")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Association of Exposure to Biomass Fuels with Occurrence of Chronic Obstructive Pulmonary Disease in Rural Western China: A Real-World Nested Case-Control Study
Authors Zhang X, Zhu X, Wang X, Wang L, Sun H, Yuan P, Ji Y
Received 17 April 2023
Accepted for publication 17 September 2023
Published 9 October 2023 Volume 2023:18 Pages 2207—2224
DOI https://doi.org/10.2147/COPD.S417600
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Min Zhang
Xuan Zhang,1 Xia Zhu,2 Xiaoli Wang,3 Liping Wang,4 Hongying Sun,5 Ping Yuan,6 Yulin Ji1
1Department of Respiratory and Critical Care Medicine, Clinical Research Center for Respiratory Disease, West China Hospital, Sichuan University, Chengdu, Sichuan Province, 610041, People’s Republic of China; 2Center of Infectious Disease, West China Hospital, Sichuan University, Chengdu, Sichuan Province, 610041, People’s Republic of China; 3Department of Infectious disease Prevention and Control, Center for Disease Control and Prevention of Fucheng, Mianyang, Sichuan Province, 621000, People’s Republic of China; 4Department of Disease Control, Health Bureau of Jiangyou, Jiangyou, Sichuan Province, 621700, People’s Republic of China; 5Department of Tuberculosis Prevention and Control, Center for Disease Control and Prevention of Mianyang, Mianyang, Sichuan Province, 621000, People’s Republic of China; 6Department of Epidemiology and Statistics, West China School of Public Health, Sichuan University, Chengdu, Sichuan Province, 610041, People’s Republic of China
Correspondence: Yulin Ji, Department of Respiratory and Critical Care Medicine, Clinical Research Center for Respiratory Disease, West China Hospital, Sichuan University, Chengdu, 610041, People’s Republic of China, Tel +86-17761196035, Fax +86-028-85422571, Email [email protected]
Background: This study investigated the potential contribution of biomass fuels exposure to the occurrence of chronic obstructive pulmonary disease (COPD) in rural areas of western China.
Methods: We analyzed data collected between October 2017 and October 2018 from a nested case-control study of individuals at least 40 years old in the general population in Mianyang City, Sichuan Province, China. Demographic information was collected using a custom-designed questionnaire, and lung function was measured using spirometry. We used multivariate logistic regression to explore the possible relationship between biomass fuels exposure and COPD, as well as between other potential risk factors and COPD. Bayes’ theorem was used to estimate weights for different COPD risk factors.
Results: COPD was newly diagnosed in 500 of the 11398 adults surveyed, corresponding to an incidence of 4.39%. Individuals who were exposed to biomass fuels were at a significantly greater risk of developing COPD than those not exposed (OR 2.58, 95% CI 2.23– 3.05). In subgroup analysis, exposure to biomass fuels increased the risk of COPD in men by 1.71 times (95% CI 1.09– 2.68) and in women by 2.88 times (95% CI 2.01– 3.48), in never-smokers by 2.18 times. Bayesian weights for COPD risk factors were highest for poor kitchen ventilation (W=31.13%) and biomass fuels exposure (W=18.08%).
Conclusion: Our data indicate that rural Chinese who are exposed to biomass fuels during cooking or heating are at greater risk of developing COPD. Efforts should be made to strengthen the construction of clean energy infrastructure, so as to reduce the use of biomass fuels and thereby help prevent COPD.
Keywords: chronic obstructive pulmonary disease, biomass fuels, contribution to COPD, incidence, prevention
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic lung disease that limits airflow in the lungs, leading to high mortality and disability.1 The decline in lung function also reduces quality of life, and the chronic nature of the disease places a heavy burden on patients, their families and society.2,3
In China, the incidence of COPD has been steadily increasing as the population ages and environmental pollution worsens, making it a serious public health crisis. The 2018 China Pulmonary Health Study (CPHS) surveyed 50 991 people from 10 provinces and cities, and found that the prevalence of COPD was 8.6% among adults 20–39 years old and 13.7% among adults at least 40 years old.4 A recent World Health Organization (WHO) report identified COPD as the third leading cause of death worldwide, causing 3.23 million deaths in 2019.5 The Chinese Center for Disease Control and Prevention, based on data from 1999 to 2017, COPD is the fourth cause of death in China.6 COPD is now considered a preventable and treatable disease, highlighting the importance of risk factor detection in order to enable early intervention,7 when it is more likely to be effective.8 However, the strongest risk factors for COPD in the rural Chinese population are unknown.
COPD risk factors can be genetic or environmental.5 One potential environmental factor is combustion of biomass fuels, mainly wood, charcoal, crop straw, animal excrement, corn cobs, and leaves,9 which create indoor air pollution. Smoke from biomass fuels has been linked to increased risk of COPD in various populations.10,11 The WHO estimates that around 2.6 billion people cook using polluting open fires or simple stoves fuelled by kerosene, biomass and coal, and close to 4 million people die prematurely from illness attributable to household air pollution from inefficient cooking practices using polluting stoves paired with solid fuels and kerosene each year.12 At the same time, environmental initiatives have led to the construction of large-scale biogas digesters in rural areas of China,13 which have substantially reduced the use of biomass fuels. The use of biomass fuels varies greatly across different regions. Therefore, the current situation of biomass fuels exposure in rural areas of western China is unclear, and a better understanding of the contribution of biomass fuels exposure to COPD in rural residents is urgently needed.
The purpose of this study was to determine the association between biomass fuels exposure and COPD occurrence in rural areas of western China. Our findings may provide a scientific basis for targeted strategies and measures to reduce biomass fuels exposure, especially in remote rural areas of China.
Methods
Study Design and Participants
The baseline survey- The National Science & Technology Pillar Program during the 12th Five-year Plan Period, implemented from June 1, 2013 to March 1, 2014, Chinese participants were recruited from the rural population (n = 48,109,000) of Mianyang, Sichuan Province in China. And the follow-up time ended between October 1, 2017 and October 1, 2018 (the 13th Five-year Plan).
At the baseline survey, we used a multistage, stratified cluster sampling procedure to enroll a nationally representative sample. In stage one, we stratified administrative divisions in Mianyang into two levels based on gross domestic product (GDP) data from the Mianyang Bureau of Statistics. In each of the two levels, we used a random number table to select one administrative division comprising Fucheng District and Jiangyou City. In stage two, we used GDP data to further stratify towns or subdistricts located in Fucheng District and Jiangyou City into two sublevels. From each of these sublevels, we randomly selected one town or subdistrict from Fucheng District (Qingyi and Xinzao) and Jiangyou City (Erlangmiao and Sanhe). In stage three, we selected all villages or residential communities from within Qingyi, Xinzao, Erlangmiao, and Sanhe. In stage four, proportional random sampling was used to select 15% of permanent residents at least 40 years old in each village or residential community for enrollment in the study (Figure 1).
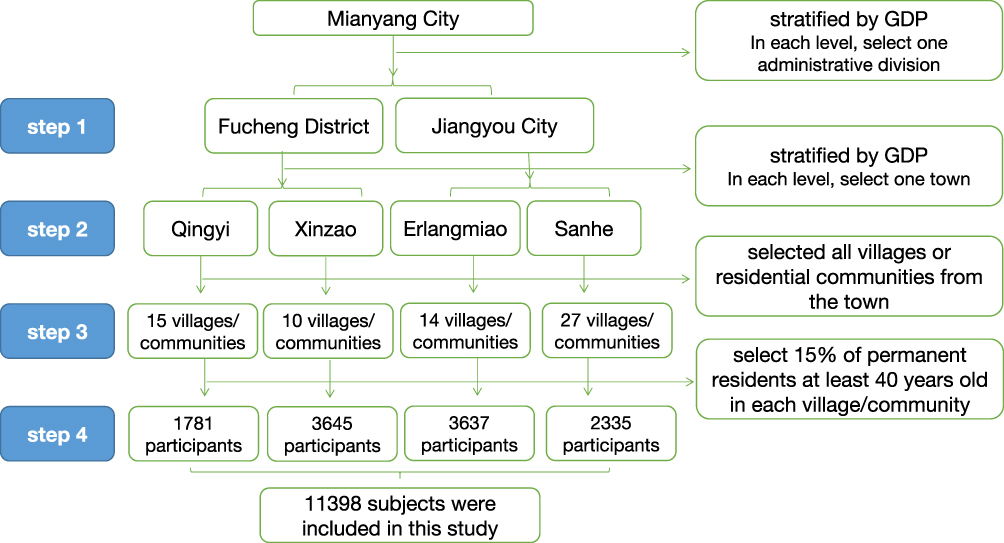 |
Figure 1 The flow chart for sampling strategy. In stage one, we stratified administrative divisions in Mianyang into two levels based on gross domestic product (GDP) data from the Mianyang Bureau of Statistics. In stage two, we used GDP data to further stratify towns or subdistricts located in Fucheng District and Jiangyou City into two sublevels. In stage three, we selected all villages or residential communities. In stage four, proportional random sampling was used to select 15% of permanent residents at least 40 years old in each village or residential community for enrollment in the study. |
For the analyses reported in this article, data were analyzed using a nested case-control study. Participants were included in this study if they satisfied the following criteria: (i) they had been living in the sampled community for more than 6 months by the time of study enrollment; (ii) they had no prior COPD diagnosis, based on registry data or interviews; (iii) they were at least 40 years old; and (iv) they participated in the physical examination of the 12th Five-year Plan (baseline survey in 2014 to 2015). Furthermore, we excluded individuals if they were physically incapable of taking a spirometry test, eg due to thoracic, abdominal, or eye surgery, retinal detachment, or myocardial infarction in the past 3 months; if they had been admitted to hospital for any cardiac condition in the past month; if their heart rate was greater than 120 beats per min; if they were on antibacterial chemotherapy for tuberculosis; or if they were pregnant or breastfeeding. The subjects in this study were recruited by doctors, nurses and village doctors in the local township health center. The principle of convenience sampling was adopted to select subjects meeting the inclusion and exclusion criteria until the expected sample size of the study in the town was reached.
The present study was approved by the Ethics Committee of West China Hospital, Sichuan University (NO.2013–55 and NO.2019–151), and it conformed to the provisions of the Declaration of Helsinki. Each participant signed an informed consent form before enrollment.
Data Collection
Demographics and Clinical Parameters
Research staff received appropriate training and then collected data at examination centers in local health facilities and community clinics in the towns/subdistricts selected for inclusion in the study. The staff conducted standardized face-to-face interviews based on a custom-made questionnaire. The questionnaire collected the following sociodemographic characteristics and clinical information: sex, age, educational level, area of residence, medical history (chronic bronchitis, asthma, COPD, emphysema, tuberculosis), COPD-related symptoms (cough, wheezing, chest tightness, expectoration), and risk factors (smoking history, passive smoking, occupational exposure, childhood history of chronic cough, family history of chronic bronchitis/COPD/emphysema). Physical examination included height, weight, waist circumference, blood pressure, and heart rate. Each questionnaire was assigned a unique identification number.
Spirometry Test
Trained and certified technicians performed pulmonary function tests on all participants using a MasterScreen Pneumo PC spirometer (JAEGER, Wurzburg, Germany). The spirometer was calibrated daily before participants were tested. Participants were required to do up to eight forced expiratory maneuvers until the forced vital capacity (FVC) and forced expiratory volume in 1 s (FEV1) were reproducible within 150 mL.14 Then, 400 μg of the bronchodilator salbutamol (Glaxo Wellcome, Brentford, UK) was administered by inhalation with a 500-mL spacer. After 20 min, spirometry testing was repeated as above. We did all spirometric manoeuvres with the participant in a seated position, wearing a nose clip, and using a disposable mouthpiece. An expert panel performed quality control analysis on the test results based on criteria from the American Thoracic Society and European Respiratory Society. Tests were excluded if they were judged to be of poor quality14.
Data Upload and Storage
Questionnaires were converted into digital data through optical character recognition (OCR) technology (PS306U, Plustek, Taiwan, China). The digitized data and spirometry data were exported and stored securely on a data cloud platform at the College of Computer Science, Sichuan University.
Nested Case-Control Study
Definition of Cases
Cases were defined as patients diagnosed with COPD. COPD was diagnosed according to the 2023 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines15 as a post-bronchodilator FEV1:FVC ratio less than 0.70. We calculated the FEV1:FVC ratio for each participant in this study. Calculated ratios were classified by stages reflecting the predicted degree of breathing obstruction. Stages were determined based on reference FEV1 values from the US general population (n=7429 adults):16 GOLD stage I, ≥ 80% predicted; GOLD stage II, ≥ 50% to < 80% predicted; GOLD stage III, ≥ 30% to < 50% predicted; and GOLD stage IV, < 30% predicted.
Definition of Controls
Controls were defined as individuals who did not occurrence of COPD during follow-up.
Exposure
Exposure to biomass fuels was the exposure of interest. The definition of biomass fuels in this study included crop straw, wood, firewood and animal manure. Subjects were considered to be exposed to biomass fuels if they cooked frequently (>5/week) using biomass fuels (wood/firewood/crop straw or animal dung), regardless of whether biomass fuels were the main cooking fuel. Subjects were considered to be exposed to coal if they cooked frequently using coal, regardless of whether coal was the primary cooking fuel. The rate of biomass exposure was defined as the proportion of subjects who were exposed to biomass fuels.
Outcomes
The primary outcomes of this study was the the occurrence of COPD.
Covariates
Covariates consisted of age, male or female sex, ethnicity, educational level, urbanisation, body mass index (BMI [calculated as weight in kilograms divided by height in meters squared]), smoking history, History of tuberculosis, history of asthma, chronic cough during childhood, family history of chronic bronchitis/COPD/emphysema, house ventilation, dust, exposure to coal, kitchen ventilation, occupational exposure, and exposure to secondhand smoke.
Statistical Analysis
Demographic information included age, sex, and region. Since older adults are more likely to develop COPD, we divided participants into two age groups: 40–59 or ≥ 60 years old. Subjects reporting biomass fuels exposure were compared to those reporting no exposure in terms of sociodemographic and clinical parameters in addition to risk factors, domestic ventilation, cooking with coal, and occupational exposure.
The measurement data such as age and lung function followed a normal distribution and were described by means±standard deviation (SD). Data on demographic characteristics, COPD occurrence, and biomass fuels exposure were reported as frequencies or percentages. We assessed the statistical significance of differences using Student’s t-test and ANOVA for continuous variables, the χ2 test and Fisher’s exact test for categorical variables. The Cochran–Armitage trend test was used to identify the trend across ordered groups such as COPD rates across groups exposed to biomass fuels for different periods of time. Multivariate logistic regression was used to model the influence of biomass fuels exposure on COPD after adjusting for confounding factors. Bayes’ theorem17 was used to weight the relative contributions of various risk factors to the occurrence of COPD.
Data were analyzed using SPSS 20.0 (IBM, Armonk, NY, USA). Differences associated with a P < 0.05 were considered significant.
Results
Characteristics of the Study Participants
Between October 2017 and October 2018, 11421 individuals were invited to participate in this study. Of the11398individuals included in the final analysis, 4848 (42.45%) were male and the mean age was 57.67±9.58 years. Approximately 47.60% of participants were living in Fucheng district, while 52.40% were living in Jiangyou county. The majority of participants were Han Chinese (98.82%). Individuals with GOLD stage III and IV were combined because of the small sample sizes. General characteristics and risk factors of the study population are presented in Table 1.
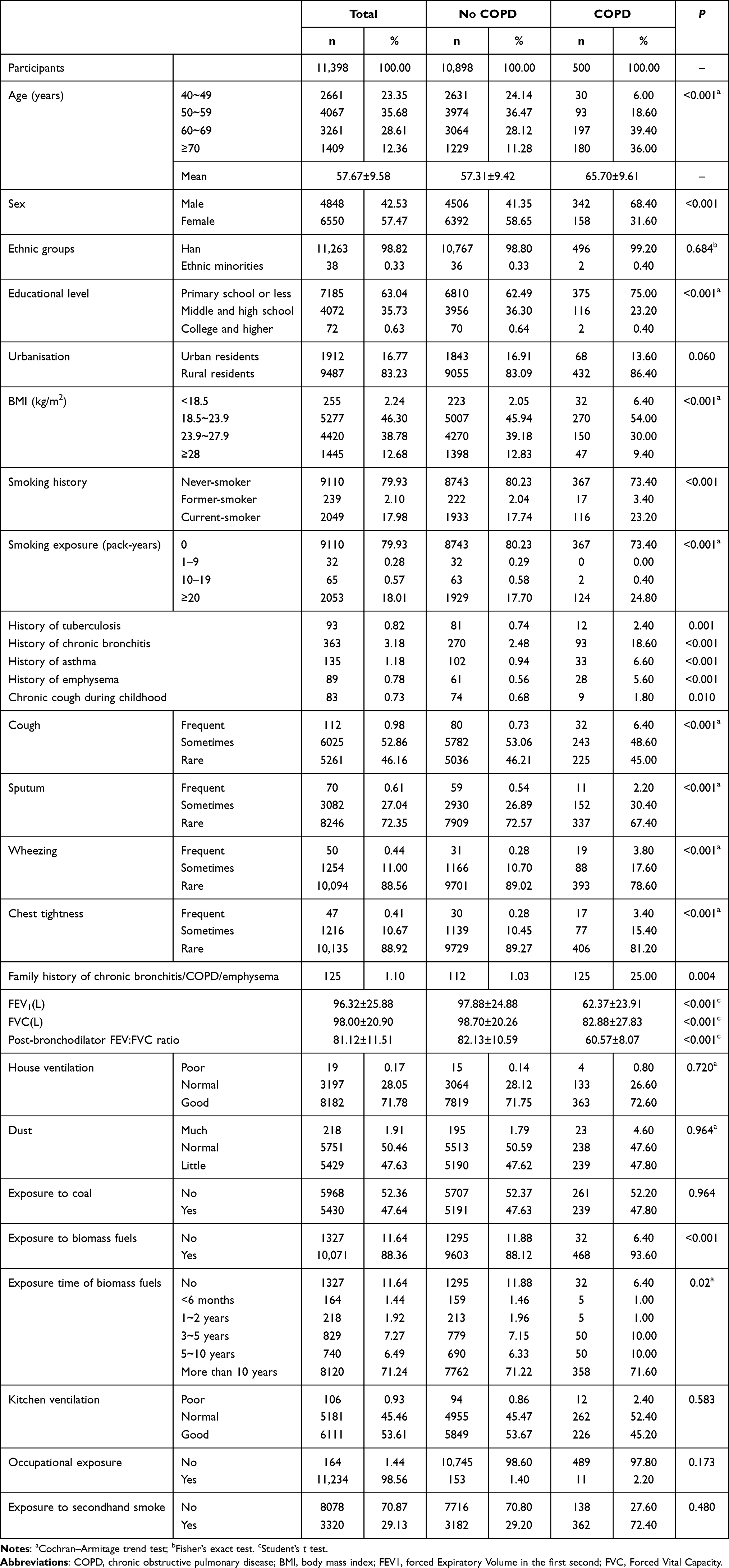 |
Table 1 Demographic Characteristics and Lung Function of the People Over 40 Years Old in Rural Western China |
According to the behavior and living habits reported by participants, most families used firewood/animal excrement for daily cooking (88.35%). Roughly half (52.36%) did not use coal for daily cooking. Most participants believed that their living environment was well ventilated (71.78%), whereas only 0.17% of the subjects considered it to be poor. Most participants believed that their kitchens were well ventilated (53.61%), whereas only 0.93% of the subjects considered the ventilation to be poor. Very few subjects (1.91%) considered their living environment dusty.
Factors Associated with COPD Occurrence
We newly diagnosed 500 participants with COPD according to the 2023 GOLD guidelines, which corresponded to an overall incidence of 4.39%. After standardizing the population composition of different age groups in Mianyang city in 2021, the standardized incidence of COPD increased to 4.51%.
Older age significantly increased likelihood of COPD (P < 0.001), as did being male (7.05% vs 2.41%) and living in a rural area (4.55% vs 3.56%). Conversely, higher levels of education were associated with lower incidence (2.85% vs 5.22%). Incidence was higher among underweight subjects than among those with normal body mass index (BMI) (12.55% vs 5.12%). A history of any of the following health conditions was associated with significantly higher incidence of COPD: tuberculosis (12.90 vs 4.32%), chronic inflammation (25.62% vs 3.67%), asthma (24.44% vs 4.10%), emphysema (31.46% vs 4.15%), chronic cough during adolescence (10.84% vs 4.34%), a family history of chronic bronchitis/COPD/emphysema (10.36% vs 4.36%), or exposure to secondhand smoke (10.90% vs 1.71%). Finally, the incidence of COPD was slightly higher among participants who were exposed to dust through their occupation than among those who were not (6.71% vs 4.35%) (Table 2).
 |
Table 2 Demographics and Risk Factors for Chronic Obstructive Pulmonary Disease Aged 40 years Older, Stratified by Exposure History of Biomass Fuels |
Among the subjects with COPD in this study, The proportion of GOLD stage I, II and III-IV was 25.20%, 40.8% and 34.00%, respectively. Those with GOLD grade III-IV disease had the most obvious clinical symptoms, including frequent cough (8.82%), expectoration (4.71%), wheezing (7.06%), air tightness (6.47%), and dyspnea (52.36%). Prevalence of these symptoms was lower among subjects with GOLD grade IorII. For example, self-reported cough in GOLD gradeIwas 3.97% and 5.88% in GOLD gradeII. As the GOLD grade increased, so did the degree of breathing difficulty (P<0.001), Those patients with GOLD grade III-IV, the mMRC score of dyspnea grade 3 accounted for 51.18% and grade 4 accounted for 1.18%. (Table 3).
 |
Table 3 The Occurrence of COPD in People Over 40 Years Old in Rural Western China, by GOLD Stage |
Associations Between Biomass Fuels Exposure and COPD
A total of 468 (4.65%) were newly diagnosed with COPD in the population exposed to biomass fuels, compared to 32 (2.41%) among those who were not exposed to biomass fuels. There was a significant difference in the incidence of COPD between the two groups (χ2 = 5.487, P < 0.05), and the odds risk (OR) was 1.83 (95% CI 1.19–2.68). Subjects with COPD in the biomass fuels exposure group showed significantly worse lower lung function than those in the non-exposure group in terms of mean FVC (75.81±27.30 vs 84.72±27.59), mean FEV1 (57.47±21.86 vs 63.93±23.79), and FEV1:FVC (57.00±8.01 vs 59.44±7.76) (all P < 0.05). Incidence of COPD increased with longer exposure to biomass fuels (χ2 trend = 9.263, P = 0.02) (Figure 2).
 |
Figure 2 The incidence of COPD at different biomass fuel exposure times. Bars represent the incidence of COPD, and error bars 95% CI. The horizontal axis represents the exposure time of biomass fuels. |
Exposure to biomass fuels was positively associated with COPD (OR= 2.58, 95% CI: 2.23–3.05, P < 0.001) after adjusting for the following potential confounding factors: age, sex, educational level, BMI, smoking, occupational exposure, use of coal in daily cooking, passive smoking, family history of chronic bronchitis/COPD/emphysema, history of tuberculosis, and childhood history of severe cough or asthma (Table 4).
 |
Table 4 Multivariate Analysis for COPD Associated with Biomass Fuels Occurrence in Rural Western Chinese Population Over 40 Years Old |
In subgroup analysis, exposure to biomass fuels increased the risk of COPD in men by 1.71 times (95% CI 1.09–2.68, P<0.001) and in women by 2.88 times (95% CI 2.01–3.48, P<0.001) (Table 5), and in never-smokers by 2.18 times (95% CI: 1.53–3.11, P<0.001) (Table 6).
 |
Table 5 Subgroup Analysis of COPD Occurrence in Rural Western Chinese Population Over 40 Years Old by Sex |
 |
Table 6 Subgroup Analysis of COPD Occurrence in Rural Western Chinese Population Over 40 Years Old by Smoking History |
Weighted Contributions of Risk Factors
Based on Bayes’ theorem, the following factors contributed most to risk of COPD: poor kitchen ventilation (W=31.13%), family history of chronic bronchitis/ emphysema/COPD (W=19.18%), biomass fuels exposure (W=18.08%), age (W=17.04%), sex (W=16.80%), and underweight (W=16.74%) (Table 7).
 |
Table 7 Weight of Risk Factors for COPD Occurrence in Rural Western Chinese Population Over 40 Years Old |
Discussion
This study found that the standardized incidence of COPD was 4.51%. The incidence of COPD varies greatly by country, region, age and sex, epidemiological studies in European, Asian and North American countries have estimated the incidence of COPD in their populations to be 1.40–8.92%.18–22 In recent years, to the best of our knowledge, there were no reports on the incidence of COPD in China. Many cross-sectional surveys have reported the prevalence of COPD in China.4,6,23 The CPH study found that the prevalence of COPD was 8.6% among adults 20–39 years old and 13.7% among adults at least 40 years old 4. It can be seen that COPD has become a major chronic noninfectious disease that seriously affects human health in the 21st century.
This study found evidence that biomass fuels exposure significantly increases risk of COPD, which meant 2.58 times higher risk in our sample, in never-smokers by 2.18 times. This relationship held true even after controlling for numerous potential confounders.
Our results are consistent with previous studies showing that indoor air pollution caused by biomass fuels contributes to respiratory tract infection, COPD, tuberculosis, asthma, cardiovascular disease and other diseases.23–26 An epidemiological investigation of 25 627 residents at least 40 years old in seven provinces or cities in China found that those who used biomass fuels for cooking or heating were at significantly higher risk of COPD than those who did not (OR=1.35, 95% CI: 1.20–1.52), after adjusting for risk factors such as smoking, age, and sex.23 A cross-sectional investigation into COPD prevalence among 50 991 people at least 20 years old in 10 provinces, municipalities or autonomous regions of China also found higher COPD risk among those who used biomass fuels for cooking or heating, after adjusting for several confounding factors (OR=1.25, 95% CI:0.95–1.65, P= 0.10).4 Similarly, meta-analyses have reported that women exposed to biomass fuels are at 2–3 times higher risk of COPD than those not exposed.25,26
This literature and the present study strengthen the association between biomass fuels exposure and development of COPD. We found that biomass fuels exposure and poor kitchen ventilation are among the greatest contributors to COPD in western rural areas. Our Bayesian weighting identified age, sex and family history of chronic bronchitis/COPD/emphysema as unmodifiable COPD risk factors, while biomass fuels exposure and kitchen ventilation emerged as the most important modifiable risk factors for COPD. In terms of the global burden of disease, household use of solid fuels (biomass fuels, coal) ranks 10th among all major risk factors and second among environmental risk factors.27 The WHO lists indoor air pollution caused by biomass fuels exposure as the 10th most important risk factor worldwide, and the fourth greatest preventable contributor to disease burden in developing countries.12 Exposure to biomass fuels and the associated indoor air pollution pose significant problems to public health, particularly in populations still using rudimentary equipment or “dirty energy”. Our data highlight the need for initiatives at local and national levels to improve living conditions in those populations, thereby lowering their COPD risk.
Subgroup analysis showed that biomass fuels exposure was more closely associated with COPD in women (OR 2.88) than in men (OR 1.71). This may be because women are more sensitive to smoke28,29 and/or are more exposed to biomass fuels, especially those living in rural areas, where they often help the mother in the kitchen from an early age. Children exposed to biomass fuels are at greater risk of respiratory tract infection,30,31 which in turn increases their risk of COPD in adulthood.32 Moreover, pregnant women exposed to smoke from biomass fuels tend to give birth to smaller babies33 who are at higher risk of adverse lung development and therefore higher risk of COPD later in life.34,35
In this study, 88.35% of our sample was exposed to biomass fuels. This exposure rate is higher than that in previous studies. One 2018 study36 showed that the rate of biomass fuels exposure from cooking among women at least 40 years old in China was 56.3% in rural areas and 19.9% in urban areas. Exposure rates due to cooking among women in other regions in China have ranged from a low of 27.9% in eastern regions to 45.0% in western regions. A 2014 study inferred from national census data that 59–75% of households in rural areas of China still used biomass fuels as the main cooking fuels.37 The reason why our incidence is higher than in other studies may be that our sample was from rural areas in Sichuan Province, located in the west of China, where people have access to abundant local crop and timber resources for biomass fuels.
Due to the large number of people affected by biomass fuels, sufficient attention should be paid to its impact on COPD burden in the population. The WHO estimates that about 2.6 billion people worldwide use biomass fuels and coal as the main source of energy for cooking, heating and other household needs 12, even more numerous than the 1.1 billion smokers of cigarettes worldwide.38 Polluting fuels such as biomass will continue to be used in China and globally for a long time, especially in rural areas, because they are inexpensive and they support traditional cooking and heating practices. Greater attention should be paid to the impact of biomass fuels on the disease burden in developing countries, particularly among children and women.
The present study had several limitations. First, our data on exposure history, family history were based on self-reporting, creating risk of recall bias. Second, the exposure to biomass fuels has not been quantified accurately, it was divided into 5 groups: “<6 months”, “1~2 years”, “3~5 years”, “5~10 years”, and more than 10 years, it is not possible to pinpoint the specific exposure time of each individual. At the same time, this study did not measure the exposure concentration of biomass fuels. Third, several known risk factors of COPD were not investigated in the present study, such as PM2.5. Fourth, this study was carried out in the rural area of Mianyang city, which is located in Sichuan Province, the west of China. The results of this study may be representative of rural areas in western China, but the incidence of COPD in rural areas across the country needs to be further explored by multi-center, large-sample cohort studies. Finally, similar to other large-scale population-based surveys, the diagnosis of COPD was based only on spirometry tests done in our study. Many participants might have airflow limitation but not clinical COPD.
Conclusion
The data from this study show that COPD is still increasing rapidly in rural areas of western China, and exposed to biomass fuels during cooking or heating are at greater risk of developing COPD. In rural areas where incomes are low and energy sources limited, residents often use inexpensive but easily accessible local materials as the main energy source for daily living. Efforts should be made to strengthen the construction of clean energy infrastructure, so as to reduce the use of biomass fuels and thereby help prevent COPD.
Abbreviations
COPD, chronic obstructive pulmonary disease; OR, odds risk; CI, confidence interval; CPHS, China Pulmonary Health Study; WHO, World Health Organization; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 s; GOLD, Global Initiative for Chronic Obstructive Lung Disease guidelines; GDP, Gross Domestic Product; OCR, optical character recognition; SD, standard deviation; AR%, attributable risk percent.
Acknowledgments
We thank the workers at the Center for Disease Control and Prevention in Mianyang City, Jiangyou County, and Fucheng District for their assistance in the development of the present study. We also thank the physicians and nurses at the community health service centers and township hospitals who helped us to perform this work. Finally, we thank the Department of Epidemiology and Statistics, West China School of Public Health, Sichuan University for performing statistical analyses.
Funding
This work was supported by the National Science and Technology Pillar Program during the 13th Five-year Plan Period: Integrated Demonstration of Major Infectious Disease Prevention in Mianyang [grant number 2018ZX10715-003].
Disclosure
The authors report no conflicts of interest in this work.
References
1. GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1545–1602. doi:10.1016/S0140-6736(16)31678-6
2. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
3. Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2163–2196. doi:10.1016/S0140-6736(12)61729-2
4. Wang C, Xu JY, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;6736(18):30841–30849.
5. World Health Organization. Chronic obstructive pulmonary disease (COPD); 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
6. Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2019;394(10204):1145–1158. doi:10.1016/S0140-6736(19)30427-1
7. Chen HZ. Practice of Internal Medicine.
8. Cerveri I, Corsico AG, Accordini S, et al. Underestimation of airflow obstruction among young adults using FEV1/FVC <70% as a fixed cut-off: a longitudinal evaluation of clinical and functional outcomes. Thorax. 2008;63(12):1040–1045. doi:10.1136/thx.2008.095554
9. Assad NA, Balmes J, Mehta S, et al. Chronic obstructive pulmonary disease secondary to household air pollution. Semin Respir Crit Care Med. 2015;36(3):408–421. doi:10.1055/s-0035-1554846
10. Gut-Gobert C, Cavaillès A, Dixmier A, et al. Women and COPD: do we need more evidence? Eur Respir Rev. 2019;28(151):180055. doi:10.1183/16000617.0055-2018
11. Jindal S, Jindal A. COPD in Biomass exposed nonsmokers: a different phenotype. Expert Rev Respir Med. 2021;15(1):51–58. doi:10.1080/17476348.2021.1835476
12. World Health Organization. Household air pollution and health; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/household-air-pollution-and-health.
13. The National Development and Reform Commission. The National Rural Biogas Project Construction Plan (200–2010); 2023. Available from: https://www.ndrc.gov.cn/fggz/fzzlgh/gjjzxgh/200709/P020191104623232335593.pdf.
14. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
15. GLOBAL INITIATIVE FOR CHRONIC OBSTRACTIVE LUNG DISEASE. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2023 Report); 2023. Available from: https://goldcopd.org/2023-gold-report-2/.
16. Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general US population. Am J Respir Crit Care Med. 1999;159(1):179–187. doi:10.1164/ajrccm.159.1.9712108
17. He HQ, Chen K, Zhou M, et al. A method for measuring the contribution of individual factor to disease caused by multiple risk factors. Chin J Epidemiol. 2005;26(5):374–377. in Chinese.
18. de Marco R, Accordini S, Marcon A, et al. Risk factors for chronic obstructive pulmonary disease in a European cohort of young adults. Am J Respir Crit Care Med. 2011;183(7):891–897. doi:10.1164/rccm.201007-1125OC
19. Kojima S, Sakakibara H, Motani S, et al. Incidence of chronic obstructive pulmonary disease, and the relationship between age and smoking in a Japanese population. J Epidemiol. 2007;17(2):54–60. 2.72%. doi:10.2188/jea.17.54
20. Moreira GL, Gazzotti MR, Manzano BM, et al. Incidence of chronic obstructive pulmonary disease based on three spirometric diagnostic criteria in Sao Paulo, Brazil: a nine-year follow-up since the PLATINO prevalence study. Sao Paulo Med J. 2015;133(3):245–251. doi:10.1590/1516-3180.2015.9620902
21. Olortegui-Rodriguez JJ, Soriano-Moreno DR, Benites-Bullón A, et al. Prevalence and incidence of chronic obstructive pulmonary disease in Latin America and the Caribbean: a systematic review and meta-analysis. BMC Pulm Med. 2022;22(1):273. doi:10.1186/s12890-022-02067-y
22. Terzikhan N, Verhamme KM, Hofman A, et al. Prevalence and incidence of COPD in smokers and non-smokers: the Rotterdam Study. Eur J Epidemiol. 2016;31(8):785–792. doi:10.1007/s10654-016-0132-z
23. Zhong N, Wang C, Yao W, et al. Prevalence of chronic obstructive pulmonary disease in China: a large, population-based survey. Am J Respir Crit Care Med. 2007;176(8):753–760. doi:10.1164/rccm.200612-1749OC
24. Suzanne M, Goodman D, Roa C, et al. The health and social implications of household air pollution and respiratory diseases. NPJ Prim Care Respir Med. 2019;29(1):12. doi:10.1038/s41533-019-0126-x
25. An J, Bao HL, Fang LW. Relationship between biomass smoke exposure and chronic obstructive pulmonary disease among residents in China: a meta-analysis. Chin J Public Health. 2016;32(7):999–1004.
26. Lee KK, Bing R, Kiang J, et al. Adverse health effects associated with household air pollution: a systematic review, meta-analysis, and burden estimation study. Lancet Glob Health. 2020;8(11):e1427–e. doi:10.1016/S2214-109X(20)30343-0
27. Smith KR, Rogers J, Cowlin SC. Household Fuels and Ill-Health in Developing Countries: What Improvements Can Be Brought by LP Gas? Paris: World LP Gas Association and Intermediate Technology Development Group; 2005.
28. Ntritsos G, Franek J, Belbasis L, et al. Gender-specific estimates of COPD prevalence: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2018;13:1507–1514. doi:10.2147/COPD.S146390
29. Han MK, Martinez FJ. Host, gender, and early-life factors as risks for chronic obstructive pulmonary disease. Clin Chest Med. 2020;41(3):329–337. doi:10.1016/j.ccm.2020.06.009
30. Pun VC, Dowling R, Mehta S. Ambient and household air pollution on early-life determinants of stunting-A systematic review and meta-analysis. Environ Sci Pollut Res Int. 2021;28(21):26404–26412. doi:10.1007/s11356-021-13719-7
31. Andualem Z, Azene ZN, Dessie A, et al. Acute respiratory infections among under-five children from households using biomass fuel in Ethiopia: systematic review and meta-analysis. Multidiscip Respir Med. 2020;15(1):710. doi:10.4081/mrm.2020.710
32. Kodgule R, Salvi S. Exposure to biomass smoke as a cause of airway disease in women and children. Curr Opin Allergy Clin Immunol. 2012;12(1):82–90. doi:10.1097/ACI.0b013e32834ecb65
33. Klepac P, Locatelli I, Korošec S, et al. Ambient air pollution and pregnancy outcomes: a comprehensive review and identification of environmental public health challenges. Environ Res. 2018;167:144–159. doi:10.1016/j.envres.2018.07.008
34. Postma DS, Bush A, van den Berge M. Risk factors and early origins of chronic obstructive pulmonary disease. Lancet. 2015;385(9971):899–909. doi:10.1016/S0140-6736(14)60446-3
35. Huang XW, Mu X, Deng L, et al. The etiologic origins for chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2019;14:1139–1158. doi:10.2147/COPD.S203215
36. He YZ. The Association Between Biomass Exposure and Chronic Obstructive Pulmonary Disease Among Chinese Women. Chinese Center for Disease Control and Prevention; 2018. in Chinese.
37. Tang X, Liao H. Energy poverty and solid fuels use in rural China: analysis based on national population census. Energy Sustain Dev. 2014;23(23):122–129. doi:10.1016/j.esd.2014.08.006
38. The world bank. Tobacco Control Program; 2023. Available from: http://web.worldbank.org/archive/website01213/WEB/0__CON-8.HTM.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.