Back to Journals » Clinical Epidemiology » Volume 15
Association Between Serum Uric Acid and Non-Alcoholic Fatty Liver Disease: An Updated Systematic Review and Meta-Analysis
Authors Sun Q, Zhang T, Manji L ![]() , Liu Y, Chang Q, Zhao Y, Ding Y, Xia Y
, Liu Y, Chang Q, Zhao Y, Ding Y, Xia Y ![]()
Received 16 January 2023
Accepted for publication 24 May 2023
Published 5 June 2023 Volume 2023:15 Pages 683—693
DOI https://doi.org/10.2147/CLEP.S403314
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Vera Ehrenstein
Qianjia Sun,1,2,* Tingjing Zhang,3,* Laeeqa Manji,4 Yashu Liu,1,2 Qing Chang,1,2 Yuhong Zhao,1,2 Yang Ding,5,6 Yang Xia1,2
1Department of Clinical Epidemiology, Shengjing Hospital of China Medical University, China Medical University, Shenyang, People’s Republic of China; 2Key Laboratory of Precision Medical Research on Major Chronic Disease, Shenyang, People’s Republic of China; 3School of Public Health, Wannan Medical College, Wuhu, People’s Republic of China; 4International Educational School, China Medical University, Shenyang, People’s Republic of China; 5Department of Infectious Diseases, Shengjing Hospital of China Medical University, China Medical University, Shenyang, People’s Republic of China; 6Diagnosis and Treatment Centre for Liver Diseases of Liaoning Province, Shenyang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yang Xia, Department of Clinical Epidemiology, Shengjing Hospital of China Medical University, No. 36, San Hao Street, Shenyang, Liaoning, 110004, People’s Republic of China, Tel +86 24-96615-13650, Email [email protected]; [email protected] Yang Ding, Department of Infectious Diseases, Shengjing Hospital of China Medical University, No. 36, San Hao Street, Shenyang, Liaoning, 110004, People’s Republic of China, Tel +86 24-96615-62211, Email [email protected]
Objective: Recent epidemiological evidence shows that there is an association between serum uric acid (SUA) levels and nonalcoholic fatty liver disease (NAFLD). The purpose of this meta-analysis is to summarize all available evidence and assess the associations between SUA levels and NAFLD.
Methods: Using two databases, Web of Science and PubMed, observational studies were applied from the establishment of the databases to June 2022. We used a random effect model to construct the pooled odds ratio (OR) and 95% confidence interval (CI) to appraise the association between SUA levels and NAFLD. The Begg’s test was conducted to appraise publication bias.
Results: A total of 50 studies were included, involving 2,079,710 participants (719,013 NAFLD patients). The prevalence and incidence rates (95% CIs) of NAFLD in the patients with hyperuricemia were 65% (57– 73%) and 31% (20– 41%), respectively. Compared to participants with lower levels of SUA, the pooled OR (95% CI) of NAFLD in those with higher levels of SUA was 1.88 (95% CI: 1.76– 2.00). In the subgroup analyses, we found that SUA levels were positively associated with NAFLD in all subgroups, according to study design, study quality, sample size, sex, comparison, age, or country.
Conclusion: This meta-analysis shows that increased SUA levels are positively associated with NAFLD. The results suggested that reducing SUA levels can be a potential strategy for the prevention of NAFLD.
Registration Number: PROSPERO-CRD42022358431.
Keywords: serum uric acid, nonalcoholic fatty liver disease, meta-analysis, updated
Introduction
One of the most prevalent chronic liver illnesses globally is non-alcoholic fatty liver disease (NAFLD). In 2020, NAFLD evolved into metabolic dysfunction-associated fatty liver disease (MAFLD).1 Although emerging studies have explored the associations between MAFLD and health outcomes over the past two years, there have been limited studies that investigate the associations between SUA and MAFLD. Additionally, there are differences in the definitions of NAFLD and MAFLD. MAFLD is defined as the evidence of overweight/obesity, the existence of type 2 diabetes or metabolic disorder on the basis of fatty liver.1 NAFLD refers to liver steatosis>5% found by imaging or histology after excluding significant recent drinking and other liver diseases with known causes.2 Therefore, based on the current available data, we summarized the associations between SUA and NAFLD in this meta-analysis. In 2018, the prevalence of NAFLD was about 25%.3 NAFLD may develop into a series of advanced liver diseases such as fibrosis, cirrhosis and liver cancer.4 Moreover, NAFLD is associated with other diseases, such as diabetes, hypertension, and cerebrovascular diseases.5,6 Considering the disease burden caused by NAFLD and its high prevalence, it is necessary to determine its risk factors.
The primary by-product of purine metabolism in the body is serum uric acid (SUA). Previous articles found that the increase in SUA levels acts an independent risk factor for NAFLD and may be utilized as an indicator to assess the NAFLD risk,7–10 and that the prevalence rates of NAFLD increases with an increase in the SUA concentration.11,12 According to previous studies, a raised SUA concentration was independently associated with the existence of NAFLD even when it was within the normal range.13–15 However, some other articles suggested that SUA levels are not associated with NAFLD risk.12,16,17 Previous meta-analyses revealed a positive association between hyperuricemia and higher SUA levels, and NAFLD.18–23 Based on these evidences, we believe that high SUA is a risk factor for NAFLD. The most recently meta-analysis was published in 2017, which included 11 studies and 92,725 participants.18 In the recent years, newer studies have been published. Nonetheless, the significant heterogeneity of findings was not explored in previous meta-analyses. Despite the relative measurements (odds ratio [ORs], risk ratio [RRs], and hazard ratio [HRs]) of the associations between SUA levels and NAFLD, no previous meta-analyses had assessed and measured the prevalence and incidence rates of NAFLD in people with hyperuricemia, which is more intuitive as absolute measurements. We thus conducted this updated meta-analysis to better understand the association between SUA levels and NAFLD and summarize the pooled prevalence and incidence rates of NAFLD in patients with hyperuricemia.
Method
Search Strategy
We identified studies that were published in the English language by reviewing the PubMed and Web of Science databases. Studies that qualified for this analysis were selected on June 2022 using the following keywords: “serum uric acid”, “hyperuricemia”, “NAFLD”, “non-alcoholic steatohepatitis”, or “hepatic steatosis” (Table S1). First, studies that appeared to be irrelevant were excluded after reading the titles and abstracts of the potential papers. Complete texts of relevant articles were retrieved, and their admissibility for inclusion was evaluated by reading the whole texts. For the purpose of obtaining the most comprehensive collection of published studies, we also searched for the chosen literature in other relevant meta-analyses. The Preferred Reporting Items for Systematic Review and Meta-analyses declaration was followed in the study selection procedure.24 The protocol of this meta-analysis has been registered in PROSPERO (CRD42022358431).
Eligibility Criteria
The following are the inclusion requirements for the chosen studies: (1) Reported an observational study; (2) Patients with a distinct NAFLD diagnosis; (3) Reporting either RRs, HRs, or ORs with 95% CIs for NAFLD (or prevalence/incidence rate of NAFLD); (4) age ≥18. The following studies were not included: (1) Those with repetitive articles or duplicate information; (2) Articles about animal experiments; (3) Subjects that were pregnant women or children (4) Conference reports, letters, or case reports. The participants included in estimating the pooled incidence rates of NAFLD in hyperuricemic population had no NAFLD at the beginning of follow-up.
Data Extraction and Quality Assessment
The following information was collected from the articles: the first author’s name; age; sex proportion; edition year; country of study; study design; duration of follow-up; number of participants and cases; diagnostic methods (NAFLD and hyperuricemia); OR (95% CI), HR (95% CI), or RR (95% CI). We used the Newcastle–Ottawa Scale (NOS) and the Agency for Healthcare Research and Quality (AHRQ) for quality evaluation.25,26 The evaluation of cohort and case-control studies used the NOS scale. The evaluation of the cross-sectional studies was performed using the AHRQ scale.
Statistical Analysis
We used the OR (95% CI) as the effect measure for pooling the associations between SUA levels and NAFLD. A random effects model was used to analyze the pooled OR if I2 > 50%, as well as the fix effects model. In estimating the pooled prevalence and incidence rates of NAFLD in the patients with hyperuricemia, a random effects model was used according to the degree of heterogeneity. Subgroup analyses were further performed according to sex, age, study quality, sample size, study design, comparison, and country. Meta-regression analysis was carried out to identify sources of heterogeneity. Possible factors include study design, study quality, sample size, country, age, and so on. We used sensitivity analysis to identify the impact of each study on the overall results. The Begg’s test was conducted to appraise publication bias. All statistical analyses were conducted using Stata version 17.0 software (Stata Corp., College Station, TX, United States). A two-sided P value < 0.05 was regarded as significantly.
Results
Study Selection
Figure 1 displays the study selection procedure. From the PubMed and Web of Science databases, 8234 premier studies were retrieved. We excluded 1139 articles that included duplicates and 6923 studies that did not achieve the inclusion requirements on the basis of reading the title and abstract screening. Through thorough reading of the texts, 50 articles7–12,14–16,27–67 conformed to the inclusion requirements and were included in the meta-analysis, which involved 2,079,710 participants (719,013 NAFLD patients). Of them, 50 studies with 54 estimates were included in the meta-analysis of the association between SUA levels and NAFLD, and 10 studies with 10 estimates were included in estimating the pooled prevalence and incidence rates of NAFLD in hyperuricemic population.
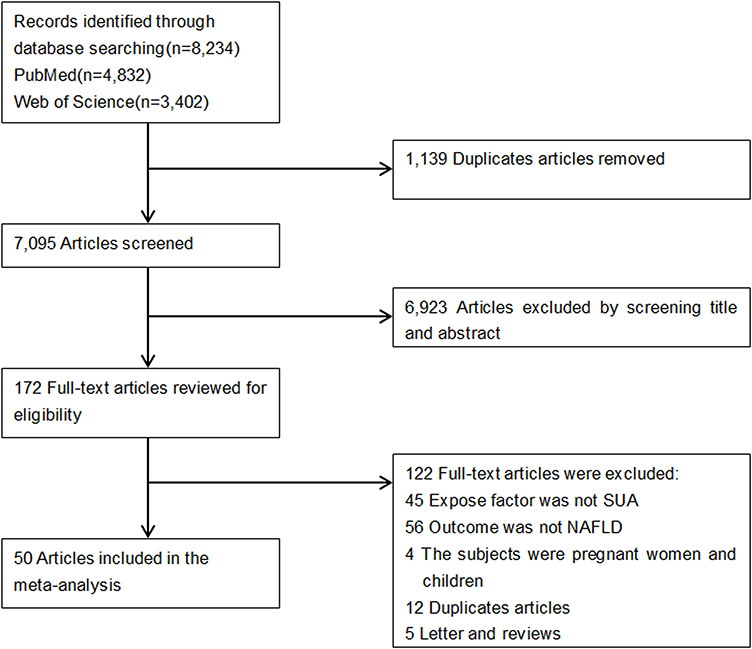 |
Figure 1 Flow chart of study selection in the meta-analysis. |
Study Characteristics
Table 1 summarizes the characteristics of the study. These studies were included in pooling the associations between NAFLD and SUA levels (detailed information is presented in Table S2). Among the included studies, there were 36 cross-sectional studies, 13 cohort studies, and 1 case-control study. Of them, 40 studies were from China, 6 studies were from Korea, 2 studies were from the USA, 1 study was from Japan, and 1 study was from Italy. Table S3 summarizes the characteristics of the studies included in the meta-analysis of the prevalence and incidence rates of NAFLD in hyperuricemic population. Among the included studies, there were 6 cross-sectional studies, and 4 cohort studies. Of them, 7 studies were from China, 1 study was from Korea, 1 study was from the USA, and 1 study was from Iran.
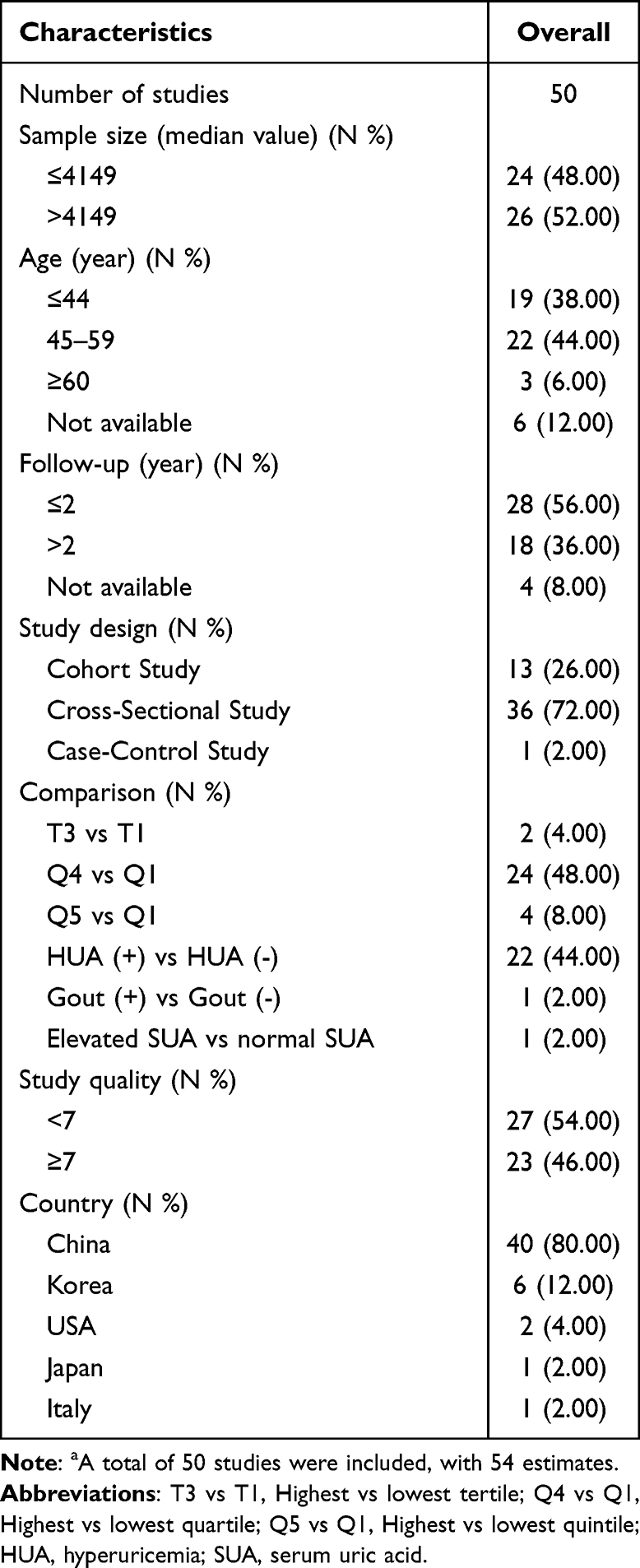 |
Table 1 Summary of the Characteristics of Included Studies (Association Between SUA Levels and NAFLD)a |
Tables S4 and S5 display the quality appraisal of the included studies according to the study designs. The mean point of cohort and case-control studies was 6.6 stars. The mean point of cross-sectional studies was 6.3 points. All studies were of medium- or high-quality.
Association Between SUA and NAFLD
Figure 2 shows the pooled OR (95% CI) of the association between SUA levels and NAFLD. The Forest plot showed that SUA was positively associated with NAFLD (OR: 1.88, 95% CI: 1.76–2.00). Table 2 shows the results of the subgroup analysis. All the studies were divided into three subgroups according to the types of study design. The ORs (95% CIs) in cross-sectional, cohort, and case-control studies were 1.91 (1.79–2.05), 1.73 (1.52–1.97), and 5.92 (3.39–10.33), respectively. We divided all the studies into five subgroups (China, Korea, USA, Japan, and Italy) according to the countries where the study was conducted. The ORs (95% CIs) in China, Korea, USA, Japan, and Italy were 1.96 (1.83–2.10), 1.57 (1.34–1.83), 1.46 (1.25–1.70), 2.00 (1.42–2.82), and 3.01 (1.40–6.48), respectively. Based on the average or median age of the study population, included studies were divided into three subgroups: young people (≤ 44 years), middle-aged people (45–59 years), or elderly people (≥ 60 years). The ORs (95% CIs) in young people, middle-aged people, and elderly people were 1.76 (1.55–2.00), 1.96 (1.77–2.17), and 3.42 (1.60–7.33), respectively. In the subgroup analysis according to sex, SUA levels was associated with NAFLD in both males and females, the ORs (95% CIs) were 1.76 (1.53–2.01) and 2.09 (1.77–2.47), respectively. All the studies were divided into two subgroups: ≤ 4149 participants (OR: 2.17, 95% CI: 1.91–2.47) or > 4149 participants (OR: 1.77, 95% CI: 1.64–1.91) based on the median sample size. The ORs (95% CIs) according to the classifications of SUA levels were as follows: Q4 vs Q1 1.95 (1.76–2.17), HUA (+) vs HUA (-) 1.73 (1.58–1.90), Q5 vs Q1 2.50 (1.57–3.99), T3 vs T1 2.26 (1.32–3.89), Gout (+) vs Gout (-) 1.42 (1.26–1.61), or elevated SUA vs normal SUA 2.12 (1.85–2.42). All studies were divided into two subgroups based on the quality score of the included literature: < 7 (OR: 1.97, 95% CI: 1.82–2.15) or ≥ 7 (OR: 1.79, 95% CI: 1.61–1.99). Sensitivity analysis showed that there was no significant change in the overall results after excluding each study in sequence. The Begg’s test suggested that there was no obvious publication bias (P = 0.068). The funnel plot is shown in Figure S1.
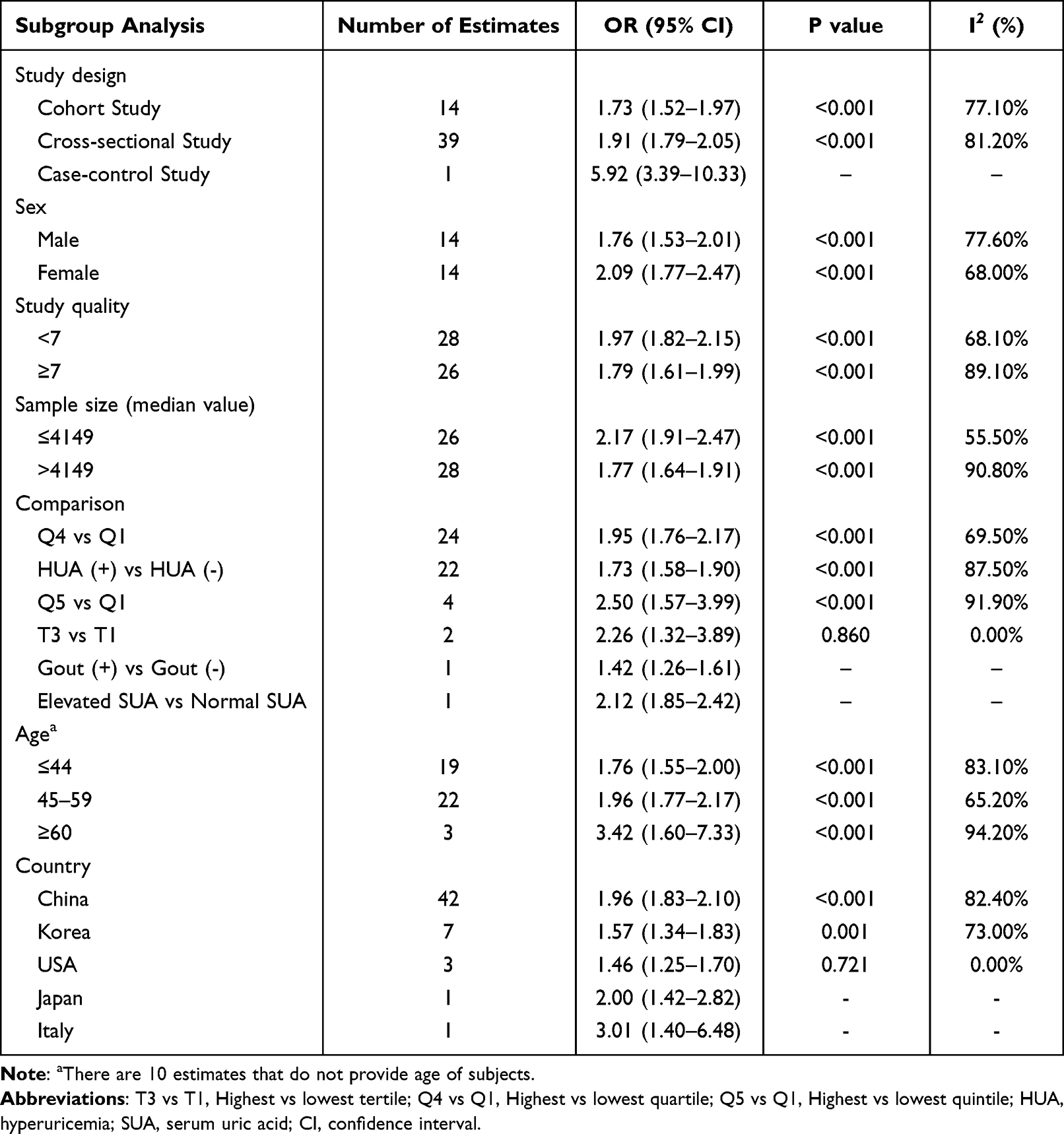 |
Table 2 Subgroup Analysis for Articles Included in the Meta-Analysis of Associations Between SUA Levels and NAFLD |
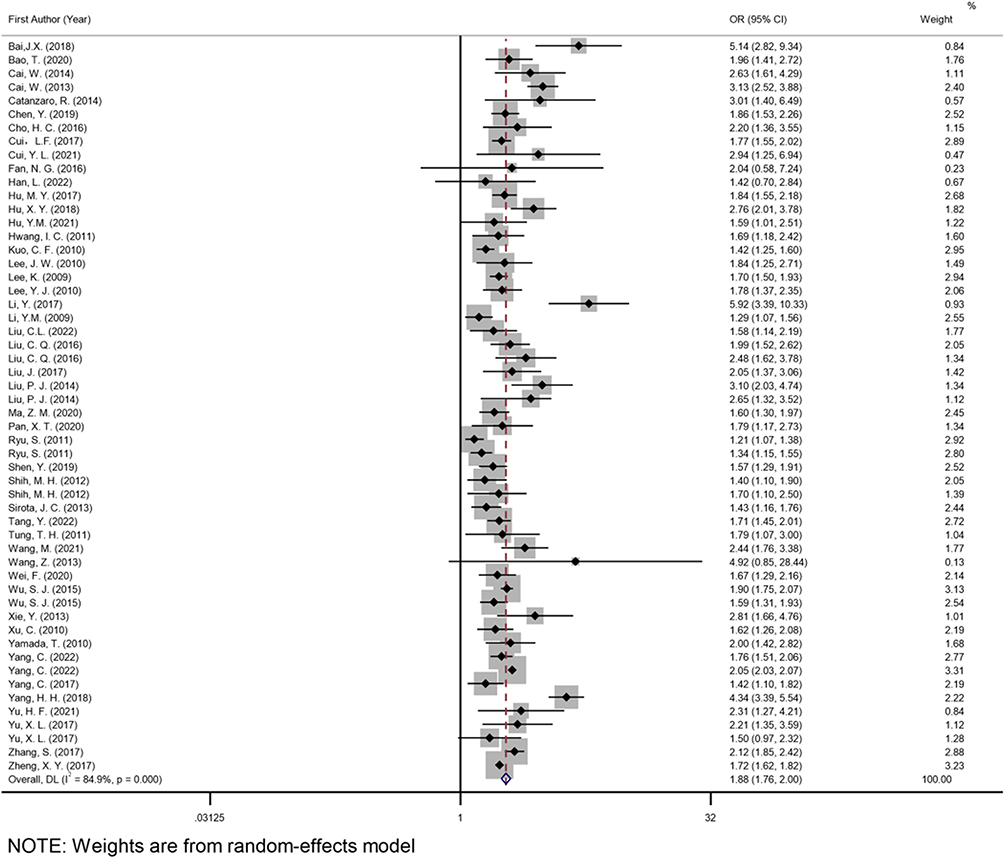 |
Figure 2 Overall pooled OR of association between SUA and NAFLD. |
Meta-Regression Analysis
Because of the obvious heterogeneity (I2 = 84.9%) in the meta-analysis, a meta-regression analysis was conducted to identify the possible sources of this heterogeneity (Table 3). It was found that the study design (P < 0.001, study quality (P < 0.001), sample size (P < 0.001), comparison (P = 0.004), country (P = 0.027) and age (P < 0.001) had significant effects on the meta-analysis, which could possibly be the source of heterogeneity.
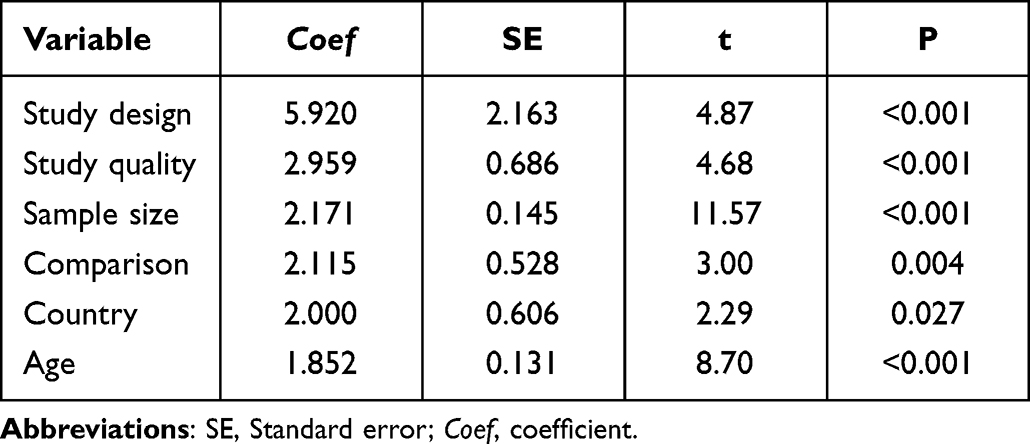 |
Table 3 Results of Meta-Regression Analysis |
Prevalence and Incidence Rates of NAFLD in the Patients with Hyperuricemia
As shown in Figure 3, the pooled overall prevalence of NAFLD in hyperuricemic population was estimated to be 65% (95% CI: 57–73%). As shown in Figure 3, the pooled overall incidence of NAFLD in patients with hyperuricemia was estimated to be 31% (95% CI: 20–41%).
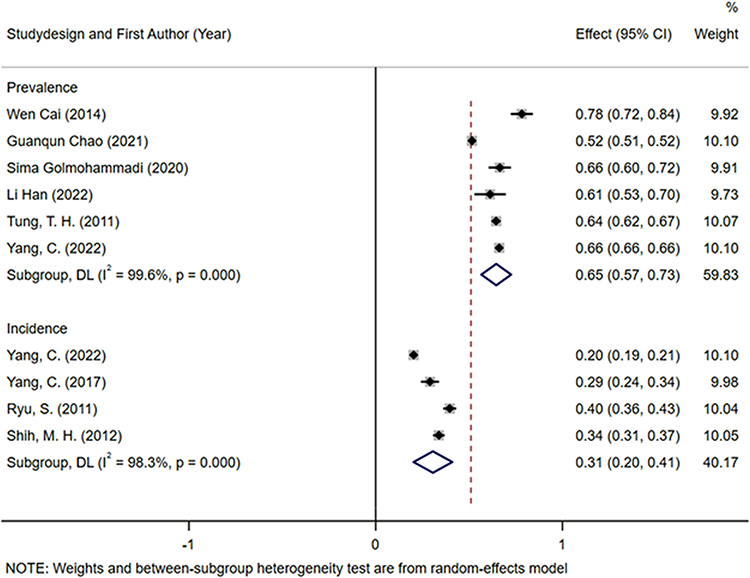 |
Figure 3 Prevalence and incidence rate of NAFLD in patients with hyperuricemia. |
Discussion
This meta-analysis included 50 studies, with 54 estimates, to identify the association between SUA levels and NAFLD. The study found that categorizing populations according to their SUA levels reveal that the group with the highest SUA level is about twice as likely to develop NAFLD compared to the group with the lowest SUA level. In all subgroups, SUA levels were positively associated with NAFLD. The prevalence and incidence rates of NAFLD in hyperuricemic population were 65% and 31%, respectively.
In the previous meta-analyses, two studies explored the associations between hyperuricemia and NAFLD;19,22 three studies explored the associations between levels of SUA and NAFLD;18,21,23 and one study combined the weighted mean difference of SUA concentration between patients with NAFLD and the control group.20 All previous meta-analyses showed a positive association between SUA levels and NAFLD. Our results were the same as those from the published meta-analyses, showing a positive association between SUA levels and NAFLD. However, previous meta-analyses18–23 have simply displayed the comparison between pooled ORs of the highest SUA level group and the lowest SUA level group. Subgroups were divided according to different SUA comparison methods. The high heterogeneity was also not explored in previous meta-analyses. Therefore, this meta-analysis was performed with the renewed data. Meta-regression was used to explore the high heterogeneity.
Subgroup analyses of study designs, sex, study quality, age, and country suggested consistent results to the main results. Our results indicated that the associations between SUA levels and NAFLD were statistically significant in both males and females. However, the pooled OR was higher in females than in males, which is also supported by previous meta-analyses.18,23 The cause of this result is unclear, but the difference in lifestyles and SUA production in the two sexes are considered as potential mechanisms.16,57 Moreover, influenced by estrogen, the SUA levels of men and women are different, which can possibly affect the relationship between SUA levels and NAFLD. Compared with middle-aged and young people, the combined ORs of NAFLD in relation to SUA levels is higher in the elderly. This suggests that the association between SUA and NAFLD may be stronger in the elderly. Subgroup analysis based on the study design revealed that the same positive association was found in all study designs. Nevertheless, the association seems to be even stronger in case-control studies, which could be due to the fact that only one case-control study was included.
The specific mechanism by which higher SUA levels increase the risk of NAFLD remains unclear, but there are several possible explanations. The increase of SUA levels can lead to insulin resistance in various ways,68,69 leading to an increase in cytotoxic substances and lipid peroxidation products in cells.70 SUA mainly promotes liver fat synthesis and accumulation through mitochondrial oxidative stress. Mitochondrial oxidative stress, by inhibiting the activity of aconitase in the tricarboxylic acid cycle, leads to a decrease in citric acid metabolism, which generates an increase in fat deposition and synthesis in liver cells.71 SUA can induce the expression of NLRP3 inflammatory complex, which is related to lipid accumulation in hepatocytes.72 However, the temporal order of the correlation between NAFLD and SUA has been controversial. One cohort study showed that NAFLD significantly increased the risk of hyperuricemia, and this result was not observed in other cohorts.73 This reverse causal pathway may be explained by a significant increase in the expression and activity of xanthine oxidase, a rate-limiting enzyme that catalyzes the production of uric acid, in NAFLD cells and mouse models, leading to a significant increase in serum uric acid levels.73
There are some advantages of this meta-analysis. Firstly, this meta-analysis updated new evidences that have emerged in recent years, with a larger sample size and more reliable results. Secondly, we performed subgroup analyses according to various classifications, especially the different comparison models. Finally, this meta-analysis assessed intuitive indicators, which are the prevalence and incidence rates of NAFLD in hyperuricemic population.
Some limitations also need to be noted. First, there is an obvious heterogeneity in this meta-analysis. Meta-regression analysis suggested that the study design, sample size, comparison, country, and age could be the sources of heterogeneity. Second, the criteria for SUA grouping were different for each included study. Third, a few included studies did not adjust confounding factors, like serum insulin, and metabolic syndrome. This will lead to biased estimation of the pooled ORs to some extent. Fourth, the inability to calculate incident density (person-years) stems from the fact that the vast majority of included articles fail to provide the necessary follow-up years.
In conclusion, these results indicate that there is a positive association between the increase of SUA levels and the presence of NAFLD. Moreover, the prevalence and incidence rates of NAFLD in hyperuricemic population were 65% and 31%, respectively.
Data Sharing Statement
All data generated or analysed during this study are included in this published article and its Supplementary Information File.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent
This paper did not involve patients enrolled by any of the authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (No. 81903302), the Young Elite Scientists Sponsorship Program by China Association for Science and Technology (grant number YESS20200151), the 345 Talent Project of Shengjing Hospital of China Medical University (grant number M0294), and the Scientific Research Project of Liaoning Province Education Department (grant number LJKMZ20221149 to Yang Xia).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Eslam M, Newsome PN, Sarin SK, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73(1):202–209. doi:10.1016/j.jhep.2020.03.039
2. Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American association for the study of liver diseases. Hepatology. 2018;67(1):328–357. doi:10.1002/hep.29367
3. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease—meta‐analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–84. doi:10.1002/hep.28431
4. Powell EE, Wong VW, Rinella M. Non-alcoholic fatty liver disease. Lancet. 2021;397(10290):2212–2224. doi:10.1016/S0140-6736(20)32511-3
5. Fan JG, Farrell GC. Epidemiology of non-alcoholic fatty liver disease in China. J Hepatol. 2009;50(1):204–210. doi:10.1016/j.jhep.2008.10.010
6. Miyake T, Kumagi T, Furukawa S, et al. Non-alcoholic fatty liver disease: factors associated with its presence and onset. J Gastroenterol Hepatol. 2013;28(s4):71–78. doi:10.1111/jgh.12251
7. Bai JX, Shu RM, Huang Y, Peng Z. 血尿酸与非酒精性脂肪性肝病发生风险相关性的随访队列研究 [Correlation between serum uric acid and risk of new-onset nonalcoholic fatty liver disease: a 5-year observational cohort study]. Zhonghua Gan Zang Bing Za Zhi. 2018;26(4):271–275. Chinese. doi:10.3760/cma.j.issn.1007-3418.2018.04.008
8. Cai W, Wu X, Zhang B, et al. Serum uric acid levels and nonalcoholic fatty liver disease in Uyghur and Han ethnic groups in northwestern China. Arq Bras Endocrinol Metabol. 2013;57(8):617–622. doi:10.1590/S0004-27302013000800006
9. Hu Y, Li Q, Min R, Deng Y, Xu Y, Gao L. The association between serum uric acid and diabetic complications in patients with type 2 diabetes mellitus by gender: a cross-sectional study. PeerJ. 2021;9:e10691. doi:10.7717/peerj.10691
10. Li Y, Xu C, Yu C, Xu L, Miao M. Association of serum uric acid level with non-alcoholic fatty liver disease: a cross-sectional study. J Hepatol. 2009;50(5):1029–1034. doi:10.1016/j.jhep.2008.11.021
11. Bao T, Ying ZY, Gong L, et al. Association between serum uric acid and nonalcoholic fatty liver disease in nonobese postmenopausal women: a cross-sectional study. Sci Rep. 2020;10(1). doi:10.1038/s41598-020-66931-9
12. Han L, Zhang Y, Yue C, Huang Y, Wu Y, Chen J. Preliminary study on risk factors for morbidity of nonalcoholic fatty liver disease in high-income male population. J Healthc Eng. 2022;2022:9331284. doi:10.1155/2022/9331284
13. Chen YL, Li H, Li S, et al. Prevalence of and risk factors for metabolic associated fatty liver disease in an urban population in China: a cross-sectional comparative study. BMC Gastroenterol. 2021;21(1):212. doi:10.1186/s12876-021-01782-w
14. Liu P, Ma F, Lou H, Zhu Y, Chen Y. 绝经后女性正常血尿酸水平与非酒精性脂肪性肝病的相关性 [Relationship between normal serum uric acid levels and nonalcoholic fatty liver disease in postmenopausal women]. Zhonghua Gan Zang Bing Za Zhi. 2014;22(1):53–57. Chinese. doi:10.3760/cma.j.issn.1007-3418.2014.01.012
15. Liu PJ, Ma F, Lou HP, Zhu YN, Chen Y. Relationship between serum uric acid levels and hepatic steatosis in non-obese postmenopausal women. Climacteric. 2014;17(6):692–699. doi:10.3109/13697137.2014.926323
16. Fan NG, Zhang LJ, Xia ZH, Peng L, Wang YF, Peng YD. Sex-specific association between serum uric acid and nonalcoholic fatty liver disease in type 2 diabetic patients. J Diabetes Res. 2016;2016:1–6. doi:10.1155/2016/3805372
17. Wang ZL, Xu M, Hu ZG, Shrestha UK. Prevalence of nonalcoholic fatty liver disease and its metabolic risk factors in women of different ages and body mass index. Menopause. 2015;22(6):667–673. doi:10.1097/GME.0000000000000352
18. Darmawan G, Hamijoyo L, Hasan I. Association between serum uric acid and non-alcoholic fatty liver disease: a meta-analysis. Acta Med Indones. 2017;49(2):136–147.
19. Gong SL, Song JQ, Wang L, Zhang SQ, Wang YG. Hyperuricemia and risk of nonalcoholic fatty liver disease: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol. 2016;28(2):132–138. doi:10.1097/MEG.0000000000000507
20. Huang F, Liu AD, Fang HS, Geng XP. Serum uric acid levels in non-alcoholic steatosis patients: a meta-analysis. Asia Pac J Clin Nutr. 2017;26(2):334–342. doi:10.6133/apjcn.092016.04
21. Liu ZT, Que SP, Zhou L, Zheng SS. Dose-response relationship of serum uric acid with metabolic syndrome and non-alcoholic fatty liver disease incidence: a meta-analysis of prospective studies. Sci Rep. 2015;5:14325.
22. Wijarnpreecha K, Panjawatanan P, Lekuthai N, Thongprayoon C, Cheungpasitporn W, Ungprasert P. Hyperuricaemia and risk of nonalcoholic fatty liver disease: a meta-analysis. Liver Int. 2017;37(6):906–918. doi:10.1111/liv.13329
23. Zhou YJ, Wei FF, Fan Y. High serum uric acid and risk of nonalcoholic fatty liver disease: a systematic review and meta-analysis. Clin Biochem. 2016;49(7–8):636–642. doi:10.1016/j.clinbiochem.2015.12.010
24. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):1–11. doi:10.1186/s13643-021-01626-4
25. Hu J, Dong Y, Chen X, et al. Prevalence of suicide attempts among Chinese adolescents: a meta-analysis of cross-sectional studies. Compr Psychiatry. 2015;61:78–89. doi:10.1016/j.comppsych.2015.05.001
26. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–605. doi:10.1007/s10654-010-9491-z
27. Cai W, Song JM, Zhang B, Sun YP, Yao H, Zhang YX. The prevalence of nonalcoholic fatty liver disease and relationship with serum uric acid level in Uyghur population. TheScientificWorldJournal. 2014;2014:393628. doi:10.1155/2014/393628
28. Catanzaro R, Calabrese F, Palermo F, et al. The relationship between serum uric acid and non alcoholic fatty liver disease: a cross-sectional retrospective study. Dig Liver Dis. 2014;46:S114.
29. Chao G, Chen L. Study on the independent effect of thyroid hormone based on uric acid level on NAFLD. J Health Popul Nutr. 2021;40(1):21. doi:10.1186/s41043-021-00247-w
30. Chen Y, Huang Q, Ai P, et al. Association between serum uric acid and non-alcoholic fatty liver disease according to different menstrual status groups. Can J Gastroenterol Hepatol. 2019;2019:2763093. doi:10.1155/2019/2763093
31. Cho HC. Prevalence and factors associated with nonalcoholic fatty liver disease in a nonobese Korean population. Gut Liver. 2016;10(1):117–125. doi:10.5009/gnl14444
32. Cui L, Meng L, Wang G, et al. Prevalence and risk factors of hyperuricemia: results of the Kailuan cohort study. Mod Rheumatol. 2017;27(6):1066–1071. doi:10.1080/14397595.2017.1300117
33. Cui YL, Liu J, Shi HY, Hu WM, Song L, Zhao Q. Serum uric acid is positively associated with the prevalence of nonalcoholic fatty liver in non-obese type 2 diabetes patients in a Chinese population. J Diabetes Complications. 2021;35(5):107874. doi:10.1016/j.jdiacomp.2021.107874
34. Golmohammadi S, Tavasoli M, Asadi N. Prevalence and risk factors of hyperuricemia in patients with chronic kidney disease and non-alcoholic fatty liver. Clin Exp Gastroenterol. 2020;13:299–304. doi:10.2147/CEG.S253619
35. Hu MY, Liu JB, Zhou CH, Li XL. Analysis of the interaction effects among the risk factors for hyperuricaemia in adults: a cross-sectional survey in Guilin, China. Int J Clin Exp Med. 2017;10(6):9376–9386.
36. Hu XY, Li Y, Li LQ, et al. Risk factors and biomarkers of non-alcoholic fatty liver disease: an observational cross-sectional population survey. BMJ Open. 2018;8(4):e019974. doi:10.1136/bmjopen-2017-019974
37. Hwang IC, Suh SY, Suh AR, Ahn HY. The relationship between normal serum uric acid and nonalcoholic fatty liver disease. J Korean Med Sci. 2011;26(3):386–391. doi:10.3346/jkms.2011.26.3.386
38. Kuo CF, Yu KH, Luo SF, et al. Gout and risk of non-alcoholic fatty liver disease. Scand J Rheumatol. 2010;39(6):466–471. doi:10.3109/03009741003742797
39. Lee JW, Cho YK, Ryan MC, et al. Serum uric acid as a predictor for the development of nonalcoholic fatty liver disease in apparently healthy subjects: a 5-year retrospective cohort study. Gut Liver. 2010;4(3):378–383. doi:10.5009/gnl.2010.4.3.378
40. Lee K. Relationship between uric acid and hepatic steatosis among Koreans. Diabetes Metab. 2009;35(6):447–451. doi:10.1016/j.diabet.2009.04.011
41. Lee YJ, Lee HR, Lee JH, Shin YH, Shim JY. Association between serum uric acid and non-alcoholic fatty liver disease in Korean adults. Clin Chem Lab Med. 2010;48(2):175–180. doi:10.1515/CCLM.2010.037
42. Li Y, Song CL, Yang HH, et al. 苏州60岁及以上老年人群非酒精性肝脏脂肪变性状况及影响因素分析 [Study about the risk factors of non-alcoholic fatty liver disease among people aged over 60 years old in Suzhou]. Zhonghua yu fang yi xue za zhi. 2017;51(5):444–446. Chinese. doi:10.3760/cma.j.issn.0253-9624.2017.05.014
43. Liu C, Liu W, Zhang G, et al. Conjunctional relationship between serum uric acid and serum nickel with non-alcoholic fatty liver disease in men: a cross-sectional study. Int J Environ Res Public Health. 2022;19(11):6424.
44. Liu CQ, He CM, Chen N, et al. Serum uric acid is independently and linearly associated with risk of nonalcoholic fatty liver disease in obese Chinese adults. Sci Rep. 2016;6:38605.
45. Liu J, Xu CF, Ying LM, et al. Relationship of serum uric acid level with non-alcoholic fatty liver disease and its inflammation progression in non-obese adults. Hepatol Res. 2017;47(3):E104–E112. doi:10.1111/hepr.12734
46. Ma ZM, Zhang JB, Kang XP, et al. Hyperuricemia precedes non-alcoholic fatty liver disease with abdominal obesity moderating this unidirectional relationship: three longitudinal analyses. Atherosclerosis. 2020;311:44–51. doi:10.1016/j.atherosclerosis.2020.08.006
47. Pan XT, Xie XX, Peng HW, et al. Risk prediction for non-alcoholic fatty liver disease based on biochemical and dietary variables in a Chinese Han Population. Front Public Health. 2020;8. doi:10.3389/fpubh.2020.00220
48. Ryu S, Chang Y, Kim SG, Cho J, Guallar E. Serum uric acid levels predict incident nonalcoholic fatty liver disease in healthy Korean men. Metabolism. 2011;60(6):860–866. doi:10.1016/j.metabol.2010.08.005
49. Shen Y, Wang Y, Chang C, Li S, Li W, Ni B. Prevalence and risk factors associated with hyperuricemia among working population at high altitudes: a cross-sectional study in Western China. Clin Rheumatol. 2019;38(5):1375–1384. doi:10.1007/s10067-018-4391-9
50. Shih MH, Lazo M, Liu SH, Bonekamp S, Hernaez R, Clark JM. Association between serum uric acid and nonalcoholic fatty liver disease in the US population. J Formos Med Assoc. 2015;114(4):314–320. doi:10.1016/j.jfma.2012.11.014
51. Sirota JC, McFann K, Targher G, Johnson RJ, Chonchol M, Jalal DI. Elevated serum uric acid levels are associated with non-alcoholic fatty liver disease independently of metabolic syndrome features in the United States: liver ultrasound data from the national health and nutrition examination survey. Metabolism. 2013;62(3):392–399. doi:10.1016/j.metabol.2012.08.013
52. Tang Y, Xu Y, Liu P, et al. No evidence for a causal link between serum uric acid and nonalcoholic fatty liver disease from the dongfeng-tongji cohort study. Oxid Med Cell Longev. 2022;2022:6687626. doi:10.1155/2022/6687626
53. Tung TH, Chang TH, Chiu WH, et al. Clinical correlation of nonalcoholic fatty liver disease in a Chinese taxi drivers population in Taiwan: experience at a teaching hospital. BMC Res Notes. 2011;4:315. doi:10.1186/1756-0500-4-315
54. Wang M, Wang M, Zhang R, et al. A combined association of serum uric acid, alanine aminotransferase and waist circumference with non-alcoholic fatty liver disease: a community-based study. PeerJ. 2022;10:e13022. doi:10.7717/peerj.13022
55. Wang Z, Xu M, Peng J, et al. Prevalence and associated metabolic factors of fatty liver disease in the elderly. Exp Gerontol. 2013;48(8):705–709. doi:10.1016/j.exger.2013.05.059
56. Wei F, Li J, Chen C, et al. Higher serum uric acid level predicts non-alcoholic fatty liver disease: a 4-year prospective cohort study. Front Endocrinol. 2020;11:179. doi:10.3389/fendo.2020.00179
57. Wu SJ, Zhu GQ, Ye BZ, et al. Association between sex-specific serum uric acid and non-alcoholic fatty liver disease in Chinese adults: a large population-based study. Medicine. 2015;94(17):e802. doi:10.1097/MD.0000000000000802
58. Xie Y, Wang M, Zhang Y, et al. Serum uric acid and non-alcoholic fatty liver disease in non-diabetic Chinese men. PLoS One. 2013;8(7):e67152. doi:10.1371/journal.pone.0067152
59. Xu C, Yu C, Xu L, Miao M, Li Y, Ng IOL. High serum uric acid increases the risk for nonalcoholic fatty liver disease: a prospective observational study. PLoS One. 2010;5(7):e11578. doi:10.1371/journal.pone.0011578
60. Yamada T, Suzuki S, Fukatsu M, Wada T, Yoshida T, Joh T. Elevated serum uric acid is an independent risk factor for nonalcoholic fatty liver disease in Japanese undergoing a health checkup. Acta Gastroenterol Belg. 2010;73(1):12–17.
61. Yang C, He Q, Chen Z, et al. A bidirectional relationship between hyperuricemia and metabolic dysfunction-associated fatty liver disease. Front Endocrinol. 2022;13:821689. doi:10.3389/fendo.2022.821689
62. Yang C, Yang SJ, Xu WW, Zhang JH, Fu WG, Feng CH. Association between the hyperuricemia and nonalcoholic fatty liver disease risk in a Chinese population: a retrospective cohort study. PLoS One. 2017;12(5):e0177249.
63. Yang HH, Li DM, Song XC, et al. Joint associations of serum uric acid and ALT with NAFLD in elderly men and women: a Chinese cross-sectional study. J Transl Med. 2018;16. doi:10.1186/s12967-018-1657-6
64. Yu HF, Zhao L, Liu LJ, Li YF, Sun J, Liu YD. Relationship between serum uric acid level and nonalcoholic fatty liver disease in type 2 diabetes patients. Medicine. 2021;100(33):e26946. doi:10.1097/MD.0000000000026946
65. Yu XL, Shu L, Shen XM, Zheng XY, Zheng PF. Gender difference on the relationship between hyperuricemia and nonalcoholic fatty liver disease among Chinese an observational study. Medicine. 2017;96(39):e8164. doi:10.1097/MD.0000000000008164
66. Zhang S, Du T, Li M, Lu H, Lin X, Yu X. Combined effect of obesity and uric acid on nonalcoholic fatty liver disease and hypertriglyceridemia. Medicine. 2017;96(12):e6381. doi:10.1097/MD.0000000000006381
67. Zheng XY, Gong LL, Luo R, et al. Serum uric acid and non-alcoholic fatty liver disease in non-obesity Chinese adults. Lipids Health Dis. 2017;16(1). doi:10.1186/s12944-017-0531-5
68. Li C, Hsieh MC, Chang SJ. Metabolic syndrome, diabetes, and hyperuricemia. Curr Opin Rheumatol. 2013;25(2):210–216. doi:10.1097/BOR.0b013e32835d951e
69. Zhu Y, Hu Y, Huang T, et al. High uric acid directly inhibits insulin signalling and induces insulin resistance. Biochem Biophys Res Commun. 2014;447(4):707–714. doi:10.1016/j.bbrc.2014.04.080
70. Vacca M, Allison M, Griffin JL, Vidal-Puig A. Fatty acid and glucose sensors in hepatic lipid metabolism: implications in NAFLD. Semin Liver Dis. 2015;35(3):250–261. doi:10.1055/s-0035-1562945
71. Xu C. Hyperuricemia and nonalcoholic fatty liver disease: from bedside to bench and back. Hepatol Int. 2016;10(2):286–293. doi:10.1007/s12072-015-9682-5
72. Wan X, Xu C, Lin Y, et al. Uric acid regulates hepatic steatosis and insulin resistance through the NLRP3 inflammasome-dependent mechanism. J Hepatol. 2016;64(4):925–932. doi:10.1016/j.jhep.2015.11.022
73. Xu C, Wan X, Xu L, et al. Xanthine oxidase in non-alcoholic fatty liver disease and hyperuricemia: one stone hits two birds. J Hepatol. 2015;62(6):1412–1419. doi:10.1016/j.jhep.2015.01.019
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.