")
Back to Journals » International Journal of General Medicine » Volume 16
Association of Plasma Lipids with White Matter Hyperintensities in Patients with Acute Ischemic Stroke
Authors Liu Y, Yuan C, Chen X, Fang X, Hao J, Zhou M, Sun X, Wu M , Wang Z
Received 16 September 2023
Accepted for publication 13 November 2023
Published 21 November 2023 Volume 2023:16 Pages 5405—5415
DOI https://doi.org/10.2147/IJGM.S440655
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yongkang Liu,1 Cuiping Yuan,1 Xiao Chen,1 Xiaokun Fang,1 Jingru Hao,1 Maodong Zhou,1 Xin Sun,1 Minghua Wu,2 Zhongqiu Wang1
1Department of Radiology, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, 210029, People’s Republic of China; 2Department of Encephalopathy Center, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, 210029, People’s Republic of China
Correspondence: Zhongqiu Wang, Department of Radiology, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, 210029, People’s Republic of China, Tel/Fax +86 25-86618472, Email [email protected] Minghua Wu, Department of Encephalopathy Center, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, 210029, People’s Republic of China, Tel/Fax +86 25-86618472, Email [email protected]
Purpose: White matter hyperintensities (WMH) are the common marker of cerebral small vessel disease (CSVD). Dyslipidemia plays a notable role in the pathogenesis of CSVD. However, the relationship between dyslipidemia and WMH is poorly elucidated. This study aims to investigate the association between serum lipid fractions and WMH in patients with acute ischemic stroke (AIS).
Patients and Methods: A total of 901 patients with AIS were included in this study. The burden of WMH, including deep white matter hyperintensities (DWMH), periventricular white matter hyperintensities (PVWMH), and total WMH load, were evaluated on magnetic resonance imaging (MRI) by the Fazekas scale. All the WMH burden were set as dichotomous variables. Serum levels of triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-c), and high-density lipoprotein cholesterol (HDL-c) were collected. The association of serum lipid fractions with WMH burden was analyzed using univariate and multivariate logistic regression models.
Results: The average age of the participants was 67.6± 11.6 years, and 584 cases (64.8%) were male. About 33.5% (n = 302) patients were smoker, and 23.5% (n = 212) patients had a history of alcohol consumption. The proportion of previous diabetes, ischemic cardiomyopathy and hypertension was 39.0% (n = 351), 21.2% (n = 191) and 75.9% (n = 684), respectively. The average of serum HDL-c, TC, TG, LDL-c levels for all participants were 1.26 ± 0.28 mmol/l, 4.54 ± 1.06 mmol/l, 1.67 ± 1.09 mmol/l, 3.08 ± 0.94 mmol/l. There were no statistical associations between HDL-c, TG, TC, LDL-c and each type of WMH burden (P > 0.05) in multivariate logistic regression analysis. Similar findings were found in subgroup analysis based on gender classification.
Conclusion: Serum lipid levels were not associated with the presence of any type of WMH in patients with AIS.
Keywords: white matter hyperintensities, HDL-c, triglyceride, total cholesterol, LDL-c, acute ischemic stroke
Introduction
Cerebral small vessel disease (CSVD) is a familiar progressive cerebral microvessels disorder that causes about a quarter of acute strokes and 45% of dementia cases.1 The typical neuroimaging phenotypes of CSVD include recent small subcortical infarcts, lacunes, white matter hyperintensities (WMH), enlarged perivascular spaces (EPVS), cerebral microbleeds (CMBs), and brain atrophy.2 As the most common marker of CSVD, WMH contributed notably to stroke risk as well as associated physical, psychological, and cognitive impairments.3–5 However, the pathogenesis of WMH is still poorly elucidated.
WMH is considered as an important feature of CSVD, reflecting abnormalities of the white matter. Increasing evidences have suggested that WMH strongly correlated with clinical outcomes, and the severity of WMH can usually be quantitative and qualitative assessed on brain magnetic resonance imaging (MRI). According to the Fazekas rating scale, the burden of WMH was divided into deep white matter hyperintensities (DWMH), periventricular white matter hyperintensities (PVWMH), which was graded from 0 to 3, respectively, and the total load of WMH was graded from 0 to 6.6 In addition, WMH segmentations can be carried out using automatic or semi-automatic software for quantitative WMH volume calculation.7
Dyslipidemia is a well-established risk factor of atherosclerosis, coronary artery disease and stroke.8 Nevertheless, it’s role in CSVD, especially in WMH remains unclear. Association of serum lipid fractions such as high-density lipoprotein cholesterol (HDL-c), low-density lipoprotein cholesterol (LDL-c), total cholesterol (TC) and triglyceride (TG) with WMH is controversial. Some researches found that hypertriglyceridemia (hyper-TG) rather than HDL-c, LDL-c, TC was associated with risk of WMH.9 High triglycerides levels were associated with larger WMH volume in 3C-Dijon Study and the EVA Study, while increasing LDL-c appeared to be associated with a decreased risk of CSVD markers.10 Yet, in a Mendelian randomization study, genetic predisposition to higher HDL-c correlated with the lower WMH volume, which was considered for the prevention of ischaemic CSVD.11 These unconsensus results hint that further studies are needed to explore the association of serum lipid fractions with WMH. In addition, few study has shown the serum lipid levels and WMH in patients with stroke. Although stroke was the second-leading cause of death and the incidence and mortality due to stroke increased substantially from 1990 to 2019.12 While in China, stroke has become the leading cause of death and disability since 2015.13,14 Exploring the relationship between serum lipid fractions with WMH in stroke subjects can facilitate the optimization of strategies for stroke prevention and treatment.
In this study, we investigated the link between the four lipid profiles (HDL-c, LDL-c, TG, TC) and WMH burden, including deep white matter hyperintensities (DWMH), periventricular white matter hyperintensities (PVWMH), and total WMH burden (Fazekas scale) in acute ischemic stroke (AIS) patients.
Materials and Methods
Patients
This retrospective cohort study was approved by the Ethics Committee of the Affiliated Hospital of Nanjing University of Chinese Medicine (2017NL-012-01). Informed consent was waived because of the retrospective design. One thousand eight hundred and thirty-five AIS patients who admitted to the Encephalopathy Center of our hospital from January 1, 2019, to July 31, 2021, were selected in our database. The inclusion criteria are as follows: 1) AIS diagnosis confirmed on diffusion weighted imaging (DWI) at admission, 2) >40 years, 3) native Chinese population. The demographics, clinical information, biochemical results and radiological data were collected from medical records. Those patients with incomplete medical information, with previous history of dementia, psychiatric illness, head surgery and younger than 40 years were not included for analyses (n = 447). And 487 patients with previous stroke were excluded. Finally, a total of 901 patients were enrolled in the current study. A flowchart showing the patient selection is shown in Figure 1. All the patients received regular pharmacotherapy, for instance, antiplatelet, anticoagulants, statin therapy. Some patients with large vessel occlusion underwent thrombolysis or thrombolysis therapy. During the study, patient data confidentiality and compliance with the Declaration of Helsinki were followed.
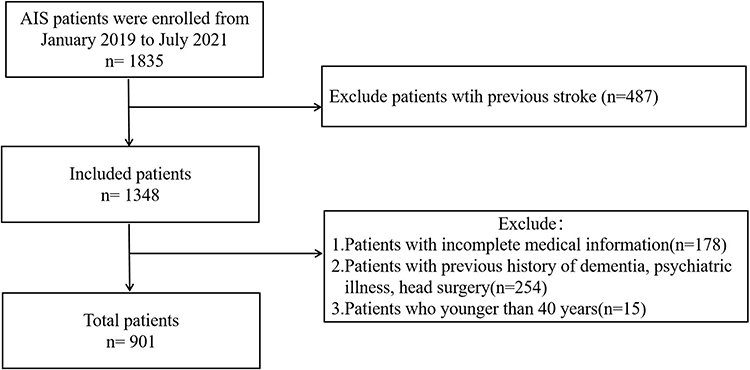 |
Figure 1 Flowchart showing the patient selection. |
Baseline Data Collection
We collected the baseline characteristics including subject demographics (age, sex), vascular risk factors (blood pressure, drinking and smoking history), medical history (hypertension, diabetes, heart disease, and stroke). Hypertension was defined as systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg or use of antihypertensive agents. Diabetes was defined as self-reported disease, use of antidiabetic agents, or nonfasting plasma glucose ≥11.1 mmol/L. Ischemic cardiomyopathy was considered if there was a history of coronary heart disease, angina or myocardial infarction. History of cerebral stroke was also recorded. Smoker or drinker was defined as a history of cigarette or alcohol taking in the past. Recent stroke severity was assessed using NIHSS score after admission by two experienced neurologists who were blind to this study. When there was a disagreement for the NIHSS evaluation, they made a consensus through negotiations.
Measurement of Serum Lipid Fractions
Samples of venous blood were obtained within 24 h of admission. The first test was used for analysis if patients who were conducted more than once. The levels of serum TC, TG, HDL-c, LDL-c were measured by enzymatic methods (Boehringer Mannheim, Mannheim, Germany). Dyslipidemia was defined according to 2016 Chinese guidelines for the management of dyslipidemia in adults. Serum lipid levels were set as continuous variables.
MRI Acquisition and Assessment
Participants were scanned in a 1.5 T whole-body scanner (GE Signa Excite II, GE Medical Systems) or 3.0 T whole-body scanner (Siemens, Germany) within 7 days after stroke. The imaging sequences consisted of axial diffusion-weighted imaging (DWI), axial apparent diffusion coefficient (ADC), axial T1-weighted imaging (T1WI), axial T2-weighted imaging (T2WI), and coronal fluid-attenuated inversion recovery (FLAIR) imaging with a slice thickness of 5 mm.
The major MRI marker of CSVD, WMH was defined based on the Standards for Reporting Vascular Changes on Neuroimaging Criteria. WMH burden was assessed separately on FLAIR and T2WI sequences and was graded according to the Fazekas scale,15 which classified lesions into 0 to 3 grades depending on the size and confluence of lesions in both areas. Then, both DWMH and PVWMH were classified into low-burden (0–1 point) and high-burden (2–3 point). The total Fazekas score was classified into low-burden (0–2 point) and high-burden (3–6 point). Figure 2 showed sample images of WMH grade.
 |
Figure 2 (A–H) Sample images of WMH grade. A 53 years male patient with DWMH grade 0 and PVWMH grade 1 (A and B); A 60 years male patient with DWMH grade 1 and PVWMH grade 1 (C and D); A 55 years male patient with DWMH grade 2 and PVWMH grade 2 (E and F); A 86 years female patient with DWMH grade 3 and PVWMH grade 3 (G and H). A, C, E, G are axial T2WI images; B, D, F, H are coronal FLAIR images. |
Statistical Analysis
The Statistical Package for the Social Sciences (SPSS, ver. 20.0; SPSS Inc., Chicago, IL, USA) was applied for all analyses. Independent-samples T-test or Mann–Whitney U-test was used to compare the continuous variables. Chi-squared test was used to compare the categorical variables. Univariate and multivariate logistic regression analyses were utilized to evaluate the association between serum lipids levels and WMH burden in all AIS patients. Age, sex, previous history, admission NIHSS and other lipid fractions were set as confounding factors. Furthermore, subgroup analysis based on gender classification was performed respectively. Values of P < 0.05 was considered statistically significant.
Results
The Characteristics of AIS patients are shown in Table 1. A total of 901 consecutive AIS patients (age: 67.6 ± 11.6 years (mean ± standard deviation)) were recruited into this study in which 64.8% of them were male. About 302 (33.5%) patients were smoker, and there were 212 (23.5%) patients with a history of alcohol consumption. The proportion of previous diabetes, ischemic cardiomyopathy and hypertension was 39.0% (n = 351), 21.2% (n = 191) and 75.9% (n = 684), respectively. The average of serum HDL-c, TC, TG, LDL-c levels for all participants were 1.26 ± 0.28 mmol/l, 4.54 ± 1.06 mmol/l, 1.67 ± 1.09 mmol/l, 3.08 ± 0.94 mmol/l, respectively.
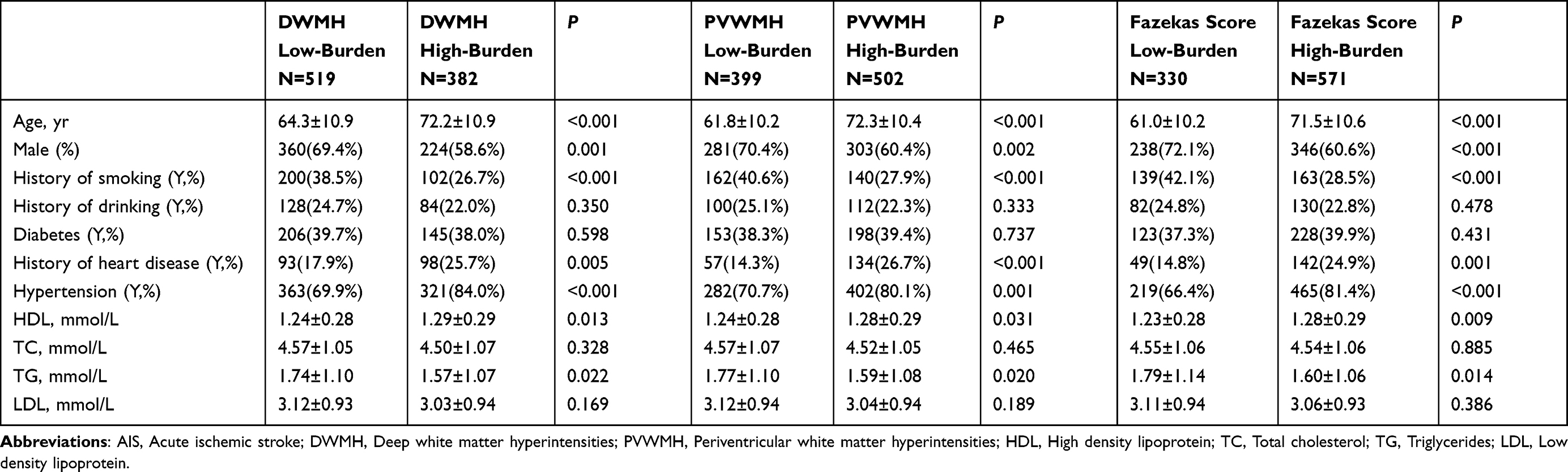 |
Table 1 Characteristics of AIS Patients without Previous Stroke |
Univariate analyses showed that HDL-c level was significantly linked with DWMH (Odds ratio (OR) = 1.809, 95% confidence interval (CI): 1.133–2.887) (Table 2), PVWMH (OR = 1.673, 95% CI: 1.047–2.674) (Table 3) and total WMH burden (OR = 1.922, 95% CI: 1.178–3.135) (Table 4). After adjustment for the confounding factors, these associations disappeared. Similar findings were observed in TG (Tables 1–4). There were no statistical associations between TC, LDL-c levels and the burden of DWMH, PVWMH and Fazekas score (Tables 1–4).
 |
Table 2 Associated Factors of DWMH Burden |
 |
Table 3 Associated Factors of PVWMH Burden |
 |
Table 4 Associated Factors of Total WMH Burden (Fazekas Score) |
Then, subgroup analysis was performed based on different gender. Age, previous history (including smoking, alcohol drinking, diabetes, ischemic cardiomyopathy, hypertension), admission NIHSS and other lipid fractions levels were considered as confounding factors. In both subgroups, there were no significant correlations between serum lipid profiles and each WMH burden (Tables 5 and 6).
 |
Table 5 Multivariate Logistic Regression Analysis in Male AIS Patients |
 |
Table 6 Multivariate Logistic Regression Analysis in Female AIS Patients |
Discussion
Few studies have shown the associations between serum lipid levels and CSVD. However, the results remain conflict and such association in patients with acute ischemic stroke is still unclear. In the current study, we found that none of the serum lipids (HDL-c, TC, TG, LDL-c) were associated with each type of WMH burden including DWMH, PVWMH and total WMH load in patients with acute ischemic stroke. The similar findings were observed in subgroup analysis. There were no correlations between serum lipids and WMH neither in male nor in female AIS patients.
Low HDL is a well-known risk factor for large artery atherosclerosis. However, findings about the relationship of HDL-c with WMH were rare and unconsensus. In a cross-sectional study comprising a total of 1270 consecutive patients with first ever ischemic stroke, HDL-c was not associated with leukoaraiosis.9 Similarly, no significant association of HDL-c with WMH and lacunes was observed in 2 large French population-based studies,10 and the findings were consistent in participants taking and without taking lipid-lowering drugs. In a study consisting of three independent cohorts, Leeuw et al meta-analyzed the relationship of 143 metabolites with cerebral atrophy and WMH, they found that the higher glucose levels were linked with WMH, rather than the HDL-c.16 These studies are in line with our findings. The current study showed that HDL-c was positively associated with any type of WMH burden in univariable analysis but not in multivariable analysis. However, in a large-scale Mendelian randomization study, genetic predisposition to higher HDL-c, especially to medium-sized high-density lipoprotein particles, was linked with lower WMH volume, which indicated that HDL-c raising strategies could be a potential candidate for the prevention of CSVD.11 However, this study is based on general population rather than AIS patients. Those AIS patients probably had overestimated WMH load for acute cerebral edema. In addition, our study did not quantitatively calculated the WMH volume. The association between HDL-c and WMH volume was not investigated. The potential mechanisms underlying the correlation of HDL-c with WMH were still hypothetical. HDL-c is involved in regulating the vascular smooth muscle cells (VSMC) function, preserving the integrity of the blood–brain barrier (BBB), which prevents the formation of WMH.17–19
Our study showed negatively correlation between TG and three types of WMH burden in univariate analysis. However, these associations disappeared after adjusting the confounding factors. Actually, the relationship between TG and leukoaraiosis severity is still controversial. In a French population-based study, Schilling found increasing triglycerides correlated with larger volume of WMH.8 Similar findings were observed in healthy subjects with no history of stroke.20 However, in a study comprise recent first lacunar infarct patients, hyper-TG showed a protective effect on WMH load.7 In another study, no statistical correlation was found between TG and WMH burden,13 which is in line with our findings. Possible mechanisms of TG involved in WMH may be the characteristic that myelin contains 70% lipids.21 Additionally, shared genetic burden is a considerable explanation.22 Future studies are need to explore the relationship between TG levels and leukoaraiosis.
Several studies reported potential correlation between other lipid fractions and WMH. In some studies, LDL-c levels showed negatively relationship with WMH,23,24 and higher visit-to-visit variability in LDL-c was associated with greater WMH load.10,25 Several studies did not report any association between LDL cholesterol and WMH.26,27 Few studies focused on the link between TC and WMH. In a group of patients with Fabry disease (FD), Stefaniak found that increasing TC was correlated with slower WMH progression, and researchers thought that this unexpected finding might be due to “survivor bias”.28 Interestingly, another study showed that TC mediated about 30% of the effect of simvastatin on WM microstructure.29 However, in a recent first lacunar infarct population, hypertriglyceridemia, rather than other lipid profiles, was associated with the severity of leukoaraiosis.9 While in a Mendelian randomization study, no relationship was found between WMH and LDL-c, TG, or TC,10 which is in agreement with our findings. These results need to be further examined in other population-based studies.
Our study has some limitations. The first is that all participators in this cross-sectional design were in a single medical center, and the sample is limited in Chinese population, which might not be suitable for other ethnicities. Second, selection bias might exist because only patients with MRI examinations were included. Third, visual rating scale rather than quantitative means was used for WMH assessment, and only dichotomous levels were adopted to characterize WMH burden. Fourth, some studies have shown the association between serum lipids levels and prognosis of stoke.30,31 The associations between WMH and stroke prognosis were also reported in some studies.32,33 In our study, we did not perform such analysis. Finally, the association between lipids level and WMH may be influenced by lipid-lowering drugs; however, detailed information such as drug dosages or species was not recorded in the current study.
Conclusion
In conclusion, in this retrospective study comprise patients with AIS, we found that serum lipids fractions were not associated with any type of WMH burden. Similar findings were observed in subgroup analysis based on gender classification. For patients with AIS, the relationship between serum lipid fractions and the WMH need to be further studied.
Data Sharing Statement
The datasets generated are available from the corresponding author (Zhongqiu Wang) on reasonable request.
Ethical Approval and Consent to Participate
This study was approved by the Ethics Board of the Affiliated Hospital of Nanjing University of Chinese Medicine (2017NL-012-01). Informed consent was waived because the retrospective design. During the study, patient data confidentiality and compliance with the Declaration of Helsinki were followed.
Acknowledgments
The authors would like to thank JinLuan Cui for her help in the clinical data collection.
Funding
This work was supported by the National Administration of Traditional Chinese Medicine: Evidence-Based Capacity Building Project (No. 2019XZZX-NB007).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cannistraro RJ, Badi M, Eidelman BH, et al. CNS small vessel disease: a clinical review. Neurology. 2019;92:1146–1156. doi:10.1212/WNL.0000000000007654
2. Wardlaw JM, Smith EE, Biessels GJ, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013;12:822–838. doi:10.1016/S1474-4422(13)70124-8
3. Sargurupremraj M, Suzuki H, Jian X, et al. Cerebral small vessel disease genomics and its implications across the lifespan. Nat Commun. 2020;11:6285. doi:10.1038/s41467-020-19111-2
4. Clancy U, Gilmartin D, Jochems ACC, et al. Neuropsychiatric symptoms associated with cerebral small vessel disease: a systematic review and meta-analysis. Lancet Psychiatry. 2021;8:225–236. doi:10.1016/S2215-0366(20)30431-4
5. Hu HY, Ou YN, Shen XN, et al. White matter hyperintensities and risks of cognitive impairment and dementia: a systematic review and meta-analysis of 36 prospective studies. Neurosci Biobehav Rev. 2021;120:16–27.
6. Zhang Y, Zhang GY, Zhang ZE, He AQ, Gan J, Liu Z. White matter hyperintensities: a marker for apathy in Parkinson’s disease without dementia? Ann Clin Transl Neurol. 2020;7(9):1692–1701. doi:10.1002/acn3.51159
7. de Kort FAS, Coenen M, Weaver NA, et al. White matter hyperintensity volume and poststroke cognition: an individual patient data pooled analysis of 9 ischemic stroke cohort studies. Stroke. 2023. doi:10.1161/STROKEAHA.123.044297
8. Kopin L, Lowenstein C. Dyslipidemia. Ann Intern Med. 2017;167:Itc81–Itc96. doi:10.7326/AITC201712050
9. Ke D, Zhou F, Liang H, et al. Hypertriglyceridemia is associated with reduced leukoaraiosis severity in patients with a small vessel stroke. Behav Neurol. 2018;2018:1361780. doi:10.1155/2018/1361780
10. Schilling S, Tzourio C, Dufouil C, et al. Plasma lipids and cerebral small vessel disease. Neurology. 2014;83:1844–1852. doi:10.1212/WNL.0000000000000980
11. Georgakis MK, Malik R, Anderson CD, et al. Genetic determinants of blood lipids and cerebral small vessel disease: role of high-density lipoprotein cholesterol. Brain. 2020;143:597–610. doi:10.1093/brain/awz413
12. GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795–820. doi:10.1016/S1474-4422(21)00252-0
13. Tu WJ, Wang LD. China stroke surveillance report 2021. Mil Med Res. 2023;10(1):33. doi:10.1186/s40779-023-00463-x
14. Tu WJ, Zhao Z, Yin P, et al. Estimated burden of stroke in China in 2020. JAMA Netw Open. 2023;6(3):e231455. doi:10.1001/jamanetworkopen.2023.1455
15. Fazekas F, Kleinert R, Offenbacher H, et al. Pathologic correlates of incidental MRI white matter signal hyperintensities. Neurology. 1993;43:1683–1689. doi:10.1212/WNL.43.9.1683
16. de Leeuw FA, Karamujić-čomić H, Tijms BM, et al. Circulating metabolites are associated with brain atrophy and white matter hyperintensities. Alzheimers Dement. 2021;17:205–214. doi:10.1002/alz.12180
17. Martínez-González J, Escudero I, Badimon L. Simvastatin potenciates PGI(2) release induced by HDL in human VSMC: effect on Cox-2 up-regulation and MAPK signalling pathways activated by HDL. Atherosclerosis. 2004;174:305–313. doi:10.1016/j.atherosclerosis.2004.01.037
18. Keul P, Polzin A, Kaiser K, et al. Potent anti-inflammatory properties of HDL in vascular smooth muscle cells mediated by HDL-S1P and their impairment in coronary artery disease due to lower HDL-S1P: a new aspect of HDL dysfunction and its therapy. FASEB J. 2019;33:1482–1495. doi:10.1096/fj.201801245R
19. Tran-Dinh A, Levoye A, Couret D, et al. High-density lipoprotein therapy in stroke: evaluation of endothelial SR-BI-dependent neuroprotective effects. Int J Mol Sci. 2020;22(1):106. doi:10.3390/ijms22010106
20. Park K, Yasuda N, Toyonaga S, et al. Significant association between leukoaraiosis and metabolic syndrome in healthy subjects. Neurology. 2007;69:974–978. doi:10.1212/01.wnl.0000266562.54684.bf
21. Schmitt S, Castelvetri LC, Simons M. Metabolism and functions of lipids in myelin. Biochim Biophys Acta. 2015;1851:999–1005. doi:10.1016/j.bbalip.2014.12.016
22. Atwood LD, Wolf PA, Heard-Costa NL, et al. Genetic variation in white matter hyperintensity volume in the Framingham Study. Stroke. 2004;35:1609–1613. doi:10.1161/01.STR.0000129643.77045.10
23. Chung C-P, Chou K-H, Peng L-N, et al. Associations between low circulatory low-density lipoprotein cholesterol level and brain health in non-stroke non-demented subjects. Neuroimage. 2018;181:627–634. doi:10.1016/j.neuroimage.2018.07.049
24. Duan D, Shen L, Cui C, et al. Association between low-density lipoprotein cholesterol and occipital periventricular hyperintensities in a group of Chinese patients: an observational study. Lipids Health Dis. 2017;16:48. doi:10.1186/s12944-017-0436-3
25. Smit RA, Trompet S, Sabayan B, et al. Higher visit-to-visit low-density lipoprotein cholesterol variability is associated with lower cognitive performance, lower cerebral blood flow, and greater white matter hyperintensity load in older subjects. Circulation. 2016;134:212–221. doi:10.1161/CIRCULATIONAHA.115.020627
26. Gouw AA, van der Flier WM, Fazekas F, et al. Progression of white matter hyperintensities and incidence of new lacunes over a 3-year period: the Leukoaraiosis and Disability study. Stroke. 2008;39:1414–1420. doi:10.1161/STROKEAHA.107.498535
27. Jimenez-Conde J, Biffi A, Rahman R, et al. Hyperlipidemia and reduced white matter hyperintensity volume in patients with ischemic stroke. Stroke. 2010;41:437–442. doi:10.1161/STROKEAHA.109.563502
28. Stefaniak JD, Parkes LM, Parry-Jones AR, et al. Enzyme replacement therapy and white matter hyperintensity progression in Fabry disease. Neurology. 2018;91:e1413–e1422. doi:10.1212/WNL.0000000000006316
29. Vogt NM, Hunt JFV, Ma Y, et al. Effects of simvastatin on white matter integrity in healthy middle-aged adults. Ann Clin Transl Neurol. 2021;8:1656–1667. doi:10.1002/acn3.51421
30. Li W, Liu M, Wu B, Liu H, Wang LC, Tan S. Serum lipid levels and 3-month prognosis in Chinese patients with acute stroke. Adv Ther. 2008;25(4):329–341. doi:10.1007/s12325-008-0045-7
31. Pikija S, Sztriha LK, Killer-Oberpfalzer M, et al. Contribution of serum lipid profiles to outcome after endovascular thrombectomy for anterior circulation ischemic stroke. Mol Neurobiol. 2019;56(6):4582–4588. doi:10.1007/s12035-018-1391-3
32. Cheng Z, Zhang W, Zhan Z, Xia L, Han Z. Cerebral small vessel disease and prognosis in intracerebral haemorrhage: a systematic review and meta-analysis of cohort studies. Eur J Neurol. 2022;29(8):2511–2525. doi:10.1111/ene.15363
33. Griessenauer CJ, McPherson D, Berger A, et al. Effects of white matter hyperintensities on 90-day functional outcome after large vessel and non-large vessel stroke. Cerebrovasc Dis. 2020;49(4):419–426.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.