Back to Journals » Journal of Inflammation Research » Volume 19
Association of the Systemic Inflammation Response Index with the One-Year All-Cause Mortality in Elderly Patients with Acute Coronary Syndrome: A Retrospective Cohort Study
Authors Li J ![]() , Wei W
, Wei W ![]() , Xiao L
, Xiao L ![]() , Luo N
, Luo N ![]() , Kang Y
, Kang Y ![]() , Chen L
, Chen L ![]() , Zeng Y
, Zeng Y ![]() , Zhang L
, Zhang L ![]() , Chen M
, Chen M
Received 14 January 2026
Accepted for publication 10 March 2026
Published 19 March 2026 Volume 2026:19 593688
DOI https://doi.org/10.2147/JIR.S593688
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Chengming Fan
Jiaxin Li,1,2,* Wenyan Wei,1,3,* Lu Xiao,4,* Nanbo Luo,5 Yuan Kang,6 Lujun Chen,7 Yuxuan Zeng,6 Liangqing Zhang,2,8 Min Chen1,9
1Faculty of Chinese Medicine and State Key Laboratory of Mechanism and Quality of Chinese Medicine, Macau University of Science and Technology, Macau, Macau SAR, People’s Republic of China; 2Department of Anesthesiology, The Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong, People’s Republic of China; 3Department of Geriatrics, The Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong, People’s Republic of China; 4Department of Basic Medicine, Zhuhai Campus, Zunyi Medical University, Zhuhai, Guangdong, People’s Republic of China; 5Department of Anesthesiology, Shenzhen Second People’s Hospital, The First Affiliated Hospital of Shenzhen University, Shenzhen, Guangdong, People’s Republic of China; 6The First School of Clinical Medicine, Guangdong Medical University, Zhanjiang, Guangdong, People’s Republic of China; 7Department of Cardiovascular Medicine, The Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong, People’s Republic of China; 8Department of Anesthesiology, The Second Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong, People’s Republic of China; 9Innovation Technology Research Institute, Macau University of Science and Technology (M.U.S.T.), Zhuhai, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Min Chen, Faculty of Chinese Medicine and State Key Laboratory of Mechanism and Quality of Chinese Medicine, Macau University of Science and Technology, Avenida Wai Long, Taipa, Macau, Macau SAR, 999078, People’s Republic of China, Email [email protected] Liangqing Zhang, Department of Anesthesiology, The Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong, 524000, People’s Republic of China, Email [email protected]
Purpose: This study aimed to investigate the association between the systemic inflammation response index (SIRI) and one-year all-cause mortality, as well as major adverse cardiovascular and cerebrovascular events (MACCE), in elderly patients with acute coronary syndrome (ACS).
Patients and Methods: This retrospective cohort study enrolled 963 elderly patients diagnosed with ACS at the Affiliated Hospital of Guangdong Medical University between January 2022 and December 2023, comprising those with unstable angina, non-ST elevation myocardial infarction, and ST elevation myocardial infarction. The cohort encompassed patients who underwent percutaneous coronary intervention as well as those managed conservatively, with a one-year follow-up. The primary endpoint was one-year all-cause mortality. Cox proportional hazards models were used to evaluate the association of SIRI, treated as both a continuous variable and as a categorical variable stratified by median value, with all-cause mortality and MACCE.
Results: Among 963 elderly ACS patients (median age 73; 69.5% male), 132 (13.7%) died within one year. The median SIRI value was 2.89 × 109/L. In continuous analyses, higher SIRI was associated with greater all-cause mortality (adjusted hazard ratio [HR] 1.031 per unit; 95% confidence interval [CI] 1.018– 1.045; P < 0.001). Compared with the low-SIRI group, the high-SIRI group had higher mortality (adjusted HR 1.543; 95% CI 1.060– 2.246; P < 0.05). High SIRI was also associated with MACCE (adjusted HR 1.037 per unit; 95% CI 1.025– 1.050; P < 0.001).
Conclusion: Elevated admission SIRI is independently associated with a higher risk of one-year all-cause mortality and MACCE among elderly ACS patients.
Keywords: systemic inflammation response index, all-cause mortality, elderly patient, acute coronary syndrome
Introduction
Acute coronary syndrome (ACS) remains a leading cause of morbidity and mortality worldwide, with elderly patients bearing a disproportionate burden.1 Aging is accompanied by increased prevalence of cardiovascular risk factors and comorbidities, which contribute to worse clinical outcomes and higher mortality rates after ACS events in older populations.2,3 Numerous studies have highlighted that elderly individuals with ACS experience significantly higher rates of adverse outcomes compared to younger patients, underscoring the importance of identifying factors associated with mortality in this vulnerable group.4
Inflammation is a key factor in the initiation and progression of atherosclerosis and plaque instability, which are fundamental mechanisms underlying ACS events.5–7 Traditional inflammatory parameters, such as C-reactive protein (CRP), have been extensively studied in cardiovascular diseases;6 however, composite indices derived from routine blood counts may offer additional information on systemic inflammatory status. The SIRI, which combines neutrophil, monocyte, and lymphocyte counts, was first proposed by Qi et al in 2016 as a marker reflecting the balance between innate and adaptive immune responses8 Although initially studied in oncology—where elevated preoperative SIRI has been associated with poorer survival in colorectal cancer and breast cancer9,10—subsequent research has also explored its relevance in cardiovascular and other non-cardiovascular conditions.11–13 In the context of cardiovascular disease, several studies have examined the association between SIRI and MACCE in patients with ACS, with SIRI showing a stronger relationship with MACCE compared to other lymphocyte-based inflammatory indices.14,15 However, most existing research has focused on the composite endpoint of MACCE, leaving the relationship between SIRI and one-year all-cause mortality largely unexplored. This shift in focus toward all-cause mortality is crucial, as it provides a more comprehensive and objective assessment of survival than cause-specific endpoints. The rationale stems from the fact that SIRI reflects a systemic state of immune-inflammatory dysregulation, which may trigger a broad spectrum of fatal complications beyond isolated cardiovascular events. This is particularly salient for elderly patients; in this population, complex comorbidities and the intricate interplay between systemic inflammation and pre-existing conditions significantly shape the all-cause mortality risk. Despite its clinical importance, there remains a substantial gap regarding the association between SIRI and one-year all-cause mortality specifically in elderly ACS patients. Accordingly, we conducted this study to address this uncertainty.
This retrospective cohort study aims to explore the association between SIRI and one-year all-cause mortality in elderly patients with ACS. We hypothesize that higher SIRI level at admission is associated with increased mortality risk within one year.
Patients and Methods
Study Design and Participants
This single-center retrospective cohort study was conducted at the Affiliated Hospital of Guangdong Medical University. We reviewed the medical records of elderly patients (aged ≥ 60 years) admitted with a diagnosis of ACS between January 2022 and December 2023. The eligibility criteria were as follows: Patients were included if they: (1) were aged ≥ 60 years; and (2) had a confirmed diagnosis of ACS according to current guidelines, encompassing unstable angina (UA), non-ST elevation myocardial infarction (NSTEMI), and ST elevation myocardial infarction (STEMI).16 Patients were excluded if they: (1) lacked baseline peripheral blood count data (neutrophil, monocyte, or lymphocyte counts); (2) had no available follow-up data regarding all-cause mortality; or (3) had their first complete blood count (CBC) results collected outside a 48-hour window of admission. The patient selection process is detailed in Figure 1. In addition, this study was reported in accordance with the STROBE guidelines.17
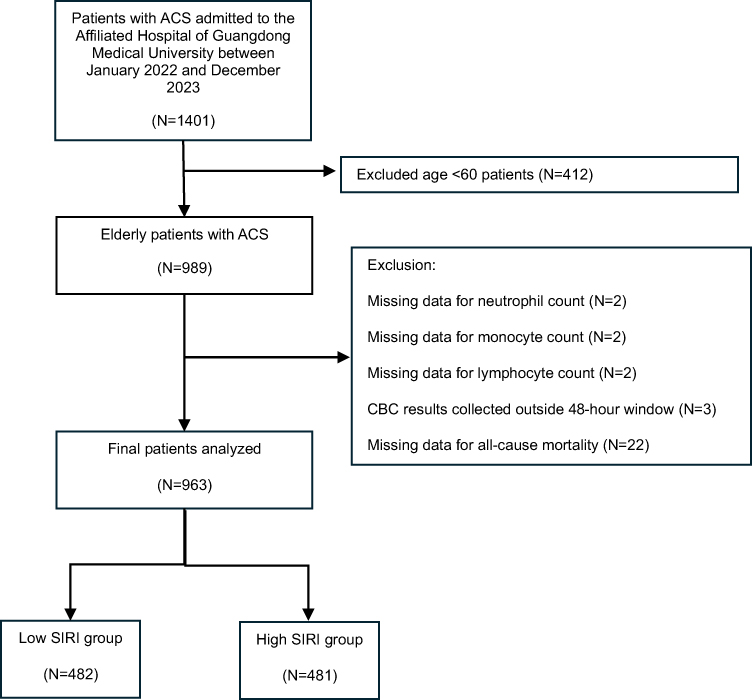 |
Figure 1 Flowchart of the study cohort. Two excluded patients lacked neutrophil, monocyte, and lymphocyte counts, and one of them also lacked all-cause mortality data. Abbreviations: ACS, acute coronary syndrome; SIRI, systemic inflammation response index. |
Outcome and Definition
The primary outcome was all-cause mortality during follow-up, which has also been used as the primary endpoint in some previous studies on ACS.18,19 The secondary outcome was MACCE, defined as all-cause mortality, recurrent myocardial infarction, ischemic stroke, heart failure rehospitalization, revascularization or in-stent thrombosis of the same vessel, and malignant arrhythmia.20
Data Collection and Follow-Up
The investigators had full access to the electronic medical record system of the Affiliated Hospital of Guangdong Medical University to identify eligible patients and extract relevant clinical data. Demographic, clinical, and laboratory data at admission were collected. We also recorded whether patients underwent percutaneous coronary intervention (PCI) during hospitalization. Furthermore, pharmacological treatments at discharge were documented, including aspirin, clopidogrel/ticagrelor, nitric acid esters, angiotensin-converting enzyme inhibitors (ACEI), angiotensin II receptor blockers (ARB), calcium channel blockers (CCB), beta-blockers, statins, and cholesterol absorption inhibitors (ezetimibe). All patients underwent the same clinical and laboratory assessments. CBC results were obtained within 48 hours after hospital admission. The systemic inflammation response index was calculated as: SIRI = (neutrophil count × monocyte count)/lymphocyte count, where all cell counts are expressed in 109/L.8
Patients were followed for up to one year from hospital admission. MACCE were identified from the hospital’s medical record system, excluding diagnoses and treatments from external hospitals; telephone follow-up was conducted only to ascertain outcomes. Survival time was calculated from admission to the date of death or censoring at 365 days for those alive at the end of follow-up.
Statistical Analysis
The normality of continuous data was evaluated via the Shapiro–Wilk test. Variables conforming to a normal distribution were summarized as mean ± standard deviation (SD) and analyzed using Student’s t-test. Conversely, non-normal variables were reported as medians with interquartile ranges (IQR) and compared using the Mann–Whitney U-test. Categorical variables were expressed as counts and percentages.
The cumulative incidence of primary and secondary endpoints was estimated using Kaplan–Meier curves, with differences between groups compared using the Log rank test. Cox proportional hazards regression models were employed to evaluate the associations of SIRI with all-cause mortality and MACCE. The selection of covariates for multivariable Cox models was based on a priori clinical relevance and previous evidence in ACS. Established cardiovascular risk factors, including age, sex, body mass index (BMI), smoking, type of ACS, hypertension, dyslipidemia, and diabetes, were treated as potential confounders and were forced into the models irrespective of their univariable P-values. In addition, key evidence‑based treatments (PCI, aspirin, beta‑blockers, and statins) were included because they are closely related to baseline risk and clinical outcomes and may confound the association between SIRI and all‑cause mortality. Considering the number of observed events, the final multivariable model was restricted to this parsimonious set of 12 covariates to reduce the risk of overfitting. The same set of covariates was used for models with MACCE as the outcome. SIRI was analyzed as both a continuous and categorical variable (high vs. low based on the median value). Additionally, to visualize the relationship between SIRI and the outcomes, we performed a multivariable logistic regression analysis and constructed a smoothed curve. This adjusted smoothed curve, along with the observed data points (displayed as a jittered scatter plot), was used to illustrate the independent association of SIRI with mortality probability. Restricted cubic spline (RCS) analyses were applied to illustrate the relationship between SIRI and the risks of all-cause mortality and MACCE as continuous variables. Finally, to assess the robustness of our findings, we performed several sensitivity analyses. These included subgroup analyses across various clinical strata, a sensitivity analysis restricting the cohort to patients aged ≥ 65 years, and the calculation of E-values to evaluate the potential impact of unmeasured confounding.21
Regarding missing data, BMI had a high missing rate of 58.4%. Given the substantial proportion of missingness, BMI was categorized into three groups: <25 kg/m2, ≥25 kg/m2, and missing. The missing category was treated as a separate group (dummy variable) in the analysis to avoid potential bias and issues associated with imputation of such a large proportion of missing data.
For other variables with less than 5% missing data (smoking, drinking, total cholesterol [TC], low-density lipoprotein cholesterol [LDL-C], triglycerides [TG], high-density lipoprotein cholesterol [HDL-C], and fasting plasma glucose [FPG]), multiple imputation by chained equations was performed using the mice package in R. Predictive mean matching was used for the continuous variables (TC, LDL-C, TG, HDL-C, and FPG), and logistic regression was used for the binary categorical variables (smoking and drinking). SIRI, age, sex, type of ACS, hypertension, dyslipidemia, and diabetes were included as predictors in the imputation models. The lipid variables (TC, LDL-C, TG, and HDL-C) were allowed to predict each other while preventing perfect collinearity between TC and LDL-C. Ten imputed datasets were generated with 30 iterations each. Diagnostic plots (trace plots of means and standard deviations across iterations, and density plots comparing observed vs. imputed value distributions) confirmed good convergence of the imputation algorithm and close agreement between observed and imputed distributions for all variables. These diagnostic plots are provided in the Supplementary Material (Supplementary Figure S1).
All statistical analyses were conducted using R software version 4.4.2. A two-sided P-value < 0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 963 elderly ACS patients were included, with a median age of 73 years (interquartile range 66–80) and 69.5% male. During follow-up, 132 patients (13.7%) died and 214 patients (22.2%) experienced MACCE. The majority of CBC results (87.3%) were obtained within 24 hours of admission, with the remaining results obtained within 48 hours. The cut-off value for SIRI was defined as the median (2.89×109/L). Based on this threshold, patients were divided into high- and low-SIRI groups for subsequent analyses. Baseline characteristics stratified by SIRI groups are summarized in Table 1.
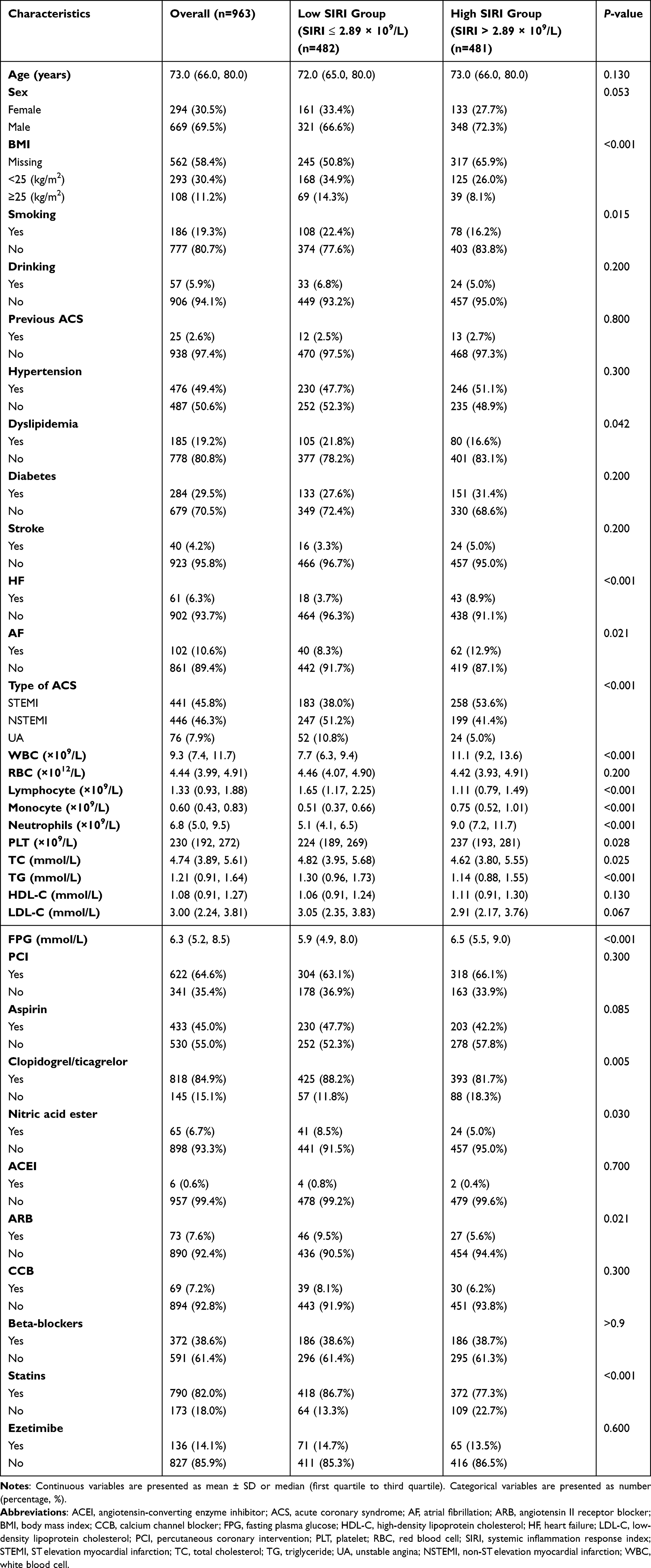 |
Table 1 Baseline Characteristics of the Study Population with Different SIRI Groups |
Association Between SIRI and All-Cause Mortality
One-year all-cause mortality occurred in 45 patients (9.3%) in the low-SIRI group and 87 patients (18.1%) in the high-SIRI group. When analyzed as a continuous variable, each 1.0 × 109/L increase in SIRI was significantly associated with an increased risk of one-year all-cause mortality (adjusted HR 1.031; 95% CI, 1.018–1.045; P < 0.001). Compared with the low-SIRI group, participants in the high-SIRI group exhibited a markedly greater risk of mortality (adjusted HR 1.543; 95% CI, 1.060–2.246; P < 0.05) (Table 2). The curve-fitting analysis for SIRI versus both all-cause mortality and MACCE demonstrated that these event rates increased consistently with rising SIRI (Figure 2A and B, respectively). For all-cause mortality, RCS analysis indicated a linear relationship between SIRI and mortality (P for nonlinearity > 0.05, Supplementary Figure S2). Kaplan–Meier survival curves showed a notably lower survival probability among individuals with elevated SIRI (Figure 3A).
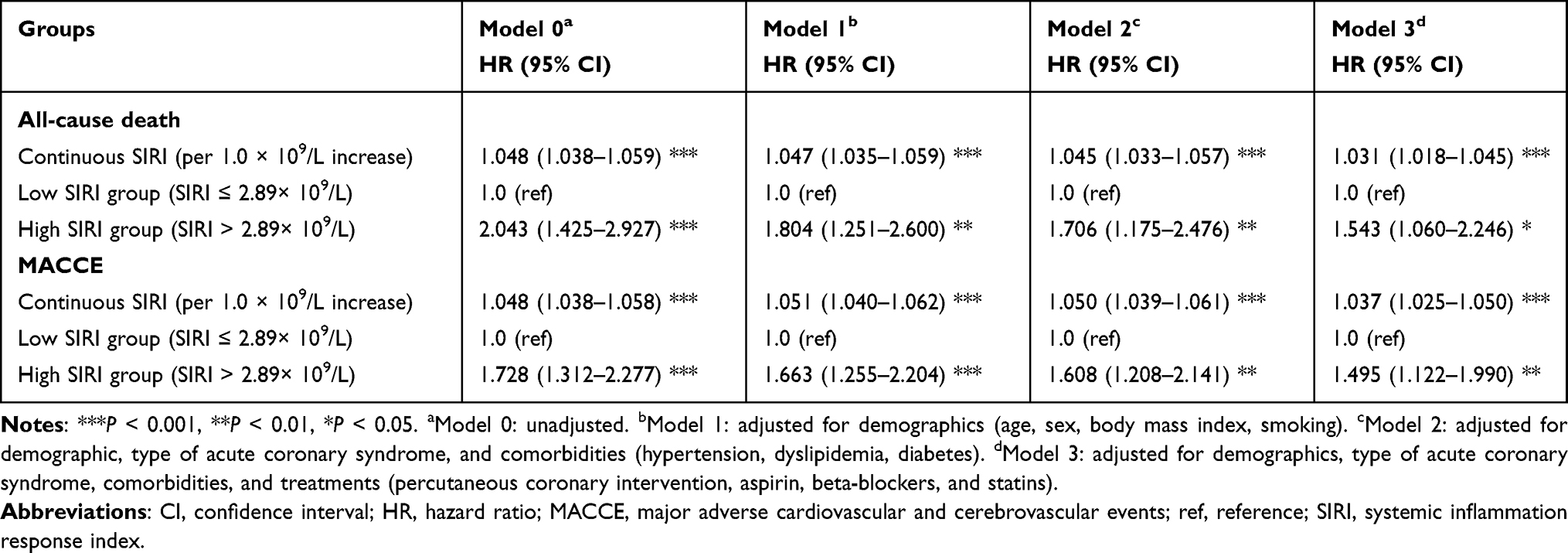 |
Table 2 Association of SIRI with One-Year All-Cause Mortality and MACCE |
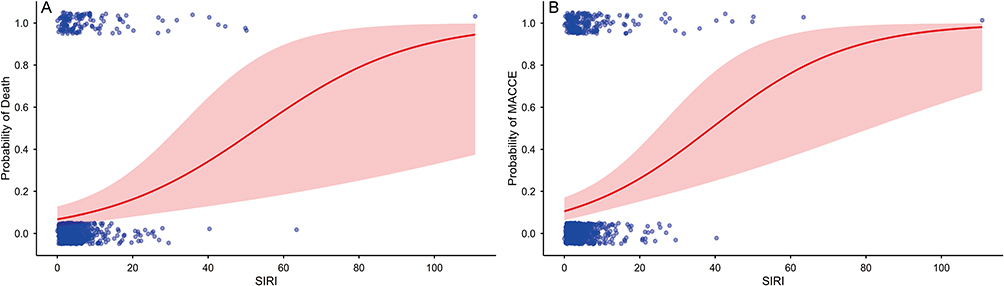 |
Figure 2 Association of SIRI with (A) death and (B) MACCE probability; blue points represent individual data, while the red curve indicates the fitted model with 95% CI. Abbreviations: MACCE, major adverse cardiovascular and cerebrovascular events; SIRI, systemic inflammation response index. |
 |
Figure 3 Kaplan-Meier curves in different SIRI groups for (A) one-year all-cause mortality rates and (B) MACCE rates. Abbreviations: MACCE, major adverse cardiovascular and cerebrovascular events; SIRI, systemic inflammation response index. |
Association Between SIRI and MACCE
Details on the incidence and distribution of MACCE are provided in Supplementary Table S1. A total of 82 (17.0%) and 132 (27.4%) patients experienced MACCE in the low- and high-SIRI groups, respectively. As a continuous variable, SIRI showed a significant association with increased MACCE risk (adjusted HR = 1.037 per unit, 95% CI: 1.025–1.050, P < 0.001). The high SIRI group had a substantially elevated risk of experiencing MACCE compared to the low SIRI group (adjusted HR = 1.495, 95% CI: 1.122–1.990, P < 0.01) (see Table 2). Consistent with the curve-fitting trends mentioned above (Figure 2B), the RCS analysis for SIRI versus MACCE also indicated a linear relationship (P for nonlinearity > 0.05, Supplementary Figure S3). Elevated SIRI was associated with a markedly decreased MACCE-free survival probability on the Kaplan–Meier curves (Figure 3B).
Sensitivity Analysis
The association between SIRI and one-year all-cause mortality remained consistent across all evaluated clinical subgroups (Supplementary Figure S4). To further verify the robustness of our findings across different age definitions, we conducted a sensitivity analysis by restricting the cohort to patients aged ≥ 65 years (N = 769). The results were highly consistent with the primary analysis. Elevated SIRI was independently associated with an increased risk of mortality, both as a continuous variable (adjusted HR 1.027; 95% CI, 1.009–1.045; P < 0.01) and a categorical variable (adjusted HR 1.524; 95% CI, 1.031–2.253; P < 0.05), as shown in Supplementary Table S2. Additionally, the E-value for this association was 2.458 (lower bound: 1.312).
Discussion
To our knowledge, research exploring the association between SIRI and one-year all-cause mortality in patients with ACS remains limited. Our study contributes to this field by evaluating this relationship and providing a visual depiction of the association in elderly ACS patients through curve-fitting illustrations. In this retrospective cohort analysis, we found that elevated SIRI levels are independently associated with a higher one-year all-cause mortality risk, as well as an increased incidence of MACCE.
Consistent with prior literature, our results reinforce the notion that SIRI correlates with adverse outcomes in ACS patients.22 Earlier study reported association between SIRI and short-term (30- and 90-day) all-cause mortality after acute myocardial infarction, though with a nonlinear relationship.23 In contrast, our analysis revealed a linear relationship between SIRI and one-year all-cause mortality in elderly ACS patients: each 1.0 × 109/L increase in SIRI corresponded to a 3.1% rise in mortality risk, and the test for nonlinearity (RCS) was not significant (P > 0.05). Figure 2A visually demonstrates this relationship illustrating that mortality increases as SIRI rises and embodies a key result of our study. The observed all-cause mortality rate of 13.7% was higher in our study than in some prior studies, which may reflect differences in study populations.24,25 Our study focused on elderly ACS patients, a demographic typically characterized by a higher burden of comorbidities and a greater predisposition to severe illness. We used 60 years as the threshold for the elderly population in this analysis, following regional standards and WHO Western Pacific Region guidelines.26,27 To ensure the stability of our findings, we also performed a sensitivity analysis using a ≥ 65-year threshold. This analysis yielded nearly identical results, confirming that the association between SIRI and mortality is independent of the specific age cutoff used. This inherent high-risk profile likely accounts for the higher mortality observed in our cohort compared with studies enrolling patients across all age groups.
Regarding MACCE, prior work by He et al demonstrated a significant association between high SIRI and increased MACCE risk in ACS patients with concurrent obstructive sleep apnea28 Similarly, Han et al reported an association between SIRI and MACCE in ACS patients undergoing PCI24 Li and Fan evaluated multiple inflammatory markers for prognostic utility in ACS, with both studies concluding that SIRI was independently associated with MACCE. Furthermore, Li’s results indicated that SIRI outperformed other lymphocyte-related indices.14,25 Notably, our study reports the highest incidence of MACCE (22.2%) to date among published studies on this specific patient population. This discrepancy likely reflects differences in patient selection; for instance, Fan’s study noted most MACCE events occurred in patients older than 65, aligning with our focus on elderly ACS patients.25 Differences in MACCE definitions and follow-up durations may also contribute to variation in incidence; nonetheless, given that our follow-up was the shortest among the five studies, prolonged observation is unlikely to account for our higher MACCE rate.
ACS is primarily caused by the rupture or erosion of vulnerable atherosclerotic plaques.29 Inflammation plays a pivotal role in both the initiation and progression of atherosclerosis, with shifts in inflammatory cell populations and circulating markers reflecting the underlying inflammatory milieu.5–7 This process is driven by the activation of neutrophils, monocytes, and lymphocytes.25 As key components of innate immunity, monocytes and neutrophils secrete pro-inflammatory mediators, including interleukin-6 (IL-6). Activated monocytes can also differentiate into foam cells, contributing to plaque destabilization and atherogenic lipid changes.30 In contrast, lymphocytes modulate the immune response and play a crucial anti-inflammatory role. In elderly individuals, immunosenescence and chronic low-grade inflammation (“inflammaging”) reshape the inflammatory response, often leading to a dysregulated state that affects both initiation and resolution of acute events.31 Given this altered immunoinflammatory background in our elderly ACS cohort, SIRI may better reflect the complex interplay between innate immune status, systemic inflammation and age-related immune alterations. This could explain the observed association between an elevated SIRI and an increased risk of all-cause mortality and MACCE in this population.
Limitation
There are certain limitations inherent to this study. Firstly, the retrospective design of this study inherently carries a risk of selection bias and limits the ability to establish causal relationships. Secondly, we excluded patients lacking SIRI and those without primary outcome, which could potentially introduce selection bias. Nonetheless, the number of patients missing SIRI was very small (only 2 cases), likely exerting minimal influence on the results. Additionally, we compared patients with and without outcome and found that nearly all baseline variables showed no statistically significant differences between the two groups. The extent of missing primary outcome data (n=21) and the comparison of clinically adjudicated covariates are detailed in Supplementary Table S3. Thirdly, SIRI was calculated based on admission CBC data, and our study lacked systematic screening for all concomitant medical conditions, such as malignancies or infections, which might influence leukocyte counts and potentially confound SIRI values. However, to address this, we calculated an E-value of 2.458 (lower bound: 1.312) for the association between SIRI and one-year all-cause mortality. This quantitative assessment suggests that the observed association is relatively robust to potential unmeasured confounding. Fourthly, conducting the study within a single institution may also limit the generalizability of the findings, as patient populations and healthcare practices can vary considerably across different settings. Fifthly, the primary endpoint was all-cause mortality, and cause-specific data were not available; therefore, we were unable to differentiate cardiovascular from non-cardiovascular deaths, which might have provided additional mechanistic insights. Finally, the results are restricted to elderly ACS patients aged over 60 years. Overall, while this study offers valuable insights, prospective and multicenter research is needed to validate these findings and elucidate the causal mechanisms involved.
Conclusion
There is an independent association between higher admission SIRI levels and increased risks of one-year all-cause mortality and MACCE in elderly patients with ACS. These findings warrant further exploration of the underlying mechanisms and tailored therapeutic strategies to potentially improve outcomes in this population.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Affiliated Hospital of Guangdong Medical University (ethical approval number: KT2025-185-01). Written informed consent was obtained from all participants or their legal guardians in cases of incapacity or death. The trial was registered at the Chinese Clinical Trial Registry (registration number: ChiCTR2500107705).
Acknowledgments
The authors thank all the participants and staff involved in this study. We also acknowledge the valuable support from the Department of Cardiology at the Affiliated Hospital of Guangdong Medical University. Besides, the authors thank Ruoxuan Mai and Yueming Chen (The First School of Clinical Medicine, Guangdong Medical University, Zhanjiang, Guangdong, People’s Republic of China) for the data collection.
Author Contributions
JL; Conceptualization, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – original draft. WW; Conceptualization, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – original draft. LX; Conceptualization, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – original draft. NL; Formal analysis, Software, Visualization. YK; Data curation, Investigation. LC; Data curation, Investigation, Resources. YZ; Data curation, Investigation. LZ; Conceptualization, Formal analysis, Methodology, Project administration, Supervision, Writing – review and editing. MC; Conceptualization, Formal analysis, Methodology, Funding acquisition, Project administration, Supervision, Writing – review and editing. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Science and Technology Development Fund, Macau SAR (grant number: 0018/2024/RIA1,0114/2022/A). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Morici N, Savonitto S, Ferri LA, et al. Outcomes of elderly patients with ST-Elevation or Non-ST-Elevation acute coronary syndrome undergoing percutaneous coronary intervention. Am J Med. 2019;132(2):209–11. doi:10.1016/j.amjmed.2018.10.027
2. Alexander KP, Newby LK, Cannon CP, et al. Acute coronary care in the elderly, part I: non-ST-segment-elevation acute coronary syndromes: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: in collaboration with the Society of Geriatric Cardiology. Circulation. 2007;115(19):2549–2569. doi:10.1161/CIRCULATIONAHA.107.182615
3. Alonso Salinas GL, Sanmartin Fernandez M, Pascual Izco M, et al. Frailty is a short-term prognostic marker in acute coronary syndrome of elderly patients. Eur Heart J Acute Cardiovasc Care. 2016;5(5):434–440. doi:10.1177/2048872616644909
4. Yeh RW, Sidney S, Chandra M, Sorel M, Selby JV, Go AS. Population trends in the incidence and outcomes of acute myocardial infarction. N Engl J Med. 2010;362(23):2155–2165. doi:10.1056/NEJMoa0908610
5. Occhipinti G, Brugaletta S, Abbate A, et al. Inflammation in coronary atherosclerosis: diagnosis and treatment. Heart. 2025;111:801–810. doi:10.1136/heartjnl-2024-325408
6. Lawler PR, Bhatt DL, Godoy LC, et al. Targeting cardiovascular inflammation: next steps in clinical translation. Eur Heart J. 2021;42(1):113–131. doi:10.1093/eurheartj/ehaa099
7. Engelen SE, Robinson AJB, Zurke YX, Monaco C. Therapeutic strategies targeting inflammation and immunity in atherosclerosis: how to proceed? Nat Rev Cardiol. 2022;19(8):522–542. doi:10.1038/s41569-021-00668-4
8. Qi Q, Zhuang L, Shen Y, et al. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016;122(14):2158–2167. doi:10.1002/cncr.30057
9. Menyhart O, Fekete JT, Gyorffy B. Inflammation and colorectal cancer: a meta-analysis of the prognostic significance of the Systemic Immune-Inflammation Index (SII) and the Systemic Inflammation Response Index (SIRI). Int J Mol Sci. 2024;25(15):8441. doi:10.3390/ijms25158441
10. Zhang S, Cheng T. Prognostic and clinicopathological value of systemic inflammation response index (SIRI) in patients with breast cancer: a meta-analysis. Ann Med. 2024;56(1):2337729. doi:10.1080/07853890.2024.2337729
11. Fang Z, Gao B, Wang Z, Chen X, Liu M. Association of systemic inflammation response index with mortality risk in older patients with hip fracture: a 10-year retrospective cohort study. Front Med Lausanne. 2024;11:1401443. doi:10.3389/fmed.2024.1401443
12. Kong F, Huang J, Xu C, Huang T, Wen G, Cheng W. System inflammation response index: a novel inflammatory indicator to predict all-cause and cardiovascular disease mortality in the obese population. Diabetol Metab Syndr. 2023;15(1):195. doi:10.1186/s13098-023-01178-8
13. Gu L, Xia Z, Qing B, et al. Systemic Inflammatory Response Index (SIRI) is associated with all-cause mortality and cardiovascular mortality in population with chronic kidney disease: evidence from NHANES (2001-2018). Front Immunol. 2024;15:1338025. doi:10.3389/fimmu.2024.1338025
14. Li Q, Ma X, Shao Q, et al. Prognostic impact of multiple lymphocyte-based inflammatory indices in acute coronary syndrome patients. Front Cardiovasc Med. 2022;9:811790. doi:10.3389/fcvm.2022.811790
15. Yilu Z, Zhanglong W, Fanke H, et al. The progression of non-culprit coronary lesion is related to higher SII, SIRI, and PIV in patients with ACS. Medicine. 2024;103(52):e41094. doi:10.1097/MD.0000000000041094
16. Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: executive Summary: a Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;144(22):e368–e454. doi:10.1161/CIR.0000000000001030
17. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
18. Eagle KA, Lim MJ, Dabbous OH, et al. A validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6-month postdischarge death in an international registry. JAMA. 2004;291(22):2727–2733. doi:10.1001/jama.291.22.2727
19. Wenzl FA, Kofoed KF, Simonsson M, et al. Extension of the GRACE score for non-ST-elevation acute coronary syndrome: a development and validation study in ten countries. Lancet Digit Health. 2025;7(10):100907. doi:10.1016/j.landig.2025.100907
20. Bosco E, Hsueh L, McConeghy KW, Gravenstein S, Saade E. Major adverse cardiovascular event definitions used in observational analysis of administrative databases: a systematic review. BMC Med Res Methodol. 2021;21(1):241. doi:10.1186/s12874-021-01440-5
21. Haneuse S, VanderWeele TJ, Arterburn D. Using the E-Value to assess the potential effect of unmeasured confounding in observational studies. JAMA. 2019;321(6):602–603. doi:10.1001/jama.2018.21554
22. Jin Z, Wu Q, Chen S, et al. The Associations of two novel inflammation indexes, SII and SIRI with the risks for cardiovascular diseases and all-cause mortality: a ten-year follow-up study in 85,154 individuals. J Inflamm Res. 2021;14:131–140. doi:10.2147/JIR.S283835
23. Wang Y, Chen H. A nonlinear relationship between systemic inflammation response index and short-term mortality in patients with acute myocardial infarction: a retrospective study from MIMIC-IV. Front Cardiovasc Med. 2023;10:1208171. doi:10.3389/fcvm.2023.1208171
24. Han K, Shi D, Yang L, et al. Prognostic value of systemic inflammatory response index in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Ann Med. 2022;54(1):1667–1677. doi:10.1080/07853890.2022.2083671
25. Fan W, Wei C, Liu Y, et al. The prognostic value of hematologic inflammatory markers in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Clin Appl Thromb Hemost. 2022;28:10760296221146183. doi:10.1177/10760296221146183
26. Bao Q, Liu T, Song H, Bao W, Fan W. prognostic role of inflammatory hematologic indices in predicting acute coronary syndrome in elderly patients with chronic coronary syndrome. J Inflamm Res. 2025;18:9637–9653. doi:10.2147/JIR.S528161
27. Molassiotis A, Leung AYM, Zhao IY. Call for urgent actions in societies and health systems in the Western Pacific Region to implement the WHO Regional Action Plan on Healthy Ageing. J Am Geriatr Soc. 2021;69(8):2374–2377. doi:10.1111/jgs.17196
28. He Q, Zhou Y, Tong X, et al. Prognostic value of the systemic inflammatory response index in patients with acute coronary syndrome and obstructive sleep apnea. J Inflamm Res. 2025;18:7515–7527. doi:10.2147/JIR.S515437
29. Fahed AC, Jang IK. Plaque erosion and acute coronary syndromes: phenotype, molecular characteristics and future directions. Nat Rev Cardiol. 2021;18(10):724–734. doi:10.1038/s41569-021-00542-3
30. Ajoolabady A, Pratico D, Lin L, et al. Inflammation in atherosclerosis: pathophysiology and mechanisms. Cell Death Dis. 2024;15(11):817. doi:10.1038/s41419-024-07166-8
31. Ajoolabady A, Pratico D, Tang D, Zhou S, Franceschi C, Ren J. Immunosenescence and inflammaging: mechanisms and role in diseases. Ageing Res Rev. 2024;101:102540. doi:10.1016/j.arr.2024.102540
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.