Back to Journals » Journal of Pain Research » Volume 14
Association of Pain Catastrophizing and Depressive States with Multidimensional Early Labor Pain Assessment in Nulliparous Women Having Epidural Analgesia – A Secondary Analysis
Authors Sim XLJ, Tan CW ![]() , Yeam CT
, Yeam CT ![]() , Tan HS, Sultana R, Sng BL
, Tan HS, Sultana R, Sng BL ![]()
Received 30 July 2021
Accepted for publication 23 September 2021
Published 7 October 2021 Volume 2021:14 Pages 3099—3107
DOI https://doi.org/10.2147/JPR.S331703
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ellen Soffin
Xiu Ling Jacqueline Sim,1 Chin Wen Tan,2,3 Cheng Teng Yeam,4 Hon Sen Tan,2,3 Rehena Sultana,5 Ban Leong Sng2,3
1Department of Anesthesiology, Singapore General Hospital, Singapore, Singapore; 2Department of Women’s Anesthesia, KK Women’s and Children’s Hospital, Singapore, Singapore; 3Anesthesiology and Perioperative Sciences Academic Clinical Program, Duke-NUS Medical School, Singapore, Singapore; 4MOH Holdings, Singapore, Singapore; 5Centre for Quantitative Medicine, Duke-NUS Medical School, Singapore, Singapore
Correspondence: Ban Leong Sng Tel +65 6394 1081
Fax +65 6291 2661
Email [email protected]
Background: Labor pain is a variable and complex experience with both sensory and affective components. Pain catastrophizing tendencies are predictive of increased distress during labor. Likewise, pain severity has important associations with increased depressive symptoms in mothers, with consequences on perinatal and infant outcomes. Hence, we investigated the association between increased early labor pain with both pre-delivery pain catastrophizing and depressive states.
Methods: We recruited nulliparous women who had requested labor epidural analgesia. Pre-delivery questionnaires including short-form McGill pain questionnaire– 2 (SF-MPQ-2), pain catastrophizing scale (PCS), and Edinburgh postnatal depression score (EPDS) were administered.
Results: A total of 712 women completed the pre-delivery questionnaires. There was a significant association between SF-MPQ-2 neuropathic subscale and EPDS ≥ 10 (unadjusted OR 1.74, 95% CI 1.11– 2.73, p = 0.0161), as well as PCS ≥ 25 (unadjusted OR 1.55, 95% CI 1.06– 2.26, p = 0.0244). SF-MPQ-2 sensory intermittent subscale and EPDS ≥ 10 (unadjusted OR 2.02, 95% CI 1.34– 3.03, p = 0.0007), and PCS ≥ 25 (unadjusted OR 1.59, 95% CI 1.14– 2.23, p = 0.0069) also showed significant association.
Conclusion: Increased sensory intermittent and neuropathic subsets of early labor pain are significantly correlated with increased pre-delivery pain catastrophizing and depressive states in nulliparous women. This positive association may be useful for pre-delivery risk stratification for early interventions towards a more holistic care management.
Keywords: labor pain, pain catastrophizing, pre-delivery depression, survey
Introduction
Labor pain is a variable, complex and multidimensional process with both sensory and affective components. The association between pain and depressive symptoms is frequently reported in perinatal period.1–3 History of depression or pre-delivery pain is associated with higher incidence of postnatal depression (PND).4–6 In addition, pain before pregnancy and a history of depression are also significantly correlated with persistent pain after childbirth.4–6 These multifaceted associations are of interest as mothers’ pain and mental experience before their delivery could impact the experience of labor pains, possibly with adverse maternal and infant outcomes.
Recent studies have also shown an association between pain catastrophizing, compounded by labor pain, and consequent adverse postnatal adjustment states.7,8 Pain catastrophizing is an exaggerated negative mental status during actual or anticipated painful stimulus, and results in rumination, magnification, and helplessness.9 Pre-existing pain catastrophizing tendencies were predictive of increased distress during contractions and childbirth.10 Similarly, women with fear of pain, feelings of helplessness and loss of control reported increased pain during childbirth, as well as heightened distress.11 Ferber et al reported that postnatal catastrophizers had poorer postnatal physical recovery and exhibited more depressive features.7 Hence, screening of at-risk women for pre-existing pain catastrophizing before delivery may be beneficial.
Pain scales most often used in the literature for measuring the intensity of labor pain include Visual analogue scale (VAS), Numerical rating scale (NRS), Face rating scale (FRS), and Verbal rating scale (VRS).12 The main disadvantage of using these scales is the unidimensional pain assessment nature, which may not fully reflect the early labor pain experience, especially neuropathic subsets.13 Neuropathic pain is “pain caused by a primary lesion or dysfunction in the nervous system”, often described as pain of “burning, electric shock-like, prickling, or itching sensations or numbness”.14,15 A recent development of short-form McGill pain questionnaire–2 (SF-MPQ-2) includes the qualities of both neuropathic and non-neuropathic pain and has since proven usefulness in patients with acute pain and cesarean delivery.16–18 However, the evidence for its use in assessing labor pain should be further explored.
With these limited literature in the area of early labour pain and mental conditions, we hypothesized there would be a positive association between increased early labor pain with both pre-delivery pain catastrophizing and depressive states in nulliparous women in a clinical setting with administration of labor epidural analgesia. We also looked into the association between the specific nature of early labor pain with pre-delivery stress and anxiety traits in these women.
Methods
Recruitment
This cohort study was a secondary analysis of data collected from a clinical trial investigating epidural delivery regimens. The study was conducted between January 2015 and March 2019 in KK Women’s and Children’s Hospital, Singapore, on women who received epidural analgesia for labor. The study protocol was developed according to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines on reporting cohort studies.19 The study was reviewed and approved by the SingHealth Centralized Institutional Review Board, Singapore (SingHealth CIRB reference number 2014/670/D and 2018/3128), and registered on ClinicalTrials.gov (NCT02278601) on October 26, 2014.
We recruited nulliparous women aged 21–50 years, 36 gestational weeks or more, with a singleton fetus, the American Society of Anesthesiologists’ physical status II, and in early labor (defined as cervical dilation <5 cm) who had requested labor epidural analgesia in the clinical trial. We excluded women with multiple pregnancies, non-cephalic fetal presentation, diagnosed obstetric complications (eg, preeclampsia, premature rupture of membranes), contraindications to neuraxial blockade, ineffective epidural analgesia during initiation, had received parenteral opioids within the 2-hours preceding the insertion of epidural, or the possibility of inadvertent dural puncture.
For the recruitment, study posters and brochures were placed in the antenatal clinics, antenatal classes, antenatal wards and delivery suite. The consent process commenced when women were not in distress (pain score of 3 or less out of 10 using numerical rating scale). All women were counselled by the investigators about the study protocol with written consent.
Labor epidural analgesia was established via a standardized protocol.20 Once the woman was comfortable, pre-delivery questionnaires in paper were given after standardized explanation by research coordinators or investigators, and women were instructed to give responses prior to the epidural analgesia as close as possible. These included: i) The short-form McGill pain questionnaire–2 (SF-MPQ-2), a multidimensional pain assessment tool that assesses the major symptoms of both neuropathic and non-neuropathic pain with four subscale scores (continuous pain, intermittent pain, predominantly neuropathic pain, and affective descriptors).13,14 There are a total of 22 items with 0–10 numerical response options (0 being none, and 10 being worst possible). In addition, a numerical rating scale (0 being no pain, and 10 being worst pain imaginable) is used to measure the labor pain intensity. The SF-MPQ-2 has shown good correlation with the standard form and has been validated in obstetric population where pain evaluation is often restricted by time distress during the labor process;15,18 ii) pain catastrophizing scale (PCS), a validated self-reported questionnaire to evaluate negative thought processes that one may have with exposure to actual/anticipated pain/painful experiences. PCS ≥ 30 is associated with clinically relevant pain catastrophizing in the general adult population.9,21,22 However, this cut-off is generally regarded as 20–25 in pregnant women.7,8 In this study, a cut-off of 25 was used as previous study has reported an association between high pain catastrophizing (PCS ≥ 25) and increased post-delivery EPDS scores;20 iii) Edinburgh postnatal depression score (EPDS), a ten-item self-reported questionnaire used as a screening tool for pre-delivery depressive symptoms and PND, with a score of 10 or more indicating clinically significant depressive symptoms;23–25 iv) Cohen’s perceived stress scale (PSS), a ten-item validated psychometric instrument to quantify the perception of stress;26 and v) Spielberger’s state-trait-anxiety inventory (STAI), a 40-item self-report tool that assesses transient anxiety (state) at the moment of scoring, the dispositional anxiety (trait), and anxiety in general.27
The demographic and obstetric data from medical records were also collected in this study. On the following day after delivery, the women were reviewed by the anesthetic team as per institution’s routine practice. The investigators were responsible for collecting the SF-MPQ-2, PCS and EPDS questionnaires, and if there was any missing data, the investigators would perform follow-up during hospital stay.
Statistical Analysis
Our primary objective was to determine if there was an association between increased early labor pain and pain catastrophizing or pre-delivery depressive states in laboring women who received labor epidural analgesia. A pre-delivery EPDS score ≥10 was treated as binary data to identify the presence of pre-delivery depressive states.25 PCS cut-offs of <25 and ≥25 was used to define the status “no” or “yes” on low and high pain catastrophizing cohorts, respectively.20
Demographic and baseline characteristics of the participants were summarized based on the PCS cohorts. Categorical data were summarized as frequency (proportion) and continuous data summarized as mean ± SD. Univariate logistic regression model was used to derive the association between pre-delivery pain catastrophizing and depressive states with early labor pain using SF-MPQ-2. Associations between pre-delivery EPDS and PCS with the subscales of SF-MPQ-2 were reported as unadjusted odds ratio (OR) with 95% confidence intervals (CIs). Pearson’s correlation coefficient was used to find strength of a linear association between SF-MPQ-2 subscales and pre-delivery EPDS and PCS scales. Significance was set at p<0.05, and all tests were two-tailed. SAS version 9.4 software (SAS Institute, Cary, NC, USA) was used for all analyses.
Results
A total of 712 women were recruited and completed the SF-MPQ-2. Women recruited had mean (SD) age, body mass index (BMI), and gestational age of 29.6 (4.2) years old, 27.5 (4.7) kgm−2, and 37.7 (2.1) weeks [range: 36–41 weeks], respectively (Table 1). Of the frequently used descriptors to describe early labor pain using the SF-MPQ-2, the intensity of “tiring-exhausting”, “cramping” and “aching” were the highest (Table 2).
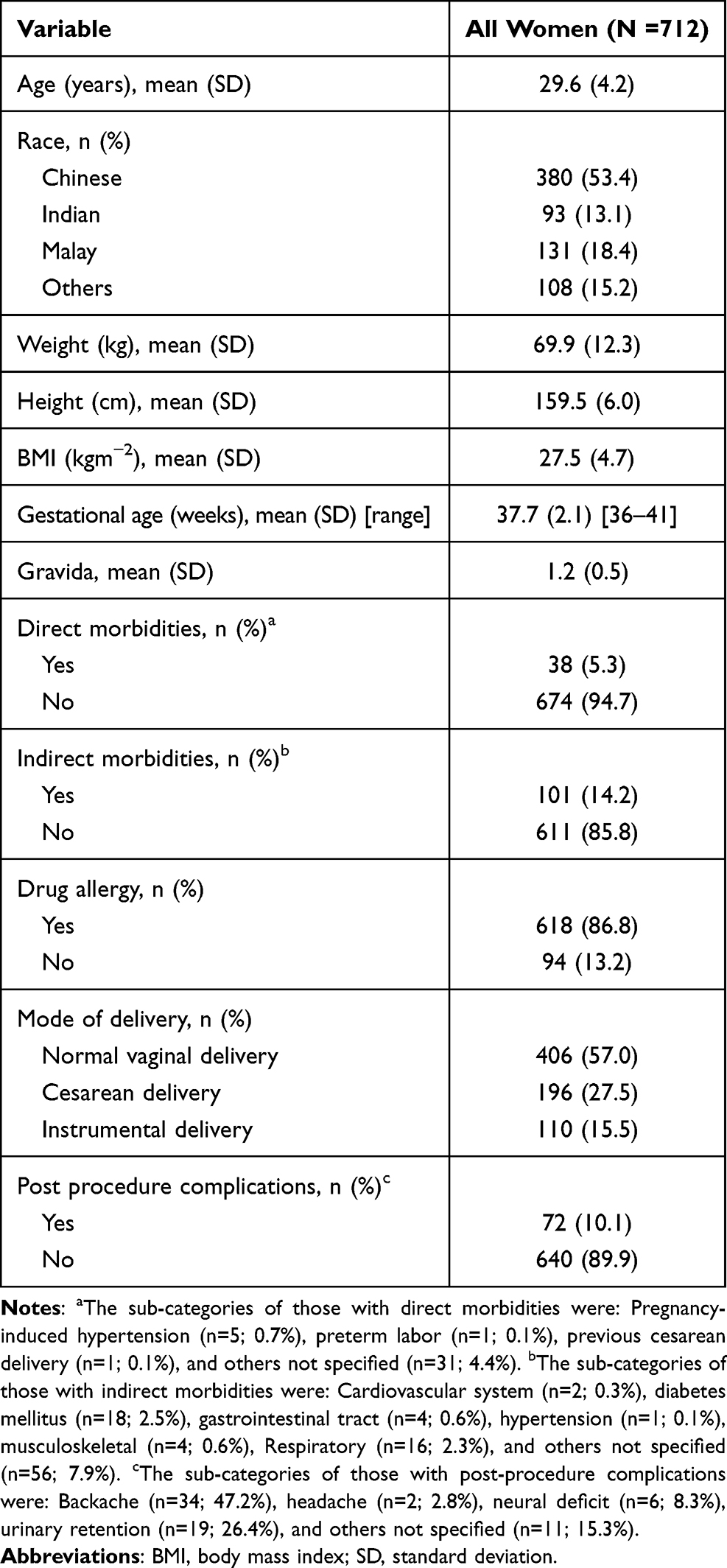 |
Table 1 Demographic Characteristics for All Recruited Women (N=712) |
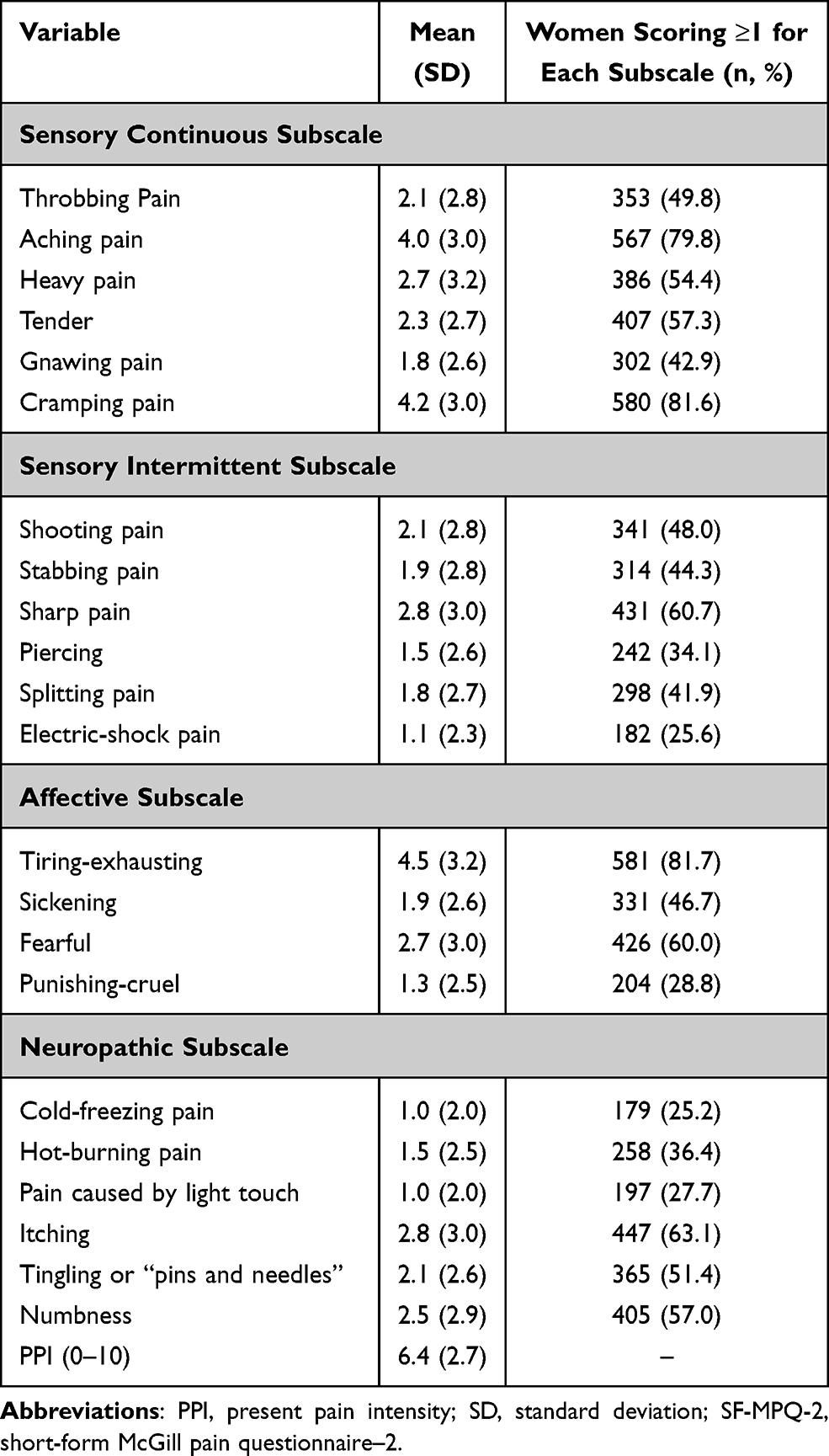 |
Table 2 SF-MPQ-2 Pain Characteristics of All Women (N = 712) |
The mean (SD) of EPDS score of the whole cohort was 7.4 (4.4), with a total of 193 (27.2%) women reporting an EPDS score of 10 or more. With regard to the PCS total score, the recruited women scored a mean (SD) of 8.4 (4.6), with 310 (43.6%) of participants having a PCS ≥ 25. The mean (SD) of PCS subscales were 9.5 (6.0), 9.5 (6.0) and 4.5 (3.0) for helplessness, magnification, and rumination, respectively. These are presented in Table 3.
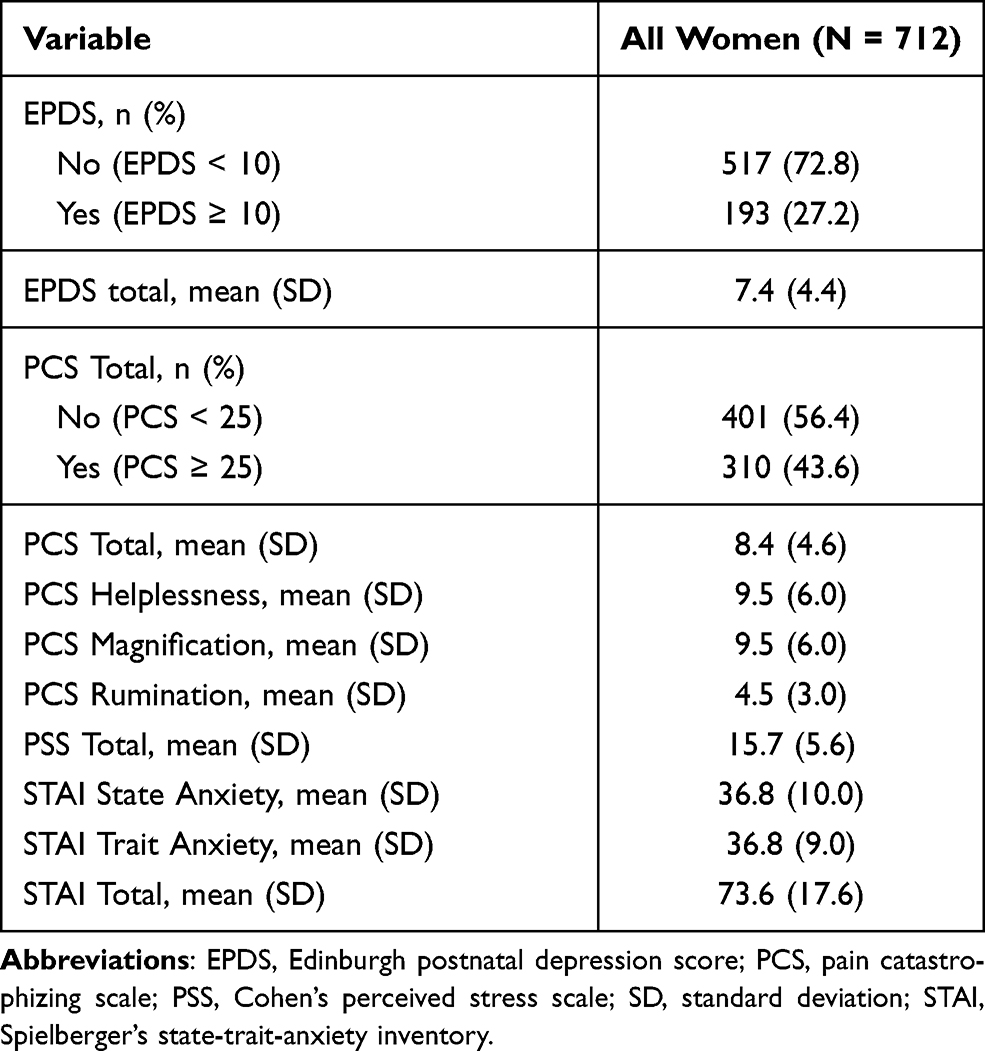 |
Table 3 Pre-Delivery Psychological Characteristics of All Women (N = 712) |
We performed a correlation analysis on the relationship between SF-MPQ-2 subscales on neuropathic and intermittent pain. Pearson correlation coefficient for the SF-MPQ-2 neuropathic subscale with pre-delivery EPDS and pre-delivery PCS was 0.279 and 0.189, respectively (Figure 1A and B). Similarly, SF-MPQ-2 intermittent pain subscale with pre-delivery EPDS and pre-delivery PCS reported Pearson correlation coefficients of 0.216 and 0.172, respectively (Figure 2A and B). Based on the findings in Table 4, there was a significant association between SF-MPQ-2 neuropathic subscale and EPDS ≥ 10 (unadjusted OR 1.74, 95% CI 1.11–2.73, p = 0.0161), as well as PCS ≥ 25 (unadjusted OR 1.55, 95% CI 1.06–2.26, p = 0.0244). There was also significant association between SF-MPQ-2 sensory intermittent subscale with EPDS ≥ 10 (unadjusted OR 2.02, 95% CI 1.34–3.03, p = 0.0007), and PCS ≥ 25 (unadjusted OR 1.59, 95% CI 1.14–2.23, p = 0.0069). No significant statistical differences were found in the associations of SF-MPQ-2 sensory continuous with EPDS ≥ 10 (unadjusted OR 1.40, 95% CI 0.70–2.79, p = 0.3372), and PCS ≥ 25 (unadjusted OR 1.36, 95% CI 0.76–2.44, p=0.3034), nor between affective subscales and pre-delivery EPDS ≥ 10 (unadjusted OR 1.68, 95% CI 0.99–2.86, p = 0.0541), and PCS ≥ 25 (unadjusted OR 1.17, 95% CI 0.76–1.80, p = 0.4775).
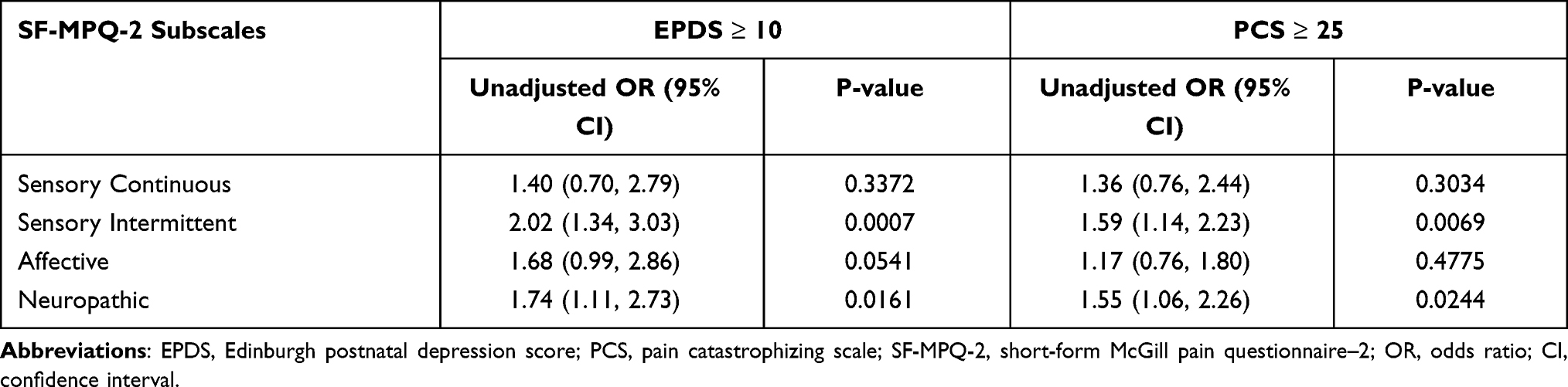 |
Table 4 Univariate Analysis Between SF-MPQ-2 Subscales and Pre-Delivery EPDS and PCS |
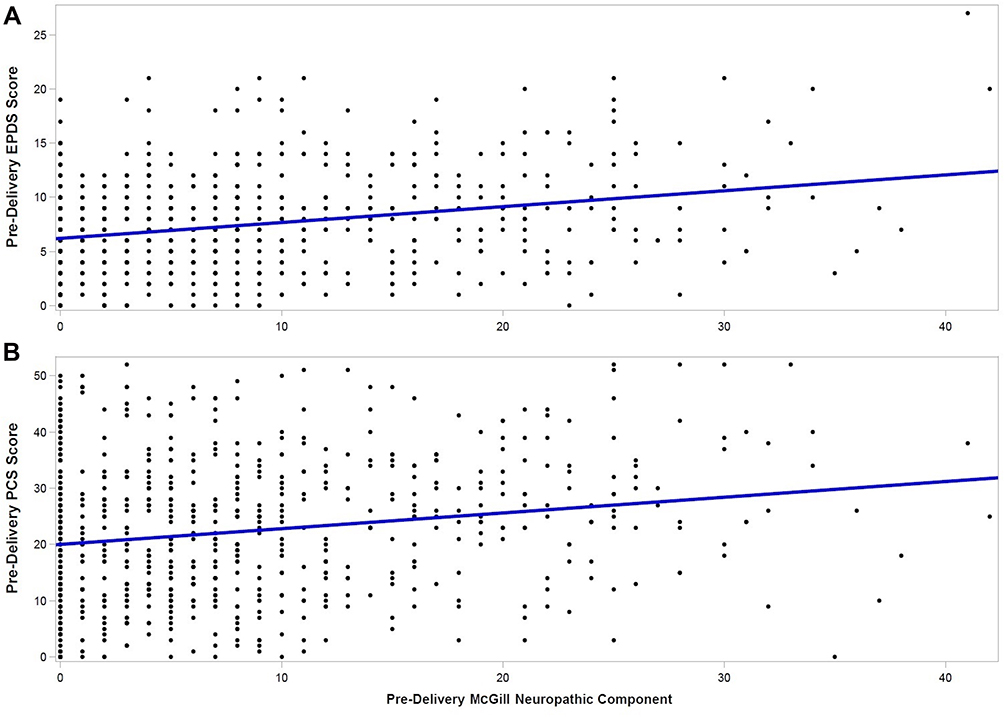 |
Figure 1 Correlation between pre-delivery SF-MPQ-2 neuropathic pain subscale and (A) pre-delivery EPDS; and (B) pre-delivery PCS. Abbreviations: EPDS, Edinburgh postnatal depression score; PCS, pain catastrophizing scale. |
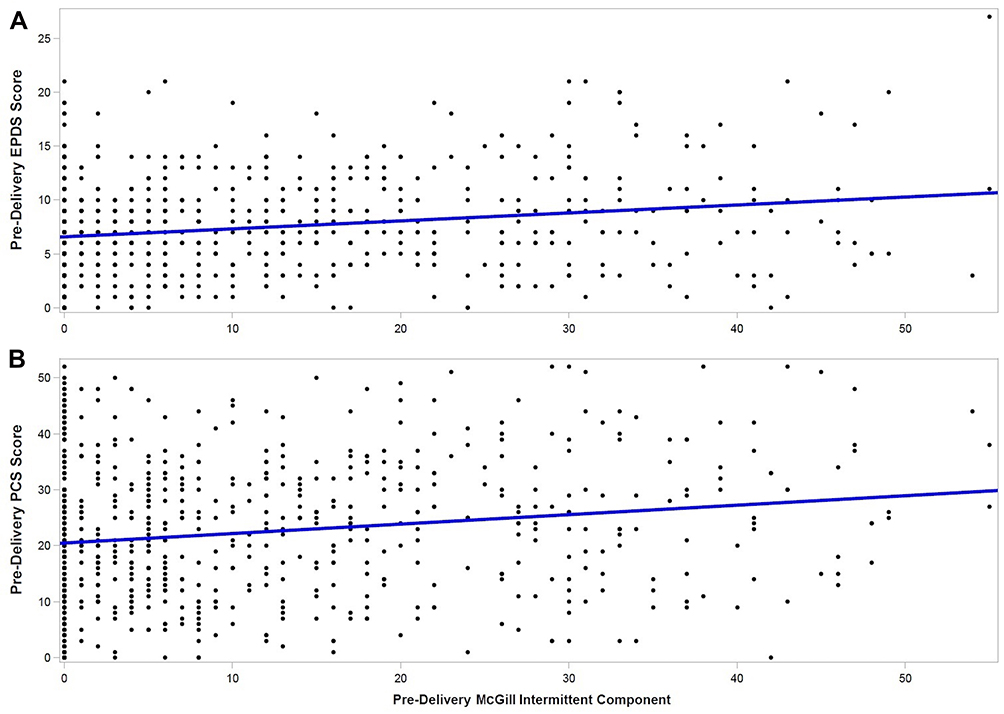 |
Figure 2 Correlation between pre-delivery SF-MPQ-2 intermittent pain subscale and (A) pre-delivery EPDS; and (B) pre-delivery PCS. Abbreviations: EPDS, Edinburgh postnatal depression score; PCS, pain catastrophizing scale. |
Discussion
By utilizing the SF-MPQ-2 in this cohort study, we found that higher pre-delivery neuropathic and intermittent nature of early labor pain positively correlated with both higher pre-delivery EPDS and PCS. Considered within this context, women’s descriptions of the pain, rather than just pain intensity, may be important. These pain descriptors may reflect the women’s psychological status during labor that may affect postnatal outcomes and could be an area of research for patient risk stratification.
The findings illustrate the multidimensional and dynamic nature of labor pain. Early stages of labor pain result in visceral pain due to uterine contractions and stretching of the cervix, resulting in dull intermittent labor pain.28 Somatic pain occurs with visceral pain closer to delivery. In this active phase, the uterus contracts more intensely and regularly, in addition to heightened stimulation via the pudendal nerves. Hence, perineal pain that occurs is often sharp and well localized.28,29 In the late part of the first stage of labor and during the second stage of labor, women may report “neuropathic” descriptors, likely due to stimulation of pain-sensitive structures in the pelvic cavity.30 Nevertheless, the most frequent descriptors given by the women (eg, “tiring-exhausting”, “cramping”, “aching”) were under the subscales of sensory continuous and affective pain based on the SF-MPQ-2, of which the subscales did not show significant association with pre-delivery pain catastrophizing nor depressive states. Again, this reiterates the variability of labor pain, in our case the early stage of labor pain, and how the varied characteristics of pain, or pain perception are just as important to grasp as pain intensity when SF-MPQ-2 is considered in the labor and delivery settings.
Studies have suggested that prenatal anxiety is associated with increased labor pain, and women with anxiety or depressive disorders are included to use epidural analgesia during labor.31,32 Pettersson et al further demonstrated that self-reported pre-delivery depressed mood was associated with increased labor pain during the initial phase of labor.33
Catastrophizing is a strong predictor of pain severity.9,34,35 Hence, anticipation of severe pain during childbirth may be associated with psychological reactions, such as pain catastrophizing. Based on the fear avoidance model, a person’s experience of pain is affected by factors such as emotional, biological, cognitive, and behavioral states. When applied in the context of our study, women with higher pain catastrophizing may interpret labor pain as threatening and evoking excessive thoughts. This may lead to an anticipation and overestimation of pain intensity. Women may place greater focus on their pain while undermining their own coping abilities.8 Women with pain catastrophizing in labor had higher anticipation and pain experience than non-catastrophizers, but studies have not investigated on specific nature of labor pain.8,10 We previously found that pre-delivery PCS is associated with increased post-delivery EPDS score, further emphasizing the importance in managing pre-delivery pain and mood.20
The limitations of this study included the secondary analysis design based on a larger clinical trial on labor epidural analgesia. Nevertheless, we addressed the current lack of knowledge on specific subsets of neuropathic pain and intermittent pain components with pre-delivery self-reported pain catastrophizing or depressive states. Another limitation of this study is that SF-MPQ-2 was initially developed for assessment of chronic pain and has not been widely used for assessing labor pain. Other pain scales that have been used to diagnose neuropathic pain in obstetric population include the Douleur Neuropathique 4 (DN4) questionnaire and the Leeds assessment of neuropathic symptoms and signs (LANNS) questionnaire, but they are also not originally designed to specify the pain characteristics in laboring women.15,36,37 Therefore, an instrument specifically designed to evaluate the neuropathic component of early labor pain would be useful. This study is also limited by the primary study design on including only healthy nulliparous women. Nulliparous women may possess different psychological frame of mind, pre-delivery perceptions and anticipations compared to multiparous women, which could affect the sensitivity of statistical outcomes of association between SF-MPQ-2 pain scores and pre-delivery EPDS/PCS scores. We also did not consider possible confounders such as BMI and age that are relevant to pain perception and may affect the correlation outcomes. In addition, only women who requested for labor epidural analgesia were recruited in this study. Women who did not receive epidural analgesia may have differing convictions, pain thresholds, and expectations that could contribute to different outcomes. On a similar note, women were instructed to report the pain prior to the epidural analgesia upon recruitment; however, the questionnaires were administered just after epidural analgesia was performed. We acknowledged this limitation, but this would also allow comfort when they were answering the questionnaires. Therefore, future research is required to generalize these findings to a wider population of pregnant women of different cultural and clinical contexts. Finally, we investigated the relationship between SF-MPQ-2 and PCS, as well as with EPDS, but the pre-delivery psychological state may be confounded by other factors such as socioeconomic status which was not included in the analysis.
Conclusions
We showed that increased intermittent and neuropathic subscales of early labor pain were significantly correlated with increased pre-delivery pain catastrophizing and depressive states in nulliparous women who requested and received labor epidural analgesia. This positive association may be useful for pre-delivery risk stratification to allow early support and interventions for postpartum care management. The use of SF-MPQ-2 in assessing early labor pain may also offer a more holistic approach in encompassing the multidimensional qualities of pain.
Abbreviations
BMI, body mass index; CI, confidence interval; DN4, Douleur Neuropathique 4; EPDS, Edinburgh postnatal depression score; FRS, face rating scale; LANNS, Leeds assessment of neuropathic symptoms and signs; NRS, numerical rating scale; OR, odds ratio, PCS, pain catastrophizing scale; PND, postnatal depression; PPI, present pain intensity; PSS, Cohen’s perceived stress scale; SD, standard deviation; SF-MPQ-2, short-form McGill pain questionnaire–2; STAI, Spielberger’s state-trait-anxiety inventory; VAS, visual analogue scale; VRS, verbal rating scale.
Data Sharing Statement
The datasets generated and analyzed in this work are available for anyone who wishes to access the data by contacting the corresponding author.
Ethics Approval and Informed Consent
The study was approved by the SingHealth Centralized Institutional Review Board, Singapore (SingHealth CIRB reference 2014/670/D or 2018/3128) and registered on ClinicalTrials.gov (NCT02278601) on October 26, 2014. The authors declare that all recruited women provided informed consent and that this work was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
All women provided informed consent on the use of their de-identified data for publication purposes.
Acknowledgments
We would like to thank Agnes Teo (Senior Clinical Research Coordinator), Yvonne Yong (Senior Clinical Research Coordinator), and Denise Anne (Clinical Research Coordinator) for their administrative support in this work.
Funding
This work was supported by funding from the National Medical Research Council Clinical Trials Grant – Investigator-Initiated Trials (CTG13feb013). The aforementioned sponsor was not involved in the study activities.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Gaudet C, Wen SW, Walker MC. Chronic perinatal pain as a risk factor for postpartum depression symptoms in Canadian women. Can J Public Health. 2013;104(5):e375–387. doi:10.17269/cjph.104.4029
2. Henderson J. Sixteen per cent of women have depression symptoms in the year after childbirth and are more likely to report physical symptoms, including tiredness and back pain. Evid Based Nurs. 2015;18(2):36. doi:10.1136/eb-2014-101880
3. Safadi RR, Abushaikha LA, Ahmad MM. Demographic, maternal, and infant health correlates of post-partum depression in Jordan. Nurs Health Sci. 2016;18(3):306–313. doi:10.1111/nhs.12268
4. Rosseland LA, Reme SE, Simonsen TB, Thoresen M, Nielsen CS, Eberhard-Gran M. Are labor pain and birth experience associated with persistent pain and postpartum depression? A Prospective Cohort Study. Scand J Pain. 2020;20(3):591–602. doi:10.1515/sjpain-2020-0025
5. Rosseland LA, Reme SE, Simonsen TB, Thoresen M, Nielsen CS, Eberhard-Gran M. Corrigendum to: are labor pain and birth experience associated with persistent pain and postpartum depression? A Prospective Cohort Study. Scand J Pain. 2020;20(4):865. doi:10.1515/sjpain-2020-2023
6. Eisenach JC, Pan PH, Smiley R, Lavand’homme P, Landau R, Houle TT. Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartum depression. Pain. 2008;140(1):87–94. doi:10.1016/j.pain.2008.07.011
7. Ferber SG, Granot M, Zimmer EZ. Catastrophizing labor pain compromises later maternity adjustments. Am J Obstet Gynecol. 2005;192(3):826–831. doi:10.1016/j.ajog.2004.10.589
8. Flink IK, Mroczek MZ, Sullivan MJ, Linton SJ. Pain in childbirth and postpartum recovery: the role of catastrophizing. Eur J Pain. 2009;13(3):312–316. doi:10.1016/j.ejpain.2008.04.010
9. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7(4):524–532. doi:10.1037/1040-3590.7.4.524
10. Van den Bussche E, Crombez G, Eccleston C, Sullivan MJ. Why women prefer epidural analgesia during childbirth: the role of beliefs about epidural analgesia and pain catastrophizing. Eur J Pain. 2007;11(3):275–282. doi:10.1016/j.ejpain.2006.03.002
11. Wuitchik M, Hesson K, Bakal DA. Perinatal predictors of pain and distress during labor. Birth. 1990;17(4):186–191. doi:10.1111/j.1523-536X.1990.tb00019.x
12. Takegata M, Haruna M, Murayama R, Matsuzaki M, Murashima S. Scales for measuring labor pain: a literature review. J Jpn Acad Midwifery. 2011;25(2):160–170. doi:10.3418/jjam.25.160
13. Melzack R. The McGill pain questionnaire: major properties and scoring methods. Pain. 1975;1(3):277–299. doi:10.1016/0304-3959(75)90044-5
14. Jensen TS, Baron R, Haanpää M, et al. A new definition of neuropathic pain. Pain. 2011;152(10):2204–2205. doi:10.1016/j.pain.2011.06.017
15. Eser F, Nebioğlu S, Aliyeva A, et al. Neuropathic pain in pregnant Turkish women with lumbopelvic pain and its impact on health-related quality of life. Eur J Rheumatol. 2018;5(1):37–39. doi:10.5152/eurjrheum.2017.16088
16. Adelmanesh F, Jalali A, Attarian H, et al. Reliability, validity, and sensitivity measures of expanded and revised version of the short-form McGill pain questionnaire (SF-MPQ-2) in Iranian patients with neuropathic and non-neuropathic pain. Pain Med. 2012;13(12):1631–1636. doi:10.1111/j.1526-4637.2012.01517.x
17. Lovejoy TI, Turk DC, Morasco BJ. Evaluation of the psychometric properties of the revised short-form McGill pain questionnaire. J Pain. 2012;13(12):1250–1257. doi:10.1016/j.jpain.2012.09.011
18. Ortner CM, Turk DC, Theodore BR, Siaulys MM, Bollag LA, Landau R. The short-form McGill pain questionnaire-revised to evaluate persistent pain and surgery-related symptoms in healthy women undergoing a planned cesarean delivery. Reg Anesth Pain Med. 2014;39(6):478–486. doi:10.1097/AAP.0000000000000158
19. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
20. Zeng Y, Tan CW, Sultana R, et al. Association of pain catastrophizing with postnatal depressive states in nulliparous parturients: a Prospective Study. Neuropsychiatr Dis Treat. 2020;16:1853–1862. doi:10.2147/NDT.S256465
21. Kortlever JT, Janssen SJ, van Berckel MM, Ring D, Vranceanu AM. What is the most useful questionnaire for measurement of coping strategies in response to nociception? Clin Orthop Relat Res. 2015;473(11):3511–3518. doi:10.1007/s11999-015-4419-2
22. Osman A, Barrios FX, Gutierrez PM, Kopper BA, Merrifield T, Grittmann L. The pain catastrophizing scale: further psychometric evaluation with adult samples. J Behav Med. 2000;23(4):351–365. doi:10.1023/A:1005548801037
23. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry. 1987;150(6):782–786. doi:10.1192/bjp.150.6.782
24. Wisner KL, Parry BL, Piontek CM. Clinical practice. Postpartum depression. N Engl J Med. 2002;347(3):194–199. doi:10.1056/NEJMcp011542
25. Chen H, Wang J, Ch’ng YC, Mingoo R, Lee T, Ong J. Identifying mothers with postpartum depression early: integrating perinatal mental health care into the obstetric setting. ISRN Obstet Gynecol. 2011;2011:309189.
26. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396. doi:10.2307/2136404
27. Spielberger CD. State-trait anxiety inventory. In: Craighead IBWaWE, editor. The Corsini Encyclopedia of Psychology. American Psychological Association; 2010:1.
28. Labor S, Maguire S. The pain of labour. Rev Pain. 2008;2(2):15–19. doi:10.1177/204946370800200205
29. Gonzalez MNTGK. Pain management during labor part 1: pathophysiology of labor pain and maternal evaluation for labor analgesia. Topics Obstet Gynecol. 2016;36(11):8.
30. McDonald JS, Noback CR. Obstetric pain. In: Handbook of Pain Management. Elsevier; 2003:147–161.
31. Andersson L, Sundström-Poromaa I, Wulff M, Aström M, Bixo M. Implications of antenatal depression and anxiety for obstetric outcome. Obstet Gynecol. 2004;104(3):467–476. doi:10.1097/01.AOG.0000135277.04565.e9
32. Lang AJ, Sorrell JT, Rodgers CS, Lebeck MM. Anxiety sensitivity as a predictor of labor pain. Eur J Pain. 2006;10(3):263–270. doi:10.1016/j.ejpain.2005.05.001
33. Pettersson FD, Hellgren C, Nyberg F, Åkerud H, Sundström-Poromaa I. Depressed mood, anxiety, and the use of labor analgesia. Arch Womens Ment Health. 2016;19(1):11–16. doi:10.1007/s00737-015-0572-6
34. Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317–332. doi:10.1016/S0304-3959(99)00242-0
35. Keefe FJ, Rumble ME, Scipio CD, Giordano LA, Perri LM. Psychological aspects of persistent pain: current state of the science. J Pain. 2004;5(4):195–211. doi:10.1016/j.jpain.2004.02.576
36. Bouhassira D, Attal N, Alchaar H, et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain. 2005;114(1–2):29–36. doi:10.1016/j.pain.2004.12.010
37. Cardaillac C, Delga B, Thubert T, et al. Description and classification of postpartum chronic pain: a multicentric prospective study. J Gynecol Obstet Hum Reprod. 2020;49(9):101769. doi:10.1016/j.jogoh.2020.101769
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.