Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Association Between the Systemic Inflammatory Response Index and Severe Infection in Patients with Diabetic Foot
Authors Wu P ![]() , Xu W, Chen R
, Xu W, Chen R ![]() , Xu Z
, Xu Z ![]()
Received 2 March 2026
Accepted for publication 8 June 2026
Published 29 June 2026 Volume 2026:19 605794
DOI https://doi.org/10.2147/DMSO.S605794
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Video abstract of “Systemic Inflammatory Response Index in Patients with Diabetic Foot” [605794].
Views: 9
Ping Wu,1,2,* Wendong Xu,3,4,* Rui Chen,3 Zhenghui Xu3
1Department of Pharmacology, The Third Affiliated Hospital of Soochow University, Changzhou, Jiangsu, People’s Republic of China; 2Department of Pharmacology, The First People’s Hospital of Changzhou, Changzhou, Jiangsu, People’s Republic of China; 3Department of Endocrinology and Metabolism, The Third Affiliated Hospital of Soochow University, Changzhou, Jiangsu, People’s Republic of China; 4Changzhou Medical Center, Nanjing Medical University, Changzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhenghui Xu, Department of Endocrinology and Metabolism, The Third Affiliated Hospital of Soochow University, No. 185, Juqian Street, Changzhou, Jiangsu Province, 213003, People’s Republic of China, Tel +86 0519-68870000, Email [email protected]
Purpose: In this study, we aimed to clarify the association between the Systemic Inflammatory Response Index (SIRI) and the severity of infection in patients with diabetic foot infection (DFI).
Patients and Methods: A retrospective study was conducted among individuals admitted to The First People’s Hospital of Changzhou with DFI from March 2021 to October 2025.Two hundred and forty-two patients with DFI were categorized to a severe infection group (n=110) or a moderate infection group (n=132). The area under the receiver operating characteristic (ROC) curve (AUC) was used to assess the accuracy of association between SIRI and the risk of severe DFI. Multivariate logistic regression analysis and restricted cubic spline (RCS) analysis were employed to characterize the relationship between SIRI and the severity of DFI. Subgroup analyses and interaction analyses were utilized to enhance the reliability of this study. The bootstrap method was utilized to calculate the confidence interval (CI) of AUC. The optimal cutoff value for the ROC curve was determined based on the principle of maximizing the Youden index, and the threshold for the RCS curve was defined at the point where the odds ratio equaled 1.
Results: The ROC curve analysis showed that SIRI was highly associated with the severity of DFI, yielding an AUC of 0.959 (95% CI: 0.932– 0.986). For every 1 unit increase in SIRI, the risk of severe DFI increases to 2.26 times the original risk. Furthermore, as SIRI increased, the risk of severe DFI increased in the RCS model. There was a nonlinear association between SIRI and the risk of severe DFI, with an inflection point of SIRI at 3.53 (OR: 0.93, 95% CI: 0.91– 0.95). Severe DFI was less likely to occur below this inflection point. Beyond this point, the risk of developing severe DFI increased significantly. When SIRI exceeded 15.96 (OR: 132.23, 95% CI: 42.94– 432.18), the increase plateaued.
Conclusion: SIRI is significantly associated with the severity of DFI in diabetes patients, and it is imperative to maintain a low SIRI level in order to prevent the occurrence of severe DFI. The importance of maintaining an appropriate SIRI level should not be overlooked among diabetic foot patients.
Keywords: systemic inflammatory response index, diabetes mellitus, diabetic foot, severe infection
Introduction
Diabetic foot is considered to be one of the most severe complications of diabetes, because of its long duration, high risk of recurrence, and substantial associated incidences of disability and mortality. Millions of patients worldwide currently are suffering from diabetic foot ulcer (DFU), which affects about 18.6 million people worldwide every year.1 It has been established that between 50% and 60% of patients who develop DFU will develop diabetic foot infection (DFI) within a year.2 DFI is the primary cause of lower limb amputation for non-trauma-related reasons. A previous study showed that 55% of patients with DFI still had an infected lesion 1 year after diagnosis, and nearly 15% underwent amputation.3 This condition has been shown to have significant deleterious effects on the quality of life of patients, including a loss of independence and psychological distress. Furthermore, the associated healthcare costs are considerable.4
Despite many studies conducted on topical materials for DFU in recent years, these novel materials have yet to demonstrate the capacity to halt the progression of disease once a severe DFI has developed.5–7 Consequently, the early identification of infection and subsequent prompt management are imperative for reducing major amputation.
Chronic inflammation is a sustained, low-grade immune response that can underlie or exacerbate a wide range of diseases, including cardiovascular disease, cancer, and autoimmune disorders. It disrupts normal tissue function and promotes cellular damage, contributing to the progression and severity of these conditions.8–10 Previous studies have also shown a close relationship between DFU and chronic inflammation. Individuals with high levels of markers of inflammation have been shown to have a higher incidence of DFU. Persistent inflammation has been demonstrated to exacerbate ulceration and impede wound healing, which is associated with amputation in severe cases.11–13 Concurrently, persistent inflammation disrupts the immune barrier of the body’s local tissue, enabling bacteria to colonize and proliferate at the ulcer site.14,15 When bacteria proliferate in large numbers and the toxin level exceeds the clearance capacity of local tissues, inflammatory cells (such as macrophages and neutrophils) are activated, resulting in the release of large amounts of proinflammatory mediators. These substances have been shown to have a series of deleterious effects on the circulatory system, including vascular endothelial injury and microcirculatory disorders.16,17 It is well documented that patients with severe infection frequently develop secondary immunosuppression, making such infections very difficult to control. This secondary immunosuppression is frequently characterized by impaired antigen presentation, low absolute CD4+ T-cell counts, T- and B-cell apoptosis, the downregulation of human leukocyte antigen-DR expression, and low concentrations of cytokines, such as TNFα, IFNγ, and IL-6.18,19 Therefore, it is inappropriate to rely on the measurement of proinflammatory marker levels as the sole means of evaluating DFI, and there is an urgent need to identify novel approaches for simultaneously evaluating inflammation and the immune status of patients.
Biomarkers of inflammation provide real-time information regarding the intensity of and changes in the systemic inflammatory response. The simplicity, rapidity, and low cost of measuring the concentrations of these substances, such as Systemic Inflammatory Response Index (SIRI),17 Systemic immune-inflammation index (SII),20 neutrophil (NEU)-to-lymphocyte (LYM) ratio (NLR),19 Albumin/NEU/LYM Ratio (ANLR),21 NEU percentage-to-albumin ratio (NPAR),22 and Prognostic nutritional index (PNI),23 have led to their use as core predictors of bacterial infections, including sepsis. SIRI is a novel marker of inflammation that reflects the status of NEU, LYM, and monocyte (MON), and thereby the inflammatory and immune status of the body. Xu et al24 showed that high SIRI was associated with poor outcomes and severe sepsis in patients with sepsis in intensive care units SIRI was shown to be a superior predictor than conventional indices, such as the SOFA and AP scores: receiver operating characteristic (ROC) analysis revealed that SIRI was associated with the largest area under the curve (AUC = 0.682, versus 0.626 and 0.597 for the SOFA and AP scores, respectively). A study by Zhu et al showed that SIRI is a useful means of assessing the prognosis of patients with sepsis and that there is a significant correlation between SIRI and 28-day mortality (P<0.001). In addition, ROC curve analysis indicated that the predictive ability of SIRI surpasses that of the APACHE II and SOFA scores.25 Finally, Hu et al26 showed that high SIRI, NLR, and PLR scores were all associated with a higher risk of DFU, with SIRI showing the closest association. Subgroup analysis revealed that the association between high SIRI and the risk of DFU is robust, with no difference between the sexes. However, to date, there have been no research reports on the relationship between SIRI and severe DFI.
For the first time, we aimed to characterize the association between SIRI and the severity of DFI, whether it is linear or nonlinear, and to identify the most appropriate threshold value for use in risk stratification. The data obtained should guide early risk assessment and personalized clinical interventions for patients with DFU.
Patients and Methods
Patients
We performed a retrospective analysis of 305 patients with diabetes who were diagnosed with foot infection at The First People’s Hospital of Changzhou between March 2021 and October 2025. A total of 242 eligible patients were ultimately recruited (Figure 1), and assigned to severe infection (n=110) and moderate infection (n=132) groups. This retrospective analysis of de-identified human serum was conducted in accordance with the Declaration of Helsinki. The Human Research and Ethics Committee of The First People’s Hospital of Changzhou approved this retrospective study (ethics approval number: 2025175). Due to the retrospective nature of the research utilizing biobank-stored serum samples, informed consent was waived by the approving institution. All data were handled with strict confidentiality to ensure the anonymity of participants.
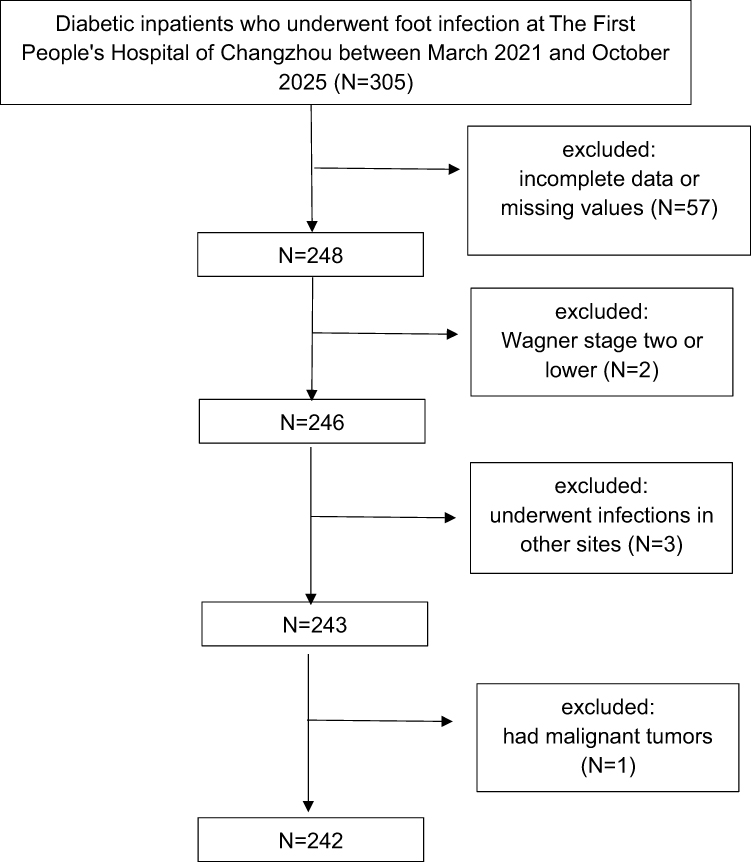 |
Figure 1 Flow of participants. |
Sample size calculation was determined using PASS v21.0.3 (NCSS, LLC, Kaysville, UT, USA). A logistic regression of severe DFI on SIRI with a sample size of 143 observations achieves 90% power at a 0.05 significance level to detect an odds ratio of 2.26 when the prevalence of DFI in the population is 0.15.27 We added an allowance of 20% for loss to follow-up, and therefore a minimum of 179 patients with DFI was required for the investigation (Supplementary Material 1).
Data Collection
We obtained the demographic and clinical characteristics of the patients from the hospital information system, including their sex, age, body mass, height, smoking status, alcohol status, duration of diabetic foot, duration of diabetes, history of cardiovascular disease (CVD), history of peripheral artery disease (PAD), history of chronic renal disease (CRD), history of foot care, history of systemic antimicrobial use, systolic blood pressure (SBP), diastolic blood pressure (DBP), hemoglobin A1c (HbA1c) level, serum total cholesterol (TC) concentration, serum triglyceride concentration, serum low-density lipoprotein cholesterol (LDL-C) concentration, serum high-density lipoprotein cholesterol (HDL-C) concentration, serum uric acid concentration, albumin, hemoglobin (HGB), culture characteristics (drug-resistance), NEU count, LYM count, MON count, CRP (C-reactive protein), PCT (procalcitonin). All these values were obtained during examinations conducted within 24 hours of admission. The blood sampling time for all patients was within 24 hours after admission. Blood collection time of all patients was within 24 hours of admission. All laboratory detections were performed by Laboratory Department of our hospital. Complete blood count analysis and PCT were conducted using Sysmex XN20 (A1) series analyzer (Sysmex Corporation, Kobe, Japan) and MAGLUMI X10 series analyzer (Snibe, Shenzhen New Industries Biomedical Engineering Co., Ltd., Shenzhen, China), respectively. Albumin and CRP were measured by a Beckman Coulter AU5800 analyzer (Beckman Coulter, Inc., Brea, CA, USA). Vital signs were measured by specialized nurses on admission. Well-controlled blood pressure was defined as an SBP <140 mmHg and a DBP <90 mmHg. Body mass index (BMI) was calculated as body mass divided by height squared. The various inflammatory scores were calculated as follows:
SIRI = (NEU count × MON count)/LYM count;
SII = (NEU count × Platelet count)/LYM count;
NLR = NEU count/LYM count;
ANLR = albumin (g/dL)/(NEU count/LYM count);
NPAR = NEU percentage (in total white blood cell count) (%) × 100/Albumin (g/dL); and
PNI =Albumin (g/L) + 5 × LYM count.
According to the guidelines of the International Diabetes Federation (IDF) and the International Working Group on the Diabetic Foot (IWGDF), the severity of DFI was defined as follows.27 1) Moderate infection: an ulcer extending to bone and fascia, erythema >2 cm in diameter, and no systemic symptoms. 2) Severe infection: the presence of two or more systemic symptoms, such as temperature >38°C or <36°C, heart rate >90 beats/min, respiratory rate >20 breaths/min, partial pressure of carbon dioxide <4.3 kPa (32 mmHg), white blood cell count >12,000 or <4,000 cells/mm3, or the presence of >10% immature (band) neutrophils.
Statistical Analysis
Statistical analysis was performed using R 4.3.1 software (R Foundation for Statistical Computing, Vienna, Austria). Missing data within 5% was imputed using the median imputation method. A ROC curve was plotted to evaluate the ability of SIRI to predict the severity of DFI and to determine the most appropriate cutoff value of SIRI to identify patients with severe DFI. The 95% CI of the AUC is calculated by the bootstrapping method, and an AUC >0.5 was considered to indicate an acceptable predictive ability. Bootstrapping methods was used to verify the risk of potential overfitting. When datasets were normally distributed, the mean ± standard deviation was used for data presentation, and the Student’s t-test was employed for data comparison. When datasets were non-normally distributed, the median and interquartile range (IQR) were used for data presentation, and the Mann–Whitney U-test was employed for data comparison. We compared categorical datasets using Pearson’s chi-square test.
Having identified an association between high SIRI and the risk of severe DFI using univariate and multivariate logistic regression analyses, we generated three multidimensional models to provide a more accurate demonstration of the effects of various covariates on this risk. The crude model only included SIRI. Model 1 incorporated sex and age. Model 2 incorporated sex, age, BMI, smoking status, and alcohol status. Model 3 incorporated sex, age, BMI, smoking status, alcohol status, CVD, PAD, CRD, HbA1c level, hypertension, TC, LDL-C, uric acid, history of foot care, history of systemic antimicrobial use, albumin, HGB and culture characteristics (drug-resistance).
In this way, we evaluated the link between SIRI and the risk of severe DFI. In the multivariate logistic regression analysis, SIRI was treated as a continuous rather than a categorical variable. We determined the effect of a 1-unit increase in SIRI on the risk of developing severe DFI, with the intention of enabling clinicians to assess this risk more accurately. Collinearity diagnostics was further performed to verify the reliability of the regression model. Restricted cubic spline (RCS) analysis was used to identify nonlinear interactions and locate inflection points, and stepwise logistic regression was used to identify threshold effects. The optimal cutoff value for the ROC curve was determined based on the principle of maximizing the Youden index. The threshold for the RCS curve was defined at the point where the odds ratio equaled 1. Subgroup and interaction analyses were used as sensitivity analyses to evaluate the robustness of the findings obtained. Subgroup analyses were conducted on the basis of age, sex, BMI, smoking status, medical history, HbA1c level, LDL-C concentration, hypertension, serum uric acid concentration, history of systemic antimicrobial use, HGB, and culture characteristics (drug-resistance). All the statistical tests were two-sided, and P<0.05 was considered to indicate statistical significance.
Results
Association Between SIRI and Severe DFI of Patients
For the model used to assess the ability of SIRI to predict severe DFI, the AUC was 0.959 (0.932–0.986). The calculated cut-off value was 3.375, with a sensitivity of 0.955 and a specificity of 0.856. To eliminate the risk of potential overfitting, we calculated 95% CI of AUC in the ROC was 0.932 to 0.986 by using bootstrapping, which indicated that our results are reliable and stable (Supplementary Figures 1 and 2). SIRI was the most useful inflammatory index for the prediction of severe DFI. The AUCs of SII, NLR, ANLR, NPAR, PNI, CRP and PCT were 0.925 (0.892–0.958), 0.929 (0.898–0.960), 0.931 (0.902–0.961), 0.878 (0.835–0.921), 0.783 (0.725–0.842), 0.563 (0.49–0.636), 0.533 (0.459–0.607), respectively. SIRI exhibited greater prognostic value (Figure 2).
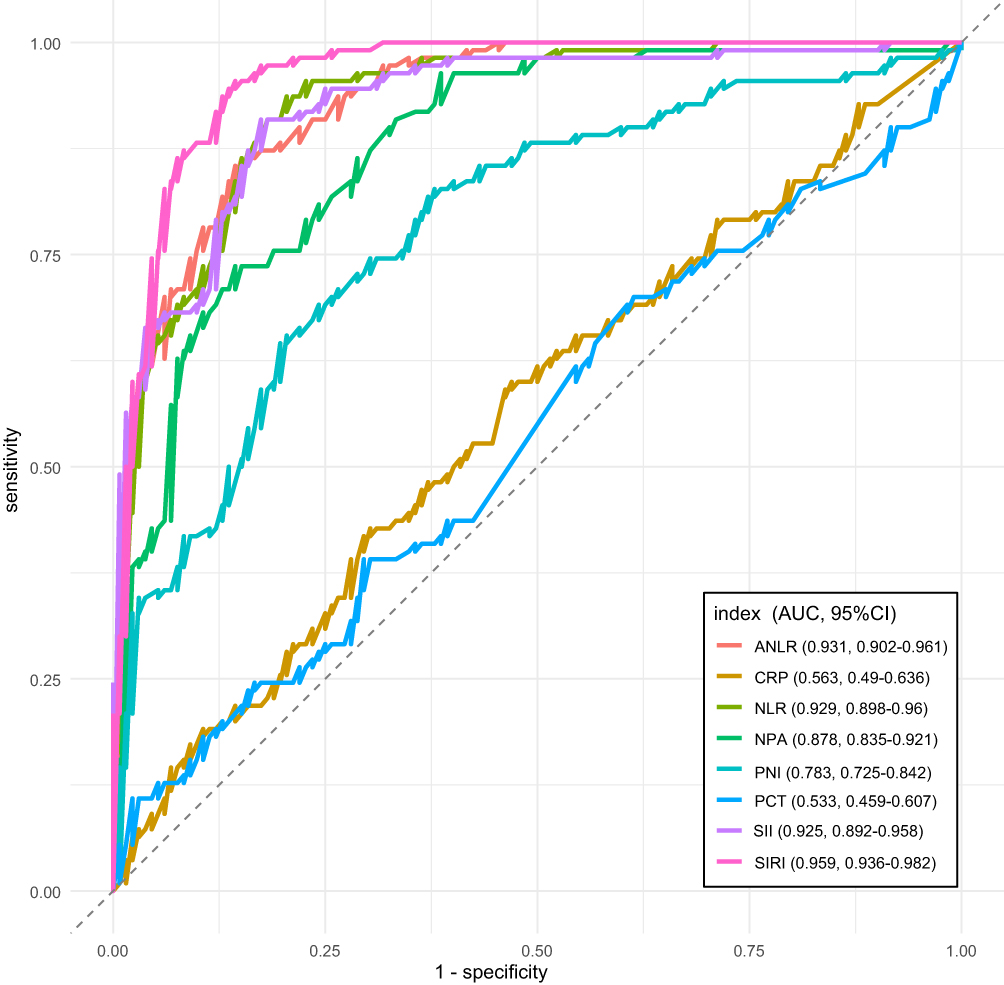 |
Figure 2 Receiver operating characteristic curves of inflammatory markers—SIRI, SII, NLR, ANLR, NPAR, PNI, CRP, and PCT among DFI patients (n = 242). Abbreviations: SIRI, Systemic Inflammatory Response Index; SII, Systemic immune-inflammation index; NLR, neutrophil-to-lymphocyte ratio; ANLR, Albumin/neutrophil/lymphocyte Ratio; NPAR, neutrophil percentage-to-albumin ratio; PNI, Prognostic nutritional index; DFI, diabetic foot infection; CRP, C-reactive protein; PCT, procalcitonin; CI, confidence interval. |
Study Sample and the Baseline Characteristics of the Patients
Table 1 provides a summary of the baseline characteristics of the patients. A total of 242 patients with DFI were studied (176 men and 66 women with a median age of 67 years), of whom 45.5% had severe DFI. The patients were categorized into two groups according to their SIRI score: those with a score ≤3.375 were placed in a low SIRI group, and those with a score >3.375 were placed in a high SIRI group. Statistical analysis revealed significant differences in severe DFI, age, BMI, TC, LDL-C, HDL-C, NEU count, LYM count, MON count and characteristics (drug-resistance) between two SIRI groups (all P<0.05). Specifically, the number of patients with severe DFI in the high SIRI group is greater than that in the low SIRI group (P<0.001).
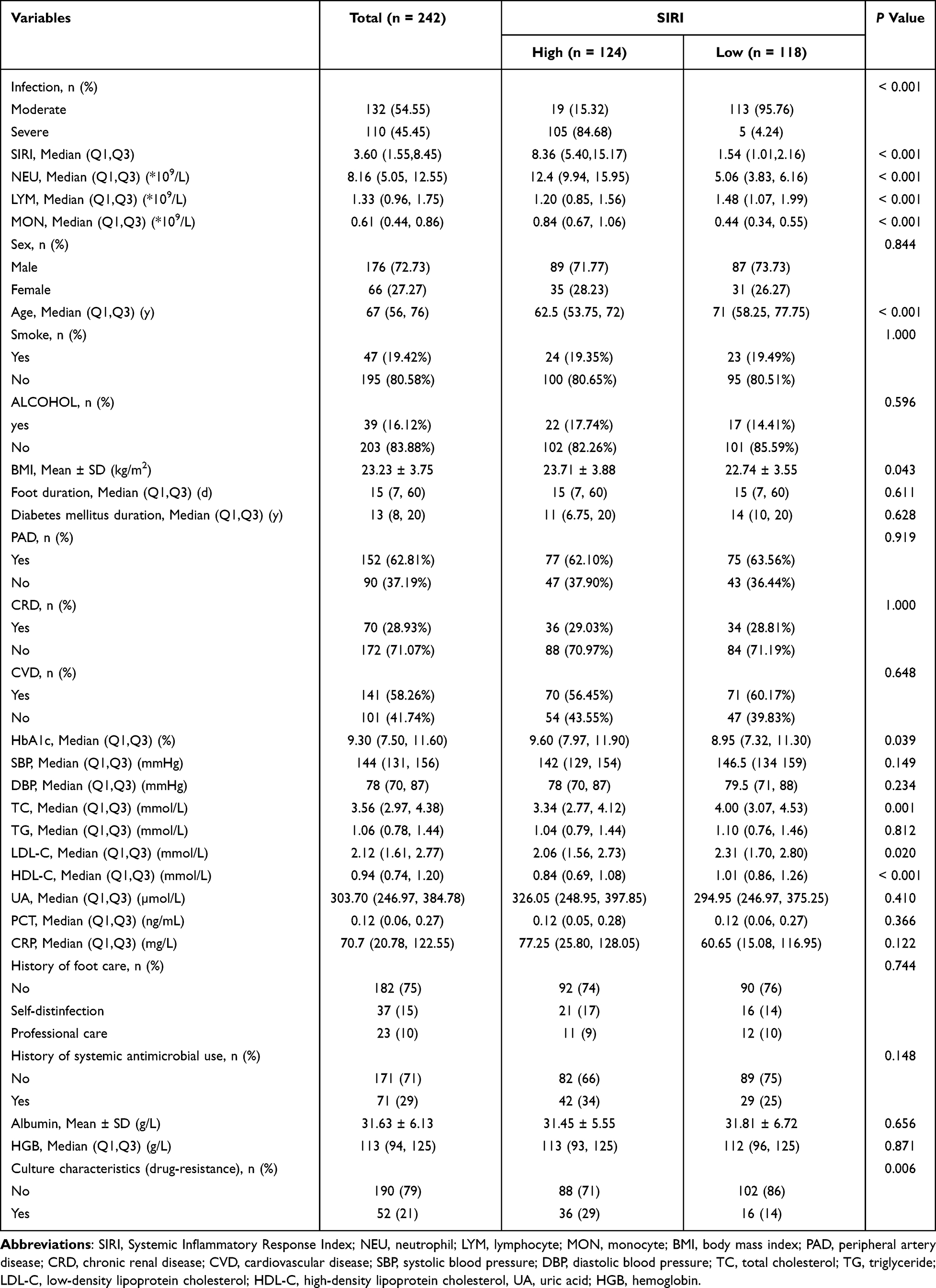 |
Table 1 Baseline Characteristics of the Study Population (n = 242) |
Findings of the Logistic Regression Analysis of the Association Between SIRI and the Severity of DFI
Table 2 presents the findings of the analysis of the association between SIRI and severe DFI. Univariate analyses across the various models indicated that high SIRI was significantly correlated with severe DFI. Furthermore, for every 1 unit increase in SIRI, the risk of severe DFI in patients increases to 2.26 times the original risk. We also calculated the variance inflation factor of the independent variables in the multiple logistic regression, and found that all variance inflation factor values were less than 5, indicated no substantial multicollinearity.
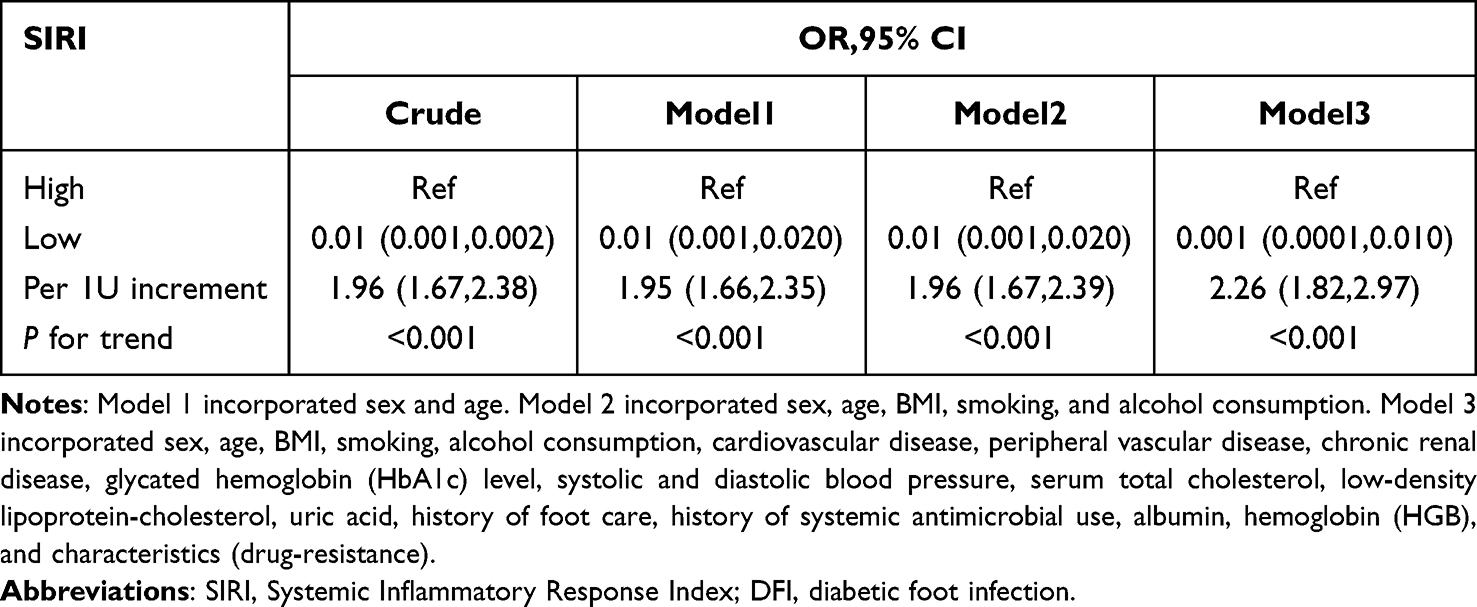 |
Table 2 Relationship Between SIRI and Severe DFI Through Logistic Regression Analysis (n = 242) |
Findings of the RCS Analysis of the Association Between SIRI and the Severity of DFI
The nature of the association between SIRI and the severity of DFI was further explored using RCS analysis. Figure 3 shows that there was a nonlinear, inverted L-shaped association between SIRI and the risk of severe DFI (P<0.001). The occurrence of severe DFI increases as SIRI increases, until an inflection point of SIRI is reached at 3.53 (OR: 0.93, 95% CI: 0.91–0.95). Specifically, when SIRI was <3.53, the risk of severe DFI occurrence was low, but when SIRI was >3.53, the risk of severe DFI occurrence increased markedly as SIRI increased (by 34% for every 1-unit increase, P=0.02). However, when SIRI reached 15.96 (OR: 132.23, 95% CI: 42.94–432.18), the increase in risk plateaued (P=0.40). In summary, a high SIRI is associated with a higher risk of severe DFI occurrence, and a SIRI <3.53 indicates a relatively low risk. More exhaustive details are presented in Table 3.
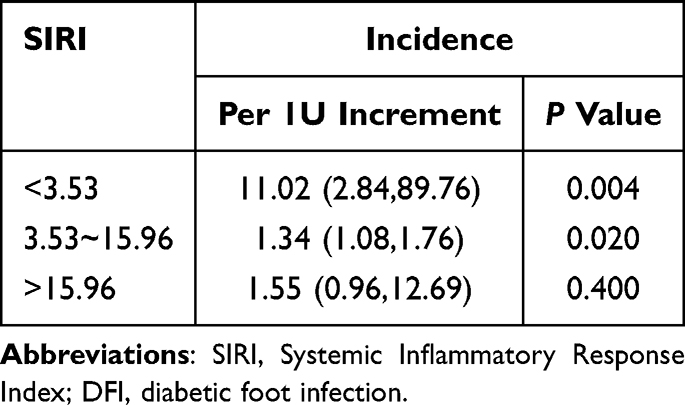 |
Table 3 Threshold Effect Analysis of SIRI and Severe DFI Through Restricted Cubic Spline Analysis (n = 242) |
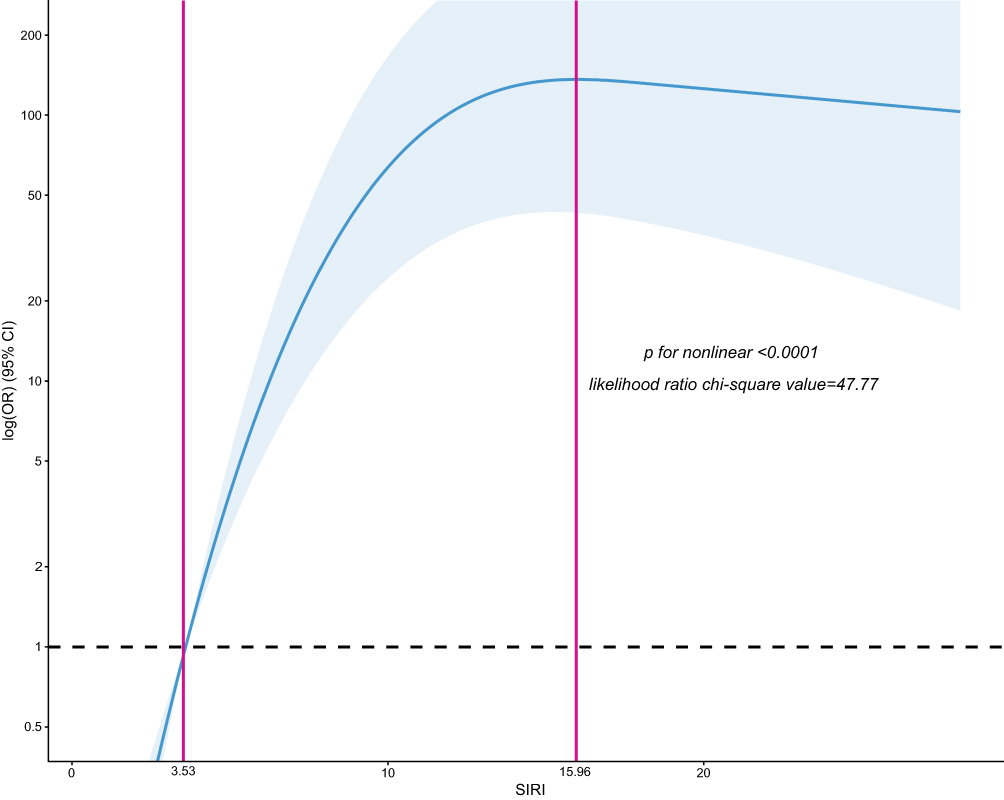 |
Figure 3 Association between SIRI and the severity of infection in DFI patients using restricted cubic spline analysis (n = 242). Abbreviations: SIRI, Systemic Inflammatory Response Index; DFI, diabetic foot infection. |
Findings of the Subgroup Analyses to Identify Variables that Might Affect the Association Between SIRI and the Severity of DFI
Stratified analysis could identify subgroups at a higher risk of developing severe DFI. Figure 4 indicates that the association was more pronounced in individuals with a history of PAD, those with SBP ≥140 mmHg (or DBP ≥90 mmHg), those with LDL-C ≥1.8 mmol/L, and those with uric acid <360 umol/L. No significant interaction was observed between the severity of DFI and sex (P=0.072), age (P=0.376), smoking (P=0.109), alcohol (P=0.607), BMI (P=0.855), diabetic foot duration (P=0.375), diabetes mellitus duration (P=0.800), history of systemic antimicrobial use (P=0.154), CVD (P=0.932), CRD (P=0.362), HbA1c (P=0.163), TC (P=0.886), HGB (P=0.086), or culture characteristics (drug-resistance) (P=0.752).
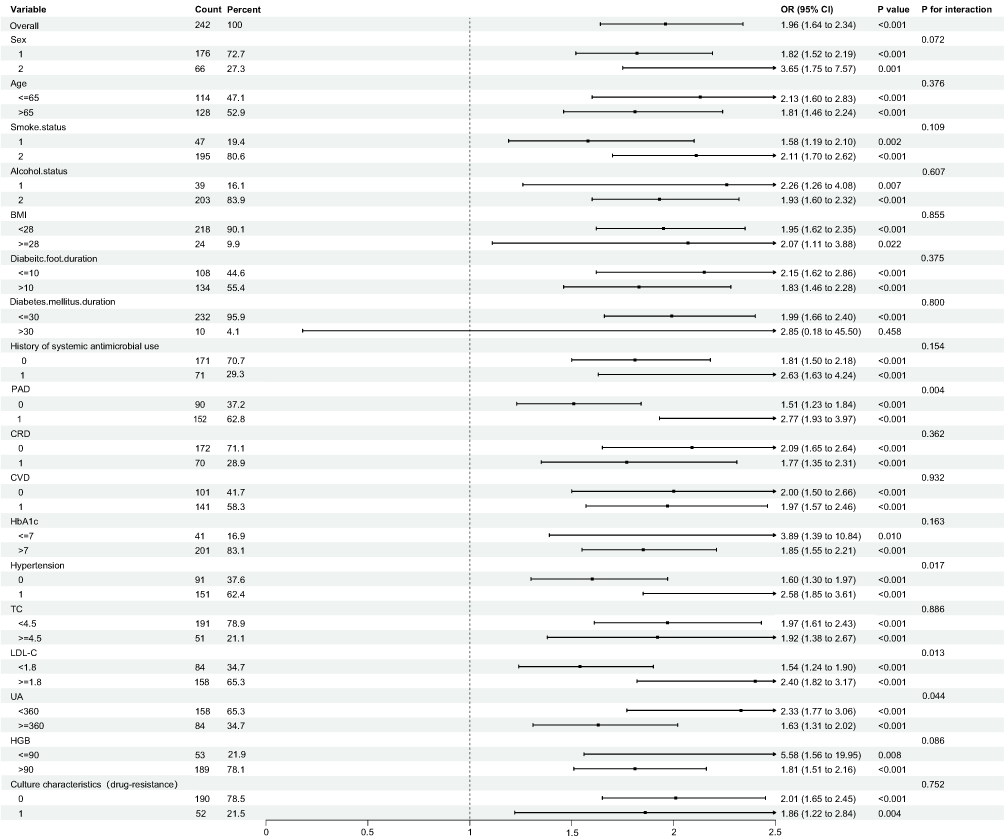 |
Figure 4 Forest plot of subgroup and interaction analyses for the association between SIRI and the severity of DFI (n = 242). Abbreviations: SIRI, Systemic Inflammatory Response Index; DFI, diabetic foot infection; BMI, body mass index; CVD, cardiovascular disease; PAD, peripheral artery disease; CRD, chronic renal disease; LDL-C, low-density lipoprotein cholesterol, UA, uric acid; HGB, hemoglobin. |
Discussion
In the present retrospective study, for the first time, SIRI was found to be independently associated with the severity of DFI, which exhibited an inverted L-shaped association with an inflection point of SIRI near 3.53. When SIRI was <3.53, the risk of severe DFI was lower; conversely, in patients with SIRI >3.53, there was a positive association between SIRI and the risk of developing severe DFI. The results of the subgroup analyses confirmed this significant association between SIRI and the severity of DFI. To the best of our knowledge, this is the first study to demonstrate a non-linear association between SIRI and the severity of DFI.
A number of studies have demonstrated the value of SIRI for the prediction of infection. A retrospective study of 619 patients with ST-segment elevation myocardial infarction (STEMI) revealed that those undergoing percutaneous coronary intervention (PCI) with SIRI ≥ 4.04 had a significantly higher risk of pneumonia (OR: 5.20, 95% CI: 3.53–7.72, P < 0.001). ROC curve analysis indicated that SIRI was a good predictor of post-PCI pneumonia in patients with STEMI, with an AUC of 0.766 (95% CI: 0.724–0.808).28 In addition, Shao et al29 reported the clinical value of NLR, MLR, PLR, SII, and SIRI for the prediction of Mycoplasma pneumoniae (MP) infection in children, identifying high MLR and SIRI as risk factors for such infection. The ROC curve analysis showed that SIRI was the superior predictor of MP infection (AUC=0.892, sensitivity=75.7%, specificity=92.0%). A previous cross-sectional study that used data from the US National Health and Nutrition Examination Survey database aimed to characterize the relationship between SIRI and the risk of DFU development. The authors studied data from 1,204 participants, 112 of whom had DFU, and found that a 1-unit increase in SIRI was associated with a 27% increase in the prevalence of DFU (OR: 1.27, 95% CI: 1.10–1.48, P=0.001). It has been hypothesized that regular SIRI monitoring may contribute to the early diagnosis and management of DFUs.26 However, there have been no studies of the association between SIRI and the severity of DFI. In the present study, we found SIRI exhibited higher sensitivity than other compounding inflammatory makers (including SII, NLR, ANLR, NPAR, and PNI) and traditional inflammatory makers (including CRP and PCT). Meanwhile, we also identified a nonlinear relationship between SIRI and the severity of DFI in the study sample. Specifically, when SIRI was <3.53, there was a lower risk of severe DFI occurrence, whereas when SIRI was >3.53, the patients had a higher risk of severe DFI occurrence.
Inflammation plays a central role in the pathophysiology of both type 1 and type 2 diabetes, contributing to disease development and the progression of complications. Research indicates that elevated cytokine levels and dysregulation of inflammatory pathways are key features in diabetes, impacting immune responses and metabolic disorders.30–32 Previous studies have shown that patients with diabetes tend to release numerous NEU extracellular traps, resulting in a significant increase in NEU numbers, which perpetuates their proinflammatory state.33 Patients with DFU are predisposed to infections and sepsis, and such infections further exacerbate systemic inflammation in these patients, despite the systemic inflammatory response mediated by extracellular traps.34 Three immune cell types, NEU, LYM, and MON, play crucial roles in the pathogenesis of infection. A high NEU count reflects ongoing inflammation and infection, and MON and LYM, which are key components of the innate and adaptive immune responses, respectively, participate in inflammatory responses and immune regulation by modulating immune-related pathways, such as the Janus Kinase-Signal Transducer and Activator of Transcription (JAK-STAT). SIRI includes all of the NEU, LYM, and MON counts, and thereby provides a more comprehensive reflection of systemic inflammatory and immune responses than individual markers of inflammation.35,36
In the present study, a high SIRI was associated with high NEU and MON counts, but a low LYM count. Table 1 shows that the high SIRI group had significantly higher NEU and MON counts (P<0.0001) and a significantly lower LYM count (P<0.0001) than the low SIRI group. Why, then, is there no further increase in the risk of severe DFI when SIRI is higher than the inflection point? We propose the following hypothesis on the basis of prior research. A sustained increase in SIRI may indicate excessive inflammation, and persistent systemic inflammation can induce vascular endothelial adhesion and the migration of circulating neutrophils into tissues. Infection-related immunosuppression has been demonstrated to lead to the apoptosis of circulating neutrophils and impaired myelopoiesis, resulting in NEU paralysis.37 Consequently, as the infection progresses, both the absolute number and function of circulating neutrophils decrease. Concurrently, other immune cell types may become exhausted and have less capacity to produce inflammatory mediators, with the consequent suppression of the immune response. Therefore, the risk of severe DFI occurrence may increase as SIRI increases, but the rate of increase slows after a certain threshold is reached.
The nonlinear association identified between SIRI and the risk of severe DFI involves an inflection point at 3.53, indicating that patients with DFI have a lower risk of severe infection when SIRI is below this threshold. This newly identified phenomenon should help facilitate early interventions and the development of personalized treatment strategies for patients with DFU, thereby making amputation less likely.
The present study has three principal strengths. First, the sample size was adequate, and the data collected were reliable and quite extensive. Second, we controlled for the influence of potential confounding factors through the use of multifactor logistic regression and sensitivity analyses. Third, we identified a novel means of comprehensively assessing the link between the inflammatory and immune state and the risk of severe DFI. Moreover, the components of SIRI, namely NEU, LYM, and MON counts, can be readily and inexpensively assessed in clinical settings, making SIRI of significant practical value.
It is also important to acknowledge the limitations of the present study. First, the study sample was drawn from a single institution, which limits the generalizability of the findings. Second, although we used multiple methods to control for confounding, unmeasured biases remain. To evaluate the clinical utility of SIRI in greater depth, it is essential that prospective studies with larger sample sizes should be conducted.
Conclusion
We have identified a nonlinear association between SIRI and the risk of severe DFI occurrence, with an inflection point of approximately 3.53: when SIRI is <3.53, there is a lower risk of severe DFI. Maintaining an appropriate SIRI level is crucial for DFI patients. Patients with SIRI>3.53 had a significantly higher prevalence of severe DFI compared with those with SIRI<3.53. SIRI can be calculated using parameters that are routinely measured in a blood sample; therefore, it is a practical and affordable index. Further multicenter, prospective studies are needed to confirm these results.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
This study has been approved by the Ethics Review Committee of Changzhou First People’s Hospital (Approval No.: 2025175) and fully complies with the ethical principles outlined in the Declaration of Helsinki and its subsequent revisions. Due to the retrospective nature of the research utilizing biobank-stored serum samples, informed consent was waived by the approving institution. All data were handled with strict confidentiality to ensure the anonymity of participants.
Acknowledgments
We would like to express our gratitude to all colleagues who provided invaluable guidance during the writing of this article. Furthermore, we extend our thanks to all participants who took part in this study.
Author Contributions
Ping Wu: Conceptualization, Funding acquisition, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. Wendong Xu: Data curation, Formal analysis, Resources, Validation, Writing – original draft. Rui Chen: Formal analysis, Investigation, Methodology, Resources, Software, Writing – original draft. Zhenghui Xu: Conceptualization, Investigation, Project administration, Validation, Writing – review and editing. All authors have agreed on the journal to which the article will be submitted. All authors reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. All authors agree to take responsibility and be accountable for the contents of the article.
Funding
This study was supported by the Changzhou Science and Technology Program (Grant Number: CJ20242025) and the Major Science and Technology Projects of Changzhou Health Commission (Grant Number: ZD202425).
Disclosure
Mr Wendong Xu reports grants from Changzhou Science and Technology Bureau, grants from Changzhou Health Commission, during the conduct of the study; Mr Zhenghui Xu reports grants from Changzhou Science and Technology Program, grants from Major Science and Technology Projects of Changzhou Health Commission, during the conduct of the study; All authors declare no other conflicts of interest for this study.
References
1. Armstrong DG, Tan TW, Boulton AJM, Bus SA. Diabetic Foot Ulcers: a Review. JAMA. 2023;330(1):62–13. doi:10.1001/jama.2023.10578
2. Jia L, Parker CN, Parker TJ, et al. Incidence and risk factors for developing infection in patients presenting with uninfected diabetic foot ulcers. PLoS One. 2017;12(5):e0177916. doi:10.1371/journal.pone.0177916
3. Ndosi M, Wright-Hughes A, Brown S, et al. Prognosis of the infected diabetic foot ulcer: a 12-month prospective observational study. Diabet Med. 2018;35(1):78–88. doi:10.1111/dme.13537
4. Kosaji D, Awad MI, Katmah R, et al. Diabetic foot prevention, assessment, and management using innovative smart wearable technology: a systematic review. J Neuroeng Rehabil. 2025;22(1):168. doi:10.1186/s12984-025-01695-9
5. Liu J, Song Q, Yin W, et al. Bioactive scaffolds for tissue engineering: a review of decellularized extracellular matrix applications and innovations. Exploration. 2025;5(1):20230078. doi:10.1002/EXP.20230078
6. Xie H, Wang Z, Wang R, Chen Q, Yu A, Lu AS. Injectable Hydrogel Dressing for Monitoring and Therapy of Diabetic Wound. Adv Funct Mater. 2024;34(36). doi:10.1002/adfm.202401209
7. Liu ZQ, Yi S, Yang ZL, Deng ZH. Hydrogel-exosome systems in the treatment of refractory diabetic ulcers: mechanisms, progress, and prospects. Eur Cells Mater. 2025;53:82–97. doi:10.22203/eCM.v053a07
8. Zha X. Challenges and opportunities for repairing the injured spinal cord: inflammation, regeneration, and functional reconstruction. Regenerative Medicine Reports. 2025;2(1):36–44. doi:10.4103/regenmed.Regenmed-d-24-00027
9. Fu H, Liu Y. Complex gut–brain interactions underlying inflammatory bowel disease-related depression have translational implications in regenerative medicine: a narrative review. Regenerative Medicine Reports. 2024;1(1):59–75. doi:10.4103/regenmed.Regenmed-d-24-00006
10. Lv S, Tian X, Yang S, Sun J, Wei Z. Shared genetic architecture between early-onset osteoarthritis and multiple sclerosis: evidence from a large-scale genome-wide cross-trait analysis and validation research techniques. Adv Technol Neurosci. 2026;3(1):7–15. doi:10.4103/atn.Atn-d-25-00019
11. Shofler D, Rai V, Mansager S, Cramer K, Agrawal DK. Impact of resolvin mediators in the immunopathology of diabetes and wound healing. Expert Rev Clin Immunol. 2021;17(6):681–690. doi:10.1080/1744666X.2021.1912598
12. Qi X, Shi Y, Zhang C, et al. A Hybrid Hydrogel with Intrinsic Immunomodulatory Functionality for Treating Multidrug-Resistant Pseudomonas aeruginosa Infected Diabetic Foot Ulcers. ACS Mater Lett. 2024;6(7):2533–2547. doi:10.1021/acsmaterialslett.4c00392
13. Cheng S, Wang H, Pan X, et al. Dendritic Hydrogels with Robust Inherent Antibacterial Properties for Promoting Bacteria-Infected Wound Healing. ACS Appl Mater Interfaces. 2022;14(9):11144–11155. doi:10.1021/acsami.1c25014
14. Wang Z, Qi B, Wang R, et al. Smart eutectogel with antibacterial activity for efficiently treating multidrug resistant infection, real-time monitoring and diabetic wound repair. Chem Eng J. 2025:520. doi:10.1016/j.cej.2025.166108.
15. Qi X, Li Y, Xiang Y, et al. Hyperthermia-enhanced immunoregulation hydrogel for oxygenation and ROS neutralization in diabetic foot ulcers. Cell Biomaterials. 2025;1(3). doi:10.1016/j.celbio.2025.100020
16. Palabiyik AA, Palabiyik E. Interleukin-33 in the Regulation of Autophagy and Apoptosis in Macrophages During Infection. Immunol Invest. 2025;54(8):1309–1325. doi:10.1080/08820139.2025.2547691
17. Cai Z, Qiao T, Chen Y, Xie M, Zhou J. The association between systemic inflammatory response index and in-hospital mortality in patients with infective endocarditis. Clin Cardiol. 2022;45(6):664–669. doi:10.1002/clc.23829
18. Islam MM, Watanabe E, Salma U, et al. Immunoadjuvant therapy in the regulation of cell death in sepsis: recent advances and future directions. Front Immunol. 2024;15:1493214. doi:10.3389/fimmu.2024.1493214
19. Lee H, Kim I, Kang BH, Um SJ. Prognostic value of serial neutrophil-to-lymphocyte ratio measurements in hospitalized community-acquired pneumonia. PLoS One. 2021;16(4):e0250067. doi:10.1371/journal.pone.0250067
20. Aragon-Sanchez J, Viquez-Molina G, Lopez-Valverde ME, Rojas-Bonilla JM. Systemic Immune-Inflammation Index in Diabetic Foot Infections and Osteomyelitis. Int J Low Extrem Wounds. 2025;24(4):1278–1280. doi:10.1177/15347346231179280
21. Ge Y, Hu D, Wang Z, Zhang C. Association between the nutritional inflammation index and mortality among patients with sepsis: insights from traditional methods and machine learning-based mortality prediction. BMC Infect Dis. 2025;25(1):1021. doi:10.1186/s12879-025-11429-w
22. Yang F, Dong R, Wang Y, et al. Prediction of pulmonary infection in patients with severe myelitis by NPAR combined with spinal cord lesion segments. Front Neurol. 2024;15:1364108. doi:10.3389/fneur.2024.1364108
23. Rutenberg TF, Gabarin R, Kilimnik V, et al. Nutritional and Inflammatory Indices and the Risk of Surgical Site Infection After Fragility Hip Fractures: can Routine Blood Test Point to Patients at Risk? Surg Infect. 2023;24(7):645–650. doi:10.1089/sur.2023.118
24. Xu T, Song S, Zhu K, et al. Systemic inflammatory response index improves prognostic predictive value in intensive care unit patients with sepsis. Sci Rep. 2025;15(1):1908. doi:10.1038/s41598-024-81860-7
25. Zhu Y, Wang Z, Li S, et al. Prognostic Value of SIRI in Sepsis: a Retrospective Study and Machine Learning-Based Model Development. J Inflamm Res. 2025;18:13609–13623. doi:10.2147/JIR.S536139
26. Hu Y, Xiong F, Zhao L, et al. Association Between Systemic Inflammatory Response index and Diabetic Foot Ulcer in the US Population with Diabetes in the NHANES: a Retrospective Cross-Sectional Study. Int J Low Extrem Wounds. 2025;24(3):611–620. doi:10.1177/15347346251324478
27. Senneville E, Albalawi Z, van Asten SA, et al. IWGDF/IDSA guidelines on the diagnosis and treatment of diabetes-related foot infections (IWGDF/IDSA 2023). Diabetes Metab Res Rev. 2024;40(3):e3687. doi:10.1002/dmrr.3687
28. Yan D, Wang S. Systemic inflammation response index (SIRI)-based risk of pneumonia following successful PCI in STEMI patients. Ann Med. 2025;57(1). doi:10.1080/07853890.2025.2462449
29. Shao L, Yu B, Lyu Y, Fan S, Gu C, Wang H. The Clinical Value of Novel Inflammatory Biomarkers for Predicting Mycoplasma pneumoniae Infection in Children. J Clin Lab Anal. 2025;39(3):e25150. doi:10.1002/jcla.25150
30. Farahani A, Farahani A, Kashfi K, Ghasemi A. Inhibition of hepatic gluconeogenesis in type 2 diabetes by metformin: complementary role of nitric oxide. Med Gas Res. 2025;15(4):507–519. doi:10.4103/mgr.MEDGASRES-D-24-00100
31. Bahadoran Z, Mirmiran P, Hosseinpanah F, Kashfi K, Ghasemi A. Nitric oxide-based treatments improve wound healing associated with diabetes mellitus. Med Gas Res. 2025;15(1):23–35. doi:10.4103/mgr.MEDGASRES-D-24-00020
32. Foo XY, Lee LK. Medical gas therapy in human diabetic wound healing. Med Gas Res. 2025;15(2):212–213. doi:10.4103/mgr.MEDGASRES-D-24-00125
33. Zhang Z, Li C, Xiao Y, et al. Integrated machine learning and population attributable fraction analysis of systemic inflammatory indices for mortality risk prediction in diabetes and prediabetes. Ann Med. 2025;57(1):2536204. doi:10.1080/07853890.2025.2536204
34. Cho H, Blatchley MR, Duh EJ, Gerecht S. Acellular and cellular approaches to improve diabetic wound healing. Adv Drug Deliv Rev. 2019;146:267–288. doi:10.1016/j.addr.2018.07.019
35. Islam MM, Satici MO, Eroglu SE. Unraveling the clinical significance and prognostic value of the neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, systemic immune-inflammation index, systemic inflammation response index, and delta neutrophil index: an extensive literature review. Turk J Emerg Med. 2024;24(1):8–19. doi:10.4103/tjem.tjem_198_23
36. Hamad DA, Aly MM, Abdelhameid MA, et al. Combined Blood Indexes of Systemic Inflammation as a Mirror to Admission to Intensive Care Unit in COVID-19 Patients: a Multicentric Study. J Epidemiol Glob Health. 2022;12(1):64–73. doi:10.1007/s44197-021-00021-5
37. Li S, Liu J, Wu J, Zheng X. Immunological Mechanisms and Effects of Bacterial Infections in Acute-on-Chronic Liver Failure. Cells. 2025;14(10):718. doi:10.3390/cells14100718
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.