Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Association of Glycated Hemoglobin Level with Self-Reported Chewing Problems in Elderly Community-Dwelling Individuals in Japan
Authors Fujishiro M ![]() , Tanaka S
, Tanaka S ![]() , Watanabe K, Imatake K, Suzuki Y, Ishihara H
, Watanabe K, Imatake K, Suzuki Y, Ishihara H ![]() , Tani S
, Tani S ![]()
Received 8 January 2023
Accepted for publication 18 April 2023
Published 2 May 2023 Volume 2023:16 Pages 1231—1238
DOI https://doi.org/10.2147/JMDH.S404028
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Midori Fujishiro,1,2 Sho Tanaka,1,3 Kentaro Watanabe,1 Kazuhiro Imatake,4 Yasuyuki Suzuki,4– 6 Hisamitsu Ishihara,1 Shigemasa Tani4– 6
1Division of Diabetes and Metabolic Diseases, Department of Internal Medicine, Nihon University School of Medicine, Tokyo, Japan; 2Department of Internal Medicine, Nihon University Hospital, Tokyo, Japan; 3Amemiya Internal Medicine Clinic, Kanagawa, Japan; 4Department of Health Planning Center, Nihon University Hospital, Tokyo, Japan; 5Department of Cardiology, Nihon University Hospital, Tokyo, Japan; 6Division of Cardiology, Department of Medicine, Nihon University School of Medicine, Tokyo, Japan
Correspondence: Sho Tanaka, Division of Diabetes and Metabolic Diseases, Department of Internal Medicine, Nihon University School of Medicine, 30-1 Oyaguchi Kami-cho, Itabashi-ku, Tokyo, 173-8610, Japan, Tel +81-3-3972-8111, Fax +81-3-3959-9775, Email [email protected]
Purpose: Chewing problems are associated with increased mortality, geriatric syndromes and poor activities of daily living. Starting in 2018, in Japan, a self-reported questionnaire investigating chewing status was implemented in the annual health checkup program. Considering the bidirectional association between hyperglycemia and poor oral health, it is hypothesized that people with self-reported chewing problems will have relatively poor glycemic profiles. We investigated the metabolic characteristics of elderly community dwellers with self-reported chewing problems, as well as the association between the problems and HbA1c levels.
Patients and Methods: This was a retrospective, cross-sectional study. We reviewed the data of 1018 adults ≥ 65 years of age who had undergone an annual health checkup at Nihon University Hospital during the period from January 2019 through December 2019. The presence of chewing problems was investigated using a self-reported questionnaire constructed based on guidance provided by the Japanese government.
Results: In the 1018 participants, the overall prevalence of chewing problems was 10.4%. Participants with chewing problems showed significantly higher levels and worse categories of HbA1c than those without such problems (HbA1c < 6.0%, 42.5% vs 54.8%; HbA1c 6.0– 6.9%, 41.5% vs 37.0%; HbA1c ≥ 7.0%, 16.0% vs 8.2%, p = 0.008). Participants with HbA1c ≥ 7.0% have a significantly increased risk of chewing problems as compared to those with HbA1c < 6.0% (odds ratio 2.76, p = 0.002), even after adjusting for the effects of age, sex, body mass index, eating behaviors, and history of diabetes mellitus.
Conclusion: HbA1c ≥ 7.0% is associated with self-reported chewing problems in elderly Japanese community-dwellers. We thus recommend a proactive assessment of oral conditions for this population.
Keywords: chewing, community dwellers, diabetes mellitus, elderly, glycated hemoglobin
Introduction
Oral health is known to be associated with systemic health. Previous studies demonstrated close relationships between poor oral health and increased mortality, cardiovascular disease, respiratory disease, and metabolic disorders including diabetes mellitus (DM).1–5 In elderly individuals, mastication plays an important role in health maintenance, because masticatory dysfunction is linked not only to the mortality rate, but also to geriatric syndromes such as sarcopenia, cognitive decline, osteoporosis, undernutrition, and impaired activities of daily living.6–11 Additionally, masticatory dysfunction is closely associated with impaired subjective quality of mastication performance.12
Aging is an important risk factor for insulin resistance and beta-cell dysfunction, both of which lead to hyperglycemia. Japan is now confronted with a super-aged society, and the number of patients with DM living in Japan has been steadily growing due to rapid population aging.13 Hyperglycemia interacts with poor oral health, and previous studies found that a poor glycemic profile increases the incidences of periodontitis and tooth loss.5,14–16 Considering the negative consequences of poor oral health and the growth of the elderly population, the impact of hyperglycemia on the oral conditions of older individuals is an important health issue in Japan.
Formerly, oral health screening for adults was not performed universally in Japan. However, starting in 2018, a self-reported questionnaire investigating chewing status was included in the annual health checkup program in accordance with guidance provided by the Ministry of Health, Labor and Welfare, Japan. In another country, a recent study confirmed self-reported chewing status to correlate with oral health condition in the elderly population.17 While evaluation and detection of chewing problems by an oral health care provider is considered to be the best approach in individualized practice, it requires significant human and equipment resources to examine large populations, such that surveillance using a questionnaire has advantages in terms of time and costs in universal screening. Accumulating information about the population with chewing problems identified by this system is important for enhancing collaboration between the medical and dental fields and providing appropriate guidance for people participating in the health checkup program. However, little is known about the clinical characteristics of the Japanese population with self-reported chewing problems.
Since there is a close association between hyperglycemia and poor oral health, we hypothesized that elderly individuals with chewing problems identified by a self-reported questionnaire have poorer glycemic profiles than those without such problems. We aimed to investigate the metabolic characteristics of the elderly Japanese population with self-reported chewing problems, as well as the association between these problems and HbA1c levels.
Materials and Methods
Study Design and Settings
This was a retrospective, cross-sectional study. Participants who had undergone an annual health checkup between January 2019 and December 2019 at Nihon University Hospital were potentially eligible. The exclusion criteria were as follows: age < 65 years; incomplete responses to the self-reported questionnaire; missing data for plasma glucose (PG) or HbA1c. After applying these exclusion criteria, participants were classified into two groups according to the presence or absence of a chewing problem using a paper-based self-reported questionnaire, as shown in Supplementary Table 1.
In this study, statistical sample size calculation was not performed because prior research on this topic is scarce and the effect size remains unknown. We determined the participant selection procedure prior to initiating the study and this was not changed during the study course.
Studied Parameters
Age, sex, height, and weight were recorded. Body mass index (BMI) was determined by dividing the body weight by the height squared (kg/m2). Blood pressure was measured twice in the sitting position, and an average value was used. Using the aforementioned paper-based self-reported questionnaires, eating behaviors were surveyed because chewing and eating are connected. Similarly, smoking status was investigated, because smoking exerts an adverse influence on oral health.18 Prior diagnoses and medication use were also collected. In this study, participants with a history of DM or anti-diabetic agent use were considered to have DM; Participants with a history of hypertension or anti-hypertensive agent use were considered to have hypertension; Participants with a history of dyslipidemia, or taking an anti-dyslipidemic agent, were considered to have dyslipidemia.
Venous blood samples were collected early in the morning after an overnight fast, and immediately examined. Whole blood was used for measuring HbA1c. Glucose concentrations were determined using blood plasma. High-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglyceride (TG) concentrations were measured using blood serum. HbA1c levels were classified into 3 categories as follows; Good, HbA1c < 6.0; Fair, HbA1c 6.0–6.9%; Poor, HbA1c ≥ 7.0%, according to the latest Japanese clinical practice guideline.19
Statistical Analysis
First, we compared metabolic characteristics and lifestyle behaviors between participants with and those without chewing problems. Continuous variables following a normal distribution were reported as means ± standard deviations and the two groups were compared using Student’s t-test. Continuous variables with skewed distributions were reported as medians with interquartile ranges and compared using the Mann–Whitney U-test. Categorical variables were examined using the chi-squared test.
Next, we carried out binary logistic regression analyses to determine the association between the HbA1c level and chewing problems. Eating behaviors collected using a self-reported questionnaire were also included in the analyses, adjusting for possible confounding effects. Eating behaviors influence oral health. The number of remaining teeth can also affect dietary patterns in older individuals.20 Furthermore, the association between eating behaviors and poor glycemic profile was previously reported.21 Therefore, the association between having a chewing problem and HbA1c categories was examined with adjustment for age (per year), sex (0, female; 1, male), BMI (per kg/m2), smoking (0, no; 1, yes), eating fast (0, no; 1, yes), eating dinner late (0, no; 1, yes), snack/sweet beverage consumption (0, no; 1, yes), skipping breakfast (0, no; 1, yes), and DM history (0, no; 1, yes).
For all statistical analyses, we used EZR version 1.54 (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R version 4.04 (The R Foundation for Statistical Computing, Vienna, Austria). Throughout, a p-value < 0.05 was considered to indicate a statistically significant association.
Results
Prevalence of Chewing Problems
Figure 1 shows the participant selection procedure. In total, 11,633 participants underwent health checkups during the study period, and 10,615 were excluded based on age. After application of the exclusion criteria, 1018 elderly participants were enrolled. Of these, 10.4% (106 of the 1018 participants) reported a chewing problem, while the others did not.
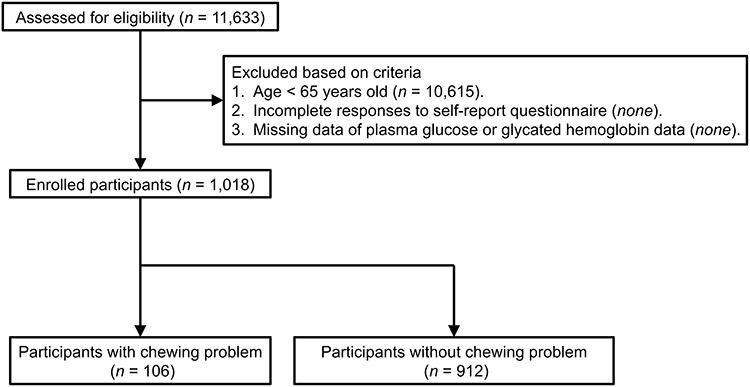 |
Figure 1 Participant selection procedure. |
Comparisons of Participant Characteristics
Comparisons of background and metabolic characteristics between subjects with and without chewing problems are shown in Table 1. There was no significant difference in age, sex, or BMI between the two groups. History of hypertension and dyslipidemia, blood pressure, and lipid panels did not differ between the two groups. Participants with chewing problems had significantly higher HbA1c levels and were more frequently classified into worse HbA1c categories (HbA1c < 6.0%, 42.5% vs 54.8%; HbA1c 6.0–6.9%, 41.5% vs 37.0%; HbA1c ≥ 7.0%, 16.0% vs 8.2%, p = 0.008), in comparison to those without chewing problems. PG tended to be higher in participants with chewing problems, but the difference did not reach statistical significance.
 |
Table 1 Comparisons of Metabolic Characteristics Between Participants with and without Chewing Problems |
Table 2 shows comparisons of lifestyle behaviors. Participants with were more likely than those without chewing problems to be smokers (23.6% vs 13.8%, p = 0.011). Fast eating tended to be less common (30.2% vs 39.7%, p = 0.072) while having dinner late in the evening tended to be more common (43.4% vs 33.3%, p = 0.050) in participants with than in those without chewing problems, although these differences did not reach statistical significance.
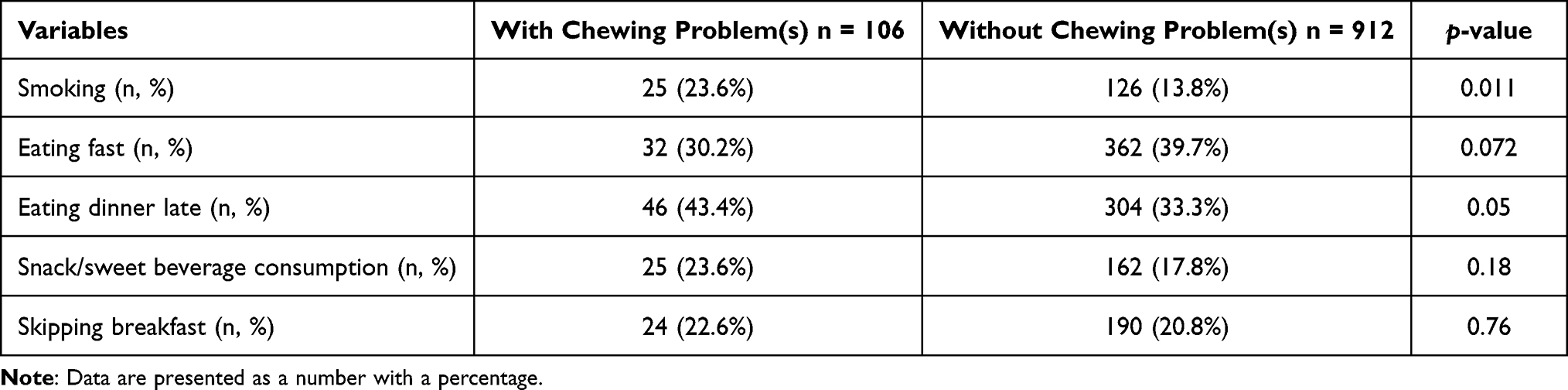 |
Table 2 Comparisons of Lifestyle Behaviors Between Participants with and without Chewing Problem(s) |
Comparisons of Participant Characteristics
Figure 2 summarizes the results of binary logistic regression analysis using the chewing problem as the dependent variable. In our multivariate model, we found a high HbA1c level (≥ 7%) to be significantly associated with an increased risk of chewing problems (odds ratio [OR] 2.76, 95% confidence interval [CI] 1.46–5.24, p = 0.002), and even moderately elevated HbA1c (6.0–6.9%) tended to be related to an increased risk though the association failed to reach statistical significance. Additionally, we found significant associations of smoking status (OR 1.55, 95% CI 1.02–2.01, p < 0.001), eating fast (OR 0.59, 95% CI 0.38–0.92, p = 0.021) and eating dinner late (OR 1.57, 95% CI 1.02–2.42, p = 0.041) with self-reported chewing problems.
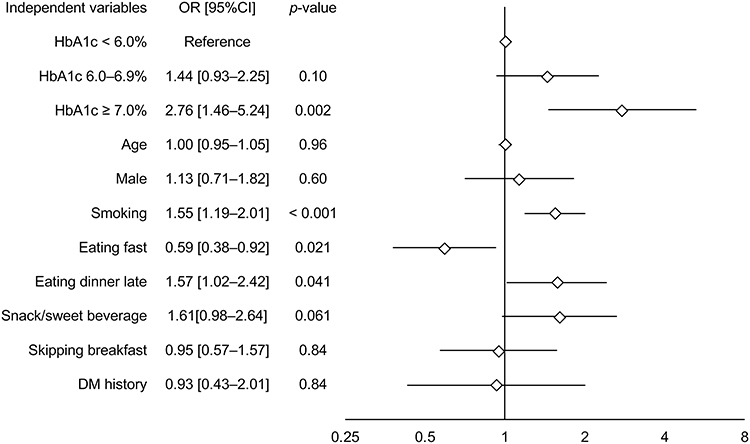 |
Figure 2 Multivariate logistic regression analysis. Adjusted OR (blank square) with 95% CI (horizontal bar) in the multivariate model is presented. Notes: CI, Confidence interval; DM, Diabetes mellitus; HbA1c, Glycated hemoglobin; OR, Odds ratio. |
Discussion
We conducted this cross-sectional study to investigate the metabolic characteristics of the elderly Japanese population with self-reported chewing problems identified by the newly implemented health checkup system, and to identify the associations between these problems and HbA1c levels. We found that 10.4% of the elderly population receiving an annual health checkup reported chewing problems, and individuals with chewing problems showed slightly, but with statistical significance, higher HbA1c levels than those without such problems. Additionally, we confirmed HbA1c ≥ 7.0% to be significantly associated with an increased risk of self-reported chewing problems even after adjustment for the effects of lifestyle behaviors and DM history.
The relationship between DM and poor oral health appeared to be bidirectional in previous studies.5,14–16 Although the underlying mechanism serving as the link between these two features is not fully understood, several pathologies are possible. In DM patients, increased salivary glucose and immunosuppression facilitate bacterial growth which in turn leads to the development of dental caries, and small-vessel damage delays tissue healing in the oral cavity.22 Additionally, RANKL and local inflammatory cytokines are increased, leading to excessive osteoclast activation, and these result in impairment of new bone formation in the periodontium.22 Conversely, infected periodontium can become a source of systemic inflammatory cytokines involving insulin resistance and pancreatic beta-cell impairment.22
Despite this close bidirectional relationship, few studies have focused on the association of self-reported oral health with the glycemic profile. In the Canadian population, adults ≥ 40 years of age with DM who reported having poor or fair oral health had an increased incidence of DM complications as compared to those who described their oral health as being good, very good, or excellent.23 Additionally, histories of DM and smoking habits are reportedly associated with poor self-reported oral status in Qatari adults 18–64 years of age.24 Although evidence confirming these observations is as yet limited, our study results support the speculation that the glycemic profile is associated with self-rated oral conditions.
Since this study was cross-sectional, the etiology of the relationship between chewing problems and the glycemic profile remains unclear. However, previous studies have demonstrated possible underlying mechanisms. First, altered postprandial hormone secretions in response to thorough mastication have been recognized. In healthy Japanese adult males, an increasing number of chews surrounding white rice consumption was reported to enhance the early-phase insulin response, which in turn decreased the postprandial glucose concentration.25 It was also reported that an increasing number of chews before swallowing reduced postprandial ghrelin levels and energy intake, and increased postprandial glucagon-like peptide-1 levels in healthy Chinese young-adult males.26 Therefore, thorough mastication depending on healthy chewing status may improve the glycemic profile. The second possible reason involves impaired oral health arising as a result of high glucose status. A previous meta-analysis of prospective longitudinal studies showed DM to increase the risk of periodontitis progression.14 The incidence of tooth loss was also reported to be higher in DM patients than in those without DM.15 Furthermore, a longitudinal study showed that the risk of caries progression accelerates in proportion to the HbA1c level, and that the rate of missing tooth surface increased faster in individuals with DM, even when they achieved HbA1c ≤ 7.0%, than in those without DM.27 A worsening glycemic profile contributes to deterioration of oral health, thereby possibly resulting in a higher frequency of complaints of chewing problems.
In the present study, we also found behaviors such as smoking, eating fast, and having dinner late in the evening to be associated with the self-reported chewing problems. An increased risk of such problems due to habitual smoking, also shown in this study, is apparently consistent with previous evidence demonstrating that smoking impairs oral health and increases the risks of periodontal disease, dental caries, tooth loss, oral cancer, and leukoplakia.18 The reduced risk of chewing problems in individuals with the fast-eating behavior was thought to reflect reverse causation; that is, people who have chewing problems cannot chew foods smoothly, hence needing longer times to consume a meal than those without such problems. Based on previous studies, the habit of eating dinner late is also assumed to contribute to chewing problems. While saliva exerts a protective effect on teeth and the oral mucosa, thereby preventing physical and chemical damage, the salivary flow rate shows circadian oscillation and is substantially decreased at night.28 Since salivary flow rate reduction results in susceptibility to dental caries due to prolonged retention of sugar in the mouth, habitually eating dinner late is potentially harmful to oral health. Indeed, awakening at midnight to eat was reported to be associated with an increased incidence of tooth loss in Danish adults.29 Another prior study revealed an association between late dinner time and an increased number of dental caries in Japanese children.30 These observations indicate that the habit of eating dinner late has a harmful influence on oral health and may contribute to the presence of chewing problems at advanced ages.
This cross-sectional study showed that elderly Japanese community dwellers with chewing problems identified employing a self-reported questionnaire, incorporated into the health checkup system, had poorer glycemic profiles than those without such problems. However, the present study has limitations because of the design used. First, while dental treatment history and denture use can affect chewing status, information relevant to these items was not available because they were not included in the annual health checkup system. Second, this study recruited only participants who had undergone an annual health checkup at Nihon University Hospital located at Chiyoda-ku, Tokyo, which is the most urbanized area in Japan. Since there are regional differences in dental care in Japan, the generalizability of our study results must be validated in other regions.31 Third, the study results suggested a dose-dependent association between HbA1c and self-reported chewing problems, but the increased risk in individuals with HbA1c levels of 6.0–6.9% failed to reach statistical significance, showing only a trend, possibly due to the relatively small sample size. Finally, objective oral health assessments were not performed in this study. Although the subjective quality of mastication performance was reported to reflect objective mastication function, the diagnostic accuracy of the self-reported questionnaire used in Japan to assess functional chewing problems needs to be validated.12 Future prospective longitudinal studies must be designed to address these limitations and clarify the causal relationship between the glycemic profile and chewing problems.
Conclusion
The present study confirms the association between HbA1c ≥ 7.0% and self-reported chewing problems in elderly Japanese community-dwellers. Elderly patients with HbA1c ≥ 7.0% are frequently encountered in clinical settings. Physicians should consider underlying chewing problems and perform a proactive assessment of oral conditions in this population.
Abbreviations
BMI, Body mass index; CI, Confidence interval; DM, Diabetes mellitus; HbA1c, Glycated hemoglobin; HDL-C, High-density lipoprotein cholesterol; LDL-C, Low-density lipoprotein cholesterol; OR, Odds ratio; PG, Plasma glucose; TG, Triglyceride.
Ethics Approval and Informed Consent
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Nihon University Hospital (No. 211001, approved on October 26th, 2021). The requirement for written informed consent was waived because this was a retrospective observational study, and an opt-out recruitment procedure was followed.
Author Contributions
All authors made a significant contribution to the work reported, in the conception, study design, execution, acquisition of data, analysis and/or interpretation; all took part in drafting, revising and/or critically reviewing the article; all gave final approval of the version to be published; all have agreed on the journal to which the article has been submitted; and all of the authors agree to be accountable for every aspect of the work.
Funding
This research received no external funding.
Disclosure
The authors have no conflicts of interest relevant to this work to disclose.
References
1. Adolph M, Darnaud C, Thomas F, et al. Oral health in relation to all-cause mortality: the IPC cohort study. Sci Rep. 2017;7:44604. doi:10.1038/srep44604
2. Humphrey LL, Fu R, Buckley DI, Freeman M, Helfand M. Periodontal disease and coronary heart disease incidence: a systematic review and meta-analysis. J Gen Intern Med. 2008;23(12):2079–2086. doi:10.1007/s11606-008-0787-6
3. Gomes-Filho IS, Cruz SSD, Trindade SC, et al. Periodontitis and respiratory diseases: a systematic review with meta-analysis. Oral Dis. 2020;26(2):439–446. doi:10.1111/odi.13228
4. Santoso CMA, Ketti F, Bramantoro T, Zsuga J, Nagy A. Association between oral hygiene and metabolic syndrome: a systematic review and meta-analysis. J Clin Med. 2021;10(13):2873. doi:10.3390/jcm10132873
5. Stöhr J, Barbaresko J, Neuenschwander M, Schlesinger S. Bidirectional association between periodontal disease and diabetes mellitus: a systematic review and meta-analysis of cohort studies. Sci Rep. 2021;11(1):13686. doi:10.1038/s41598-021-93062-6
6. Abe T, Tominaga K, Ando Y, et al. Number of teeth and masticatory function are associated with sarcopenia and diabetes mellitus status among community-dwelling older adults: a Shimane CoHRE study. PLoS One. 2021;16(6):e0252625. doi:10.1371/journal.pone.0252625
7. Laudisio A, Gemma A, Fontana DO, et al. Self-reported masticatory dysfunction and mortality in community dwelling elderly adults: a 9-year follow-up. J Am Geriatr Soc. 2016;64(12):2503–2510. doi:10.1111/jgs.14331
8. Krishnamoorthy G, Narayana AI, Balkrishanan D. Mastication as a tool to prevent cognitive dysfunctions. Japanese Dental Sci Rev. 2018;54(4):169–173. doi:10.1016/j.jdsr.2018.06.001
9. Laudisio A, Marzetti E, Antonica L, et al. Masticatory dysfunction is associated with osteoporosis in older men. J Clin Periodontol. 2007;34(11):964–968. doi:10.1111/j.1600-051X.2007.01142.x
10. Motokawa K, Mikami Y, Shirobe M, et al. Relationship between Chewing Ability and Nutritional Status in Japanese Older Adults: a Cross-Sectional Study. Int J Environ Res Public Health. 2021;18:3. doi:10.3390/ijerph18031216
11. Takata Y, Ansai T, Awano S, et al. Activities of daily living and chewing ability in an 80-year-old population. Oral Dis. 2004;10(6):365–368. doi:10.1111/j.1601-0825.2004.01047.x
12. Barbe AG, Javadian S, Rott T, et al. Objective masticatory efficiency and subjective quality of masticatory function among patients with periodontal disease. J Clin Periodontol. 2020;47(11):1344–1353. doi:10.1111/jcpe.13364
13. Goto A, Noda M, Inoue M, Goto M, Hadrien C. Increasing Number of People with Diabetes in Japan: is This Trend Real? Internal Medicine. 2016;55(14):1827–1830. doi:10.2169/internalmedicine.55.6475
14. Nascimento GG, Leite FRM, Vestergaard P, Scheutz F, López R. Does diabetes increase the risk of periodontitis? A systematic review and meta-regression analysis of longitudinal prospective studies. Acta Diabetol. 2018;55(7):653–667. doi:10.1007/s00592-018-1120-4
15. Jimenez M, Hu FB, Marino M, Li Y, Joshipura KJ. Type 2 diabetes mellitus and 20 year incidence of periodontitis and tooth loss. Diabetes Res Clin Pract. 2012;98(3):494–500. doi:10.1016/j.diabres.2012.09.039
16. Morita I, Inagaki K, Nakamura F, et al. Relationship between periodontal status and levels of glycated hemoglobin. J Dent Res. 2012;91(2):161–166. doi:10.1177/0022034511431583
17. Chantaraboot Y, Sermsuti-Anuwat N. Factors Associated with Self-reported Oral Health Among Community-Dwelling Older Adults in a Rural Province of Thailand. J Multidiscip Healthc. 2022;15:2111–2119. doi:10.2147/JMDH.S386993
18. World Health Organization. WHO Monograph on Tobacco Cessation and Oral Health Integration. Geneva: World Health Organization; 2017.
19. Araki E, Goto A, Kondo T, et al. Japanese Clinical Practice Guideline for Diabetes 2019. Diabetol Int. 2020;11(3):165–223. doi:10.1007/s13340-020-00439-5
20. Savoca MR, Arcury TA, Leng X, et al. Severe tooth loss in older adults as a key indicator of compromised dietary quality. Public Health Nutr. 2010;13(4):466–474. doi:10.1017/S1368980009991236
21. Iwasaki T, Hirose A, Azuma T, et al. Association between eating behavior and poor glycemic control in Japanese adults. Sci Rep. 2019;9(1):3418. doi:10.1038/s41598-019-39001-y
22. Ahmad R, Haque M. Oral Health Messiers: diabetes Mellitus Relevance. Diabetes Metab Syndr Obes. 2021;14:3001–3015. doi:10.2147/DMSO.S318972
23. Kaura Parbhakar K, Rosella LC, Singhal S, Quiñonez CR. Risk of complications among diabetics self-reporting oral health status in Canada: a population-based cohort study. PLoS One. 2020;15(1):e0218056. doi:10.1371/journal.pone.0218056
24. Cheema S, Maisonneuve P, Al-Thani MH, et al. Oral health behavior and factors associated with poor oral status in Qatar: results from a national health survey. J Public Health Dent. 2017;77(4):308–316. doi:10.1111/jphd.12209
25. Sato A, Ohtsuka Y, Yamanaka Y. Morning Mastication Enhances Postprandial Glucose Metabolism in Healthy Young Subjects. Tohoku J Exp Med. 2019;249(3):193–201. doi:10.1620/tjem.249.193
26. Li J, Zhang N, Hu L, et al. Improvement in chewing activity reduces energy intake in one meal and modulates plasma gut hormone concentrations in obese and lean young Chinese men. Am J Clin Nutr. 2011;94(3):709–716. doi:10.3945/ajcn.111.015164
27. Schmolinsky J, Kocher T, Rathmann W, Völzke H, Pink C, Holtfreter B. Diabetes status affects long-term changes in coronal caries - The SHIP Study. Sci Rep. 2019;9(1):15685. doi:10.1038/s41598-019-51086-z
28. Dawes C, Pedersen AM, Villa A, et al. The functions of human saliva: a review sponsored by the World Workshop on Oral Medicine VI. Arch Oral Biol. 2015;60(6):863–874. doi:10.1016/j.archoralbio.2015.03.004
29. Lundgren JD, Williams KB, Heitmann BL. Nocturnal eating predicts tooth loss among adults: results from the Danish MONICA study. Eat Behav. 2010;11(3):170–174. doi:10.1016/j.eatbeh.2010.02.003
30. Nishide S, Yoshihara T, Hongou H, Kanehira T, Yawaka Y. Daily life habits associated with eveningness lead to a higher prevalence of dental caries in children. Journal of Dental Sciences. 2019;14(3):302–308. doi:10.1016/j.jds.2019.01.015
31. Taira K, Mori T, Ishimaru M, et al. Regional Inequality in Dental Care Utilization in Japan: an Ecological Study Using the National Database of Health Insurance Claims. Lancet Reg Health West Pac. 2021;12:100170. doi:10.1016/j.lanwpc.2021.100170
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Glycated Hemoglobin Improvement After Medical and Surgical Eye Care in American Veterans Involves Multidisciplinary Care
Santilli CM, Johnson S, Thunstrom CR, Armbrust KR
Clinical Ophthalmology 2023, 17:1675-1682
Published Date: 10 June 2023