Back to Journals » Nature and Science of Sleep » Volume 17

Association of Novel Hematologic Inflammatory Biomarkers with Cardiovascular Disease in Patients with Obstructive Sleep Apnea
Authors Ou Y, Wang X, Zong D ![]() , Ouyang R
, Ouyang R ![]()
Received 17 July 2025
Accepted for publication 4 October 2025
Published 17 October 2025 Volume 2025:17 Pages 2715—2728
DOI https://doi.org/10.2147/NSS.S554387
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Yanru Ou,1– 4 Xiufang Wang,1– 4 Dandan Zong,1– 4,* Ruoyun Ouyang1– 4,*
1Department of Pulmonary and Critical Care Medicine, The Second Xiangya Hospital, Central South University, Changsha, Hunan, 410011, People’s Republic of China; 2Research Unit of Respiratory Disease, Central South University, Changsha, Hunan, 410011, People’s Republic of China; 3Clinical Medical Research Center for Respiratory and Critical Care Medicine in Hunan Province, Changsha, Hunan, 410011, People’s Republic of China; 4Diagnosis and Treatment Center of Respiratory Disease, Central South University, Changsha, Hunan, 410011, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dandan Zong, Email [email protected] Ruoyun Ouyang, Email [email protected]
Background: Heightened inflammatory state is considered a key factor linking obstructive sleep apnea (OSA) with cardiovascular disease (CVD).
Objective: This study aimed to assess the level of novel hematologic inflammatory biomarkers including neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), ratio of neutrophil count to HDL level (NHR), ratio of monocyte count to HDL level (MHR), monocyte count multiplied by neutrophil-to-lymphocyte ratio (SIRI) in OSA patients, and explored the relationships between these inflammatory biomarkers and cardiovascular risk.
Methods: This study enrolled 974 patients with OSA and all data were collected after admission. Spearman correlation was used to explore the correlations between sleep parameters and inflammatory indices. Logistic regression and receiver operating characteristic (ROC) analysis were employed to assess the association between the novel hematologic inflammatory indices and CVD in OSA patients.
Results: Correlation analysis showed that most inflammatory indices were closely related to nocturnal hypoxia in OSA patients. Multivariate logistic regression suggested that NLR (OR=1.085, 95% CI: 1.017– 1.158), MLR (OR=3.708, 95% CI: 1.322– 10.404), NHR (OR=1.074, 95% CI: 1.020– 1.131), MHR (OR=2.116, 95% CI: 1.205– 3.715), and SIRI (OR=1.148, 95% CI: 1.035– 1.272) were positively correlated with CVD in OSA patients after adjusting all confounding factors. Moreover, the area under the curve (AUC) of NLR, MLR, NHR, MHR, and SIRI for discriminating OSA patients with CVD was 0.734, 0.735, 0.736, 0.734, and 0.735, respectively, after adjusting for all confounders.
Conclusion: Inflammatory indices including NLR, MLR, NHR, MHR, and SIRI were promising biomarkers for CVD in OSA patients, which might aid in the early identification of CVD risk in clinical. These easily obtainable markers may facilitate CVD risk stratification in OSA patients.
Keywords: OSA, NLR, MLR, NHR, MHR, SIRI, cardiovascular disease
Introduction
Obstructive sleep apnea (OSA) is a common sleep breathing disorder characterized by repeated airway collapse or obstruction during sleep, resulting in hypopnea and apnea, and further leading to several physiologic disturbances such as intermittent hypoxia (IH), sleep fragmentation (SF).1 The global prevalence of OSA is rising year by year, a recent study estimated that one in seven of the world’s adult population had OSA.2 A large amount of evidence has shown that OSA is an independent risk factor for metabolic, cardiovascular, and neuropsychiatric diseases and other complications.3 Besides, excessive daytime sleepiness of OSA patients was significantly associated with road traffic accidents.4 OSA not only brings health and life burden but also increases the economic burden, which is associated with a high prevalence of costly comorbidities and accidents.5,6
OSA is associated with an increased incidence of various cardiovascular diseases (CVD) including systemic arterial hypertension, coronary artery disease, congestive cardiac failure, and stroke.7 The prevalence of OSA in patients with coronary heart disease, stroke, heart failure, and arrhythmia has been reported to be higher than 50%.8 A meta-analysis showed that OSA was associated with a 94% relative increase in the risk of cardiovascular death.9 For moderate to severe OSA, Continuous positive airway pressure (CPAP) is the standard treatment.10 OSA patients who adhere to CPAP may have improvement in adverse cardiovascular conditions, but low CPAP adherence will not have the same effect,11,12 early identification of high-risk individuals may facilitate clinical management.
As we all know, OSA is considered to be a low-grade chronic inflammatory disease, the inflammation induced by IH and SF is involved in the formation of various adverse outcomes in OSA patients.13,14 Inflammation is one of the signaling mechanisms connected OSA to CVD.15 IH can promote the secretion of pro-inflammatory factors, and recruit and activate inflammatory cells, leading to impaired vascular endothelial function.15 Many novel immunoinflammatory markers derived from complete blood count emerged to have predicted effects for CVD. The ratio of different kinds of white blood cell counts has been reported to reflect the balance of inflammatory and immune responses.16–19 Moreover, recent studies have shown that ratios combining leukocyte counts with high-density lipoprotein cholesterol (HDL) capture both pro-inflammatory and anti-inflammatory or anti-atherogenic processes. By integrating markers of inflammation and lipid metabolism, these composite indices may provide a more comprehensive assessment of CVD risk.20 Besides, the fact that these biomarkers are calculated from routine laboratory data makes them exceptionally practical and accessible tools for risk stratification, offering a cost-effective strategy that can be implemented without the need for costly, specialized assays.
Currently, no study has systematically evaluated the association of multiple hematological inflammatory biomarkers (NLR, MLR, NHR, MHR, and SIRI) with CVD risk in OSA patients. CVD includes coronary heart disease, stroke, and heart failure, all of which have been associated with systemic inflammation and OSA. We hypothesized that systemic inflammatory indices, especially HDL-based inflammatory indices, would show a strong association with the risk of cardiovascular disease since they capture both pro-inflammatory activity and impaired HDL-mediated vascular protection.
Methods
Study Design and Subjects
In this study, we retrospectively enrolled 2185 subjects who were admitted to the sleep medicine center at the Second Xiangya Hospital of Central South University from 2017 to 2023, and the study flow diagram is shown in Figure 1. All participants underwent polysomnography (Alice LDE, Philips, USA) or wore the portable sleep monitor (NOX T3, ResMed, USA) on the first night in the hospital. Exclusion criteria for subject enrollment included: (1) age of less than 18 years; (2) malignant disease; (3) active inflammatory disease; (4) severe life-threatening infection; (5) surgery within the last week; (6) missing sleep data or clinical data. Finally, 1304 subjects were included in this study, and we divided them into the non-OSA group and the OSA group according to the apnea-hypopnea index (AHI). Respiratory events were scored in accordance with the American Academy of Sleep Medicine 2017 recommended criteria:21 apnea was defined as the absence of airflow for ≥10 seconds, hypopnea was defined as a ≥30% reduction in airflow for ≥10 seconds associated with either a≥3% oxygen desaturation or the occurrence of an electroencephalographic arousal. The diagnosis of OSA was confirmed if the apnea-hypopnea index (AHI) was ≥5 events per hour. A total of 974 OSA patients were enrolled in the present study.
 |
Figure 1 Study flow diagram. |
This study was approved by the medical ethics Committee of the Second Xiangya Hospital of Central South University, approval number [Acceptance no. LYEC2024-0078], and informed consent was signed by each individual. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Hematology Test and Assessment of the Inflammatory Indices
Fasting venous blood samples of all subjects were collected in the morning after sleep monitoring and were sent to the laboratory department in the hospital. The blood samples were analyzed in the central laboratory of our hospital, and that laboratory staff were blinded to the CVD status of all participants. Complete blood counts were measured using an automated hematology analyzer (Sysmex XN-1500, Kobe, Japan). Serum lipid profiles were assessed using enzymatic methods on a fully automated biochemical analyzer (Roche Cobas C702, Mannheim, Germany). We recorded the results of high-density lipoprotein cholesterol (HDL) and blood routine test including white blood cell (WBC), neutrophils (NEU), platelet (PLT), lymphocyte (LYM), eosinophilic granulocyte (EO), and monocyte (MON). We utilized the data from hematology test to calculate the following inflammatory indices: platelet-to-lymphocyte ratio (PLR), neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), eosinophil-to-lymphocyte ratio (ELR), lymphocyte to monocyte ratio (LMR), ratio of neutrophil count to HDL level (NHR), ratio of monocyte count to HDL level (MHR), ratio of lymphocyte count to HDL level (LHR), ratio of platelet count to HDL level (PHR), platelet count multiplied by neutrophil-to-lymphocyte ratio (SII), monocyte count multiplied by neutrophil-to-lymphocyte ratio (SIRI), and neutrophil count multiplied by platelet count multiplied by monocyte-to-lymphocyte ratio (AISI).
Covariates
This study mainly included 2 kinds of covariates: (1) demographic characteristics and lifestyles: sex, age, body mass index (BMI), smoking, and alcohol. (2) comorbidities: hypertension, hyperlipemia, diabetes, fatty liver disease (FLD), and cardiovascular disease (CVD).
Demographic data, lifestyles, and comorbidities were all collected from the electronic medical record. Hypertension was defined as systolic blood pressure≥140 mmHg and (or) diastolic blood pressure≥90 mmHg, which measured three times on different days in the clinic,22 or current use of antihypertensive medication. Hyperlipidemia was defined if any of these four criteria was abnormal: triglycerides ≥ 1.7 mmol/L, total cholesterol ≥ 5.2 mmol/L, low-density lipoprotein cholesterol ≥ 3.4 mmol/L, or high-density lipoprotein cholesterol < 1.0 mmol/L.23 Diabetes was defined as diabetes symptoms (typical symptoms caused by high blood glucose, including polydipsia, polyphagia, polyuria, weight loss, skin pruritus, and blurred vision) + random blood glucose ≥ 11.1 mmol/L, or fasting blood glucose (FPG) ≥ 7.0 mmol/L, or 2-hour blood glucose ≥ 11.1 mmol/L, and/or a previous diagnosis of diabetes,24 or use of antidiabetic treatment. Fatty liver disease was diagnosed by abdominal ultrasonography. Smoking status and alcohol consumption were recorded as yes/no according to medical records and patient self-report. CVD was defined as the presence of major cardiovascular disorders including coronary heart disease, stroke,25 and heart failure.26 All diagnoses in this study were clinically validated.
Sample Size Calculation
An a priori power calculation was conducted to ensure that the study was adequately powered to detect meaningful associations between inflammatory indices and CVD in OSA patients. The sample size was calculated a priori using PASS software. Assuming α=0.05, 90% power, R2=0.5, CVD prevalence was 40%,27 and an expected odds ratio of 1.5, we estimated that required participants should over 665 (dropout rate=20%).
Statistical Analysis
The median (25th percentile, 75th percentile) was used to describe the continuous variables, and the number (percentage) was used to describe the categorical variables. Mann–Whitney U-test and Chi-square test were conducted to compare the differences between 2 groups (OSA patients with and without CVD). Spearman correlation was used to explore the correlations between sleep parameters and inflammatory indices. The relationships between the inflammatory indices and CVD in OSA patients were evaluated by logistic regression analyses in the form of odds ratio (OR) with a 95% confidence interval (CI) and receiver operating characteristic (ROC) curves, and adjusted for sex, age, BMI, smoking, alcohol consumption, hypertension, hyperlipemia, diabetes, and FLD. False discovery rate (FDR) correction was applied using the Benjamini–Hochberg procedure across all regression and ROC analyses. Multicollinearity among the independent variables was assessed using the variance inflation factor (VIF) (Table S3).
All statistical analyses were performed using the IBM SPSS Statistics 25, and GraphPad Prism 10.1.2. Two-tailed P value<0.05 was considered to be statistically significant.
Results
Characteristics of OSA Patients with and without CVD
We compared the baseline characteristics of OSA patients with and without CVD (Table 1). 432 (44.35%) OSA patients enrolled in this study had CVD. It seemed that OSA patients with CVD were more likely to have older age, a higher proportion of hypertension (68.06%) and diabetes (34.03%) compared with OSA patients without CVD. For the hematology test, there are more white blood cells (P=0.005), neutrophils (P<0.001), and monocytes (P=0.005), but fewer platelets (P=0.010) and lymphocytes (P<0.001) in OSA patients with CVD. Meanwhile, most of the inflammatory indices involved in this study had great discrepancies between the CVD and non-CVD groups. OSA patients with CVD had higher levels of inflammatory indices. Moreover, we found that the CVD group had more severe OSA. AHI was increased in OSA patients with CVD, but the MaSO2 and TS90 were decreased.
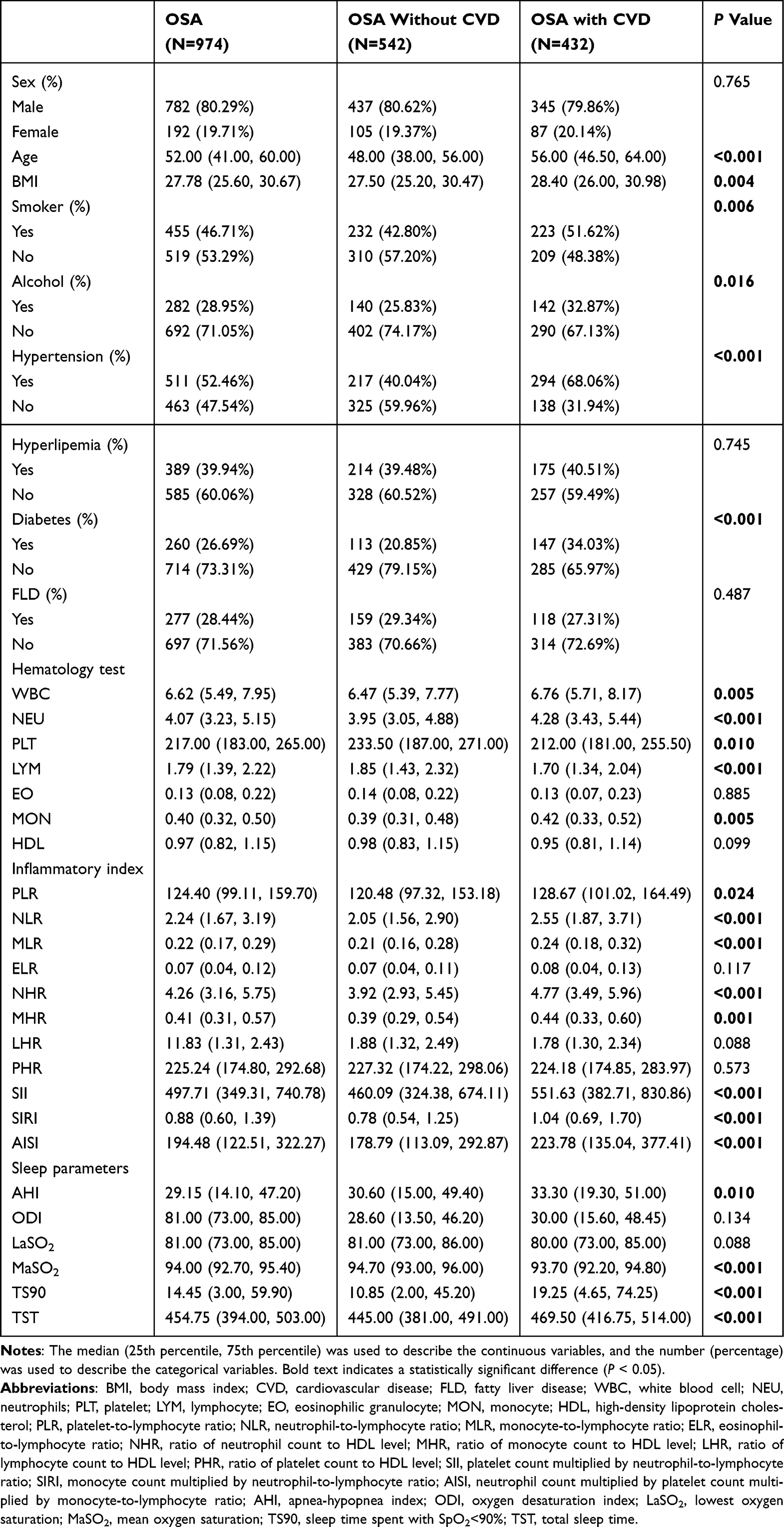 |
Table 1 Baseline Characteristics of OSA Patients with and without CVD |
Correlation of Inflammatory Indices and Sleep Parameters in OSA Patients
Correlation analysis was performed between inflammation indices and sleep parameters in OSA patients, the correlation coefficients were presented in the heat map (Figure 2) and detailed in Table 2. AHI, oxygen desaturation index (ODI), and sleep time spent with SpO2<90% (TS90) were positively correlated with most inflammatory indices. Nevertheless, lowest oxygen saturation (LaSO2) and mean oxygen saturation (MaSO2) had a reverse trend. MaSO2 and TS90 were the sleep parameters that were associated with the largest number of inflammatory indices, the former had a negative correlation with almost all inflammatory indices except ELR and LHR, while the latter had a positive correlation. In addition, there was no significant association between TST and the inflammatory indices involved in this study.
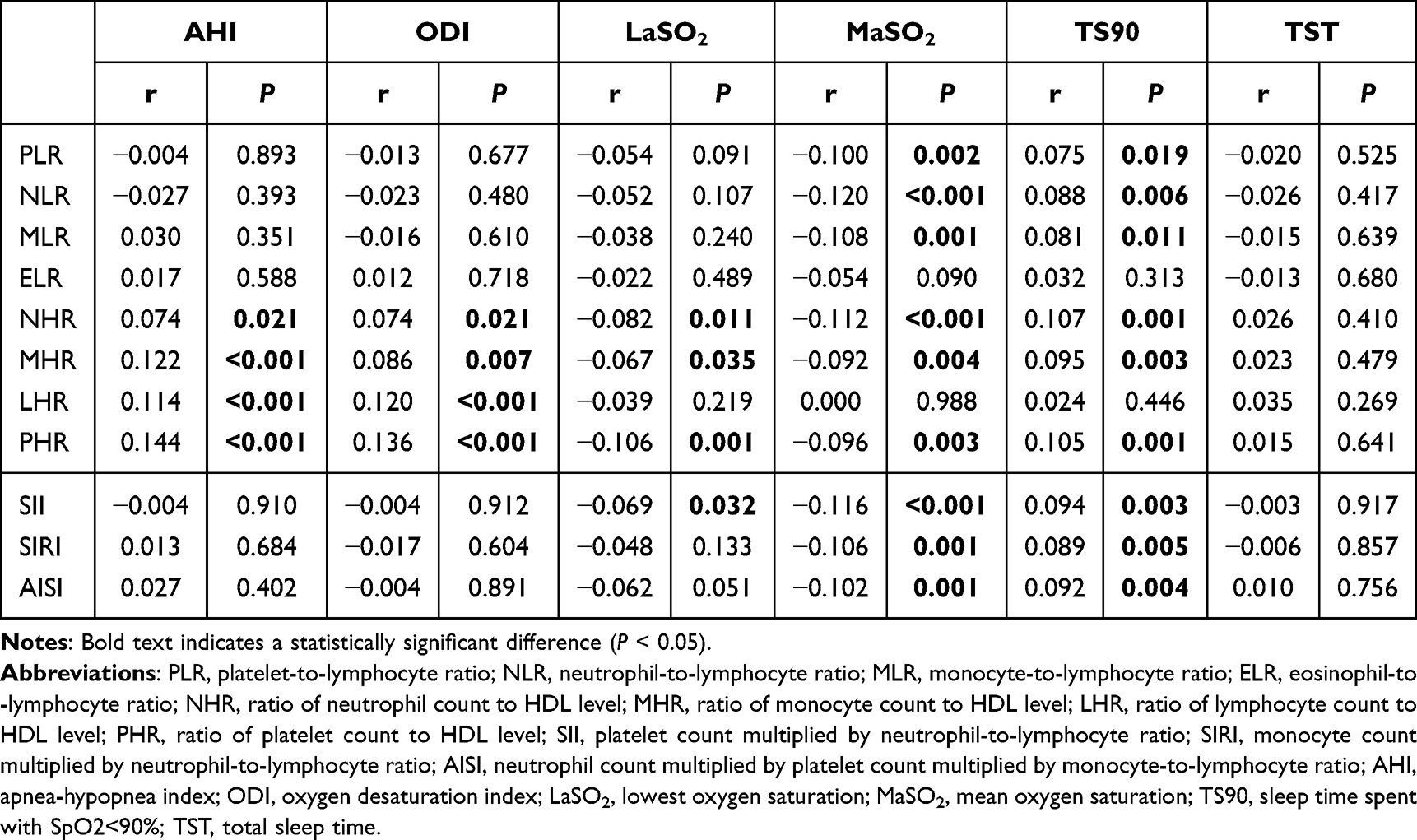 |
Table 2 Correlation Analysis of Inflammatory Indices and Sleep Parameters in OSA Patients |
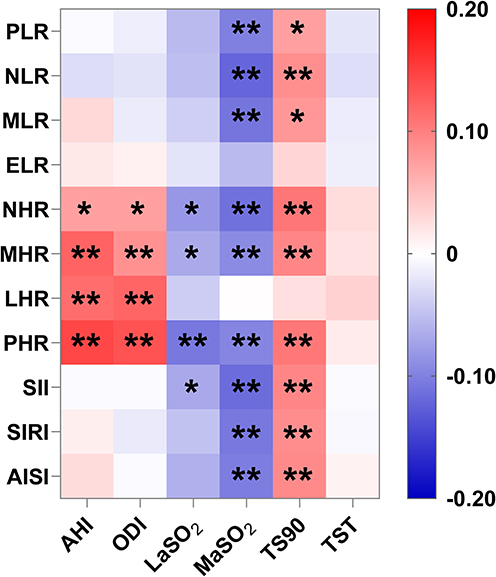 |
Figure 2 Correlation analysis of inflammatory indices and sleep parameters in OSA patients. Positive correlations are shown in red and negative correlations are shown in blue. *means P < 0.05, **means P < 0.01. Abbreviations: PLR, platelet-to-lymphocyte ratio; NLR, neutrophil-to-lymphocyte ratio; MLR, monocyte-to-lymphocyte ratio; ELR, eosinophil-to-lymphocyte ratio; NHR, ratio of neutrophil count to HDL level; MHR, ratio of monocyte count to HDL level; LHR, ratio of lymphocyte count to HDL level; PHR, ratio of platelet count to HDL level; SII, platelet count multiplied by neutrophil-to-lymphocyte ratio; SIRI, monocyte count multiplied by neutrophil-to-lymphocyte ratio; AISI, neutrophil count multiplied by platelet count multiplied by monocyte-to-lymphocyte ratio; AHI, apnea-hypopnea index; ODI, oxygen desaturation index; LaSO2, lowest oxygen saturation; MaSO2, mean oxygen saturation; TS90, sleep time spent with SpO2<90%; TST, total sleep time. |
Associations Between Inflammatory Indices and CVD in OSA Patients
Inflammatory indices with significant differences between the CVD and non-CVD groups were selected for subsequent analysis. Multivariate logistic regression revealed the association between the inflammatory indices and CVD in OSA patients (Table 3). When treated as a continuous variable, NLR, MLR, NHR, MHR, and SIRI were suggested to be the risk factors for CVD in OSA patients. After adjusting sex, age, BMI, smoking and alcohol, hypertension, hyperlipemia, diabetes, and FLD in model 3, these inflammatory indices still indicated a strong association with CVD risk in OSA patients.
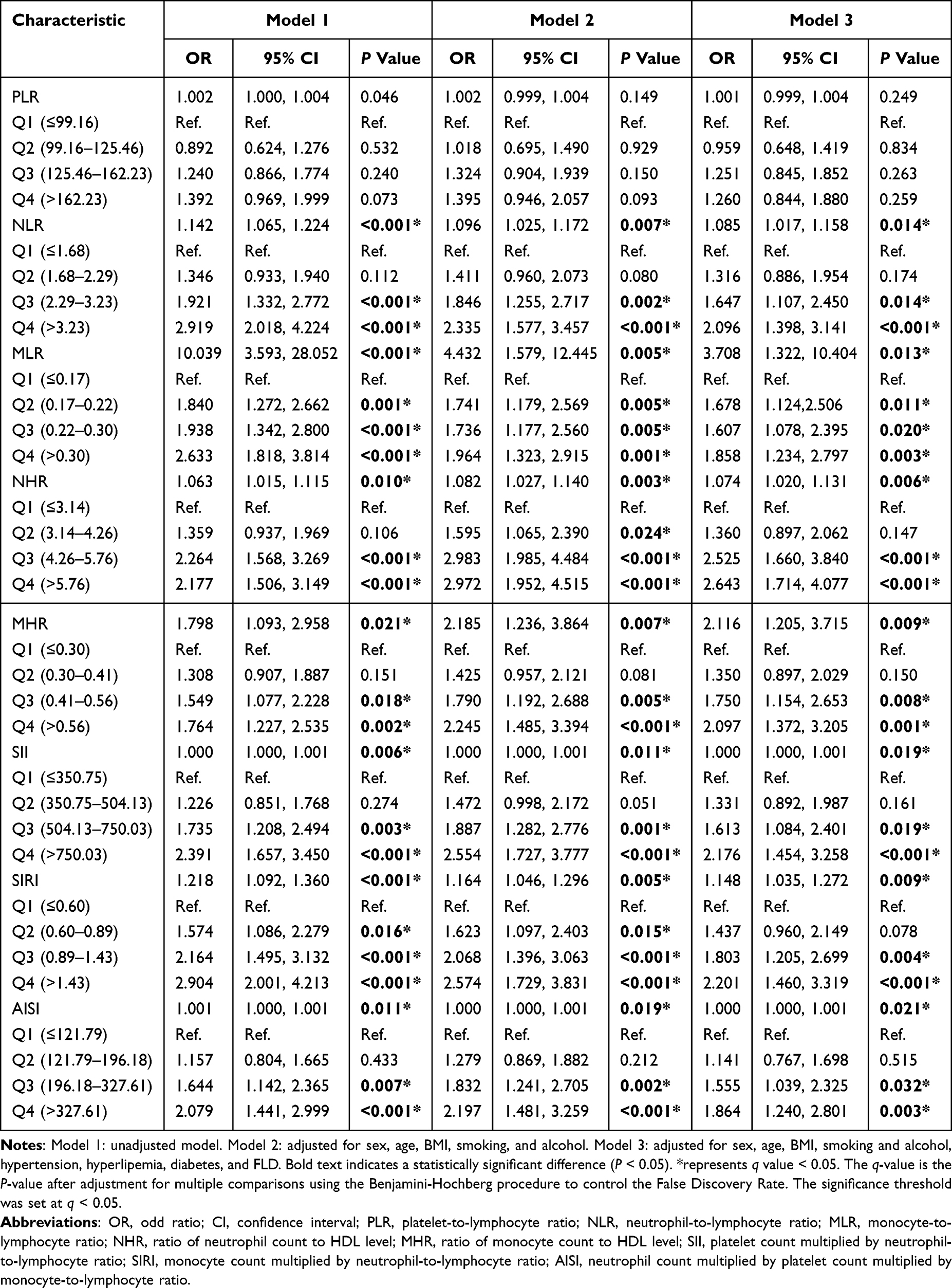 |
Table 3 ORs (95% CIs) for CVD According to Inflammatory Indices in OSA Patients |
When the inflammatory indices were categorized into quartiles, this positive correlation remained to exist in MLR. We set the Q1 group of MLR as the reference, and the risk of CVD was increased in Q2, Q3 and Q4 group. Besides, other inflammatory markers including NLR NHR, MHR, and SIRI were significantly associated with CVD at Q3 and Q4 levels compared with their Q1 groups. After FDR correction, NLR, MLR, NHR, MHR, and SIRI remained significantly associated with CVD in OSA patients (Table S1).
ROC Analysis of Inflammation Indices in Discriminating CVD in OSA Patients
ROC curves were depicted to evaluate the discriminatory ability of NLR, MLR, NHR, MHR, and SIRI on CVD of OSA patients (Figure 3), and the detailed information was presented in Table 4. After adjusted for sex, age, BMI, smoking and alcohol, hypertension, hyperlipemia, diabetes, and FLD in model 3, all five indices demonstrated fair discrimination for CVD, with AUC values ranging from 0.734 to 0.736. These associations remained significant after FDR correction (Table S2).
 |
Table 4 ROC Analysis of NLR, MLR, NHR, MHR, and SIRI in Discriminating CVD in OSA Patients |
 |
Figure 3 ROC Curve of NLR, MLR, NHR, MHR, and SIRI for discriminating OSA patients with CVD. After adjusting for sex, age, BMI, smoking and alcohol, hypertension, hyperlipemia, diabetes, and FLD in model 3, the ROC curves of 5 inflammatory indices for discriminating OSA patients with CVD were plotted. (A) NLR: AUC=0.734 (0.703,0.765), P<0.001. (B) MLR: AUC= 0.735 (0.704,0.766), P<0.001. (C) NHR: AUC=0.736 (0.705,0.767), P<0.001. (D) MHR: AUC=0.734 (0.703, 0.765), P<0.001. (E) SIRI: AUC=0.735 (0.704,0.766), P<0.001. Abbreviations: NLR, neutrophil-to-lymphocyte ratio; MLR, monocyte-to-lymphocyte ratio; NHR, ratio of neutrophil count to HDL level; MHR, ratio of monocyte count to HDL level; SIRI, monocyte count multiplied by neutrophil-to-lymphocyte ratio; AUC, area under the curve. |
Discussion
The study comprehensively explored the direct relationship between 11 immuno-inflammatory biomarkers (PLR, NLR, MLR, ELR, NHR, MHR, LHR, PHR, SII, SIRI, and AISI) and OSA, providing valuable insights into the inflammatory profile of the disorder. Furthermore, we focused on the associations between these biomarkers and CVD in OSA patients, and the results indicated that NLR, MLR, NHR, MHR, and SIRI showed significant associations with CVD and demonstrated discriminatory ability in distinguishing OSA patients with CVD.
OSA can lead to a range of physiological disorders that cannot be characterized by AHI alone, including hypoxic burden, heart rate response, and respiratory arousal intensity, which further trigger autonomic, inflammatory, oxidative, metabolic, and vascular abnormalities, thereby increasing the risk of cardiovascular and cerebrovascular disease.28 In China, many OSA patients refuse to do other examinations except polysomnography and hematologic examination, so it is necessary to develop some convenient indicators to screen for CVD comorbidities. These accessible hematology indices can be utilized for preliminary screening of OSA patients at risk of CVD, helping to identify high-risk individuals. Especially when access to advanced cardiovascular tests is limited, or when patients refuse additional tests beyond polysomnography and basic blood tests, in such cases, abnormal inflammatory indices can serve as early warning signals, suggesting closer cardiovascular assessment, cardiology referral, or enhanced management of modifiable risk factors. This strategy not only guides further targeted examinations more effectively—avoiding both unnecessary procedures and potential missed diagnoses—but also optimizes medical resource allocation by reducing excessive healthcare expenditure. These indices may be utilized as complementary markers that may enhance established risk stratification algorithms of cardiovascular outcomes in OSA populations.
NLR has been considered a homeostatic marker of the immune system in many diseases.29 Neutrophils mainly reflect innate immunity, which could recruit, activate, and program other immune cells, and secrete a series of proinflammatory and immunomodulatory cytokines and chemokines.30 Low lymphocyte counts are common during systemic inflammatory responses and are associated with poor outcomes in cardiovascular diseases including heart failure, chronic ischemic heart disease, and acute coronary syndromes.31 NLR was regarded as a reliable marker of systemic inflammation and disease severity in OSA patients. A recent meta-analysis suggested that NLR was significantly higher in OSA patients compared to controls, especially those with severe OSA.32,33 Our results suggest that NLR is associated with nocturnal blood oxygen in OSA patients. Moreover, NLR was found to be significantly decreased in severe OSA patients after upper airway surgical intervention. However, the effect of CPAP treatment on NLR levels in OSA patients is inconsistent in different studies.34,35 Therefore, more research is needed to focus on the treatment of OSA patients and NLR levels in the future. Extensive evidence indicated that NLR was associated with cardiovascular risk.36 High log-transformed NLR was reported to be independently associated with the presence of atrial fibrillation in OSA patients.37 Similar to published literature, the result of this study suggested that NLR was independently associated with CVD in OSA patients. Peripheral blood monocytes are significantly increased in OSA patients and are considered biomarkers of inflammation.38 The increased inflammatory responsiveness of monocytes and macrophages may play an important role in chronic inflammatory diseases. The number of systemic monocytes and circulating monocytes increases gradually with the progression of atherosclerosis.39 MLR was identified as an independent predictor of all-cause mortality and CVD mortality in the general population.18 Our results suggested that MLR was strongly associated with nocturnal hypoxia in OSA patients and was an independent risk factor for patients with CVD.
Similar to NLR and MLR, NHR and MHR were also regarded as inflammatory biomarkers in many diseases.40,41 HDL is negatively associated with the risk of CVD and has reverse cholesterol transport, anti-inflammatory, antioxidant, vasodilatation, and antithrombotic functions.42 In this study, the median HDL of OSA patients with CVD was lower than that of the non-CVD group, although the statistical difference was not significant. This might be caused by the limitation of the study population. NHR and MHR are HDL-based inflammatory indices, which are associated with CVD risk. NHR was positively correlated with intima-media thickness of common carotid arteries43 and CVD risk in healthy populations.44 MHR has a high diagnostic value in acute aortic dissection,45 all-cause death, and poor functional outcomes of cerebrovascular accidents.46 Our study found that the levels of NHR and MHR were significantly correlated with sleep parameters in OSA patients, and the logistic analysis and ROC curves suggested their discriminatory power for CVD.
In addition, SIRI is a comprehensive indicator of systemic inflammatory response based on neutrophils, monocytes, and lymphocytes.47 Recent studies have shown that SIRI was associated with CVD risk48 and CVD mortality.49 Our study further confirmed the associative role of SIRI in relation to CVD risk in OSA patients, demonstrating its potential discriminatory ability.
The inflammatory indices that showed significant associations with CVD in our study are all derived from neutrophil counts, monocyte counts, and HDL cholesterol, which are key players in cardiovascular pathophysiology. Neutrophils promote vascular damage by promoting inflammation, releasing a series of proteases and generating reactive oxygen species, thereby promoting endothelial dysfunction and atherosclerosis.50 Monocytes can secrete inflammatory factors, infiltrate the vessel walls and differentiate into macrophages, driving the formation of foam cells and the progression of plaques.51,52 In contrast, HDL cholesterol exerts protective effects through reverse cholesterol transport, antioxidant, and anti-inflammatory functions. Consequently, ratios combining neutrophil or monocyte counts with HDL capture the imbalance between pro-inflammatory activation and loss of anti-atherogenic protection.53,54 Similarly, composite indices such as SIRI integrate neutrophil, monocyte, and lymphocyte counts, reflecting a broader systemic inflammatory state that may exacerbate vascular injury. These mechanisms provide a plausible explanation for the observed significant associations of NLR, MLR, NHR, MHR, and SIRI with CVD risk in OSA patients.
Although the AUC values of NLR, MLR, NHR, MHR, and SIRI ranged from 0.734 to 0.736, indicating fair discriminatory ability, these effect sizes should be interpreted with caution. First, the moderate AUC values highlight the clinical utility limitations of these indices, as they cannot provide definitive diagnostic accuracy on their own. Instead, their primary value lies in serving as practical, easily accessible screening tools that may flag OSA patients at increased cardiovascular risk. From a clinical decision-making perspective, these hematologic indices can assist physicians in identifying high-risk individuals who may warrant further cardiovascular assessment, lifestyle modification, or preventive interventions. Importantly, they should not replace established diagnostic modalities but rather complement existing clinical frameworks by providing a cost-effective, preliminary stratification method. Integration of these indices into routine OSA management could therefore enhance early risk recognition, and optimize allocation of healthcare resources without adding excessive burden to patients or clinical systems.
There are some limitations. Firstly, this study is a cross-sectional study and cannot provide evidence of causality. Second, our study was conducted at a single center using a retrospective design, which may introduce selection bias and limit generalizability to other populations, and the absence of follow-up data or prospective cardiovascular outcomes prevented us from determining whether these indices predict incident CVD events over time. Third, we did not perform external validation in an independent cohort. Moreover, the statistical power of our study was calculated based on an odds ratio of 1.5. Consequently, for exposure variables with effect sizes weaker than this threshold, the power to detect statistically significant associations is reduced. This means that our study might have failed to identify some true weak associations, potentially leading to type II errors for those factors. Larger sample sizes are needed to explore these subtler associations. Future prospective, multi-center longitudinal studies are necessary to confirm the prognostic value of these indices for incident CVD events in OSA patients.
Conclusion
In conclusion, our study identified NLR, MLR, NHR, MHR, and SIRI as hematologic inflammatory biomarkers associated with CVD in patients with OSA. These easily obtainable markers may assist in early risk stratification and should be regarded as adjunctive indicators that complement, rather than substitute, established CVD risk assessment approaches. Their primary utility lies in preliminary screening and early recognition of high-risk individuals, thereby facilitating subsequent comprehensive cardiovascular evaluation within current clinical practice frameworks. Future multicenter and longitudinal studies are needed to validate their prognostic role.
Data Sharing Statement
The data used during the current study is available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the medical ethics Committee of the Second Xiangya Hospital of Central South University, approval number [Acceptance no. LYEC2024-0078]. Informed consent was obtained from all enrolled subjects.
Author Contributions
D.Z. and R.O. – conceptualization, writing – review and editing. Y.O. – writing – original draft, formal analysis. X.W. – writing – review and editing, investigation, resources. D.Z. – funding acquisition, project administration. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the National Major Science and Technology Project for the Prevention and Treatment of Cancer, Cardiovascular and Cerebrovascular Diseases, Respiratory and Metabolic Diseases (Grant No. 2024ZD0529100), the Natural Science Foundation of Hunan Province (Grant No. 2024JJ5488), the Health Commission of Hunan Province (Grant No. W20243062), and the National Key Clinical Specialty Construction Projects of China.
Disclosure
The authors declare that they have no competing interests.
References
1. Lv R, Liu X, Zhang Y, et al. Pathophysiological mechanisms and therapeutic approaches in obstructive sleep apnea syndrome. Signal Transduct Target Ther. 2023;8(1):218. doi:10.1038/s41392-023-01496-3
2. Lyons MM, Bhatt NY, Pack AI, et al. Global burden of sleep-disordered breathing and its implications. Respirology. 2020;25(7):690–702. doi:10.1111/resp.13838
3. Gleeson M, McNicholas WT. Bidirectional relationships of comorbidity with obstructive sleep apnoea. Eur Respir Rev. 2022;31(164):210256. doi:10.1183/16000617.0256-2021
4. Simpamba K, May JL, Waghat A, et al. Obstructive sleep apnea and excessive daytime sleepiness among commercial motor vehicle drivers in Lusaka, Zambia. J Clin Sleep Med. 2023;19(7):1191–1198. doi:10.5664/jcsm.10538
5. Alakörkkö I, Törmälehto S, Leppänen T, et al. The economic cost of obstructive sleep apnea: a systematic review. Sleep Med Rev. 2023;72:101854. doi:10.1016/j.smrv.2023.101854
6. Streatfeild J, Smith J, Mansfield D, et al. The social and economic cost of sleep disorders. Sleep. 2021;44(11). doi:10.1093/sleep/zsab132
7. O’Donnell C, O’Mahony AM, McNicholas WT, et al. Cardiovascular manifestations in obstructive sleep apnea: current evidence and potential mechanisms. Pol Arch Intern Med. 2021;131(6):550–560. doi:10.20452/pamw.16041
8. Tan JWC, Leow LC, Wong S, et al. Asian Pacific Society of Cardiology consensus statements on the diagnosis and management of obstructive sleep apnoea in patients with cardiovascular disease. Eur Cardiol. 2022;17:e16. doi:10.15420/ecr.2021.59
9. Heilbrunn ES, Ssentongo P, Chinchilli VM, et al. Sudden death in individuals with obstructive sleep apnoea: a systematic review and meta-analysis. BMJ Open Respir Res. 2021;8(1). doi:10.1136/bmjresp-2020-000656
10. Lorenzi-Filho G, Almeida FR, Strollo PJ. Treating OSA: current and emerging therapies beyond CPAP. Respirology. 2017;22(8):1500–1507. doi:10.1111/resp.13144
11. Sánchez-de-la-Torre M, Gracia-Lavedan E, Benitez ID, et al. Adherence to CPAP treatment and the risk of recurrent cardiovascular events: a meta-analysis. JAMA. 2023;330(13):1255–1265. doi:10.1001/jama.2023.17465
12. Javaheri S, Javaheri S, Gozal D, et al. Treatment of OSA and its impact on cardiovascular disease, part 2: JACC state-of-the-art review. J Am Coll Cardiol. 2024;84(13):1224–1240. doi:10.1016/j.jacc.2024.07.024
13. Kheirandish-Gozal L, Gozal D. Obstructive sleep apnea and inflammation: proof of concept based on two illustrative cytokines. Int J Mol Sci. 2019;20(3):459. doi:10.3390/ijms20030459
14. Veler H. Sleep and inflammation: bidirectional relationship. Sleep Med Clin. 2023;18(2):213–218. doi:10.1016/j.jsmc.2023.02.003
15. Li YE, Ren J. Association between obstructive sleep apnea and cardiovascular diseases. Acta Biochim Biophys Sin. 2022;54(7):882–892. doi:10.3724/abbs.2022084
16. Seo I-H, Lee Y-J. Usefulness of complete blood count (CBC) to assess cardiovascular and metabolic diseases in clinical settings: a comprehensive literature review. Biomedicines. 2022;10(11):2697. doi:10.3390/biomedicines10112697
17. Lan -C-C, Su W-L, Yang M-C, et al. Predictive role of neutrophil-percentage-to-albumin, neutrophil-to-lymphocyte and eosinophil-to-lymphocyte ratios for mortality in patients with COPD: evidence from NHANES 2011–2018. Respirology. 2023;28(12):1136–1146. doi:10.1111/resp.14589
18. Hua Y, Sun J-Y, Lou Y-X, et al. Monocyte-to-lymphocyte ratio predicts mortality and cardiovascular mortality in the general population. Int J Cardiol. 2023;379:118–126. doi:10.1016/j.ijcard.2023.03.016
19. Li J, He D, Yu J, et al. Dynamic status of SII and SIRI alters the risk of cardiovascular diseases: evidence from Kailuan cohort study. J Inflamm Res. 2022;15:5945–5957. doi:10.2147/JIR.S378309
20. Inonu koseoglu H, Pazarli AC, Kanbay A, et al. Monocyte count/HDL cholesterol ratio and cardiovascular disease in patients with obstructive sleep apnea syndrome: a multicenter study. Clin Appl Thromb Hemost. 2016;24(1):139–144. doi:10.1177/1076029616677803
21. Berry RB, Brooks R, Gamaldo C, et al. AASM scoring manual updates for 2017 (Version 2.4). J Clin Sleep Med. 2017;13(5):665–666. doi:10.5664/jcsm.6576
22. Liu L-S. [2010 Chinese guidelines for the management of hypertension]. Zhonghua Xin Xue Guan Bing Za Zhi. 2011;39(7):579–615. Polish
23. Li -J-J, Zhao S-P, Zhao D, et al. 2023 Chinese guideline for lipid management. Front Pharmacol. 2023;14:1190934. doi:10.3389/fphar.2023.1190934
24. Jia W, Weng J, Zhu D, et al. Standards of medical care for type 2 diabetes in China 2019. Diabetes Metab Res Rev. 2019;35(6):e3158. doi:10.1002/dmrr.3158
25. Zhao J, Cai X, Hu J, et al. J-shaped relationship between weight-adjusted-waist index and cardiovascular disease risk in hypertensive patients with obstructive sleep apnea: a cohort study. Diabetes Metab Syndr Obes. 2024;17:2671–2681. doi:10.2147/DMSO.S469376
26. Bozkurt B, Coats AJS, Tsutsui H, et al. Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur J Heart Fail. 2021;23(3):352–380. doi:10.1002/ejhf.2115
27. Yeghiazarians Y, Jneid H, Tietjens JR, et al. Obstructive sleep apnea and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;144(3):e56–e67. doi:10.1161/CIR.0000000000000988
28. Redline S, Azarbarzin A, Peker Y. Obstructive sleep apnoea heterogeneity and cardiovascular disease. Nat Rev Cardiol. 2023;20(8):560–573. doi:10.1038/s41569-023-00846-6
29. Buonacera A, Stancanelli B, Colaci M, et al. Neutrophil to lymphocyte ratio: an emerging marker of the relationships between the immune system and diseases. Int J Mol Sci. 2022;23(7):3636. doi:10.3390/ijms23073636
30. Li Y, Wang W, Yang F, et al. The regulatory roles of neutrophils in adaptive immunity. Cell Commun Signal. 2019;17(1):147. doi:10.1186/s12964-019-0471-y
31. Núñez J, Miñana G, Bodí V, et al. Low lymphocyte count and cardiovascular diseases. Curr Med Chem. 2011;18(21):3226–3233. doi:10.2174/092986711796391633
32. Attia MM, Qasim MA, Alhamwi HS, et al. Using the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as prognostic markers for obstructive sleep apnea: a systematic review and meta-analysis of observational studies. Cureus. 2024;16(10):e72539. doi:10.7759/cureus.72539
33. Rha M-S, Kim C-H, Yoon J-H, et al. Association between the neutrophil-to-lymphocyte ratio and obstructive sleep apnea: a meta-analysis. Sci Rep. 2020;10(1):10862. doi:10.1038/s41598-020-67708-w
34. Zota IM, Adam CA, Marcu DTM, et al. CPAP influence on readily available inflammatory markers in OSA-A pilot study. Int J Mol Sci. 2022;23(20):12431. doi:10.3390/ijms232012431
35. Al-Halawani MD, Kyung C, Liang F, et al. Treatment of obstructive sleep apnea with CPAP improves chronic inflammation measured by neutrophil-to-lymphocyte ratio. J Clin Sleep Med. 2020;16(2):251–257. doi:10.5664/jcsm.8176
36. Trtica Majnarić L, Guljaš S, Bosnić Z, et al. Neutrophil-to-lymphocyte ratio as a cardiovascular risk marker may be less efficient in women than in men. Biomolecules. 2021;11(4):528. doi:10.3390/biom11040528
37. Yu B, Wei J, Zhao J, et al. The neutrophil-to-lymphocyte ratio is a potential biomarker for the occurrence of atrial fibrillation in patients with obstructive sleep apnea: a BIOMARKER OF AF IN OSA PATIENTS. Sleep Med. 2023;110:259–267. doi:10.1016/j.sleep.2023.08.004
38. Jiang Y, Lin C, Xu M, et al. Differences and risk factors of peripheral blood immune cells in patients with obstructive sleep apnea. Nat Sci Sleep. 2024;16:737–749. doi:10.2147/NSS.S458098
39. Hoogeveen RM, Nahrendorf M, Riksen NP, et al. Monocyte and haematopoietic progenitor reprogramming as common mechanism underlying chronic inflammatory and cardiovascular diseases. Eur Heart J. 2018;39(38):3521–3527. doi:10.1093/eurheartj/ehx581
40. Chen L, Zheng C, Luan H, et al. Clinical and diagnostic value of high-density lipoprotein-based inflammatory indices and lipid ratios in young adults with schizophrenia. J Inflamm Res. 2024;17:6363–6374. doi:10.2147/JIR.S473528
41. Villegas García L, Patró E, Barbero JD, et al. Lymphocyte-derived and lipoprotein-derived inflammatory ratios as biomarkers in bipolar disorder type I: characteristics, predictive values, and influence of current psychopharmacological treatments. Psychoneuroendocrinology. 2025;171:107209. doi:10.1016/j.psyneuen.2024.107209
42. Endo Y, Fujita M, Ikewaki K. HDL functions-current status and future perspectives. Biomolecules. 2023;13(1):105. doi:10.3390/biom13010105
43. Boughanem H, Torres-Peña JD, Arenas-de Larriva AP, et al. Mediterranean diet, neutrophil count, and carotid intima-media thickness in secondary prevention: the CORDIOPREV study. Eur Heart J. 2024.
44. Pan X, Zhang X, Ban J, et al. Association of neutrophil to high-density lipoprotein cholesterol ratio with cardiac ultrasound parameters and cardiovascular risk: a cross-sectional study based on healthy populations. J Inflamm Res. 2023;16:1853–1865. doi:10.2147/JIR.S406102
45. Du X, Zhang S, Xu J, et al. Diagnostic value of monocyte to high-density lipoprotein ratio in acute aortic dissection in a Chinese han population. Expert Rev Mol Diagn. 2020;20(12):1243–1252. doi:10.1080/14737159.2020.1847647
46. Xu Q, Wu Q, Chen L, et al. Monocyte to high-density lipoprotein ratio predicts clinical outcomes after acute ischemic stroke or transient ischemic attack. CNS Neurosci Ther. 2023;29(7):1953–1964. doi:10.1111/cns.14152
47. Zheng Y, Zhong D, Li J, et al. Systemic immune-inflammation index and long-term mortality in patients with hypertension: a cohort study. J Hypertens. 2024.
48. Lin K, Lan Y, Wang A, et al. The association between a novel inflammatory biomarker, systemic inflammatory response index and the risk of diabetic cardiovascular complications. Nutr Metab Cardiovasc Dis. 2023;33(7):1389–1397. doi:10.1016/j.numecd.2023.03.013
49. Kong F, Huang J, Xu C, et al. System inflammation response index: a novel inflammatory indicator to predict all-cause and cardiovascular disease mortality in the obese population. Diabetol Metab Syndr. 2023;15(1):195. doi:10.1186/s13098-023-01178-8
50. Chistiakov DA, Bobryshev YV, Orekhov AN. Neutrophil’s weapons in atherosclerosis. Exp Mol Pathol. 2015;99(3):663–671. doi:10.1016/j.yexmp.2015.11.011
51. Hristov M, Heine GH. Monocyte subsets in atherosclerosis. Hamostaseologie. 2014;35(2):105–112. doi:10.5482/HAMO-14-08-0030
52. Wu W, Bao W, Chen X, et al. Endothelial Gata6 deletion reduces monocyte recruitment and proinflammatory macrophage formation and attenuates atherosclerosis through Cmpk2-Nlrp3 pathways. Redox Biol. 2023;64:102775. doi:10.1016/j.redox.2023.102775
53. Navab M, Reddy ST, Van Lenten BJ, et al. HDL and cardiovascular disease: atherogenic and atheroprotective mechanisms. Nat Rev Cardiol. 2011;8(4):222–232. doi:10.1038/nrcardio.2010.222
54. Linton MF, Yancey PG, Tao H, et al. HDL function and atherosclerosis: reactive dicarbonyls as promising targets of therapy. Circ Res. 2023;132(11):1521–1545. doi:10.1161/CIRCRESAHA.123.321563
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.