")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Association Between Severity of Diabetic Neuropathy and Success in Weight Loss During Hospitalization Among Japanese Patients with Type 2 Diabetes: A Retrospective Observational Study
Authors Nakanishi S , Hirukawa H , Shimoda M, Tatsumi F, Kohara K, Obata A, Okauchi S, Sanada J, Fushimi Y, Mashiko A, Mune T, Kaku K, Kaneto H
Received 5 March 2020
Accepted for publication 30 April 2020
Published 15 May 2020 Volume 2020:13 Pages 1669—1676
DOI https://doi.org/10.2147/DMSO.S252673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Shuhei Nakanishi,1 Hidenori Hirukawa,1 Masashi Shimoda,1 Fuminori Tatsumi,1 Kenji Kohara,1 Atsushi Obata,1 Seizo Okauchi,1 Junpei Sanada,1 Yoshiro Fushimi,1 Akiko Mashiko,1 Tomoatsu Mune,1 Kohei Kaku,2 Hideaki Kaneto1
1Division of Diabetes, Metabolism and Endocrinology, Kawasaki Medical School, Okayama, Japan; 2Department of Internal Medicine, Kawasaki Medical School, Okayama, Japan
Correspondence: Shuhei Nakanishi Email [email protected]
Introduction: This study aimed to examine the association between severity of diabetic neuropathy and weight loss during hospitalization in overweight participants with type 2 diabetes.
Patients and Methods: Participants of this study comprised 193 patients who were hospitalized for type 2 diabetes treatment. The participants were divided into two groups in the study, based on whether or not reduction of bodyweight was at least 3% during hospitalization. Using Cox models, the association between severity of neuropathy and effectiveness of weight loss under a controlled diet was analyzed. Autonomic neuropathy was assessed on patient admission by R-R interval, as measured in an electrocardiogram (CVRR), and sensory neuropathy was assessed using both 128-Hz tuning-fork vibration and Achilles tendon reflex (ATR).
Results: The adjusted hazard ratio for weight loss of at least 3% for CVRR was 1.17 (95% confidence interval 1.07– 1.28, P=0.0006) and for vibration time 1.93 (1.01– 3.68, P=0.045). After dividing CVRR and vibration time into tertiles based on participant number, the adjusted hazard ratio for the high tertile of CVRR was 2.17 (1.29– 3.62, P=0.003), and for the long tertile of vibration time 1.84 (1.10– 3.08, P=0.02), compared with the low and short tertiles, respectively. No association was detected between ATR category and weight loss.
Conclusion: Severity of diabetic neuropathy was found to be a determinant in weight loss under a caloric restriction regimen for patients with type 2 diabetes. The results of the study suggest that the peripheral nervous system is involved in responses to medical intervention for treatment for type 2 diabetes including bodyweight management.
Keywords: diabetic neuropathy, weight loss, R-R interval as measured in an electrocardiogram, type 2 diabetes
Introduction
Type 2 diabetes mellitus (T2D) is a chronic metabolic disease affecting populations worldwide that has become an important public health challenge in not only Japan but also other Asian countries.1,2 Obesity is one of the important drivers of what can be called the T2D epidemic,2 with much of the recent increase in diabetes prevalence related to changes in dietary pattern, sedentary behavior, and obesity layered upon a background of genetic and epigenetic susceptibility.3 Obesity is associated with an increased risk of developing lifestyle-related diseases such as hypertension, insulin resistance, and dyslipidemia, which are major elements comprising metabolic syndrome. For treatment of T2D, intensive bodyweight management based on strict diet therapy is a key strategy, with remission of the disease a potential outcome.4 Under such circumstances, the 2013 AHA/ACC/TOS guidelines recommend sustained weight loss of at least 3%, because that level likely results in clinically meaningful reductions in blood glucose and HbA1c levels.5 In overweight and obese Japanese subjects as well, weight loss of at least 1–3% was reported to reduce HbA1c levels.6
Vagal afferent nerves are understood to sense peripheral metabolic signals, including nutrients, hormones, and metabolites, converting them to neural signals. These neural signals are conveyed to the central nervous system for the regulation of energy metabolism. For example, reduction of food intake by intraperitoneal injection of pancreatic polypeptide (PP) and peptide YY3–36 (PYY3-36), potential orexigenic peptides, was impaired in abdominal-vagotomized animals,7,8 suggesting that PP and PYY3-36 impact anorexigenic effects through the action of vagal afferent nerves. Moreover, fasting signals derived from the liver transmitted through the vagal nerve might have comprehensive effects on the regulation of systemic energy metabolism,9 suggesting that the vagal nerve comprises a crucial constituent for appetite regulation via the gut-brain axis.10 Specifically, adipose tissue might be an effector of neurocircuitry. On the other hand, the most common manifestation of diabetic neuropathy is a generalized and approximately symmetrical polyneuropathy that predominantly involves sensory and autonomic function. Accordingly, transfer of food-consumption information from gastric peptides via autonomic nerves may be obstructed by diabetic autonomic neuropathy, leading to disorders such as overeating in patients with T2D, but presumably not by sensory or motor nerve damage. In addition, the response in T2D patients with autonomic neuropathy may be poor with respect to several treatments for T2D, such as caloric restriction, caused by the defective transfer of metabolic signals. However, human data investigating any association between bodyweight and neuropathy are as yet scarce.
Coefficient variation of R-R intervals in electrocardiogram (CVRR) testing is routinely used to assess parasympathetic nerve function. Such analysis is the simplest and most convenient technique for evaluating cardiac autonomic function.11 High variation in R-R interval indicates strong activation of cardiac parasympathetic nerves. Accordingly, CVRR is used to assess diabetic autonomic neuropathy. In addition, vibratory sensation assessed with a 128-Hz tuning fork at the medial malleolus and Achilles tendon reflex (ATR) are two methods commonly used in routine medical care to assess sensory nerve damage caused by diabetic neuropathy.
The aim of this retrospective study was to evaluate diabetic neuropathy in three ways on patient admission: CVRR, vibratory sensation, and ATR, as well as to investigate their association with quantity of weight loss during hospitalization for treatment of T2D by strict and controlled diet therapy, based on the hypothesis that severity of diabetic autonomic neuropathy might affect and be involved in bodyweight changes.
Patients and Methods
Study Population and Preparation of Participants
The participants of this study comprised 116 men and 77 women who had been hospitalized for treatment of T2D at Kawasaki Medical School Hospital at some point in time between January 2016 and March 2019. All patients were admitted to the hospital with the aim of improving their control over hyperglycemia and management of the patients’ lifestyles, because they exhibited difficulty in diabetes management, including diet and exercise. As inclusion criteria, all 260 patients with T2D hospitalized for treatment of T2D were included. All hospitalized patients underwent a medical interview and examinations on admission to confirm they were free from autoimmune disease, infection, or other acute condition, such as ongoing treatment for malignancies, and not currently using steroids, beta-blockers, or supplements. As a result of such assessments, 32 patients were excluded from the study. Participants younger than 30 years of age (n=8) and older than 80 (n=13) were excluded to manage age and generational disparities. Also, excluded were participants who experienced a shorter hospitalization than seven days (n=14). At the beginning of hospitalization, height and bodyweight were measured with all participants in the standing position. CVRR data in 10 patients were missing due to irregular pulse during examination. Vibratory sensation data and ATR in 28 and four patients, respectively, were missing for neurologic or orthopedic reasons. For each participant, body mass index (BMI) was calculated as bodyweight (kg) divided by the square of standing height (m) on admission and at discharge. Urine and blood samples were taken the day following admission after an overnight fast from all participants. HbA1c was measured using the HPLC method and glycoalbumin (GA) with an enzymatic method. Diabetic microangiopathy was assessed in all participants as follows: nephropathy was categorized from normal to dialysis, in accordance with the classification of diabetic nephropathy 2014,12 based on eGFR status and albuminuria; retinopathy was diagnosed by experienced ophthalmologists;13 and neuropathy was diagnosed by the physician in charge based on abbreviated criteria by the Diabetic Neuropathy Study Group in Japan.14 During hospitalization, the bodyweight of all study participants was measured each morning and the participants were prohibited from snacking between three mealtimes, and caloric intake from meals was calculated15 and managed by the physicians in charge based on each of the participants ideal bodyweight. All medications were selected and administered by the physician, together with the diabetes health-care team, based on a patient-centered approach considering the best and latest evidence in terms of benefits, risks, preferences, patient values, and context in time, not only target HbA1c or glucose levels. This study protocol was approved by the hospital ethics committee, and information on the study was provided to the public via the internet, instead of obtaining informed consent from each patient individually (No. 3115-1). Patient charts were also handled properly, and data were kept confidential and anonymous, in accordance with the Declaration of Helsinki.
Measurement of Diabetic Neuropathy Severity
After the participants had rested in the supine position for at least 10 min, a standard 12-lead ECG was measured (CardiMax8 FCP-8800; Fukuda Denshi, Tokyo, Japan). R-R intervals were counted for 200 beats, and CVRR was calculated by dividing the standard deviations (SD) by the means (M): CV (%) = (SD/M) x 100. During a period of rest breathing, the participants were instructed to breathe naturally. During deep breathing, they were instructed to breathe deeply, at a rate of six times per minute. In this study, CVRR was employed during this deep-breathing phase, because the deep-breathing load was estimated to stimulate cardiac vagal tone.
Vibratory sensation was assessed using a 128-Hz tuning fork at the medial malleolus,14,16,17 as follows: The physician stroked the end of a 128-Hz tuning fork hard enough that both sides touched and immediately placed the vibrating tuning fork firmly on the medial malleolus. The patient was instructed to inform the examiner, the exact moment when he or she felt the vibration stop. The examiner recorded the seconds during which the patient recognized the vibration. Before the examinations, the physician applied the vibrating tuning fork to the patient’s wrist, to confirm that the patient could recognize any vibration in subsequent testing. ATR was examined with the patient in a kneeling position and diagnosed as “normal,” “decreased,” or “absent.” The vibratory sensation and ATR were assessed by certified diabetes educators.
Statistical Analysis
The data are expressed as mean and standard deviation. Continuous variables at baseline were compared using age- and gender-adjusted analysis of covariance (ANCOVA) for comparisons between categories. Since HbA1c, BMI, and vibration data were not distributed normally, analysis was conducted after logarithmic transformation. To test the potency of hospitalization on weight loss, the percentage of decrease in bodyweight based on bodyweight at admission and each morning ((bodyweight in the morning-bodyweight at admission)/bodyweight at admission) was calculated for all participants, with successful weight loss designated for cases in which bodyweight declined at least 3% during hospitalization.5,6 This category was designated the dependent variable (1, effective weight loss of at least 3%; 0, ineffective weight loss of less than 3%). To elucidate the significance of CVRR, vibration test results, and categories of ATR as predictors of weight-loss effectiveness, the first two data were divided into tertile based on subject number (<2.8, 2.8–4.4, and >4.4% in CVRR; <9, 9–11, and >11 s in vibration test), in addition to the numerical concentrations or categories themselves used as continuous variables. Numerical and tertile-specific hazard ratios were estimated using a Cox proportional hazards model. Participant numbers were 63, 58, and 62, respectively, for the CVRR category, and 55, 55, and 55, respectively, for the vibration category. To confirm the impact of the three examinations at admission on the extent of weight loss during hospitalization, a Cox proportional hazards model was used, after adjustment was made for the confounders age, gender, duration of diabetes, medication of sodium-glucose cotransporter 2 (SGLT2) inhibitors or glucagon-like peptide-1 (GLP-1) analogues, reduced caloric intake during hospitalization, and HbA1c and BMI on admission. No missing data concerning these confounders in this study were found. Statistical analyses were performed using JMP software (version 13.2 for Windows, SAS Institute).
Results
Clinical Characteristics of All Study Participants
Mean age of all participants was 60.4±12.9 years. Duration of T2D at admission and hospitalization period were 12.0±9.5 years and 12.3±2.7 days, respectively. Mean HbA1c, CVRR, vibration test, and ATR (normal/decreased/absent) were 9.7±2.1%, 3.9±2.0%, 9.3±3.8 s, and 112/14/63, respectively. Mean weight loss during hospitalization was 3.6±3.5%. BMI declined from 26.9±6.2 kg/m2 to 26.0±5.9 kg/m2. GA decreased from 24.5±7.9% to 21.0±5.4%. The clinical characteristics of all participants at baseline are indicated in Table 1.
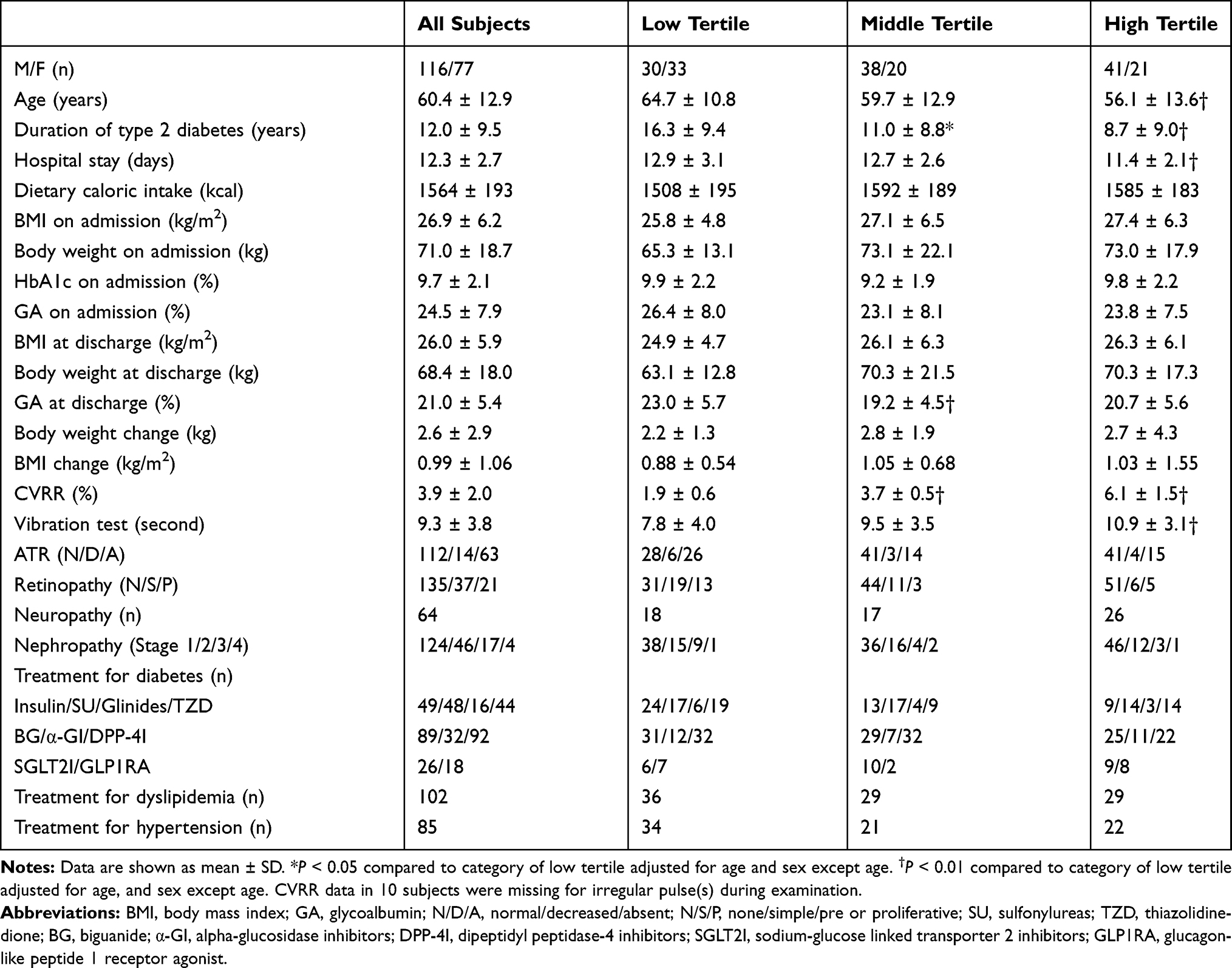 |
Table 1 Clinical Characteristics of Study Subjects According to CVRR Category |
Impact of CVRR, Vibration Test, and ATR on Effective Weight Loss During Hospitalization
A Cox proportional hazards model was used in analysis based on CVRR, after adjustment was made for the previously indicated confounders, with the hazard ratio for successful weight loss during hospitalization 1.17 (95% CI 1.07–1.28, P=0.0006). Also, using a Cox proportional hazards model in analysis including the three categories based on CVRR, after adjustment was made for the previously mentioned confounders, the hazard ratios by increasing tertile of CVRR were 1.0, 1.79 (1.11–2.88, P=0.018), and 2.17 (1.29–3.62, P=0.003), respectively (P=0.003 for trend) (Figure 1A).
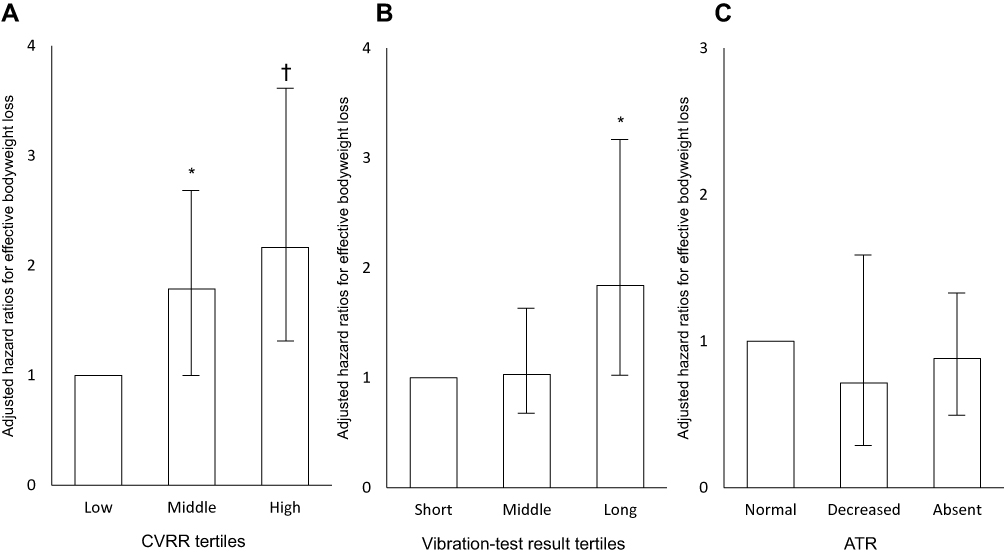 |
Figure 1 Adjusted hazard ratios for effective bodyweight loss among patients with type 2 diabetes. Notes: (A) The participants were divided into tertiles by CVRR on admission. *P<0.05 and †P<0.01 compared to the low tertile. (B) The participants were divided into tertiles by vibration test results on admission. *P<0.05 compared to the low tertile. (C) The participants were divided into three categories “normal,” “decreased,” and “absent,” by ATR on admission. |
The same model was used for vibration test results, after adjustment was made for the same confounders, with the hazard ratio for successful weight loss during hospitalization being 1.93 (1.01–3.68, P=0.045). The same model also was used for the three categories based on the vibration test, after adjustment was made for the same confounders. As a result, the hazard ratios by increasing tertile of vibration tests were 1.0, 1.03 (0.61–1.71, P=0.92), and 1.84 (1.10–3.08, P=0.02), respectively (P=0.02 for trend) (Figure 1B).
The same model was used for the three categories of ATR, after adjustment was made for the same confounders. As a result, the hazard ratios by worsening ATR were 1.0, 0.72 (0.33–1.54, P=0.39), and 0.88 (0.58–1.34, P=0.56), respectively (Figure 1C).
Comparisons of Clinical Characteristics Among the Study Participants Divided into Tertiles by CVRR
As described above, because a strong association between tertiles of CVRR, as well as of vibration tests and weight loss, was observed, the study participants were divided into tertiles of CVRR. The clinical characteristics of participants in each tertile are indicated in Table 1. Compared with the patients in the low tertile, the patients in the high tertile were significantly younger, after adjustment was made for sex. In addition, duration of T2D in the middle and high tertiles and hospital stay in the high tertile were significantly shorter compared with the low tertile, after adjustment was made for age and sex. On the other hand, among the three categories, no differences were observed in BMI, bodyweight, HbA1c, and GA on admission and at discharge, or in dietary caloric intake after adjustment was made for sex and age.
Discussion
In this retrospective observational study, results of CVRR and the vibration test were significantly associated with bodyweight change by strict caloric restriction among Japanese patients with T2D. To the best of our knowledge, this is the first study to investigate the association between diabetic neuropathy and bodyweight change during hospitalization under strict caloric restriction. These results suggest that severity of diabetic neuropathy lessens the effectiveness of diabetic treatment such as caloric restriction especially among overweight patients with T2D.
The main hypothesis of this study was that diabetic autonomic neuropathy among patients with T2D would induce insufficient metabolic regulation, resulting in the blocking of successful weight loss under strict caloric restriction during hospitalization. The results of this study might support this hypothesis and indicate the possibility that diabetic neuropathy directly or indirectly affects bodyweight.
Although the mechanisms responsible for the association are unclear, several hypotheses can be proposed. Autonomic nerves have recently been recognized as a key constituent of the endogenous system for maintaining energy homeostasis.18 Several studies investigated the importance of neurological pathways in medication for management of diabetes. For example, it was reported that duodenal GLP-1 receptor–protein kinase A signaling and a neuron-mediated gut–brain–liver pathway were required for metformin to lower hepatic glucose production.19 In addition, it was shown that GLP-1 in the portal vein evoked a strong neuron-mediated insulinotropic effect, suggesting a neuro-incretin effect in a rat model.20 Again, in a rat model, food-intake suppression after peripheral injection of exendin-4 and liraglutide was shown to be mediated by activation of GLP-1 receptor expressed on vagal afferents.21 The effect of SGLT2 inhibition on bodyweight is also reported to be mediated via the liver-brain-adipose neurocircuitry in a mouse model.22 Accordingly, the effect of several medications for T2D could be negatively modified by autonomic nerve damage such as in the vagal nerve. More directly, the vagal nerve stimulation system, comprising a flexible and biocompatible nanogenerator on the surface of the stomach and generating biphasic electric pulses in response to peristalsis of the stomach, was reported to reduce food intake and achieve weight management by stimulating vagal afferent fibers.23 Including these findings, our results suggest that diabetic autonomic neuropathy affects the selection of medical treatment for T2D including bodyweight management.
Clinical characteristics of patients with high CVRR in this study included a comparatively young age with a short duration since T2D onset (Table 1). Subjects in this study were between the ages of 30 and 80, with age adjusted statistically, because CVRR results are known to be influenced by age. However, younger patients could measure differently vis-à-vis environmental factors because of such variation as high exercise tolerance. Other undetermined factors related to age or generation besides CVRR might have influenced the impact of bodyweight. Accordingly, further study is needed to generalize these results and draw definitive conclusions regarding the impact of diabetic neuropathy on bodyweight change.
Results of the vibration test, an examination of somatic sensory function, were also associated with bodyweight reduction in our study. Considering progression patterns and natural history of diabetic neuropathy, this result was expected. In general, diabetic polyneuropathy progresses from somatic sensory nerve dysfunction, represented by vibration test results, to autonomic nerve dysfunction, represented by CVRR test results, and then to somatic motor nerve dysfunction.14,24 Accordingly, the worsening of CVRR test results has the potential to be accompanied by increased severity in vibration test results. This study’s findings showed that diabetic autonomic neuropathy generally coexisted with peripheral neuropathy. As a result, it was reasonable that the hazard ratios of tertiles for both the CVRR and vibration tests were comparable, as indicated in Figure 1A and B. Contrary to the vibration test, ATR was found to not be associated with bodyweight reduction, although ATR was used mainly for sensory nerve assessment. One reason for this negative result could have been the result of the small number of study participants. In addition, patient distribution was skewed: normal, diminished, and absent patient numbers were 112, 14, and 63, respectively. The other and most plausible reason might have been that this was a qualitative rather than a quantitative examination. Furthermore, presumably the most plausible reason might only explain the limitation of the three existing examinations for evaluation of somatic and sensory neuropathy with high sensitivity and specificity.
The present study has several limitations, other than age as described above. First, it was a retrospective, observational, and single-center study with a limited study population. Second, the observation period was also limited. Third, CVRR is an examination used mainly to assess parasympathetic nerve function, especially with regard to the cardiovascular autonomic nerve system, not sympathetic nerve function or the gastrointestinal autonomic nerve system, the latter of which would directly affect parasympathetic nerve function. Furthermore, the three examinations for neuropathy were conducted only once, and neuropathy symptoms were not considered. In addition, for the treatment of diabetes, the medications that would affect bodyweight change during hospitalization, except SGLT2 inhibitors and GLP-1 analogues, were not taken into consideration, because every treatment was individualized and patient-centered, not standardized. Lastly, evaluation of central obesity, smoking status or activity of daily lives, namely habitual and comorbid factors, were not assessed in the study.
Conclusion
This study found that T2D patients with diabetic neuropathy had difficulty in effectively reducing bodyweight under strict caloric restriction during hospitalization. These results suggest that, in patients with T2D, maintaining good glycemic control to prevent diabetic neuropathy is a critical part of bodyweight management.
Acknowledgments
We thank all staff members in our group for managing the study.
Disclosure
Hideaki Kaneto has received honoraria for lectures and received scholarship grants from Sanofi, Novo Nordisk, Eli Lilly, Boehringer Ingelheim, Taisho Toyama Pharma, MSD, Takeda, Ono Pharma, Daiichi Sankyo, Sumitomo Dainippon Pharma, Mitsubishi Tanabe Pharma, Kissei Pharma, Astellas, Novartis, Kowa, Chugai, the Japan Foundation for Applied Enzymology, and A2 Healthcare. Kohei Kaku has been an advisor to, received honoraria for lectures from, and received scholarship grants from Novo Nordisk Pharma, Sanwa Kagaku Kenkyusho, Takeda, Taisho Pharmaceutical Co., MSD, Taisho Toyama Pharma., Astellas, Kissei Pharma., Mitsubishi Tanabe Pharma. Co., Ono Pharma. Co., Sumitomo Dainippon Pharma, Novartis, Mitsubishi Tanabe Pharma, AstraZeneca, Nippon Boehringer Ingelheim Co., Fujifilm Pharma Co., and Sanofi. Masashi Shimoda and Shuhei Nakanishi have received honoraria for lectures from AstraZeneca and Sanofi, respectively. Dr Shuhei Nakanishi also reports personal fees from Kohei Kaku, Hideaki Kaneto, and Masashi Shimoda, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Cho NH, Shaw JE, Karuranga S, et al. IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diab Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
2. Nanditha A, Ma RC, Ramachandran A, et al. Diabetes in Asia and the pacific: implications for the global epidemic. Diab Care. 2016;39(3):472–485. doi:10.2337/dc15-1536
3. Hu FB. Globalization of diabetes: the role of diet, lifestyle, and genes. Diab Care. 2011;34(6):1249–1257. doi:10.2337/dc11-0442
4. Lean ME, Leslie WS, Barnes AC, et al. Primary care-led weight management for remission of type 2 diabetes (DIRECT): an open-label, cluster-randomised trial. Lancet. 2018;391(10):541–551. doi:10.1016/S0140-6736(17)33102-1
5. American College of Cardiology/American Heart Association Task Force on Practice Guidelines; Obesity Society. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society. Circulation. 2014;129(Suppl2):S102–S138. 10.1161/01.cir.0000437739.71477.ee.
6. Muramoto A, Matsushita M, Kato A, et al. Three percent weight reduction is the minimum requirement to improve health hazards in obese and overweight people in Japan. Obes Res Clin Pract. 2014;8(5):e466–e475. doi:10.1016/j.orcp.2013.10.003
7. Asakawa A, Inui A, Yuzuriha H, et al. Characterization of the effects of pancreatic polypeptide in the regulation of energy balance. Gastroenterology. 2003;124(5):1325–1336. doi:10.1016/S0016-5085(03)00216-6
8. Koda S, Date Y, Murakami N, et al. The role of the vagal nerve in peripheral PYY3–36-induced feeding reduction in rats. Endocrinology. 2005;146(5):2369–2375. doi:10.1210/en.2004-1266
9. Izumida Y, Yahagi N, Takeuchi Y, et al. Glycogen shortage during fasting triggers liver-brain-adipose neurocircuitry to facilitate fat utilization. Nat Commun. 2013;4:2316. doi:10.1038/ncomms3316
10. Cork SC. The role of the vagus nerve in appetite control: implications for the pathogenesis of obesity. J Neuroendocrinol. 2018;30(11):e12643. doi:10.1111/jne.12643
11. Rothschild AH, Weinberg CR, Halter JB, Porte D, Pfeifer MA. Sensitivity of R-R variation and valsalva ratio in assessment of cardiovascular diabetic autonomic neuropathy. Diab Care. 1987;10(6):735–741. doi:10.2337/diacare.10.6.735
12. Haneda M, Utsunomiya K, Koya D, et al. Classification of diabetic nephropathy 2014. J Japan Diab Soc. 2014;57(7):529–534.
13. Davis MD. Vitreous contraction in proliferative diabetic retinopathy. Arch Ophthalmol. 1965;74(6):741–751. doi:10.1001/archopht.1965.00970040743003
14. Yasuda H, Sanada M, Kitada K, et al. Rationale and usefulness of newly devised abbreviated diagnostic criteria and staging for diabetic polyneuropathy. Diab Res Clin Pract. 2007;77(Suppl 1):S178–S183. doi:10.1016/j.diabres.2007.01.053
15. The Japan Diabetes Society. Diet therapy. In: Practice Guideline for the Treatment for Diabetes in Japan. Nankodo:Tokyo, Japan. 2016.
16. Jin Y, Kanamori A, Ito S, et al. Cross-sectional survey of diabetic neuropathy in Kanagawa and clinical significance of a touch test using tissue paper. J Diab Investig. 2012;3(3):252–258. doi:10.1111/j.2040-1124.2011.00174.x
17. Takahara M, Fujiwara Y, Sakamoto F, et al. Assessment of vibratory sensation with a tuning fork at different sites in Japanese patients with diabetes mellitus. J Diab Investig. 2014;5(1):90–93. doi:10.1111/jdi.12126
18. Yamada T, Oka Y, Katagiri H. Inter-organ metabolic communication involved in energy homeostasis: potential therapeutic targets for obesity and metabolic syndrome. Pharmacol Ther. 2008;117(1):188–198. doi:10.1016/j.pharmthera.2007.09.006
19. Duca FA, Côté CD, Rasmussen BA, et al. Metformin activates a duodenal Ampk-dependent pathway to lower hepatic glucose production in rats. Nat Med. 2015;21(5):506–511. doi:10.1038/nm.3787
20. Nishizawa M, Nakabayashi H, Uehara K, et al. Intraportal GLP-1 stimulates insulin secretion predominantly through the hepatoportal-pancreatic vagal reflex pathways. Am J Physiol Endocrinol Metab. 2013;305(3):E376–E387. doi:10.1152/ajpendo.00565.2012
21. Kanoski SE, Fortin SM, Arnold M, Grill HJ, Hayes MR. Peripheral and central GLP-1 receptor populations mediate the anorectic effects of peripherally administered GLP-1 receptor agonists, liraglutide and exendin-4. Endocrinology. 2011;152(8):3103–3112. doi:10.1210/en.2011-0174
22. Sawada Y, Izumida Y, Takeuchi Y, et al. Effect of sodium-glucose cotransporter 2 (SGLT2) inhibition on weight loss is partly mediated by liver-brain-adipose neurocircuitry. Biochem Biophys Res Commun. 2017;493(1):40–45. doi:10.1016/j.bbrc.2017.09.081
23. Yao G, Kang L, Li J, et al. Effective weight control via an implanted self-powered vagus nerve stimulation device. Nat Commun. 2018;9(1):5349. doi:10.1038/s41467-018-07764-z
24. Ogawa K, Sasaki H, Yamasaki H, et al. Peripheral nerve functions may deteriorate parallel to the progression of microangiopathy in diabetic patients. Nutr Metab Cardiovasc Dis. 2006;16(5):313–321. doi:10.1016/j.numecd.2005.06.003
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.