Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Association Between Subclinical Albuminuria and Early Arterial Stiffness in Chinese Adults with Type 2 Diabetes
Authors Xuan Y ![]() , Zhu F, Tang D, Wang X, Wang S, Shen Y, Lu L
, Zhu F, Tang D, Wang X, Wang S, Shen Y, Lu L
Received 22 October 2025
Accepted for publication 14 January 2026
Published 5 February 2026 Volume 2026:19 575958
DOI https://doi.org/10.2147/DMSO.S575958
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Yan Xuan, Fanfan Zhu, Dou Tang, Xun Wang, Sujie Wang, Ying Shen, Leiqun Lu
Department of Endocrinology, Shanghai Ruijin Hospital, Luwan Branch, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China
Correspondence: Ying Shen, Email [email protected] Leiqun Lu, Email [email protected]
Background: While elevated microalbuminuria is closely associated with arterial stiffness, the relationship between high-normal albuminuria and arterial stiffness remains unclear among Chinese adults with type 2 diabetes.
Objective: This study aimed to investigate the association between subclinical albuminuria and early arterial stiffness in a cohort of Chinese adults with T2DM, focusing on sex-specific differences and threshold effects.
Methods: In this cross-sectional study, 1119 Chinese adults with type 2 diabetes and without overt kidney or cardiovascular disease were enrolled. Arterial stiffness was assessed by brachial-ankle pulse wave velocity (baPWV). Participants were stratified by tertiles of the logarithmically transformed urinary albumin-to-creatinine ratio (lg-UACR). We employed correlation analysis to examine continuous relationships and multivariable logistic regression to assess the odds of high baPWV across lg-UACR tertiles. Sex-stratified and restricted cubic spline analyses were conducted to explore effect modification and nonlinearity.
Results: Higher lg-UACR tertiles demonstrated a dose-dependent association with arterial stiffness risk in the overall cohort. Sex-stratified analysis revealed this association was statistically significant only in women. Among postmenopausal women, a threshold effect was observed at lg-UACR =1.1 (UACR =12.6 mg/g), beyond which the significant correlation between microalbuminuria and arterial stiffness was attenuated.
Conclusion: Elevated UACR in normal range is associated with arterial stiffness risk in Chinese women with type 2 diabetes, but not in men. Among postmenopausal women, this link is significant only below a lg-UACR threshold of 1.1 and is abolished at or above this level. This critical threshold effect, modulated by menopause, suggests sex-specific UACR criteria for vascular risk assessment.
Keywords: urinary albumin-creatinine ratio, brachial-ankle pulse wave velocity, arterial stiffness, type 2 diabetes
Introduction
High-normal albuminuria (urinary albumin-to-creatinine ratio, UACR), ranging from 6.36 mg/g to 30 mg/g, recognized as a subclinical manifestation of vascular dysfunction, is associated with an increased risk of cardiovascular events even among individuals without overt kidney disease.1,2 In this study, we focused on high-normal albuminuria, defined as UACR levels above the median of a normal population but below the microalbuminuria threshold (30 mg/g). It aligns with clinical concepts for identifying elevated risk within the normoalbuminuric range and ensures comparability with prior key studies.3,4 Accordingly, we set the UACR range at 6–30 mg/g. Our operational definition (UACR 6–30 mg/g) was based on: (1) consistency with prior literature; (2) alignment with the upper UACR tertile in our cohort; and (3) inclusion of values where cardiovascular risk begins to increase. While microalbuminuria (UACR 30–300 mg/g) is a well-established indicator of endothelial damage, particularly in high-risk populations,5,6 accumulating evidence suggests that albuminuria levels below this conventional diagnostic threshold may also signify early vascular injury.2,5 This aligns with the Steno hypothesis, which proposes a mechanistic link between albuminuria and systemic endothelial dysfunction.7
Arterial stiffness, a key driver of cardiovascular events, is commonly assessed by carotid-femoral pulse wave velocity (cfPWV) or brachial-ankle pulse wave velocity (baPWV).3,4,8,9 Although cfPWV is the gold standard for measuring aortic elasticity, its technical complexity limits widespread clinical application.9 In contrast, baPWV provides a noninvasive and practical alternative validated in Asian populations,3,4 including Chinese cohorts where it correlates strongly with hypertension and diabetes.3,4 However, significant inconsistencies persist across studies examining the association between albuminuria (UACR) and arterial stiffness quantified by baPWV, particularly regarding population characteristics and age effects. For example, Schutte et al reported a UACR-arterial stiffness association in African males but not Caucasians.10 In China, research on diabetic populations yields conflicting results. Huang et al identified a strong association between high-normal albuminuria and arterial stiffness in young adults with diabetes,3 whereas Liu et al reported weaker associations in older cohorts using stricter UACR thresholds.4 Thus, the sex-specific association between high-normal albuminuria and arterial stiffness in Chinese T2DM, particularly across menopausal status, remains unresolved. The key reason for inconsistent findings across studies is likely methodological variation. This includes insufficient age grouping, which can hide effects specific to certain age ranges. Additionally, studies often mix different types of vascular measurements, comparing peripheral artery stiffness (like brachial-ankle PWV) with central aortic function. Finally, the definition of high-normal albuminuria varies significantly, with some studies including a broad UACR range (6–30 mg/g) and others focusing only on values near the microalbuminuria threshold (30 mg/g).3,4 Such methodological variations limit clinical generalizability, particularly in China, where hypertension11 and diabetes12 synergistically accelerate vascular aging.
To resolve these methodological inconsistencies, we conducted a Shanghai type 2 diabetes cohort study examining the association between high-normal albuminuria, defined as a UACR of 6–30 mg/g, and arterial stiffness quantified by baPWV in Chinese adults with type 2 diabetes. Key methodological improvements addressing prior heterogeneity include comprehensive inclusion across the age spectrum, implementation of standardized baPWV measurement protocols, and the application of uniform UACR thresholds. Our objective is to generate population-specific evidence for optimizing early cardiovascular risk stratification in this high-burden population.
Materials and Methods
Study Population
This prospective cohort enrolled adult patients with type 2 diabetes mellitus (T2DM) at the Metabolic Management Center (MMC), Shanghai Ruijin Hospital Luwan Branch, between March 2020 and December 2024. The MMC constitutes a nationwide initiative establishing standardized platforms for metabolic disease management. All centers adhere to identical facility designs, database structures, operational protocols, and daily workflows, facilitating uniform diagnosis, treatment, and longitudinal follow-up. Patients benefit from integrated care encompassing registration, diagnostic testing, clinical evaluation, medication dispensing, and health education within a single visit. The MMC project methodology has been previously detailed in publication.13 The exclusion criteria were applied in the following order: 1) diagnosis of other diabetes types (including type 1 diabetes mellitus, gestational diabetes, and other specific types, n=34); 2) participants lacking essential data (blood/urine samples (n=30) or baPWV values (n=44)); 3) estimated glomerular filtration rate (eGFR) <60 mL/min/1.73m2 (n=112); 4) urinary albumin-to-creatinine ratio (UACR) ≥30 mg/g (n=51); and 5) a documented history of cardiovascular disease (CVD) or stroke (n=93). Finally, 1119 participants were included in the final analysis (Figure 1).
 |
Figure 1 The flowchart of this study. |
Clinical, Anthropometric and Laboratory Measurements
Research personnel, uniformly trained in standardized protocols, conducted structured face-to-face interviews using a predefined questionnaire. This instrument assessed sociodemographic characteristics, individual and family medical histories, and lifestyle factors. Menopausal status was categorized according to World Health Organization (WHO) criteria: women reporting ≥12 consecutive months of amenorrhea unrelated to other pathological or physiological causes were classified as postmenopausal. Premenopausal status was assigned to women with regular menstrual cycles and no clinical indications of approaching menopause. Body mass index (BMI) was computed as weight in kilograms divided by height in meters squared (kg/m2). Following the criteria established by the Cooperative Meta-Analysis Group of the Working Group on Obesity in China, participants with BMI < 25 kg/m2 were classified as normal weight, while those with BMI ≥ 25 kg/m2 were categorized as overweight/obese.14 Blood pressure measurements adhered to standardized protocols. Following a seated rest period of ≥5 minutes, triplicate readings were acquired at 5-minute intervals using an oscillometric device (Omron HEM-7200; validated by the ESH). The final blood pressure value was calculated as the meaning of the last two measurements. Urinary albumin-to-creatinine ratio (UACR) underwent logarithmic transformation for analysis (denoted as logarithmically transformed urinary albumin-to-creatinine ratio, lg-UACR). Smoking status was defined as self-reported consumption of ≥100 lifetime cigarettes combined with active tobacco use within the 30 days preceding enrollment.15 Educational attainment was categorized into two groups based on high school completion status. Physical activity levels, encompassing both occupational and leisure components, were evaluated against World Health Organization (WHO) guidelines. Participants were subsequently classified into those meeting the WHO-recommended threshold (≥150 minutes per week of moderate-to-vigorous activity across both domains) and those with inadequate activity levels.16 This study employed brachial-ankle pulse wave velocity (baPWV) as a comprehensive functional indicator for assessing arterial stiffness. Following a 15-minute rest period, the examiner assessed brachial-ankle pulse wave velocity (baPWV, cm/s) using an OMRON BP-203RPE III atherosclerosis detection system (China). This apparatus simultaneously captured pulse wave forms from the brachial and anterior tibial arteries on both sides. The principle relies on calculating baPWV from the transmission time and path length between these sites. The highest value obtained from the bilateral readings was designated as the result. A baPWV value ≥1400 cm/s defined high baPWV.17
Fasting (≥8h) venous samples were processed under strict protocols: refrigerated at 4°C immediately post-collection, centrifuged ≤120 min later, and stored at −80°C as aliquots. HbA1c quantification used NGSP-certified HPLC (MQ-2000PT, MEDCONN). Lipid profiles (TG [AUZ5612 kit; sensitivity 0.01 mmol/L, CV<7%], TC, HDL-C, LDL-C), fasting glucose, and renal markers were assayed on an AU680 platform (Beckman Coulter). First-void urine determined ACR. eGFR was calculated via CKD-EPI China (2014). All procedures complied with ISO 15189, including daily calibration and 5% random duplicates (intra-assay CV<8%).18
Definition of Variables
Hypertension was defined according to the 2023 ACC/AHA guidelines as systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, or self-reported antihypertensive medication usage within the preceding two weeks.19 Chronic kidney disease (CKD) was defined by an estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2 and a urinary albumin-to-creatinine ratio (UACR) ≥ 30 mg/g.20 The composite cardiovascular disease (CVD) outcome encompassed documented diagnoses of coronary heart disease (CHD), stroke, or peripheral arterial disease (PAD). These outcomes were ascertained from prior study records.21,22 Hyperlipidemia was defined by elevated plasma levels of total cholesterol (≥5.17 mmol/L), LDL cholesterol (≥3.36 mmol/L), or triglycerides (≥2.26 mmol/L).23
Statistical Analysis
Statistical analyses were conducted using IBM SPSS Statistics (v.25; IBM Corp., Armonk, NY). Continuous variables are reported as mean ± standard deviation (SD), non-normally distributed data as median (interquartile range [IQR]), and categorical variables as frequencies (%). Statistical significance was defined as two-tailed P < 0.05. Spearman correlation was used to assess association between baPWV and metabolism indexes. Because raw UACR data often exhibits a skewed distribution, applying a base-10 logarithmic transformation (logarithmic transformation-urine albumin-to-creatinine Ratio, lg-UACR) enables the data to more closely approximate a normal distribution, thereby enhancing the accuracy and validity of statistical analyses. Logistic regression was used to assess the association between lg-UACR, categorized into tertiles based on its distribution in the cohort and high baPWV. Model 1 was adjusted for age, sex, BMI, smoker. Model 2 was adjusted for Model 1 plus LDL, HbA1c, eGFR, systolic blood pressure, heart rate, antidiabetic agents (including sodium-glucose cotransporter-2 inhibitors, SGLT-2i), hypertension, antihypertensive drugs and education status. In addition, stratified analyses by sex, BMI, HbA1c, diabetes duration, smoke, presence of hypertension were performed. The restricted cubic spline (RCS) analysis was applied to explore potential nonlinear correlations between the lg-UACR and high baPWV. Partial correlation analyses relationship between lg-UACR and baPWV after adjusting for age, body mass index, heart rate, systolic blood pressure, LDL-C, fasting blood glucose, eGFR. A receiver operating characteristic (ROC) curve analysis was used to evaluate the predictive value of lg-UACR for high baPWV, with performance quantified by the area under the curve (AUC).
Results
Baseline Clinical Characteristics
Baseline characteristics stratified by lg-UACR tertiles are presented in Table 1 (the lowest tertile T1: 0.09–0.83; middle tertile T2: 0.83–1.10; the highest tertile T3: 1.10–1.48). The mean age of the participants was 58.69 ± 11.15 years, and 670 (59.9%) were male. No significant trends were observed across the groups in terms of age or sex distribution. Participants in T3 demonstrated significantly higher HbA1c (T3 vs T1: 7.11±1.83% vs 7.04±2.63%), and baPWV (1688(1485,1948) vs 1547(1357,1755) cm/s; P < 0.001) compared with T1. The current smoking prevalence was also significantly higher in T3 (P =0.011).
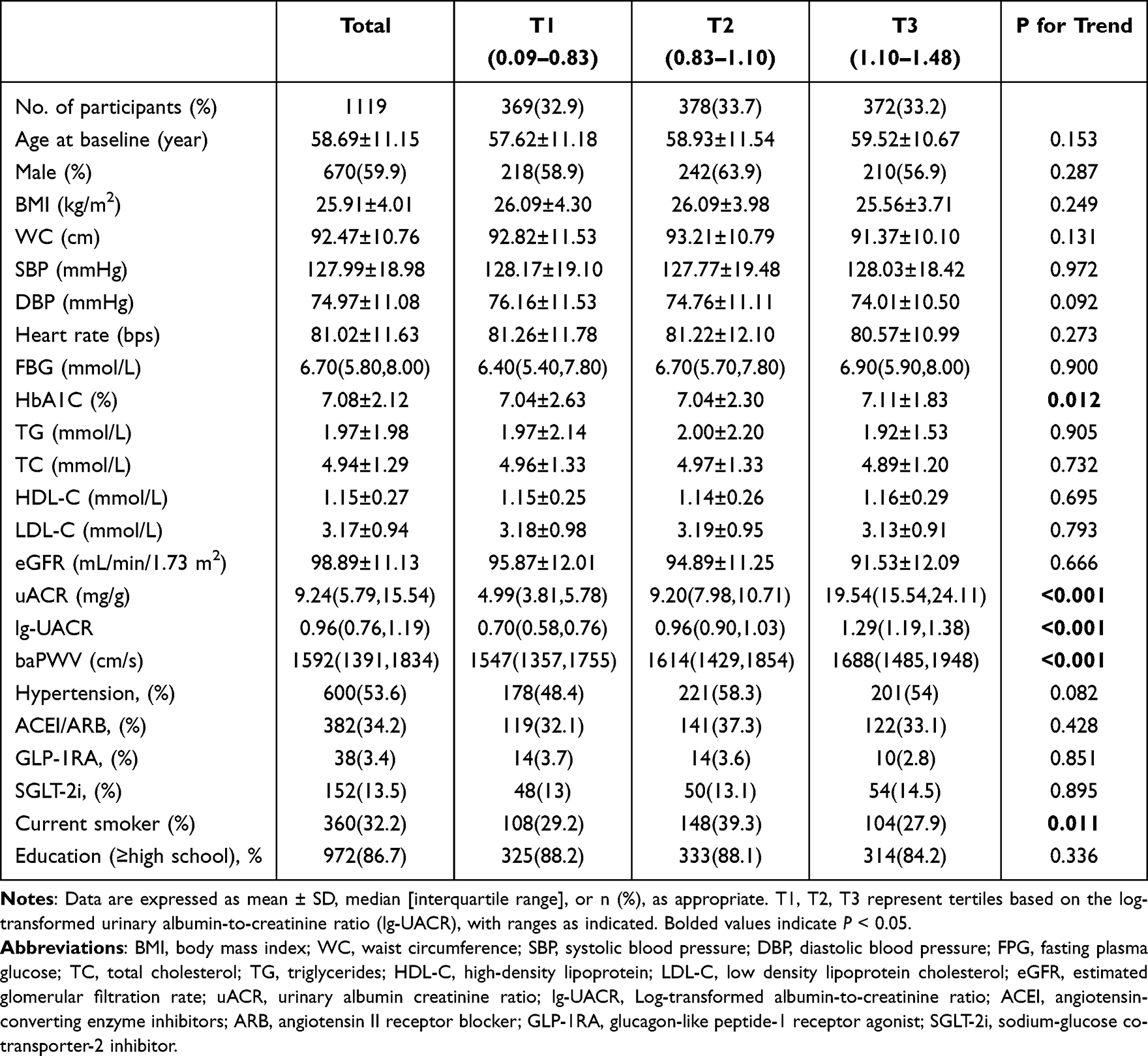 |
Table 1 Characteristics of the Participants in Lg-UACR Tertiles Groups (n = 1119) |
Correlation of Lg-UACR Levels with baPWV
Spearman correlation analysis revealed a significant positive association between baPWV and lg-UACR (r = 0.181, P < 0.001; Figure 2). After adjustment for covariates including age, body mass index, heart rate, systolic blood pressure, LDL-C, fasting plasma glucose and eGFR, the partial correlation analyses demonstrated persistent positive correlations in all participants (r = 0.203, P < 0.001). This association remained significant in sex-stratified analyses (males: r = 0.285, P < 0.001; females: r = 0.112, P = 0.013; in Supplementary Figure 1 A–C) after adjusting for age, body mass index, heart rate, systolic blood pressure, LDL-C, fasting blood glucose, eGFR.
 |
Figure 2 Correlation of lg-UACR levels with baPWV. |
Associations of Lg-UACR with High baPWV
Building upon these correlations, we further examined the relationship between lg-UACR tertiles and elevated baPWV risk to assess clinical relevance. Multivariable-adjusted logistic regression analyses demonstrated progressively higher odds of high baPWV with increasing lg-UACR levels in the overall cohort. Compared to the reference tertile (T1), both T2 and T3 showed statistically significant associations after sequential adjustment in Model 1 and Model 2, with T3 exhibiting an adjusted OR of 2.23 (95% CI 1.41–3.52) in the fully adjusted model (Figure 3).
 |
Figure 3 Odds ratios for High baPWV at Tertiles of lg-UACR (lg-UACR: the base-10 logarithmically transformed urinary albumin-to-creatinine ratio). Model 1was adjusted for age, sex, BMI, smoker. Model 2 was adjusted for model 1 plus LDL, eGFR, education status, systolic blood pressure, heart rate, hypertension, anti-diabetes agents, anti-hypertension drug. |
Prespecified subgroup analyses stratified by key clinical variables including age, sex, BMI, diabetes duration, education, smoking status, hypertension status, although some subgroups had confidence intervals crossing the null value (Figure 4). Notably, sex-specific analyses demonstrated differential risk patterns: whereas males exhibited attenuated associations after multivariable adjustment (T2-T3 vs T1: OR 1.58, 95% CI 0.87–2.84), females maintained significantly elevated risk (T2-T3 vs T1: OR 4.22, 95% CI 1.94–9.16).
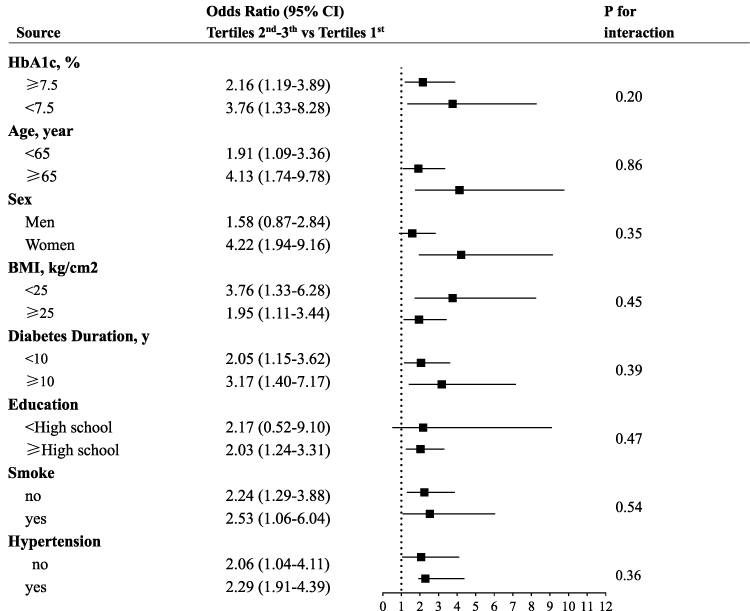 |
Figure 4 Stratified analyses odds ratios for High baPWV at Tertiles of lg-UACR was adjusted for LDL, eGFR, education status, systolic blood pressure, heart rate, hypertension, anti-diabetes agents, anti-hypertension drug. |
Receiver operating characteristic (ROC) analysis evaluated the discriminative capacity of lg-UACR for elevated baPWV (Supplementary Figure 2). The area under the curve (AUC) was 0.583 (95% CI 0.502–0.679) in the overall cohort. Sex-stratified analyses yielded AUCs of 0.564 (95% CI 0.502–0.639) in males and 0.626 (95% CI 0.583–0.688) in females.
Nonlinear Relationship Between Lg-UACR with High baPWV
RCS analysis demonstrated a nonlinear association between lg-UACR and high baPWV (Figure 5). After adjusting for age, sex, BMI, and other covariates, the risk of high baPWV increased significantly with higher lg-UACR levels in all participants and in women. However, sex-stratified analysis revealed no significant association in men. Given that menopausal status is a significant determinant of cardiovascular pathology, we stratified female participants by menopausal status and found no significant association in premenopausal women. Furthermore, the risk increased progressively until lg-UACR > 1.1 (UACR ≥ 12.6 mg/g) in postmenopausal women. To further investigate this threshold effect in the vulnerable group, we specifically evaluated the association between lg-UACR (<1.1 vs ≥1.1) and high baPWV in postmenopausal women (Table 2). Using participants with lg-UACR ≥1.1 as the reference, logistic regression analyses consistently showed a significantly higher risk of high baPWV for those with lg-UACR <1.1 (Crude: OR = 2.43, 95% CI 1.25–4.23; Model 1: OR = 2.46, 95% CI 1.27–4.80; Model 2: OR = 2.36, 95% CI 1.19–4.68). This finding robustly supports the RCS-derived observation of an increased arterial stiffness risk below the lg-UACR threshold of 1.1 in postmenopausal women.
 |
Table 2 Odds Ratios for High baPWV at Lg-UACR of Cut-off 1.1 in Postmenopausal Women |
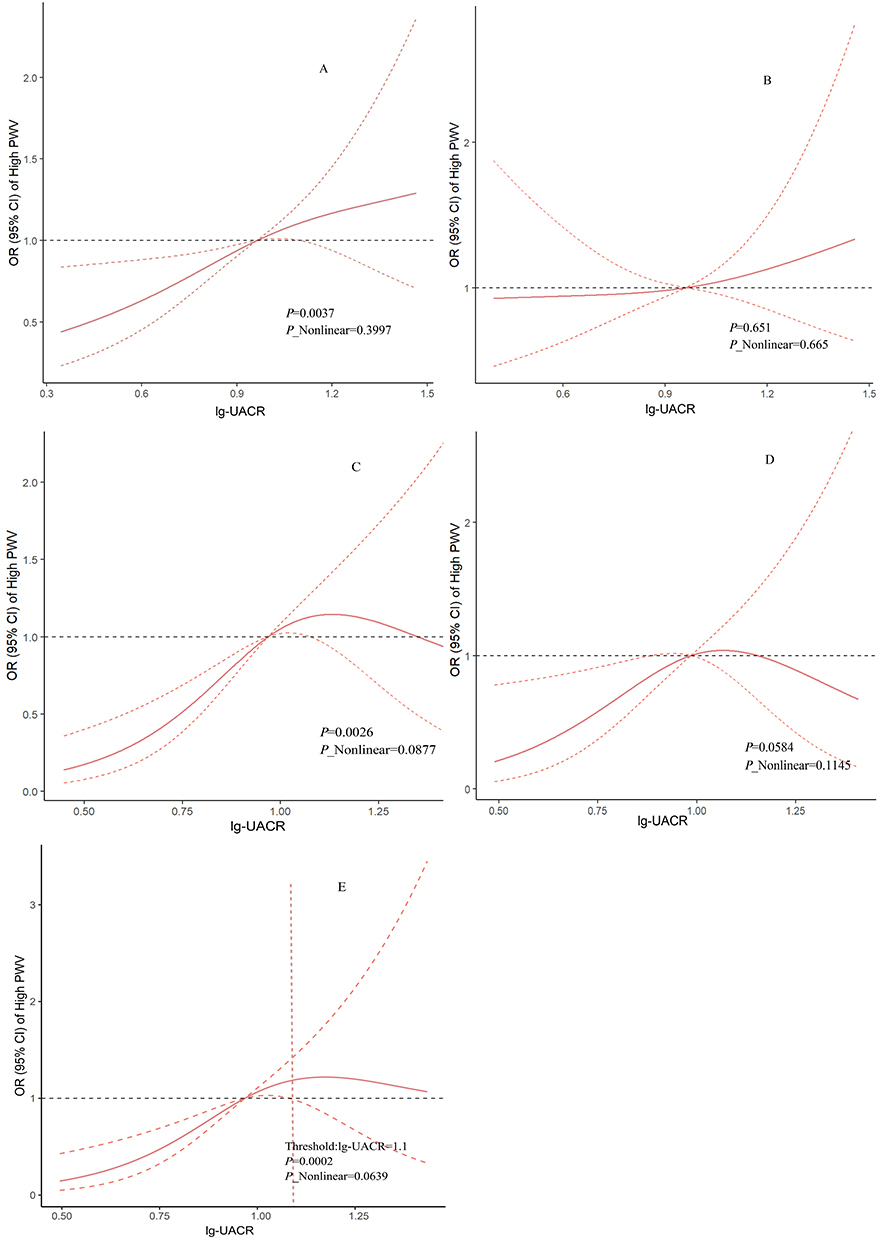 |
Figure 5 The relationship between lg-UACR and the risk of high baPWV using restricted cubic spline (RCS). The odds ratios for baPWV (solid line) and 95% confidence intervals are presented. Adjusts for age, sex, BMI, current smoker, LDL, HbA1c, eGFR, education status, systolic blood pressure, heart rate, hypertension, anti-diabetes agents and anti-hypertension drug. (A) The nonlinear relationship between the lg-UACR and risk of high baPWV in all participants. (B)The nonlinear relationship between the lg-UACR and risk of high baPWV in men. (C)The nonlinear relationship between the lg-UACR and risk of high baPWV in women. (D)The nonlinear relationship between the lg-UACR and risk of high baPWV in premenopausal women. (E) The nonlinear relationship between the lg-UACR and risk of high baPWV in postmenopausal women. |
Discussion
In this cohort study of Chinese individuals with diabetes, we established several pivotal findings. Firstly, a dose-dependent association was observed between higher lg-UACR tertiles and arterial stiffness risk across the entire cohort, with individuals in the highest tertile exhibiting a 2.23-fold increased risk compared to the lowest tertile in the fully adjusted model (Model 2). Secondly, sex-stratified analyses demonstrated this association remained statistically significant exclusively in women. This suggests potential sex-based pathophysiological divergence. Despite non-significant interaction testing, sex-stratified analyses were retained due to established biological plausibility of sexual dimorphism in disease mechanisms and clinical guidelines mandating sex-specific risk assessment. Finally, and most notably, postmenopausal women displayed a threshold effect at lg-UACR =1.1, the high-normal albuminuria-arterial stiffness correlation disappeared when lg-UACR reached ≥1.1, suggesting menopausal transition may critically modulate vascular susceptibility to albuminuria. Although the standalone discriminative capacity of lg-UACR was modest (AUC 0.626 in females), its significant subclinical associations challenge current diagnostic paradigms that disregard normal-range albuminuria.
Urinary albumin-to-creatinine ratio is a validated biomarker for albuminuria and renal impairment, with established associations to cardiovascular and all-cause mortality. Although 30 mg/g remains the conventional upper normal limit, contemporary studies report substantially lower population mean values. Importantly, cardiovascular risk increases continuously across UACR levels, including values below 30 mg/g, demonstrating a biological risk continuum that supports threshold redefinition.24
These findings consolidate prior evidence linking high-normal albuminuria to vascular damage in metabolic disorders. Specifically, our observation of a dose-dependent UACR-arterial stiffness relationship extends similar patterns reported in young diabetic adults3 and broader cohorts,4 reinforcing albuminuria’s role as a continuum biomarker of vascular risk. This vascular continuum extends beyond arterial stiffness phenotypes. Population-based evidence from independent cohorts indicates that the higher UACR within the normal range was independently associated with carotid atherosclerotic lesions accessed by carotid intima-media thickness (cIMT) in community-based patients with type 2 diabetes.25 In this cohort of individuals with diabetes, high-normal albuminuria independently associated with elevated arterial stiffness, as quantified by brachial-ankle pulse wave velocity. Participants exhibiting high-normal albuminuria demonstrated adverse metabolic profiles, including significantly higher fasting blood glucose, HbA1c, and smoking prevalence. These concomitant cardiovascular risk factors may partially mediate the observed association, yet high-normal albuminuria retained robust independence as a biomarker of arterial stiffness after multivariable adjustment for conventional risk factors. Importantly, this independence manifests clinically as divergent sex-specific risk profiles: our findings corroborate established female-predominant associations between albuminuria and carotid atherosclerosis, with amplified arterial vulnerability in women in this study.26 The absence of association in males aligns with ethnic heterogeneity reported by Schutte et al,10 potentially reflecting earlier vascular pathology in men.
Critically, the risk threshold we identified (lg-UACR = 1.1, corresponding to a UACR of 12.6 mg/g) lies well below the conventional microalbuminuria cutoff of 30 mg/g. This UACR level of 12.6 mg/g is substantially lower than the near-microalbuminuria range (UACR 25–30 mg/g) often linked to vascular risk in older diabetic cohorts.9 These findings highlight that clinically significant vascular susceptibility, particularly in women with T2DM, manifests at albuminuria levels (UACR <30 mg/g) far lower than traditionally recognized. This sex-specific vulnerability profile underscores the potential of UACR = 12.6 mg/g as an early warning signal for arterial stiffening risk in this high-risk group. The sex-specific vulnerability profile suggests clinically meaningful vascular susceptibility in women at subthreshold albuminuria levels (UACR <30 mg/g), conceptually extending Huang et al’s population-level observations toward personalized risk stratification.8 Critically, in postmenopausal women, we identified a distinct nonlinear, threshold-dependent relationship between lg-UACR and arterial stiffness (Figure 5A–E, Table 2). The risk of high baPWV increased progressively with rising lg-UACR until reaching a critical point of approximately 1.1 (UACR ≈ 12.6 mg/g), beyond which the association plateaued (Figure 5E). This pattern suggests a biphasic pathological model. Within the high-normal range, albuminuria likely acts as a dynamic biomarker of ongoing endothelial dysfunction and potentially reversible vascular remodeling. However, once this lg-UACR threshold of 1.1 is surpassed, the disease process may transition into a phase dominated by irreversible structural alterations (eg, medial calcification, collagen deposition). In this advanced phase, functional biomarkers like UACR lose incremental predictive sensitivity for arterial stiffness progression, which may explain the observed risk plateau. This threshold, potentially modulated by postmenopausal estrogen deficiency, may thus represent a pivotal transition from functional vascular disturbance to fixed arteriosclerotic pathology.
Estrogen deficiency drives this process through progressive elastin degradation27,28 and hemodynamic stress, creating a self-perpetuating vascular-renal cycle. Concurrently, chronic low-grade inflammation and endothelial hyperpermeability1 facilitate atherogenic lipoprotein retention and elastin degradation in the arterial external elastic lamina,4 culminating in irreversible structural remodeling. Sex hormones, particularly estrogen, exert significant effects on vascular integrity. In premenopausal women, estrogen confers potent vascular protection by enhancing nitric oxide (NO) bioavailability and suppressing angiotensin activity, thereby mitigating endothelial injury.29 Following menopause, however, the marked decline in estrogen eliminates this protective effect. Estrogen deficiency is associated with heightened oxidative stress and accumulation of advanced glycation end-products (AGEs),27 accelerating the transition from reversible endothelial dysfunction to irreversible arterial stiffening and structural remodeling.
An lg-UACR >1.1 marks an accelerated pathological shift, particularly in postmenopausal women.27 This threshold effect is critically driven by estrogen deficiency. Elevated UACR primarily reflects systemic endothelial dysfunction. Concurrently, increased arterial stiffness reduces aortic-peripheral pressure gradients, transmitting amplified pulsatile energy to the renal microvasculature and driving glomerular hyperfiltration – establishing a hemodynamically-mediated bidirectional vascular-renal vicious cycle27 Chronic low-grade inflammation and endothelial hyperpermeability further facilitate atherogenic lipoprotein retention and elastin degradation within the arterial external elastic lamina,4 culminating in irreversible structural changes. Therefore, lg-UACR >1.1 marks the exacerbation of vascular-renal dysfunction, driven by estrogen deficiency. Beyond this threshold, the plateau in baPWV risk may reflect completed structural remodeling where functional biomarkers like UACR lose sensitivity, necessitating imaging-based assessments. Consistent with the RCS-derived threshold, logistic regression confirmed no incremental arterial stiffness risk beyond lg-UACR >1.1 in postmenopausal women. This suggests that UACR loses discriminative power for vascular remodeling after surpassing this critical point, likely due to irreversible structural changes.
Additionally, the observed disparity in SGLT-2i usage (significantly lower in women: 10.5% vs 17.4% in men, p=0.002) represents a potential confounding factor. Given the established effects of SGLT-2i on reducing both albuminuria30 and arterial stiffness,31 this differential treatment exposure might have contributed to the attenuated association observed in males. However, this remains a hypothesis-generating observation based on cross-sectional data; future longitudinal studies specifically accounting for antidiabetic medication regimens, particularly SGLT-2i use, are warranted to clarify its role in sex-specific vascular risk associations.
These findings carry direct implications for clinical risk assessment in Chinese T2DM patients. Our results advocate for a sex-stratified approach: Specifically, in women with type 2 diabetes, particularly those who are postmenopausal, cardiovascular risk stratification should consider UACR levels well below the conventional microalbuminuria threshold. We propose that a UACR value of 12.6 mg/g (lg-UACR = 1.1) could serve as a critical indicator to trigger more intensive vascular evaluation, such as baPWV screening, even in the absence of overt albuminuria. Implementing such targeted screening based on this lower, sex-specific UACR threshold may facilitate earlier identification of arterial stiffening and allow for timely preventive interventions.
Beyond the primary findings, our results can be further contextualized within a growing conceptual framework that distinguishes different dimensions of arterial stiffness—namely, its positional, functional, and structural components. The baPWV employed in our study is best characterized as a composite, integrative functional biomarker, providing a clinically practical measure of overall arterial function. Consequently, the association we observed between elevated lg-UACR and increased baPWV primarily reflects a link between subclinical albuminuria and impaired integrated arterial function. Our study design, employing baPWV as a composite functional measure, does not permit delineation of whether this association is driven more by structural remodeling of large arteries, localized endothelial dysfunction in the microvasculature, or a combination thereof. To move beyond this integrative assessment and pinpoint the primary anatomical and functional loci of albuminuria-associated vascular injury, future studies that combine baPWV with modality-specific techniques will be essential.
There were still some limitations in this research. First, the single-center design and exclusive focus on Chinese adults with type 2 diabetes may limit the generalizability of findings to populations with distinct ethnic backgrounds or albuminuria etiologies. Second, the cross-sectional nature of the data precludes causal inferences; longitudinal studies are required to delineate temporal relationships between UACR and arterial stiffening. Third, unmeasured confounders—such as menopausal hormone therapy, inflammatory cytokines, and genetic polymorphisms—could partially explain the observed associations. Fourth, the modest predictive accuracy of lg-UACR (AUC: 0.583–0.626) underscores the need for composite models incorporating novel biomarkers to improve clinical utility. While the AUC in females (0.626) indicates modest predictive utility, its clinical applicability may be enhanced through integration with established cardiovascular risk biomarkers. Finally, while the identified threshold (lg-UACR >1.1) aligns with mechanistic studies of vascular remodeling, its universal applicability requires validation in multiethnic cohorts.
Conclusion
In conclusion, elevated lg-UACR within the high-normal range independently predicts arterial stiffness in Chinese adults with type 2 diabetes, with a critical sex-specific threshold in postmenopausal women. These findings advocate for sex-stratified vascular risk assessment below conventional albuminuria thresholds and support lg-UACR-guided baPWV screening in high-risk populations. As part of the Metabolic Management Cohort (MMC), a nationwide Chinese diabetes cohort study, we will further conduct longitudinal investigations within this population to validate these associations and explore their temporal dynamics. Future research should prioritize multiethnic validation of UACR cutoffs, mechanistic exploration of estrogen-albuminuria interactions, and development of integrated biomarker panels combining UACR with inflammatory or genetic markers to optimize cardiovascular risk prediction and guide targeted interventions.
Institutional Review Board Statement
The study protocol of the MMC project was approved by the Ethics Committee of the Shanghai Ruijin Hospital, Luwan branch, Shanghai Jiao Tong University School of Medicine (No. LWEC202024). These subjects provided written informed consent, and the study protocol was approved by the institute’s committee on human research.
This study was conducted in accordance with the Declaration of Helsinki.
Data Sharing Statement
The raw data supporting the conclusions of this manuscript will be made available by the authors, the corresponding author Leiqun Lu, without undue reservation, to any qualified researcher.
Acknowledgment
We express profound gratitude to the physicians within the Department of Endocrinology at both the Luwan Branch and the main campus of Ruijin Hospital, Shanghai Jiaotong University School of Medicine. Their essential contributions were indispensable to the completion of this research.
We express profound gratitude to all participants whose engagement made this research possible.
Author Contributions
Yan Xuan, Fanfan Zhu and Dou Tang share first authorship. Conceptualization was carried out by Yan Xuan and Ying Shen; methodology was designed by Dou Tang, Xun Wang, and Leiqun Lu; investigation (experimentation) was performed by Fanfan Zhu and Sujie Wang; formal analysis was conducted by Xun Wang and Dou Tang; resources were provided by Sujie Wang and Leiqun Lu; writing – original draft preparation was done by Yan Xuan; writing – review and editing involved all authors; visualization was created by Xun Wang; supervision was undertaken by Ying Shen and Leiqun Lu; project administration was managed by Ying Shen; funding acquisition was secured by Ying Shen and Leiqun Lu. All authors have given final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Shanghai Municipal Huangpu District Commission (HLQ202205) and Healthy Commission Research Project of Shanghai Huangpu District (HLM202206, HLM202401, HLM202506). The funder played no role in the design or conduct of the study, collection, management, analysis, or interpretation of data, or in the preparation, review, or approval of the article.
Disclosure
The authors declare no conflicts of interest.
References
1. Tanaka F, Komi R, Makita S, et al. Low-grade albuminuria and incidence of cardiovascular disease and all-cause mortality in nondiabetic and normotensive individuals. J Hypertens. 2016;34(3):506–512;discussion512. doi:10.1097/HJH.0000000000000809
2. Wang T, Zhong H, Lian G, et al. Low-grade albuminuria is associated with left ventricular hypertrophy and diastolic dysfunction in patients with hypertension. Kidney Blood Press Res. 2019;44(4):590–13. doi:10.1159/000500782
3. Huang L, Yang L, Zhang S, et al. Low-grade albuminuria associated with brachial-ankle pulse wave velocity in young adults with type 2 diabetes mellitus in China. Diabetes Metab Res Rev. 2015;31(3):262–268. doi:10.1002/dmrr.2598
4. Liu JJ, Tavintharan S, Yeoh LY, et al. High normal albuminuria is independently associated with aortic stiffness in patients with Type 2 diabetes. Diabet Med. 2014;31(10):1199–1204. doi:10.1111/dme.12461
5. Mule G, Castiglia A, Cusumano C, et al. Subclinical kidney damage in hypertensive patients: a renal window opened on the cardiovascular system. Focus on microalbuminuria. Adv Exp Med Biol. 2017;956:279–306.
6. Swoboda PP, McDiarmid AK, Erhayiem B, et al. Diabetes Mellitus, Microalbuminuria, and Subclinical Cardiac Disease: identification and Monitoring of Individuals at Risk of Heart Failure. J Am Heart Assoc. 2017;6(7). doi:10.1161/JAHA.117.005539
7. Deckert T, Feldt-Rasmussen B, Borch-Johnsen K, et al. Albuminuria reflects widespread vascular damage. The Steno hypothesis. Diabetologia. 1989;32(4):219–226. doi:10.1007/BF00285287
8. Mitchell GF, Hwang S-J, Vasan RS, et al. Arterial stiffness and cardiovascular events: the Framingham Heart Study. Circulation. 2010;121(4):505–511. doi:10.1161/CIRCULATIONAHA.109.886655
9. Van Bortel LM, Laurent S, Boutouyrie P, et al. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J Hypertens. 2012;30(3):445–448. doi:10.1097/HJH.0b013e32834fa8b0
10. Schutte R, Schutte AE, Huisman HW, et al. Arterial stiffness, ambulatory blood pressure and low-grade albuminuria in non-diabetic African and Caucasian men: the SABPA study. Hypertens Res. 2011;34(7):862–868. doi:10.1038/hr.2011.45
11. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021–3104. doi:10.1093/eurheartj/ehy339
12. American Diabetes A. Standards of medical care in diabetes--2014. Diabetes Care. 2014;37(Suppl 1):S14–80.
13. Zhang Y, Wang W, Ning G. Metabolic Management Center: an innovation project for the management of metabolic diseases and complications in China. J Diabetes. 2019;11(1):11–13. doi:10.1111/1753-0407.12847
14. Bonora E, Targher G, Alberiche M, et al. Homeostasis model assessment closely mirrors the glucose clamp technique in the assessment of insulin sensitivity: studies in subjects with various degrees of glucose tolerance and insulin sensitivity. Diabetes Care. 2000;23(1):57–63. doi:10.2337/diacare.23.1.57
15. Lee SB, Ahn CW, Lee BK, et al. Association between triglyceride glucose index and arterial stiffness in Korean adults. Cardiovasc Diabetol. 2018;17(1):41. doi:10.1186/s12933-018-0692-1
16. Ainsworth BE, Haskell WL, Whitt MC, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. 2000;32(9 Suppl):S498–504. doi:10.1097/00005768-200009001-00009
17. Yu XY, Zhao Y, Song X-X, et al. Association between non-alcoholic fatty liver disease and arterial stiffness in the non-obese, non-hypertensive, and non-diabetic young and middle-aged Chinese population. J Zhejiang Univ Sci B. 2014;15(10):879–887. doi:10.1631/jzus.B1400028
18. Kong X, Ma Y, Chen J, et al. Evaluation of the Chronic Kidney Disease Epidemiology Collaboration equation for estimating glomerular filtration rate in the Chinese population. Nephrol Dial Transplant. 2013;28(3):641–651. doi:10.1093/ndt/gfs491
19. Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: a Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024;149(1):e1–e156. doi:10.1161/CIR.0000000000001193
20. Hashimoto Y, Tanaka M, Okada H, et al. Metabolically healthy obesity and risk of incident CKD. Clin J Am Soc Nephrol. 2015;10(4):578–583. doi:10.2215/CJN.08980914
21. Xuan Y, Shen Y, Wang S, et al. The association of hypertriglyceridemic waist phenotype with hypertension: a cross-sectional study in a Chinese middle aged-old population. J Clin Hypertens. 2022;24(2):191–199. doi:10.1111/jch.14424
22. Xuan Y, Zhang W, Wang Y, et al. Association between uric acid to HDL cholesterol ratio and diabetic complications in men and postmenopausal women. Diabetes Metab Syndr Obes. 2023;16:167–177. doi:10.2147/DMSO.S387726
23. Yancy WS, Olsen MK, Guyton JR, et al. A low-carbohydrate, ketogenic diet versus a low-fat diet to treat obesity and hyperlipidemia: a randomized, controlled trial. Ann Intern Med. 2004;140(10):769–777. doi:10.7326/0003-4819-140-10-200405180-00006
24. Danziger J. Importance of low-grade albuminuria. Mayo Clin Proc. 2008;83(7):806–812. doi:10.4065/83.7.806
25. Li MF, Tu Y-F, Li L-X, et al. Low-grade albuminuria is associated with early but not late carotid atherosclerotic lesions in community-based patients with type 2 diabetes. Cardiovasc Diabetol. 2013;12(1):110. doi:10.1186/1475-2840-12-110
26. Huang Y, Chen Y, Xu M, et al. Low-grade albuminuria is associated with carotid intima-media thickness in Chinese type 2 diabetic patients. J Clin Endocrinol Metab. 2010;95(11):5122–5128. doi:10.1210/jc.2010-0544
27. Barzilay JI, Farag YMK, Durthaler J. Albuminuria: an underappreciated risk factor for cardiovascular disease. J Am Heart Assoc. 2024;13(2):e030131. doi:10.1161/JAHA.123.030131
28. Ooi CY, Wang Z, Tabima DM, et al. The role of collagen in extralobar pulmonary artery stiffening in response to hypoxia-induced pulmonary hypertension. Am J Physiol Heart Circ Physiol. 2010;299(6):H1823–31. doi:10.1152/ajpheart.00493.2009
29. Connelly PJ, Casey H, Montezano AC, et al. Sex steroids receptors, hypertension, and vascular ageing. J Hum Hypertens. 2022;36(2):120–125. doi:10.1038/s41371-021-00576-7
30. Agarwal A, Zeng X, Li S, et al. Sodium-glucose cotransporter-2 (SGLT-2) inhibitors for adults with chronic kidney disease: a clinical practice guideline. BMJ. 2024;387:e080257. doi:10.1136/bmj-2024-080257
31. Aroor AR, Das NA, Carpenter AJ, et al. Glycemic control by the SGLT2 inhibitor empagliflozin decreases aortic stiffness, renal resistivity index and kidney injury. Cardiovasc Diabetol. 2018;17(1):108. doi:10.1186/s12933-018-0750-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
MRI-Measured Pancreatic Fat Correlates with Increased Arterial Stiffness in Patients Who are Overweight and Obese
Li C, Chen X, Zhu X, Cao M, Tang Q, Wu W
Diabetes, Metabolic Syndrome and Obesity 2024, 17:2283-2291
Published Date: 6 June 2024