")
Back to Journals » Nature and Science of Sleep » Volume 15
Association of Bedtime with Early-Onset Diabetes and Islet Beta Cell Function in Patients with Newly Diagnosed Type 2 Diabetes Mellitus
Authors Ma M, Jiang T , Zhang D , Yao X, Wen Z, Xiu L
Received 24 March 2023
Accepted for publication 25 July 2023
Published 16 August 2023 Volume 2023:15 Pages 653—662
DOI https://doi.org/10.2147/NSS.S413992
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Minglei Ma, Tao Jiang, Dongxue Zhang, Xiaoai Yao, Zhen Wen, Lei Xiu
Department of Endocrinology, Beijing Shijitan Hospital, Capital Medical University, Beijing, 100038, People’s Republic of China
Correspondence: Tao Jiang, Email [email protected]
Objective: To investigate the association of bedtime with the risk of early-onset diabetes mellitus (DM) and islet beta cell function.
Methods: 138 participants with treat-naïve DM were included in this study. All participants underwent a 75g oral glucose tolerance test. Sleep habit was obtained through a standardized questionnaire. Bedtime was categorized as < 22:00, 22:00– 24:00, and ≥ 24:00 in this study. Multivariate logistic regression and multiple linear regression were used to estimate the association between bedtime and risk of early-onset DM and islet beta cell function, respectively.
Results: Patients with early-onset DM had a later bedtime than those with late-onset DM. Individuals with bedtime ≥ 24:00 had a higher prevalence of early-onset DM than those with bedtime at 22:00– 24:00 and < 22:00 (51.2% vs 29.3% vs 14.3%, respectively, p = 0.028). The multivariate logistic regression showed that per hour later in bedtime was associated with a 52% increased risk of early-onset DM (p = 0.023). Patients with bedtime after 24:00 had a 146% increased risk of early-onset DM compared to those went to bed between 22:00 to 24:00 (OR = 2.46, 95% CI 1.05 to 5.77, p = 0.039). The multiple linear regression showed that bedtime was independently negatively correlated with late-phase insulin secretion (assessed by disposition index, DI120).
Conclusion: Later bedtime was associated with worse late-phase insulin secretion and may be a risk factor for early-onset DM. Proper bedtime to lower risk of early-onset DM deserves further investigation.
Keywords: diabetes mellitus, early-onset, sleep, bedtime, islet beta cell function
Background
The prevalence of diabetes mellitus (DM) has been increasing in recent decades.1 According to a large-scale survey in China, the prevalence of DM rose from 10.9% in 2013 to 12.4% in 2018. Moreover, the median onset age of DM has gradually advanced, from 55.8 years old in 2013 to 51.3 years old in 2018.2 Among them, the proportion of patients with early-onset DM (onset age earlier than 40 years old) has increased from 5.9% in 2013 to 11.5% in 2018.2,3 The earlier the age of onset, the longer and heavier the economic burden on the individual and society, suggesting that early-onset DM is becoming one of the significant health burdens in China. Studies have shown that patients with early-onset DM are characterized by increased insulin resistance (IR) and impaired islet beta cell function compared with patients with late-onset DM.4,5 What’s more, early-onset DM was reported to be associated with an increased risk of development of cardiovascular disease6,7 and progression of diabetic microvascular complications, like diabetic kidney disease8–10 and diabetic retinopathy11 compared to those with late-onset DM.
The development of early-onset type 2 diabetes mellitus (T2DM) is the result of a combination of genetic and multiple environmental factors. Among the many environmental risk factors associated with early-onset T2DM, obesity, sedentary lifestyle, low physical activity, and socioeconomic status have been widely recognized.12 In recent years, studies have reported that sleep disorders are less known risk factors for the development of T2DM. Previous studies on sleep and DM have primarily focused on sleep quality and duration.13–15 For example, a meta-analysis included 10 studies, with a total of 107,756 participants, showed that short sleep duration (≤ 5–6 h) and long sleep duration (> 8–9 h) were both associated with an increased risk of T2DM, with a RR 1.28 (95% CI 1.03–1.60) and 1.48 (95% CI 1.13–1.96), respectively.16 Previous studies have also reported that bedtime is associated with the risk of developing DM,17 abdominal obesity,18 and non-alcoholic fatty liver disease.19,20 However, no studies have explored the correlation between bedtime and the risk of early-onset DM. Besides, it is unknown whether bedtime affects insulin resistance and islet beta cell function, two main mechanisms contributing to the development of T2DM.
To fill this gap, we administered a sleep questionnaire in newly diagnosed, untreated T2DM to investigate the correlation between bedtime and the risk of early-onset T2DM and islet beta cell function.
Methods
Population
The participants were recruited from Mar. 2020 to Dec. 2022 in the Department of Endocrinology, Beijing Shijitan Hospital, Capital Medical University. 138 adult patients aged 18 to 80 with newly diagnosed, treat-naïve T2DM were included in this study (Figure 1). The diagnosis of DM was based on the World Health Organization (WHO) diagnostic criteria, 1999. Those with fasting plasma glucose (FPG) ≥ 7.0 mmol/L or 2-h postprandial plasma glucose (PPG) ≥ 11.1 mmol/L were defined as having DM. The exclusion criteria were as follows: 1) patients already receiving glucose-lowering medication; 2) patients diagnosed with type 1 diabetes, gestational diabetes, or other types of diabetes; 3) patients with severe cardiovascular, hepatic, or kidney disease. The study protocol was approved by the Ethics Committee of Beijing Shijitan Hospital, Capital Medical University (Approval Number: sjtkyll-lx-2021(27)) and was conducted following the Declaration of Helsinki. All patients provided written informed consent to participate in the study.
 |
Figure 1 Flowchart of the study. Abbreviations: DM, diabetes mellitus; T2DM, type 2 diabetes mellitus; yo, years old; OGTT, oral glucose tolerance test; IR, insulin resistance. |
Data Collection
Height and weight measurements were performed after overnight fasting with thin clothes. Body mass index (BMI) was calculated as BMI = weight (kg) / height (m)2. Waist circumference (WC) was measured midway between the iliac crest and the costal margin. Venous blood was collected through the elbow vein from patients who had fasted for at least 10 hours. All the participants underwent a 75-g oral glucose tolerance test (OGTT) after overnight fasting. Venous blood was collected at 0, 30, 60, and 120 min and used to measure plasma glucose (hexokinase method), serum insulin (INS, chemiluminescent enzyme immunoassay), and C peptide (CP, chemiluminescent enzyme immunoassay). Glycosylated hemoglobin (HbA1c) was detected using a high-performance liquid chromatography method (Tosoh HLC-723 G8; Tosoh Bioscience, Inc, Tokyo, Japan). The serum uric acid (UA) and lipid profiles, including total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-c), and low-density lipoprotein cholesterol (LDL-c), were measured using an automatic biochemical analyzer.
Assessment of Insulin Resistance and Islet Beta Cell Function
Homeostasis model assessment of insulin resistance (HOMA–IR) was used to assess IR:  .21 Besides, the Matsuda insulin sensitivity index (ISIM) and Quantitative insulin sensitivity check index (QUICKI) were used to assess whole-body insulin sensitivity and were calculated using the formula as follows:
.21 Besides, the Matsuda insulin sensitivity index (ISIM) and Quantitative insulin sensitivity check index (QUICKI) were used to assess whole-body insulin sensitivity and were calculated using the formula as follows:  ,22
,22  .23 Homeostasis model assessment of beta cell function (HOMA–β) was calculated to assess beta cell function:
.23 Homeostasis model assessment of beta cell function (HOMA–β) was calculated to assess beta cell function:  .21 The insulinogenic index (IGI) was used to assess the early-phase insulin secretion (
.21 The insulinogenic index (IGI) was used to assess the early-phase insulin secretion ( ) and late-phase insulin secretion (
) and late-phase insulin secretion ( ).24 The disposition index (DI), a comprehensive evaluation of insulin secretion and insulin resistance, was measured as
).24 The disposition index (DI), a comprehensive evaluation of insulin secretion and insulin resistance, was measured as  , and
, and  .25
.25
Assessment of Sleep Information
Information on sleep habits, shift work, and chronotype was obtained by a self-reported questionnaire. The Pittsburgh Sleep Quality Index (PSQI) questionnaire was used to assess sleep quality and sleep habits during the past month.26 Bedtime was derived from the question: “During the past month, at what time do you usually go to bed?”. Sleep duration was obtained by asking: “During the past month, how many hours of actual sleep did you get at night (this may differ from the number of hours you spent in bed)?”. The PSQI score was calculated to reflect the patient’s sleep quality. Sleep efficiency was calculated by dividing the actual length of sleep by the interval between waking time and bedtime.
Definition and Grouping
Because of the insidious onset of T2DM and the delay in diagnosis in some patients, the age of onset is not equivalent to the age of diagnosis. Duration of DM is defined as the interval between the diagnosis of DM and the appearance of symptoms. The onset age of DM is calculated by subtracting the duration of DM from the diagnosis age of DM. Early-onset DM was defined as the onset age of DM less than 40 years old, according to previous studies.6,8,27 Thus, patients were grouped into two groups according to the onset age of DM: early-onset DM (onset age < 40 years old) and late-onset DM (onset age ≥ 40 years old). A PSQI score of ≥ 5 is defined as having poor sleep quality. Due to the median of bedtime among the participants was 23:00, the bedtime was divided into 3 groups: early bedtime group (< 22:00), median bedtime group (22:00–24:00), and late bedtime group (≥ 24:00). Sleep duration was categorized into three groups in a similar way: < 5 h, 5–7 h, and ≥ 7 h.
Statistical Analysis
Normality was assessed for all continuous variables. Normally distributed data were expressed as the mean ± SD, and Student’s t-test was used to evaluate differences between groups. Non-normally distributed data were expressed as the median (Q1, Q3), and differences between groups were assessed using the Mann‐Whitney U-test. Categorical variables were expressed as counts/percentiles (%), and Pearson’s χ2‐test was used to compare the difference between groups. Multivariable logistic regression and multiple linear regression analysis with stepwise variable selection procedure were used to assess the association of bedtime with early-onset DM and DI120 (ln transformed), respectively. Statistically significant variables (p < 0.1) from the univariate logistic regression analyses were included in the multiple logistic regression analysis. All statistical analyses were performed using IBM SPSS Statistics 23.0 (IBM Corp., Armonk, NY, USA). A p-value < 0.05 was considered significant.
Results
Basic Characteristics of Patients Grouped by Onset Age of DM
The average age of patients with newly diagnosed, untreated T2DM in this study was 48 years old. The median duration of DM was 10 months, with an average onset age of DM 41 years old, among which 54 (39.1%) patients were early-onset DM. Patients with early-onset DM were heavier and had larger WC than those with late-onset DM. The proportion of obesity and family history of DM was significantly higher in patients with early-onset DM than in those with late-onset DM. The two groups had no significant differences in plasma glucose, IR, or islet beta cell function. HbA1c was relatively higher in patients with early-onset DM, but there were no statistically significant differences (Table 1). Early-onset diabetic patients had a later bedtime compared to those with late-onset DM. Yet, there were no statistically significant differences in sleep duration, sleep efficiency or sleep quality between the two groups. More than half of the patients went to bed between 22:00 and 24:00, and the proportion of patients who went to bed after 24:00 was significantly higher in early-onset DM than in late-onset DM. Besides, early-onset diabetic patients tend to have an evening chronotype (Table 2).
 |
Table 1 Basic Characteristics of Patients with Different Onset-Age of DM |
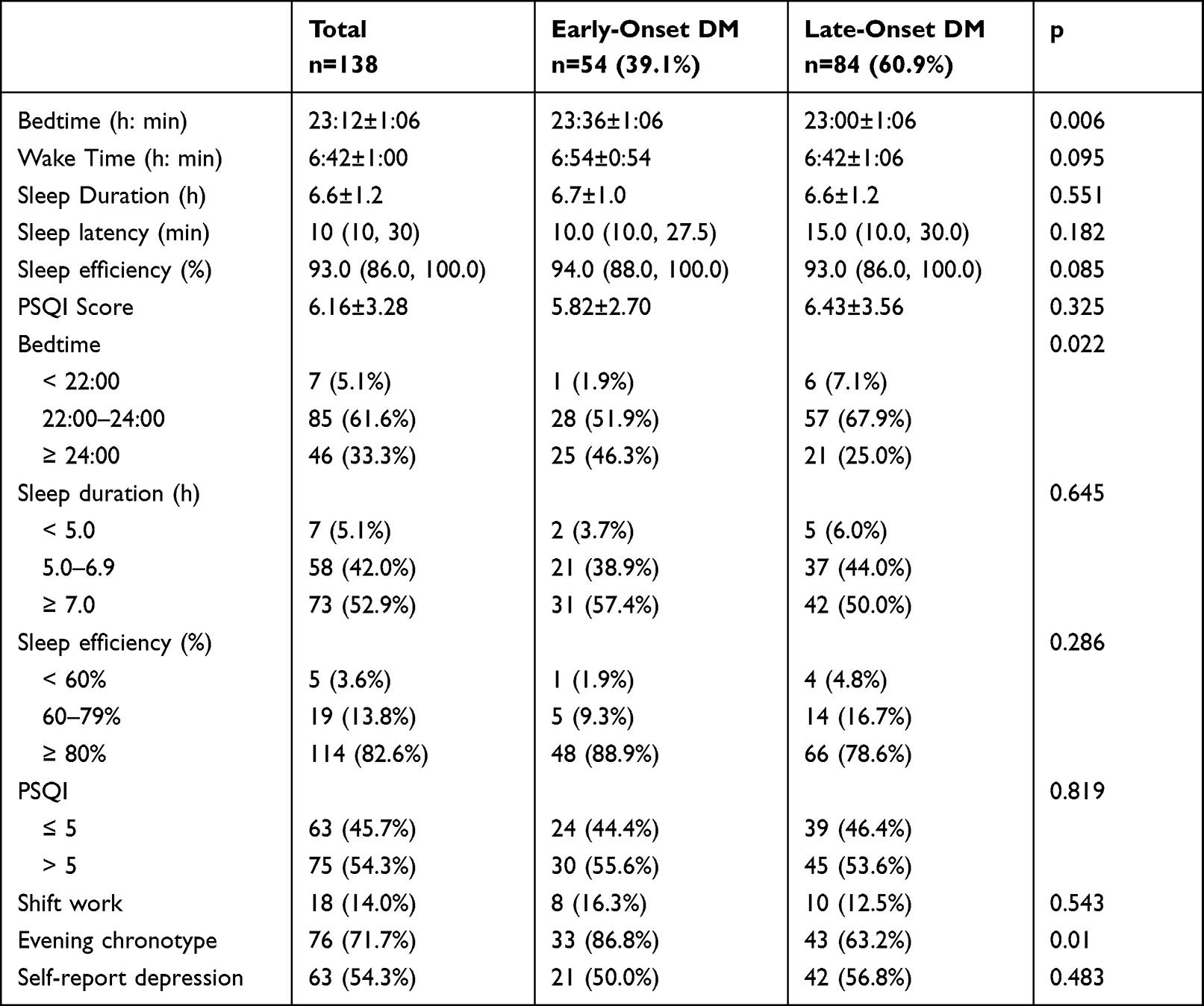 |
Table 2 Comparison of Sleep in Patients with Early-Onset or Late-Onset DM |
Comparison of Characteristics Among Patients with Different Bedtime
The average bedtime was 23:12, with 61.6% of patients going to bed between 22:00 and 24:00. The later the bedtime, the younger the patient, and the earlier the onset age of DM. More than half of the patients who went to bed after 24:00 had early-onset DM, a much higher proportion than those who went to bed before 24:00. BMI was similar among the three groups, but WC was significantly higher in those who went to bed after 24:00 than the other two groups. Although glycemic control did not differ significantly among the three groups, the 2hCP, 2hINS, IGI120 and DI120 were significantly lower in patients with a bedtime more than 24:00 compared to those in the other two groups. In addition, those who went to bed after 24:00 had higher TG and lower HDL-c levels (Table 3).
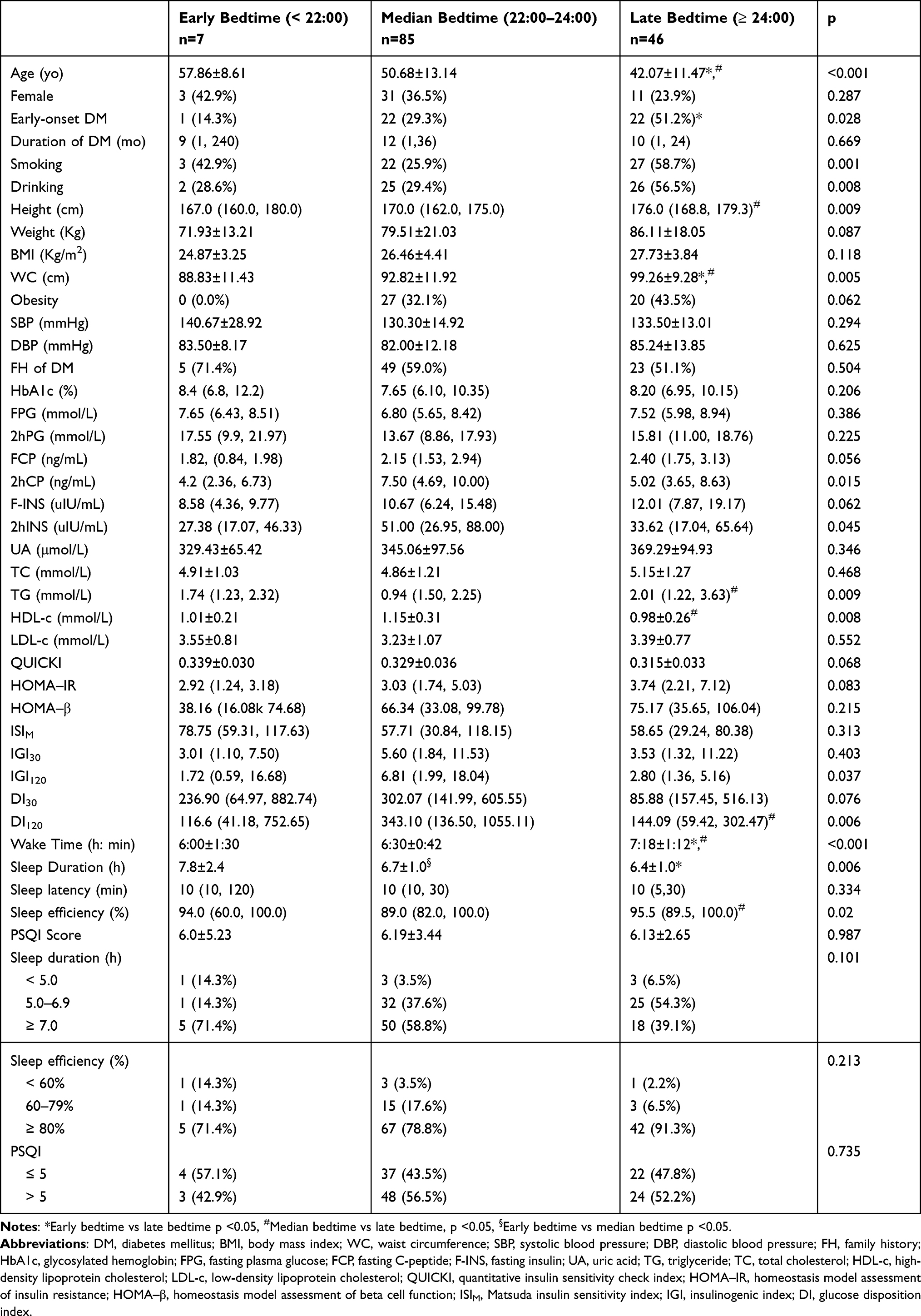 |
Table 3 Clinical and Sleep-Related Characteristics in Patients with Different Bedtime |
Correlation of Bedtime with Early-Onset DM and Islet Beta Cell Function
The logistic regression analysis showed that family history of DM and bedtime were associated with early-onset DM independently of gender, BMI, smoking, alcohol consumption, duration of DM, FPG, UA, lipids, and other sleep measures. Each one hour later in bedtime was associated with a 52% increase in the risk of early-onset DM (OR = 1.52, 95% CI 1.06, 2.17, p = 0.023). When bedtime was included as a categorical variable in the regression model, patients who went to bed after 24:00 had a 1.46-fold increased risk of developing early-onset DM compared to those who went to bed between 22:00 and 24:00 (Table 4). Multiple linear regression analysis showed that bedtime, FPG, and UA were independent risk factors associated with DI120 after correcting for confounding factors (Table 5).
 |
Table 4 Association of Bedtime with Early-Onset DM |
 |
Table 5 The Multiple Linear Regression of LnDI120 |
Discussion
Early-onset DM accounted for 39.1% of the participants in this study, which was higher than the proportion reported in previous studies.12 In this study, early-onset diabetic patients had a higher proportion of overweight and obesity and family history of DM than those with late-onset DM. However, there were no significant differences in diabetic duration, glycemic control, and islet beta cell function between patients with early-onset and late-onset DM. Despite no significant differences in sleep quality, duration, and efficiency, patients with early-onset DM had a later bedtime than those with late-onset DM. Grouping by bedtime showed that patients with a bedtime after 24:00 had a higher ratio of a smoker, drinker, early-onset DM, and greater WC despite similar BMI. In addition, the 2hCP, 2hINS, IGI120, and DI120 were significantly lower in the late bedtime group than in the early bedtime group. Further regression analysis showed that late bedtime was an independent risk factor for early-onset DM and worse late-phase insulin secretion, even adjusting for confounding factors, including sleep duration and other sleep habits.
Previous studies have reported that patients with early-onset DM have poorer glycemic control, more severe IR, and poorer insulin secretion function than patients with late-onset DM.4,12 However, no significant differences were observed in this study between early-onset and late-onset DM regarding glycemic control, IR, and islet beta cell function. A possible explanation is that there was no significant difference in the duration of DM between early-onset DM and late-onset DM in this study, based on the fact that all patients included in this study were newly diagnosed untreated diabetic patients. The duration of DM is essential because the poorer islet beta cell function and higher risk of CVD and chronic complications in patients with early-onset DM largely depend on the longer duration of DM, as reported in previous studies.6,11,27
In this study, patients with early-onset DM have a significantly later bedtime and a higher proportion of evening chronotype than those with late-onset DM. Regression analysis showed that late bedtime was independently associated with early-onset DM, suggesting that late bedtime might be an independent risk factor for early-onset DM. Previous studies have reported that late bedtime increases the risk of DM, but no studies have explored the impact of bedtime on the development of early-onset DM. To our knowledge, this is the first report that bedtime is associated with the prevalence of early-onset DM. This study showed that the risk of early-onset DM increased by 52% for each 1-h increase in bedtime. The risk of early-onset DM increased 1.46-fold in patients whose bedtime was after 24:00 compared with those between 22:00–24:00. More than one study has reported that sleep duration is associated with the incidence of DM and that either short or long sleep duration increases the risk of DM.13,28 In the present study, patients with late bedtime tended to wake up later but slept for a shorter duration. However, we did not detect significant associations between sleep duration and early-onset DM. After correcting for sleep efficiency, late bedtime was still significantly associated with increased risk of early-onset DM, suggesting that bedtime might be a risk factor for prevalence of early-onset DM independent of other sleep characteristics and confounding factors.
Possible reasons for the increased risk of early-onset DM in individuals with late bedtime include shorter sleep duration, less activity, increased calorie intake, more weight gain, more prolonged light exposure, and hormonal disruption, such as less melatonin secretion.29–32 In addition, in the current study, we explored the effect of bedtime on insulin secretory function. It turned out that patients who went to bed after 24:00 had lower IGI120 and DI120 than those who went to bed between 22:00 and 24:00, suggesting an impaired late-phase insulin secretion in patients with late bedtime. Regression analysis showed that bedtime was an independent risk factor associated with DI120 after correcting for other confounding factors. Thus, we speculate that late bedtime may increase the risk of early-onset DM by impairing late-phase insulin secretion, which has not been reported before. Therefore, we have reason to believe that improving the sleep habit by going to bed earlier may help to delay the impaired insulin secretion function in the late phase, which in turn may help to delay the occurrence of early-onset DM. Future studies are needed to confirm this speculation further.
Limitations and disadvantages: This cross-sectional study can only infer the correlation but cannot determine the causal relationship. Besides, bedtime and other sleep habits were self-reported; thus, recall bias might be inevitable. Therefore, prospective cohort studies with objective methods to assess sleep are needed to explore the influence of bedtime on the onset age of DM and islet beta cell function. In addition, the sample size of this study was relatively small. Thus, future studies with larger sample sizes are needed to validate the results of this study.
In general, patients with early-onset DM tend to go to bed late. Meanwhile, patients with late bedtime have poorer late-phase insulin secretion and a higher proportion of early-onset DM. Regression analysis showed that later bedtime is correlated with worse late-phase insulin secretion and increased risk of early-onset DM. Therefore, we have reason to believe that going to bed early might be a potentially effective strategy to prevent the development of early-onset DM by delaying the impairment of late-phase insulin secretion. Further research is needed to confirm the speculation and explore the specific mechanisms in the future.
Data Sharing Statement
The datasets used and analyzed in the current study are available from the corresponding author upon reasonable request.
Acknowledgment
Thank all the authors and patients who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Project of Science and Technology Research and Development of China Railway Corporation (No. J2021Z608).
Disclosure
All the authors declare no conflict of interest.
References
1. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
2. Wang L, Peng W, Zhao Z, et al. Prevalence and treatment of diabetes in China, 2013–2018. JAMA. 2021;326(24):2498–2506. doi:10.1001/jama.2021.22208
3. Wang L, Gao P, Zhang M, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA. 2017;317(24):2515–2523. doi:10.1001/jama.2017.7596
4. Zou X, Zhou X, Ji L, et al. The characteristics of newly diagnosed adult early-onset diabetes: a population-based cross-sectional study. Sci Rep. 2017;7(1):46534. doi:10.1038/srep46534
5. Zhou S, Meng X, Wang S, et al. A 3-year follow-up study of β-cell function in patients with early-onset type 2 diabetes. Exp Ther Med. 2016;12(2):1097–1102. doi:10.3892/etm.2016.3394
6. Huo X, Gao L, Guo L, et al. Risk of non-fatal cardiovascular diseases in early-onset versus late-onset type 2 diabetes in China: a cross-sectional study. Lancet Diabetes Endocrinol. 2016;4(2):115–124. doi:10.1016/S2213-8587(15)00508-2
7. Yen F-S, Lo Y-R, Hwu C-M, Hsu -C-C. Early-onset type 2 diabetes <60 years and risk of vascular complications. Diabetes Res Clin Pract. 2021;182:109129. doi:10.1016/j.diabres.2021.109129
8. Wu Y, Wang Y, Zhang J, et al. Early-onset of type 2 diabetes mellitus is a risk factor for diabetic nephropathy progression: a biopsy-based study. Aging. 2021;13(6):8146–8154. doi:10.18632/aging.202624
9. Liu -J-J, Liu S, Gurung RL, et al. Risk of progressive chronic kidney disease in individuals with early-onset type 2 diabetes: a prospective cohort study. Nephrol Dial Transplant. 2018. doi:10.1093/ndt/gfy211
10. Zheng L, Chen X, Luo T, et al. Early-onset type 2 diabetes as a risk factor for end-stage renal disease in patients with diabetic kidney disease. Prev Chronic Dis. 2020;17:E50. doi:10.5888/pcd17.200076
11. Song SH, Gray TA. Early-onset type 2 diabetes: high risk for premature diabetic retinopathy. Diabetes Res Clin Pract. 2011;94(2):207–211. doi:10.1016/j.diabres.2011.07.030
12. Pan J, Jia W. Early-onset diabetes: an epidemic in China. Front Med. 2018;12(6):624–633. doi:10.1007/s11684-018-0669-1
13. Gottlieb DJ, Punjabi NM, Newman AB, et al. Association of sleep time with diabetes mellitus and impaired glucose tolerance. Arch Intern Med. 2005;165(8):863–867. doi:10.1001/archinte.165.8.863
14. Mokhlesi B, Temple KA, Tjaden AH, et al. Association of self-reported sleep and circadian measures with glycemia in adults with prediabetes or recently diagnosed untreated type 2 diabetes. Diabetes Care. 2019;42(7):1326–1332. doi:10.2337/dc19-0298
15. Yang Y, Zhao L, Li D, et al. Association of sleep quality with glycemic variability assessed by flash glucose monitoring in patients with type 2 diabetes. Diabetol Metab Syndr. 2021;13(1):102. doi:10.1186/s13098-021-00720-w
16. Cappuccio FP, D’Elia L, Strazzullo P, Miller MA. Quantity and quality of sleep and incidence of type 2 diabetes: a systematic review and meta-analysis. Diabetes Care. 2010;33. doi:10.2337/dc09-1124
17. Yan B, Fan Y, Zhao B, et al. Association between late bedtime and diabetes mellitus: a Large Community-Based Study. J Clin Sleep Med. 2019;15:1621–1627. doi:10.5664/jcsm.8026
18. Liu M, Cao B, Luo Q, et al. Associations between sleep duration, wake-up time, bedtime, and abdominal obesity: results from 9559 Chinese children aged 7–18 years. Front Endocrinol. 2021;12:735952. doi:10.3389/fendo.2021.735952
19. Hu C, Zhang Y, Wang S, et al. Association of bedtime with the risk of non‐alcoholic fatty liver disease among middle‐aged and elderly Chinese adults with pre‐diabetes and diabetes. Diabetes Metab Res Rev. 2020;36:e3322. doi:10.1002/dmrr.3322
20. Wang H, Gu Y, Zheng L, et al. Association between bedtime and the prevalence of newly diagnosed non-alcoholic fatty liver disease in adults. Liver Int. 2018;38(12):2277–2286. doi:10.1111/liv.13896
21. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412–419. doi:10.1007/BF00280883
22. Matsuda M, DeFronzo RA. Insulin sensitivity indices obtained from oral glucose tolerance testing: comparison with the euglycemic insulin clamp. Diabetes Care. 1999;22(9):1462–1470. doi:10.2337/diacare.22.9.1462
23. Katz A, Nambi SS, Mather K, et al. Quantitative insulin sensitivity check index: a simple, accurate method for assessing insulin sensitivity in humans. J Clin Endocrinol Metab. 2000;85(7):2402–2410. doi:10.1210/jcem.85.7.6661
24. Haffner SM, Miettinen H, Gaskill SP, Stern MP. Decreased insulin secretion and increased insulin resistance are independently related to the 7-year risk of NIDDM in Mexican-Americans. Diabetes. 1995;44(12):1386–1391. doi:10.2337/diab.44.12.1386
25. Abdul-Ghani MA, Williams K, DeFronzo RA, Stern M. What is the best predictor of future type 2 diabetes? Diabetes Care. 2007;30(6):1544–1548. doi:10.2337/dc06-1331
26. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
27. Cho Y, Park H-S, Huh BW, et al. Prevalence and risk of diabetic complications in young-onset versus late-onset type 2 diabetes mellitus. Diabetes Metab. 2022;48(6):101389. doi:10.1016/j.diabet.2022.101389
28. Buxton OM, Marcelli E. Short and long sleep are positively associated with obesity, diabetes, hypertension, and cardiovascular disease among adults in the United States. Soc Sci Med. 2010;71(5):1027–1036. doi:10.1016/j.socscimed.2010.05.041
29. Shechter A, St-Onge M-P. Delayed sleep timing is associated with low levels of free-living physical activity in normal sleeping adults. Sleep Med. 2014;15(12):1586–1589. doi:10.1016/j.sleep.2014.07.010
30. Olds TS, Maher CA, Matricciani L. Sleep duration or bedtime? Exploring the relationship between sleep habits and weight status and activity patterns. Sleep. 2011;34(10):1299–1307. doi:10.5665/SLEEP.1266
31. Baron KG, Reid KJ, Kern AS, Zee PC. Role of sleep timing in caloric intake and BMI. Obesity. 2011;19(7):1374–1381. doi:10.1038/oby.2011.100
32. Park Y-MM, White AJ, Jackson CL, Weinberg CR, Sandler DP. Association of exposure to artificial light at night while sleeping with risk of obesity in women. JAMA Intern Med. 2019;179(8):1061–1071. doi:10.1001/jamainternmed.2019.0571
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.