")
Back to Journals » Vascular Health and Risk Management » Volume 20
Association of Handgrip Strength and Cardiovascular Disease Risk Among Middle-Aged Postmenopausal Women: An Analysis of the Korea National Health and Nutrition Examination Survey 2014–2019
Received 6 November 2023
Accepted for publication 9 April 2024
Published 12 April 2024 Volume 2024:20 Pages 183—194
DOI https://doi.org/10.2147/VHRM.S442277
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roland Asmar
Jinkyung Park,1 Sooyeon Park2
1College of Nursing, Chonnam National University, Gwangju, 61469, Republic of Korea; 2College of Nursing, Konyang University, Daejeon, 35365, Republic of Korea
Correspondence: Sooyeon Park, Medical Campus, 158 Gwanjeodong-ro, Seo-gu, Daejeon, 35365, South Korea, Tel +82 42 600 8584, Fax +82 42 600 8555, Email [email protected]
Purpose: Handgrip strength is an indicator of overall muscle strength and has been associated with an increased risk of cardiovascular disease. Evidence suggests that menopause is a risk factor for cardiovascular disease in women, and muscle strength decreases progressively after menopause. Despite the prognostic importance of the decline in muscle strength and increased cardiovascular disease risk among postmenopausal women, evidence of their association is limited. This study aimed to investigate the relationship between handgrip strength and cardiovascular disease risk among postmenopausal, middle-aged Korean women.
Patients and Methods: Using pooled cohort equations, we calculated the 10-year risk of atherosclerotic cardiovascular disease (ASCVD) among postmenopausal women (N = 2019) aged 50– 64 years without cardiovascular disease history from the 2014– 2019 Korea National Health and Nutrition Examination Survey. Relative grip strength was defined as measured grip strength divided by body mass index. Logistic regression analysis of a complex sampling design was performed to evaluate the association between relative grip strength and a predicted 10-year ASCVD risk ≥ 7.5%.
Results: The average handgrip strength was 24.8 kg, and 5.2% of women were considered for sarcopenia (< 18 kg). The quartile-stratified relative grip strength was negatively associated with 10-year ASCVD risk (p < 0.001). In the multiple logistic regression analysis, the adjusted odds ratio for the highest relative grip strength quartile was 0.53 (95% confidence interval [CI]: 0.36– 0.78), and that of the group who breastfed for more than 12 months was 1.75 (95% CI: 1.36– 2.25) for 10-year ASCVD risk.
Conclusion: Increased handgrip strength may be associated with lower cardiovascular disease risk among middle-aged postmenopausal women in Korea. Our findings provide critical evidence regarding the importance of increasing handgrip strength among postmenopausal, middle-aged women to reduce cardiovascular disease risk. Handgrip strength measurement might be a valuable screening tool for cardiovascular disease prevention.
Keywords: cardiovascular disease, relative grip strength, menopause, sarcopenia
Introduction
Cardiovascular disease (CVD) is the leading cause of death globally and remains one of the most serious public health concerns. Generally, CVD encompasses a group of heart and blood vessel disorders, including coronary heart disease, cerebrovascular disease, peripheral arterial disease, rheumatic heart disease, congenital heart disease, deep vein thrombosis, and pulmonary embolism.1 The overall prevalence of CVD has steadily increased, nearly doubling from 271 million in 1990 to 523 million in 2019[Roth, 2020]. The World Health Organization1 reports that CVD accounted for nearly 32% of all global deaths in 2019, with 85% of those deaths due to heart attacks and strokes. In South Korea, heart disease has been the leading cause of death for nearly a decade, and the prevalence of atherosclerotic CVD (ASCVD) continues to increase with age until 79 years.2 Over the past decade, mortality and hospitalization rates due to CVD have steadily increased in South Korea. While the mortality rate decreased until 2010, it subsequently increased to 123 per 100,000 people in 2018.3 In this context, identifying and quantifying the major risk factors for CVD is essential to optimize preventive strategies.4
There are many risk factors that contribute to CVD, including modifiable factors such as high blood pressure, abdominal obesity, abnormal lipid levels, smoking, diabetes mellitus, stress, unhealthy diets, and physical inactivity. These factors are the leading causes of cardiovascular morbidity and mortality.5 Recently, there has been growing interest in understanding the role of muscle strength as a CVD risk factor, given its association with other risk factors such as hypertension, diabetes, and metabolic syndrome.6
Muscle strength is an important predictor of health, but losses of skeletal muscle mass and strength typically occur with increasing age.7,8 Sarcopenia, the age-related loss of skeletal muscle mass accompanied by declining strength and function,9 is generally evaluated based on three criteria: muscle mass, physical performance, and strength. Handgrip strength correlates with the strength of other body compartments10 and is gaining attention as a diagnostic measure for sarcopenia.11,12 Higher handgrip strength has been associated with cardiac structure and function (with less cardiac hypertrophy and remodeling)13 and has been used as a reliable tool for screening CVD risk. Recent studies recognize the association between strength and CVD risk.12,14
Although muscle strength has recently gained support as a consistent and reliable indicator of cardiovascular risk,15–17 there is currently no formalized standard measure for muscle strength. Studies have investigated the associations between muscle strength and various diseases, leading to a wide variety of muscle strength types and measurement methods in academia and clinical practice. Recently, relative grip strength (absolute handgrip strength divided by body mass index) has been recommended as a handgrip strength measure because physical characteristics such as weight and height can affect absolute handgrip strength.16 Relative grip strength has been evaluated as a more reliable predictor of CVD risk than absolute handgrip strength.15,17,18
Decreased muscle strength has been reported to increase the risk of cardiovascular death and all-cause mortality and is associated with cardiometabolic risk, including the risk of metabolic syndrome19 and diabetes.20 Low handgrip strength, a representative indicator of low muscle strength, has been shown to increase the risk of all-cause mortality, including mortality from CVD.14 Many epidemiological studies have reported a correlation between handgrip strength and cardiometabolic diseases and mortality. The PURE (Prospective Urban Rural Epidemiology) study, a large longitudinal study conducted in 17 countries, found that handgrip strength was inversely associated with all-cause mortality, cardiovascular mortality, myocardial infarction, and stroke. Handgrip strength was a more effective predictor of CVD than systolic blood pressure over a 4-year follow-up period.21 Additionally, relative grip strength was significantly associated with cardiovascular health biomarkers in adults, with higher relative grip strength associated with favorable cardiovascular profiles.16
Meanwhile, muscle strength varies with age, gender, and body size.22,23 Age-related muscle strength loss correlates with a loss of skeletal muscle mass.24 Although sarcopenia is known as a geriatric disease, it is seen across all age groups, including in middle age.10 Muscle loss begins around 40 years of age,25 with loss of muscle mass and strength becoming evident around the age of 50.26,27 Although muscle mass loss with aging is more prevalent in men, sarcopenia is a more serious public health problem for women due to longer lifespans and higher disability rates.28 Decreased estrogen levels, decreased bone density and muscle mass, decreased muscle strength, and increased intramuscular fat are particularly pronounced among middle-aged women during menopause.29–31 A recent study in Asia found that about 12% of postmenopausal, middle-aged women were in the pre-sarcopenic stage.32 Furthermore, hormonal changes in menopausal women are associated with a higher risk of CVD.33 Specifically, one study found that the risk of CVD was significantly higher in middle-aged women entering menopause relative to those who were premenopausal.34 This highlights middle-aged women as a population in need of early detection and prevention, as they lose muscle mass and strength during menopause and aging and face increased cardiovascular risk.35,36
Identifying patients at high risk of developing CVD is a key component of CVD prevention.37 Therefore, effective screening strategies for CVD in high-risk postmenopausal women can be used to detect and prevent risk factors early, both clinically and in everyday life. However, few studies have examined the association of relative grip strength with CVD in postmenopausal women, and most such studies have had relatively broad inclusion criteria, including both middle-aged and older adults.38 Additionally, although handgrip strength has been evaluated as a reliable indicator in several health outcome and association studies of older adults,39 there is a lack of evidence about muscle strength as a reliable marker in middle-aged adults. CVDs differ between the sexes and require a sex-specific and lifespan approach. To date, few studies in Korea have evaluated the independent prognostic significance of relative grip strength as a marker of muscle strength among postmenopausal, middle-aged women. Therefore, this study aimed to determine the association between relative grip strength and CVD risk and evaluate the utility of relative grip strength among middle-aged postmenopausal women using data from the latest 6 years of the Korea National Health and Nutrition Examination Survey (KNHANES), a dataset representative of the Korean population.
Methods
Data Collection and Participants
This study used data from the 2014–2019 KNHANES, encompassing the sixth through eighth survey waves. The KNHANES is a national research survey conducted annually by the Korean Ministry of Health and Welfare. This publicly available database contains information on Korean citizens aged 1 year or older and is designed to produce population-level statistics on health behaviors, outcomes, diet, and nutritional status. The sample design for KNHANES was drawn using a two-stage stratified cluster sampling method to ensure representativeness of the population, with household weights for household-level analysis and individual weights for individual-level analysis. The Korea Center for Disease Control and Prevention recommends using complex sampling methods when analyzing KNHANES raw data.40
A total of 45,022 individuals participated in the KNHANES from 2014–2019. Of these, we focused on 4343 postmenopausal women aged 45–64 years. The following individuals were excluded from our analysis: subjects with cancer (n = 292); subjects with a history of CVD, liver disease, kidney disease, hepatitis, thyroid disease, or arthritis (n = 1241); and subjects with missing data (n = 791). This resulted in a final sample size of 2019 individuals for analysis. Figure 1 depicts the sample selection procedures.
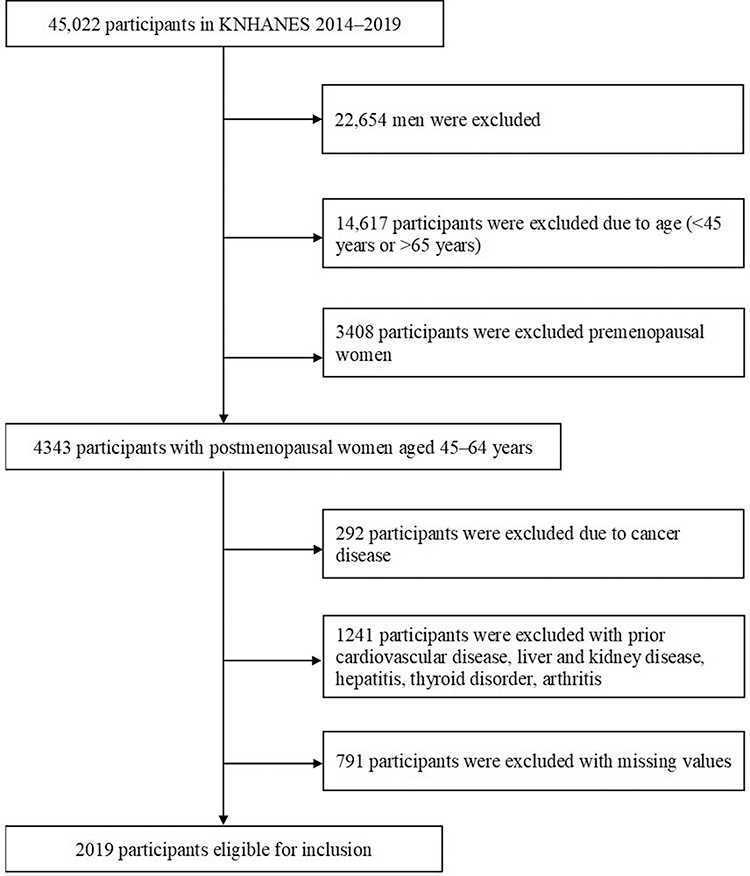 |
Figure 1 Flowchart of the study participant selection process. |
Estimated ASCVD Risk/Dependent Variable
We calculated the 10-year risk of a first hard ASCVD event using the pooled cohort equations for non-Hispanic Whites. Following the ACC/AHA (American College of Cardiology/American Heart Association) guidelines, the nine variables included in the 10-year ASCVD risk calculation are race, sex, age, total cholesterol, high-density lipoprotein cholesterol, blood pressure, diabetes diagnosis, treatment for hypertension, and smoking status. Table 1 presents relevant data for the subjects in this study, extracted from the KNHANES. Results were categorized into low-risk (less than 7.5% risk) and high-risk (greater than 7.5% risk) groups.31
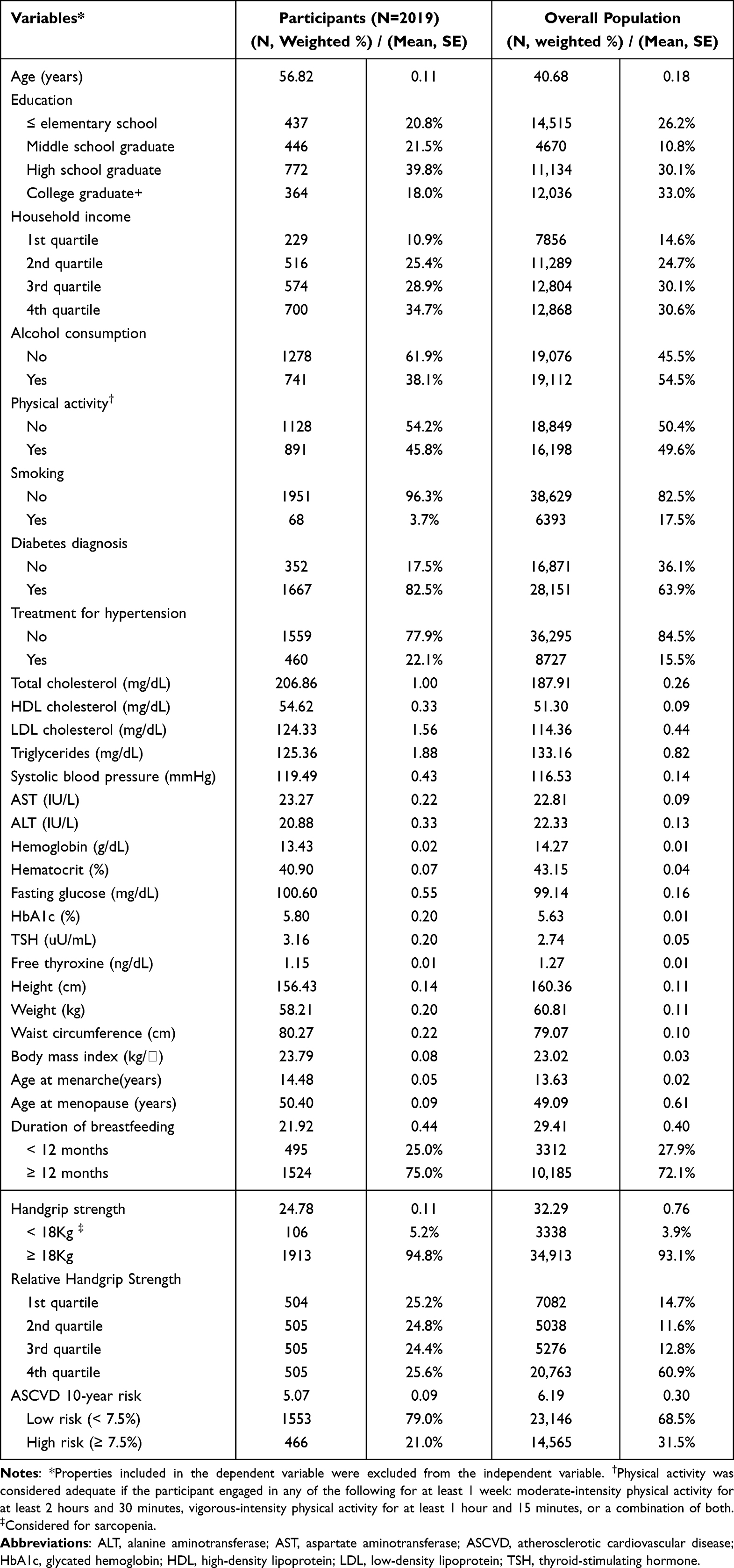 |
Table 1 General Characteristics of the Study Population According to the 2014–2019 KNHANES Survey |
Measurements and surveys were conducted following a minimum of 8 hours of fasting. Blood pressure readings were obtained using a sphygmomanometer; three measurements were taken, with the mean of the second and third readings constituting the examination blood pressure. We assessed serum glucose levels (using the hexokinase ultraviolet method) and hemoglobin A1C (using the high-performance liquid chromatography method). Diabetes mellitus was defined as a serum fasting glucose level ≥126 mg/dL, a hemoglobin A1C level ≥6.5%, the use of diabetes medication, the use of insulin injections, or a physician diagnosis. Total cholesterol and high-density lipoprotein cholesterol levels were determined using a standard enzymatic method. Cigarette smoking status was self-reported, and the use of antihypertensive medication was verified by research assistants. The pooled cohort equations for non-Hispanic Whites have demonstrated good discrimination for ASCVD prediction in Korean male and female subjects.32
Measurement of Grip Strength
We measured grip strength using a digital hand dynamometer (Digital grip strength dynamometer, T.K.K. 5401, Takei Scientific Instruments Co., Ltd., Tokyo, Japan), a tool with proven reliability and validity.33 Measurements were performed in accordance with the Southampton protocol for adult grip strength assessment. Subjects were seated with their forearms resting neutrally on the arms of a chair. We obtained three grip strength measurements for each hand, selecting the maximum strength for analysis. Participants were given a minimum of 30 seconds of rest between measurements. Grip strength was defined as the maximum measurement obtained from the dominant hand.34 Relative grip strength was calculated by dividing absolute grip strength by body mass index.35,36
Covariates
We evaluated covariates including individual sociodemographic characteristics and health-related factors. Individual sociodemographic variables were education (categorized as elementary school, middle school, high school, and college) and socioeconomic status (divided into quintiles). Health-related factors included alcohol consumption (dichotomized as yes/no for drinking at least once a month in the past year) and physical activity (dichotomized as yes/no for engaging in high-intensity activity for >75 min/week, moderate-intensity activity for >150 min/week, or a combination of both). Based on the guidance of previous studies, we also selected the duration of breastfeeding and age at menarche as covariates.37–40
Statistical Analysis
The KNHANES dataset was designed using complex, stratified, multistage, and probability-cluster sampling, certified as appropriate for generating representative statistics. Given these characteristics, we employed a complex sampling method to analyze the KNHANES data. We calculated descriptive statistics, including means and standard deviations for continuous variables, and relative frequencies for categorical variables. Chi-square tests were used for categorical variables and t-tests for continuous variables to analyze associations between demographic characteristics and 10-year ASCVD risk. We performed logistic regression analysis (considering the complex sampling design) to identify the association between relative grip strength quartiles and 10-year ASCVD risk, controlling for education, income, alcohol consumption, physical activity, breastfeeding duration, and age at menarche. All statistical analyses were conducted using SPSS Statistics for Windows, version 27.0 (IBM Corp., Armonk, NY, USA), with a significance level of p < 0.05.
Results
Participant Characteristics
Table 1 presents the sociodemographic and clinical characteristics of the 2014–2019 KNHANES survey population alongside those of the postmenopausal, middle-aged women included in this study.
The mean age of the overall population was 40.68 years, whereas the mean age of the postmenopausal, middle-aged women in our study was 56.82 years. In the study cohort, 39.8% had completed high school, while 33.0% of the overall population had attained a college education or higher. The distribution across household income quartiles was fairly even, though the fourth quartile was most prominently represented. In contrast to the overall population, postmenopausal, middle-aged women were less active (less likely to participate in moderate to vigorous physical activity) and less likely to smoke. Notably, the postmenopausal, middle-aged women had slightly higher mean ages at menarche (14.48 years) and menopause (50.4 years) relative to the overall population. Furthermore, 75% of these women had breastfed for longer than 12 months. Regarding handgrip strength, 5.2% of the postmenopausal, middle-aged women fell into the ≤18 kg category, indicative of sarcopenia. This percentage was higher than that of the overall population. To examine whether relative grip strength affects ASCVD risk, we categorized the participants into quartiles and presented the characteristics of each group (Supplementary Table 1). The 10-year ASCVD risk was 31.5% in the overall population, compared with 21.0% among the postmenopausal, middle-aged women.
Differences in Characteristics According to 10-Year ASCVD Risk
Table 2 shows the differences in baseline characteristics between subjects with high versus low 10-year ASCVD risk. There was a statistically significant difference between the high– and low–ASCVD-risk groups according to education levels (p < 0.001). There was also significant variation in 10-year ASCVD risk by household income quartile (p < 0.001) and alcohol consumption status (p = 0.009). Age at menarche (p = 0.002) and breastfeeding duration (p < 0.001) were also significant determinants influencing the 10-year ASCVD risk. The relative grip strength quartile groups also varied significantly in terms of their associations with 10-year ASCVD risk (p < 0.001).
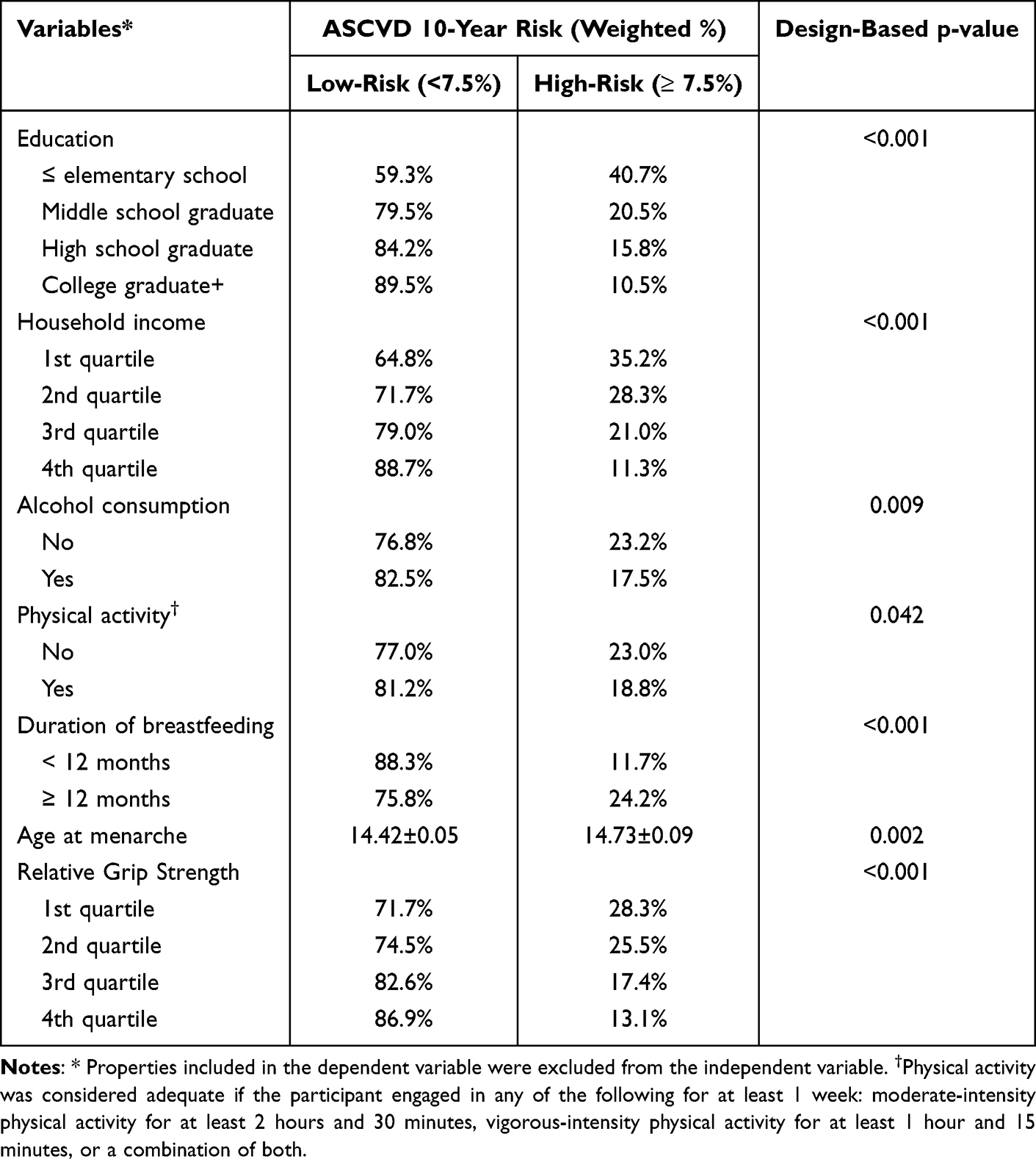 |
Table 2 Relationship Between Participant Characteristics and the 10-Year ASCVD Risk |
Factors Associated with Relative Grip Strength
Table 3, derived from a multiple logistic regression analysis, highlights the variables independently associated with relative grip strength. Relative to subjects with elementary education or below, participants who had completed middle school, high school, or college had odds ratios of 2.187, 2.551, and 3.440 respectively, signifying a diminished 10-year ASCVD risk. This suggests that higher educational attainment corresponded with a reduced 10-year ASCVD risk (p < 0.001).
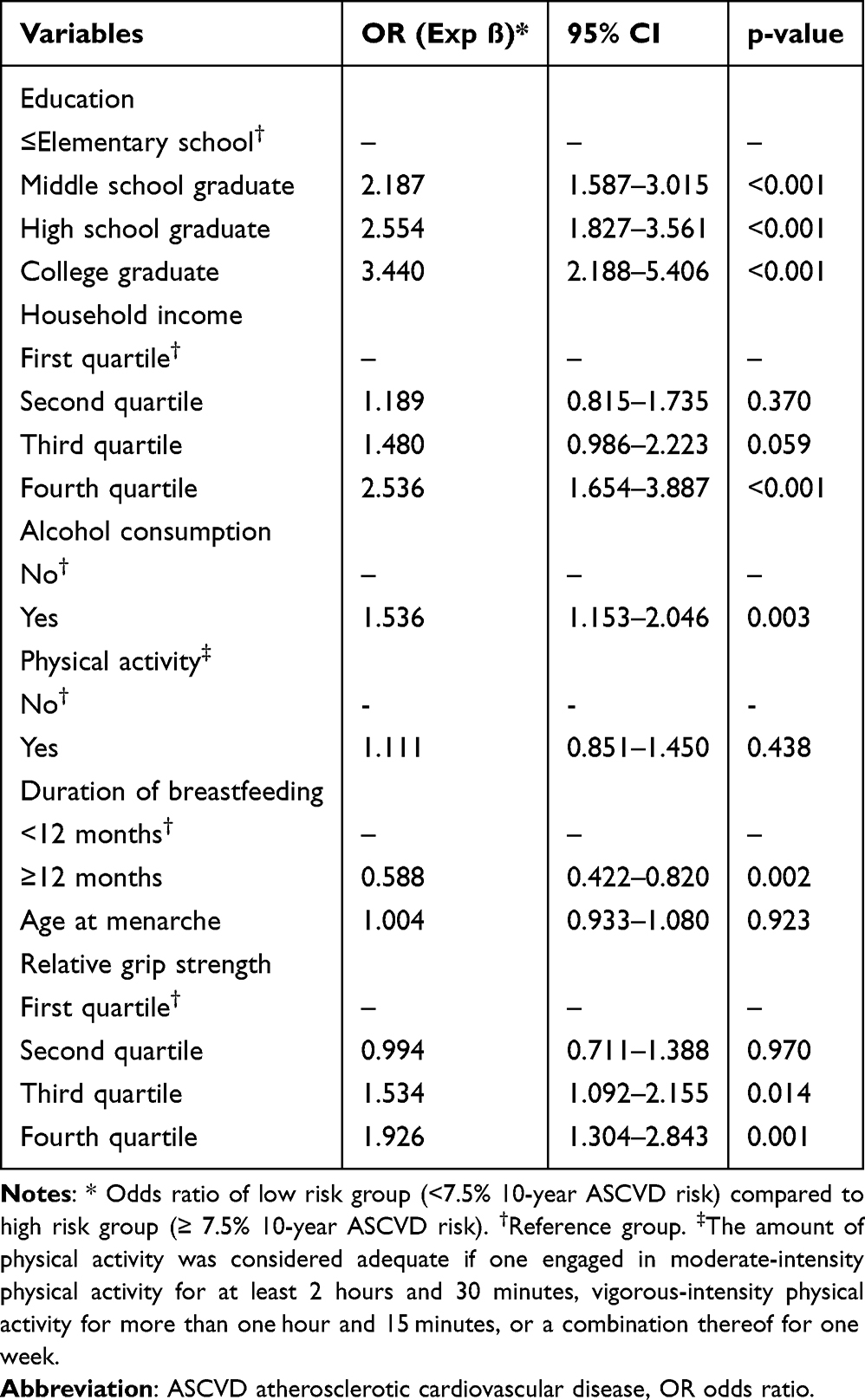 |
Table 3 Weighted Logistic Regression Analysis of Factors Affecting the 10-Year ASCVD Risk (N = 2019) |
Relative to the lowest income bracket, the subsequent higher income quartiles—lower-middle, upper-middle, and upper—had odds ratios of 1.189, 1.480, and 2.536, respectively, all suggesting a decreased 10-year ASCVD risk. In other words, higher household income was associated with lower ASCVD risk (p < 0.001). Subjects who consumed alcohol at least once a month had 1.536 times the odds of lower 10-year ASCVD risk relative to non-drinkers. Those who breastfed for more than 12 months had 0.588 times the odds of lower 10-year ASCVD risk than their counterparts who breastfed for less than 12 months. Relative to the low-relative-grip-strength category, the other grip strength quartiles—lower-middle, upper-middle, and high—had odds ratios of 0.994, 1.534, and 1.926, respectively, indicative of their association with a lower 10-year ASCVD risk.
Discussion
This study examined the association between relative grip strength and CVD risk among middle-aged, postmenopausal women using national population-based data from South Korea. To our knowledge, this was the first study to focus exclusively on middle-aged, postmenopausal women and to reveal the relationship between relative grip strength and 10-year cardiovascular disease risk after adjusting for socioeconomic factors, health-related behaviors, comorbidities, and reproductive factors.
The results showed that higher household income and education were associated with significantly lower CVD risk. Notably, a previous study found education and income to be key socioeconomic determinants that negatively impacted CVD outcomes among women, consistent with our findings.41 Additionally, previous studies, including systematic reviews and meta-analyses of gender differences in CVD and socioeconomic status, have found socioeconomic status to be inversely associated with cardiovascular risk. Recent European cardiovascular disease statistics show an increased risk of CVD in lower-income groups.42 A meta-analysis found that lower levels of education and living in low-income, disadvantaged neighborhoods were significantly associated with cardiovascular risk in women.42 Additionally, previous studies have consistently found increased cardiovascular risk among poorer women compared with their wealthier counterparts.43 In a study of African Americans, the age-adjusted hazard ratio for low versus high wealth was 1.06 (95% CI 0.62–1.81) in men but 2.14 (95% CI 0.62–1.81) in women.44 These socioeconomic factors contribute to disparities in women’s cardiovascular health. Compared with men, women of lower socioeconomic status have less time to seek medical care and preventive care45 and are reported to have inadequate healthcare and healthcare coverage.46 Moreover, low-income women often work long hours or temporary jobs for economic reasons, such as family support and childcare, which exposes them to high levels of stress, leaves them with less time to care for themselves, and reduces their time for exercise and other leisure activities.14,15 Therefore, reducing socioeconomic inequalities associated with coronary heart disease and CVD outcomes may require differing approaches for men and women.47
In this study, physical activity was not significantly associated with 10-year ASCVD risk. A recent study found that the middle-aged population (35–65 years) faces a higher risk of developing cardiovascular disease due to a predominantly sedentary lifestyle.48 In general, regular physical activity plays a positive role as a modifiable factor in preventing CVD. A previous study has shown the benefits of physical activity in middle-aged women, with moderate physical activity being associated with a lower risk of coronary heart disease, venous thromboembolic events, and cerebrovascular disease than inactivity.49 The insignificant association between physical activity and ASCVD in this study may be due to the dichotomous use of “physical activity (yes/no)” as a categorization criterion, a variable provided in the KNHANES raw data user guideline. Therefore, future studies should further examine cardiovascular risk in middle-aged postmenopausal women by subdividing physical activity into light, moderate, and vigorous intensity categories, for example.
This study found that breastfeeding for more than 12 months was associated with an increased risk of CVD, somewhat contradicting previous research. Breastfeeding is protective against many maternal cardiovascular risk factors and outcomes, and there is evidence that longer breastfeeding duration may have a protective effect,50–52 but this remains unclear. Some studies found no clear associations between breastfeeding and CVD.53 A recent study on the association between reproductive factors and CVD in postmenopausal women in Korea found that the longer the duration of breastfeeding, the higher the risk of CVD, consistent with our findings.54 These inconsistent findings regarding breastfeeding and cardiovascular risk may be due to differences in the selection of subjects and differences in the duration and intensity of breastfeeding.54–56 Overall, these factors should be considered when conducting future large-scale studies of breastfeeding and CVD in postmenopausal women.
This study evaluated the association between relative grip strength and 10-year ASCVD risk and found that those with higher relative grip strength had a significantly lower risk of ASCVD compared with those with lower relative grip strength. These findings are consistent with a growing body of evidence suggesting that relative grip strength may be an important marker of overall health, including cardiovascular health. Relative grip strength is used as a more objective marker than absolute handgrip strength, as it can reflect both muscle strength and obesity by taking into account body mass index.57 Previous studies have also reported that it provides the most consistent results.15 Laukkanen et al58 found inverse associations between relative grip strength and cardiovascular events and all-cause mortality. A cohort study in Taiwan identified associations between CVD risk factors by distinguishing between relative and dominant grip strength and found that relative grip strength was significantly associated with cardiometabolic disease risk, with a stronger association than dominant grip strength.17 Leong et al21 examined the relationship between relative grip strength and mortality risk according to sex in different populations. They found that the inverse relationship between relative grip strength and mortality was stronger among women than among men, highlighting the potential importance of grip strength in assessing cardiovascular risk in women. A study using the Framingham Risk Score to determine the 10-year risk of CVD among middle-aged women found that increasing relative grip strength was associated with a decreased 10-year risk of cardiovascular events.59
Menopause is an important life stage for women characterized by hormonal changes and changes in cardiovascular risk factors. Additionally, monitoring relative grip strength could be a simple and cost-effective way to identify individuals at higher risk of CVD. Understanding the complex interplay between relative grip strength and cardiovascular health in middle-aged, postmenopausal women has important implications for prevention strategies and personalized healthcare interventions. Incorporating relative grip strength measurement into routine health assessments may help mitigate cardiovascular risk through early detection and tailored interventions. This study emphasized the potential importance of relative grip strength in assessing cardiovascular risk in middle-aged postmenopausal women.
Conclusion
This study found that low relative grip strength was associated with increased CVD risk. Relative grip strength was determined to be an independent predictor of CVD risk in middle-aged, postmenopausal women. Given that postmenopausal women are a high-risk group for CVD and experience progressive muscle weakness, relative grip strength has potential value as a simple, useful, and accessible screening tool for community CVD risk prevention and health promotion. These findings provide a rationale for designing and expanding future intervention programs aimed at promoting health behaviors to prevent CVD in middle-aged, postmenopausal women.
Ethics Approval and Informed Consent
The study design was approved and exempted by the Institutional Review Board of Konyang University (KYU IRB-2023-10-011). This study was analyzed using data from KNHANES, an annual survey conducted by the Korean Ministry of Health and Welfare. This survey was approved by the Institutional Review Board of the Korea Health and Nutrition Service, the KCDC discloses only de-identified data on its website so that individuals cannot be extrapolated from the survey data in accordance with the Personal Information Protection Act and the Statistics Act. The data accessed for this study was in compliance with applicable data protection and privacy regulations.
Author Contributions
All authors made significant contributions to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis, or interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This paper was supported by the Konyang University Research Fund in 2022 and supported by the National Research Foundation (NRF) funded by the Korean government (No.RS-2023-00213556).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Health topic. Cardiovascular disease. Available from https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).
2. Kim H, Kim S, Han S, et al. Prevalence and incidence of atherosclerotic cardiovascular disease and its risk factors in Korea: a nationwide population-based study. BMC Public Health. 2019;19:1–11. doi:10.1186/s12889-019-7439-0
3. Lee -H-H, Cho SMJ, Lee H, et al. Korea heart disease fact sheet 2020: analysis of nationwide data. Korean Circul J. 2021;51:495. doi:10.4070/kcj.2021.0097
4. Pencina MJ, Navar AM, Wojdyla D, et al. Quantifying importance of major risk factors for coronary heart disease. Circulation. 2019;139:1603–1611. doi:10.1161/CIRCULATIONAHA.117
5. Dahlöf B. Cardiovascular disease risk factors: epidemiology and risk assessment. Am j Cardiol. 2010;105:3A–9A. doi:10.1016/j.amjcard.2009.10.007
6. Lopez-Jaramillo P, Lopez-Lopez JP, Tole MC, Cohen DD. Muscular strength in risk factors for cardiovascular disease and mortality: a narrative review. Anatol J Cardiol. 2022;26:598. doi:10.5152/AnatolJCardiol.2022.1586
7. Delmonico MJ, Harris TB, Visser M, et al. Longitudinal study of muscle strength, quality, and adipose tissue infiltration. Am J Clin Nutr. 2009;90:1579–1585. doi:10.3945/ajcn.2009.28047
8. Morley JE. Anorexia, sarcopenia, and aging. Nutrition. 2001;17:660–663. doi:10.1016/S0899-9007(01)00574-3
9. Rosenberg IH. Sarcopenia: origins and clinical relevance. J Nutr. 1997;127:990S–991S. doi:10.1093/jn/127.5.990S
10. Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019;393:2636–2646. doi:10.1016/S0140-6736(19)31138-9
11. Chen L-K, Woo J, Assantachai P, et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Directors Assoc. 2020;21:300–307. e302. doi:10.1016/j.jamda.2019.12.012
12. Jang S-K, Kim J-H, Lee Y. Effect of relative handgrip strength on cardiovascular disease among Korean adults aged 45 years and older: results from the Korean Longitudinal Study of Aging (2006–2016). Arch Gerontol Geriatrics. 2020;86:103937. doi:10.1016/j.archger.2019.103937
13. Beyer SE, Sanghvi MM, Aung N, et al. Prospective association between handgrip strength and cardiac structure and function in UK adults. PLoS One. 2018;13:e0193124. doi:10.1371/journal.pone.0193124
14. López-Bueno R, Andersen LL, Calatayud J, et al. Longitudinal association of handgrip strength with all-cause and cardiovascular mortality in older adults using a causal framework. Exp Gerontology. 2022:111951. doi:10.1016/j.exger.2022.111951
15. Kim WB, Park J-B, Kim Y-J. Usefulness of relative handgrip strength as a simple indicator of cardiovascular risk in middle-aged Koreans. Am J Med Sci. 2021;362:486–495. doi:10.1016/j.amjms.2021.07.010
16. Lawman HG, Troiano RP, Perna FM, et al. Associations of relative handgrip strength and cardiovascular disease biomarkers in US adults, 2011–2012. Am J Preventive Med. 2016;50:677–683. doi:10.1016/j.amepre.2015.10.022
17. Lee W-J, Peng L-N, Chiou S-T, Chen L-K. Relative handgrip strength is a simple indicator of cardiometabolic risk among middle-aged and older people: a nationwide population-based study in Taiwan. PLoS One. 2016;11:e0160876. doi:10.1371/journal.pone.0160876
18. Gao Y, Huang H, Ni C, et al. Comparison of five expressions of handgrip strength for predicting cardiovascular disease risk factors in Chinese middle-aged community residents. Front Public Health. 2022;10:903036. doi:10.1371/journal.pone.0160876
19. Sayer AA, Syddall H, Dennison E, et al. Grip strength and the metabolic syndrome: findings from the Hertfordshire Cohort Study. QJM. 2007;100:707–713. doi:10.1093/qjmed/hcm095
20. Carbone S, Kirkman DL, Garten RS, et al. Muscular strength and cardiovascular disease: an updated state-of-The-art narrative review. J Cardiopulm Rehabil Prevent. 2020;40:302–309. doi:10.1097/HCR.0000000000000525
21. Leong D, Teo K, Rangarajan S, et al. Prognostic value of grip strength: findings from the prospective urban rural epidemiology (PURE) study. Lancet. 2015;386:266–273. doi:10.1016/S0140-6736(14)62000-6
22. Cooper R, Hardy R, Aihie Sayer A, et al. Age and gender differences in physical capability levels from mid-life onwards: the harmonisation and meta-analysis of data from eight UK cohort studies. PLoS One. 2011;6:e27899. doi:10.1371/journal.pone.0027899
23. Nevill AM, Holder RL. Modelling handgrip strength in the presence of confounding variables: results from the Allied Dunbar National Fitness Survey. In: Advances in Sport. Leisure and Ergonomics: Routledge; 2003:291–302.
24. Roos MR, Rice CL, Vandervoort AA. Age‐related changes in motor unit function. Muscle and Nerve. 1997;20:679–690. doi:10.1002/(SICI)1097-4598(199706)20:6<679::AID-MUS4>3.0.CO;2-5
25. Park HM. Current status of sarcopenia in Korea: a focus on Korean geripausal women. Ann Geriatr Med Res. 2018;22:52. doi:10.4235/agmr.2018.22.2.52
26. Lexell J, Taylor CC, Sjöström M. What is the cause of the ageing atrophy?: total number, size and proportion of different fiber types studied in whole vastus lateralis muscle from 15-to 83-year-old men. J Neurol Sci. 1988;84:275–294. doi:10.1016/0022-510X(88)90132-3
27. Rogers MA, Evans WJ. Changes in skeletal muscle with aging: effects of exercise training. Exer Sport Sci Rev. 1993;21:65–102.
28. Roubenoff R, Hughes VA. Sarcopenia: current concepts. J Gerontol Ser A. 2000;55:M716–M724. doi:10.1093/gerona/55.12.M716
29. Keller K, Engelhardt M. Strength and muscle mass loss with aging process. Age and strength loss. Muscle Ligament Tend J. 2013;3:346.
30. Maltais M, Desroches J, Dionne IJ. Changes in muscle mass and strength after menopause. J Musculoskelet Neuronal Interact. 2009;9:186–197.
31. Messier V, Rabasa-Lhoret R, Barbat-Artigas S, et al. Menopause and sarcopenia: a potential role for sex hormones. Maturitas. 2011;68:331–336. doi:10.1016/j.maturitas.2011.01.014
32. Orprayoon N, Wainipitapong P, Champaiboon J, et al. Prevalence of pre-sarcopenia among postmenopausal women younger than 65 years. Menopause. 2021;28:1351–1357. doi:10.1097/GME.0000000000001866
33. Manrique-Acevedo C, Chinnakotla B, Padilla J, Martinez-Lemus LA, Gozal D. Obesity and cardiovascular disease in women. Int J Obesity. 2020;44:1210–1226. doi:10.1038/s41366-020-0548-0
34. Tiwari S, Gupta V, Paul BN, et al. IL-6 gene expression in adipose tissue of postmenopausal women and its association with metabolic risk factors. Mole Cell Endocrinol. 2015;399:87–94. doi:10.1016/j.mce.2014.08.008
35. Wild RA, Hovey KM, Andrews C, et al. Cardiovascular disease (CVD) risk scores, age, or years since menopause to predict cardiovascular disease in the Women’s Health Initiative. Menopause. 2021;28:610–618. doi:10.1097/GME.0000000000001753
36. Zhu D, Chung H-F, Dobson AJ, et al. Age at natural menopause and risk of incident cardiovascular disease: a pooled analysis of individual patient data. Lancet Public Health. 2019;4:e553–e564. doi:10.1016/S2468-2667(19)30155-0
37. Davis M, Andrade J, Taylor C, Ignaszewski A. Cardiovascular risk factors and models of risk prediction: recognizing the leadership of Dr Roy Dawber. BCMJ. 2010;52:342–348.
38. Lee K. Mediation of grip strength on the association between self-rated health and estimated cardiovascular disease risk. Metabol Synd Relat Disorders. 2022;20:344–350. doi:10.1089/met.2022.0003
39. Bohannon RW. Grip strength: an indispensable biomarker for older adults. Clin IntervenT Aging. 2019;1681–1691. doi:10.2147/CIA.S194543
40. Korea Disease Control and Prevention Agency. Guidebook for data users of Korea National Health & Nutrition Examination Survey, 7th wave(2016–2018). National statistics No.117002. Korea Disease Control and Prevention Agency; 2021.
41. Lindley KJ, Aggarwal NR, Briller JE, et al. Socioeconomic determinants of health and cardiovascular outcomes in women: JACC review topic of the week. J Am Coll Cardiol. 2021;78:1919–1929. doi:10.1016/j.jacc.2021.09.011
42. Timmis A, Vardas P, Townsend N, et al. European Society of Cardiology: cardiovascular disease statistics 2021. Eur Heart J. 2022;43:716–799. doi:10.1093/eurheartj/ehab892
43. Shaw LJ, Bairey Merz CN, Bittner V, et al. Importance of socioeconomic status as a predictor of cardiovascular outcome and costs of care in women with suspected myocardial ischemia. Results from the National Institutes of Health, National Heart, Lung and Blood Institute-sponsored Women’s Ischemia Syndrome Evaluation (WISE). J Women’s Health. 2008;17:1081–1092. doi:10.1089/jwh.2007.0596
44. Gebreab SY, Diez Roux AV, Brenner AB, et al. The impact of lifecourse socioeconomic position on cardiovascular disease events in African Americans: the Jackson Heart Study. J Am Heart Assoc. 2015;4:e001553. doi:10.1161/JAHA.114.001553
45. Garfield C. Variations in family composition. Develop Behav Paediatr. 2009;2:94–102.
46. Rosengren A, Smyth A, Rangarajan S, et al. Socioeconomic status and risk of cardiovascular disease in 20 low-income, middle-income, and high-income countries: the Prospective Urban Rural Epidemiologic (PURE) study. Lancet Glob Health. 2019;7:e748–e760. doi:10.1016/S2214-109X(19)30045-2
47. Kim YJ, Lee JS, Park J, et al. Trends in socioeconomic inequalities in five major risk factors for cardiovascular disease in the Korean population: a cross-sectional study using data from the Korea National Health and Nutrition Examination Survey, 2001–2014. BMJ open. 2017;7:
48. Shakoor H, Platat C, Ali HI, et al. The benefits of physical activity in middle-aged individuals for cardiovascular disease outcomes. Maturitas. 2023;168:49–52. doi:10.1016/j.maturitas.2022.11.002
49. Armstrong ME, Green J, Reeves GK, Beral V, Cairns BJ. Frequent physical activity may not reduce vascular disease risk as much as moderate activity: large prospective study of women in the United Kingdom. Circulation. 2015;131:721–729. doi:10.1161/CIRCULATIONAHA.114.010296
50. Nguyen B, Jin K, Ding D. Breastfeeding and maternal cardiovascular risk factors and outcomes: a systematic review. PLoS One. 2017;12:e0187923. doi:10.1371/journal.pone.0187923
51. Peters SA, Yang L, Guo Y, et al. Breastfeeding and the risk of maternal cardiovascular disease: a prospective study of 300 000 Chinese women. J Am Heart Assoc. 2017;6:e006081. doi:10.1161/JAHA.117.006081
52. Schwarz EB, Ray RM, Stuebe AM, et al. Duration of lactation and risk factors for maternal cardiovascular disease. Obstetrics Gynecol. 2009;113:974. doi:10.1097/01.AOG.0000346884.67796.ca
53. Gallagher LG, Davis LB, Ray RM, et al. Reproductive history and mortality from cardiovascular disease among women textile workers in Shanghai, China. Int J Epidemiol. 2011;40:1510–1518. doi:10.1093/ije/dyr134
54. Kang J, Kim J, Yu N, Kang H. Association between reproductive factors and cardiovascular disease risk in post-menopausal women: cross-sectional study from the 2016–2017 Korea National Health and Nutrition Examination Survey. Korean J Fam Pract. 2020;10:182–191. doi:10.21215/kjfp.2020.10.3.182
55. Oken E, Patel R, Guthrie LB, et al. Effects of an intervention to promote breastfeeding on maternal adiposity and blood pressure at 11.5 y postpartum: results from the Promotion of Breastfeeding Intervention Trial, a cluster-randomized controlled trial. Am J Clin Nutri. 2013;98:1048–1056. doi:10.3945/ajcn.113.065300
56. Stuebe AM, Schwarz EB, Grewen K, et al. Duration of lactation and incidence of maternal hypertension: a longitudinal cohort study. Am J Epidemiol. 2011;174:1147–1158. doi:10.1093/aje/kwr227
57. Choquette S, Bouchard D, Doyon C, et al. Relative strength as a determinant of mobility in elders 67–84 years of age. a nuage study: nutrition as a determinant of successful aging. J Nutr Health Aging. 2010;14:190–195. doi:10.1007/s12603-010-0047-4
58. Laukkanen JA, Voutilainen A, Kurl S, et al. Handgrip strength is inversely associated with fatal cardiovascular and all-cause mortality events. Ann Med. 2020;52:109–119. doi:10.1080/07853890.2020.1748220
59. Shim J, Yoo HJ. Effects of handgrip strength on 10-year cardiovascular risk among the Korean middle-aged population: the Korea National Health and Nutrition Examination Survey 2014. Healthcare. 2020;8:458. doi:10.3390/healthcare8040458
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.