Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Association of Disease Knowledge, Comorbidity, and Biochemical Parameters in Adults with Type 2 Diabetes
Authors Küçükkatırcı Baykan H ![]()
Received 7 August 2025
Accepted for publication 15 December 2025
Published 23 January 2026 Volume 2026:19 558893
DOI https://doi.org/10.2147/DMSO.S558893
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Hürmet Küçükkatırcı Baykan
Department of Nutrition and Dietetics, Cappadocia University School of Health Sciences, Nevşehir, Türkiye
Correspondence: Hürmet Küçükkatırcı Baykan, Email [email protected]
Purpose: This study examines how disease-related knowledge is associated with comorbidities, metabolic and anthropometric indicators, and dietary patterns in individuals with Type 2 diabetes.
Methods: This cross-sectional study included 184 adults with Type 2 diabetes. Data were collected using sociodemographic questionnaires, the Diabetes Knowledge Scale for Adults, and a food frequency questionnaire. Anthropometric and biochemical data were also obtained. Participants were grouped by median knowledge score (low or high). Mann–Whitney U and chi-square tests were used to analyze the data. Structural equation modeling (SEM) was used to model the effect of disease knowledge on health indicators.
Results: Participants with higher knowledge had lower total cholesterol, triglycerides, body weight, BMI, and neck circumference, and demonstrated better dietary compliance (p < 0.05). Retinopathy was more common in the high-knowledge group, while hypertension was more prevalent in the low-knowledge group (p=0.037 and p=0.002, respectively). SEM analysis revealed a weak yet directional relationship between knowledge level and health indicators.
Conclusion: The level of knowledge about the disease positively affects specific metabolic and behavioral indicators. Therefore, educational programmes aimed at increasing patients’ knowledge and supporting behavioural change should be developed and implemented at the primary care level.
Plain Language Summary: People with Type 2 diabetes who know more about their condition tend to have healthier body weight, lower cholesterol levels, and better eating habits. This study highlights that learning about diabetes and following nutrition advice can improve everyday health and help prevent complications.
Keywords: Biochemical parameters, comorbidities, disease knowledge, structural equation modeling, type 2 diabetes
Introduction
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by persistent hyperglycemia due to impaired insulin secretion, action, or both.1 It is primarily classified as Type 1 or Type 2.2 Type 2 DM, the most common form, is mainly linked to insulin resistance, relative insulin deficiency, obesity, sedentary behavior, and poor diet.3
Type 2 DM has become a rapidly growing public health problem worldwide and in Turkey. As of 2021, an estimated 537 million adults worldwide live with diabetes, and this number is projected to reach 783 million by 2045.4 Studies conducted in Turkey, “The Turkish Diabetes, Hypertension, Obesity and Endocrine Diseases Prevalence Study (TURDEP-I) (1997–1998) and TURDEP-II (2010), have shown a significant increase in diabetes prevalence; the 2017 Turkey Nutrition and Health Survey reported this rate as 13.6%.5 These increasing rates underscore the need for effective diabetes management strategies at the primary care level, where early detection and education play a crucial role.6
This increases burdens on healthcare systems and creates economic, social, and psychological challenges for individuals. According to the International Diabetes Federation’s (IDF) 2021 report, global healthcare expenditures related to diabetes increased from $232 billion in 2007 to $966 billion in 2021, representing a rise of approximately 316%.4 In Turkey, the direct healthcare costs of diabetes are estimated to exceed 10 billion dollars annually.4
Effective management of Type 2 DM requires not only pharmacological therapy, but also self-care practices including nutrition, physical activity, and regular monitoring, supported by sufficient disease knowledge.7–9 Individuals with better knowledge demonstrate improved adherence, glycemic control, and fewer complications.10,11 While many studies have linked diabetes knowledge with A1C levels,12–14 the relationship between diabetes knowledge and broader biochemical markers and comorbidities remains underexplored. However, the impact of disease-related knowledge not only on glycaemic control but also on biochemical parameters (eg, lipid profile, thyroid function) and comorbidities (eg, obesity, hypertension) remains underexplored. This study addresses this gap by examining these associations within the context of primary care.
In summary, from a theoretical perspective, health literacy positively influences individuals’ self-efficacy and health literacy levels, thereby affecting their self-care behaviours. This enhances patients’ ability to make informed decisions and adhere to treatment recommendations. Previous studies have primarily focused on glycaemic indicators (eg, A1C), and relationships with broader health indicators, such as biochemical parameters and comorbidities, have not been sufficiently explored. This study aims to fill this gap and provide evidence to guide education and counselling practices in primary care.
Materials and Methods
Study Population and Data Collection
This cross-sectional correlation study includes 184 patients who visited various healthcare facilities in Nevşehir and Kayseri provinces and voluntarily agreed to share their biochemical data and participate in the study. The study was conducted between March and June 2024.
Inclusion and Exclusion Criteria
Eligible participants were aged 20–65, diagnosed with type 2 diabetes for ≥1 year, cognitively intact, and suitable for anthropometric assessment. Those who were pregnant, breastfeeding, or had major illnesses were excluded.
The age range for inclusion (20–65 years) was determined by considering the validity range of the Diabetes Knowledge Scale for Adults (Yavuz & Erol, 2022) (18–90 years). Although the scale is valid for individuals aged 18 and above, participants under 20 were excluded from the sample. There are three main reasons for this decision: Firstly, individuals diagnosed with type 2 diabetes in the 18–19 age group may be confused with late-onset type 1 diabetes (LADA) or secondary types of diabetes, creating diagnostic uncertainty. Secondly, the lifestyles, levels of responsibility, and health behaviours of individuals in this age group differ significantly from those of older adults; therefore, selecting individuals aged 20 and above is more appropriate given their cognitive maturity and ability to provide reliable self-reports of their health. Thirdly, data from the Turkish Health Survey (2017) show that cases of early-onset type 2 diabetes are increasing due to obesity and sedentary lifestyles. Therefore, the 20–65 age range provides a diagnostically transparent and homogeneous adult sample representing both early-onset and established forms of diabetes. Thus, a meaningful coverage area has been established to include different age groups in the targeted education programmes within primary healthcare services.
Power Analysis and Number of Participants
The study’s sample size was calculated using G*Power version 3.1.9.2.15 The sample size calculation, with α = 0.05 and β = 0.95, determined that 155 people should be included. Considering the possibility of faulty questionnaires, the study’s sample size was targeted at 170. Since some patients volunteered to participate, the study enrolled 184 participants.
Sociodemographic Data Form
A socio-demographic data form was used to assess participants’ age, gender, education, and employment status; smoking and alcohol use; self-reported health status; diabetes treatment; hypoglycaemia management; meal patterns; exercise habits; diabetes-related complications; and comorbidities.
Diabetes Knowledge Scale for Adults
The “Diabetes Knowledge Scale for Adults (DKSA)” was used to assess participants’ diabetes knowledge. Developed in 2021 by Yavuz and Erol for Turkish adults aged 18–90, the 28-item scale includes five subdimensions: general knowledge, symptoms, blood glucose, risk factors, and complications. Items are answered with “yes,” “no,” or “I don’t know.” Correct answers score 1 point; incorrect and “I don’t know” responses score 0. Higher scores indicate greater knowledge.16 Permission for use was obtained from the original developers via e-mail.
Biochemical Parameters
Biochemical parameters such as fasting blood glucose (mg/dL), postprandial blood glucose (mg/dL), A1C (%), total cholesterol (mg/dL), HDL (mg/dL), LDL (mg/dL), triglyceride (mg/dL), TSH (mIU/L), T3 (pg/mL) and T4 (ng/dL) levels were evaluated.
Anthropometric Measurements
The researcher measured the participants’ heights, weights, and circumferences of the waist, hips, and neck. Based on these, body mass index (BMI), waist-to-hip ratio (WHR), and waist-to-height ratio (WHtR) were calculated.
Food Consumption Frequency
To assess dietary habits, the researcher-developed semi-structured “Food Consumption Frequency Form” was applied.17 The form was created based on foods commonly consumed by adults in Turkey and organised according to the main food groups in the TÜBER-2022 nutrition guide. During development, two specialist dietitians were consulted on content validity, and a pilot study with 20 participants was conducted to assess the form’s comprehensibility and cultural appropriateness. The form includes more than 25 food items, such as milk and dairy products, red and white meat, processed meat products, dried legumes, green leafy vegetables, root vegetables, fruits, grains (bread, pasta, etc)., sweets, and beverages (tea, coffee, fruit juice, etc).
Participants were asked to indicate their consumption frequency for each food item using standard categories ranging from “every meal” to “never”. Portion sizes were recorded in grams or millilitres; to increase the accuracy of this assessment, TÜBER portion definitions, household measurements, and standard portion images from the Turkish Food Photo Atlas were used.
TÜBER compliance was assessed based on whether the recommended consumption ranges for each food group were met. Participants were classified as 1 point (compliant) if they met the TÜBER recommendations for the relevant food group, or 0 points (non-compliant) if they did not. Based on these data, the compliance rates for each knowledge level group within each food group were compared to identify the group with the highest compliance with the guidelines.
Statistical Analyses
Due to the absence of a validated clinical cut-off for the Diabetes Knowledge Scale for Adults (DKSA), participants were grouped as “low” (<19) or “high” (≥19) based on the sample median score. The median-split approach is frequently used in health-outcomes research when no consensus cut-off is available, as it yields groups of comparable size and facilitates the clinical interpretation of differences in comorbidities and metabolic outcomes between individuals with relatively lower versus higher knowledge.18,19
To address potential information loss associated with dichotomising the DKSA, additional analyses were conducted using the continuous DKSA score. Spearman correlation coefficients and simple linear regression models were applied to examine the associations between continuous knowledge scores and key metabolic and anthropometric outcomes (BMI, neck circumference, total cholesterol, and triglycerides). These supplementary analyses were conducted to assess the robustness of the findings from the median-split approach. Full results are presented in Supplementary Table S1.
Data were analysed using SPSS 22.0 (IBM, NY, USA) statistical package programme. Normality was assessed with the Shapiro–Wilk test. Categorical variables were summarized as frequencies and percentages; continuous variables were summarized as mean ( ) ± SD, median (
) ± SD, median ( ), and minimum and maximum values. Non-normally distributed data were compared using the Mann–Whitney U-test, while categorical variables were analysed with the chi-square test. A p-value <0.05 was considered statistically significant.20
), and minimum and maximum values. Non-normally distributed data were compared using the Mann–Whitney U-test, while categorical variables were analysed with the chi-square test. A p-value <0.05 was considered statistically significant.20
In addition, for biochemical parameters, effect sizes (Cohen’s d) were calculated to quantify the magnitude of group differences and to support the evaluation of clinical relevance.
Structural Equation Modelling (SEM)
A path analysis model (as a simplified form of SEM) was employed to investigate the direct effects of disease knowledge level on clinical, anthropometric, and biochemical variables. Analyses were performed using AMOS v20. The independent variable was the two-level categorical knowledge score (low/high). Dependent variables included total cholesterol and triglyceride (mg/dL); body weight, BMI (kg/m2), and neck circumference (cm); and the presence of comorbidities and complications (1 = yes, 2 = no).
Only parameters that showed statistically significant differences across knowledge level groups were included in the structural model. This selection was made to maintain the model’s simplicity and to evaluate the effects of meaningful variables more clearly.
Continuous variables were entered as observed variables; categorical variables were dummy-coded. Within the scope of this study, a path analysis model without latent variables was applied to examine the directional relationships between behavioural and clinical variables. In the model, knowledge level was defined as an independent variable, and directional paths were added to the variables of BMI, neck circumference, total cholesterol, comorbidity, and complications. The knowledge level variable was included in the model using dummy coding (0 = low, 1 = high) to make it suitable for SEM analysis. The path analysis approach is an appropriate method for evaluating the direct effects of observed variables, and, as it does not include latent structures, classical SEM fit indices were not used in this model. Direct paths were drawn from the knowledge level to all outcome variables.21
Standardised coefficients (β), standard errors, and p-values for all paths are presented in Supplementary Table S2, and the overall model structure is illustrated in Figure 1.
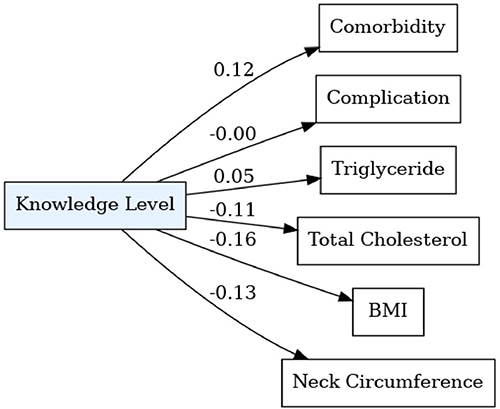 |
Figure 1 Path model of knowledge influence on clinical and anthropometric variables Standardised regression coefficients (β) reflect the direction and strength of associations. Notes: Negative coefficients indicate lower values of the corresponding variable with higher knowledge levels (neck circumference, BMI, total cholesterol). Model fit indices supported overall adequacy. |
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. Approval from the Cappadocia University Scientific Research and Publication Ethics Committee (31.10.2023/23.15) was obtained for the study. “Participant Information and Consent Form” was obtained from the participants.
Results
Main Characteristics of Participants
Table 1 shows the main characteristics of the participants. One hundred eighty-four individuals diagnosed with type 2 diabetes participated in the study. The mean age of the participants was 54.00 ± 10.80 years.
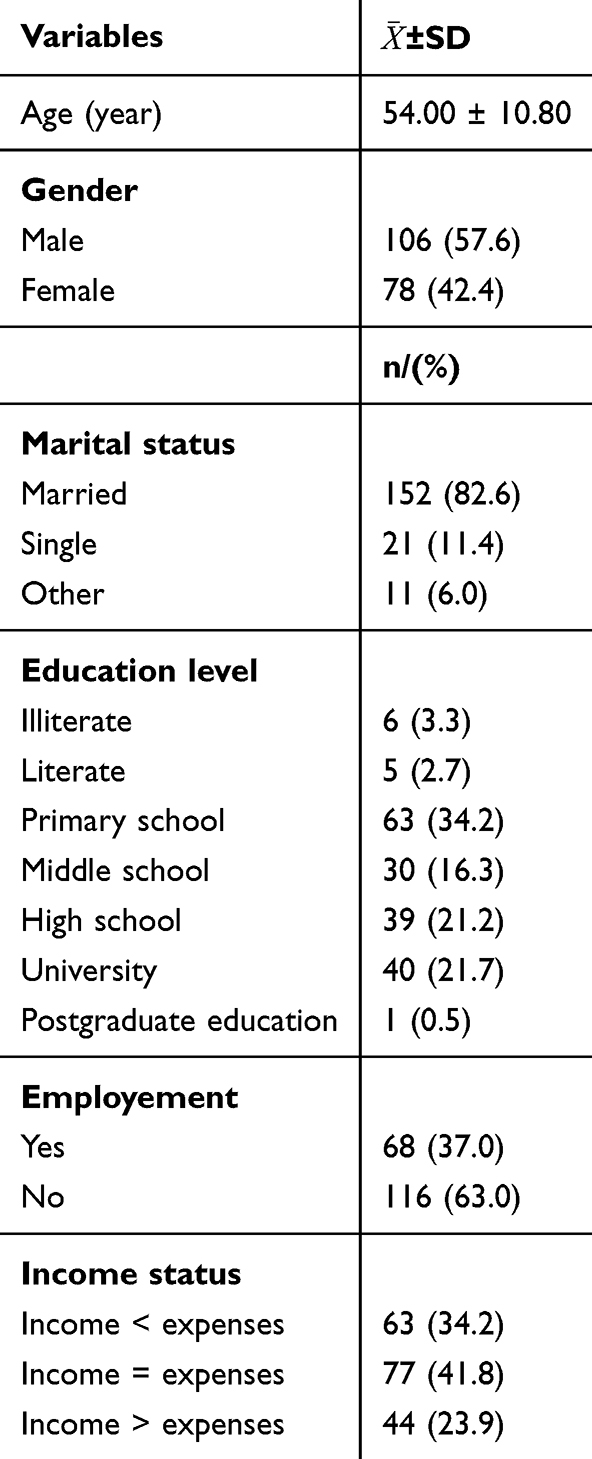 |
Table 1 Main Characteristics of Participants |
Participants were grouped into “low” and “high” knowledge levels based on the distribution of scale scores, following descriptive analyses.
Comparison of Behavioural and Clinical Variables by Knowledge Level
Significant associations were observed between diabetes knowledge level and several behavioural and clinical variables (Table 2). Participants with higher knowledge more often rated their health as good (39.4% vs. 24.4%, p = 0.005), received diabetes education (80.9% vs. 65.6%, p = .019), and monitored blood glucose regularly (46.8% vs. 16.7%, p < 0.001). Diet adherence was higher among those with lower knowledge (82.2% vs. 69.1%, p = 0.021).
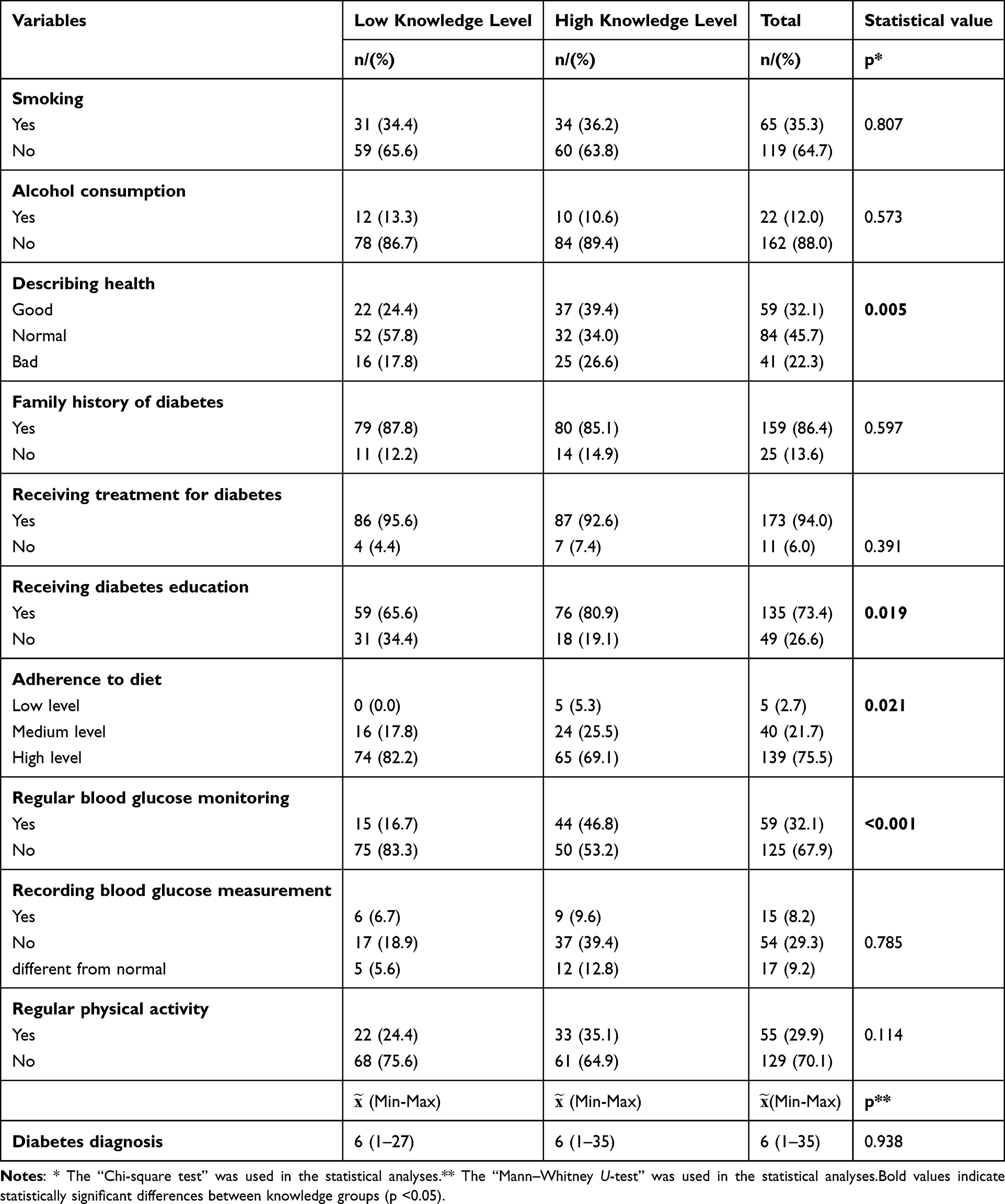 |
Table 2 Comparison of Behavioural and Clinical Variables by Knowledge Level |
Comparison of Anthropometric Measurements and Biochemical Parameters by Knowledge Level
Individuals with lower knowledge had significantly higher body weight (p = 0.044), BMI (p = 0.014), and neck circumference (p = 0.046) (Table 3). In contrast, those with higher knowledge had lower total cholesterol (p = .015) and triglyceride levels (p = 0.018) (Table 4).
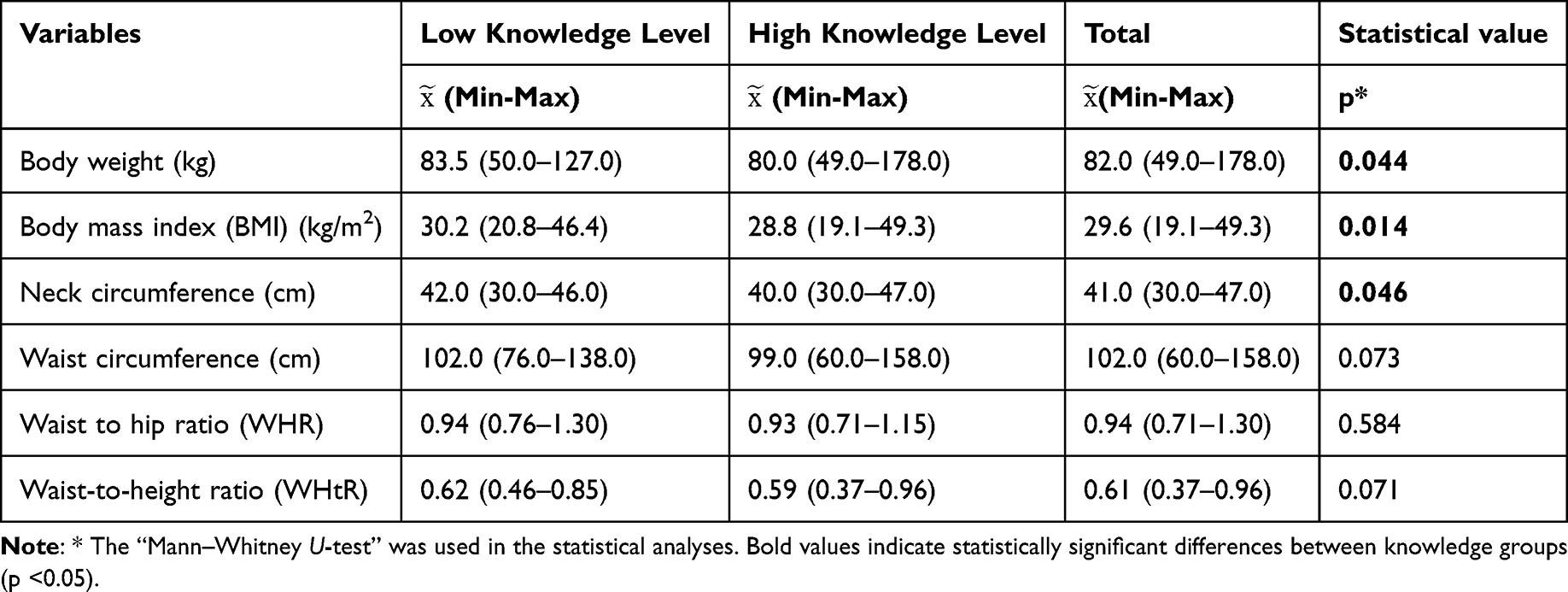 |
Table 3 Comparison of Anthropometric Measurements by Knowledge Level |
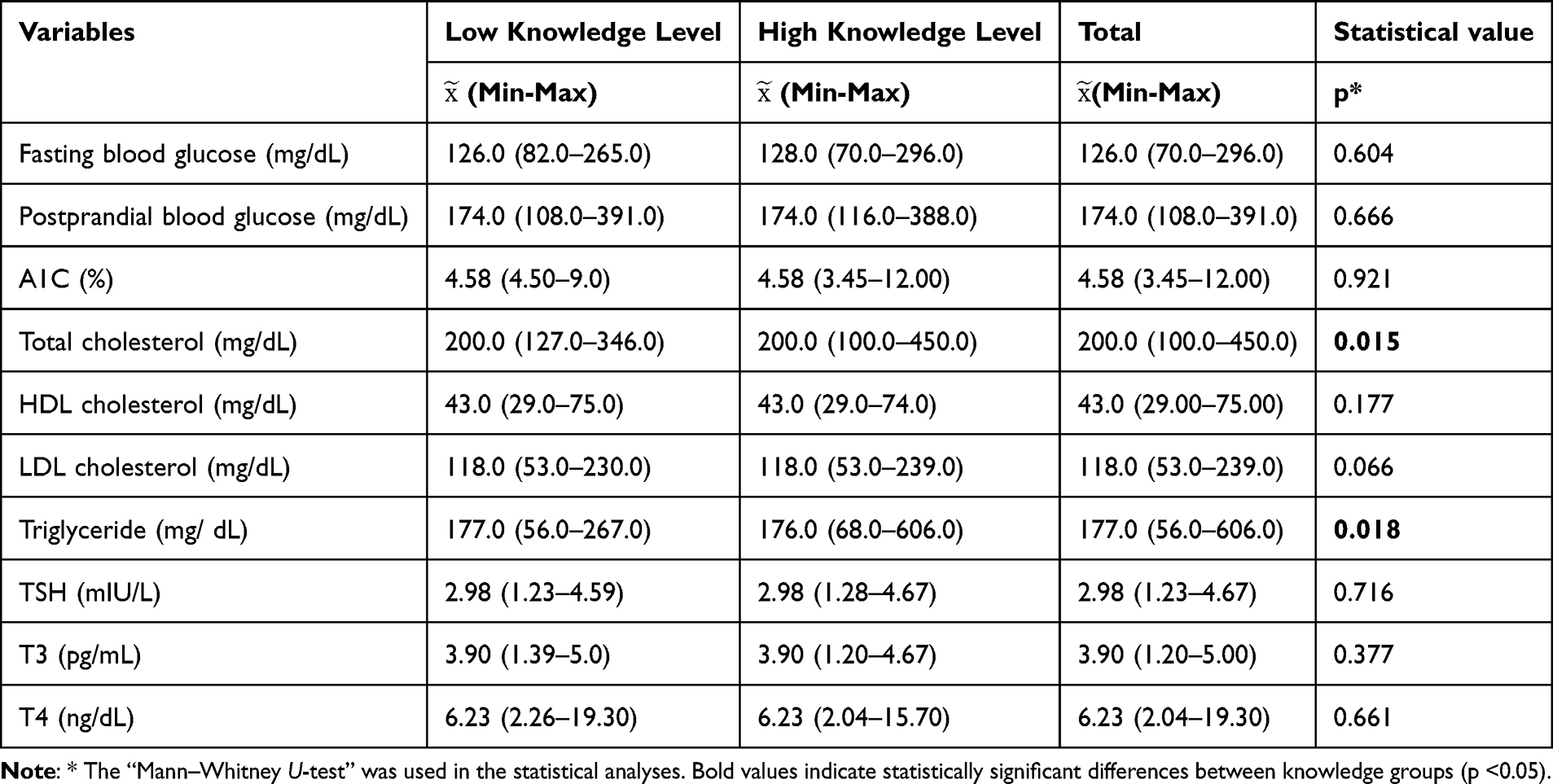 |
Table 4 Comparison of Biochemical Parameters by Knowledge Level |
Although total cholesterol levels differed significantly between knowledge groups (p = 0.015), the magnitude of this difference was small (Cohen’s d = 0.22), indicating limited clinical relevance. Triglyceride levels also differed significantly between groups (p = 0.018); however, the effect size was trivial (Cohen’s d = 0.10), suggesting that this statistically significant difference does not reflect a clinically meaningful metabolic variation.
Food consumption frequencies were compared across 25 food groups, including dairy, meats, legumes, vegetables, fruits, grains, and beverages, by knowledge level using the chi-square test. Significant differences were found for red meat, legumes, white bread, wholemeal bread, pasta, sugar, and non-acidic beverages (p < .05). For these items, a binary classification—'adequate' vs. 'inadequate' consumption—was applied based on the Turkish Nutrition Guide (TÜBER, 2022).22 For instance, consuming red meat 3–4 times per week was defined as adequate. Compliance with dietary recommendations was then re-analysed across knowledge levels. This narrower categorization reduced statistical significance in some comparisons. The SEM analysis yielded a saturated model (X2 ≈ 0, df = 0), rendering the chi-square test interpretation impossible. All fit indices (SRMR = 0.000, RMSEA = 0.000, CFI = 1.000) reflected a perfect fit due to this saturated structure. Therefore, model fit statistics confirmed the saturated nature but provided no additional interpretive value (Data not shown).
SEM-Based Estimates, Confidence Intervals, and Explained Variance (R2) for Dependent Variables
SEM results showed a significant negative relationship between knowledge and BMI (β² = −0.15, p = 0.030), while borderline effects were observed on neck circumference (β² = −0.12) and comorbidity (β² = 0.12). No significant effects were found for cholesterol, triglycerides, or complications (p > 0.05). Knowledge explained limited variance (R2 range: <0.001−0.025), with the highest R2 for BMI (R2 = 0.0250) and the lowest for complications (R2 = 0.00002) (Table 5).
Covariance analyses showed significant associations between neck circumference and BMI, between total cholesterol and triglycerides, and between BMI and both triglycerides and total cholesterol (p < 0.001). Additionally, BMI was negatively associated with complications (β² = −0.19, p = .009) and comorbidities (β² = −0.28, p < 0.001) (Supplementary Table S2).
Upon examining the fixed coefficients in the model, it was found that the mean values of all variables were statistically significant (p < .001). These values reflect the initial levels of the dependent variables, after controlling for knowledge level. For example, when the impact of knowledge level is ignored, the average neck circumference is 41.86 cm, the BMI is 33.25, and the total cholesterol level is 218.18 mg/dL (Data not shown).
Discussion
The study revealed significant relationships between diabetes knowledge and basic self-management indicators. As shown in Table 1, baseline sociodemographic characteristics such as age, education level, and employment status varied across participants and provided important context for interpreting these self-management patterns. Participants with higher levels of knowledge reported better-perceived health, greater access to diabetes education, and more frequent monitoring of their blood sugar levels (Table 2). These findings emphasise the importance of patient education and self-management support in primary care settings, where individuals typically first encounter diabetes services. Similarly, Kindrara (2025)23 reported improved self-care practices among individuals with higher levels of education, while Watcharanat (2021)24 and Abd-Allah (2024)25 emphasized the critical roles of knowledge, attitudes, and literacy in diabetes management. However, unexpectedly high dietary adherence among those with low levels of knowledge may reflect social desirability bias,26 highlighting the importance of carefully interpreting data based on self-reported information.
When comparing complication prevalence by knowledge level, only retinopathy showed a significant difference (p = 0.037), with the high-knowledge group unexpectedly more common. This may reflect more frequent eye exams and greater diagnostic awareness. However, this association should be interpreted with caution, as individuals with pre-existing complications often undergo more frequent screening and follow-up visits, which may increase their exposure to diabetes education and artificially elevate knowledge scores. Therefore, the observed difference is more likely related to screening frequency and contact with healthcare services rather than an actual effect of knowledge on retinopathy. Supporting this, Backa (2020)27 reported that individuals actively seeking diabetes-related knowledge had more clinical visits than those who were passive participants. While hypoglycaemia, hyperglycaemia, and cardiovascular disease were more common in the low-knowledge group, these differences were not statistically significant (p > 0.05) (Figure 2).
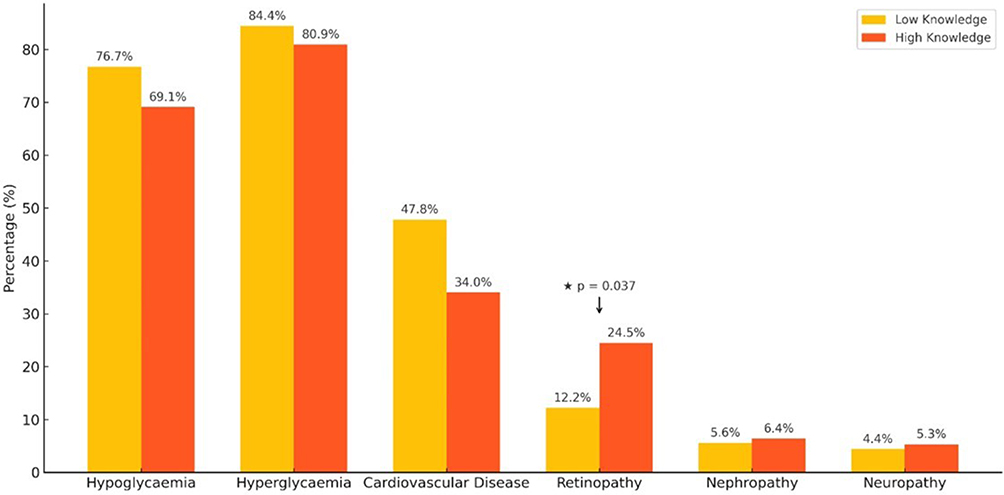 |
Figure 2 Comparison of diabetes-related by knowledge level Retinopathy was significantly more common in the high-knowledge group (p =0.037). Notes: The chi-square test was applied. Error bars represent group proportions. |
Among diabetes-related comorbidities, only hypertension showed a significant association with knowledge level (p = 0.002) and was more prevalent among those with low knowledge levels (Figure 3). This suggests that knowledge may influence both diabetes and cardiovascular risk management. According to Amelia (2018),29 optimal self-management in diabetes encompasses glycemic control, prevention of cardiovascular complications, reduction in the use of unnecessary healthcare services, and enhancement of personal satisfaction. Especially in primary health care, where early diagnosis is emphasized, awareness of silent comorbidities, such as hypertension, highlights the role of knowledge in treatment adherence.29 The absence of significant differences in other comorbidities may indicate more complex or indirect relationships.
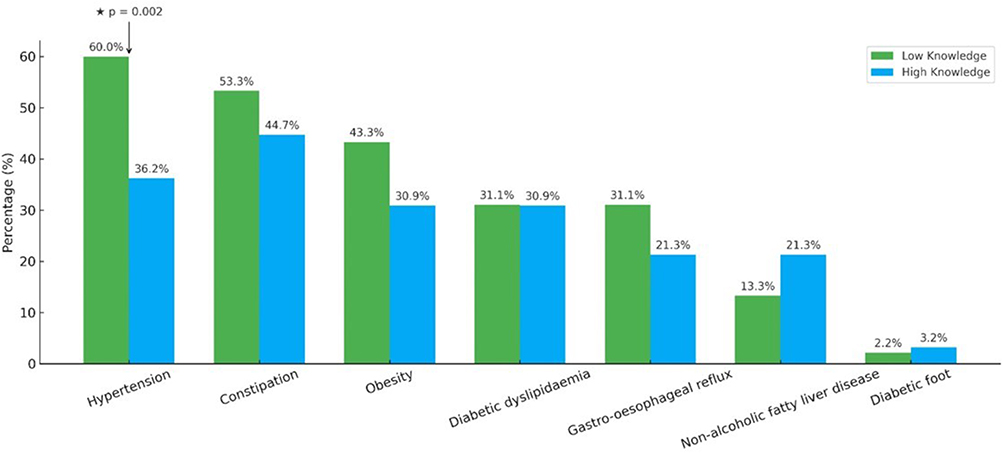 |
Figure 3 Comparison of diabetes-related comorbidities by knowledge level Hypertension was significantly more prevalent in the low-knowledge group (p =0.002). Notes: The chi-square test was applied. Error bars represent group proportions. |
Although life experience has not been directly measured, variables representing this concept, such as illness duration, complications, and comorbidities, have been used as indirect indicators. These variables reflect individuals’ experiences of coping with and managing diabetes over time. Interestingly, no significant relationship was found between knowledge level and illness duration. This finding indicates that the duration of living with diabetes alone does not explain knowledge acquisition; rather, knowledge acquisition is shaped by factors such as educational opportunities and health literacy level.
In anthropometric comparisons between knowledge groups, body weight, body mass index, and neck circumference were significantly lower in individuals with higher knowledge levels (p < 0.05; Table 3). These findings suggest that greater disease-related knowledge may support healthier body composition. Notably, Velázquez–López (2023)30 found similar results in a study involving diabetic patients with an average disease duration of six years, which closely matches the mean diabetes duration observed in the present study.
Neck circumference (NC) is a simple, reliable, and independent anthropometric indicator. Kamarlı (2022),31 in a study of 464 individuals with type 2 diabetes, reported that those with high NC had significantly higher body weight, BMI, waist and hip circumferences, and WHR and WHtR values (p < 0.05). Similarly, a meta-analysis of 16 observational studies (n = 4,764) found that NC was significantly associated with T2DM risk, even after adjusting for BMI (OR = 1.94; 95% CI: 1.35–2.79). Moreover, a 1 cm increase in NC was associated with a 16% increased risk of T2DM.32 Yan (2021)33 found that the risk increased by 18% per 1 cm in men and 25% in women, underscoring NC as an independent predictor of T2DM. Consistent with the literature, the present study showed that participants with lower disease knowledge had significantly higher NC values (p < 0.05).
Current findings suggest that enhancing individuals’ diabetes knowledge may positively influence both metabolic and anthropometric outcomes. Although no significant differences were observed in waist circumference, WHR, and WHtR between groups, high-knowledge individuals tended to have more favorable values. This lack of statistical significance may stem from high intergroup variability and wide standard deviations. Moreover, changes in anthropometric measures may take time to reflect behavioral improvements. Finally, multiple factors, such as genetics, age, gender, physical activity, and treatment regimen, may have obscured the specific effect of knowledge level.
When evaluating the association between disease knowledge and biochemical parameters, statistically significant differences were observed only in total cholesterol and triglycerides (Table 4). However, both the proximity of median values and the calculated effect sizes indicate that these differences are unlikely to be clinically meaningful. Total cholesterol showed a small effect size (d = 0.22). At the same time, triglycerides demonstrated a trivial effect (d = 0.10), suggesting that the observed statistical significance may reflect sample variability rather than physiologically relevant differences attributable to knowledge level. Moreover, the influence of knowledge on biochemical outcomes is not expected to be direct, but instead mediated through dietary behaviors. Consistent with our findings, previous studies have shown that information alone does not lead to healthier eating practices, underscoring the critical role of structured, continuous nutrition counseling in primary healthcare settings.34–36
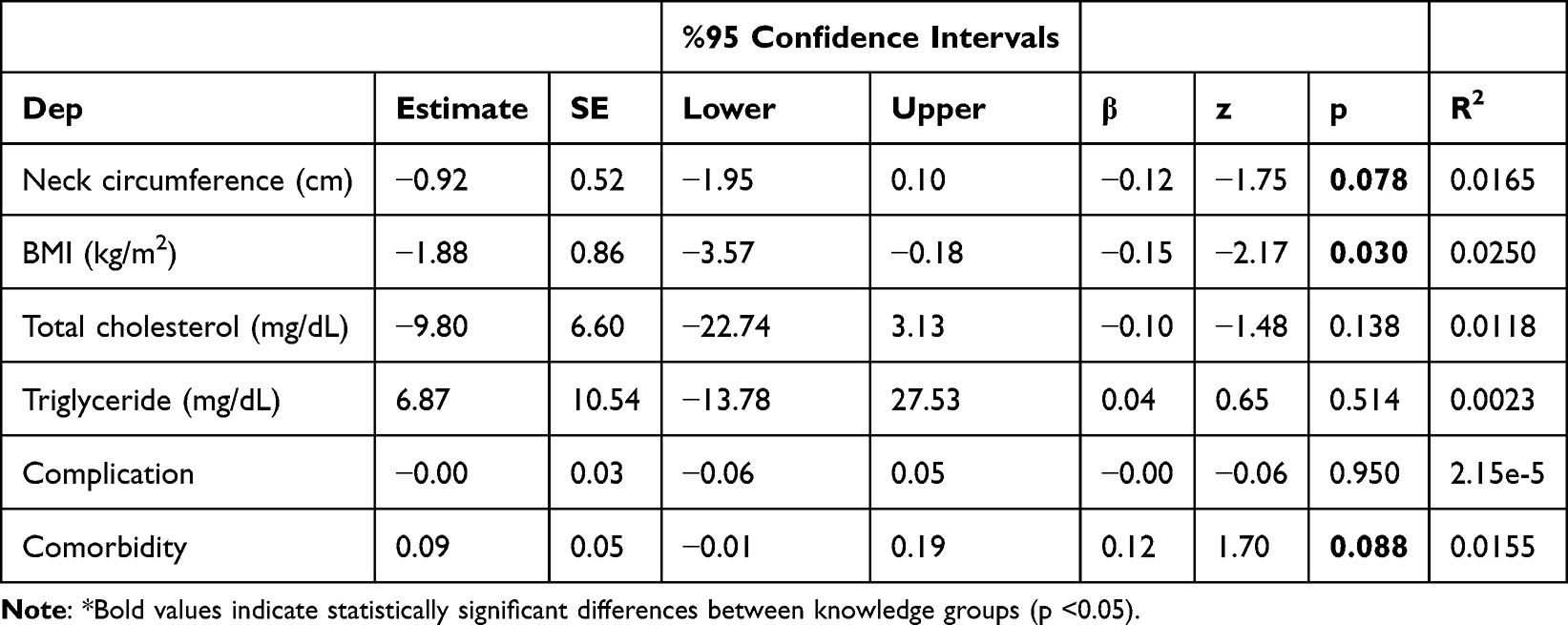 |
Table 5 SEM-Based Estimates, Confidence Intervals, and Explained Variance (R2) for Dependent Variables |
Participants with higher disease knowledge exhibited dietary patterns more compliant with TÜBER (2022)22 guidelines, particularly regarding white bread, sugar, red meat, and non-acidic beverages (Figure 4). This supports the idea that knowledge positively influences food choices, consistent with Alsaidan (2025),37 who also found a positive correlation between diabetes knowledge and dietary behavior. Limited knowledge has been linked to poor glycemic control and inadequate self-care in other studies as well.28,38–40 This may stem from better awareness of dietary consequences and increased access to professional counseling.
 |
Figure 4 Comparison of some food groups’ consumption frequency by knowledge level Higher knowledge was associated with more appropriate consumption patterns across the assessed food groups. Notes: The chi-square test was applied. Asterisks (*) indicate statistically significant differences between knowledge groups (p <0.05). |
The structural equation model assessed the impact of disease-related knowledge on clinical and anthropometric variables. Higher knowledge showed weak negative associations with neck circumference (β = –0.13), BMI (β = –0.16), and total cholesterol (β = –0.11), aligning with prior findings linking knowledge to lower metabolic risk26–33,41 (Figure 1). By contrast, its effects on complications (β = –0.00) and comorbidities (β = 0.12) were negligible (Figure 4). These weak coefficients suggest limited but potentially directional effects. The findings highlight that knowledge alone is not decisive and should be interpreted in conjunction with behavioral, lifestyle, socioeconomic, and healthcare access factors. Finally, acceptable fit indices support the model’s statistical validity, although the multifaceted nature of health outcomes remains evident.
In summary, these findings suggest that structured patient education focusing on disease awareness, nutrition, and lifestyle counseling could translate the observed statistical associations into tangible improvements in metabolic outcomes.
Strengths and Limitations
This study is among the few to examine links among disease knowledge, comorbidities, and biochemical, anthropometric, and dietary variables. Strengths include a validated scale, in-person data collection, and nutrition analysis in accordance with TÜBER guidelines. Additionally, the use of SEM strengthens theoretical interpretation.
However, the cross-sectional design precludes causal inference, and the directionality of associations cannot be established. In particular, the possibility of reverse causality should be considered, as individuals with existing complications may have more frequent healthcare contact and thereby acquire higher levels of disease-related knowledge, rather than knowledge exerting a direct influence on health outcomes. Self-reported data may also reflect social desirability bias, and limiting the sample to two provinces reduces generalisability. Median-based grouping, used due to the lack of a scale cut-off, may involve subjectivity. However, sensitivity analyses using the continuous DKSA score produced directionally consistent results, suggesting that the conclusions were not dependent on dichotomisation and remained robust across analytic approaches. Lastly, weak SEM coefficients indicate limited but directional effects of knowledge on health indicators.
Conclusion
This study examined the relationships among knowledge level, comorbidities, biochemical parameters, anthropometric measures, and dietary habits. Findings showed that higher knowledge was associated with better metabolic and anthropometric profiles and greater adherence to TÜBER dietary guidelines.
Structural equation modelling revealed modest but directional effects of knowledge on health indicators, suggesting that knowledge alone is insufficient to determine outcomes, but it supports healthier lifestyle behaviors.
Enhancing knowledge about diabetes can improve glycemic control, diet, body composition, and cardiometabolic risk. Therefore, standardized education, combined with tailored nutrition counseling, should be integrated into primary care services. Future longitudinal and experimental studies may clarify the long-term effects of knowledge on outcomes. Clarifying how knowledge leads to sustained behavior change is essential for designing effective, patient-centered interventions.
Highlights
- Higher diabetes knowledge is linked to better metabolic and anthropometric outcomes
- High-knowledge individuals follow dietary habits aligned with nutrition guidelines
- Disease knowledge is associated with reduced BMI, NC, cholesterol, and triglycerides
- Structural equation modeling shows that knowledge has a directional but weak effect
- Findings support patient education and lifestyle counseling in primary care settings
Data Sharing Statement
The dataset used in this study has been uploaded to the Mendeley Data Repository (DOI: 10.17632/z4m9x98zbf.1)
During the preparation of this work, the author used ChatGPT-4o for language editing. After using this service, the author reviewed and edited the content as needed and takes full responsibility for the publication’s content.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. Approval from the Cappadocia University Scientific Research and Publication Ethics Committee (31.10.2023/23.15) was obtained for the study. “Participant Information and Consent Form” was obtained from the participants.
Acknowledgments
Graphical abstract created in https://BioRender.com. I want to thank the participants in the study and the 4th students in the Nutrition and Dietetics Department (Ayşegül Kahraman, Begüm Nur Kara, Derya Demircan, Edanur Develi, İrem Su Akgün, Melike Kavas, Vildan Aleyna Yapır, and Selin Özpolat) for their support during the data collection process in the 2023–2024 academic year.
Author Contributions
Conceptualization, HKB; methodology, HKB; software, HKB; validation, HKB; formal analysis, HKB; investigation, HKB; resources, HKB; data curation, HKB; writing-original draft preparation, HKB; writing-review and editing, HKB; visualization, HKB. All authors have agreed on the journal to which the article will be submitted; reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage, and agree to take responsibility and be accountable for the contents of the article.
Funding
There is no funding in the study.
Disclosure
There is no conflict of interest.
References
1. Jian Y, Pasquier M, Sagahyroon A, Aloul FA. Machine learning approach to predicting diabetes complications. Healthcare. 2021,;9(12):1712. doi:10.3390/healthcare9121712
2. Mengstie MA, Seid MA, Gebeyehu NA, et al. Ferroptosis in diabetic nephropathy: mechanisms and therapeutic implications. Metabol Open. 2023;18:100243. doi:10.1016/j.metop.2023.100243
3. Suardi S. Effectiveness of physical activity interventions in type 2 diabetes mellitus patients: a literature review. Ijnhs. 2021;4(4):477. doi:10.35654/ijnhs.v4i4.506
4. International Diabetes Federation. The IDF Diabetes Atlas. 2021. Available from: https://diabetesatlas.org/resources/idf-diabetes-atlas-2025/.
5. Republic of Turkey Ministry of Health General Directorate of Public Health. Turkey Nutrition and Health Survey. Available from: https://hsgm.saglik.gov.tr/depo/birimler/saglikli-beslenme-ve-hareketli-hayat-db/Dokumanlar/Ingilizce_Yayinlar/TBSA_RAPOR_KITAP_2017_ENG_.pdf.
6. Akturk HK. Access todiabetes care should be a universal right for people with type 1 diabetes: lessons learned from the Norwegian Childhood Diabetes Registry. Diabetes Care. 2024;47(7):1111–14. doi:10.2337/dci24-0002
7. Borse S, Chhipa AS, Sharma V, Singh DP, Nivsarkar M. Management of type 2 diabetes: current strategies, unfocused aspects, challenges, and alternatives. Med Princ Pract. 2020;30(2):109. doi:10.1159/000511002
8. Valencia Y, Dols JD. Facilitating adherence to evidence-based practices for adults with type 2 diabetes mellitus. J Nurse Pract. 2021;17(6):744. doi:10.1016/j.nurpra.2020.12.027
9. Kumah E, Afriyie EK, Abuosi AA, et al. Influence of the model of care on the outcomes of diabetes self-management education program: a scoping review. J Diabetes Res. 2021;2021:1. doi:10.1155/2021/2969243
10. Huang Y-C, Zúñiga JA, Kuo H-J, et al. The effect of acculturation on diabetes knowledge among Chinese Americans with Type 2 diabetes. Sci Diabetes Self Manag Care. 2025. doi:10.1177/26350106251326503
11. Wong SKW, Soon W, Griva K, Smith HE. Diabetes knowledge, self-efficacy and dietary, psychological and physical health barriers: comparing young and usual-onset type 2 diabetes. Diabet Med. 2024;41(3):e15207. doi:10.1111/dme
12. AlShayban DM, Naqvi AA, Alhumaid O, et al. Association of disease knowledge and medication adherence among out-patients with type 2 diabetes mellitus in Khobar, Saudi Arabia. Front Pharmacol. 2020;11:60. doi:10.3389/fphar.2020.00060
13. Kim J, Hur M-H. The effects of dietary education interventions on individuals with type 2 diabetes: a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18(16):8439. doi:10.3390/ijerph18168439
14. Popoviciu MS, Marin VN, Vesa CM, et al. Correlations between diabetes mellitus self-care activities and glycaemic control in the adult population: a cross-sectional study. Healthcare. 2022;10(1):174. doi:10.3390/healthcare10010174
15. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
16. Yavuz K, Erol S. Development and psychometric properties of the diabetes knowledge scale for adults. Clin Exp Health Sci. 2022;12(3):711–718. doi:10.33808/clinexphealthsci.1014888
17. Arechavala T, Continente X, Pérez-Giménez A, et al. Food consumption frequency and excess body weight in adolescents in the context of financial crisis in Barcelona (Spain). Gac Sanit. 2016;30(6):457–463. doi:10.1016/j.gaceta.2016.03.013
18. Streiner DL, Norman GR. Chapter 5. In: Health Measurement Scales: A Practical Guide to Their Development and Use.
19. Iacobucci D, Posavac SS, Kardes FR, et al. The median split: robust, refined, and revived. J Consum Psychol. 2015;25(4):690–704. doi:10.1016/j.jcps.2015.06.014
20. Bensken WP, Ho VP, Pieracci FM. Basic introduction to statistics in medicine, part 2: comparing data. Surg Infect. 2021;22(6):597. doi:10.1089/sur.2020.430
21. Stage FK, Carter HC, Nora A. Path analysis: an ıntroduction and analysis of a decade of research. J Educ Res. 2004;98(1):5–13. doi:10.3200/JOER.98.1.5-13
22. Türkiye Cumhuriyeti Sağlık Bakanlığı Halk Sağlığı Genel Müdürlüğü. Türkiye Beslenme Rehberi (TÜBER) 2022. Available from: https://hsgm.saglik.gov.tr/depo/birimler/saglikli-beslenme-ve-hareketli-hayat-db/Dokumanlar/Rehberler/Turkiye_Beslenme_Rehber_TUBER_2022_min.pdf.
23. Kindarara DM, Murondere JB. Diabetes knowledge and self-care practices among patients with type 2 diabetes mellitus in Uvira, Kiliba, Sange, and Luvungi, South Kivu Province of the Democratic Republic of Congo. Sci Diabetes Self Manag Care. 2025;51(2):141–155. doi:10.1177/26350106251323611
24. Watcharanat P, Khuancheree K, Lee B. Factors associated with self-care behavior of elderly patients with type 2 diabetes in Thailand. Open Public Health J. 2021;14(1):494. doi:10.2174/1874944502114010494
25. Abd-Allah SM, Ayoub AI, Makhlouf M, Ashour A, Vejborg I. Diabetes knowledge, health literacy and diabetes self-care among older adults living with diabetes in Alexandria, Egypt. BMC Public Health. 2024;24(1):2024. doi:10.1186/s12889-024-20238-w
26. Veselý Š, Klöckner CA. Social desirability in environmental psychology research: three meta-analyses. Front Psychol. 2020;11. doi:10.3389/fpsyg.2020.01395
27. Backa KE, Nguyen H. Health information-seeking styles and health information literacy in relation to anticipated health-promoting behaviour—results from an online diabetes risk test survey. Int J Telemed Clin Pract. 2020;3(3):192. doi:10.1504/ijtmcp.2020.104893
28. Amelia R. The model of self care behaviour and the relationship with quality of life, metabolic control and lipid control of type 2 diabetes mellitus patients in Binjai city, Indonesia. Open Access Maced J Med Sci. 2018;6(9):1762–1767. doi:10.3889/oamjms.2018.363
29. Rintamäki R, Rautio N, Peltonen M, et al. Long-term outcomes of lifestyle intervention to prevent type 2 diabetes in people at high risk in primary health care. Prim Care Diabetes. 2021;15(3):444–450. doi:10.1016/j.pcd.2021.03.002
30. Velázquez–López L, Torres AVM, Medina‐Bravo P, Escobedo J. Inadequate diabetes knowledge is associated with poor glycemia control in patients with type 2 diabetes. Aten Primaria. 2023;55(5):102604. doi:10.1016/j.aprim.2023.102604
31. Kamarli Altun H, Suna G. Is neck circumference related to other anthropometric measurements and biochemical parameters in Type 2 diabetes? Cureus. 2022;14(10):e30750. doi:10.7759/cureus.30750
32. Li D, Zhao Y, Zhang L, et al. Association between neck circumference and diabetes mellitus: a systematic review and meta-analysis. Diabetol Metab Syndr. 2023;15(1):133. doi:10.1186/s13098-023-01111-z
33. Yan Q, Sun D, Li X, et al. Neck circumference and incidence of type 2 diabetes in Chinese elderly individuals: a community-based cohort study. Obes Facts. 2021;14(5):450–455. doi:10.1159/000514219
34. Sapała AM, Staśkiewicz‐Bartecka W, Grochowska‐Niedworok E, Kardas M. Dietary habits, nutritional knowledge, and nutritional status among cardiological patients, including those with obesity and diabetes. Front Nutr. 2024;11. doi:10.3389/fnut.2024.1455236
35. Dawuda AS, Abdul-Aziz A. Nutritional knowledge and dietary habits among diabetic patients at the Bono Regional Hospital, Sunyani, Ghana. J Adv Med Pharm Sci. 2023;25(9):18. doi:10.9734/jamps/2023/v25i9640
36. Abboud M, Nacouzi C, Chahine Z, et al. Dietary knowledge and eating habits among patients with type 2 diabetes in Lebanon. Glob Health. 2024;2024:1. doi:10.1155/2024/3623555
37. Alsaidan AA, Alanazi MI, Thirunavukkarasu A. Assessment of diabetes-related knowledge and dietary patterns among type 2 diabetes mellitus patients in Central Saudi Arabia: insights for tailored health education strategies. Healthcare. 2025;13:233. doi:10.3390/healthcare13030233
38. Sharma PK, Rajpal N, Upadhyay S, et al. Status of diabetes control and knowledge about diabetes in patients. Endocrinol Diabetes Nutr. 2021;68(10):716–727. doi:10.1016/j.endien.2021.12.003
39. Phillips E, Rahman R, Mattfeldt-Beman M. Relationship between diabetes knowledge, glycemic control, and associated health conditions. Diabetes Spectr. 2018;31(2):196–199. doi:10.2337/ds17-0058
40. Bukhsh A, Khan TM, Sarfraz Nawaz M, et al. Association of diabetes knowledge with glycemic control and self-care practices among Pakistani people with type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2019;12:1409–1417. doi:10.2147/DMSO.S209711
41. Lema GD, Gebeyaw ED. Diabetes knowledge and glycemic control among type 2 diabetes patients at public hospitals in Debre Berhan, Ethiopia. PLoS One. 2025;20(1):e0317288. doi:10.1371/journal.pone.0317288
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Implementation of a Multidisciplinary Clinic Focused on the Care of Adolescents with Youth-Onset Type 2 Diabetes
Schaaf L, Ley S, Riegler A, Poetker A, Xanthakos S, Sizemore J, Crimmins N, Helmrath M, Tracy R, Arce-Clachar AC, Crail J, Morwessel N, Frenck K, Tariq F, Shah AS
Journal of Multidisciplinary Healthcare 2023, 16:2799-2807
Published Date: 20 September 2023