")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Association of Red Cell Index and Hospital Mortality in Chronic Obstructive Pulmonary Disease Patients Admitted to the Intensive Care Unit: A Retrospective Cohort Study
Authors Shi Y , Shi Y , Xu Z , Wang Y
Received 24 July 2023
Accepted for publication 3 October 2023
Published 16 October 2023 Volume 2023:18 Pages 2267—2276
DOI https://doi.org/10.2147/COPD.S427433
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Yushan Shi,1 Yanfei Shi,2 Zhangmeng Xu,3 Yan Wang4
1Department of Laboratory, Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, Shandong, 250000, People’s Republic of China; 2Department of Pulmonary Disease, Dezhou Hospital of Traditional Chinese Medicine, Dezhou, Shanfdong, 253000, People’s Republic of China; 3School of Health Preservation and Rehabilitation, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, 610075, People’s Republic of China; 4Department of Pulmonary and Critical Care Medicine, Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, 250000, People’s Republic of China
Correspondence: Yan Wang, Department of Respiratory and Critical Care Medicine, Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jingshi Road, Lixia District, Jinan, Shandong, People’s Republic of China, Tel +86 159-53182611, Fax +86 531-68616927, Email [email protected]
Purpose: This study aims to explore the association between red cell index (RCI) and hospital mortality in Chronic Obstructive Pulmonary Disease (COPD) patients in the intensive care unit.
Patients and Methods: This was a retrospective cohort research. The study included 821 COPD patients. Clinical data from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database was conducted. Multivariate logistic regression analysis was used to assess the correlation between RCI and in-hospital mortality. Age, SOFA score, diabetes mellitus, cerebrovascular disease, congestive heart failure and mechanical ventilation were considered for subgroup analysis.
Results: This study comprised 821 patients, of which 16.5% (124/821) suffered hospital mortality. In the multivariate logistic regression model, RCI was positively associated with hospital mortality, each unit increase in RCI was associated with a 3% increase in hospital mortality (odds ratio [OR] =1.03; 95% confidence interval [95CI%] =1.01– 1.06). Meanwhile, compare with the lowest RCI group, the highest RCI groups tended to have higher risks of hospital mortality (OR [95% CI] 2.33 [1.27– 4.27]). Additionally, subgroup analysis result was persistent among all the groups.
Conclusion: Higher RCI was positively associated with a higher risk of mortality in critically ill patients with COPD. Further investigation is necessary to confirm these findings.
Keywords: red cell index, chronic obstructive pulmonary disease, hospital mortality, retrospective cohort study, MIMIC-IV
Introduction
Chronic Obstructive Pulmonary Disease (COPD), characterized by persistent respiratory symptoms and progressive airflow limitations, is a significant cause of morbidity, mortality, and healthcare utilization worldwide.1,2 Patients with COPD often require hospitalization or ICU admission for acute exacerbations.3 Consequently, COPD has a significant impact on patients’ quality of life, healthcare expenditures, and clinical and economic burden.4 Furthermore, in critically ill patients, the risk-adjusted mortality of patients with COPD was higher than in patients without COPD. The presence of COPD was an independent risk factor for increased mortality and was associated with prolonged mechanical ventilation and prolonged weaning.5 Therefore, identifying easily accessible and technically undemanding markers during hospitalization for COPD patients that are associated with hospital mortality becomes essential for reducing the disease burden and mortality rates.
There is a new indicator red cell index (RCI) that obtained from complete blood count measurements. RCI is related to red blood cell (RBC) count (10^12/L), hemoglobin (Hb) level (g/L), lymphocytes (Lym) count (10^9/L), and platelets (PLT) count (10^9/L), calculation formulas of RCI is (RBC × Hb)/(Lym × PLT).6 RCI has been shown to be associated with decreased lung function and severity of disease, higher RCI level is associated with lower FEV1/FVC and higher PCO2.7 Previous studies have also confirmed that RCI level was an effective biomarker to predict 3-month mortality in acute ischemic stroke (AIS) patients or pulmonary embolism (PE) patients.8,9 RCI is positively correlated with adverse hospitalization outcomes in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD).10
Nevertheless, the association between RCI level and hospital mortality in critically ill COPD patients is unclear. Therefore, we aimed to investigate the association between RCI and hospital mortality with COPD patients in the ICU.
Materials and Methods
Database introduction
The data were obtained from the open-source clinical database, Medical Information Mart for Intensive Care IV (MIMIC IV), an update to MIMIC-III, which covered over 50,000 patients admitted to the intensive care unit (ICU) at Beth Israel Deaconess Medical Center during the years from 2008 to 2019.11 The first author, Yushan Shi, has gained access to the database (Certification No: 54017638) after passing the online exams and signing a data use agreement. The institutional review boards of both Beth Israel Deaconess Medical Center and MIT Affiliates have approved the establishment of the MIMIC-IV database. As database is anonymous, so informed consent was not applicable. The Ethics Committee of Affiliated Hospital of Shandong University of Traditional Chinese Medicine has granted an exemption from review for this particular study, ethics number was 2023–0020.
Selection of Study Population
The total number of patients in MIMIC IV database was 73.181 and 50,920 of them first admitted to the ICU. This study was based on the real-world study concept and included all COPD patients from the MIMIC-IV database. Our inclusion criteria were as follows: (1) Patients were older than 18 years and stayed in the ICU for more than 24 hours;12–14 (2) Patients were diagnosed as COPD by ICD-9 codes (code = 49120, 49121, 49122) and ICD-10 codes (code = J44, J440, J441 and J442). Patients whose red cell, platelets, lymphocyte, hemoglobin levels were unavailable during the first day of ICU admission were excluded, as well as, the length of hospital time and ICU stay time was less than 24h. For patients with multiple ICU admissions, we only included data from patients with their first hospital and first ICU admission.15
Variable Extraction and Outcome
Data were extracted using PostgreSQL (version 13.9). Data included demographic information, vital signs, laboratory tests, comorbidities, intervention and critical score. The baseline data were obtained within the first 24 hour after ICU admission. The initial value was considered for a variable that was measured multiple times within 24 hour after ICU admission.
Demographic information: age, gender, race and insurance status, length of hospital stays, and hospital death sign.
Vital signs: heart rate (HR), systolic blood pressure (SBP); diastolic blood pressure (DBP), mean blood pressure (MBP), respiratory rate (RR), and oxygen saturation (SpO2).
Laboratory data: routine blood tests included red blood cell (RBC) count, hemoglobin (Hb) level, lymphocytes (Lym) count, and platelets (PLT) count, glucose, serum sodium, serum potassium, serum chloride, creatinine, blood urea nitrogen (BUN), serum alanine transaminases (ALT), serum aspartate aminotransferase (AST) and bicarbonate, anion gap.
Comorbidities: cerebrovascular disease, congestive heart failure, peripheral vascular disease, diabetes, mild liver disease, moderate or severe liver disease, myocardial infarct, malignant cancer, and renal disease. It was identified by the ninth or tenth revision of the International Classification of Diseases (ICD-9 or ICD-10), chronic hepatitis or cirrhosis without or with portal hypertension was considered as mild or moderately to severe liver disease, respectively.16
Critical score: simplified acute physiology II score (SAPS II), oxford acute severity of illness score (OASIS) sequential organ failure assessment score (SOFA)
The RCI was estimated using the following equation: RCI = (RBC × Hb)/(Lym × PLT), In accordance with RCI at 24 hour, all patients were divided into tertiles.
The outcome of this study was hospital mortality.
Statistical Analysis
Participants were divided into tertiles based on RCI levels (RCI <1.18; 1.18 ≤ RCI<2.62; RCI ≥2.62).
Categorical variables are expressed as proportions (%) and tested with Chi-square or Fisher exact test. Continuous variables are expressed as mean ± standard deviation (SD) and tested with T-test or one-way ANOVA (normally distributed), non-normally distributed are expressed as median and interquartile range (IQR) and tested with Kruskal–Wallis H-test.
A univariate model was used to evaluate whether the RCI and other biochemical variables were associated with hospital mortality. Multivariate logistic regression models were used to examine whether RCI had an independent effect on hospital mortality. Variables, which differed significantly with p values of <0.05 in univariate logistic regression analysis, were acknowledged as covariates for multivariate logistic regression analysis. RCI was analyzed as continuous and categorical variables in regression analyses, respectively. Values of the variation inflation factor (VIF) were used to assess multicollinearity. More than 10 VIFs showed multicollinearity. We constructed five models: crude model, unadjusted; model 1, adjusted for age, sex, and race; model 2, adjusted for model 1 and additionally for HR, RR, SBP, SpO2, cerebrovascular disease, liver disease, congestive heart failure, and diabetes; model 3, adjusted for model 2 and additionally for anion gap, chloride, bicarbonate, BUN, serum creatinine, ALT, and AST; model 4, adjusted for model 3 and additionally for SAPSII, OASIS, SOFA, and mechanical ventilation.
To further explore the stability of results, we conducted interaction and subgroup analyses based on age (<65 years and ≥65 years), congestive heart failure, diabetes, ventilation, and SOFA score (<4 and ≥4). Each stratification was adjusted for factors in multivariate logistic regression analysis model 4, except for the stratification factor itself. Interaction across subgroups was tested using the likelihood ratio test.
Percentage of covariates with missing data is about 40%, Missing values of covariates were imputed via multiple imputations.17 Specifically, we imputed five sets of missing values and then selected one set for logistic regression analysis and subgroup analysis. We also performed sensitivity analysis with variable deletion for missing values and then conducted multivariate analysis using only the non-missing population. The results of this analysis can be found in Table S1.
We performed all analyses using the statistical software packages R 3.3 and Free Statistics software versions 1.7.15 All statistical tests were two-tailed, and p < 0.05 was considered significant.
Results
Population of the Study
Based on the above inclusion and exclusion criteria, 821 patients were identified in the final cohort, including 697 survivors and 124 non-survivors. The flow chart of the study patients is presented in Figure 1.
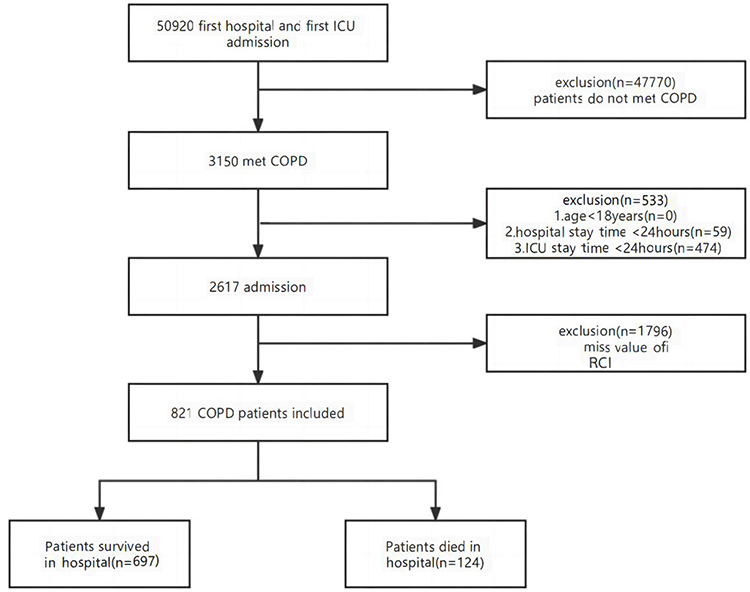 |
Figure 1 Flowchart of participant selection. Abbreviations: ICU, intensive care unit; COPD, chronic obstructive pulmonary disease; RCI, red cell index. |
Baseline Characteristics of the Study Subjects
The baseline characteristics of patients are presented in Table 1. The overall rate of hospital mortality was 15.1% (124/821). The patient age was 71.1 ± 10.6 years, and approximately 56.3% (462/821) patients were men, most of whom were white. According to RCI values at first 24 hour, patients were divided into tertiles (RCI <1.18; 1.18 ≤ RCI<2.62; RCI ≥2.62).
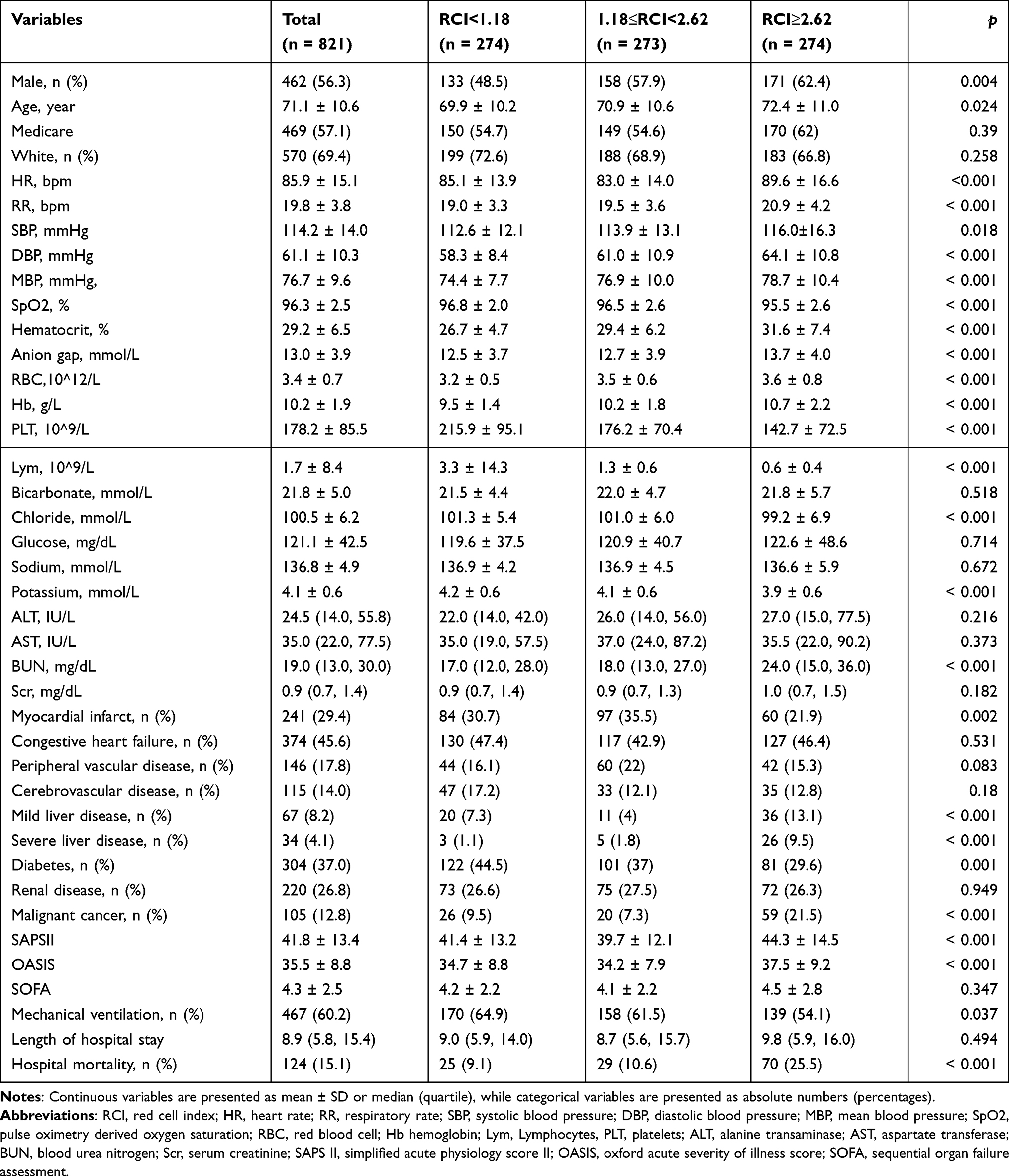 |
Table 1 Baseline and Clinical Characteristics of the Study Population |
RCI <1.18 was considered as the lower group,1.18 ≤ RCI<2.62 was considered as the middle group, and ≥2.62 was considered as the higher group. Among three groups, no significant correlation was found in terms of bicarbonate, glucose, sodium, ALT, AST, serum creatinine, SOFA score, and length of hospital stay history of congestive heart failure, peripheral vascular disease, cerebrovascular disease, renal disease. Patients in the higher red cell index (RCI) group were more likely to develop liver disease, malignant cancer and were less likely to develop diabetes than patients in the lower group (all P < 0.05). As the red cell index (RCI) increased, age, respiratory rate, MBP, RBC and Hb, anion gap, creatinine level, BUN, increased, whereas PLT, Lym, SpO2 and serum potassium, chloride levels decreased.
Results of Logistic Regression Analysis
Univariate regression analyses were performed to identify factors associated with hospital mortality (Table 2), it indicated that age, race, RCI, HR, RR, BUN, ALT, AST, liver disease, SOFA score, mechanical ventilation were risk factors for in-hospital mortality (all P<0.05,).
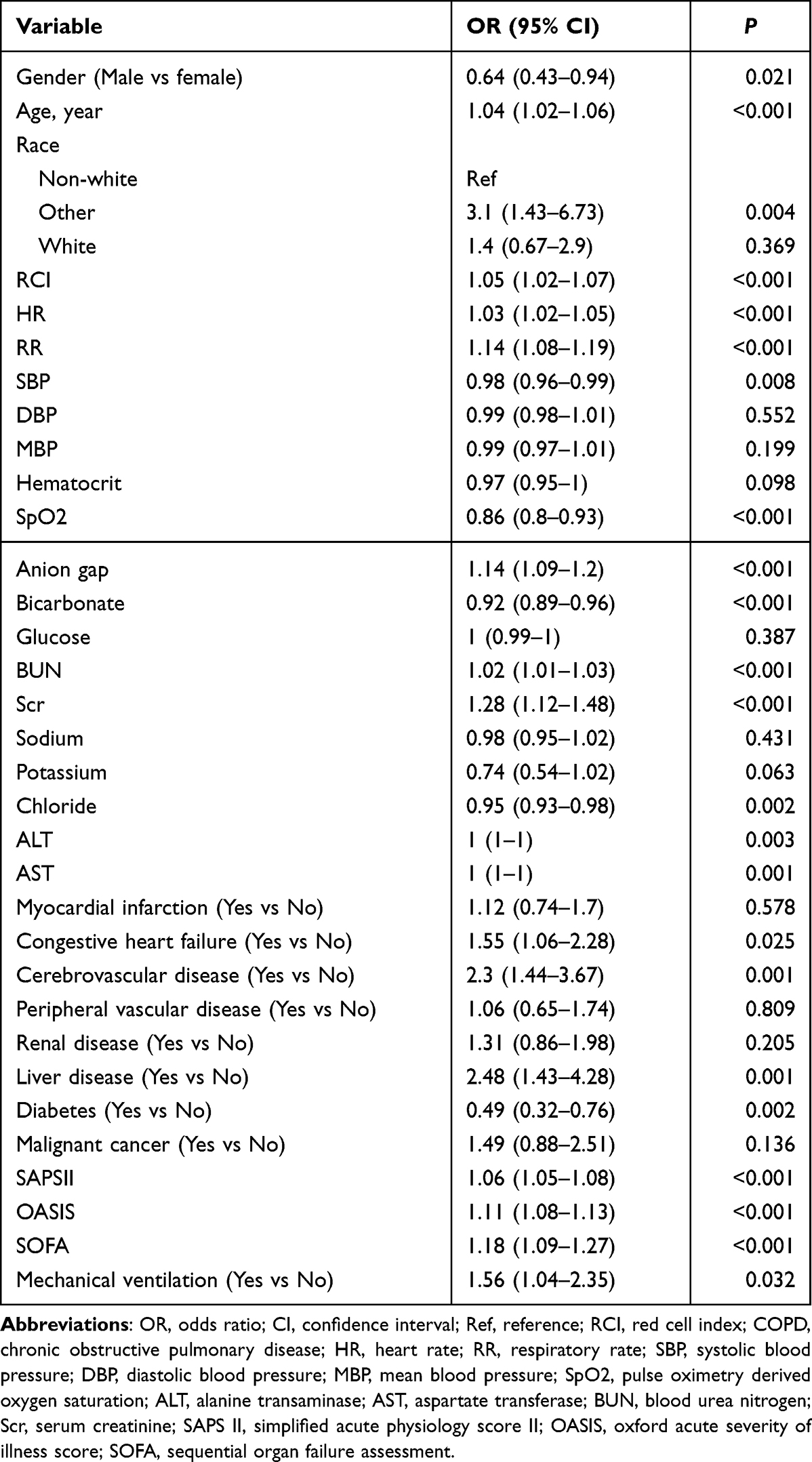 |
Table 2 Univariate Analysis of Risk Factor Associated with Hospital Mortality in Patients with COPD |
Multivariate logistic regression analysis was constructed in five different models, the odds ratios (OR) and 95% confidence interval (95% CI) are shown in Table 3. Crude model, unadjusted; model 1, adjusted for age, sex, and race; model 2, adjusted for model 1 and additionally for HR, RR, SBP, SpO2, cerebrovascular disease, liver disease, congestive heart failure, and diabetes; model 3, adjusted for model 2 and additionally for anion gap, chloride, bicarbonate, BUN, serum creatinine, ALT, and AST; model 4, adjusted for model 3 and additionally for SAPSII, OASIS, SOFA, and mechanical ventilation. When RCI level was used as a continuous variable, in the non-adjusted model, it was significantly associated with hospital mortality (OR=1.05, 95% CI: 1.02–1.07, p<0.001), as well as in the fully adjusted model 4 (OR=1.03, 95% CI: 1.01–1.06, p=0.012). When RCI was turned into a categorical variable, comparison with the lower group, the fully adjusted model 4 OR were 1.4 (95% CI: 0.73–2.7, p=0.31) and 2.33 (95% CI: 1.27–4.27, p=0.006) in the second and third tertiles, respectively.
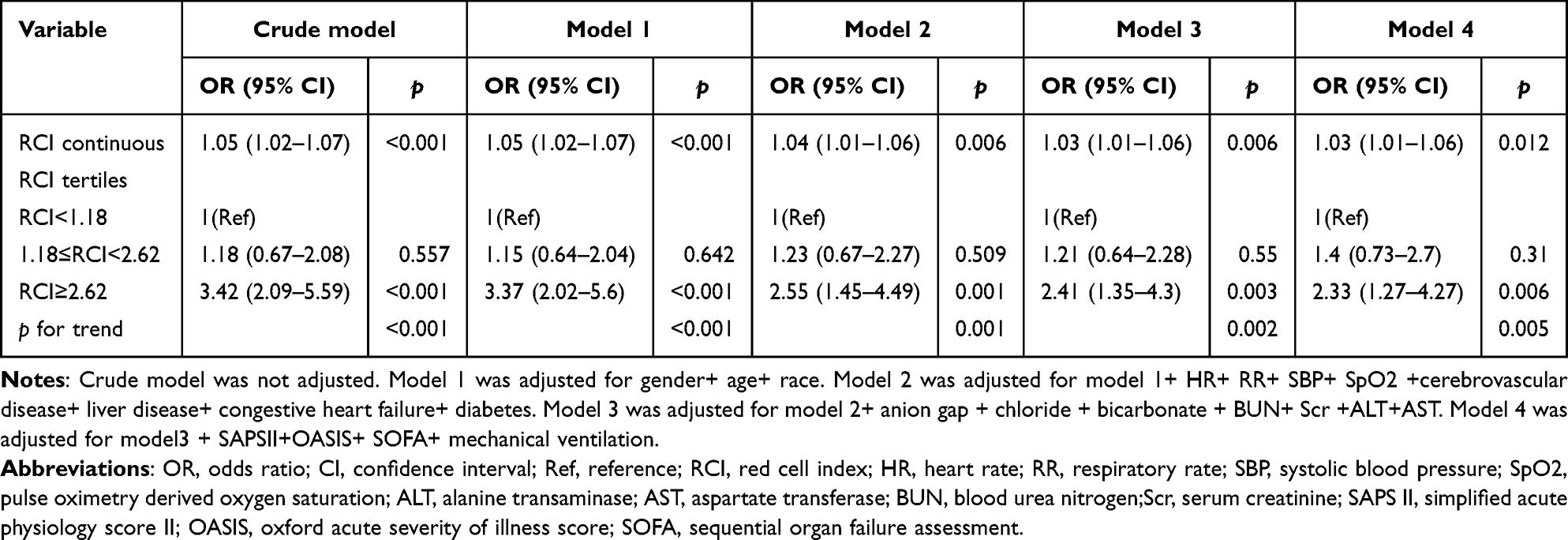 |
Table 3 Relationship Between Red Cell Index and Hospital Mortality in Different Models |
Subgroup Analyses and Sensitivity Analyses
To evaluate the underlying clinical heterogeneity, we used interaction and stratified analysis. We used subgroups and interactive analyses according to age (<65 and ≥65 years), sofa score (<4 and ≥4), diabetes mellitus (No and Yes), cerebrovascular disease (No and Yes), congestive heart failure (No and Yes), mechanical ventilation (No and Yes) (Figure 2). Effect size of RCI on the hospital mortality in subgroups were stable. No significant interactions were observed in the subgroups (all p for interaction > 0.05).
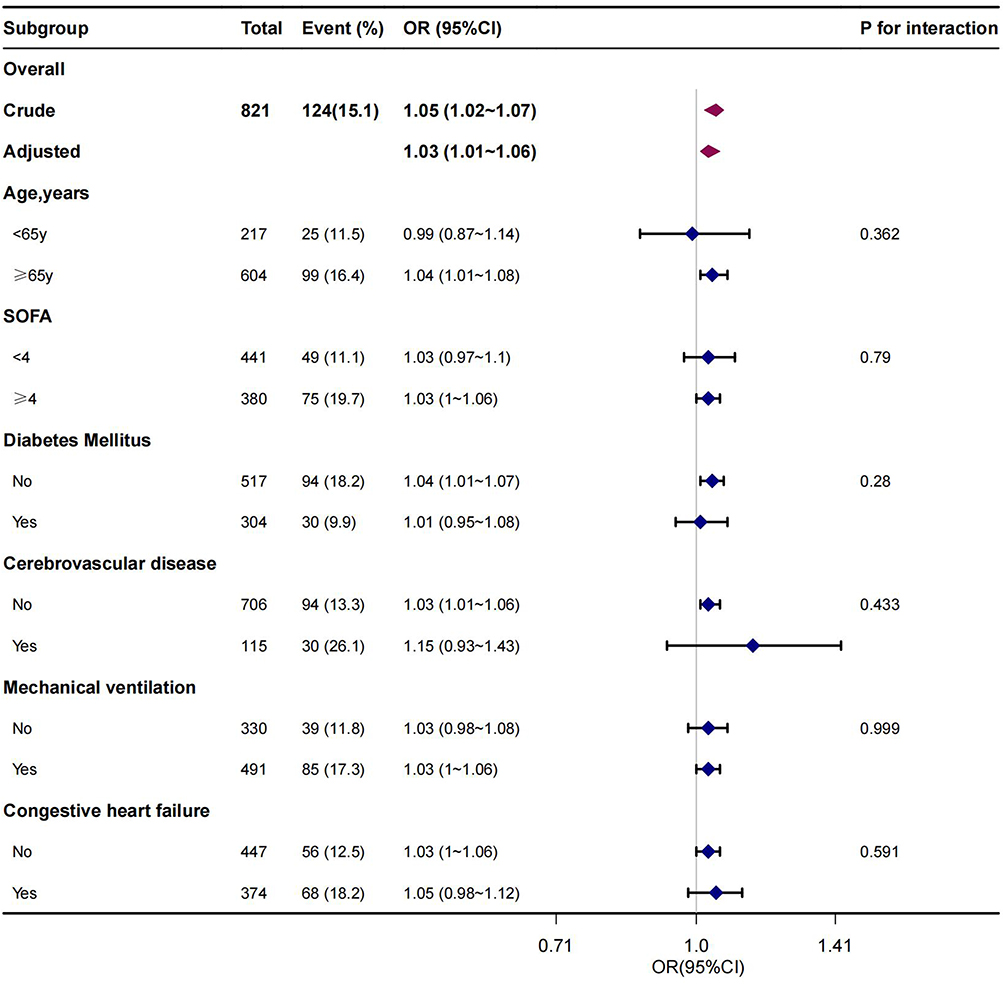 |
Figure 2 Forest plot of association between red cell index (RCI) and hospital mortality. Crude: unadjusted; Adjusted: adjusted for gender, age, race, HR, RR, SBP, SpO2, cerebrovascular disease, liver disease, congestive heart failure, diabetes, anion gap, chloride, bicarbonate, BUN, Scr, ALT, AST, APSII, OASIS, SOFA, mechanical ventilation. Abbreviations: OR, odds ratio; CI, confidence interval; HR, heart rate; RR, respiratory rate; SBP, systolic blood pressure; SpO2, pulse oximetry derived oxygen saturation; BUN, blood urea nitrogen; Scr, serum creatinine; ALT, alanine transaminase; AST, aspartate transferase; SAPS II, simplified acute physiology score II; OASIS, oxford acute severity of illness score; SOFA, sequential organ failure assessment. |
Sensitivity analysis was further performed with variable deletion for missing values, and then multivariate analysis was performed with a non-missing population, and the results are in Table S1.
Discussion
For the first time, to our knowledge, this retrospective cohort study indicated that high levels of RCI were positively correlated with hospital mortality in severe COPD patients in the ICU. In fully adjusted model 4, the effect value was 1.03 (95% CI: 1.01–1.06), indicating that the risk of hospital mortality increases by 3% for per unit increase in RCI. When RCI was turned into categorical variable, the result was stable and reliable, while the results were stable in all subgroups without any interaction.
RCI is a relatively recent and complex marker that combines hemoglobin, platelet, lymphocyte, and RBC. Being calculated by trusted formulas, which are more stable and have more accurate prognostic results than a single blood parameter. RCI could provide researchers with a more accurate assessment of disease severity.7 Hb is an iron-containing metalloprotein that transports oxygen, and red blood cells carry Hb and play an important role in delivering oxygen to tissues.18 RBC and Hb levels compensate for low lung function and reflect sensitivity to hypoxia.19 In cases of poor pulmonary function, increased RBC and Hb levels can act as compensatory mechanisms.20 However, some studies have reported that anemia might be more common in COPD patients.21,22 and anemia increased mortality in COPD.23,24 Our current study observed that higher RBC and Hb levels in the higher RCI group. The reason could be due to severe COPD has associated with secondary polycythemia and which contributes to the development of pulmonary heart disease and pulmonary hypertension, linked to poor prognosis.25,26
Lymphopenia has been related to poor outcome in acute inflammatory diseases.27 It has been shown that lymphocyte counts were lower in patients with COPD than healthy controls.28 Furthermore, lymphocytopenia has been related to all-cause mortality in COPD patients.29–31 In our study, we identified that lymphocyte count in the higher RCI group is lower in patients with severe COPD. Similar study found an association between a low relatively lymphocyte count and high mortality among elderly patients with COPD32 An immune response characteristic of lymphocytes is likely to explain the lymphocyte’s influence on COPD. Although platelet counts in COPD patients is unclear extensively, thrombocytopenia has been reported in COPD patients and has been associated with poor outcomes and increased mortality.33 Consistent with these findings, we also found lower platelet counts in the higher RCI group. Since lymphocytes and platelets tend to be little affected by other factors, they are used as benchmarks for measuring the total permeability of a blood cell.
Previously, the RCI index was widely recognized as an effective measure for evaluating lung function and severity of COPD.6,7 Other study demonstrated that RCI was significantly associated with 3-month mortality in among acute ischemic stroke (AIS) patients treated with recombinant tissue plasminogen activator (r-tPA).9 This study is the first to explore the connection of RCI and hospital mortality in COPD patients being treated in ICU. RCI, which is based on the complete blood count parameter, is easier to obtain and identify critically ill patients early and thus to reduce the burden of disease and mortality. The data for the study come from large public databases, the sample size is large and the results will be compelling. Additionally, after multiple adjustment of covariates, the result was still stable and higher RCI levels are associated with mortality. Patients with chronic obstructive pulmonary disease (COPD) will have varying degrees of pulmonary dysfunction, especially critically ill patients admitted to the ICU, however, the use of RCI allows for the assessment of the patient’s pulmonary functional status and prognosis.
However, our study also has some limitations. Firstly, it is impossible to account for all confounding variables in a retrospective cohort study. Despite attempts to adjust for known confounding factors, there may still be some unmeasured variables impacting the results. Furthermore, since not all variables are tracked in MIMIC-IV, certain indicators such as pulmonary function are missing which may have an impact on our results. Secondly, we excluded patients aged <18 years. Therefore, our findings cannot be generalized to these patients. Thirdly, the ALT, AST, and SOFA data for covariates were missing about 40% of the participants. However, we employed multiple interpolation to address the challenges presented by the missing data. What’s more, we utilized multivariate regression analysis after removing the missing values, the obtained results remained robust. Finally, it is important to note that our study did not involve mechanistic studies, and future research must delve deeper into the underlying mechanisms to further elucidate the results.
Conclusion
RCI was positively correlated with hospital mortality. Higher RCI value was associated with higher risk of hospital mortality in COPD patients admitted to the ICU. Nevertheless, it is crucial to conduct rigorously planned, prospective, and multicenter studies to validate our results in the future.
Acknowledgments
Thanks to all the authors of this article. We are also thankful to J. Liu (People’s Liberation Army of China General Hospital, Beijing, China) for his help in revision.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/S0140-6736(22)00470-6
2. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011
3. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
4. MacLeod M, Papi A, Contoli M, et al. Chronic obstructive pulmonary disease exacerbation fundamentals: diagnosis, treatment, prevention and disease impact. Respirology. 2021;26(6):532–551. doi:10.1111/resp.14041
5. Funk GC, Bauer P, Burghuber OC, et al. Prevalence and prognosis of COPD in critically ill patients between 1998 and 2008. Eur Respir J. 2013;41(4):792–799. doi:10.1183/09031936.00226411
6. Guang Y, Jie Z, Feng D, et al. Surrogate scale for evaluating respiratory function based on complete blood count parameters. J Clin Lab Anal. 2018;32(5):e22385. doi:10.1002/jcla.22385
7. Huang Y, Wang J, Shen J, et al. Relationship of red cell index with the severity of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2021;16:825–834. doi:10.2147/COPD.S292666
8. Babaoglu E, Ulasli SS. Clinical importance of red cell distribution width and red cell index in pulmonary embolism. Eur Rev Med Pharmacol Sci. 2023;27(9):4108–4115. doi:10.26355/eurrev_202305_32319
9. Qian M, Zhou X, Gao B, et al. Red cell index: a novel biomarker for 3-month mortality in acute ischemic stroke patients treated with intravenous thrombolysis. Brain Behav. 2021;11(6):e02170. doi:10.1002/brb3.2170
10. Yuan FZ, Shui W, Xing Y-L, et al. Association of red cell index and adverse hospitalization outcomes in chronic obstructive pulmonary disease patients with acute exacerbation: a retrospective cohort study. Int J Chron Obstruct Pulmon Dis. 2022;17:2263–2275. doi:10.2147/COPD.S373114
11. Johnson AEW, Bulgarelli L, Shen L, et al. MIMIC-IV, a freely accessible electronic health record dataset. Sci Data. 2023;10(1):1. doi:10.1038/s41597-022-01899-x
12. Guo X, Lin H, Guo D, et al. Azithromycin use prior to ICU admission is associated with a lower short-term mortality for critically ill acute exacerbations of chronic obstructive pulmonary disease patients: a retrospective cohort study. Chron Respir Dis. 2022;19:14799731221140797. doi:10.1177/14799731221140797
13. Qiu Y, Wang Y, Shen N, et al. Association between red blood cell distribution width-albumin ratio and hospital mortality in chronic obstructive pulmonary disease patients admitted to the intensive care unit: a retrospective study. Int J Chron Obstruct Pulmon Dis. 2022;17:1797–1809. doi:10.2147/COPD.S371765
14. Ling M, Huiyin L, Shanglin C, et al. Relationship between human serum albumin and in-hospital mortality in critical care patients with chronic obstructive pulmonary disease. Front Med. 2023;10:1109910. doi:10.3389/fmed.2023.1109910
15. Yang Q, Zheng J, Chen W, et al. Association between preadmission metformin use and outcomes in intensive care unit patients with sepsis and type 2 diabetes: a cohort study. Front Med. 2021;8:640785. doi:10.3389/fmed.2021.640785
16. Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
17. Austin PC, White IR, Lee DS, et al. Missing data in clinical research: a tutorial on multiple imputation. Can J Cardiol. 2021;37(9):1322–1331. doi:10.1016/j.cjca.2020.11.010
18. Tariq S, Ismail D, Thapa M, et al. Chronic obstructive pulmonary disease and its effect on red blood cell indices. Cureus. 2023;15(3):e36100. doi:10.7759/cureus.36100
19. Xu L, Chen Y, Xie Z, et al. High hemoglobin is associated with increased in-hospital death in patients with chronic obstructive pulmonary disease and chronic kidney disease: a retrospective multicenter population-based study. BMC Pulm Med. 2019;19(1):174. doi:10.1186/s12890-019-0933-4
20. Santos MC, Oliveira AL, Viegas-Crespo AM, et al. Systemic markers of the redox balance in chronic obstructive pulmonary disease. Biomarkers. 2004;9(6):461–469. doi:10.1080/13547500400024768
21. Hoepers AT, Menezes MM, Fröde TS. Systematic review of anaemia and inflammatory markers in chronic obstructive pulmonary disease. Clin Exp Pharmacol Physiol. 2015;42(3):231–239. doi:10.1111/1440-1681.12357
22. Similowski T, Agusti A, MacNee W, et al. The potential impact of anaemia of chronic disease in COPD. Eur Respir J. 2006;27(2):390–396. doi:10.1183/09031936.06.00143704
23. Ergan B, Ergün R. Impact of anemia on short-term survival in severe COPD exacerbations: a cohort study. Int J Chron Obstruct Pulmon Dis. 2016;11:1775–1783. doi:10.2147/COPD.S111758
24. Toft-Petersen AP, Torp-Pedersen C, Weinreich UM, et al. Association between hemoglobin and prognosis in patients admitted to hospital for COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:2813–2820. doi:10.2147/COPD.S116269
25. Criner GJ. Effects of long-term oxygen therapy on mortality and morbidity. Respir Care. 2000;45(1):105–118.
26. Vlahakos V, Marathias K, Lionaki S, et al. The paradigm shift from polycythemia to anemia in COPD: the critical role of the renin-angiotensin system inhibitors. Expert Rev Respir Med. 2022;16(4):391–398. doi:10.1080/17476348.2022.2045958
27. Drewry AM, Samra N, Skrupky LP, et al. Persistent lymphopenia after diagnosis of sepsis predicts mortality. Shock. 2014;42(5):383–391. doi:10.1097/SHK.0000000000000234
28. Şahin F, Koşar AF, Aslan AF, et al. Serum biomarkers in patients with stable and acute exacerbation of chronic obstructive pulmonary disease: a comparative study. J Med Biochem. 2019;38(4):503–511. doi:10.2478/jomb-2018-0050
29. Günay E, Sarınç Ulaşlı S, Akar O, et al. Neutrophil-to-lymphocyte ratio in chronic obstructive pulmonary disease: a retrospective study. Inflammation. 2014;37(2):374–380. doi:10.1007/s10753-013-9749-1
30. Sørensen AK, Holmgaard DB, Mygind LH, et al. Neutrophil-to-lymphocyte ratio, calprotectin and YKL-40 in patients with chronic obstructive pulmonary disease: correlations and 5-year mortality - a cohort study. J Inflamm. 2015;12(1):20. doi:10.1186/s12950-015-0064-5
31. Cao Y, Xing Z, Long H, et al. Predictors of mortality in COPD exacerbation cases presenting to the respiratory intensive care unit. Respir Res. 2021;22(1):77. doi:10.1186/s12931-021-01657-4
32. Acanfora D, Scicchitano P, Carone M, et al. Relative lymphocyte count as an indicator of 3-year mortality in elderly people with severe COPD. BMC Pulm Med. 2018;18(1):116. doi:10.1186/s12890-018-0685-6
33. Rahimi-Rad MH, Soltani S, Rabieepour M, et al. Thrombocytopenia as a marker of outcome in patients with acute exacerbation of chronic obstructive pulmonary disease. Pneumonol Alergol Pol. 2015;83(5):348–351. doi:10.5603/PiAP.2015.0056
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.