Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Association of Complete Blood Cell Count-Derived Inflammatory Biomarkers with Psoriasis and Mortality
Authors Zhao Y ![]() , Yang XT, Bai YP, Li LF
, Yang XT, Bai YP, Li LF ![]()
Received 23 September 2023
Accepted for publication 7 November 2023
Published 13 November 2023 Volume 2023:16 Pages 3267—3278
DOI https://doi.org/10.2147/CCID.S437936
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Yang Zhao,1,2 Xu Tong Yang,1 Yan Ping Bai,3 Lin Feng Li2
1Department of Dermatology, Daxing Teaching Hospital, Capital Medical University, Beijing, 102600, People’s Republic of China; 2Department of Dermatology, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China; 3Department of Dermatology, China-Japan Friendship Hospital, Beijing, 100029, People’s Republic of China
Correspondence: Lin Feng Li, Department of Dermatology, Beijing Friendship Hospital, Capital Medical University, 95 Yong an Road, Xicheng District, Beijing, 100050, People’s Republic of China, Email [email protected]
Background and Aim: Psoriasis is a persistent inflammatory disorder that affects 3% of the population and is associated with cardiovascular diseases. Therefore, this study aimed to investigate the correlations between complete blood cell count (CBC)-derived inflammatory biomarkers, psoriasis prevalence, and all-cause mortality.
Methods: Data were obtained from the National Health and Nutrition Examination Survey (NHANES) spanning 2003– 2006 and 2009– 2014. Mortality data up to December 31, 2019 were obtained using the National Death Index. The following CBC-derived inflammatory biomarkers were examined: neutrophil/lymphocyte ratio (NLR), neutrophil/(white blood cells ˗ neutrophils) ratio (dNLR), monocyte count/lymphocyte ratio (MLR), (neutrophil + monocyte)/lymphocyte ratio (NMLR), platelet/lymphocyte ratio (PLR), and systemic inflammatory response index (SIRI). Weighted logistic and Cox regression analyses were used to calculate odds ratios, hazard ratios, and the corresponding 95% confidence intervals. Additionally, the prognostic value of the inflammatory indicators was assessed and ranked using the random survival forest approach.
Results: In total, data from 21,431 participants with average age of 45.02 ± 0.27 years (49.51% male) were included in the study, among which 600 participants were positive for psoriasis (prevalence rate, 2.80%). Additionally, 79 all-cause deaths were recorded during a median follow-up period of 8.83 (6.67– 11.00) years. Moreover, NLR, dNLR, NMLR, PLR, and SIRI were positively associated with the prevalence of psoriasis. Furthermore, MLR, NMLR, and SIRI were positively correlated with all-cause mortality in patients with psoriasis, with NMLR being the most valuable predictor of all-cause mortality.
Conclusion: CBC-derived inflammatory biomarkers were associated with psoriasis prevalence, NMLR, SIRI, and MLR values were associated with all-cause mortality in patients with psoriasis. Overall, assessment of these CBC-derived indicators may serve as a simple method for screening high-risk individuals among patients with psoriasis.
Keywords: association, biomarker, inflammatory, NHANES, psoriasis
Introduction
Psoriasis is a persistent inflammatory disorder characterized by the excessive proliferation of epidermal keratinocytes and affects 3% of the population.1–3 Although the pathophysiological mechanisms of psoriasis are complex, it is believed that chronic inflammation plays a pivotal role in its development and associated comorbidities, including cardiovascular diseases (CVDs).4 Clinical assessments, such as the Psoriasis Area and Severity Index (PASI) and Body Surface Area (BSA), are conventionally employed to assess disease severity; however, these parameters may not comprehensively capture the chronic inflammatory aspects of the condition.5
Various cytokines and inflammatory cells influence the development of psoriatic lesions, ultimately resulting in endothelial dysfunction.6,7 Systemic inflammation plays a crucial role in psoriasis occurrence, development, comorbidities, and mortality. IL-17, IL-23, and TNF-α inhibitors have demonstrated remarkable efficacy in the treatment of psoriatic skin lesions and their associated comorbidities.8,9 Inflammatory biomarkers derived from complete blood cell count analyses, including the neutrophil-to-lymphocyte ratio (NLR), derived NLR (dNLR), monocyte-to-lymphocyte ratio (MLR), neutrophil-to-lymphocyte ratio (NMLR), platelet-to-lymphocyte ratio (PLR), and systemic inflammatory response index (SIRI), reflect systemic inflammation.10 These inflammatory biomarkers possess considerable clinical application and can be conveniently assessed through routine blood tests. Notably, they have the potential to serve as invaluable tools for the prognosis of several medical conditions and prediction of disease progression.11–15 Specifically, NLR and PLR have been used in the fields of dermatology and immunodermatology16,17 to predict various inflammatory skin disorders, including erythema nodosum, Behcet’s disease, and sarcoidosis.16,17 For example, NLR, PLR, SIRI, and systemic inflammation index (SII) were used to estimate the efficacy of omalizumab for chronic urticaria treatment.18 Additionally, NLR and PLR were positively correlated with PASI score and the presence of arthritis in individuals with psoriasis, indicating their ability to reflect systemic inflammation. Moreover, these markers can serve as useful tools for monitoring disease progression and assessing the effectiveness of antiinflammatory drugs.19
Despite some existing research on the association between complete blood cell count (CBC)-derived inflammatory biomarkers and psoriasis, as well as their predictive value for psoriasis treatment, the relationship between CBC-derived inflammatory biomarkers and psoriasis-associated mortality is unclear. Therefore, this study aimed to investigate the correlation between CBC-derived inflammatory biomarkers and psoriasis prevalence and mortality rates in the United States, using data from the National Health and Nutrition Examination Survey (NHANES).
Materials and Methods
Data Sources
The NHANES is designed to collect data on the health and nutritional status of adults and children residing in the United States. This nationally representative survey was conducted by the National Center for Health Statistics (NCHS) using a meticulously stratified, multistage probability cluster sampling design, and the database was updated biennially. Particularly, the NHANES collected data during the 2003–2006 and 2009–2014 survey cycles, which provided invaluable insights into psoriasis. However, comprehensive information on psoriasis severity was available only for the 2003–2006 and 2011–2014 survey cycles. Mortality data for the study population were ascertained using the National Death Index for a period up to December 31, 2019.
Notably, the NHANES study was performed in accordance with ethical standards and approved by the NCHS Research Ethics Review Board. Additionally, written informed consent was obtained from all participants before their enrollment in the survey. Ethical approval for this study was obtained from the Ethics Review Board of the Daxing Teaching Hospital of the Capital Medical University. The requirement for informed consent was waived due to the use of publicly available databases and ethical considerations. Data analysis was performed between March and May 2023.
Study Design and Population
Psoriasis-related data for 50,938 individuals were extracted from the NHANES database (2003–2006 and 2009–2014 survey cycles). Exclusion criteria for the study were follows: patients without CBC count data (n = 8, 858), participants aged < 20 years, participants with missing psoriasis assessment data (n = 19,959), and pregnant participants (n = 690). In total, 21,431 participants, including 20,831 with psoriasis and 600 without psoriasis were selected for the study. Additionally, 600 participants in a follow-up cohort were included for survival analysis (Figure S1).
Psoriasis Diagnosis and Assessment of CBC-Derived Inflammatory Biomarkers
Psoriasis diagnosis was typically based on questionnaires in the dermatology or medical condition sections, which asked if the patient had ever been clinically diagnosed with psoriasis, and a positive response indicated psoriasis. Psoriasis severity was assessed using questionnaires that asked about the extent of the condition and was evaluated using the BSA scoring method.20 Given the limited participant pool of individuals with psoriasis, stratifying the severity of psoriasis into two distinct categories was necessary. The first category, termed “mild psoriasis”, included cases characterized by either the absence of psoriatic manifestations or the presence of only a limited number of lesions that can be concealed by a surface area equivalent to one or two palm spans. The second category, termed “moderate to severe psoriasis”, included cases characterized by psoriatic lesions scattered across a surface area equivalent to 3–10 palm spans, or cases with extensive psoriasis covering an area that cannot be concealed by ≥ 10 palm spans.
CBC was quantified using automated hematology analyzers, which tallied the absolute number of diverse blood cell types within specific units of blood volume. Thereafter, we calculated the biomarkers, including NLR, dNLR, PLR, MLR, NMLR, and SIRI, using specific mathematical formulas based on the absolute counts of diverse blood cell subpopulations. NLR = neutrophil (NEU) count/lymphocyte (LYM) count; dNLR = NEU count/(WBC counts-NEU counts); PLR = platelet (PLT) count/LYM count; MLR = monocyte (MON) count/LYM count; NMLR = (NEU counts + MON counts)/LYM count; SIRI = NEU count × MON count/LYM count).21,22
Covariates
Based on previous literature, the following covariates were included in the analysis: age, sex, racial background, educational attainment, household income, smoking habits, alcohol consumption patterns, physical activity levels, and the presence of metabolic syndrome. Participants enrolled in the study were categorized into three categories based on smoking history: “never smokers” (participants who reported a lifetime consumption of fewer than 100 cigarettes); “current smokers” (participants who had consumed more than 100 cigarettes and continued to do so at the time of the study); and “former smokers” (participants who had previously exceeded the threshold of 100 cigarettes but had since ceased smoking).23 Similarly, participants were classified into three categories based on alcohol consumption patterns: “nondrinker”, “low-to-moderate drinker” (defined as consuming fewer than two alcoholic beverages per day for males and fewer than one alcoholic beverage per day for females), and “heavy drinker” (characterized by an intake of two or more alcoholic beverages per day for males and one or more alcoholic beverages per day for females).23 Physical activity levels were categorized as follows: “inactive” (absence of leisure-time physical activity); “insufficiently active” (individuals engaging in leisure-time moderate activity ranging from 1–5 times per week with a metabolic equivalent of task (MET) ranging from 3–6, or leisure-time vigorous activity ranging from 1–3 times per week with a MET > 6); and “active” (participants who reported a higher frequency of leisure-time moderate or vigorous activity compared with that in the aforementioned categories).24 Income was evaluated using the poverty income ratio (PIR). This metric represents the ratio of family income to the poverty threshold, tailored to accommodate family size in accordance with the guidelines stipulated by the US Department of Health and Human Services.25 The 2009 International Diabetes Federation (IDF) 2009 criteria for metabolic syndrome were employed.26
Statistical Analysis
Statistical analysis was performed using the protocol specified by the NHANES. The protocols accounted for the intricate sampling design and associated sampling weights. To calculate the sampling weight, we divided the MEC examination weight (wtmec2yr) into five. For the continuous variables, normally distributed data are presented as the mean ± standard error (SE), whereas non-normally distributed data are presented as the median ± interquartile range (IQR). Categorical variables were expressed as counts accompanied by their respective percentages. Normally distributed continuous variables were compared using Student’s t-test, whereas non-normally distributed data were compared using Mann–Whitney U-test. Categorical variables were compared using the chi-squared test. To address missing values in our covariates, we employed imputation techniques facilitated by the “mice” package, which harnesses the capabilities of the random forest algorithm.
Weighted logistic and Cox regression analyses were used to calculate odds ratios (ORs), hazard ratios (HRs), and 95% confidence intervals (CIs). We applied the Kaplan–Meier method in conjunction with the Log rank test to compute the cumulative survival rates. Restricted cubic spline regression analysis was used to elucidate the dose-response relationships between CBC-derived inflammatory biomarkers and mortality in patients with psoriasis. The knots were strategically positioned at the 10th, 50th, and 90th percentiles of each exposure variable. Spearman correlation analysis was performed to calculate the correlation coefficients between the inflammatory indicators. Random survival forest (RSF) analyses was performed to assess and rank the predictive value of CBC-derived inflammatory indicators for all-cause mortality using the “randomForestSRC” package. To mitigate the potential influence of reverse causality bias, we conducted an additional Cox regression analysis, excluding participants with a pre-existing history of cancer. All statistical analyses were performed using R software (version 4.2.0).
Results
Participant Characteristics
A comprehensive overview of the baseline characteristics of the participants is shown in Table 1. Among the participants, 600 (2.8%) were positive for psoriasis, as determined by weight analysis. Patients with psoriasis had a higher mean age (47.64 ± 0.75 years), proportion of non-Hispanic white individuals (81.07%), and prevalence of comorbid metabolic syndrome (39.54%) than those without the disease. Additionally, patients with psoriasis had a considerably higher level of the CBC-derived indicators (NLR, dNLR, MLR, NMLR, PLR, and SIRI) than those without psoriasis. Moreover, there were significant differences in family income, smoking history, and other relevant factors, between participants with psoriasis and those without psoriasis.
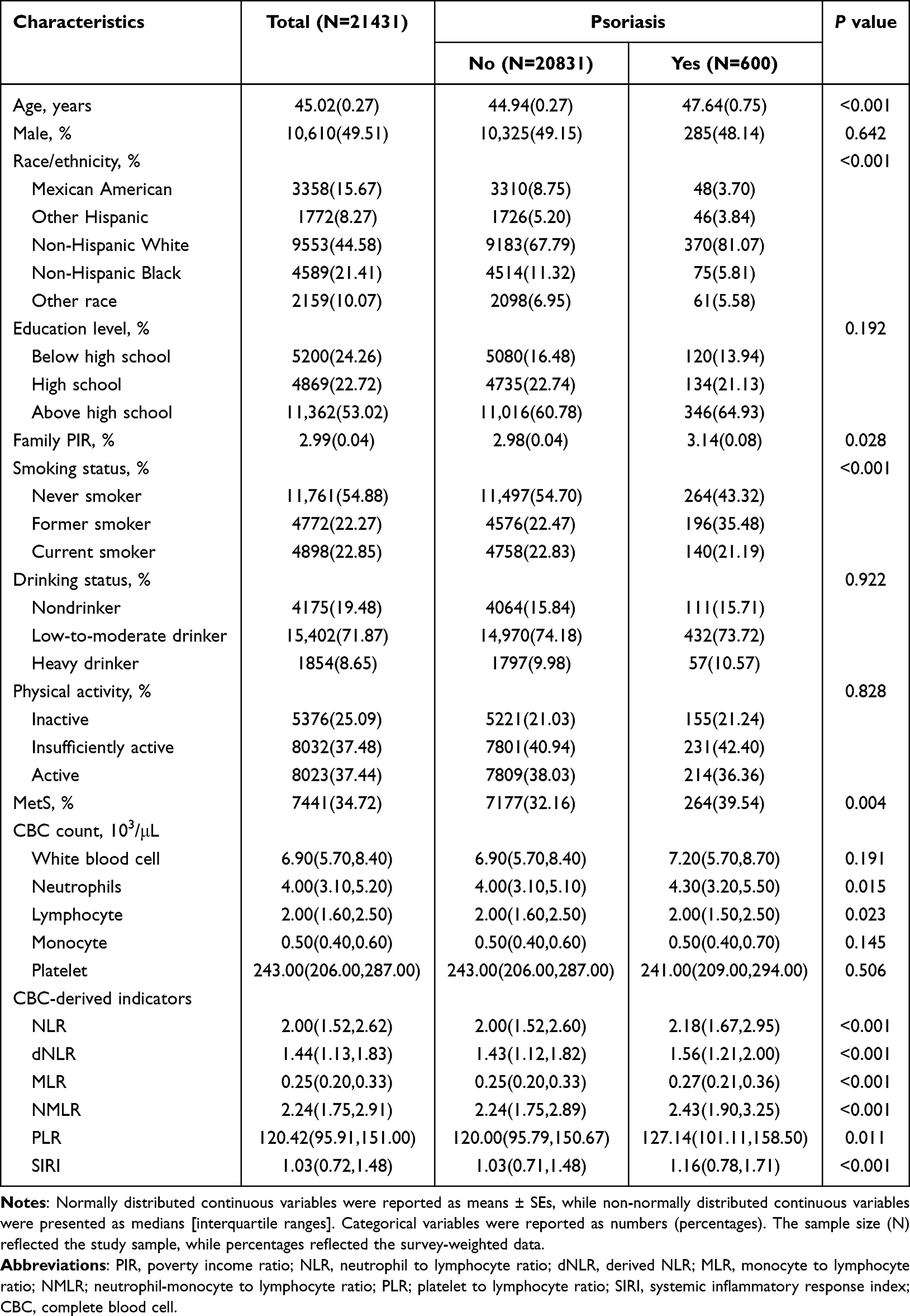 |
Table 1 Baseline Characteristics of Adults with CBC-Derived Inflammatory Biomarkers in NHANES 2003–2006 and 2009–2014 |
Association Between the CBC-Derived Indicators and Psoriasis
The results of the multivariate regression analyses are summarized in Table 2. The association between the CBC-derived indicators (NLR, dNLR, MLR, NMLR, PLR, and SIRI) and psoriasis is shown in Model 2 (fully adjusted model). For the analysis, the levels of the CBC-derived indicators were divided into quartiles, with the lowest quartile (Q1) as the reference. Among the indicators, NLR (Q 4 vs 1: OR = 1.414 [1.034–1.932], p = 0.002), dNLR (Q 4 vs 1: OR = 1.492 [1.084–2.053], p = 0.002), NMLR (Q 4 vs 1: OR = 1.538 [1.123–2.105], p < 0.001), PLR (Q 4 vs 1: OR = 1.358 [1.004–1.836], p = 0.023), and SIRI (Q 4 vs 1: OR = 1.589 [1.152–2.193], p = 0.002) were significantly positively associated with the incidence of psoriasis. The associations between CBC quartiles and adults with psoriasis in the United States is shown in Table S1. Among the indicators, NEU quartile alone was significantly associated (p < 0.05) with psoriasis. Additionally, the quartiles of the CBC-derived inflammatory biomarkers were not significantly associated (p > 0.05) with the severity of psoriasis (mild vs moderate-to-severe) among adults during the survey period (NHANES 2003–2006 and 2009–2014; Table S2). Multivariate-adjusted RCS regression confirmed the linear association between CBC-derived inflammatory indicators and psoriasis (Figure S2).
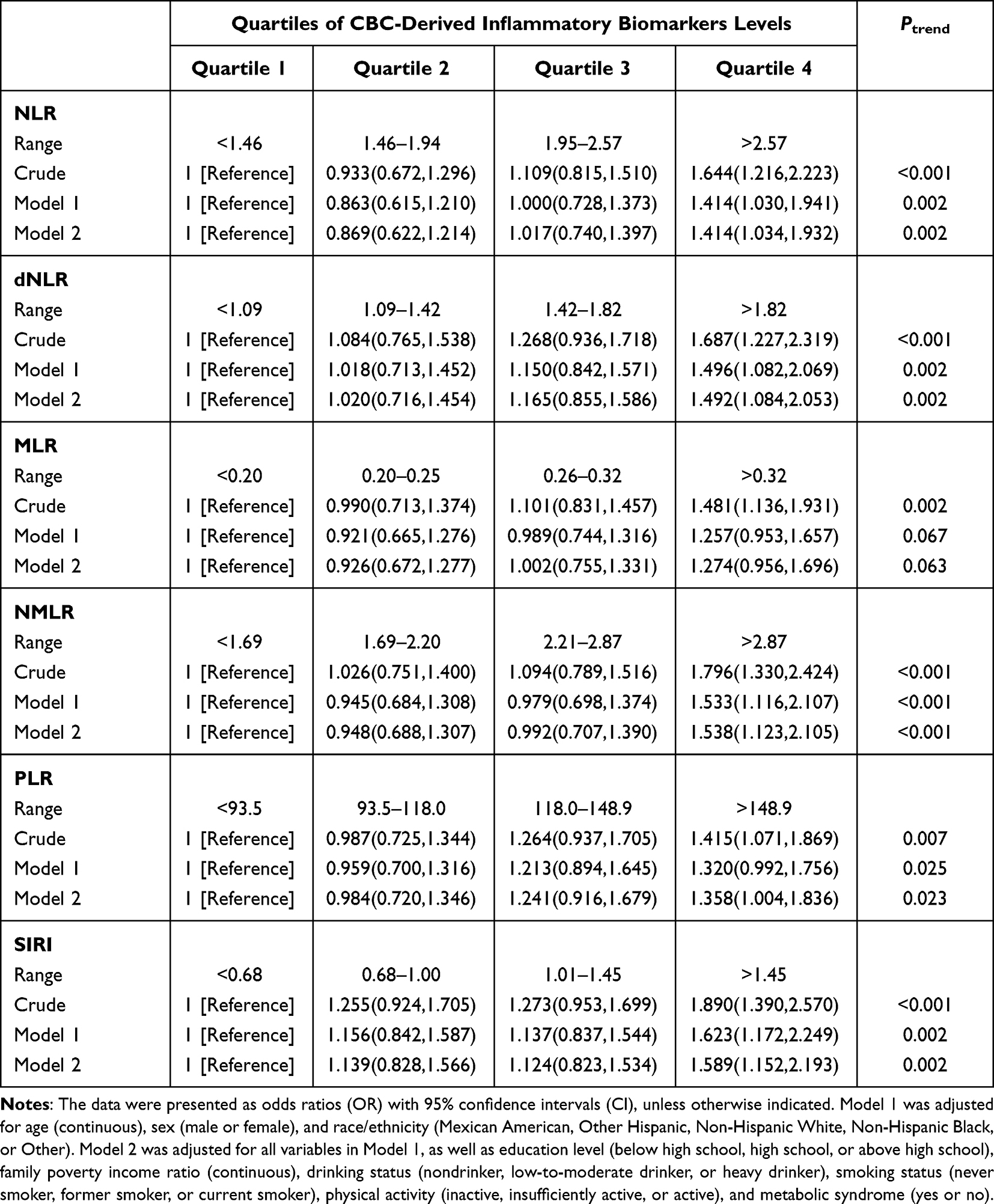 |
Table 2 OR (95% CIs) of the Prevalence of Psoriasis According to Quartiles of Complete Blood Cell (CBC)-Derived Inflammatory Biomarkers Among Adults in NHANES 2003–2006 and 2009–2014 |
Association Between the CBC-Derived Inflammatory Indicators and Mortality Among Adults with Psoriasis
Among 600 patients with psoriasis who were followed up until December 2019, 521 survived whereas 79 died (Table S3). Figure 1 shows the Kaplan–Meier survival curves, providing a visual representation of the association between the quartiles of the inflammatory biomarkers and mortality among participants with psoriasis. Survival curves showed significant differences (all log-rank p < 0.05) between the groups for various inflammatory biomarkers, including NLR, dNLR, MLR, NMLR, and SIRI. Weighted Cox regression analysis revealed that the predictive value of MLR, NMLR, and SIRI for all-cause mortality differed significantly across quartiles (Table 3). MLR (Q 4 vs 1: HR = 2.505 [1.032–6.080], p = 0.008), NMLR (Q 4 vs 1: HR = 2.525 [1.143–5.578], p = 0.004), and SIRI (Q 4 vs 1: HR = 2.135 [0.933–4.882], p = 0.007) were positively correlated with all-cause mortality among patients with psoriasis. The quartiles of the CBC parameters (WBC, NEU, and MON) were significantly associated (p < 0.05) with mortality in adults with psoriasis (Table S4).
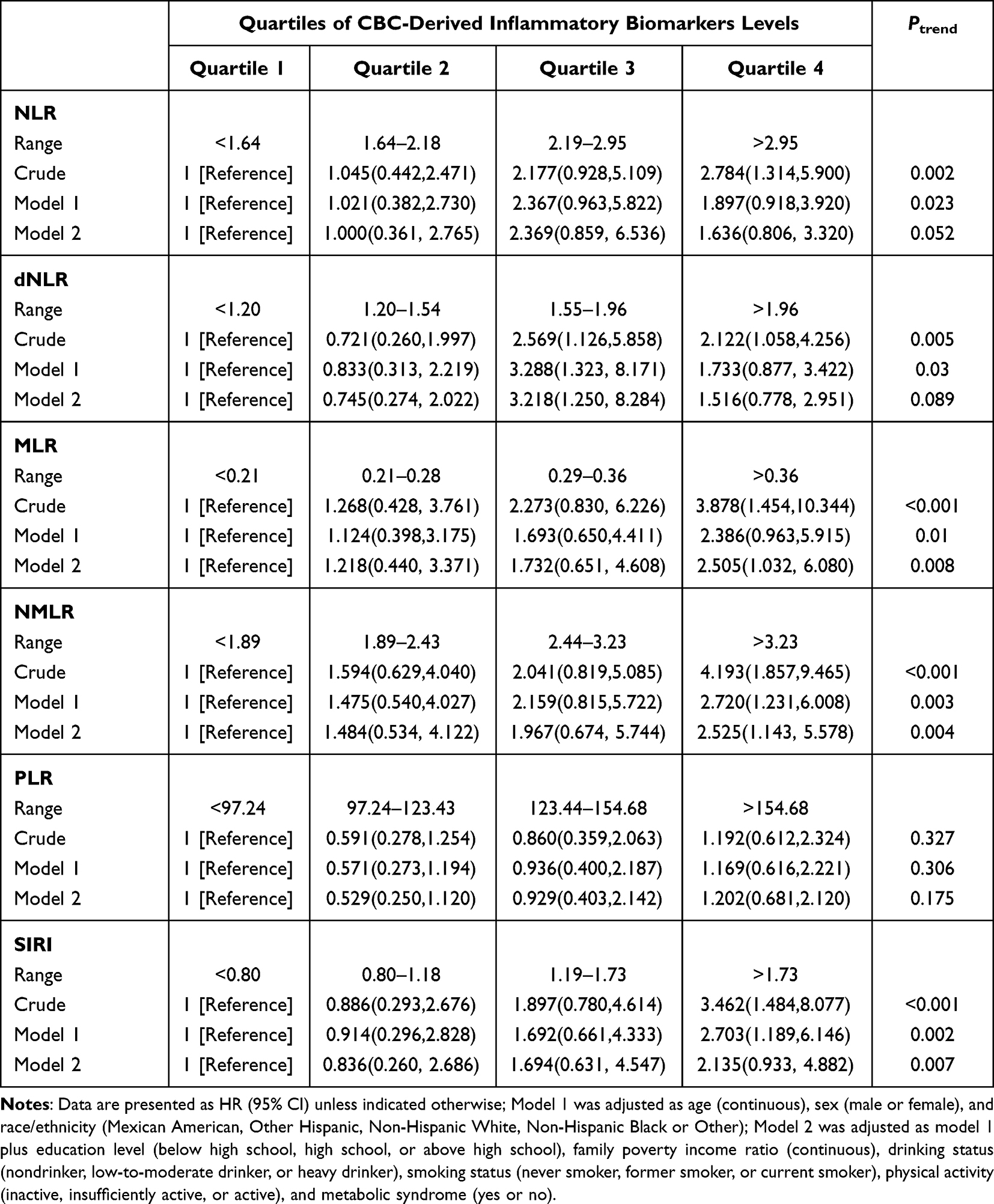 |
Table 3 HRs (95% CIs) of All-Cause Mortality According to Quartiles of Complete Blood Cell (CBC)-Derived Inflammatory Biomarkers Among Adults with Psoriasis in NHANES 2003–2006 and 2009–2014 |
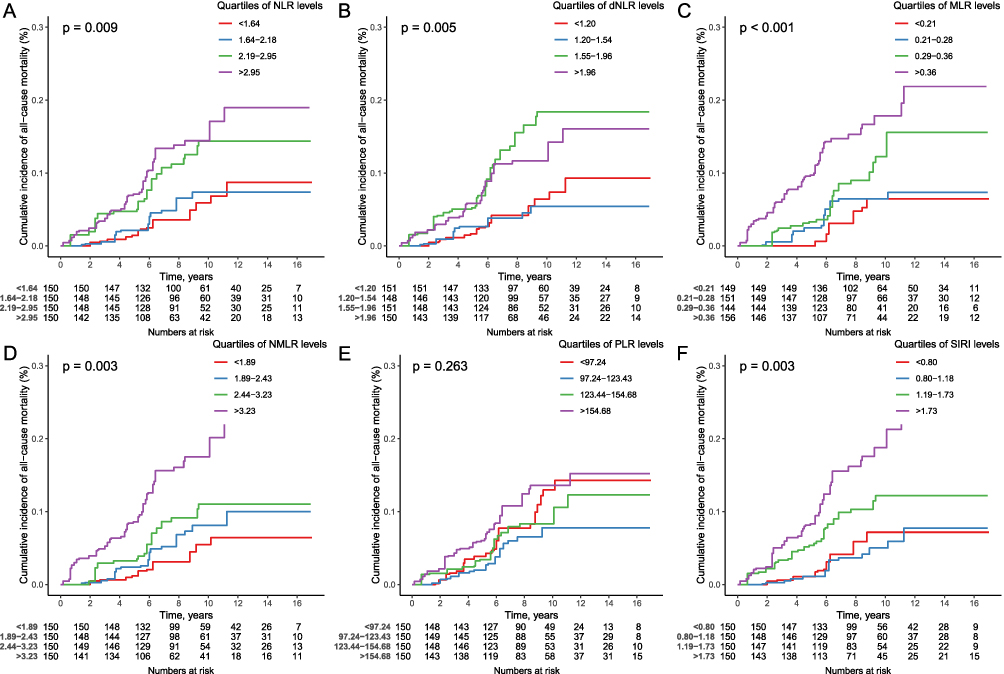 |
Figure 1 Kaplan-Meier survival curves for all-cause mortality in adults with psoriasis grouped by quartiles of complete blood cell (CBC)-derived inflammatory biomarkers ((A) NLR; (B) dNLR; (C) MLR; (D) NMLR; (E) PLR; (F) SIRI). |
The results of the sensitivity analysis offer valuable insights into the relationship between the quartiles of CBC-derived inflammatory indicators and the incidence of all-cause mortality in adults with psoriasis (Table S5). Notably, the associations between the indicators and all-cause mortality in adults with psoriasis remained significant (p < 0.05) even after excluding participants with prior history of cancer. Moreover, multivariate restricted cubic spline analysis demonstrated a linear association between the CBC-derived indicators and mortality in adults with psoriasis (Figure 2).
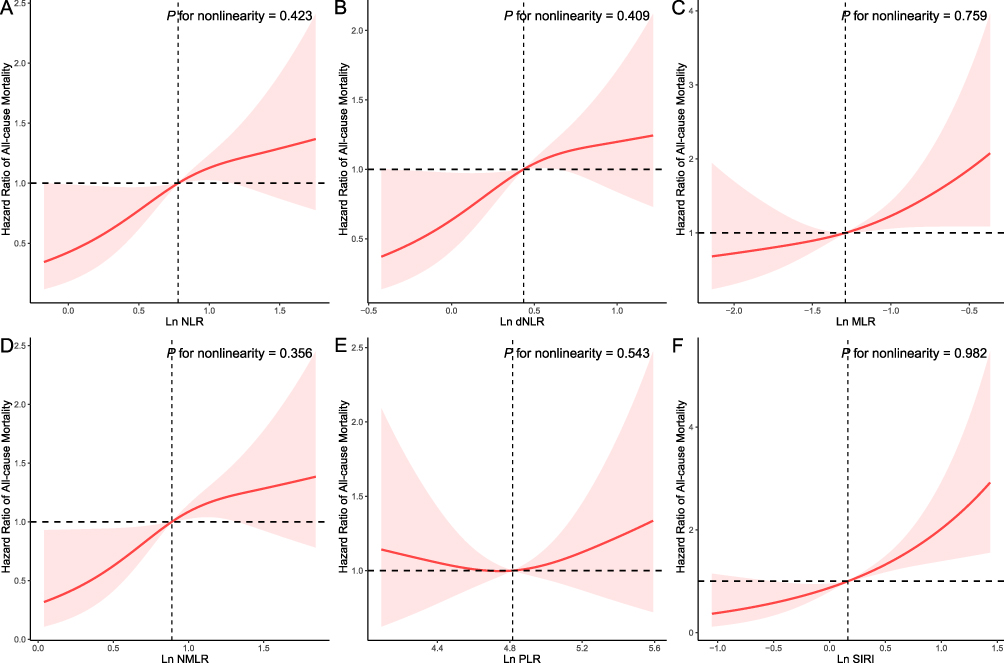 |
Figure 2 Restricted cubic spline analyses the association of complete blood cell count (CBC)-derived indicators ((A) NLR; (B) dNLR; (C) MLR; (D) NMLR; (E) PLR; (F) SIRI) with all-cause mortality in adults with psoriasis. Adjusted for age (continuous), sex (male or female), race/ethnicity (Mexican American, Other Hispanic, Non-Hispanic White, Non-Hispanic Black or Other), education level (below high school, high school, or above high school), family poverty income ratio (continuous), drinking status (nondrinker, low-to-moderate drinker, or heavy drinker), smoking status (never smoker, former smoker, or current smoker), physical activity (inactive, insufficiently active, or active), and metabolic syndrome (yes or no). |
Prognostic Importance of CBC Parameters and CBC-Derived Indicators
To assess the relationships between CBC parameters and CBC-derived inflammatory biomarkers, we conducted Spearman correlation analysis. The correlation coefficients are represented in Figure S3A, with positive and negative correlations indicated using blue and red circles, respectively. Each circle represents the strength of correlation. The RSF method was used to evaluate the prognostic value of the inflammatory biomarkers for predicting mortality among patients with psoriasis. Variable importance (VIP) rankings were compared among all inflammatory indicators, and NMLR, SIRI, and MLR were identified as the three most predictive indicators (Figure S3B). Notably, NMLR had the strongest association with all-cause mortality in patients with psoriasis.
Discussion
Inflammatory factors and cytokines play pivotal roles in the pathogenesis of psoriasis, demonstrating the intricate connections between WBC and PLT.27,28 Although psoriasis is a systemic inflammatory skin disorder, conventional inflammatory markers such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) do not manifest elevated levels.29,30 Moreover, the assessment of serum levels of inflammatory cytokines does not constitute a standard practice because it is time-consuming and cost-intensive.19
In the present study, we investigated the association between seven CBC-derived inflammatory markers (NLR, dNLR, PLR, MLR, NMLR, and SIRI) and psoriasis in US adults. Among the markers, six (NLR, dNLR, NMLR, PLR, and SIRI) were positively associated with psoriasis, which was consistent with previous findings that reported a significant association among NLR, PLR, and psoriasis.31,32 However, the inflammatory indicators investigated in the present study were more comprehensive. Collectively, these results confirm that systemic inflammation is associated with psoriasis. For comparison, we examined the association between the quartiles of CBC count quartiles and the prevalence of psoriasis and found that NEU quartile alone was significantly associated with psoriasis. These results indicate that CBC-derived inflammatory parameters are better markers of the inflammatory state of psoriasis than CBC. Some studies have reported a positive correlation between NLR and PLR and psoriasis severity, as determined using PASI score.19,33 NLR and PLR are valuable indicators for assessing systemic inflammation in individuals with psoriasis, as they offer a convenient and cost-effective means for monitoring disease progression after systemic therapy.19,34 However, the results of the present study indicated that the quartiles of CBC-derived inflammatory biomarkers were not significantly associated with the severity of psoriasis among adult participants. These variations in results may be attributed to differences in research cohorts or assessment methodologies. Alternatively, these indicators can better reflect the overall level of inflammation in psoriasis, including systemic damage due to comorbidities, rather than the size of the skin lesions.
Research evidence has shown significant associations between NLR, NMLR, PLR, SIRI, and SII and the prognosis of patients with cancer, and the parameters exhibited good predictive value.10,35,36 MLR, PLR, and NLR are effective indicators for assessing CVD risk and predicting mortality.37–39 Moreover, SIRI and SII are associated with the risk of acute coronary syndrome (ACS) in patients with chest pain.40 Psoriasis is a chronic inflammatory skin disease that is commonly associated with CVD, metabolic syndrome, obesity, diabetes, hypertension, and dyslipidemia. Among these comorbidities, CVD is associated with the highest risk of morbidity and mortality in individuals with psoriasis. Clinical studies have demonstrated that biological therapies targeting inflammatory cytokines can effectively mitigate CVD risk.41
Furthermore, we conducted a comprehensive analysis of the relationships between CBC-derived indicators and all-cause mortality in patients with psoriasis. The indicators were stratified into quartiles, using the lowest quartile (Q1) as the reference category. Notably, the highest quartile (Q4) of MLR, NMLR, and SIRI was positively associated with all-cause mortality in adults with psoriasis. When adjusted for multivariate confounders, a linear relationship was observed between CBC-derived indicators and all-cause mortality in adults with psoriasis. This indicates that the systemic inflammatory state of patients with psoriasis has an impact on their survival prognosis. Notably, the systemic inflammatory state is closely related to comorbidities and OS of patients with psoriasis. Additionally, systemic comorbidities have been linked to systemic inflammation, leading to a potential reduction in life expectancy by up to 5 years, predominantly due to cardiovascular events.42–44 Moreover, various organ systems, including the gastrointestinal tract, musculoskeletal system, neurological system, and respiratory system, are affected by inflammation.45–47 Overall, the assessment of CBC-derived inflammatory biomarkers via routine blood test is an affordable and convenient method to detect systemic inflammation. Notably, individuals with psoriasis who have comorbid conditions, such as CVDs, exhibit elevated levels of these markers, indicating that these CBC-derived indicators may possess potential prognostic value for patients with psoriasis and associated comorbidities.5,13,48 Research has shown that traditional treatment methods (such as phototherapy) are ineffective against systemic inflammation in psoriasis. However, biological agents can reduce the levels of inflammatory indicators (such as NLR and PLR,) in patients with psoriasis.34,49 Therefore, treatment strategies for psoriasis should also address systemic inflammation and comorbidities in addition to skin lesions.50,51 Effective systemic antiinflammatory therapy can reduce the mortality rate in patients with psoriasis.52
In the present study, we assessed the prognostic significance of CBC-derived inflammatory biomarkers for the prediction of all-cause mortality in patients with psoriasis. Among the three indicators (NMLR, SIRI, and MLR) that were associated with all-cause mortality, NMLR had the highest predictive value for all-cause mortality in patients with psoriasis. Collectively, these results indicate that CBC-derived inflammatory biomarkers possess superior prognostic value to CBC for the prediction of all-cause mortality in patients with psoriasis.
Despite the promising results, this study had some limitations. For example, the use of a cross-sectional design, focusing on the association between CBC-derived inflammatory biomarkers and the occurrence of psoriasis, precluded the establishment of a causal relationship. Additionally, it is essential to highlight that the diagnosis of psoriasis relied on self-reporting, which may introduce bias and possibly the underestimation of psoriasis prevalence. Moreover, the confounding factors used for adjustment were limited, and other confounders (such as rheumatoid and respiratory system diseases) may have affected the results.
Conclusion
CBC-derived inflammatory biomarkers were positively correlated with the prevalence of psoriasis and all-cause mortality. Among adults with psoriasis, elevated NMLR, SIRI, and MLR values were associated with increased all-cause mortality, and monitoring NMLR may help identify high-risk adults with psoriasis. Therefore, further studies are necessary to investigate the mechanism and potential treatments for psoriasis-associated systemic inflammation.
Data Sharing Statement
The data produced and/or examined in the present research can be accessed at https://wwwn.cdc.gov/nchs/nhanes/default.aspx
Ethical Approval and Consent to Participate
The NCHS Research Ethics Review Board approved the NHANES research protocols, and all participants provided written informed consent.
Acknowledgments
We thank all the patients and their families for participating in the study.
Funding
This work did not receive any dedicated funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hoffmann JHO, Enk AH. Evaluation of Psoriasis Area and Severity Index Thresholds as Proxies for Systemic Inflammation on an Individual Patient Level. Dermatology. 2022;238(4):609–614.
2. Kanda N, Hoashi T, Saeki H. Nutrition and Psoriasis. Int J Mol Sci. 2020;21(15):5405.
3. Kanda N, Hoashi T, Saeki H. The Defect in Regulatory T Cells in Psoriasis and Therapeutic Approaches. J Clin Med. 2021;10(17):3880.
4. Lopez-Candales A, Hernandez Burgos PM, Hernandez-Suarez DF, Harris D. Linking Chronic Inflammation with Cardiovascular Disease: from Normal Aging to the Metabolic Syndrome. J Nat Sci. 2017;3(4):56.
5. Nguyen HT, Vo LDH, Pham NN. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as inflammatory markers in psoriasis: a case-control study. Dermatol Reports. 2023;15(1):9516.
6. von Stebut E, Reich K, Thaci D, et al. Impact of Secukinumab on Endothelial Dysfunction and Other Cardiovascular Disease Parameters in Psoriasis Patients over 52 Weeks. J Invest Dermatol. 2019;139(5):1054–1062.
7. Lynch M, Ahern T, Sweeney CM, et al. Adipokines, psoriasis, systemic inflammation, and endothelial dysfunction. Int J Dermatol. 2017;56(11):1103–1118.
8. Wei JC, Kim TH, Kishimoto M, et al. Efficacy and safety of brodalumab, an anti-IL17RA monoclonal antibody, in patients with axial spondyloarthritis: 16-week results from a randomised, placebo-controlled, Phase 3 trial. Ann Rheum Dis. 2021;80(8):1014–1021.
9. Seo SJ, Shin BS, Lee JH, Jeong H. Efficacy and safety of brodalumab in the Korean population for the treatment of moderate to severe plaque psoriasis: a randomized, Phase III, double-blind, placebo-controlled study. J Dermatol. 2021;48(6):807–817.
10. Korkmaz M, Erylmaz MK. Systemic Inflammatory Markers Predicting the Overall Survival of Patients Using Tyrosine Kinase Inhibitors in the First-line Treatment of Metastatic Renal Cell Carcinoma. J Coll Physicians Surg Pak. 2023;33(6):653–658.
11. Hammad M, Shehata OZ, Abdel-Latif SM, El-Din AMM. Neutrophil/lymphocyte ratio and platelet/lymphocyte ratio in Behcet’s disease: which and when to use? Clin Rheumatol. 2018;37(10):2811–2817.
12. Kosekli MA. Mean platelet volume and platelet to lymphocyte count ratio are associated with hepatitis B-related liver fibrosis. Eur J Gastroenterol Hepatol. 2022;34(3):324–327.
13. Seaoud E, Mohamed A, Elkot MA. The Role of the Platelet/Lymphocyte Ratio and Neutrophil/Lymphocyte Ratio in Predicting High-Risk Heart Score in Patients Admitted with Non-ST Elevation Acute Coronary Syndrome. Pulse. 2020;8(1–2):66–74.
14. Hirahara T, Arigami T, Yanagita S, et al. Combined neutrophil-lymphocyte ratio and platelet-lymphocyte ratio predicts chemotherapy response and prognosis in patients with advanced gastric cancer. BMC Cancer. 2019;19(1):672.
15. Urbanowicz T, Michalak M, Olasinska-Wisniewska A, et al. Neutrophil Counts, Neutrophil-to-Lymphocyte Ratio, and Systemic Inflammatory Response Index (SIRI) Predict Mortality after Off-Pump Coronary Artery Bypass Surgery. Cells. 2022;11(7):1124.
16. Hayran Y, Oktem A, Sahin B, Incel Uysal P, Alli N, Yalcin B. Elevated neutrophil to lymphocyte ratio as an indicator of secondary erythema nodosum, a retrospective observational study. Turk J Med Sci. 2019;49(2):624–634.
17. Korkmaz C, Demircioglu S. The Association of Neutrophil/Lymphocyte and Platelet/Lymphocyte Ratios and Hematological Parameters with Diagnosis, Stages, Extrapulmonary Involvement, Pulmonary Hypertension, Response to Treatment, and Prognosis in Patients with Sarcoidosis. Can Respir J. 2020;2020:1696450.
18. Tarkowski B, Lawniczak J, Tomaszewska K, Kurowski M, Zalewska-Janowska A. Chronic Urticaria Treatment with Omalizumab-Verification of NLR, PLR, SIRI and SII as Biomarkers and Predictors of Treatment Efficacy. J Clin Med. 2023;12(7):2639.
19. Asahina A, Kubo N, Umezawa Y, Honda H, Yanaba K, Nakagawa H. Neutrophil-lymphocyte ratio, platelet-lymphocyte ratio and mean platelet volume in Japanese patients with psoriasis and psoriatic arthritis: response to therapy with biologics. J Dermatol. 2017;44(10):1112–1121.
20. Strober B, Ryan C, van de Kerkhof P, et al. Recategorization of psoriasis severity: delphi consensus from the International Psoriasis Council. J Am Acad Dermatol. 2020;82(1):117–122.
21. Shoji F, Kozuma Y, Toyokawa G, Yamazaki K, Takeo S. Complete Blood Cell Count-Derived Inflammatory Biomarkers in Early-Stage Non-Small-Cell Lung Cancer. Ann Thorac Cardiovasc Surg. 2020;26(5):248–255.
22. Zhou D, Yang H, Zeng L, et al. Calculated inflammatory markers derived from complete blood count results, along with routine laboratory and clinical data, predict treatment failure of acute peritonitis in chronic peritoneal dialysis patients. Ren Fail. 2023;45(1):2179856.
23. Qiu Z, Chen X, Geng T, et al. Associations of Serum Carotenoids With Risk of Cardiovascular Mortality Among Individuals With Type 2 Diabetes: results From NHANES. Diabetes Care. 2022;45(6):1453–1461.
24. Beddhu S, Baird BC, Zitterkoph J, Neilson J, Greene T. Physical activity and mortality in chronic kidney disease (NHANES III). Clin J Am Soc Nephrol. 2009;4(12):1901–1906.
25. Services USDoHaH. Poverty Guidelines, Research, and Measurement. Available from: http://aspe.hhs.gov/POVERTY/index.shtml.
26. Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640–1645.
27. Harden JL, Krueger JG, Bowcock AM. The immunogenetics of Psoriasis: a comprehensive review. J Autoimmun. 2015;64:66–73.
28. Kocaaga A, Kocaaga M. Psoriasis: an Immunogenetic Perspective. Glob Med Genet. 2022;9(2):82–89.
29. Wu J, Yan L, Chai K. Systemic immune-inflammation index is associated with disease activity in patients with ankylosing spondylitis. J Clin Lab Anal. 2021;35(9):2639.
30. Ritchlin CT, Colbert RA, Gladman DD. Psoriatic Arthritis. N Engl J Med. 2017;376(21):2095–2096.
31. Kim DS, Shin D, Lee MS, et al. Assessments of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in Korean patients with psoriasis vulgaris and psoriatic arthritis. J Dermatol. 2016;43(3):305–310.
32. Wang WM, Wu C, Gao YM, Li F, Yu XL, Jin HZ. Neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and other hematological parameters in psoriasis patients. BMC Immunol. 2021;22(1):64.
33. Aktas Karabay E, Aksu Cerman A, Demir D, Kivanc Altunay I. The Effects of Systemic Psoriasis Therapies on the C-Reactive Protein and the Neutrophil-Lymphocyte Ratio. Ann Dermatol. 2019;31(6):601–610.
34. Annen S, Horiguchi G, Teramukai S, et al. Association of Transition of Laboratory Markers with Transition of Disease Activity in Psoriasis Patients Treated with Biologics. J Nippon Med Sch. 2022;89(6):587–593.
35. Zhou ZQ, Pang S, Yu XC, et al. Predictive Values of Postoperative and Dynamic Changes of Inflammation Indexes in Survival of Patients with Resected Colorectal Cancer. Curr Med Sci. 2018;38(5):798–808.
36. Xiao Z, Wang X, Chen X, et al. Prognostic role of preoperative inflammatory markers in postoperative patients with colorectal cancer. Front Oncol. 2023;13:1064343.
37. Fan Z, Ji H, Li Y, Jian X, Li L, Liu T. Relationship between monocyte-to-lymphocyte ratio and coronary plaque vulnerability in patients with stable angina. Biomark Med. 2017;11(11):979–990.
38. Ates AH, Aytemir K, Kocyigit D, et al. Association of Neutrophil-to-Lymphocyte Ratio with the Severity and Morphology of Coronary Atherosclerotic Plaques Detected by Multidetector Computerized Tomography. Acta Cardiol Sin. 2016;32(6):676–683.
39. Balta S, Ozturk C. The platelet-lymphocyte ratio: a simple, inexpensive and rapid prognostic marker for cardiovascular events. Platelets. 2015;26(7):680–681.
40. Dziedzic EA, Gasior JS, Tuzimek A, et al. Investigation of the Associations of Novel Inflammatory Biomarkers-Systemic Inflammatory Index (SII) and Systemic Inflammatory Response Index (SIRI)-With the Severity of Coronary Artery Disease and Acute Coronary Syndrome Occurrence. Int J Mol Sci. 2022;23(17):9553.
41. Terui H, Asano Y. Biologics for Reducing Cardiovascular Risk in Psoriasis Patients. J Clin Med. 2023;12(3):1162.
42. Abuabara K, Azfar RS, Shin DB, Neimann AL, Troxel AB, Gelfand JM. Cause-specific mortality in patients with severe psoriasis: a population-based cohort study in the U.K. Br J Dermatol. 2010;163(3):586–592.
43. Boehncke WH, Boehncke S, Tobin AM, Kirby B. The ‘psoriatic march’: a concept of how severe psoriasis may drive cardiovascular comorbidity. Exp Dermatol. 2011;20(4):303–307.
44. Boehncke WH. Systemic Inflammation and Cardiovascular Comorbidity in Psoriasis Patients: causes and Consequences. Front Immunol. 2018;9:579.
45. Boehncke WH, Schon MP. Psoriasis. Lancet. 2015;386(9997):983–994.
46. Fiore M, Leone S, Maraolo AE, Berti E, Damiani G. Liver Illness and Psoriatic Patients. Biomed Res Int. 2018;2018:3140983.
47. Santus P, Rizzi M, Radovanovic D, et al. Psoriasis and Respiratory Comorbidities: the Added Value of Fraction of Exhaled Nitric Oxide as a New Method to Detect, Evaluate, and Monitor Psoriatic Systemic Involvement and Therapeutic Efficacy. Biomed Res Int. 2018;2018:3140682.
48. Kvist-Hansen A, Kaiser H, Wang X, et al. Neutrophil Pathways of Inflammation Characterize the Blood Transcriptomic Signature of Patients with Psoriasis and Cardiovascular Disease. Int J Mol Sci. 2021;22(19):1162.
49. Ataseven A, Temiz SA, Eren G, Ozer I, Dursun R. Comparison of anti-TNF and IL-inhibitors treatments in patients with psoriasis in terms of response to routine laboratory parameter dynamics. J Dermatolog Treat. 2022;33(2):1091–1096.
50. Vena GA, Vestita M, Cassano N. Can early treatment with biologicals modify the natural history of comorbidities? Dermatol Ther. 2010;23(2):181–193.
51. Kanelleas A, Liapi C, Katoulis A, et al. The role of inflammatory markers in assessing disease severity and response to treatment in patients with psoriasis treated with etanercept. Clin Exp Dermatol. 2011;36(8):845–850.
52. Langley RG, Poulin Y, Srivastava B, et al. Reduced risk of mortality associated with systemic psoriasis treatment in the Psoriasis Longitudinal Assessment and Registry (PSOLAR): a nested case-control analysis. J Am Acad Dermatol. 2021;84(1):60–69.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fibrinogen-Like Protein 1 as a Novel Biomarker of Psoriasis Severity
Sun X, Liu L, Chen S, Wang J, Cai X, Song J, Zhou M, Guo D, Kuai L, Ding X, Li B, Li X
Journal of Inflammation Research 2022, 15:4637-4647
Published Date: 15 August 2022
The SELP, CD93, IL2RG, and VAV1 Genes Associated with Atherosclerosis May Be Potential Diagnostic Biomarkers for Psoriasis
Liu S, Liu F, Zhang Z, Zhuang Z, Yuan X, Chen Y
Journal of Inflammation Research 2023, 16:827-843
Published Date: 27 February 2023
Metabolomics Reveals Molecular Signatures for Psoriasis Biomarkers and Drug Targets Discovery
Song Q, Chen Y, Ma J, Zhou W, Song J, Wu C, Liu J
Clinical, Cosmetic and Investigational Dermatology 2023, 16:3181-3191
Published Date: 4 November 2023
Association Between Non-HDL to HDL Cholesterol Ratio (NHHR) and Psoriasis in Adults: A Cross-Sectional Study Using 2009–2014 Data
Jiang Y, Jia M
Clinical, Cosmetic and Investigational Dermatology 2024, 17:2523-2531
Published Date: 9 November 2024
The Association Between Life’s Essential 8 and Psoriasis in American Adults: A Cross-Sectional NHANES Study
Zhang W, Yuan Z, Wang Y, Jin Z, Luo Z, Wang X
Clinical, Cosmetic and Investigational Dermatology 2024, 17:2555-2563
Published Date: 12 November 2024