Back to Journals » International Journal of General Medicine » Volume 16
Association of Apolipoprotein E Gene Polymorphism with Type 2 Diabetic Nephropathy in the Southern Chinese Population
Authors Gan C, Zhang Y, Zhang X, Huang Q, Guo X
Received 13 September 2023
Accepted for publication 12 November 2023
Published 24 November 2023 Volume 2023:16 Pages 5549—5558
DOI https://doi.org/10.2147/IJGM.S440103
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Caiyan Gan,1– 3 Yinmei Zhang,1– 3 Xianyan Zhang,4 Qionghui Huang,1– 3 Xuemin Guo1– 4
1Research Experimental Center, Meizhou People’s Hospital, Meizhou, People’s Republic of China; 2Guangdong Engineering Technological Research Center of Clinical Molecular Diagnosis and Antibody Drugs, Meizhou, People’s Republic of China; 3Guangdong Provincial Engineering and Technological Research Center for Molecular Diagnostics of Cardiovascular Diseases, Meizhou, People’s Republic of China; 4Clinical Laboratory Center, Meizhou People’s Hospital, Meizhou, People’s Republic of China
Correspondence: Xuemin Guo, Research Experimental Center, Meizhou People’s Hospital, 63 Huangtang Road, Meijiang District, Meizhou, 514031, People’s Republic of China, Email [email protected]
Background: Common polymorphisms within the apolipoprotein E (APOE) gene are rs429358 and rs7412, which result in three major alleles (ɛ2, ɛ3, and ɛ4) and six genotypes (E2/E2, E2/E3, E3/E3, E3/E4, E4/E4, and E2/E4). Although APOE gene polymorphisms have been suggested to be associated with the development of diabetic nephropathy (DN), their potential association remains unclear in different regions. This study aims to unveil the genetic effects of APOE gene polymorphisms on DN susceptibility and serum lipid profiles in southern Chinese population.
Methods: A total of 306 DN patients and 483 type 2 diabetic patients as controls were included in the study. The APOE gene polymorphisms were analyzed by polymerase chain reaction (PCR) microarray gene chip. Relevant medical records and information of these participants were collected.
Results: There were statistically significant differences (p < 0.05) in gender, SBP, hypertension, hyperuricemia, UTP, TG and HDL-C between DN patients and controls. DN patients exhibited a higher frequency of the ϵ2 allele and E2/E3 genotype than controls (p < 0.001). Logistic regression analysis indicated that the ϵ2 allele and E2/E3 genotype were independent risk factors (adjusted OR: 3.237, 95% CI: 1.789– 5.854, p < 0.001; adjusted OR: 3.453, 95% CI: 1.873– 6.368, p < 0.001), while the ϵ3 allele or E3/E3 genotype might serve as protective role (adjusted OR: 0.395, 95% CI: 0.255– 0.612, p < 0.001) for development of DN.
Conclusion: Our study indicates a correlation between APOE polymorphisms and DN in the southern Chinese Hakka population. Specifically, individuals carrying the APOE ϵ2 allele and E2/E3 genotype are at a higher risk of developing DN. Conversely, those with the APOE ϵ3 allele and E3/E3 genotype have a lower risk of DN in southern Chinese population.
Keywords: Apolipoprotein E, diabetic nephropathy, gene polymorphism, southern China
Introduction
Diabetic nephropathy (DN) is one of the major complication of type 2 diabetes mellitus (T2DM) and the leading cause of end-stage renal disease (ESRD) or chronic kidney disease (CKD).1–4 It is estimated that around 40% of individuals with diabetes will develop DN.5 By 2030, the projected incidence of ESRD in the United States is estimated to be between 971,000 and 1,259,000 cases.6 In Europe, approximately 50% of new diabetic patients requiring dialysis treatment are due to DN.7 In China, the prevalence and incidence of DN have also increased dramatically over the past decade, affecting approximately 150.5 million individuals.8 DN is characterized by the presence of mass proteinuria, hypertension, renal failure, and persistent albuminuria (> 300 mg/24 hours).9 Risk factors for DN include race, systemic hypertension, age, hyperglycemia, male gender, smoking, dyslipidemia and genetic factors.10–12 DN not only leads to kidney impairment but has also been associated with an increased risk of atrial fibrillation (AF), colorectum cancer, liver cancer, larynx cancer and mitochondrial dysfunction.13–17 Diabetic dyslipidemia is characterized by elevated levels of triglycerides, LDL-cholesterol, low levels of HDL-cholesterol, and an abundance of small dense LDL particles.18–20 Although the pathogenesis of DN is complex and not yet fully understood, previous studies have identified a correlation between DN and various proteins involved in lipid metabolism.21–23 Dyslipidemia contributes to the deposition of lipids in the kidney, leading to inflammation, lipotoxicity, podocyte dysfunction, and fibrosis, ultimately resulting in the development of DN.24 These lipid alterations or abnormalities in lipoproteins increase the risk of nephropathy in individuals with diabetes.25,26 Apolipoproteins play a crucial role in lipid metabolism by interacting with plasma lipids to form lipoproteins, which are soluble lipid-protein complexes. Apolipoprotein E (APOE) is a polymorphic glycoprotein that plays a key role in dyslipidemia.27,28 APOE accomplishes its lipid metabolism mainly through binding to LDL receptors and mediating the removal of chylomicron remnants and VLDL from serum. Both VLDL and chylomicron particles become enriched in APOE as they circulate through the capillaries and are lipolyzed on the surface of endothelial cells by lipoprotein lipase. This enzyme hydrolyzes triglycerides, releasing fatty acids that serve as energy sources for cell utilization. In this manner, APOE plays a crucial role in directing the metabolism of both endogenous triglycerides and VLDL and dietary triglycerides and chylomicrons.29 It accomplishes this by delivering these lipids either to extrahepatic cells (via VLDL and their remnants) or to the liver (via chylomicron remnants). In the liver, dietary fatty acids can be metabolized or resecreted as triglycerides with VLDL, while cholesterol is eliminated through the bile. In this context, APOE exhibits an “endocrine-like” functionality. Additionally, it can redistribute lipids among various cells within a tissue, thereby fulfilling a “paracrine-like” role in lipid transport and delivery.30
APOE is a protein encoded by the APOE gene. The human APOE gene consists of 3597 nucleotides located on chromosome 19q13.2, which is a 34 kD protein with 4 exons and 3 introns. The APOE gene has three different alleles (ε2, ε3, ε4) which give rise to six genotypes (E3/E3, E3/E4, E2/E2, E2/E3, E2/E4 and E4/E4).30 These genotypes are determined by two common single nucleotide polymorphisms (SNPs), namely rs429358 and rs7412. The APOE alleles are associated with specific amino acids at positions 112 (rs429358) and 158 (rs7412): ε2 has cysteine at both positions (cysteine/cysteine), ε4 has arginine at both positions (arginine/arginine), and ε3 has cysteine at position 112 and arginine at position 158 (cysteine/arginine), which is considered the wild type.31,32 Moreover, the APOE alleles are known to be related to lipoprotein metabolism. Compared to the ε3 allele, carriers of the ε2 have been associated with lower low-density lipoprotein cholesterol (LDL-C) and total cholesterol (TC) levels, while ε4 carriers have been associated with higher levels of LDL-C, TC and triglycerides (TG).33 Studies have shown that the most common genotype is E3/E3, and the ε3 allele is the most frequent allele in most population.34–36 In the Hakka population of southern China, the frequencies of ε3 allele, and E3/E3 genotype are approximately 80%, and 65%, respectively.37 The APOE polymorphisms have been reported to be associated with DN. Previous studies have demonstrated that the ε2 allele is a genetic risk factor for DN in patients with T2DM.38,39
Studies showed that racial and ethnic differences exist in the prevalence of DN.40 However, the relationship between APOE polymorphisms and DN has yielded inconsistent results.41 Furthermore, there is currently no published information regarding the association between APOE polymorphism and the risk of DN in southern China. Therefore, the present study was to investigate the potential role of APOE gene polymorphism in relation to the risk of DN in Hakka ethnic group in southern China. It is hypothesized that the APOE gene polymorphism may influence the development of DN by affecting the lipid profiles. The findings of this study may contribute to the identification of genetic factors associated with the development of DN.
Methods
Subjects
A total of 789 patients with T2DM were recruited from the inpatients of Meizhou People’s Hospital (Huangtang Hospital), from May 2016 to July 2020. The study included 306 patients with diabetic nephropathy (DN) and 483 T2DM patients without nephropathy as controls. Patients with cardiovascular and cerebrovascular diseases, malignant tumors, benign tumors, type 1 diabetes mellitus (T1DM) and patients under 18 years of age were excluded. The data collected for the participants included APOE genotyping, age, gender, history of smoking, blood pressure, lipid profile, alcohol intake, hypertension, hyperuricemia, dyslipidemia, fatty liver and risk factors for DN. Hypertension was defined as blood pressure SBP/DBP level ≥ 140/90 mmHg or current antihypertensive therapy. Hyperuricemia was defined as the level of uric acid (UA) ≥ 420 mmol/L in men and ≥ 360 mmol/L in women. Dyslipidemia was defined as any one of the following conditions of serum lipid profile: serum level of total cholesterol (TC) > 5.5 mmol/L, triglycerides (TG) > 1.7 mmol/L, LDL-cholesterol (LDL-C) > 3.1 mmol/L, and high-density lipoprotein-cholesterol (HDL-C) < 0.88 mmol/L. The fatty liver diagnosis according to the guideline of the American Association for the Study of Liver Diseases (AASLD).42 DN was diagnosed by the professional clinician based on clinical manifestations, complications, history, examinations, imaging, and pathology.43 T2DM was confirmed according to the American Diabetes Association’s 2013 standards.44 The main causes of this disease are relatively low insulin secretion and insulin resistance.45,46
Ethics approval was obtained from the Human Ethics Committee of Meizhou People’s Hospital (NO: 2021-C-111). The study was in Accordance with the 1975 Declaration of Helsinki. All participants gave written informed consent to participate in the study.
DNA Extraction and Genotyping
A 2 mL venous blood sample was collected from each participant into an ethylene diamine tetraacetic acid (EDTA) sample tube. Genomic DNA was extracted from whole blood using a Blood DNA Isolation Kit (Tiangen Biotech, Guangdong, China) following the manufacturer’s protocol. The quality and concentration of the DNA were assessed using a Nano-Drop 2000™ spectrophotometer (ThermoFisher Scientific, Waltham, MA, USA). APOE genotyping was performed using the TaqMan probe fluorescent polymerase chain reaction (PCR) gene chip method. The PCR primer sequences were 5’-GCTTGGCACGGCTGTCCAAGGA-3’ (forward primer) and 5’-ATTCGCCCCGGCCTGGTACAC-3’ (reverse primer). Protocol for PCR was performed as the following program: 50 °C for 2 min, initial denaturation at 95 °C for 15 min, denaturation at 94 °C for 30s (amplification of 45 cycles), annealing, and extension at 65 °C for 45s. The PCR product was subsequently dispensed into a specific hybridization reaction chamber. The genotype was detected using an APOE gene chip assay kit (Zhuhai Sinochips Bioscience Co., Ltd., Guangdong, China) according to the manufacturer’s protocol. For the quality control, blank control, positive control, and negative control were included in all the APOE gene SNPs that were analyzed and Sanger sequencing was also randomly performed by duplicate analysis of 10% samples.
Biochemical Measurements
Approximately 3 mL of fasting blood was collected from all participants in the morning after an overnight fast of 8–12 hours. The serum lipid levels of TC, TG, LDL-C, HDL-C were examined by Olympus AU5400 analyzer (Olympus Corporation, Tokyo, Japan). The concentration of HbA1c was measured by Premier Hb9210 HbA1c Analytical Column (Trinity Biotech, Wicklow, Ireland).
Statistical Analysis
The statistical analysis of the data was conducted using SPSS version 22.0 (IBM Inc., State of New York, USA). Kolmogorov–Smirnov test was examined to evaluate data normality. Continuous variables were presented as median (interquartile) or means ± standard deviation (SD) and analyzed using the Mann–Whitney U-test or Student’s t-test. Categorical variables were presented as numbers and frequency and analyzed using the Chi-square test or Fisher’s exact test.47 The Hardy-Weinberg equilibrium of the APOE allele and genotype was assessed using the Chi-square test. Logistic regression analysis was performed to evaluate the association between APOE genotypes and the risk factors for DN with the adjusted odds ratio (OR). p < 0.05 was considered statistically significant.
Results
Clinical Characteristics of Participants
The clinical characteristics of all T2DM participants in the study are presented in Table 1. The study included a total of 789 T2DM patients, with 306 individuals in the DN group (181 males and 125 females) and 483 individuals without DN (247 males and 236 females) serving as controls. The average age of the DN patients was 60.85 ± 11.35 years, while the controls had an average age of 58.83 ± 12.09 years. The DN group had a higher percentage of hypertension (46.1% vs 26.5%, p < 0.001), and Hyperuricemia (12.7% vs 3.3%, p < 0.001). The levels of SBP, UTP, and TG were significantly higher in the DN patients (p < 0.05), while the level of HDL-C was lower in the DN group (p < 0.01) compared to the control group. Additionally, there were no statistically significant differences in age, DBP, smoking, drinking, dyslipidemia, fatty liver, HbA1c, TC, and LDL-C between the two groups.
 |
Table 1 Characteristic and Laboratory Features of DN Patients and Controls |
Distribution of APOE Genotype and Allele Frequencies
The distributions of APOE genotypes and alleles in the DN and control group are listed in Table 2. The genotype and allele distribution of DN group and control group were consistent with the Hardy-Weinberg equilibrium (χ2 = 0.555, p = 0.968 and χ2 = 7.964, p = 0.093, respectively). In this study, the percentages of APOE E2/E2, E2/E3, E2/E4, E3/E3, E3/E4, and E4/E4 genotype were 0.89%, 11.16%, 2.03%, 70.34%, 14.20%, and 0.89% in all subjects, respectively. The ɛ3 allele exhibited the highest frequency, with the E3/E3 genotype being the most prevalent in our study population. Compared to the control group, the frequency of E3/E3 (63.07% vs 74.95%, p < 0.001) and ε3 (79.25% vs 85.82%, p = 0.001) were significantly decreased in the DN group, while those of the E2/E3 (19.28% vs 6.83%, p < 0.001) and ε2 (12.25% vs 4.87%, p < 0.001) were significantly increased in the DN group. Moreover, there were no statistically significant differences in the other genotypes (E2/E2, E2/E4, E3/E4, and E4/E4) or the ɛ4 allele of the APOE gene between the DN patients and the controls (all p > 0.05) (Table 2).
 |
Table 2 Genotype Distributions and Allele Frequencies in DN Patients and Controls |
Relationships Between APOE Allele and Serum Lipid Profiles
The differences in serum lipid profile levels associated with the APOE alleles (ε2, ε3 and ε4) and DN were presented in Table 3. Patients carrying the E2/E4 genotype (n = 16) were excluded due to the opposing roles in lipid metabolism by ε2 and ε4 alleles.48 The subjects were divided into three subgroups: ε2 (E2/E2 and E2/E3), ε3 (E3/E3) and ε4 (E3/E4 and E4/E4). The results showed that the serum TG levels were higher in the ε2 carrier DN group compared to the ε2 carrier control group (p < 0.001) and there was a lower level of HDL-C (p < 0.001). Similarly, the ε3 carrier DN patients exhibited higher TG levels (p < 0.01). Additionally, the TC, TG, LDL-C and HDL-C concentrations in the ε4 carrier control participants showed a trend towards higher levels compared to the DN group (all p > 0.05). We also analyzed the HbA1c and UTP between DN patients and controls in different subgroups. It was observed that DN patients presented significantly higher level of UTP (p < 0.001) in all subgroups.
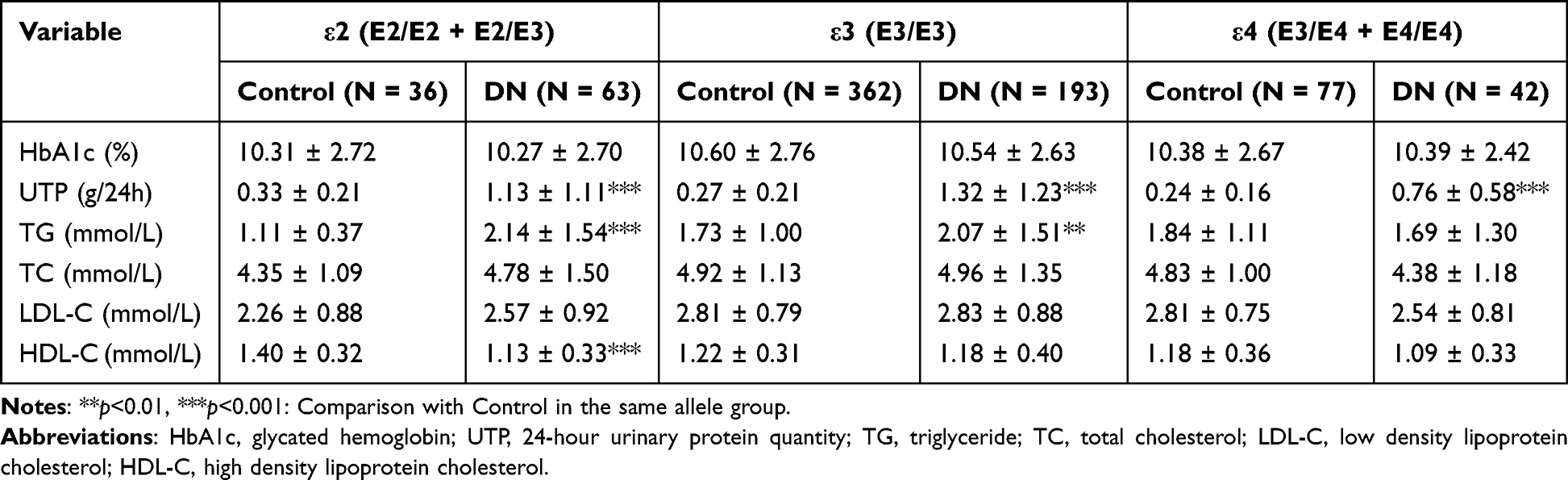 |
Table 3 Relationship Between Serum Lipid-Lipoprotein Levels and ApoE Phenotype in DN Patients and Controls |
Logistic Regression Analysis of the Risk of DN
Logistic regression analysis was used to evaluate the predicting value of APOE genotype and allele for DN. Adjusting the traditional factors including gender, SBP, hypertension, hyperuricemia, TG, HDL-C, and UTP. The results indicated that E2/E3 genotype and ε2 allele were risk factors for DN (adjusted OR: 3.453, 95% CI: 1.873–6.368, p < 0.001; adjusted OR: 3.237, 95% CI: 1.789–5.854, p < 0.001, respectively), whereas the E3/E3 genotype and ε3 allele were protective factors for DN (adjusted OR: 0.395, 95% CI: 0.255–0.612, p < 0.001; adjusted OR: 0.395, 95% CI: 0.255–0.612, p < 0.001, respectively) (Table 4). Previous clinical studies investigating the relationship between APOE gene polymorphisms and DN are summarized in Table 5. The association between APOE gene polymorphisms and DN varied across different regions. In the present study, we observed that the APOE E2/E3 genotype and ε2 allele served as independent risk factors for DN, while the E3/E3 genotype and ε3 allele acted as protective factors in the development of DN among the southern Chinese population.
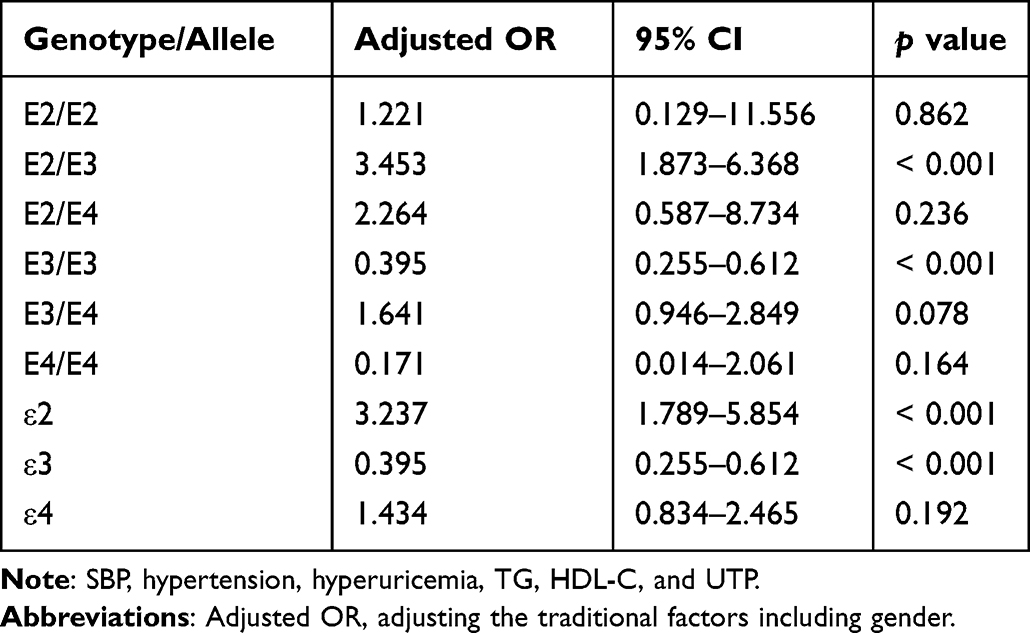 |
Table 4 Logistic Regression Analysis of Risk Factors for DN |
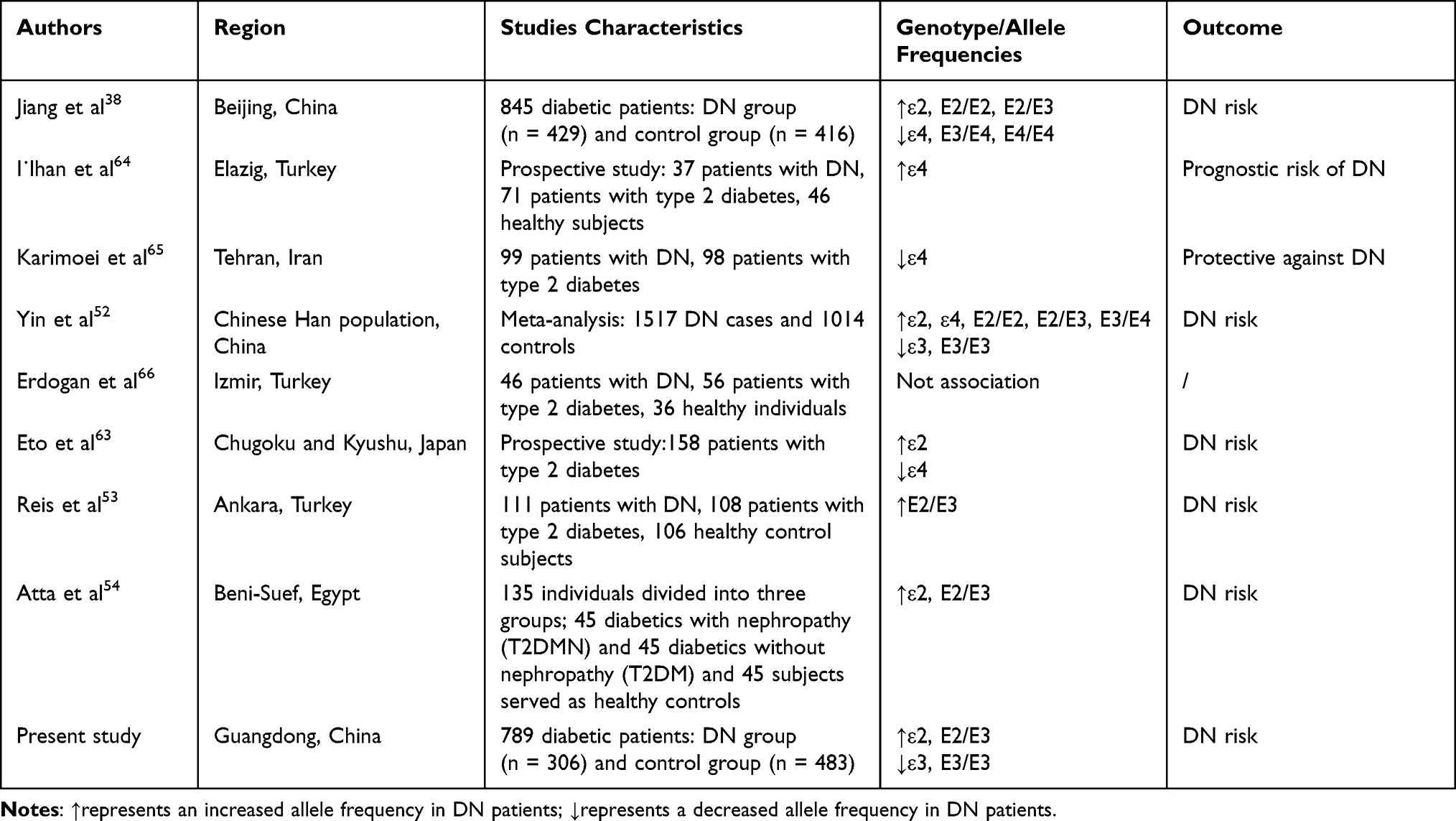 |
Table 5 Studies of ApoE Polymorphism on DN in Humans |
Discussion
DN is a major complication of T2DM.49,50 Accompanied with the global rise in prevalence of T2DM, DN has now become the most common cause of ESRD.2 Dyslipidemia has been associated with an increased risk of DN. APOE gene polymorphism has been related to the serum lipid levels.51 Previous studies have investigated the relationship between APOE gene polymorphism and DN in diverse populations. In the present study, we identified the relationship between APOE gene polymorphism and DN, as well as their impact on serum lipid profiles in southern Chinese population. Our study revealed that E2/E3 genotype and ε2 allele were independent risk factors for DN, while the E3/E3 genotype and ε3 allele were protective factors, consistent with the previous research.38,52–54 APOE gene polymorphism significantly influenced serum lipid profiles in DN patients.
APOE is a crucial plasma protein primarily synthesized, secreted, and metabolized by the liver, and it was synthesized in many other organs, including adrenal gland and kidney. Interestingly, APOE expression in kidney cortex is relatively greater amounts than that in kidney medulla.55,56 It is involved in regulating lipid metabolism, transport and storage.30 APOE gene has two single nucleotide polymorphisms (SNPs) rs7412 (Arg158Cys) and rs429358 (Cys112Arg), resulting in three alleles and six genotypes. Studies have demonstrated that individuals carrying the ε2 allele have lower levels of TC and LDL-C, while those carrying the ε4 allele exhibit the opposite effect due to its affinity with the LDL receptor.57 Previous studies have reported that the APOE gene is a genetic risk factor for Alzheimer’s disease (AD), atherosclerosis (AS), hypertension, T2DM, cancer, nonalcoholic fatty liver disease (NAFLD), cardiovascular and cerebrovascular disease.47,58–62 APOE gene polymorphism also has been associated with DN.63 However, the exact impact of APOE polymorphisms on the risk of DN is yet to be fully established. The relationship between APOE gene polymorphism and DN varies among different populations and regions. For instance, a case-control study including 429 DN patients and 416 diabetic patients as controls conducted by Jiang et al in the Beijing China population reported that the APOE ε2 allele was a risk factor for DN, while the ε4 allele exhibited a protective role.38 In Turkey population, the APOE ε4 allele was identified as a prognostic risk factor in the development of DN.64 Similarly, a study in Iran involving 99 DN patients and 98 patients with type 2 diabetes suggested that the APOE ε4 allele might have a protective against the development of DN.65 A meta-analysis of 29 studies, including 1517 DN cases and 1014 controls from the Chinese Han population, revealed that the APOE ɛ2, ɛ4, E2/E2, E2/E3, and E3/E4 were associated with a increased risk of DN, while the ɛ3 allele and E3/E3 genotype were associated with a decreased risk of DN.52 However, a study conducted in Turkey involving 46 DN patients, 56 T2DM patients, and 36 healthy controls showed no significant association between APOE gene polymorphism and DN.66 Additional studies investigating the relationship of between APOE polymorphisms and DN were shown in Table 5. In our present study, after adjusting for gender, SBP, hypertension, hyperuricemia, TG, HDL-C, and UTP, logistic regression analysis showed that the APOE ε2 allele and E2/E3 genotype increased the risk of DN by 3.237 times and 3.453 times (all p < 0.001), respectively. Conversely, the ε3 allele or E3/E3 genotype appeared to decrease the risk of DN by 0.395 times (all p < 0.001).
DN is associated with the lipid profiles characterized by elevated TG, LDL-C, very low density lipoprotein cholesterol (VLDLC), intermediate-density lipoprotein cholesterol, but lower level of HDL-C.67 These abnormalities in lipid metabolism often accompany renal disease and play a crucial role in the pathogenesis and progression of renal injury. Animal studies have shown that rats fed with high-fat diet has shown the development of focal glomerulosclerosis.68 Focal glomerulosclerosis, related albuminuria, and diabetic glomerulopathy are the main manifestations of DN.69 Numerous animal studies also have demonstrated that hyperlipidemia has a damaging effect on the tubulointerstitium, which is also a major feature of DN and one of the important predictors of renal dysfunction.70,71 The serum lipids can induce both tubulointerstitial and glomerular injury through various mediators such as chemokines, cytokines, reactive oxygen species, and hemodynamic changes.72 DN patients often exhibit a more atherogenic lipid profile compared to healthy controls or diabetics without nephropathy.73 In this study, the comparison of the serum lipid profile levels between APOE ε2 allele, ε3 allele, and ε4 allele in the controls and DN patients were analyzed. We found that the TG levels were higher in ε2 DN patients compared to controls (p < 0.001). HDL-C level in ε2 DN patients was lower than those in controls (p < 0.001). Additionally, DN patients exhibited significantly higher UTP level in all of subgroups (p < 0.001).
This case-control study has certain limitations. Firstly, this study was conducted in a single medical institution of Meizhou, southern China, which may introduce a certain degree of selection bias. Secondly, the sample size of the study is relatively small, which could potentially lead to some deviations in the results. Thirdly, the findings of other populations need to be further investigated. In the future, more researches, larger samples, more other genes, and APOE gene polymorphism will be required to analyze this relationship.
Conclusions
The present study showed APOE ε2 allele and E2/E3 genotype act as independent risk factors, while the ε3 allele and E3/E3 genotype serve as protective factors in the development of DN among the southern Chinese Hakka population. The results may facilitate the development of individualized practical strategies in the management of DN in the studied population.
Data Sharing Statement
The datasets that support the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Ethics approval was obtained from the Human Ethics Committee of Meizhou People’s Hospital (NO: 2021-C-111). The study was in Accordance with the 1975 Declaration of Helsinki. All participants gave written informed consent to participate in the study.
Funding
This study was supported by the Science and Technology Program of Meizhou (Grant No.: 2019B0202001).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Satirapoj B. Nephropathy in diabetes. Adv Exp Med Biol. 2012;771:107–122. doi:10.1007/978-1-4614-5441-0_11
2. Jadawji C, Crasto W, Gillies C, et al. Prevalence and progression of diabetic nephropathy in South Asian, white European and African Caribbean people with type 2 diabetes: a systematic review and meta-analysis. Diabetes Obes Metab. 2019;21(3):658–673. doi:10.1111/dom.13569
3. Demir Y, Ceylan H, Turkes C, Beydemir S. Molecular docking and inhibition studies of vulpinic, carnosic and usnic acids on polyol pathway enzymes. J Biomol Struct Dyn. 2022;40(22):12008–12021. doi:10.1080/07391102.2021.1967195
4. Sever B, Altintop MD, Demir Y, Akalin Ciftci G, Beydemir S, Ozdemir A. Design, synthesis, in vitro and in silico investigation of aldose reductase inhibitory effects of new thiazole-based compounds. Bioorg Chem. 2020;102:104110. doi:10.1016/j.bioorg.2020.104110
5. Gross JL, de Azevedo MJ, Silveiro SP, Canani LH, Caramori ML, Zelmanovitz T. Diabetic nephropathy: diagnosis, prevention, and treatment. Diabetes Care. 2005;28(1):164–176. doi:10.2337/diacare.28.1.164
6. McCullough KP, Morgenstern H, Saran R, Herman WH, Robinson BM. Projecting ESRD incidence and prevalence in the United States through 2030. J Am Soc Nephrol. 2019;30(1):127–135. doi:10.1681/ASN.2018050531
7. Tuttle KR, Bakris GL, Bilous RW, et al. Diabetic kidney disease: a report from an ADA Consensus Conference. Diabetes Care. 2014;37(10):2864–2883. doi:10.2337/dc14-1296
8. Li Y, Ning Y, Shen B, et al. Temporal trends in prevalence and mortality for chronic kidney disease in China from 1990 to 2019: an analysis of the Global Burden of Disease Study 2019. Clin Kidney J. 2023;16(2):312–321. doi:10.1093/ckj/sfac218
9. Molitch ME, DeFronzo RA, Franz MJ, et al. Nephropathy in diabetes. Diabetes Care. 2004;27(Suppl 1):S79–83. doi:10.2337/diacare.27.2007.s79
10. Sever B, Altıntop MD, Demir Y, et al. An extensive research on aldose reductase inhibitory effects of new 4H-1,2,4-triazole derivatives. J Mol Struct. 2021;1224:129446. doi:10.1016/j.molstruc.2020.129446
11. Sever B, Altintop MD, Demir Y, et al. Identification of a new class of potent aldose reductase inhibitors: design, microwave-assisted synthesis, in vitro and in silico evaluation of 2-pyrazolines. Chem Biol Interact. 2021;345:109576. doi:10.1016/j.cbi.2021.109576
12. Ayodele OE, Alebiosu CO, Salako BL. Diabetic nephropathy--a review of the natural history, burden, risk factors and treatment. J Natl Med Assoc. 2004;96(11):1445–1454.
13. Akdağ M, Özçelik AB, Demir Y, Beydemir Ş. Design, synthesis, and aldose reductase inhibitory effect of some novel carboxylic acid derivatives bearing 2-substituted-6-aryloxo-pyridazinone moiety. J Mol Struct. 2022;1258:132675. doi:10.1016/j.molstruc.2022.132675
14. Turkes C, Arslan M, Demir Y, Cocaj L, Nixha AR, Beydemir S. N-substituted phthalazine sulfonamide derivatives as non-classical aldose reductase inhibitors. J Mol Recognit. 2022;35(12):e2991. doi:10.1002/jmr.2991
15. Cheung CY, Ma MKM, Chak WL, Tang SCW. Cancer risk in patients with diabetic nephropathy: a retrospective cohort study in Hong Kong. Medicine. 2017;96(38):e8077. doi:10.1097/MD.0000000000008077
16. Mise K, Galvan DL, Danesh FR. Shaping up mitochondria in diabetic nephropathy. Kidney360. 2020;1(9):982–992. doi:10.34067/kid.0002352020
17. Seyed Ahmadi S, Svensson AM, Pivodic A, Rosengren A, Lind M. Risk of atrial fibrillation in persons with type 2 diabetes and the excess risk in relation to glycaemic control and renal function: a Swedish cohort study. Cardiovasc Diabetol. 2020;19(1):9. doi:10.1186/s12933-019-0983-1
18. Alim Z, Kilic D, Demir Y. Some indazoles reduced the activity of human serum paraoxonase 1, an antioxidant enzyme: in vitro inhibition and molecular modeling studies. Arch Physiol Biochem. 2019;125(5):387–395. doi:10.1080/13813455.2018.1470646
19. Caliskan B, Demir Y, Turkes C. Ophthalmic drugs: in vitro paraoxonase 1 inhibition and molecular docking studies. Biotechnol Appl Biochem. 2022;69(6):2273–2283. doi:10.1002/bab.2284
20. Wu L, Parhofer KG. Diabetic dyslipidemia. Metabolism. 2014;63(12):1469–1479. doi:10.1016/j.metabol.2014.08.010
21. Ng MC, Baum L, So WY, et al. Association of lipoprotein lipase S447X, apolipoprotein E exon 4, and apoC3 −455T>C polymorphisms on the susceptibility to diabetic nephropathy. Clin Genet. 2006;70(1):20–28. doi:10.1111/j.1399-0004.2006.00628.x
22. Shah VN, Cheema BS, Sharma R, et al. ACACbeta gene (rs2268388) and AGTR1 gene (rs5186) polymorphism and the risk of nephropathy in Asian Indian patients with type 2 diabetes. Mol Cell Biochem. 2013;372(1–2):191–198. doi:10.1007/s11010-012-1460-2
23. Wu LS, Hsieh CH, Pei D, Hung YJ, Kuo SW, Lin E. Association and interaction analyses of genetic variants in ADIPOQ, ENPP1, GHSR, PPARgamma and TCF7L2 genes for diabetic nephropathy in a Taiwanese population with type 2 diabetes. Nephrol Dial Transplant. 2009;24(11):3360–3366. doi:10.1093/ndt/gfp271
24. Herman-Edelstein M, Scherzer P, Tobar A, Levi M, Gafter U. Altered renal lipid metabolism and renal lipid accumulation in human diabetic nephropathy. J Lipid Res. 2014;55(3):561–572. doi:10.1194/jlr.P040501
25. Demir Y, Tokali FS, Kalay E, et al. Synthesis and characterization of novel acyl hydrazones derived from vanillin as potential aldose reductase inhibitors. Mol Divers. 2023;27(4):1713–1733. doi:10.1007/s11030-022-10526-1
26. Tokali FS, Demir Y, Turkes C, Dincer B, Beydemir S. Novel acetic acid derivatives containing quinazolin-4(3H)-one ring: synthesis, in vitro, and in silico evaluation of potent aldose reductase inhibitors. Drug Dev Res. 2023;84(2):275–295. doi:10.1002/ddr.22031
27. Beydemir S, Demir Y. Antiepileptic drugs: impacts on human serum paraoxonase-1. J Biochem Mol Toxicol. 2017;31(6). doi:10.1002/jbt.21889
28. DemİR Y, BeydemİR Ş. Purification, refolding, and characterization of recombinant human paraoxonase-1. Turk J Chem. 2015;39:764–776. doi:10.3906/kim-1501-51
29. Mahley RW. Apolipoprotein E: cholesterol transport protein with expanding role in cell biology. Science. 1988;240(4852):622–630. doi:10.1126/science.3283935
30. Mahley RW, Rall SC Jr. Apolipoprotein E: far more than a lipid transport protein. Annu Rev Genomics Hum Genet. 2000;1:507–537. doi:10.1146/annurev.genom.1.1.507
31. Marais AD. Apolipoprotein E in lipoprotein metabolism, health and cardiovascular disease. Pathology. 2019;51(2):165–176. doi:10.1016/j.pathol.2018.11.002
32. Saadat M. Apolipoprotein E (APOE) polymorphisms and susceptibility to breast cancer: a Meta-Analysis. Cancer Res Treat. 2012;44(2):121–126. doi:10.4143/crt.2012.44.2.121
33. Horejsi B, Ceska R. Apolipoproteins and atherosclerosis. Apolipoprotein E and apolipoprotein(a) as candidate genes of premature development of atherosclerosis. Physiol Res. 2000;49(Suppl 1):S63–9.
34. Achouri-Rassas A, Ali NB, Cherif A, et al. Association between ACE polymorphism, cognitive phenotype and APOE E4 allele in a Tunisian population with Alzheimer disease. J Neural Transm. 2016;123(3):317–321. doi:10.1007/s00702-015-1468-3
35. Al-Dabbagh NM, Al-Dohayan N, Arfin M, Tariq M. Apolipoprotein E polymorphisms and primary glaucoma in Saudis. Mol Vis. 2009;15:912–919.
36. Jairani PS, Aswathy PM, Gopala S, Verghese J, Mathuranath PS. Interaction with the MAPT H1H1 genotype increases dementia risk in APOE epsilon4 carriers in a population of southern India. Dement Geriatr Cogn Disord. 2016;42(5–6):255–264. doi:10.1159/000447446
37. Zhong Z, Wu H, Wu H, Zhao P. Analysis of apolipoprotein E genetic polymorphism in a large ethnic Hakka population in southern China. Genet Mol Biol. 2018;41(4):742–749. doi:10.1590/1678-4685-GMB-2017-0301
38. Jiang Y, Ma L, Han C, et al. Effects of Apolipoprotein E isoforms in diabetic nephropathy of Chinese Type 2 Diabetic Patients. J Diabetes Res. 2017;2017:3560920. doi:10.1155/2017/3560920
39. Araki S, Koya D, Makiishi T, et al. APOE polymorphism and the progression of diabetic nephropathy in Japanese subjects with type 2 diabetes: results of a prospective observational follow-up study. Diabetes Care. 2003;26(8):2416–2420. doi:10.2337/diacare.26.8.2416
40. Resnick HE, Foster GL, Bardsley J, Ratner RE. Achievement of American Diabetes Association clinical practice recommendations among U.S. adults with diabetes, 1999–2002: the National Health and Nutrition Examination Survey. Diabetes Care. 2006;29(3):531–537. doi:10.2337/diacare.29.03.06.dc05-1254
41. Hsieh MC, Lin SR, Yang YC, Chen HC, Lin JN, Shin SJ. Higher frequency of apolipoprotein E2 allele in type 2 diabetic patients with nephropathy in Taiwan. J Nephrol. 2002;15(4):368–373.
42. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the study of liver diseases. Hepatology. 2018;68(2):723–750. doi:10.1002/hep.29913
43. Remuzzi G, Schieppati A, Ruggenenti P. Clinical practice. Nephropathy in patients with type 2 diabetes. N Engl J Med. 2002;346(15):1145–1151. doi:10.1056/NEJMcp011773
44. American Diabetes A. Standards of medical care in diabetes--2013. Diabetes Care. 2013;36(Suppl 1):S11–66. doi:10.2337/dc13-S011
45. Turkes C, Demir Y, Beydemir S. Anti-diabetic properties of calcium channel blockers: inhibition effects on aldose reductase enzyme activity. Appl Biochem Biotechnol. 2019;189(1):318–329. doi:10.1007/s12010-019-03009-x
46. Xu M, Wu P, Shen F, Ji J, Rakesh KP. Chalcone derivatives and their antibacterial activities: current development. Bioorg Chem. 2019;91:103133. doi:10.1016/j.bioorg.2019.103133
47. Gan C, Zhang Y, Liang F, Guo X, Zhong Z. Effects of APOE gene epsilon4 allele on serum lipid profiles and risk of cardiovascular disease and tumorigenesis in southern Chinese population. World J Surg Oncol. 2022;20(1):280. doi:10.1186/s12957-022-02748-2
48. Hou J, Deng Q, Guo X, Deng X, Zhong W, Zhong Z. Association between apolipoprotein E gene polymorphism and the risk of coronary artery disease in Hakka postmenopausal women in southern China. Lipids Health Dis. 2020;19(1):139. doi:10.1186/s12944-020-01323-6
49. Altintop MD, Demir Y, Turkes C, et al. A new series of hydrazones as small-molecule aldose reductase inhibitors. Arch Pharm. 2023;356(4):e2200570. doi:10.1002/ardp.202200570
50. Ertano BY, Demir Y, Nural Y, Erdoğan O. Investigation of the effect of acylthiourea derivatives on diabetes-associated enzymes. ChemistrySelect. 2022;7(46):e202204149. doi:10.1002/slct.202204149
51. Khalil YA, Rabes JP, Boileau C, Varret M. APOE gene variants in primary dyslipidemia. Atherosclerosis. 2021;328:11–22. doi:10.1016/j.atherosclerosis.2021.05.007
52. Yin YW, Qiao L, Sun QQ, et al. Influence of apolipoprotein E gene polymorphism on development of type 2 diabetes mellitus in Chinese Han population: a meta-analysis of 29 studies. Metabolism. 2014;63(4):532–541. doi:10.1016/j.metabol.2013.12.008
53. Reis KA, Ebinc FA, Koc E, et al. Association of the angiotensinogen M235T and APO E gene polymorphisms in Turkish type 2 diabetic patients with and without nephropathy. Ren Fail. 2011;33(5):469–474. doi:10.3109/0886022X.2011.568133
54. Atta MI, Abo Gabal K, El-Hadidi K, Swellam M, Genina A, Zaher NF. Apolipoprotein E genotyping in Egyptian diabetic nephropathy patients. IUBMB Life. 2016;68(1):58–64. doi:10.1002/iub.1460
55. Rall SC Jr, Weisgraber KH, Mahley RW. Human apolipoprotein E. The complete amino acid sequence. J Biol Chem. 1982;257(8):4171–4178. doi:10.1016/S0021-9258(18)34702-1
56. Blue ML, Williams DL, Zucker S, Khan SA, Blum CB. Apolipoprotein E synthesis in human kidney, adrenal gland, and liver. Proc Natl Acad Sci U S A. 1983;80(1):283–287. doi:10.1073/pnas.80.1.283
57. Seripa D, D’Onofrio G, Panza F, Cascavilla L, Masullo C, Pilotto A. The genetics of the human APOE polymorphism. Rejuvenation Res. 2011;14(5):491–500. doi:10.1089/rej.2011.1169
58. Rao H, Wu H, Yu Z, Huang Q. APOE genetic polymorphism rs7412 T/T genotype may be a risk factor for essential hypertension among Hakka people in Southern China. Int J Hypertens. 2022;2022:8145896. doi:10.1155/2022/8145896
59. Karahan Z, Ugurlu M, Ucaman B, et al. Relation between apolipoprotein E gene polymorphism and severity of coronary artery disease in acute myocardial infarction. Cardiol Res Pract. 2015;2015:363458. doi:10.1155/2015/363458
60. Demirag MD, Onen HI, Karaoguz MY, et al. Apolipoprotein E gene polymorphism in nonalcoholic fatty liver disease. Dig Dis Sci. 2007;52(12):3399–3403. doi:10.1007/s10620-007-9740-5
61. Chaudhary R, Likidlilid A, Peerapatdit T, et al. Apolipoprotein E gene polymorphism: effects on plasma lipids and risk of type 2 diabetes and coronary artery disease. Cardiovasc Diabetol. 2012;11:36. doi:10.1186/1475-2840-11-36
62. Broce IJ, Tan CH, Fan CC, et al. Dissecting the genetic relationship between cardiovascular risk factors and Alzheimer’s disease. Acta Neuropathol. 2019;137(2):209–226. doi:10.1007/s00401-018-1928-6
63. Eto M, Saito M, Okada M, et al. Apolipoprotein E genetic polymorphism, remnant lipoproteins, and nephropathy in type 2 diabetic patients. Am J Kidney Dis. 2002;40(2):243–251. doi:10.1053/ajkd.2002.34502
64. Ilhan N, Kahraman N, Seckin D, Ilhan N, Colak R. Apo E gene polymorphism on development of diabetic nephropathy. Cell Biochem Funct. 2007;25(5):527–532. doi:10.1002/cbf.1348
65. Karimoei M, Pasalar P, Mehrabzadeh M, et al. Association between apolipoprotein E polymorphism and nephropathy in Iranian diabetic patients. Saudi J Kidney Dis Transpl. 2017;28(5):997–1002. doi:10.4103/1319-2442.215137
66. Erdogan M, Eroglu Z, Biray C, et al. The relationship of the apolipoprotein E gene polymorphism Turkish Type 2 diabetic patients with and without nephropathy. J Endocrinol Invest. 2009;32(3):219–222. doi:10.1007/BF03346455
67. Bonnet F, Cooper ME. Potential influence of lipids in diabetic nephropathy: insights from experimental data and clinical studies. Diabetes Metab. 2000;26(4):254–264.
68. Kasiske BL, O’Donnell MP, Schmitz PG, Kim Y, Keane WF. Renal injury of diet-induced hypercholesterolemia in rats. Kidney Int. 1990;37(3):880–891. doi:10.1038/ki.1990.62
69. Hung CC, Tsai JC, Kuo HT, Chang JM, Hwang SJ, Chen HC. Dyslipoproteinemia and impairment of renal function in diabetic kidney disease: an analysis of animal studies, observational studies, and clinical trials. Rev Diabet Stud. 2013;10(2–3):110–120. doi:10.1900/RDS.2013.10.110
70. Grone HJ, Hohbach J, Grone EF. Modulation of glomerular sclerosis and interstitial fibrosis by native and modified lipoproteins. Kidney Int Suppl. 1996;54:S18–22.
71. Gilbert RE, Cooper ME. The tubulointerstitium in progressive diabetic kidney disease: more than an aftermath of glomerular injury? Kidney Int. 1999;56(5):1627–1637. doi:10.1046/j.1523-1755.1999.00721.x
72. Chen HC, Guh JY, Chang JM, Hsieh MC, Shin SJ, Lai YH. Role of lipid control in diabetic nephropathy. Kidney Int Suppl. 2005;94:S60–2. doi:10.1111/j.1523-1755.2005.09415.x
73. Hirano T. Lipoprotein abnormalities in diabetic nephropathy. Kidney Int Suppl. 1999;
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.