Second Affiliated Hospital of Xi’an Jiaotong University between 2012 and 2023. After applying the inclusion and exclusion criteria outlined in Figure 1, 1,102 patients with complete data were included. The inclusion criteria were as follows: (1) age was ≥18 years old, (2) patients with thyroid hormone test results, (3) patients who have undergone overnight polysomnography (PSG) examination, (4) no previous continuous positive airway pressure (CPAP) or surgical treatment. The exclusion criteria were as follows: (1) patients with neuromuscular diseases (including sublingual nerve paralysis), (2) patients with severe cardiopulmonary disease, severe liver and kidney dysfunction, and malignant tumors cannot cooperate with treatment, (3) pregnancy, (4) newly thyroid dysfunction, (5) incomplete baseline data. All eligible patients completed PSG and thyroid related indicators.
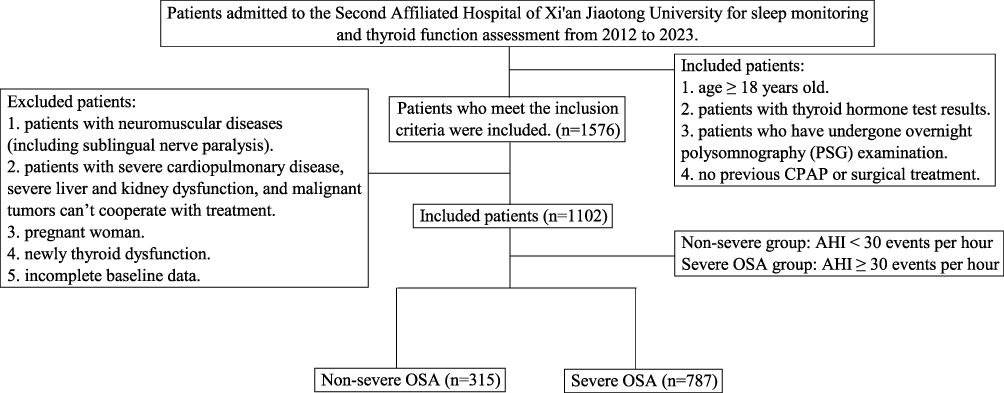 |
Figure 1 Summary of patient inclusion. |
The study protocol complied with the ethical guidelines of the 1975 Declaration of Helsinki. It was approved by the ethics committee of the Second Affiliated Hospital of Xi’an Jiaotong University (approval no. 2022e1417). And moreover, patients who in this study afforded informed consent.
Data Elements
Thirty related clinical parameters are collected, and overall the 30 candidate variables included were as follows: (1) demographic characteristics, including, gender, age, body mass index (BMI), history of hypertension, history of diabetes, (2) lifestyle habits, including, smoking and drinking, (3) OSA related medical history and indicators, including, apnea hypopnea index (AHI), the average transcutaneous oxygen saturation at night (mean SpO2), the lowest transcutaneous oxygen saturation at night (lowest SpO2). (4) thyroid function related indicators, including, serum thyroid stimulating hormone (TSH) (mIU/L), FT3 (pmol/L), serum free thyroxine (FT4) (pmol/L), TT3 (nmol/L), TT4 (nmol/L), thyroid globulin antibodies (Anti-TG) (IU/mL), thyroid peroxidase antibodies (Anti-TPO) (IU/mL), reverse triiodothyronine (RT3) (ng/dL), (5) thyroid morphology related indicators, including, the results of thyroid nodules, the diameter of the left-inferior thyroid artery (L-ITA) (mm), left max-blood flow velocity (BFV) (cm/s), left min-BFV (cm/s), left-blood flow resistance index (L-RI), the diameter of the right-inferior thyroid artery (R-ITA) (mm), right max-BFV (cm/s), right min-BFV (cm/s), right-blood flow resistance index (R-RI), thyroid volume (mL), thyroid isthmus length (mm).
Polysomnography
PSG was used to diagnose and group the patients. All enrolled patients were monitored by PSG overnight in the Department of Otolaryngology—Head and Neck Surgery Sleep Center’s Sleep Laboratory at the Second Affiliated Hospital of Xi’an Jiaotong University or in their homes with portable sleep monitors (the equipment is classified as a Type III device certified by the American Academy of Sleep Medicine). Each recording was meticulously evaluated by certified clinical polysomnographers, who analyzed various parameters, such as electroencephalogram, electrooculogram, electromyogram, electrocardiogram, nasal and oral airflow recordings, oxygen saturation levels, thoracic movements, and muscle activity. The AHI was utilized to assess the severity of sleep apnea and served as the primary parameter to differentiate between the two groups according to the frequency of apnea and hypopnea events. When the AHI was <30 events per hour, the patients were assigned to the non-severe group; when the AHI was ≥30 events per hour, the patients were assigned to the severe OSA group.16
Thyroid Morphology
Data related to thyroid morphology were measured by an experienced clinician using Doppler ultrasound, and thyroid volume was calculated as V=0.479 × a × b × c/1000,17 where V is the volume of the thyroid gland, expressed as mL; a is the length of each lobe of the thyroid gland, expressed in mm; b is the width of each lobe of the thyroid gland, expressed in mm; and c is the thickness of each lobe of the thyroid gland, expressed in mm.
Statistical Analysis
All analyses were performed with PASW Statistics 18 Origin 2024b, and G*power (3.1.9.7). The participants were divided into non-severe and severe OSA groups according to the standards described above. The relationships between PSG findings and other variables were examined through univariate and multivariate logistic regression analyses. Because the data did not conform to a normal distribution, the Mann‒Whitney U, Fisher’s exact, and Wilcoxon rank–sum tests were used to explore whether the components differed. Exploratory subgroup analyses were performed with a Bonferroni-adjusted significance threshold to account for multiple testing. The power analysis was determined through post-hoc power analysis, with effect sizes interpreted as follows: r=0.3 (small), r=0.5 (medium), and r=0.8 (large) according to conventional benchmarks in behavioral research.18 The effect size for the nonparametric rank-sum test was calculated using the formula |r| = Z/√N, where Z is the standardized test statistic and N is the total sample size.19 Numerical variables are presented as median (interquartile range, IQR), and categorical variables are presented as numbers (n) and proportions (%). Spearman correlation was used to explore the correlation between variables, and multiple linear regression was used to determine the relationship between the filtered variables. A test level α of 0.05 was used to determine significance.
Results
Demographic Characteristics
After screening (Figure 1), 1,102 patients met the inclusion criteria. We conducted a preliminary analysis of their demographic characteristics (Table 1). There were significant differences in sex, age, and BMI between the severe (n=787) and the non-severe (n=315) OSA groups (p < 0.05). There were no significant differences in their history of diabetes, hypertension, smoking, or drinking. Compared with patients in the non-severe group, more severe OSA patients were male; severe OSA patients were also younger, and had a higher BMI.
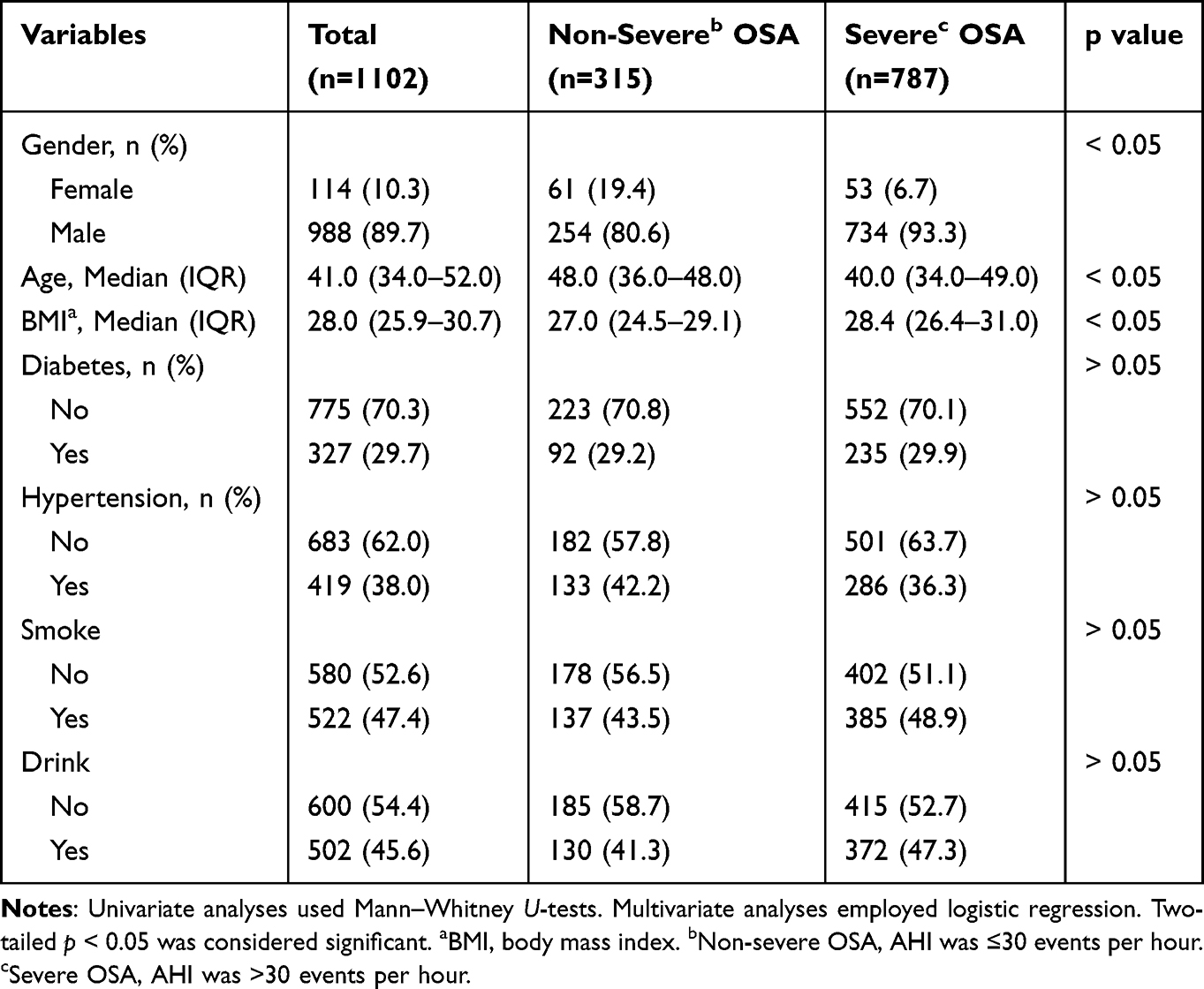 |
Table 1 Demographic and Clinical Characteristics (N=1102) |
Thyroid Function
Some patients had incomplete thyroid function test data; thus, 867 patients with complete data were included in the primary analysis. First, we explored the relationship between OSA and thyroid function. There were significant differences in FT3, TT3, and RT3 levels between the severe OSA and non-severe OSA groups (p < 0.05); however, there were no significant differences in FT4, TT4, TSH, anti-TPO, or anti-TG levels (all p > 0.05) (Table 2).
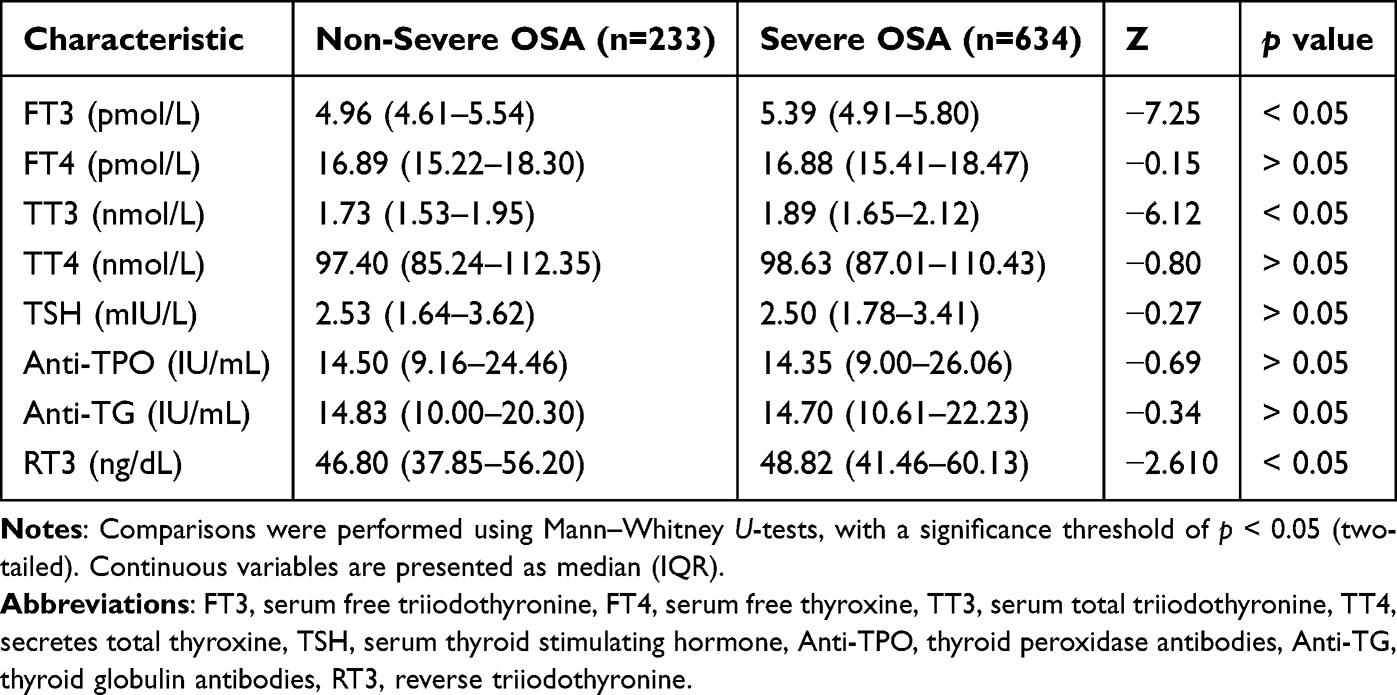 |
Table 2 Thyroid Function Evaluation Characteristics of the Different Groups (N=867) |
In addition to grouping patients according to OSA severity, we also grouped patients according to sex and age. In the male population (n=788), FT3, TT3, and RT3 were increased in the severe OSA group versus the non-severe group (p < 0.05) (Table 3). The trend in the male population was the same as that in the whole population analysis. However, in the female population (n=79), there were no significant differences in any of the thyroid function parameters (all p > 0.05) (Table 4). The patients were categorized into two groups: a nonelderly group, comprising individuals younger than 60 years of age, and an elderly group, encompassing those aged 60 years and older. In the nonelderly population (n=781), there were significant differences in FT3 and TT3 levels between the severe and non-severe OSA groups (p < 0.05); however, there were no significant differences in FT4, TT4, TSH, Anti-TPO, Anti-TG, or RT3 levels (all p > 0.05) (Table 5). In the elderly population (n=86), only RT3 demonstrated a significant difference between the two groups (p < 0.05) (Table 6).
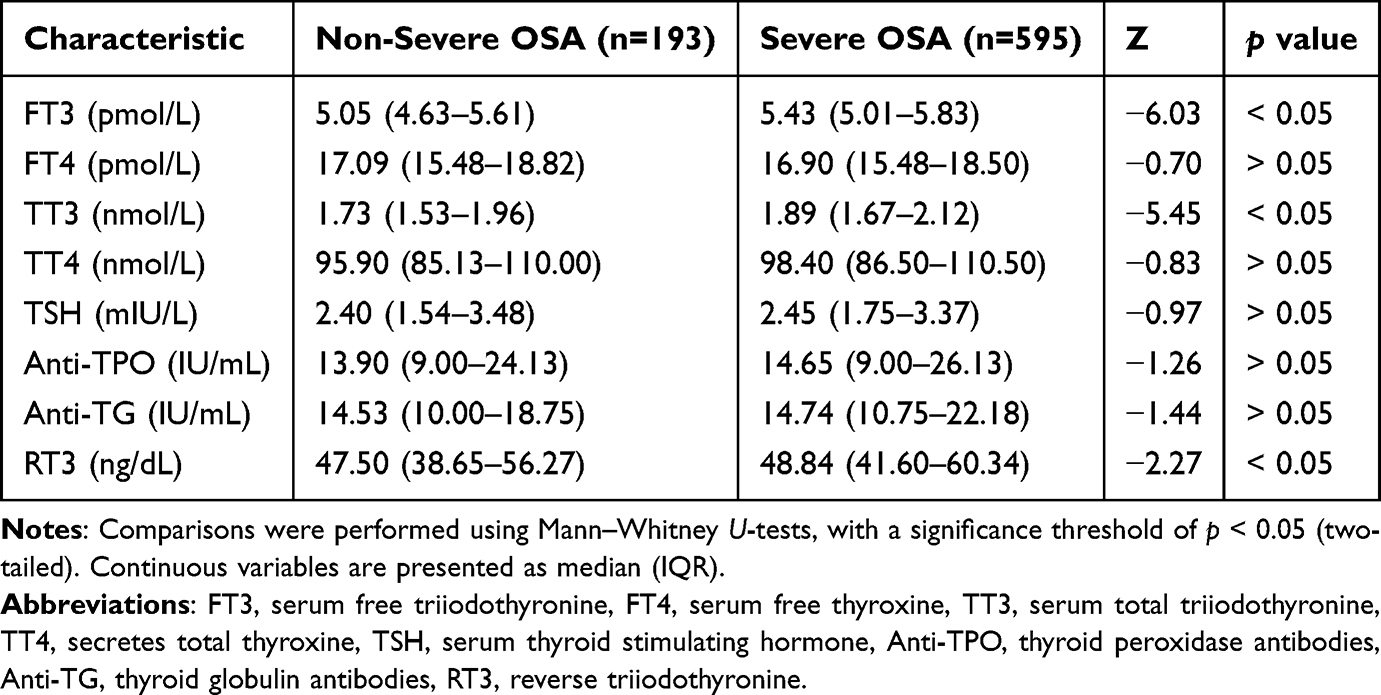 |
Table 3 Thyroid Function Evaluation Characteristics in the Male Population of the Different Groups (N=788) |
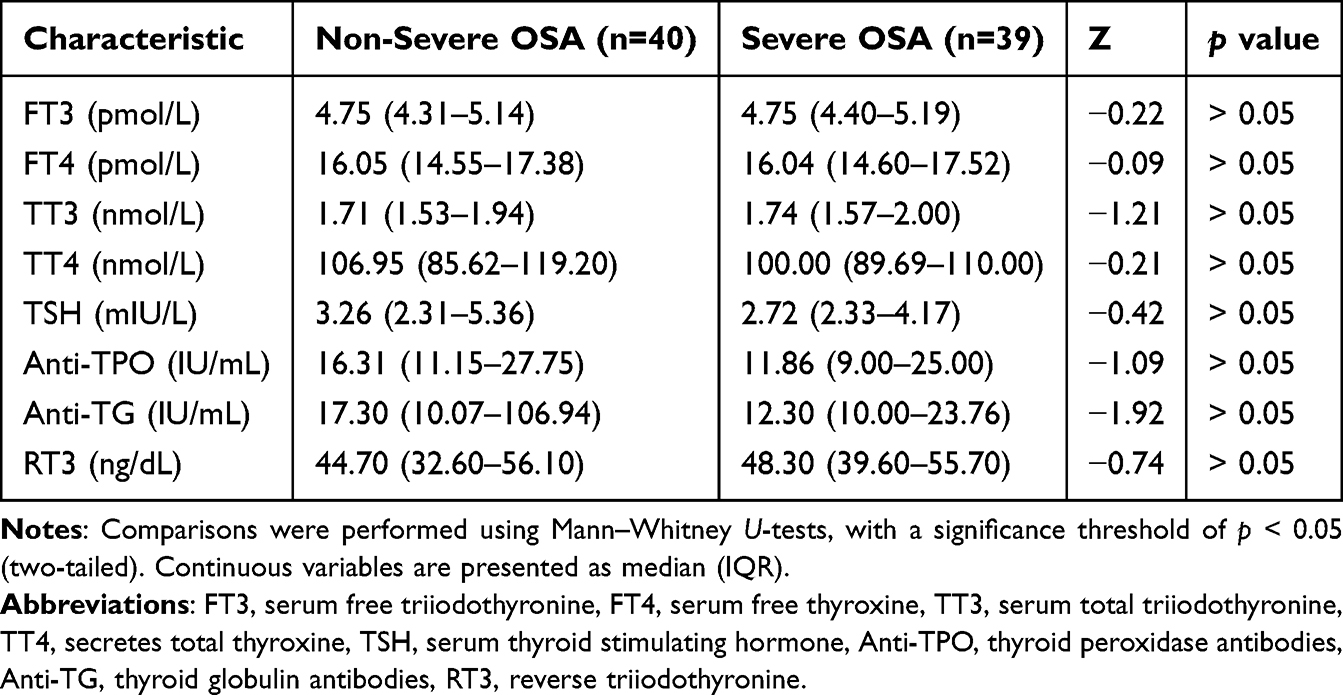 |
Table 4 Thyroid Function Evaluation Characteristics in the Female Population of the Different Groups (N=79) |
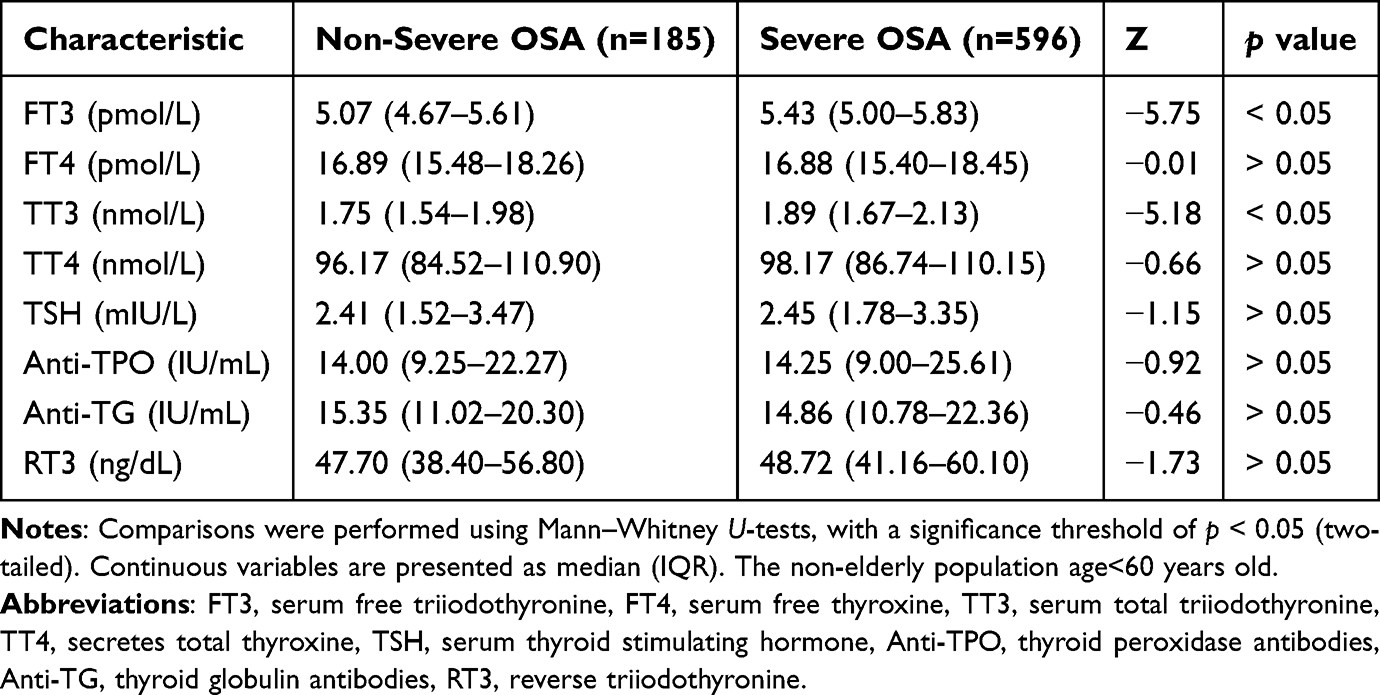 |
Table 5 Thyroid Function Evaluation Characteristics in the Non-Elderly Population of the Different Groups (N=781) |
 |
Table 6 Thyroid Function Evaluation Characteristics in the Elderly Population of the Different Groups (N=86) |
It should be noted that to mitigate potential errors arising from multiple testing, we applied Bonferroni correction across all subgroups (Supplementary Tables 1–6). Following this adjustment, the previously observed significant association between RT3 and OSA in various populations was no longer evident. This finding suggests that a more cautious interpretation of these results may be warranted. Post-hoc power calculations revealed sufficient statistical power (>50%) to detect clinically meaningful effects for both FT3 and TT3 in all demographic subgroups. However, the association involving RT3 remained underpowered despite reaching nominal significance (Supplementary Tables 9–12).
Thyroid Morphology
In addition, we measured thyroid morphology using Doppler ultrasound. All patients underwent thyroid sonography, and 383 patients had accurate lobe values for calculating thyroid volumes. The inferior thyroid artery related variables were measured in 77 patients by experienced clinicians in the Department of Ultrasound of our hospital. Analyses stratified by age and sex were not performed because of the small sample size.
There were no differences in the occurrence of thyroid nodules between the severe and non-severe OSA groups (all p > 0.05) (Table 7). Moreover, the thyroid volume and thyroid isthmus lengths were greater in the severe OSA group than in the non-severe OSA group (p < 0.05) (Table 8).
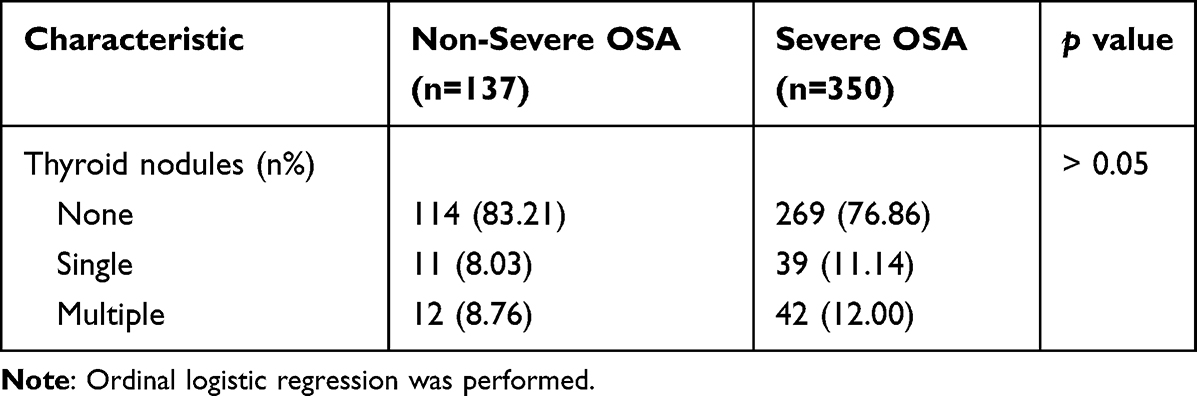 |
Table 7 Thyroid Nodules in the Severe and Non-Severe OSA Groups (N=487) |
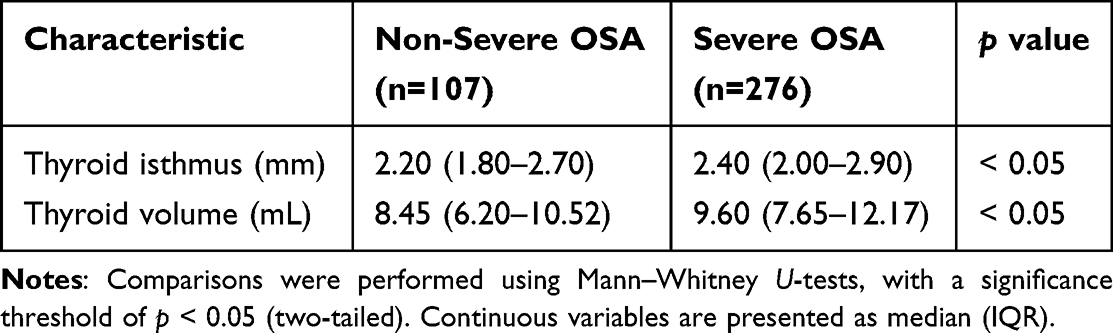 |
Table 8 Thyroid Isthmus and Volume in the Severe and Non-Severe OSA Groups (N=383) |
We then assessed the inferior thyroid artery related variables in the bilateral thyroid lobes in all patients, revealing significant differences in the inferior thyroid artery, max-BFV, and thyroid volume between the bilateral thyroid lobes. Compared with the left lobe, the right lobe demonstrated a wider vessel diameter in the inferior thyroid artery, a faster maximum BFV, and a larger volume (p < 0.05). The remaining parameters did not differ significantly (all p > 0.05) (Table 9). Furthermore, the severe OSA group demonstrated a wider L-ITA vessel diameter and a lower left lobe RI in the thyroid gland (p < 0.05). No significant differences were found in the remaining parameters (all p > 0.05) (Table 10).
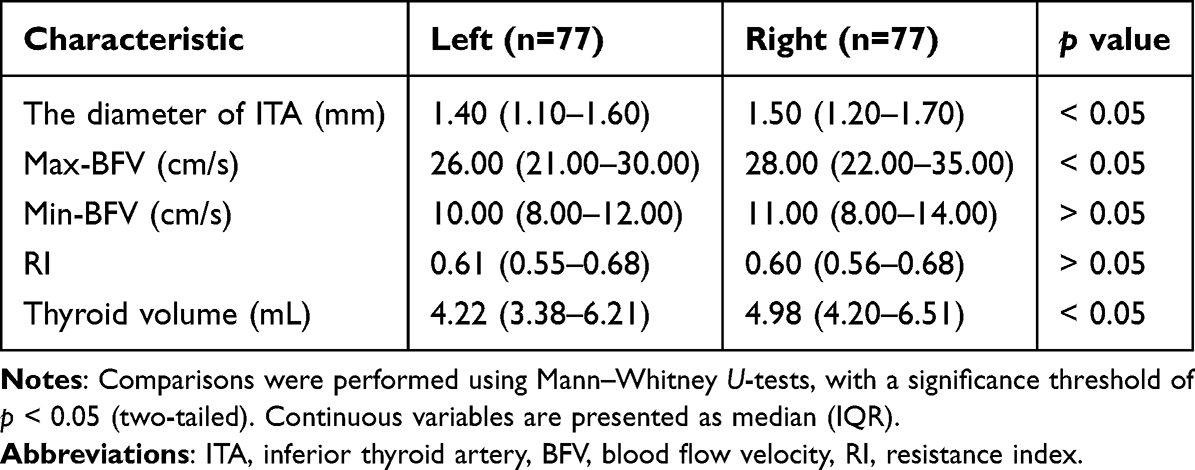 |
Table 9 Comparison of Bilateral Thyroid Lobes (N=77) |
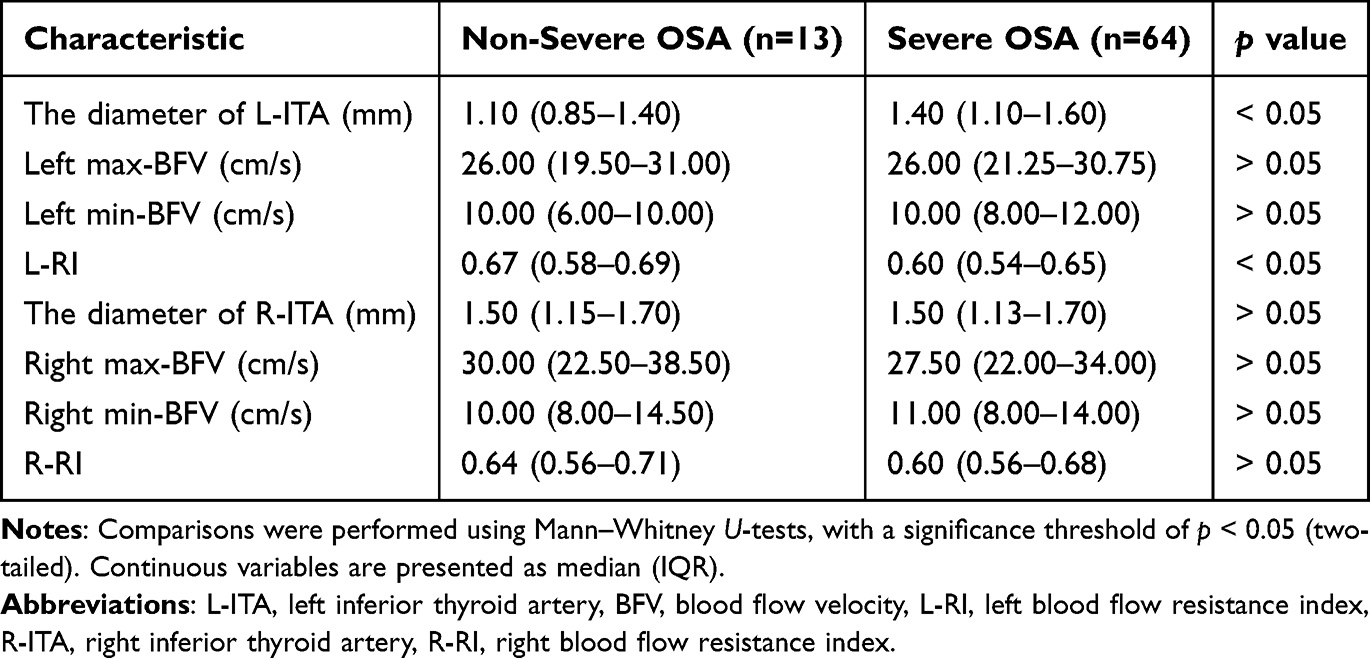 |
Table 10 Inferior Thyroid Artery Related Variables in the Severe and Non-Severe OSA Groups (N=77) |
Consistent with the investigation of OSA-thyroid function relationships, Bonferroni correction was implemented to control for type I error inflation in analyses of thyroid morphology-related subgroups (Supplementary Tables 7 and 8). Post-adjustment, the association between thyroid volume and OSA retained statistical significance, whereas other morphological correlations did not. Post-hoc power analysis revealed inadequate statistical power (<50%) for all thyroid morphology metrics (volume, isthmus thickness, and inferior thyroid artery parameters) (Supplementary Tables 13 and 14). These results indicate that a more conservative interpretation of thyroid morphology findings may be warranted.
Exploration of the Correlation of Variables and Regression Analysis
Based on the above analysis, we preliminarily explored the correlations among several variables to demonstrate that regression analysis is necessary. In patients with complete data, there were significant correlations between FT3-TT3 (r=0.583, p < 0.05), RT3-′L-TIA′ (r=0.394, p < 0.05), RT3-lowest SpO2 (r=−0.269, p < 0.05), thyroid volume-lowest SpO2 (r=−0.234, p < 0.05), AHI-mean SpO2 (r=−0.613, p < 0.05), AHI-lowest SpO2 (r=−0.706, p < 0.05), mean SpO2-lowest SpO2 (r=0.700, p < 0.05) (Figure 2). No obvious correlations were observed for the remaining variables.
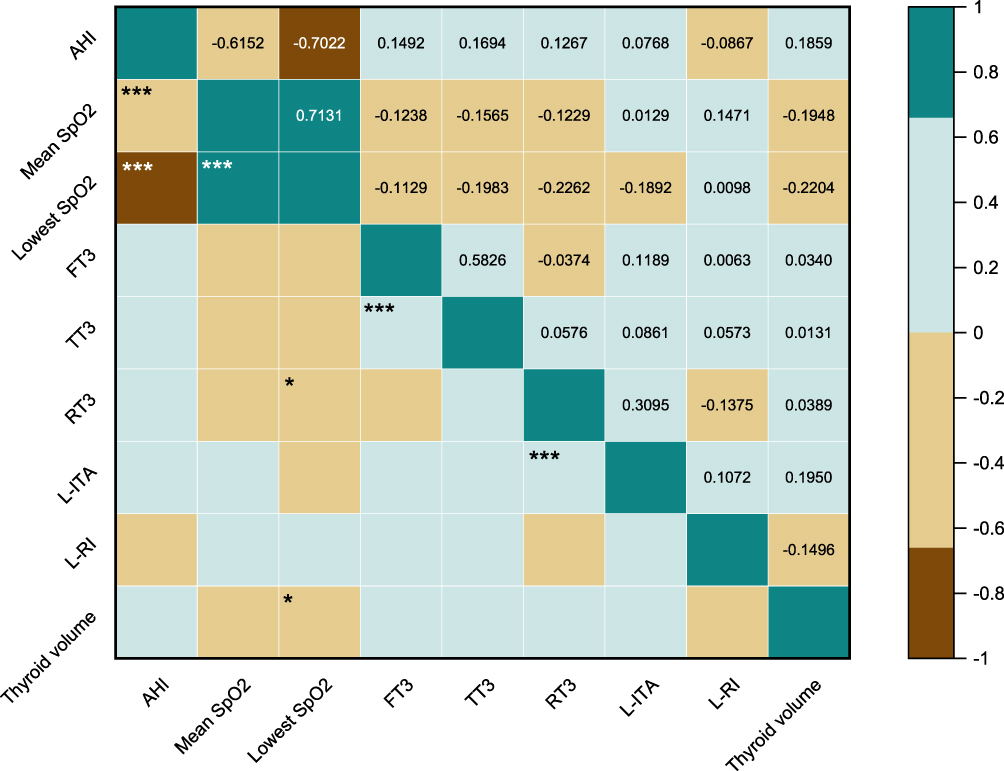 |
Figure 2 Correlation among FT3, TT3, RT3, L-ITA, L-RI, thyroid volume, AHI, mean SpO2 and lowest SpO2. Variables were analyzed using Spearman correlation. Significant correlations are indicated with asterisks: *p < 0.05, ***p < 0.001. Abbreviations: AHI, apnea hypopnea index; mean SpO2, average transcutaneous oxygen saturation at night; lowest SpO2, the lowest transcutaneous oxygen saturation at night; FT3, serum free triiodothyronine; TT3, serum total triiodothyronine; RT3, reverse triiodothyronine; L-ITA, left inferior thyroid artery; L-RI, left blood flow resistance index. |
Combining the above results, we explored the linear relationships between variables. Linear regression results indicated that FT3, TT3, RT3, L-ITA, L - RI, and thyroid volume were linearly correlated with the AHI (Figure 3).
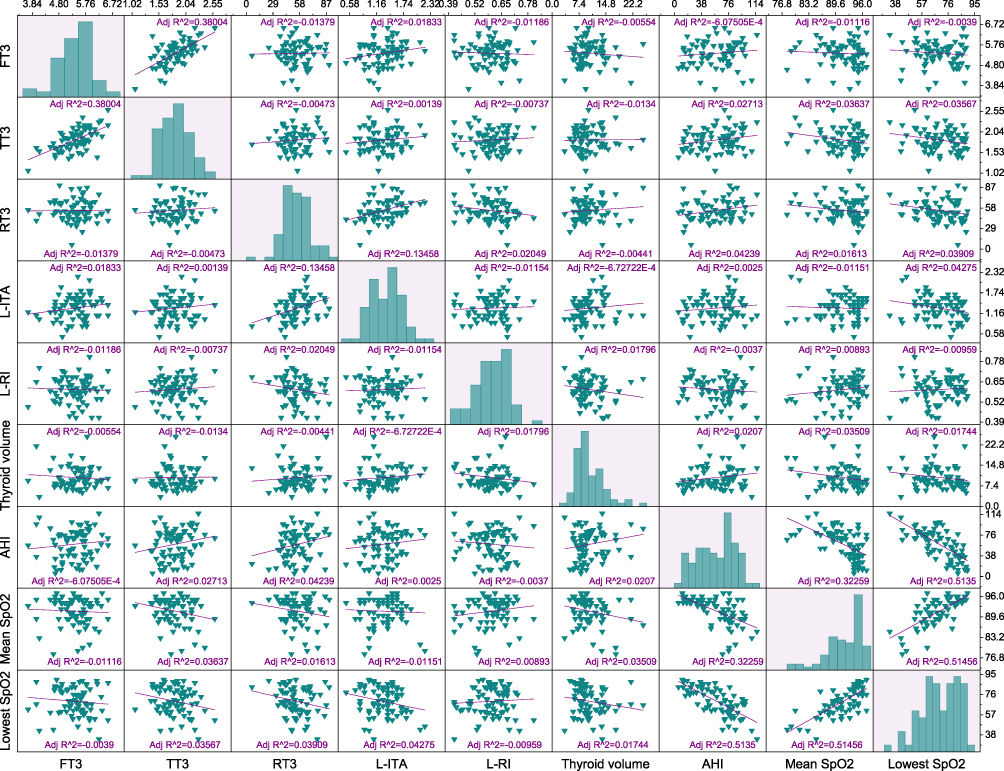 |
Figure 3 Correlation among FT3, TT3, RT3, L-ITA, L-RI, thyroid volume, AHI, mean SpO2 and lowest SpO2. Multivariate associations between continuous variables were assessed using rank-based regression analysis and visualized with scatter plots. Correlation strength is reported as coefficient (adjusted R2). Abbreviations: AHI, apnea hypopnea index; mean SpO2, average transcutaneous oxygen saturation at night; lowest SpO2, the lowest transcutaneous oxygen saturation at night; FT3, serum free triiodothyronine; TT3, serum total triiodothyronine; RT3, reverse triiodothyronine; L-ITA, left inferior thyroid artery; L-RI, left blood flow resistance index. |
After the baseline data (including sex, age, and BMI) were supplemented, a linear regression equation was established: y=212.161–28.517x1+0.007x2+2.525x3–0.771x4-0.949x5–5.586x6–0.989x7+0.126x8–5.220x9–33.635x10–0.396x11 (Adj. R2=0.66, Pearson’s r=0.82, p < 0.05). The residual plot is shown in (Figure 4a–k) as a random distribution. The residual plot did not vary with the predicted value; thus, it met the homogeneity of variance. Finally, we generated an independent variable into a linear regression equation to reach the predicted AHI (AHI-pre). The equations fit well with the real AHI (r=0.82, Adj. R2=0.66) (Figure 4l).
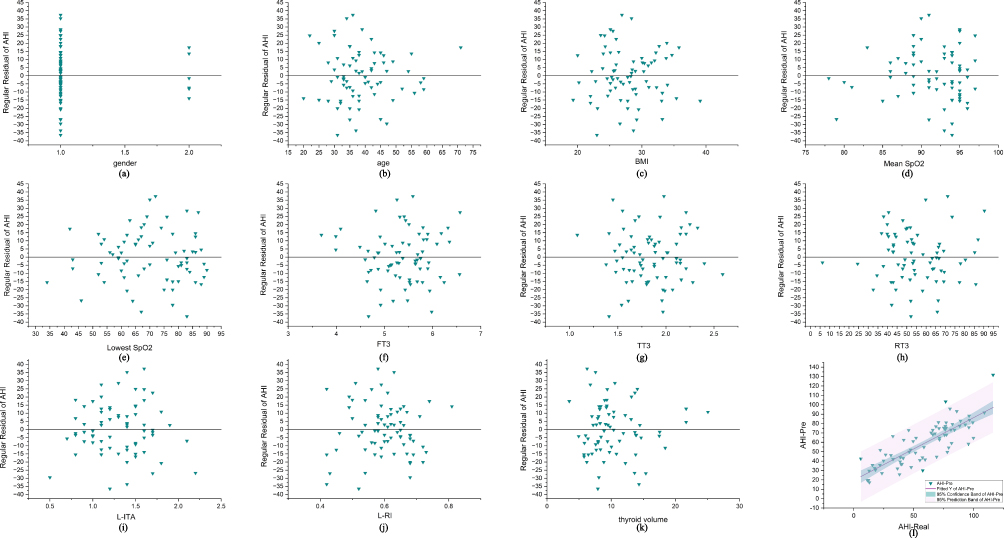 |
Figure 4 Regular residual of linear regression for the relationship between AHI and gender, age, BMI, mean SpO2, lowest SpO2, FT3, TT3, RT3, L-ITA, L-RI, thyroid volume. Multiple linear regression was performed to assess specific associations between variables, adjusting for potential confounders (eg, age, sex, BMI). Model fit was evaluated using adjusted R2, and regression diagnostics included residual analysis (a–k) and predicted vs real AHI plots (l). Abbreviations: AHI, apnea hypopnea index; BMI, body mass index; mean SpO2, average transcutaneous oxygen saturation at night; lowest SpO2, the lowest transcutaneous oxygen saturation at night; FT3, serum free triiodothyronine; TT3, serum total triiodothyronine; RT3, reverse triiodothyronine; L-ITA, left inferior thyroid artery; L-RI, left blood flow resistance index; AHI-Pre, predicted AHI; AHI-Real, real AHI. |
Discussion
In this study, we investigated the relationships among OSA, thyroid function, and thyroid morphology. We evaluated 1,102 patients admitted to our hospital from 2012 to 2023. Compared with the patients in the non-severe OSA group, more patients in the severe group were men, were younger, and had a higher BMI. Most of our results were consistent with previous findings; however, the relationship between age and OSA contradicts previous research conclusions.11,12 Our study suggested that more younger people experience OSA. The median age of the patients was 41 years. This finding might be because young and middle-aged people are more willing to seek medical treatment than older adults.
The relationship between thyroid function and OSA in our study was associated with increased thyroid hormone levels, contradicting the findings of most previous studies.14,20,21 In this study, the FT3, TT3, and RT3 levels in the severe OSA group were greater than those in the non-severe OSA group. The trend in male was the same as that in the population, and the elderly population partially matched the nonelderly population; however, no significant differences were found in female. One study investigated the effects of hormone levels in the hypothalamic–pituitary–thyroid axis and depression in patients with OSA,22 and the results showed that the FT3 and FT4 levels in the severe hypoxia group were greater than those in the control group. In addition, in a study on thyroid dysfunction and sleep disorders, the authors suggested that elevated thyroid hormone levels might result in sleep maintenance difficulties and excessive daytime sleepiness, potentially attributed to tremors induced by heightened hormone levels that exacerbate the challenges in maintaining sleep.23 However, our previous study revealed that OSA progression may be related to increased thyroid hormone levels. The underlying mechanism may be associated with oxidative stress and inflammatory reactions, which are also involved in the pathogenesis of many metabolic disorders.2 The results of our current study support those of our previous study, providing stronger evidence for the previous conclusion. It is well known that thyroid hormone mainly exists in the form of TT4 in the human body, which can be converted into TT3 and RT3 in peripheral tissues. When there is a greater need for thyroid hormone conversion from TT4 to TT3 rather than RT3, the ratio of TT4 to RT3 increases, such as during stress, pregnancy, and metabolic disorders.24
OSA is related to oxidative stress,4 which concurrently plays a physiological role in normal thyroid hormone homeostasis through regulated ROS signaling.25 To oxidative damage, thyroid hormone synthesis by TPO requires ROS (eg, H2O2) for iodide oxidation, making the gland uniquely vulnerable.26 The thyroid gland mitigates oxidative stress by activating the Keap1/Nrf2 signaling cascade, a key regulator of antioxidant defense.27 Furthermore, studies have consistently demonstrated significant oxidative damage to membrane lipids in patients with hyperthyroidism.28 By integrating these findings, we hypothesize that CIH, a defining characteristic of OSA, induces systemic oxidative stress. This stress disrupts the normal physiological function of thyroid follicular cells, potentially leading to elevated levels of thyroid hormones. Consequently, this cellular dysfunction may explain the observed increases in FT3, TT3, and RT3 among severe OSA patients in our study. One study on the pathophysiology of neuroendocrine regulation in OSA patients suggested that patients with severe OSA had decreased TT4 concentrations and decreased TSH activity, indicating that OSA may cause neuroendocrine system disorders.29 We speculate that the correlation between OSA and TH during certain periods results from thyroid cell damage rather than hyperfunction.2 In our study, TT4 and TSH levels decreased in the severe OSA group; however, the differences were not significant. This finding might be because the total concentrations of TT4 and TSH in the human body are large and do not change significantly.
In a study on thyroid hormones and aging, the authors suggested that in the elderly population, most studies have demonstrated that FT3 decreases in an age-dependent manner, whereas FT4 levels remain relatively unchanged and RT3 levels increase with increasing age.30 This finding is supported by our study, which revealed that RT3 is elevated in the elderly population with severe OSA, whereas other thyroid hormone levels tend to be unchanged.
Moreover, thyroid hormones are potentially affected by estrogen. One study demonstrated lower FT4 and higher FT3 levels among euthyroid postmenopausal women with more visceral adipose tissue.13 In an animal experiment, TT4 and TT3 levels were improved by estrogen. Therefore, the differences in thyroid hormone changes between women and the total population may be due to the effect of estrogen and may also be related to the small number of women with severe OSA in our study.
OSA may lead to vascular endothelial cell injury by inducing an inflammatory response, resulting in arterial morphology and function changes.3 Previous research revealed that TSH positively correlates with carotid artery intima-media thickness (IMT), whereas FT3 levels negatively correlate with IMT. The IMT and apnea-hypopnea index were also positively correlated.4 The inferior thyroid artery, as one of the main blood supply arteries of the thyroid gland, may also have undergone similar changes, but this cannot explain the diameter of the left inferior thyroid artery in the severe OSA group in our study. We speculate that this may be related to sympathetic activation induced by chronic intermittent hypoxia, leading to contraction of the peripheral region and relaxation of major arteries.31 This has not been mentioned in previous studies.
The RI index is used to evaluate the resistance and compliance of blood vessels, and a higher RI index indicates narrowing of the anterior vessel or increased resistance to vascular flow. The RI index has been frequently used in previous studies to assess neonatal umbilical and cerebral blood flow to identify high-risk neonates32 or to assess acute kidney injury,33 It can also be used to assess coronary blood flow microcirculation and infer the occurrence of benign and malignant nodules and Graves’ disease in thyroid studies.34–36 However, this measure has not previously been used to assess vascular changes that may be caused by OSA. In our study, we assessed the effect of chronic intermittent hypoxia on blood vessels. The RI was reduced in the left side of the inferior thyroid artery in the severe OSA group. This finding is consistent with the widening diameter of the inferior thyroid artery described above. These findings may have potential clinical implications, suggesting that the RI could serve as a novel biomarker for assessing vascular health in OSA patients. Further validation studies are warranted to establish its diagnostic utility. However, due to the small sample size, whether this result can be extrapolated to the OSA population needs further investigation.
In the comparison of the bilateral thyroid lobes, we suspected that the right inferior thyroid artery might be the dominant artery. Our study revealed that the thyroid volume and length of the thyroid isthmus were greater in the severe OSA group. An enlarged thyroid gland may also be one of the causes of OSA.14 Some scholars believe that thyroid enlargement is caused by hypothyroidism.20 Whether thyroid enlargement leads to aggravated OSA or hypoxia can lead to increased thyroid function has not yet been determined. There is insufficient evidence to support the effect of OSA on thyroid volume.37 Most patients with severe OSA have a higher BMI; thus, increased BMI may contribute to increased thyroid volume. Another speculation is that an increase in the thyroid artery diameter and a decrease in the BFV suggest an increase in thyroid blood flow, potentially affecting thyroid gland volume;38 however, this hypothesis needs further verification. Previous studies did not compare the bilateral lobes of the thyroid separately or simultaneously analyze thyroid function, morphology, or OSA. Based on previous research and our research, we added more indices associated with thyroid volume and blood flow and compared the bilateral thyroid lobes. The length of the thyroid isthmus and the thyroid volume increased in the severe OSA group, the diameter of the L-ITA also widened, and the L-RI decreased. Combined with the finding of increased thyroid hormone levels in the severe OSA group mentioned above, we hypothesize that the change in thyroid volume in the severe OSA group may be related to BMI and blood flow, and the greater thyroid volume in the severe OSA group may also explain the greater thyroid hormone levels.
We conducted a retrospective study with a substantial sample size, incorporating clinical data spanning the last 10 years, to delve into the intricate relationships among OSA, thyroid function, and morphology. This study supports previous findings and introduces novel metrics for further analysis. The advantage of our study is that we explored the relationships among thyroid function, thyroid morphology, and OSA simultaneously, and the data were analyzed after stratification by sex and age. Our study analyzed the clinical data of 1,102 patients over nearly 11 years, representing a larger sample size than that assessed in previous studies. However, our study still has several limitations. First, this was a single-center retrospective study. Second, there are more accurate ways to assess thyroid ultrasound data, but we did not use them due to a lack of conditions. Third, although we screened a large sample of 1,102 patients among 3,767 across the past decade, only 77 patients had complete PSG, thyroid function, and thyroid ultrasound data. Our investigation into the association between OSA and thyroid characteristics was exploratory in nature. Following Bonferroni correction for multiple comparisons across subgroups, some previously observed significant differences were no longer statistically significant. Post-hoc power analysis revealed suboptimal statistical power (<50%) for all thyroid morphology measurements, suggesting these findings require cautious interpretation. Nevertheless, these findings may still suggest potential underlying relationships between OSA and both thyroid function and morphology, which warrant further validation through large-scale prospective studies. Consequently, in the future, we will collect more thyroid ultrasound data. Finally, the causal relationships between OSA and thyroid disease and the underlying mechanisms remain unclear. In the future, we aim to expand the sample size, include multicenter studies, and utilize animal and cell experiments to validate the conclusions and hypotheses of this study, while continually delving into the intricate interaction mechanism between OSA, thyroid function, and morphological changes.
However, it is crucial to highlight that although we have investigated associations between OSA and thyroid characteristics, our study design does not allow for the establishment of causal relationships between these variables. The observed interactions might be bidirectional, and more conclusive evidence of causality would necessitate rigorously designed prospective studies with longitudinal follow-up.
Conclusions
This study revealed a significant association between thyroid function and morphology and OSA severity. Notably, among male and nonelderly populations, severe OSA was significantly more strongly associated with elevated levels of FT3, TT3, and RT3 than non-severe OSA. Conversely, no marked differences in thyroid function were observed in females between the two OSA severity groups, suggesting a potential estrogen-mediated effect. Among the elderly individuals, only RT3 levels were elevated in severe OSA patients, which may be related to the influence of age. Furthermore, this study revealed increased thyroid volume and thyroid isthmus length in individuals with severe OSA, although the precise causal relationship between OSA severity and thyroid enlargement remains elusive. In addition, this investigation explored the application of the RI as a tool to assess the vascular consequences of chronic intermittent hypoxia, providing potential evidence that the R-ITA demonstrates a significant contribution to the thyroid blood supply, with its diameter serving as an indicator of this effect. In summary, the findings underscore the intricate relationship between OSA severity and thyroid function, with notable sex- and age-related variations, while also introducing the potential of RI measurements to inform vascular health in OSA patients. In the future, we will continue to conduct animal experiments and cell-level exploration to explore the intricate relationship between OSA and thyroid morphology and function. Animal models can provide a controlled environment to observe the physiological and pathological changes associated with OSA, while cell-level experiments can offer insights into the molecular mechanisms that underlie these changes. This comprehensive approach will help us better understand the interplay between OSA and thyroid health, ultimately leading to more effective diagnostic and therapeutic strategies.
Abbreviations
AHI, apnea hypopnea index; Anti-TG, thyroid globulin antibodies; Anti-TPO, thyroid peroxidase antibodies; BFV, blood flow velocity; BMI, body mass index; CIH, chronic intermittent hypoxia; CPAP, continuous positive airway pressure; FT3, serum free triiodothyronine; FT4, serum free thyroxine; ITA, inferior thyroid artery; IMT, intima-media thickness; lowest SpO2, lowest transcutaneous oxygen saturation at night; mean SpO2, average transcutaneous oxygen saturation at night; OSA, obstructive sleep apnea; PSG, polysomnography; RI, resistance index; RT3, reverse triiodothyronine; TH, thyroid hormone; TSH, serum thyroid stimulating hormone; TT3, serum total triiodothyronine; TT4, secretes total thyroxine.
Data Sharing Statement
Data are available on reasonable request. The datasets generated and analyzed during this study are available from the first author (YX) upon reasonable request. Data sharing will comply with institutional and ethical regulations.
Ethics Approval
This retrospective study was approved by the Ethics Committee of the Second Affiliated Hospital of Xi’an Jiaotong University (approval no. 2022e1417). The procedures used in this study adhered to the tenets of the Declaration of Helsinki.
Acknowledgments
We wish to thank all who volunteered to participate in this study.
Author Contributions
YX: Conceptualization, Methodology, Writing original draft. HZ: Conceptualization, Methodology, Writing review and editing. ZC: Software, Writing review and editing, Data curation. YZ: Investigation, Resources, Writing review and editing. CL: Investigation, Resources, Writing review and editing. LY: Investigation, Resources, Writing review and editing. SZ: Investigation, Resources, Writing review and editing. YS: Investigation, Resources, Writing review and editing. XN: Investigation, Resources, Writing review and editing. LM: Formal analysis, Writing review and editing, Validation. YY: Writing review and editing, Software. YZ: Writing review and editing, Software. ZW: Investigation, Resources, Writing review and editing. HL: Funding acquisition, Writing review and editing, Resources. XR: Conceptualization, Methodology, Supervision, Funding acquisition, Writing review and editing, Project administration. YS: Conceptualization, Methodology, Supervision, Writing review and editing, Project administration. XR and YS directed the research, XR is the guarantors of the paper who takes full responsibility for the integrity of the work, from its inception to the published article.
All authors have approved the submission of this manuscript to Nature and Science of Sleep and unanimously agree to take responsibility for the content, reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage, agreed to take responsibility and be accountable for the contents of the article.
Funding
This work was supported by the Free Exploration and Innovation Project of Basic Scientific Research Fund of Xi’an Jiaotong University (xzy012023119), the National Natural Science Foundation of China (grant No. 82371129, 82303887, 62076198), the Key Research and Development Program in the Social Development Field of Shaanxi, China (2020GXLH-Y005, 2021SF-286) and the General Research and Development Program in the Social Development Field of Shaanxi, China (2023-YBSF-298).
Disclosure
The authors have no competing interests to disclose.
References
1. Redline S, Azarbarzin A, Peker Y. Obstructive sleep apnoea heterogeneity and cardiovascular disease. Nat Rev Cardiol. 2023;20(8):560–573. doi:10.1038/s41569-023-00846-6
2. Shi Y, Cao Z, Xie Y, et al. Association between obstructive sleep apnea and thyroid function: a 10-year retrospective study. Sleep Med. 2023;103:106–115. doi:10.1016/j.sleep.2023.01.027
3. Kazukauskiene N, Fineberg NA, Podlipskyte A, et al. Contribution of obstructive sleep apnoea to cognitive functioning of males with coronary artery disease: a relationship with endocrine and inflammatory biomarkers. Front Neurosci. 2022;16:899597. doi:10.3389/fnins.2022.899597
4. Bozkus F, Dikmen N, Güngör G, et al. The effect of obstructive sleep apnea syndrome and hypothyroidism to intima-media thickness of carotid artery. Sleep Breath. 2017;21(1):31–36. doi:10.1007/s11325-016-1384-2
5. Peeters RP, Wouters PJ, Kaptein E, et al. Reduced activation and increased inactivation of thyroid hormone in tissues of critically ill patients. J Clin Endocrinol Metab. 2003;88(7):3202–3211. doi:10.1210/jc.2002-022013
6. Duksal F, Eren F. Evaluation of thyroid functions and obesity in obstructive sleep apnea syndrome. Rev Assoc Med Bras. 2023;69(9):e20230376. doi:10.1590/1806-9282.20230376
7. Mohawk JA, Green CB, Takahashi JS. Central and peripheral circadian clocks in mammals. Annu Rev Neurosci. 2012;35:445–462. doi:10.1146/annurev-neuro-060909-153128
8. Fliers E, Kalsbeek A, Boelen A. Beyond the fixed setpoint of the hypothalamus-pituitary-thyroid axis. Eur J Endocrinol. 2014;171(5):R197–208. doi:10.1530/EJE-14-0285
9. Luongo C, De Stefano MA, Ambrosio R, et al. Type 2 deiodinase Thr92Ala polymorphism and aging are associated with a decreased pituitary sensitivity to thyroid hormone. Thyroid. 2023;33(3):294–300. doi:10.1089/thy.2022.0472
10. Xiong J, Hu H, Huang Y, et al. Lack of associations between thyroid dysfunction and obstructive sleep apnea-hypopnea syndrome: a meta-analysis. Medicine. 2023;102(49):e36531. doi:10.1097/MD.0000000000036531
11. Jordan AS, McSharry DG, Malhotra A. Adult obstructive sleep apnoea. Lancet. 2014;383(9918):736–747. doi:10.1016/S0140-6736(13)60734-5
12. Fietze I, Laharnar N, Obst A, et al. Prevalence and association analysis of obstructive sleep apnea with gender and age differences - results of SHIP-trend. J Sleep Res. 2019;28(5):e12770. doi:10.1111/jsr.12770
13. Yang Q, Wan YH, Hu SD, et al. Associations between the levels of thyroid hormones and abdominal obesity in euthyroid post-menopausal women. Endokrynol Pol. 2020;71(4):299–305. doi:10.5603/EP.a2020.0037
14. Kuczyński W, Gabryelska A, Mokros Ł, et al. Obstructive sleep apnea syndrome and hypothyroidism - merely concurrence or causal association? Pneumonol Alergol Pol. 2016;84(5):302–306. doi:10.5603/PiAP.2016.0038
15. Ding C, Mao L, Lu Y, et al. Does obstructive sleep apnea-induced intermittent hypoxia increase the incidence of solitary pulmonary nodules, thyroid nodules, and other disorders? A retrospective study based on 750 cardiovascular disease patients. Sleep Breath. 2024;28:1553–1562. doi:10.1007/s11325-024-03036-x
16. Gottlieb DJ, Punjabi NM. Diagnosis and management of obstructive sleep apnea: a review. JAMA. 2020;323(14):1389–1400. doi:10.1001/jama.2020.3514
17. Brunn J, Block U, Ruf G, et al. Volumetrie der Schilddrüsenlappen mittels Real-time-Sonographie * 1 [Volumetric analysis of thyroid lobes by real-time ultrasound (author’s transl)]. Dtsch Med Wochenschr. 1981;106(41):1338–1340. doi:10.1055/s-2008-1070506
18. Cohen J. Students whose behaviour causes concern: role of universities. Br Med J. 2008;336:337. doi:10.1136/bmj.39456.470880.80
19. Wang JH, Stebbins A, Ferdig RE. Examining the effects of students’ self-efficacy and prior knowledge on learning and visual behavior in a physics game. Comput Educ. 2022;178.
20. Green ME, Bernet V, Cheung J. Thyroid dysfunction and sleep disorders. Front Endocrinol. 2021;12:725829. doi:10.3389/fendo.2021.725829
21. Takeuchi S, Kitamura T, Ohbuchi T, et al. Relationship between sleep apnea and thyroid function. Sleep Breath. 2015;19(1):85–89. doi:10.1007/s11325-014-0966-0
22. Liang Y, Xu JH, Li WY, et al. [The effect of hypothalamic-pituitary-thyroid axis hormone levels and depression in obstructive sleep apnea-hypopnea syndrome]. Zhonghua Jie He He Hu Xi Za Zhi. 2019;42(8):591–595. doi:10.3760/cma.j.issn.1001-0939.2019.08.006
23. Xia L, Chen G-H, Li Z-H, et al. Alterations in hypothalamus-pituitary-adrenal/thyroid axes and gonadotropin-releasing hormone in the patients with primary insomnia: a clinical research. PLoS One. 2013;8(8):e71065. doi:10.1371/journal.pone.0071065
24. Cheng SY, Leonard JL, Davis PJ. Molecular aspects of thyroid hormone actions. Endocr Rev. 2010;31(2):139–170. doi:10.1210/er.2009-0007
25. Kochman J, Jakubczyk K, Bargiel P, et al. The Influence of Oxidative Stress on Thyroid Diseases. Antioxidants. 2021;10(9):1442. doi:10.3390/antiox10091442
26. Paunkov A, Chartoumpekis DV, Ziros PG, et al. Impact of antioxidant natural compounds on the thyroid gland and implication of the Keap1/Nrf2 signaling pathway. Curr Pharm Des. 2019;25(16):1828–1846. doi:10.2174/1381612825666190701165821
27. Thanas C, Ziros PG, Chartoumpekis DV, et al. The Keap1/Nrf2 signaling pathway in the thyroid-2020 update. Antioxidants. 2020;9(11):1082. doi:10.3390/antiox9111082
28. Wang D, Feng J-F, Zeng P, et al. Total oxidant/antioxidant status in sera of patients with thyroid cancers. Endocr Relat Cancer. 2011;18(6):773–782. doi:10.1530/ERC-11-0230
29. Madaeva IM, Berdina ON, Sholokhov LF, et al. [Pathophysiological aspects of neuro-endocrine regulation system in patients with obstructive sleep apnea syndrome]. Zh Nevrol Psikhiatr Im S S Korsakova. 2018;118(4. Vyp. 2):55–59. doi:10.17116/jnevro20181184255
30. Papaleontiou M, Haymart MR. Approach to and treatment of thyroid disorders in the elderly. Med Clin North Am. 2012;96(2):297–310. doi:10.1016/j.mcna.2012.01.013
31. Lévy P, Kohler M, McNicholas WT, et al. Obstructive sleep apnoea syndrome. Nat Rev Dis Primers. 2015;1:15015. doi:10.1038/nrdp.2015.15
32. Kamel SM, Badr-Eldin RM, Arafat MM, et al. Role of transcranial Doppler in assessment of cerebral blood flow in full term neonates with extreme unconjugated hyperbilirubinemia. J Ultrasound. 2023;26(1):175–184. doi:10.1007/s40477-022-00704-0
33. Watchorn J, Huang D, Bramham K, et al. Decreased renal cortical perfusion, independent of changes in renal blood flow and sublingual microcirculatory impairment, is associated with the severity of acute kidney injury in patients with septic shock. Crit Care. 2022;26(1):261. doi:10.1186/s13054-022-04134-6
34. Camici PG, d’Amati G, Rimoldi O. Coronary microvascular dysfunction: mechanisms and functional assessment. Nat Rev Cardiol. 2015;12(1):48–62. doi:10.1038/nrcardio.2014.160
35. De Nicola H, Szejnfeld J, Logullo ÂF, et al. Flow pattern and vascular resistive index as predictors of malignancy risk in thyroid follicular neoplasms. J Ultrasound Med. 2005;24(7):897–904. doi:10.7863/jum.2005.24.7.897
36. Wang K, Yang Y, Wu Y, et al. The association between insulin resistance and vascularization of thyroid nodules. J Clin Endocrinol Metab. 2015;100(1):184–192. doi:10.1210/jc.2014-2723
37. Fister P, Gaberšček S, Zaletel K, et al. Thyroid volume changes during pregnancy and after delivery in an iodine-sufficient Republic of Slovenia. Eur J Obstet Gynecol Reprod Biol. 2009;145(1):45–48. doi:10.1016/j.ejogrb.2009.03.022
38. Fister P, Gaberšček S, Zaletel K, et al. Thyroid volume and intrathyroidal blood flow increase during pregnancy. Clin Endocrinol. 2006;65(6):828–829. doi:10.1111/j.1365-2265.2006.02657.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Independent Association of Sleep Apnea-Specific Hypoxic Burden and Sleep Breathing Impairment Index with Thyroid Function in Obstructive Sleep Apnea: A Retrospective Study
Zhou Y, Shi Y, Zhu S, Cao Z, Xie Y, Lu C, Niu X, Ma L, Wang Z, Su Y, Xia Z, Yuan Y, Yang J, Lu R, Feng Y, Ren X, Hou W
Nature and Science of Sleep 2025, 17:1543-1556
Published Date: 5 July 2025