Back to Journals » International Journal of General Medicine » Volume 19
Association Between Stress Hyperglycemia Ratio and Coronary Slow Flow Phenomenon in Patients with MINOCA
Authors Altınkaya O ![]() , Aydemir S, Özmen M, Özkoç M
, Aydemir S, Özmen M, Özkoç M ![]() , Macit R
, Macit R ![]() , Aksakal E
, Aksakal E
Received 9 January 2026
Accepted for publication 16 March 2026
Published 20 March 2026 Volume 2026:19 592704
DOI https://doi.org/10.2147/IJGM.S592704
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Onur Altınkaya,1 Selim Aydemir,1 Murat Özmen,1 Mustafa Özkoç,1 Rauf Macit,2 Emrah Aksakal1,3
1Department of Cardiology, University of Health Sciences, Erzurum City Hospital, Erzurum, Turkey; 2Department of Cardiology, Kağızman State Hospital, Kars, Turkey; 3Department of Medical Pharmacology, Ataturk University, Erzurum, Turkey
Correspondence: Onur Altınkaya, Department of Cardiology, University of Health Sciences, Erzurum City Hospital, Erzurum, Turkey, Tel +90 5426758997, Email [email protected]
Background: Myocardial infarction with non-obstructive coronary arteries (MINOCA) is a heterogeneous clinical entity in which coronary microvascular dysfunction plays a central pathophysiological role. The coronary slow flow phenomenon (CSFP) represents an angiographic manifestation of microvascular dysfunction; however, reliable and practical biomarkers for its identification remain limited. The stress hyperglycemia ratio (SHR) reflects acute metabolic stress beyond chronic glycemic status. This study aimed to investigate the association between SHR and CSFP in patients with MINOCA.
Methods: In this single-center retrospective cohort study, 2073 patients undergoing coronary angiography for suspected myocardial infarction between 1 January 2020 and 1 December 2025 were screened. 354 patients with MINOCA were included. Patients with CSFP were matched 1:2 with controls according to age and sex using exact matching. SHR and other laboratory parameters were assessed. Logistic regression and receiver operating characteristic (ROC) analyses were performed to identify independent predictors of CSFP.
Results: Among the study population, 118 patients (33.3%) had CSFP. Patients with CSFP had significantly higher SHR levels, along with increased C-reactive protein, triglycerides, low-density lipoprotein cholesterol, and uric acid, whereas HbA1c and serum albumin levels were lower (all p < 0.05). In multivariable logistic regression analysis, SHR emerged as the strongest independent predictor of CSFP (OR: 1.48, 95% CI: 1.30– 1.69; p < 0.001). In ROC analysis, SHR demonstrated the highest discriminative performance for CSFP (AUC: 0.74), with an optimal cut-off value of 0.998, yielding a sensitivity of 66.1% and a specificity of 64.3%.
Conclusion: SHR is independently associated with CSFP in patients with MINOCA, suggesting that acute metabolic stress plays a key role in coronary microvascular dysfunction. SHR may serve as a simple and readily available marker for identifying high-risk microvascular phenotypes in MINOCA patients.
Keywords: myocardial infarction with non-obstructive coronary arteries, coronary slow flow phenomenon, stress hyperglycemia ratio, coronary microvascular dysfunction
Introduction
Myocardial infarction with non-obstructive coronary arteries (MINOCA) accounts for approximately 5–10% of all acute myocardial infarction cases and represents a clinically challenging syndrome due to its heterogeneous pathophysiology, which complicates both diagnosis and management.1 Despite angiographically normal or near-normal epicardial coronary arteries, patients with MINOCA may develop significant myocardial injury and ischemia, highlighting the importance of pathophysiological mechanisms beyond epicardial coronary disease. Current evidence and consensus reports indicate that coronary microvascular dysfunction, endothelial dysfunction, vasospasm, inflammation, and acute metabolic stress play a central role in the pathogenesis of MINOCA.2
The coronary slow flow phenomenon (CSFP) is characterized by delayed contrast progression within the epicardial coronary arteries in the absence of obstructive coronary artery disease and is considered an angiographic manifestation of coronary microvascular dysfunction.3 Contemporary studies have demonstrated that CSFP is associated with recurrent angina, acute coronary syndrome–like clinical presentations, and an increased risk of major adverse cardiovascular events.4,5 Notably, the presence of CSFP in patients with MINOCA further underscores the clinical relevance of impaired coronary microvascular perfusion.
Despite growing interest in this area, clinically practical and reliable markers capable of predicting adverse outcomes and underlying microvascular dysfunction in patients with MINOCA and CSFP remain limited. In recent years, several inflammatory and metabolic biomarkers have been reported to be associated with CSFP and coronary microvascular dysfunction.6–8 However, most of these markers predominantly reflect chronic metabolic burden and may inadequately capture the contribution of acute stress–related metabolic responses.
The stress hyperglycemia ratio (SHR) is a parameter that differentiates acute stress–induced hyperglycemia from an individual’s underlying chronic glycemic status, thereby providing a more specific reflection of the metabolic component of systemic stress.9 Previous studies have demonstrated that SHR is independently associated with adverse clinical outcomes and poor prognosis in patients with coronary artery disease.10,11 In addition, studies conducted in heart failure and MINOCA cohorts have reported that elevated SHR levels are associated with worse long-term outcomes.12,13
To date, no study has directly explored the relationship between SHR and CSFP, an angiographic marker of coronary microvascular dysfunction, beyond clinical outcomes. Therefore, the present study aimed to investigate the association between SHR and CSFP in patients with MINOCA and to evaluate the potential predictive value of SHR for the presence of CSFP.
Materials and Methods
Study Design and Population
This single-center study was designed as a retrospective cohort study. A total of 2073 patients aged ≥18 years who presented to our clinic with chest pain between 1 January 2020 and 1 December 2025, underwent coronary angiography with a preliminary diagnosis of myocardial infarction, and were found to have no obstructive coronary artery disease (≥50% stenosis) were included.
MINOCA was defined as cases fulfilling the universal definition of myocardial infarction, with <50% coronary stenosis on angiography and no alternative clinically overt cause explaining the acute presentation.14–16
Based on coronary angiographic findings, patients with CSFP were matched with controls in a 1:2 ratio using exact matching for age and sex to reduce potential confounding. Control patients were randomly selected from individuals meeting the matching criteria.
Patients with heart failure, moderate-to-severe valvular heart disease, cardiomyopathy, previously known coronary artery disease, coronary artery aneurysm, spasm, ectasia or dissection, peripheral arterial disease, non-sinus rhythm, advanced liver or renal failure (eGFR <30 mL/min/1.73 m2), acute or chronic infection, malignancy, trauma, chronic obstructive pulmonary disease, anemia, autoimmune, hematologic or chronic inflammatory diseases, as well as those with missing laboratory or angiographic data, were excluded (Figure 1).
 |
Figure 1 Flowchart of the study population. |
Data Collection
Demographic, clinical, laboratory, and angiographic data were obtained from the hospital electronic medical records. Angiographic images and clinical data were evaluated by an experienced interventional cardiologist.
Laboratory Measurements
Venous blood samples were collected after at least 8 hours of fasting prior to coronary angiography. Complete blood count, fasting plasma glucose, HbA1c, C-reactive protein (CRP), high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, uric acid, creatinine, triglycerides, thyroid function tests, aspartate aminotransferase (AST), and albumin levels were measured using standard automated analyzers. SHR was calculated using the following formula (with glucose expressed in mmol/L): Fasting glucose (mmol/L)/ [1.59×HbA1c (%)−2.59]. Glucose values measured in mg/dL were converted to mmol/L by dividing by 18.17–19 The triglyceride–glucose index (TGI) was calculated as: ln [Triglycerides (mg/dL)×fasting glucose (mg/dL)/2].20
Coronary Angiographic Assessment
Coronary angiography was performed using the standard Judkins technique at 30 frames per second. At least four projections were obtained for the left coronary system and two projections for the right coronary artery (RCA). The first frame was defined as the frame in which contrast filled >70% of the arterial lumen antegradely, and the final frame as the moment contrast reached predefined distal landmarks (distal bifurcation for the left anterior descending coronary artery (LAD), distal bifurcation of the obtuse marginal branch for the circumflex coronary artery (LCX), and the first branch of the posterolateral artery for the RCA. CSFP was defined as a corrected TIMI frame count (TFC) exceeding the established normal reference values in at least one major epicardial coronary artery. Due to vessel length, LAD TFC values were corrected by dividing by 1.7, yielding the corrected TFC (cTFC) Validation and normal reference values were based on the original work by Gibson et al Normal cut-off values for epicardial coronary filling were defined as 36.2 ± 2.6 for the LAD (corrected: 21.1 ± 1.5), 22.1 ± 4.1 for the LCX, and 20.4 ± 3 for the RCA.21
Statistical Analysis
Statistical analyses were performed using SPSS software (version 27.0; IBM Corp., Armonk, NY, USA). Continuous variables were tested for normality using the Kolmogorov–Smirnov test and are presented as mean ± standard deviation or median (interquartile range), as appropriate. Categorical variables are expressed as numbers and percentages. Group comparisons were conducted using the Student’s t-test or Mann–Whitney U-test for continuous variables and the chi-square test for categorical variables. Factors associated with CSFP were evaluated using logistic regression analysis. Pearson correlation analysis was performed. The correlated parameters were not included in the regression analysis. Multicollinearity was assessed using the variance inflation factor (VIF), and variables with VIF >10 were excluded from the multivariable model. Discriminative performance was assessed using receiver operating characteristic (ROC) curve analysis, and the optimal cut-off value was determined using the Youden index. A p-value <0.05 was considered statistically significant.
Results
A total of 354 patients were included in the study. Based on coronary angiographic findings, patients were classified into two groups according to the presence or absence of CSFP and were matched in a 1:2 ratio according to age and sex. The mean age of the overall cohort was 55.6 ± 6.8 years, and 66.9% of the patients were male.
Baseline demographic, clinical, and laboratory characteristics of the study population are summarized in Table 1. Patients with CSFP had significantly higher levels of CRP, glucose, triglycerides, LDL cholesterol, uric acid, SHR, and TGI compared with those without CSFP (all p < 0.05). In contrast, HbA1c and serum albumin levels were significantly lower in the CSFP group (p < 0.05). No significant differences were observed between the two groups with respect to other demographic variables, medication use, or routine hematological and biochemical parameters.
 |
Table 1 Baseline Demographic, Clinical, and Laboratory Characteristics Stratified by CSFP Status |
Angiographic characteristics are presented in Table 2. TFC values for the left anterior descending artery (LAD), circumflex artery (CX), and right coronary artery (RCA) were significantly higher in the CSFP group than in the control group (all p < 0.001). Among patients with CSFP, single-vessel involvement was observed in 55.9% of cases, while two- and three-vessel involvement were present in 23.7% and 20.3%, respectively. The RCA was the most frequently affected vessel (61.9%).
 |
Table 2 Angiographic Characteristics of the Two Groups |
Pearson correlation analysis revealed a significant positive correlation between SHR and HbA1c (r = 0.323) as well as between SHR and fasting glucose (r = 0.860). Multicollinearity analysis demonstrated that the variance inflation factor (VIF) values for SHR, glucose, and HbA1c exceeded 10. Therefore, glucose and HbA1c were excluded from the regression model. Accordingly, SHR was retained as a composite marker reflecting acute glycemic stress.
Variables significantly associated with CSFP were entered into logistic regression analyses (Table 3). In univariable analysis, higher levels of CRP, uric acid, LDL cholesterol, triglycerides, and SHR were significantly associated with the presence of CSFP, whereas serum albumin levels showed an inverse association. In multivariable logistic regression analysis, uric acid (OR: 1.27, 95% CI: 1.03–1.56; p = 0.020), LDL cholesterol (OR: 1.02, 95% CI: 1.01–1.03; p < 0.001), and triglyceride levels (OR: 1.01, 95% CI: 1.01–1.01; p < 0.001) remained independently associated with CSFP. Notably, SHR emerged as the strongest independent predictor of CSFP. Each 0.1-unit increase in SHR was associated with a 48% higher likelihood of CSFP after adjustment for potential confounders (OR: 1.483, 95% CI: 1.30–1.68; p < 0.001).
 |
Table 3 Logistic Regression Analysis of Parameters Significantly Associated with CSFP |
Receiver operating characteristic (ROC) curve analysis was performed to compare the discriminatory performance of SHR with previously reported biomarkers associated with CSFP (Figure 2). SHR demonstrated the highest predictive value for CSFP, with an area under the curve (AUC) of 0.740 (95% CI: 0.688–0.792; p < 0.001), outperforming TGI and the LDL/HDL ratio (Table 4). Using the optimal cut-off value of 0.998 determined by the Youden index, SHR predicted CSFP with a sensitivity of 66.1% and a specificity of 64.3%.
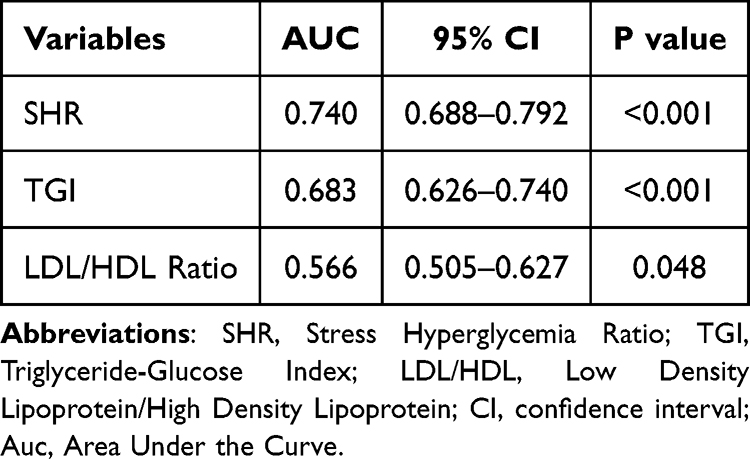 |
Table 4 Area Under the Curve Values (AUC) of Parameters |
 |
Figure 2 Receiver operating characteristic (ROC) curve analysis. |
Discussion
In this study, we investigated the association between SHR and CSFP in patients with MINOCA. Our findings demonstrated that SHR was significantly and independently associated with the presence of CSFP. Elevated SHR emerged as a novel predictive parameter for CSFP, an angiographic manifestation of coronary microvascular dysfunction in MINOCA patients. Moreover, SHR showed superior discriminative ability for predicting CSFP compared with previously reported metabolic and lipid parameters. To the best of our knowledge, this is the first study to directly examine the relationship between SHR and CSFP within the MINOCA spectrum.
MINOCA accounts for approximately 5–10% of all acute myocardial infarction cases and represents a clinically challenging syndrome due to its heterogeneous and complex pathophysiology.1 Accumulating evidence suggests that coronary microvascular dysfunction, endothelial impairment, vasospasm, inflammation, and acute metabolic stress play central roles in the pathogenesis of MINOCA.2 In this context, CSFP, which is frequently observed in MINOCA, is considered an angiographic surrogate of impaired microvascular perfusion.3 Despite the absence of obstructive coronary artery disease, both MINOCA and CSFP have been associated with a substantial long-term risk of major adverse cardiovascular events and mortality.3,13,22,23 However, data regarding reliable risk stratification tools and predictors of adverse outcomes in this population remain limited. Recent studies have highlighted potential associations between inflammatory and metabolic biomarkers and both MINOCA and CSFP.6–8,24,25
CSFP is an angiographic finding observed in patients without obstructive coronary artery disease, with a reported incidence ranging from 1% to 7% across different series.4 Although previously regarded as a benign angiographic variant, growing evidence indicates that CSFP is closely associated with adverse cardiovascular outcomes, including malignant ventricular arrhythmias, acute coronary syndromes, and sudden cardiac death.3,5 A substantial proportion of patients with CSFP experience recurrent angina-like chest pain leading to repeated emergency department visits or hospital admissions.26,27
The pathogenesis of CSFP remains incompletely understood; however, current evidence suggests a multifactorial process involving coronary microvascular dysfunction, endothelial dysfunction, heightened inflammatory activity, and metabolic dysregulation. Increased TIMI frame count values in the absence of epicardial stenosis reflect impaired microvascular perfusion.26 The lack of clearly defined risk factors and the association of CSFP with adverse clinical outcomes underscore that it represents more than a simple angiographic finding. Consequently, various biomarkers have been investigated to improve CSFP identification and prediction. Several inflammatory and nutritional indices, including the inflammatory burden index, systemic immune-inflammation index, neutrophil percentage-to-albumin ratio, and global immune-nutritional inflammation index, as well as metabolic markers such as the triglyceride–glucose index, atherogenic lipid parameters, and uric acid levels, have been linked to CSFP.28–32 In line with these mechanisms, microvascular perfusion abnormalities such as the no-reflow phenomenon have also been linked to endothelial dysfunction and metabolic disturbances. In a recent study, elevated homocysteine levels were reported to be associated with the occurrence of the coronary no-reflow phenomenon in patients undergoing primary percutaneous coronary intervention.33 Consistent with these reports, our study demonstrated significantly higher CRP, glucose, triglyceride, LDL cholesterol, and uric acid levels in patients with CSFP, supporting the presence of a pronounced inflammatory–metabolic milieu underlying this phenomenon.
SHR is a parameter that distinguishes acute stress-induced hyperglycemia from chronic glycemic status, thereby more specifically reflecting the metabolic component of systemic stress.9 During acute stress, elevations in catecholamines, cortisol, and glucagon promote insulin resistance, accelerate gluconeogenesis and glycogenolysis, and result in marked hyperglycemia. Beyond a metabolic response, this process is closely linked to endothelial dysfunction, oxidative stress, and inflammatory activation.34,35 Experimental and clinical data indicate that acute hyperglycemia reduces nitric oxide bioavailability, increases reactive oxygen species, and impairs endothelial vasodilatory responses.35,36 In addition, stress hyperglycemia may exacerbate microvascular perfusion abnormalities by enhancing platelet activation and coagulation.37,38 Acute stress hyperglycemia may contribute to CSFP development by promoting microvascular dysfunction through these pathophysiological mechanisms.39
SHR has been associated with adverse outcomes across a wide range of cardiovascular conditions. In studies evaluating SHR, elevated SHR has been associated with adverse clinical outcomes in patients with ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention.10 Another study demonstrated that higher SHR levels were independently associated with poor prognosis in patients with acute coronary syndrome.11 In a recent meta-analysis assessing the prognostic value of SHR in patients with heart failure, studies using an SHR cut-off value of ≥1.05 showed a more pronounced association with all-cause mortality compared with those applying a cut-off value of <1.05.40 In patients with heart failure with preserved ejection fraction (HFpEF), a study evaluating long-term clinical outcomes reported that an SHR ≥0.99 was independently associated with increased risks of all-cause mortality, cardiovascular mortality, and rehospitalization due to heart failure.12 Other studies have shown that SHR is an important predictor of major adverse cardiovascular events (MACE) in patients with chronic total occlusion41 and triple-vessel coronary artery disease.42 In a study conducted by Fuad A. Abdu et al, elevated SHR was associated with poor long-term prognosis in patients with MINOCA.13 Similarly, in a MINOCA cohort analyzed by Gao et al, higher SHR levels were also linked to adverse clinical outcomes.43 However, most of these studies evaluated SHR solely in relation to clinical outcomes.
Our study demonstrates that SHR, which integratively assesses acute glycemic response and chronic glycemic status, is significantly and independently associated with CSFP—an angiographic marker of microvascular dysfunction—in patients with MINOCA, thereby offering a novel perspective beyond clinical prognosis.
In line with the existing literature, the present study demonstrated that patients with CSFP had significantly higher levels of CRP, glucose, uric acid, LDL cholesterol, triglycerides, and SHR, whereas HbA1c and serum albumin levels were lower. Elevated CRP, uric acid, and atherogenic lipid parameters may reflect an enhanced inflammatory and oxidative stress milieu, which has been implicated in endothelial dysfunction and impaired coronary microvascular perfusion. In contrast, lower albumin levels may indicate an increased inflammatory burden and reduced antioxidant capacity, while relatively lower HbA1c levels suggest that acute stress–related hyperglycemia, rather than chronic glycemic exposure, may play a more prominent role in the pathogenesis of CSFP. Moreover, the independent associations of uric acid, LDL cholesterol, triglycerides, and particularly SHR with CSFP in multivariable regression analysis further underscore the contribution of acute metabolic stress to this pathophysiological process. Additionally, in ROC curve analysis, SHR exhibited superior discriminative performance compared with other biomarkers (AUC: 0.74). The SHR cut-off value of 0.998 identified in our study is consistent with previously reported SHR cut-off values in the literature and further supports its clinical applicability.
Given that CSFP in MINOCA patients is associated with increased symptom burden, recurrent angina, and adverse cardiovascular outcomes, early recognition of this phenotype is clinically important. In the setting of MINOCA, where conventional angiography often fails to identify an obvious culprit lesion, SHR may help identify a high-risk microvascular phenotype requiring closer surveillance and tailored management. As a readily available parameter derived from routine laboratory tests, SHR represents a practical and accessible tool for early risk stratification and suspicion of coronary microvascular dysfunction in this patient population.
Limitations
This study has several limitations. The retrospective and single-center design limits causal interpretation of the findings. Patients were carefully matched for age and sex; however, despite multivariable regression analyses, residual confounding may still exist. Coronary microvascular function was evaluated using TFC rather than invasive physiological measurements. Moreover, CSFP is a dynamic condition, and a single angiographic assessment may not fully reflect temporal variations in microvascular function. Nevertheless, the real-world nature of this cohort mirrors routine clinical practice and supports the clinical relevance of our results. Finally, large-scale multicenter prospective studies are needed to validate the role of SHR in different populations and clinical subgroups.
Conclusion
In conclusion, this study demonstrated that SHR is independently associated with CSFP in patients with MINOCA. Our findings suggest that acute metabolic stress and systemic inflammation may contribute to the development of coronary microvascular dysfunction. Given its simplicity and availability, SHR can be considered a potential risk stratification marker for CSFP. Further prospective studies are needed to clarify its clinical utility and predictive value in MINOCA patients.
Abbreviations
ACEI, Angiotensin-Converting Enzyme Inhibitor; ACS, Acute Coronary Syndrome; ARB, Angiotensin Receptor Blocker; AST, Aspartate Aminotransferase; AUC, Area Under the Curve; BMI, Body Mass Index; CCB, Calcium Channel Blocker; CI, Confidence Interval; CRP, C-Reactive Protein; CSFP, Coronary Slow Flow Phenomenon; cTFC, Corrected TIMI Frame Count; CX (LCX), Circumflex Coronary Artery; DM, Diabetes Mellitus; eGFR, Estimated Glomerular Filtration Rate; Hb, Hemoglobin; HbA1c, Glycated Hemoglobin; HDL, High-Density Lipoprotein; HFpEF, Heart Failure with Preserved Ejection Fraction; HT, Hypertension; LAD, Left Anterior Descending Coronary Artery; LDL, Low-Density Lipoprotein; MACE, Major Adverse Cardiovascular Events; MI, Myocardial Infarction; MINOCA, Myocardial Infarction with Non-Obstructive Coronary Arteries; OR, Odds Ratio; PLT, Platelet; RCA, Right Coronary Artery; ROC, Receiver Operating Characteristic; SHR, Stress Hyperglycemia Ratio; TFC, TIMI Frame Count; TG, Triglyceride; TGI, Triglyceride–Glucose Index; VIF, Variance Inflation Factor; WBC, White Blood Cell.
Data Sharing Statement
The dataset examined in this study is available upon reasonable request from the corresponding author.
Ethics Approval and Consent to Participate
The studies involving human participants were approved by the University of Health Sciences Erzurum Faculty of Medicine Scientific Research Ethics Committee (Approval No: 2025/12-336; Date: December 10, 2025). This study was conducted in accordance with local legislation, institutional requirements, and the principles of the Declaration of Helsinki. Due to the retrospective design of the study, the requirement for informed consent was waived by the Ethics Committee. Patient confidentiality was strictly maintained, and all data were anonymized prior to analysis.
Acknowledgments
We express our gratitude to all individuals who contributed to this project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Lindahl B, Baron T, Albertucci M, Prati F. Myocardial infarction with non-obstructive coronary artery disease. EuroIntervention. 2021;17(11):e875–11. doi:10.4244/EIJ-D-21-00426
2. Sucato V, Comparato F, Ortello A, Galassi AR. Myocardical infarction with non-obstructive coronary arteries (MINOCA): pathogenesis, diagnosis and treatment. Curr Probl Cardiol. 2024;49(7):102583. doi:10.1016/j.cpcardiol.2024.102583
3. Mareai RM, Mohammed AQ, Zhang H, et al. Prognostic implication of coronary slow flow assessed by cTFC in patients with myocardial infarction with non-obstructive coronary arteries. Eur J Intern Med. 2023;108:74–80. doi:10.1016/j.ejim.2022.11.026
4. Dai XT, Kong TZ, Zhang XJ, Luan B, Wang Y, Hou AJ. Relationship between increased systemic immune-inflammation index and coronary slow flow phenomenon. BMC Cardiovasc Disord. 2022;22(1):362. doi:10.1186/s12872-022-02798-0
5. Cutri N, Zeitz C, Kucia AM, Beltrame JF. ST/T wave changes during acute coronary syndrome presentation in patients with the coronary slow flow phenomenon. Int J Cardiol. 2011;146(3):457–458. doi:10.1016/j.ijcard.2010.10.120
6. Ma W, Gao S, Huang S, Yuan J, Yu M. Hyperuricemia as a prognostic marker for long-term outcomes in patients with myocardial infarction with nonobstructive coronary arteries. Nutr Metab. 2021;18(1):107. doi:10.1186/s12986-021-00636-2
7. Eggers KM, Baron T, Hjort M, Nordenskjold AM, Tornvall P, Lindahl B. Clinical and prognostic implications of C-reactive protein levels in myocardial infarction with nonobstructive coronary arteries. Clin Cardiol. 2021;44(7):1019–1027. doi:10.1002/clc.23651
8. Nordenskjold AM, Baron T, Eggers KM, Jernberg T, Lindahl B. Predictors of adverse outcome in patients with myocardial infarction with non-obstructive coronary artery (MINOCA) disease. Int J Cardiol. 2018;261:18–23. doi:10.1016/j.ijcard.2018.03.056
9. Roberts GW, Quinn SJ, Valentine N, et al. Relative hyperglycemia, a marker of critical illness: introducing the stress hyperglycemia ratio. J Clin Endocrinol Metab. 2015;100(12):4490–4497. doi:10.1210/jc.2015-2660
10. Yang Y, Kim TH, Yoon KH, et al. The stress hyperglycemia ratio, an index of relative hyperglycemia, as a predictor of clinical outcomes after percutaneous coronary intervention. Int J Cardiol. 2017;241:57–63. doi:10.1016/j.ijcard.2017.02.065
11. Zeng G, Song Y, Zhang Z, et al. Stress hyperglycemia ratio and long-term prognosis in patients with acute coronary syndrome: a multicenter, nationwide study. J Diabetes. 2023;15(7):557–568. doi:10.1111/1753-0407.13400
12. Mohammed AQ, Luo Y, Wang K, et al. Stress hyperglycemia ratio as a prognostic indicator for long-term adverse outcomes in heart failure with preserved ejection fraction. Cardiovasc Diabetol. 2024;23(1):67. doi:10.1186/s12933-024-02157-7
13. Abdu FA, Galip J, Qi P, et al. Association of stress hyperglycemia ratio and poor long-term prognosis in patients with myocardial infarction with non-obstructive coronary arteries. Cardiovasc Diabetol. 2023;22(1):11. doi:10.1186/s12933-023-01742-6
14. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138(20):e618–e651. doi:10.1161/CIR.0000000000000617
15. Bakhshi H, Gibson CM. MINOCA: myocardial infarction no obstructive coronary artery disease. Am Heart J Plus. 2023;33:100312. doi:10.1016/j.ahjo.2023.100312
16. Tamis-Holland JE, Jneid H, Reynolds HR, et al. Contemporary diagnosis and management of patients with myocardial infarction in the absence of obstructive coronary artery disease: a scientific statement from the American heart association. Circulation. 2019;139(18):e891–e908. doi:10.1161/CIR.0000000000000670
17. Nathan DM, Kuenen J, Borg R, et al. Translating the A1C assay into estimated average glucose values. Diabetes Care. 2008;31(8):1473–1478. doi:10.2337/dc08-0545
18. Xia Z, Gu T, Zhao Z, et al. The stress hyperglycemia ratio, a novel index of relative hyperglycemia, predicts short-term mortality in critically ill patients after esophagectomy. J Gastrointest Oncol. 2022;13(1):56–66. doi:10.21037/jgo-22-11
19. Riemsma R, Ramos IC, Birnie R, et al. Appendix 5: conversion tables for glycated haemoglobin and glucose values. In: Integrated Sensor-Augmented Pump Therapy Systems for Managing Blood Glucose Levels in Type 1 Diabetes. NIHR Journals Library; 2016.
20. Araujo SP, Juvanhol LL, Bressan J, Hermsdorff HHM. Triglyceride glucose index: a new biomarker in predicting cardiovascular risk. Prev Med Rep. 2022;29:101941. doi:10.1016/j.pmedr.2022.101941
21. Gibson CM, Cannon CP, Daley WL, et al. TIMI frame count: a quantitative method of assessing coronary artery flow. Circulation. 1996;93(5):879–888. doi:10.1161/01.cir.93.5.879
22. Dreyer RP, Tavella R, Curtis JP, et al. Myocardial infarction with non-obstructive coronary arteries as compared with myocardial infarction and obstructive coronary disease: outcomes in a medicare population. Eur Heart J. 2020;41(7):870–878. doi:10.1093/eurheartj/ehz403
23. Pasupathy S, Air T, Dreyer RP, Tavella R, Beltrame JF. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation. 2015;131(10):861–870. doi:10.1161/CIRCULATIONAHA.114.011201
24. Khorasani N, Mohammadi Y, Sarpoli M, Kazemi T, Riahi SM. Understanding myocardial infarction with non-obstructive coronary arteries (MINOCA): a comprehensive meta-analysis of clinical characteristics, management, and prognosis compared to MI with the obstructive coronary artery (MIOCA). BMC Cardiovasc Disord. 2025;25(1):143. doi:10.1186/s12872-025-04504-2
25. Berbach L, Fadel E, Potter BJ, Forcillo J, Pacheco C. Clinical and prognostic value of biomarkers in patients with non-obstructive coronary artery disease: a systematic review and meta-analysis. Biomarker Med. 2025;19(22):1161–1180. doi:10.1080/17520363.2025.2590780
26. Aparicio A, Cuevas J, Moris C, Martin M. Slow coronary blood flow: pathogenesis and clinical implications. Eur Cardiol. 2022;17:e08. doi:10.15420/ecr.2021.46
27. Kaplan M, Abacioglu OO, Yavuz F, Kaplan GI, Topuz M. Slow flow phenomenon impairs the prognosis of coronary artery ectasia as well as coronary atherosclerosis. Braz J Cardiovasc Surg. 2021;36(3):346–353. doi:10.21470/1678-9741-2020-0618
28. Wen ZG, Long JJ, Wang Y. Association between inflammatory burden index and coronary slow flow phenomenon in patients with chest pain and no obstructive coronary arteries. BMC Cardiovasc Disord. 2024;24(1):595. doi:10.1186/s12872-024-04281-4
29. Guo J, Xiang ZZ, Ma DD. The global immune-nutrition inflammation index for predicting coronary slow flow phenomenon in patients with angina and no obstructive coronary arteries. Int J Gen Med. 2025;18:1325–1332. doi:10.2147/IJGM.S516108
30. Zang SW, Long JJ, Wang Y. Neutrophil percentage to albumin ratio as a predictor for coronary slow flow phenomenon in patients with myocardial ischemia with no obstructive coronary arteries. Int J Gen Med. 2024;17:3511–3519. doi:10.2147/IJGM.S477431
31. Gao S, Ma W, Huang S, Lin X, Yu M. Impact of triglyceride-glucose index on long-term cardiovascular outcomes in patients with myocardial infarction with nonobstructive coronary arteries. Nutr Metab Cardiovasc Dis. 2021;31(11):3184–3192. doi:10.1016/j.numecd.2021.07.027
32. Zhang XJ, Hou AJ, Luan B, Wang CF, Li JJ. Uric acid to albumin ratio as a novel predictor for coronary slow flow phenomenon in patients with chronic coronary syndrome and non-obstructive coronary arteries. BMC Cardiovasc Disord. 2024;24(1):358. doi:10.1186/s12872-024-04040-5
33. Omar T, Karabağ Y, Öğün M, et al. The relationship between homocysteine and no-reflow phenomenon in patients undergoing primary percutaneous coronary intervention. J Health Sci Med. 2024;7(2):199–205. doi:10.32322/jhsm.1413552
34. Yuan T, Yang T, Chen H, et al. New insights into oxidative stress and inflammation during diabetes mellitus-accelerated atherosclerosis. Redox Biol. 2019;20:247–260. doi:10.1016/j.redox.2018.09.025
35. Paneni F, Beckman JA, Creager MA, Cosentino F. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part I. Eur Heart J. 2013;34(31):2436–2443. doi:10.1093/eurheartj/eht149
36. Meza CA, La Favor JD, Kim DH, Hickner RC. Endothelial dysfunction: is there a hyperglycemia-induced imbalance of NOX and NOS? Int J Mol Sci. 2019;20(15):3775. doi:10.3390/ijms20153775
37. Song G, Liu X, Lu Z, et al. Relationship between stress hyperglycaemic ratio (SHR) and critical illness: a systematic review. Cardiovasc Diabetol. 2025;24(1):188. doi:10.1186/s12933-025-02751-3
38. Lemkes BA, Hermanides J, Devries JH, Holleman F, Meijers JC, Hoekstra JB. Hyperglycemia: a prothrombotic factor? J Thromb Haemost. 2010;8(8):1663–1669. doi:10.1111/j.1538-7836.2010.03910.x
39. Meziat C, Loader J, Reboul C, Walther G. Acute hyperglycemia impairs flow-mediated dilatation through an increase in vascular oxidative stress: winter is coming for excess sugar consumption. J Thorac Dis. 2016;8(9):E1103–E1105. doi:10.21037/jtd.2016.07.99
40. Li L, Zhao Z, Wang S, Wang J. Stress hyperglycemia ratio and the clinical outcome of patients with heart failure: a meta-analysis. Front Endocrinol. 2024;15:1404028. doi:10.3389/fendo.2024.1404028
41. Song Y, Cui K, Yang M, et al. High triglyceride-glucose index and stress hyperglycemia ratio as predictors of adverse cardiac events in patients with coronary chronic total occlusion: a large-scale prospective cohort study. Cardiovasc Diabetol. 2023;22(1):180. doi:10.1186/s12933-023-01883-8
42. Qiao Z, Bian X, Song C, et al. High stress hyperglycemia ratio predicts adverse clinical outcome in patients with coronary three-vessel disease: a large-scale cohort study. Cardiovasc Diabetol. 2024;23(1):190. doi:10.1186/s12933-024-02286-z
43. Gao S, Huang S, Lin X, Xu L, Yu M. Prognostic implications of stress hyperglycemia ratio in patients with myocardial infarction with nonobstructive coronary arteries. Ann Med. 2023;55(1):990–999. doi:10.1080/07853890.2023.2186479
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Stress Hyperglycemia Ratio Outperforms Admission Glucose in Predicting Coronary Slow Flow in Patients with Type 2 Diabetes Mellitus
Bedir Ö, Polat İ
International Journal of General Medicine 2026, 19:615891
Published Date: 7 July 2026