Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Association Between Subsegmental Dosing Accuracy and Outcomes of Bronchoscopic Thermal Vapor Ablation: An Exploratory Retrospective Study in Severe Heterogeneous Emphysema
Authors Yang H, Chen S, Zheng X, Cui N, Xie F, Hou H, Ye L, Herth FJF ![]() , Sun J
, Sun J ![]()
Received 13 August 2025
Accepted for publication 12 January 2026
Published 23 January 2026 Volume 2026:21 560457
DOI https://doi.org/10.2147/COPD.S560457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vanesa Bellou
Han Yang,1,* Si Chen,2,3,* Xiaoxuan Zheng,2,3,* Ningxin Cui,1 Fangfang Xie,2,3 Huan Hou,2,3 Lin Ye,2,3 Felix J F Herth,4,5 Jiayuan Sun1– 3
1Department of Respiratory and Critical Care Medicine, Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2Department of Respiratory Endoscopy, Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 3Shanghai Engineering Research Center of Respiratory Endoscopy, Shanghai, People’s Republic of China; 4Pneumology and Critical Care Medicine, Thoraxklinik, University of Heidelberg, Heidelberg, Germany; 5Translational Lung Research Center Heidelberg, German Center for Lung Research, Heidelberg, Germany
*These authors contributed equally to this work
Correspondence: Jiayuan Sun, Department of Respiratory Endoscopy, Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200030, People’s Republic of China, Email [email protected] Felix J F Herth, Pneumology and Critical Care Medicine, Thoraxklinik, University of Heidelberg, Heidelberg, 69126, Germany, Email [email protected]
Purpose: Bronchoscopic thermal vapor ablation (BTVA) is a minimally invasive treatment for severe emphysema. However, the treatment doses are typically generated at the segmental level. In specific cases, treatment needs to be conducted at the subsegmental level, and the proportion can only be roughly allocated based on CT image review, potentially leading to dose mismatch. This retrospective exploratory study investigated the relationship between subsegmental dose accuracy (theoretical-to-actual matching) and clinical outcomes following BTVA.
Methods: Patients who underwent BTVA at the Shanghai Chest Hospital between 2023 and 2024 were analyzed. Subsegmental theoretical doses (BroncQCT software) were compared to previously administered actual treatment doses. Dose matching was defined as: 1) segmental treatments were presumed matched (uniform vapor assumption), 2) subsegmental treatments required ≤ 10% deviation between actual and theoretical dose ratios (|Actual ratio - Theoretical ratio| × 100%). Patients with > 10% deviation or BroncQCT-identified nontarget subsegments were unmatched. Clinical parameters at 1, 3, 6, and 12 months after single treatment were compared.
Results: Among 21 patients (15 matched, 6 unmatched), the mean changes in FEV1 for the overall cohort were +70mL at 1 month (n = 19, P = 0.018), +90mL at 3 months (n = 14, P = 0.056), and +130mL at 6 months (n = 8, P = 0.015). The matched group demonstrated superior median increases compared to unmatched patients (+150mL [n = 9] vs +10mL [n = 5]; P = 0.012) at 3 months where between-group differences were maximal. Similar trends were observed at 1 month (median +110mL [n = 14] vs 0mL [n = 5]; P = 0.044) and 6 months (median +150mL [n = 5] vs +60mL [n = 3]; P = 0.036). Adverse events (including two late deaths in comorbid patients) were documented, though small sample sizes prevent definitive safety conclusions.
Conclusion: This exploratory study found that subsegmental dose matching was associated with greater FEV1 changes after BTVA. These hypothesis-generating findings require prospective validation in a randomized controlled trial (NCT06152107).
Keywords: bronchoscopic thermal vapor ablation, BTVA, chronic obstructive pulmonary disease, COPD, emphysema, bronchoscopic lung volume reduction, BLVR
Introduction
Chronic obstructive pulmonary disease (COPD) is a major cause of morbidity, disability, and mortality worldwide,1 primarily manifests as chronic bronchitis and emphysema.2 The main characteristics of the emphysema phenotype are progressive enlargement of the airspaces and destruction of alveoli, resulting in a reduced surface area for gas exchange, leading to progressive dyspnea and decreased quality of life.3,4 Conventional pharmacological treatments for COPD have limited efficacy in severe emphysema.5 Lung volume reduction surgery (LVRS) was initially proposed as the treatment option for emphysema.6 This surgical procedure entails removal of the most severely damaged lung regions, allowing healthier lung tissue to function more efficiently.7 Despite substantial evidence supporting the effectiveness of LVRS, its adoption remains limited,8 likely due to the associated surgical risks,9 and there has been growing interest in nonsurgical alternatives that can provide similar benefits.8 Recently, bronchoscopic lung volume reduction (BLVR) techniques have gained increasing attention. These techniques include bronchoscopic thermal vapor ablation (BTVA), endobronchial valves (EBV),10,11 and lung volume reduction coils (LVRC),12,13 all of which are recommended by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines14 to reduce hyperinflation in severe emphysema.
BTVA is a minimally invasive technique for severe emphysema. This procedure delivers heated water vapor via bronchoscopy, inducing a localized inflammatory response that reduces the volume of emphysematous segments.15 Unlike EBV and LVRC, BTVA requires no foreign device implantation, distinguishing its approach and avoiding long-term implant management. By reducing the volume of severely affected emphysematous regions, BTVA has the potential to improve lung function, as evidenced by the STEP-UP study, which found an average relative increase of 14.7% in forced expiratory volume in 1 second (FEV1) and a decrease of 9.7 points in St George’s Respiratory Questionnaire for COPD Patients (SGRQ-C) score after 6 months.9 In patients with collateral ventilation (CV), BTVA led to a 9.2% improvement in FEV1 at 12 months, compared to a 5.4% decrease in the control group (between-group difference of 14.6%).16 Whereas STEP-UP established the benefits of segmental-level targeting by addressing interlobar heterogeneity, this approach ignored existing subsegmental heterogeneity, which might even affect vapor distribution and therapeutic outcomes.
Previous studies have focused on BTVA treatment at the segmental level, targeting the most severely affected lung segments. In certain cases, treatment was administered to the subsegments due to a short segmental bronchus, large segment volume (>10s vapor delivery, exceeding the device’s single-dose limit), or unfavorable catheter angle raising concerns of uneven vapor distribution. However, emphysema severity varies markedly among subsegments within a single segment, implying that subsegmental heterogeneity critically influences the treatment outcomes. Notably, subsegmental therapy dosing was often guided by computed tomography (CT) estimates, not precise measurements, risking unmatched dosing. Recent advances in quantitative CT (QCT) software (eg, BroncQCT) now enable precise subsegmental-level emphysema quantification and theoretical vapor dose calculation, providing a tool to optimize targeting. In this study, we conducted a QCT-based subsegmental analysis to retrospectively evaluate whether more accurate treatment dosing at this level is associated with patient outcomes.
Methods
Study Population
This retrospective study included all patients who underwent BTVA treatment at Shanghai Chest Hospital between January 2023 and December 2024. To reflect real-world clinical practice, no formal inclusion/exclusion criteria were applied at the screening stage, all BTVA cases performed during this period were systematically captured in the study. Patient selection for BTVA at our center was primarily based on comprehensive evaluation incorporating key criteria, including (1) heterogeneous emphysema with HI (Heterogeneity Index) ≥1.2, (2) hyperinflation (RV/TLC >55% and RV >150% predicted), (3) Severe to very-severe airflow obstruction (GOLD grades 3–4), and (4) no respiratory infections or COPD exacerbations within 4 weeks prior to the procedure.
This retrospective study was approved by the Ethics Committee of Shanghai Chest Hospital (No. IS25023) in accordance with the Declaration of Helsinki, with waiver of informed consent granted for retrospective data analysis.
Data Collection
Patients were routinely suggested to undergo follow-up visits at 1, 3, 6, and 12 months postoperatively. Baseline and follow-up data were collected, including demographic characteristics, imaging findings, pulmonary function test results [FEV1, forced vital capacity (FVC), residual volume (RV), and total lung capacity (TLC)], 6-minute walking test (6MWT) measured by certified pulmonary function technicians according to ATS guidelines (2002),17 and symptom scores [using validated Mandarin Chinese versions: the COPD Assessment Test (CAT) and modified Medical Research Council (mMRC) dyspnea scale from the Chinese COPD Guidelines (2021),18 and St. George’s Respiratory Questionnaire (SGRQ) China /Mandarin Chinese version - “Past 4 weeks” version]. To ensure comparability, only the data collected after a single treatment were compared, despite some patients having undergone sequential treatment. All adverse events were retrospectively graded according to CTCAE v5.0 criteria19 and classified as early phase (0–30 days post-BTVA) or late phase (31–365 days) based on documented occurrence. Events were independently adjudicated by two senior pulmonologists with cross-verification to ensure consensus.
Consistent with prior studies,9,20,21 we also analyzed the proportion of patients achieving the minimal clinically important difference (MCID) for key endpoints: FEV1% (≥12%), FEV1 (≥0.1L), SGRQ (≤-8 points), and 6MWT (≥26 m).
BTVA Treatment
The BTVA procedure utilized the InterVapor® system, developed by Uptake Medical Technology, Inc. (Seattle, WA, USA) and is now owned by Hangzhou Broncus Medical Co., Ltd. (Hangzhou, Zhejiang, China). Pre-procedural High-Resolution CT (HRCT) scans were acquired following the Broncus Medical InterVapor CT Scan Protocol (detailed parameters in Supplementary File S1). Scans were analyzed using a quantitative CT software to determine the treatment area and vapor dose. Under general anesthesia, an InterVapor catheter was introduced into the target area via the bronchoscope. After balloon inflation for airway sealing, heated sterile water vapor was delivered. In certain cases, treatment was administered to each subsegment of the target lung segment for the aforementioned reasons. For patients prior to the implementation of the precise subsegmental analysis, physicians determined subsegmental vapor dose distribution empirically based on CT findings. For patients following the implementation of the subsegmental analysis, software-guided dose allocation was implemented.
Grouping Based on Dose Matching
BroncQCT software (Hangzhou Broncus Medical Co., Ltd., Zhejiang, China, version 1.0.3) can calculate the tissue volume, air volume, and low-attenuation area at −950 HU (LAA-950) at both the segmental and subsegmental levels. All automated segmentations at these levels were mandatorily reviewed and confirmed by an experienced bronchoscopist before formal analysis. In addition, the software provides calculations for the theoretical vapor dose, targeting the optimal thermal ablation (8.5 cal/g), with detailed computational methodology described in our published protocol.22
To evaluate the accuracy of subsegmental dosing, we categorized patients into matched and unmatched groups based on BroncQCT-guided theoretical dosing versus actual clinical delivery. For segmental treatments, we assumed a uniform vapor distribution (matched by default). For subsegmental treatments, we assessed matching using the dose-ratio difference method:
- Actual dose ratio: dose to subsegment A/subsegment B (per procedural record).
- Theoretical dose ratio: dose of subsegment A/subsegment B (per BroncQCT calculation).
- Mismatch threshold: Cases with |Actual dose ratio − theoretical dose ratio|× 100% >10% were classified as unmatched. Patients with any subsegment(s) deemed unnecessary for treatment by BroncQCT analysis were also unmatched.
Example Case
- Actual dose ratio: 5.2s (RB1a) / 5.2s (RB1b) = 1.
- Theoretical dose ratio: 4.3s (RB1a) / 7.1s (RB1b) = 0.61.
- Mismatch calculation: |1.0−0.61| × 100% = 39% (>10% was classified as unmatched).
An overview of the patient’s lung treatment is shown in Figure 1a, and a focused subsegmental analysis of RB1 is shown in Figure 1b.
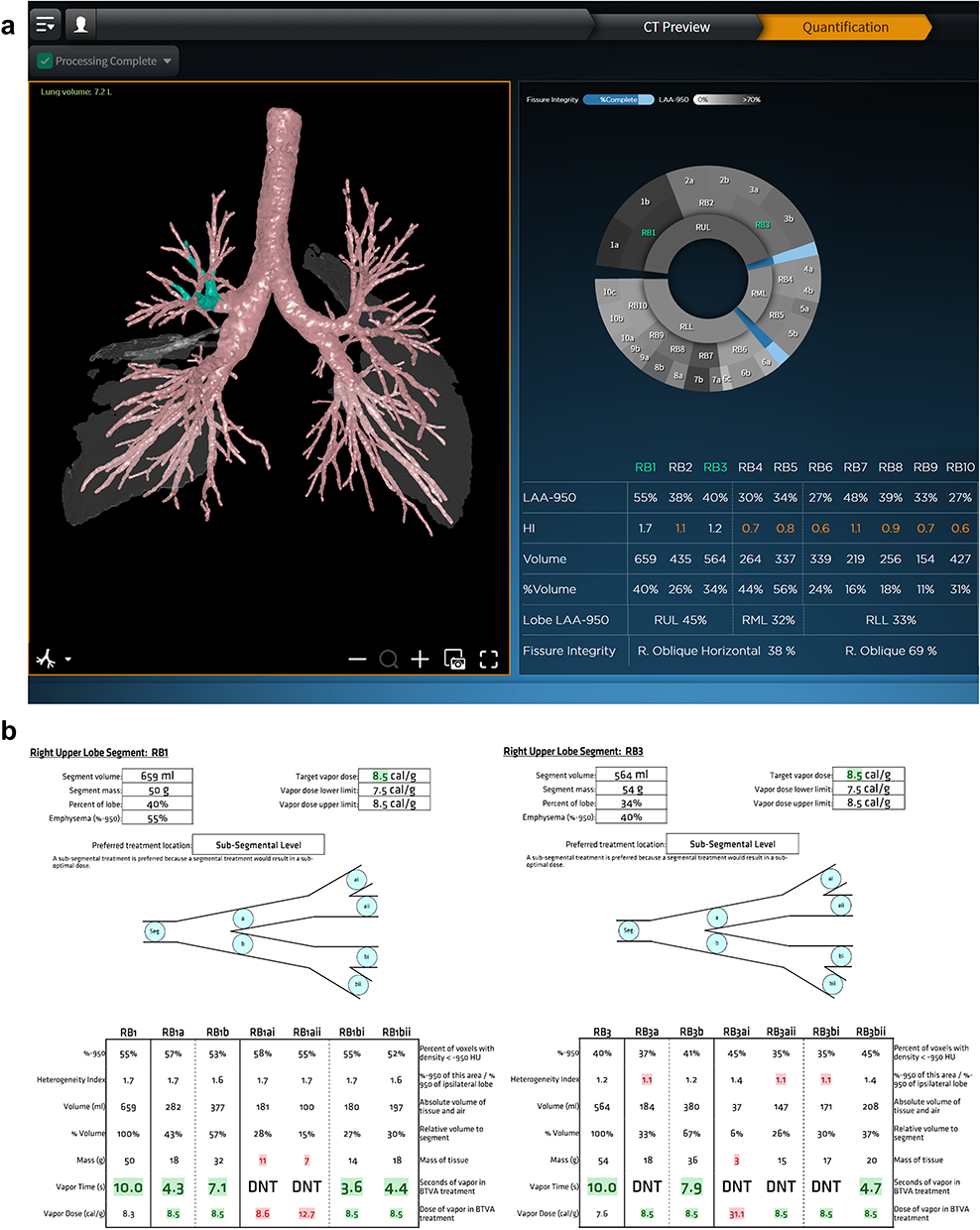 |
Figure 1 BroncQCT Analysis Results. (a) Lung segment treatment overview; (b) Subsegmental analysis of RB1 and RB3. Abbreviation: DNT, Do Not Treat. |
Statistics
Descriptive statistics for baseline characteristics are presented as mean ± standard deviation (SD) for normally distributed data and median (IQR) for non-normal data. Efficacy analysis was performed to compare baseline and post-treatment changes using paired t-tests (normal data) or paired Wilcoxon signed-rank tests (non-normal data). Between-group comparisons (matched vs unmatched) were performed using the Mann–Whitney U-test for variables (expressed as median [IQR]) and Fisher’s exact test for adverse events. Within-group comparisons were performed using a paired Wilcoxon signed-rank test. Correlation analyses between mismatch degree and other parameters were conducted using Spearman’s rank correlation. Effect sizes for between-group comparisons were quantified using Cliff’s Delta (95% CI; calculated via the function cliff.delta in the R package effsize 0.8.1). For multiple testing corrections, false discovery rate (FDR)-adjusted p-values were generated using the Benjamini-Hochberg method (implemented via R function p.adjust). Potential confounding factors were addressed using linear mixed-effects models. All analyses were performed using SPSS 24.0 (IBM, Armonk, NY, USA) and R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria), with two-tailed tests and statistical significance set at P < 0.05.
Results
Twenty-one patients underwent BTVA treatment at the Shanghai Chest Hospital between January 2023 and December 2024. At the 1-month follow-up, 2 patients missed visits and 1 lacked questionnaire data. By 3 months, 2 patients had undergone the second BTVA procedure (excluded from analysis), 5 had missed visits, and 2 lacked CT data. At 6 months, 4 patients underwent the second procedure, 1 died, 4 missed visits, and 4 provided questionnaires only. By 12 months, 7 underwent the second procedure, 2 died, 6 missed visits, and 1 provided questionnaires only. Detailed individual patient follow-up records are presented in Supplementary File S2, Table S1. Pulmonary function tests consistently included FEV1 and FVC, although the RV and TLC data were incomplete.
Baseline Characteristics
The baseline characteristics of the patients are summarized in Table 1. All 21 patients were male, with a median age of 69 years and mean BMI of 22.48 kg/m2. Importantly, these patients had severe airflow limitation (mean FEV1% 28.25%±8.82%, range 11–44.8%); FEV1% was >15% in all but one patient, with the most severe case at 11%. All patients demonstrated significant hyperinflation (RV ≥150%) and clinically significant dyspnea (mMRC ≥ 2), consistent with an advanced disease.
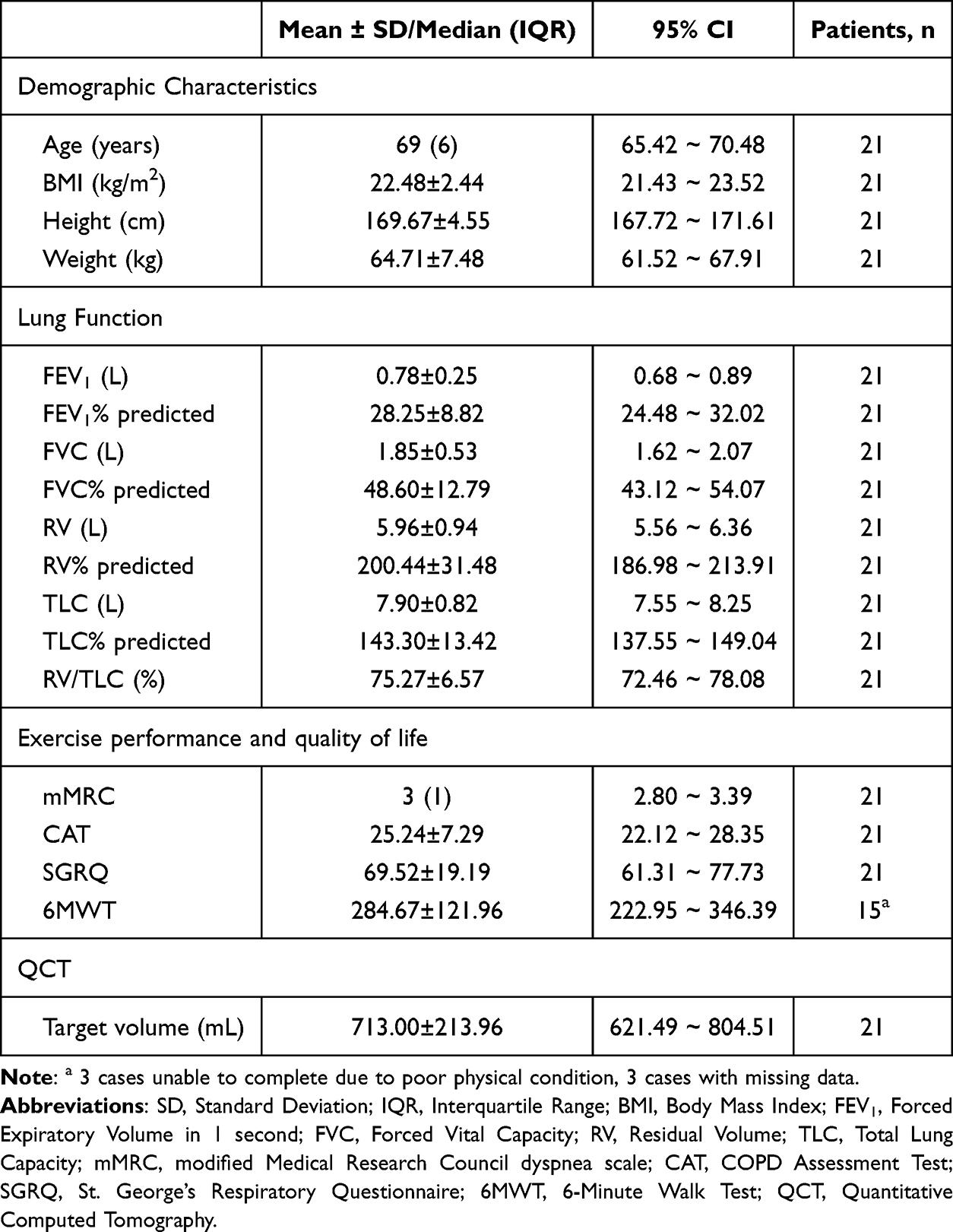 |
Table 1 Baseline Characteristics |
Efficacy Outcomes
Changes in pulmonary function, exercise performance, quality of life, and target lung volume at 1, 3, 6, and 12 months post-treatment relative to baseline are shown in Table 2 and Figure 2. The changes in FEV1 at 1 and 6 months post-treatment was statistically significant, with mean increases of 70 mL (n = 19) and 130 mL (n = 8), respectively. SGRQ scores showed significant changes at all time points (1, 3, 6, and 12 months), with mean changes of −17.62 (n = 18), −11.16 (n = 14), −14.32 (n = 12), and −20.02 (n = 6), respectively. Additionally, the target lung volume, as assessed using QCT, demonstrated significant changes at 1, 3, 6, and 12 months post-treatment, with median changes of −168.50 mL (n = 18), −148.50 mL (n = 12), −157.00 mL (n = 7), and −109.00 mL (n = 6), respectively.
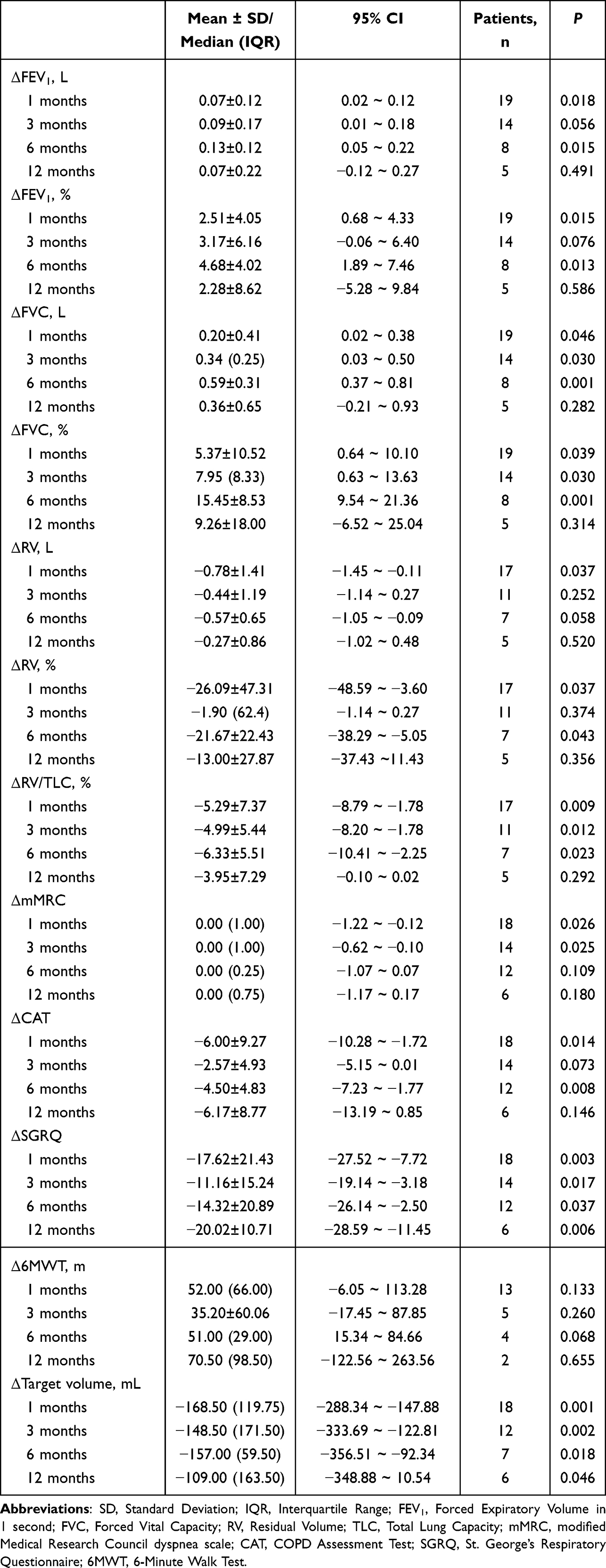 |
Table 2 Efficacy Outcomes of BTVA |
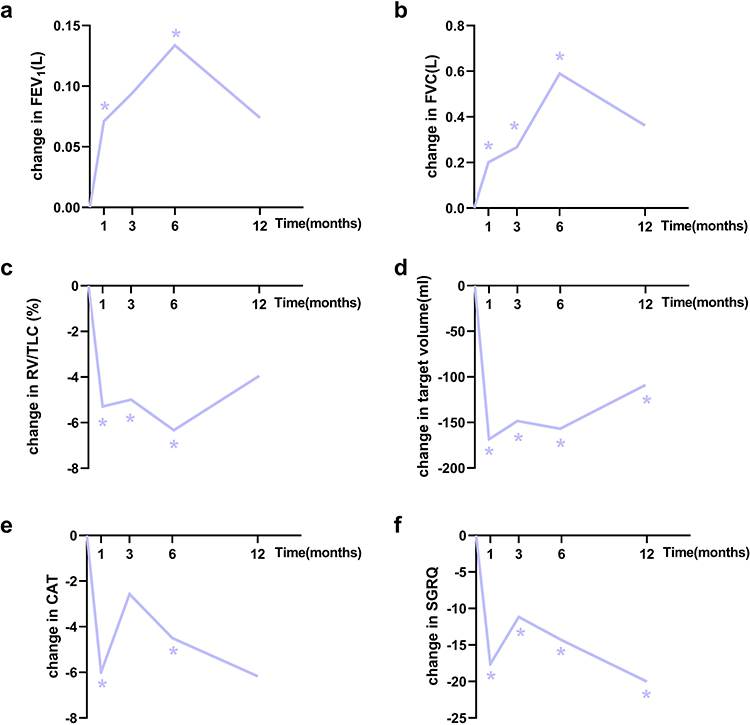 |
Figure 2 Changes in clinical outcomes compared to baseline. The line graph showing changes in (a) FEV1, (b) FVC, (c) RV/TLC, (d) target volume, (e) CAT, and (f) SGRQ at 1, 3, 6, and 12 months. All values are presented as means, except for target volume, which is presented as the median. *indicates a statistically significant change compared to baseline. |
Baseline Comparison Between Matched and Unmatched Groups
The study included 21 patients: 7 treated at the segmental level and 14 at the subsegmental level (8 pre-implementations and 6 post-implementations of precise subsegmental analysis). 6 pre-implementation subsegmental cases showed a >10% absolute difference between the actual and theoretical dose ratios (unmatched group), whereas the remaining 8 subsegmental and 7 segmental cases comprised the matched group (n = 15).
Baseline characteristics (Table 3) revealed no significant differences in lung function, such as FEV1, FVC, RV, RV/TLC, or target volume, between the groups. However, a significant age difference was found, with median ages of 68 years and 73 years in the matched and unmatched groups, respectively. Additionally, the mMRC scores differed significantly, with median scores of 3 in the matched group (n = 15) and 4 in the unmatched group (n = 6).
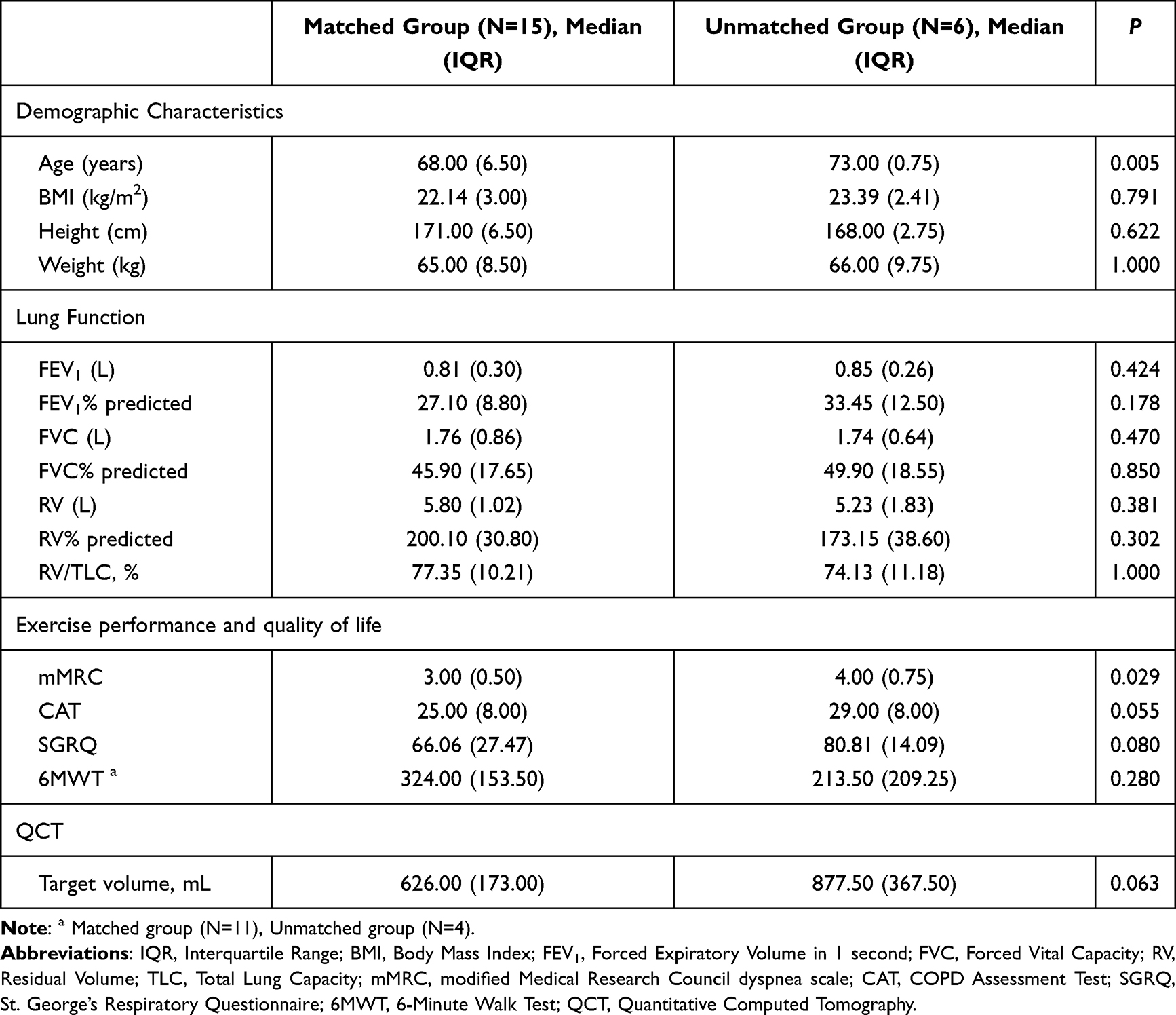 |
Table 3 Baseline Characteristics Between Matched and Unmatched Groups |
Comparison of Efficacy Outcomes Between Matched and Unmatched Groups
The matched group showed significantly greater median changes in FEV1 than the unmatched group at 1 month (+110 mL [n = 14] vs 0 mL[n = 5]; P = 0.044), 3 months (+150 mL [n = 9] vs +10 mL [n = 5]; P = 0.012), and 6 months (+150 mL [n = 5] vs +60 mL [n = 3]; P = 0.036) post-treatment (Table 4). Changes from baseline in FEV1, FVC, RV/TLC, and CAT at 1, 3, 6, and 12 months post-treatment in both the groups are shown in Figure 3. While non-significant, consistent directional trends were observed in the matched group for FVC changes (3-month: +0.39L [n = 9] vs +0.16L [n = 5], P = 0.147), RV/TLC changes (3-month: −5.88% [n = 7] vs −3.46% [n = 4], P = 0.273) and CAT score changes (1-month: −5 [n = 13] vs +3 [n = 5], P = 0.059). The complete data are presented numerically in Table 4 and visually in Figure 3.
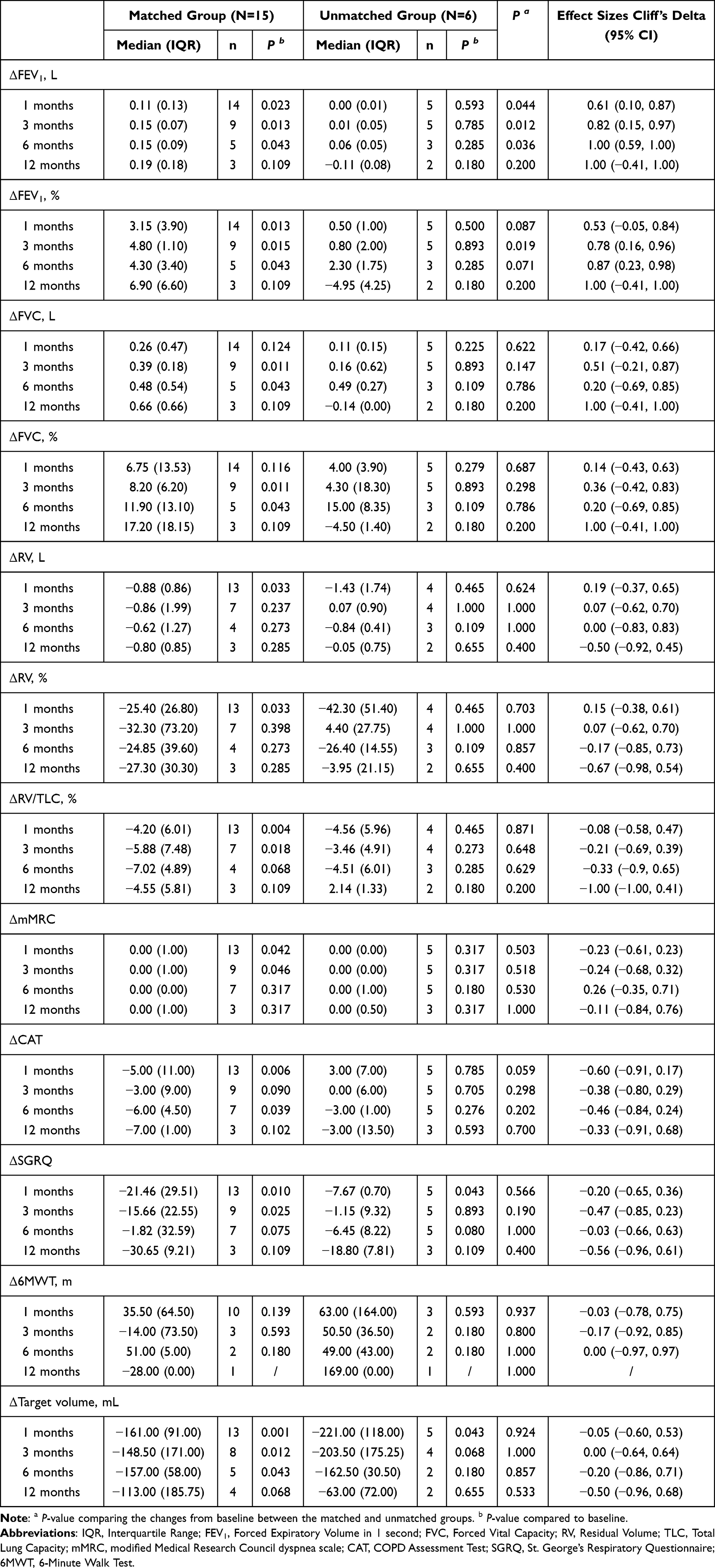 |
Table 4 Efficacy Outcomes Between Matched and Unmatched Groups |
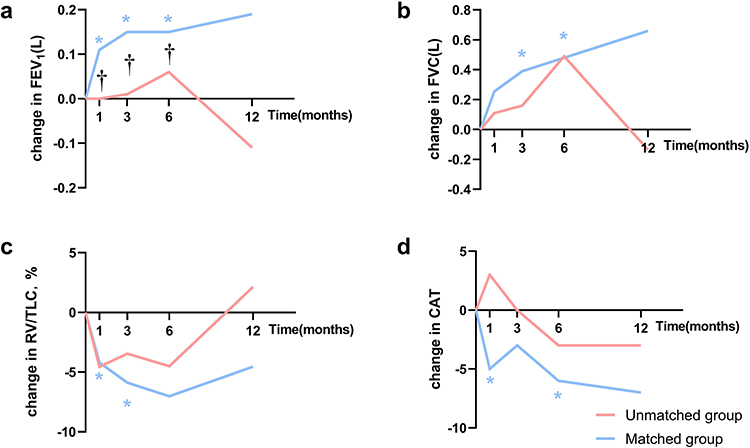 |
Figure 3 Clinical outcomes in matched and unmatched groups. The line graph illustrates changes in (a) FEV1, (b) FVC, (c) RV/TLC, and (d) CAT at 3, 6, and 12 months for both matched and unmatched groups. All values are presented as medians. The blue * indicate a statistically significant change from baseline in the matched group; the black † indicates a statistically significant difference between the matched and unmatched groups. |
Although only a few comparisons between the two groups showed statistically significant differences, the trends observed in the line graphs suggested that the matched group generally exhibited better outcomes. Additionally, we assessed correlations between mismatch degree and changes in FEV1, FVC, RV/TLC, and CAT scores (Supplementary File S2, Figure S1). FEV1 improvement tended to demonstrate stronger negative correlations with mismatch degree than other parameters. Binary responder analyses for FEV1, SGRQ, and 6MWT are summarized in Supplementary File S2, Table S2. At 3 months post-procedure, 78% (7/9) of patients in the matched group achieved a clinically significant FEV1 improvement (≥0.1 L), compared to 0% (0/5) in the unmatched group.
To assess the robustness of our primary findings, sensitivity analysis using a 15% mismatch threshold (Supplementary File S2, Table S3) demonstrated consistent therapeutic differences between matched and unmatched groups. Importantly, this analysis revealed statistically significant difference in CAT scores at 1-month post-procedure (P = 0.038).
Given the observed baseline differences in age and mMRC scores between groups, we performed adjusted analyses using linear mixed-effects models controlling for these covariates. The adjusted models revealed a statistically significant difference in CAT scores at 1 month (adjusted P = 0.04) while other outcome differences became non-significant compared to unadjusted analyses, detailed results are presented in Supplementary File S2, Table S4. Since this was an exploratory analysis without prespecified endpoints, we applied FDR correction to account for multiple comparisons. All between-group differences became nonsignificant after adjustment (Supplementary File S2, Table S5), but we present these results for transparency.
Safety Outcomes
Adverse events are summarized in Table 5. Hemoptysis occurred in 6 patients (28.6%) within the first week post-treatment, all of which resolved completely after oral administration of Yunnan Baiyao or Carbazochrome Tablets. Other adverse events included exacerbation of COPD (19.0%), pneumonia (9.5%), increased dyspnea (9.5%), increased sputum production (9.5%), and chest pain (4.8%). Most cases occurred within the first month and responded well to treatment with no significant between-group differences.
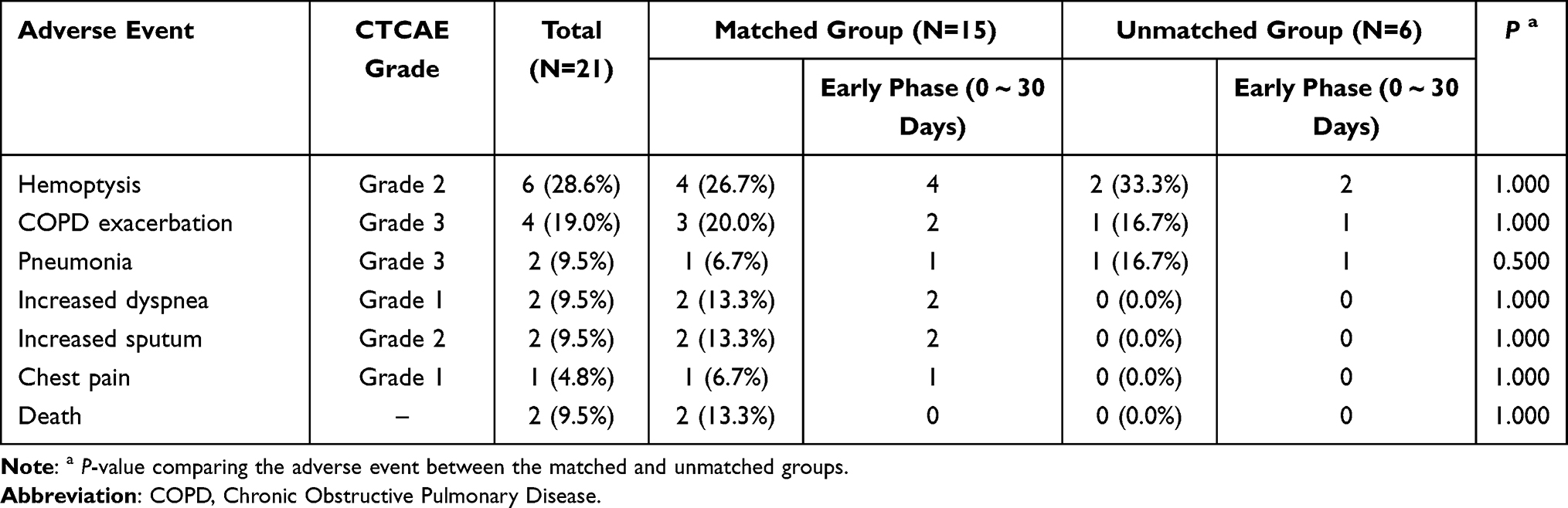 |
Table 5 Adverse Events |
Two deaths were reported, first at 4 months and the second at 11 months. The first patient (male, 68 years old) had severely impaired baseline pulmonary function (FEV1 21.2%, DLCO 38.1%), high symptom burden (mMRC 4, CAT 29), and comorbidities (coronary atherosclerosis, pulmonary hypertension). At the 1- and 3-month follow-ups, FEV1 increased by 2.8% and 4.8%, respectively, from baseline. The second patient (male, 70 years old), with severe baseline impairment (FEV1 32.8%, DLCO 31.4%) and comorbidities (diabetes and hypertension), demonstrated early post-treatment improvement (FEV1 +5.2%, 6 MWT +52m at 1 month). Causality assessment (procedure-relatedness) was not formally adjudicated in this study, consistent with its retrospective exploratory design.
Discussion
Patients with COPD often continue to deteriorate despite optimal pharmacological therapy, particularly in advanced emphysema, where hyperinflation and alveolar destruction impair lung function.5 Although LVRS is effective, its invasiveness limits widespread use.9 Bronchoscopic techniques (eg, valves, coils, and vapor ablation) offer less-invasive alternatives for emphysema, although their success depends on careful patient selection.6 The persistent lack of novel drug therapies has highlighted the need for interventional approaches.23 This study evaluated whether achieving accurate subsegmental dosing in BTVA correlates with improved clinical outcomes in severe emphysema, which may refine current treatment strategies for better therapeutic precision.
BTVA is a bronchoscopic lung volume reduction procedure that uses heated water vapor to induce lung lobe volume reduction through an inflammatory process, without the need for implants.24 In this study, BTVA treatment led to significant improvements in FEV1 and FVC, with a reduction in RV, as well as an improvement in patient symptoms, as indicated by the mMRC, CAT, and SGRQ scores. The STEP-UP study (treatment group n = 45, control group n = 24) reported between-group differences of +80.5 mL in FEV1 and −6.6 points in SGRQ at 3 months post-treatment.9 By comparison, our study observed within-group changes of +90 mL in FEV1 and −11.16 points in SGRQ at the same timepoint (n = 14). At 6 months post-treatment, the STEP-UP study reported an absolute difference in FEV1 of 130.8 mL between the treatment and control groups, whereas in this study, FEV1 increased by 130 mL (n = 8) from baseline. While differences in study design (controlled trial vs uncontrolled cohort) and sample size preclude direct comparison, the observed trends were directionally consistent with STEP-UP.
Although BTVA treatment has shown promising results, it still has the potential to improve treatment precision. The previous QCT software could only estimate treatment doses at the segment level, which posed challenges when the treatment had to be divided into subsegments. In such cases, the distribution of doses across subsegments is often estimated to be 1:1, 2:1, or 3:1, which could result in potential inaccuracies in dose allocation. In this study, BroncQCT, a new software capable of assessing emphysema severity at the subsegment level, was used to allow for more precise dose allocation. Based on this analysis, patients were classified into dose-matched and dose-unmatched groups. The results showed that the dose-matched group experienced greater changes in FEV1 1, 3, and 6 months post-treatment, with statistically significant differences between the two groups. Similar trends were observed in FVC, RV/TLC, CAT, and SGRQ scores. While baseline pulmonary function (FEV1, FVC, RV/TLC) and exercise capacity (6MWT) were comparable between groups, we acknowledge that differences in age and mMRC scores may introduce confounding bias. Our adjusted analyses demonstrated that only the 1-month CAT score difference reached nominal significance after controlling for these confounders (adjusted P = 0.04), whereas the unadjusted analysis showed borderline significance (P = 0.059) and other outcomes lost statistical significance entirely, a pattern potentially attributable to limited statistical power in this exploratory study. Furthermore, broader clinical adoption of BroncQCT-based dosing for BTVA faces standardization challenges, including the need for advanced bronchoscopy expertise to perform BTVA precisely and strict adherence to CT acquisition protocols for reliable subsegmental analysis.
The adverse events observed in our study (COPD exacerbation, pneumonia, increased dyspnea, and hemoptysis) are consistent with previous reports,9,16,24–26 although we observed no pneumothorax cases.9,16 Notably, one case of non-cardiac chest pain resolved within 5 days, a finding that appears to have been previously unreported in research, and we hypothesize that it may be related to a localized inflammatory response.24 Two late deaths occurred (4 and 11 months post-procedure), beyond the typical 2–4 week period for BTVA-related localized inflammatory responses.24 COPD carries a high mortality risk, with 3-year mortality rates of 23.8% and 36.9% for the former GOLD groups B and D, respectively.27 Notably, patients with FEV1 <30% predicted, lower DLCO, emphysema phenotype, or comorbidities (cardiovascular disease and diabetes) had significantly higher mortality.28–30 Both deceased patients in our study exhibited baseline FEV1 <35%, DLCO <40%, and high-risk comorbidities (atherosclerosis/pulmonary hypertension; diabetes/hypertension), which is consistent with this profile. Both deaths occurred beyond the peri-procedural period and involved preexisting comorbidities. However, formal attribution requires cautious interpretation in the absence of standardized adjudication. Standardized safety adjudication will be implemented in the subsequent RCT (NCT06152107) to definitively address causality.
This study had several limitations inherent to its retrospective design and small sample size. First, high loss-to-follow-up rates beyond 3 months (attributable to disease severity, logistical challenges with long-distance travel, and the retrospective design without mandated close follow-up), a recognized challenge in real-world non-malignant chronic disease studies, may affect durability assessments and late phase adverse event capture (although early phase events were systematically recorded, the retrospective nature implies potential underreporting of late phase events). Second, our primary analysis treated all segmental BTVA as matched (due to the absence of quantitative dose-matching criteria), though sensitivity analyses supported outcome robustness. Third, while an association was observed between assignment to the dose-matched group and efficacy outcomes, the limited sample size and baseline imbalances in age and mMRC scores (despite comparable pulmonary function) may introduce confounding. These gaps motivate our ongoing multicenter RCT (NCT06152107), which will rigorously assess these findings using standardized protocols, broader demographics, and enhanced longitudinal monitoring.
Conclusion
In this retrospective analysis, subsegment-level dose-matched BTVA was associated with greater FEV1 changes versus unmatched treatments, particularly at 1 month (+110 mL [n = 14] vs 0 mL [n = 5], P = 0.044), 3 months (+150 mL [n = 9] vs +10 mL [n = 5], P = 0.012), and 6 months (+150 mL [n = 5] vs +60 mL [n = 3], P = 0.036). Limitations include small sample sizes, incomplete follow-up, and baseline imbalances. These findings require confirmation in our ongoing prospective trial (NCT06152107), which will assess predefined FEV1 endpoints at 6 months with standardized safety monitoring. Subsegment-level software-guided dose planning appears feasible and may aid BTVA standardization efforts.
Abbreviations
COPD, chronic obstructive pulmonary disease; LVRS, lung volume reduction surgery; BLVR, bronchoscopic lung volume reduction; BTVA, bronchoscopic thermal vapor ablation; EBV, endobronchial valves; LVRC, lung volume reduction coils; GOLD, Global Initiative for Chronic Obstructive Lung Disease; FEV1, forced expiratory volume in 1 second; SGRQ-C, St. George’s Respiratory Questionnaire for COPD Patients; CV, collateral ventilation; CT, computed tomography; QCT, quantitative CT; FVC, forced vital capacity; RV, residual volume; TLC, total lung capacity; 6MWT, 6-minute walking test; CAT, COPD Assessment Test; mMRC, modified Medical Research Council; HRCT, High-Resolution CT; LAA-950, Low Attenuation Area at −950 HU; SD, standard deviation; IQR, interquartile range.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author Jiayuan Sun upon reasonable request.
Ethics Approval
This retrospective study was approved by the Ethics Committee of Shanghai Chest Hospital (Ethics Approval No. IS25023) and was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Consent to Participate
Given the retrospective design of the study, the requirement for informed consent was waived by the Ethics Committee of Shanghai Chest Hospital.
Acknowledgments
This study was technically supported by the Broncus®. We would like to thank Riqing Chen and Mingwei Cui from Broncus® for their technical support with quantitative CT. Their contributions are invaluable for the completion of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Shanghai Hospital Development Center Foundation (SHDC12025115), Science and Technology Commission of Shanghai Municipality (23440790102).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Adeloye D, Song P, Zhu Y, Campbell H, Sheikh A, Rudan I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–16. doi:10.1016/s2213-2600(21)00511-7
2. Jarhyan P, Hutchinson A, Khaw D, Prabhakaran D, Mohan S. Prevalence of chronic obstructive pulmonary disease and chronic bronchitis in eight countries: a systematic review and meta-analysis. Bull World Health Organ. 2022;100(3):216–230. doi:10.2471/blt.21.286870
3. Litmanovich D, Boiselle PM, Bankier AA. CT of pulmonary emphysema--current status, challenges, and future directions. Eur Radiol. 2009;19(3):537–551. doi:10.1007/s00330-008-1186-4
4. Duffy SP, Criner GJ. Chronic obstructive pulmonary disease: evaluation and management. Med Clin North Am. 2019;103(3):453–461. doi:10.1016/j.mcna.2018.12.005
5. Bulsei J, Leroy S, Perotin JM, et al. Cost-effectiveness of lung volume reduction coil treatment in patients with severe emphysema: results from the 2-year follow-up crossover REVOLENS study (REVOLENS-2 study). Respir Res. 2018;19(1):84. doi:10.1186/s12931-018-0796-x
6. Yang H, Chen S, Sun J, Herth FJF. Interventional pulmonology for chronic inflammatory airway diseases. Chin Med J Pulm Crit Care Med. 2024;2(3):171–181. doi:10.1016/j.pccm.2024.08.001
7. Buttery SC, Banya W, Bilancia R, et al. Lung volume reduction surgery versus endobronchial valves: a randomised controlled trial. Eur Respir J. 2023;61(4):2202063. doi:10.1183/13993003.02063-2022
8. Criner GJ, Cordova F, Sternberg AL, Martinez FJ. The national emphysema treatment trial (NETT) Part II: lessons learned about lung volume reduction surgery. Am J Respir Crit Care Med. 2011;184(8):881–893. doi:10.1164/rccm.201103-0455CI
9. Herth FJ, Valipour A, Shah PL, et al. Segmental volume reduction using thermal vapour ablation in patients with severe emphysema: 6-month results of the multicentre, parallel-group, open-label, randomised controlled STEP-UP trial. Lancet Respir Med. 2016;4(3):185–193. doi:10.1016/s2213-2600(16)00045-x
10. Strange C, Herth FJ, Kovitz KL, et al. Design of the endobronchial valve for emphysema palliation trial (VENT): a non-surgical method of lung volume reduction. BMC Pulm Med. 2007;7:10. doi:10.1186/1471-2466-7-10
11. Sciurba FC, Ernst A, Herth FJ, et al. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med. 2010;363(13):1233–1244. doi:10.1056/NEJMoa0900928
12. Slebos DJ, Ten Hacken NH, Hetzel M, Herth FJF, Shah PL. Endobronchial coils for endoscopic lung volume reduction: best practice recommendations from an expert panel. Respiration. 2018;96(1):1–11. doi:10.1159/000490193
13. Shah PL, Zoumot Z, Singh S, et al. Endobronchial coils for the treatment of severe emphysema with hyperinflation (RESET): a randomised controlled trial. Lancet Respir Med. 2013;1(3):233–240. doi:10.1016/s2213-2600(13)70047-x
14. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2025 report). Available from: https://goldcopd.org/2025-gold-report/.
15. Gompelmann D, Shah PL, Valipour A, Herth FJF. Bronchoscopic thermal vapor ablation: best practice recommendations from an expert panel on endoscopic lung volume reduction. Respiration. 2018;95(6):392–400. doi:10.1159/000489815
16. Gompelmann D, Eberhardt R, Schuhmann M, et al. Lung volume reduction with vapor ablation in the presence of incomplete fissures: 12-month results from the STEP-UP randomized controlled study. Respiration. 2016;92(6):397–403. doi:10.1159/000452424
17. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117. doi:10.1164/ajrccm.166.1.at1102
18. Chronic Obstructive Pulmonary Disease Group of Chinese Thoracic Society, & Chronic Obstructive Pulmonary Disease Committee of Chinese Association of Chest Physician. Guidelines for the diagnosis and management of chronic obstructive pulmonary disease (revised version 2021). Chinese Journal of Tuberculosis and Respiratory Diseases. 2021;44(3):170–205. doi:10.3760/cma.j.cn112147-20210109-00031
19. Department of Health and Human Services NIoH, National Cancer Institute. Common terminology criteria for adverse events (CTCAE) version 5. Available from: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_5.0.
20. Donohue JF. Minimal clinically important differences in COPD lung function. Copd. 2005;2(1):111–124. doi:10.1081/copd-200053377
21. Welling JB, Hartman JE, Ten Hacken NH, Klooster K, Slebos DJ. The minimal important difference for the St George’s respiratory questionnaire in patients with severe COPD. Eur Respir J. 2015;46(6):1598–1604. doi:10.1183/13993003.00535-2015
22. Yang H, Chen S, Ye L, Herth FJ, Sun J. Study protocol for a multicentre, randomised controlled trial in China to evaluate the efficacy and safety of precise subsegmental bronchoscopic thermal vapour ablation treatment in severe emphysema. BMJ open. 2025;15(10):e099367. doi:10.1136/bmjopen-2025-099367
23. Stolz D, Mkorombindo T, Schumann DM, et al. Towards the elimination of chronic obstructive pulmonary disease: a lancet commission. Lancet. 2022;400(10356):921–972. doi:10.1016/s0140-6736(22)01273-9
24. Gompelmann D, Eberhardt R, Herth FJ. Technology update: bronchoscopic thermal vapor ablation for managing severe emphysema. Med Devices. 2014;7:335–341. doi:10.2147/mder.S49369
25. Snell GI, Hopkins P, Westall G, Holsworth L, Carle A, Williams TJ. A feasibility and safety study of bronchoscopic thermal vapor ablation: a novel emphysema therapy. Ann Thorac Surg. 2009;88(6):1993–1998. doi:10.1016/j.athoracsur.2009.06.038
26. Snell G, Herth FJ, Hopkins P, et al. Bronchoscopic thermal vapour ablation therapy in the management of heterogeneous emphysema. Eur Respir J. 2012;39(6):1326–1333. doi:10.1183/09031936.00092411
27. Gedebjerg A, Szépligeti SK, Wackerhausen LH, et al. Prediction of mortality in patients with chronic obstructive pulmonary disease with the new global initiative for chronic obstructive lung disease 2017 classification: a cohort study. Lancet Respir Med. 2018;6(3):204–212. doi:10.1016/s2213-2600(18)30002-x
28. Whittaker H, Rothnie KJ, Quint JK. Cause-specific mortality in COPD subpopulations: a cohort study of 339 647 people in England. Thorax. 2024;79(3):202–208. doi:10.1136/thorax-2022-219320
29. Papaioannou AI, Hillas G, Loukides S, Vassilakopoulos T. Mortality prevention as the centre of COPD management. ER J Open Research. 2024;10(3):00850–2023. doi:10.1183/23120541.00850-2023
30. Alupo P, Wosu AC, Mahofa A, et al. Incidence and predictors of COPD mortality in Uganda: a 2-year prospective cohort study. PLoS One. 2021;16(2):e0246850. doi:10.1371/journal.pone.0246850
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Improvement of Progressive Vanishing Lung Syndrome in COPD: A 7-Year Radiological Evolution Case Report and Literature Review
Zhong X, Liu Q, Huang J, Liao H, Huang X
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:566280
Published Date: 14 January 2026