Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Association Between Serum Uric Acid and Lung Function in People with and without Chronic Obstructive Pulmonary Disease
Authors Yang H, Wang Z, Xiao S, Dai C ![]() , Wen X
, Wen X ![]() , Wu F
, Wu F ![]() , Peng J, Tian H, Zhou Y, Ran P
, Peng J, Tian H, Zhou Y, Ran P
Received 18 January 2022
Accepted for publication 30 April 2022
Published 5 May 2022 Volume 2022:17 Pages 1069—1080
DOI https://doi.org/10.2147/COPD.S356797
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Huajing Yang,1,* Zihui Wang,1,* Shan Xiao,1 Cuiqiong Dai,1 Xiang Wen,1 Fan Wu,1,2 Jieqi Peng,1 Heshan Tian,1 Yumin Zhou,1,2 Pixin Ran1,2
1National Center for Respiratory Medicine, State Key Laboratory of Respiratory Disease, National Clinical Research Center for Respiratory Disease, Guangzhou Institute of Respiratory Health, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou, People’s Republic of China; 2Guangzhou Laboratory, Bio-Island, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Pixin Ran; Yumin Zhou, National Center for Respiratory Medicine, State Key Laboratory of Respiratory Disease, National Clinical Research Center for Respiratory Disease, Guangzhou Institute of Respiratory Health, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou, People’s Republic of China, Tel +86 2083205187, Fax +86 20-81340482, Email [email protected]; [email protected]
Background: The effect of serum uric acid (SUA) levels on lung function in chronic obstructive pulmonary disease (COPD) people remained unclear. We aimed to investigate the association between SUA and lung function.
Methods: A cross-sectional study was performed to measure the SUA levels and lung function in 2797 consecutive eligible individuals. Of these, individuals in our study were divided into two groups, the COPD group (n=1387) and the non-COPD group (n=1410). The diagnosis of COPD is defined as post-bronchodilator first second of forced expiratory volume (FEV1)/forced vital capacity (FVC) ratio of less than 0.70. Multivariable adjustment linear models were applied to estimate the effect of SUA levels on FEV1% predicted, FVC% predicted, and FEV1/FVC stratified by COPD status.
Results: After multivariable adjustment, each 1 mg/dL increase of SUA was significantly associated with a decrease in FEV1% predicted (− 1.63%, 95% confidence interval [CI] − 2.37 to − 0.90), FVC % predicted (− 0.89%, 95% CI − 1.55 to − 0.24), and FEV1/FVC (− 0.70%, 95% CI − 1.10 to − 0.30). In the COPD group, each 1 mg/dL increase of SUA was significantly associated with decreases in FEV1% predicted (− 1.87%, 95% CI − 2.91 to − 0.84), FVC% predicted (− 1.35%, 95% CI − 2.35 to − 0.34), and FEV1/FVC (− 0.63%, 95% CI − 1.18 to − 0.08). However, no significant association between lung function and SUA was found among people without COPD.
Conclusion: High SUA levels were associated with lower lung function, especially in COPD patients. However, no statistically significant effect of SUA on lung function was found in people without COPD.
Keyword: serum uric acid, lung function, COPD, non-COPD
Introduction
Serum uric acid (SUA) is the final breakdown product of purines or purine-containing compounds and is present at high concentrations in the epithelial lining fluid of the airway and in plasma.1–3 SUA has the double-edged characteristic of having antioxidant properties as well as pro-oxidant and pro-inflammatory properties.4,5 Based on these characteristics, there are complicated interpretations of whether SUA has a beneficial or noxious effect on lung function.6–8 An experimental study revealed that high SUA levels could improve emphysematous phenotype and lung dysfunction by reducing oxidative stress in mice with chronic obstructive pulmonary disease (COPD), and also found no significant effects of SUA on the lung function in non-diseased mice.9 What they found suggests that SUA levels may only affect lung function in individuals with impaired lung tissue but not normal lung structure.
Impairment of lung tissue reduces oxygen intake, which may result in tissue hypoxia. Tissue hypoxia elevates the SUA levels by inducing the degradation of adenosine.10 Previous studies have found a negative association between SUA levels and measures of lung function, such as forced vital capacity (FVC) and the first second of forced expiratory volume (FEV1) in individuals with COPD.8,11 Another study found no effect of SUA on lung function in the same population.12
For the population with normal lung structure, the effect of high SUA levels on lung function have been conflicting in cross-sectional studies; while a positive effect was found in a large Korean population (n=69,928) without any clinical diseases,6 a negative effect was observed in the Korean National Health and Nutrition Examination Survey,13 and also no significant effect was found in young adults aged 22–29 years.14
Current researchers have paid greater attention to differential effects of SUA on lung function stratified by smoking status15 or gender status,13 but no attention to respiratory disease status. To the best of our knowledge, this is the first epidemiological study focusing on the different effects of SUA on lung function in individuals with or without COPD. In currently available research, the relationships between SUA and lung function stratified by COPD status are not well-characterized for reasons of different populations and the heterogeneous analysis methods among others.
Based on this, our study aimed to identify the relationship between SUA and lung function in individuals with or without COPD.
Methods
Study Population and Blood Tests
Our study applied the baseline data set of a cohort study of people with chronic airway disease in Guangdong, China (ChiCTR1900024643), which was a population-based, multicenter randomized survey of COPD, conducted from June 2019 to June 2021. This study included people: 1) people aged over 30 years old; 2) people who had signed informed consent; 3) who returned complete COPD-related questionnaires; 4) who had undergone the standardized spirometry; 5) who had completed blood tests. Exclusion criteria were the following: 1) a history of malignancy; 2) acute inflammatory diseases or infectious diseases (such as pneumonia, bronchiectasis with infection and active pulmonary tuberculosis); 3) acute exacerbation of COPD within four weeks; 4) cardiovascular or chronic pulmonary diseases (such as hypertension, asthma, bronchiectasis, pneumoconiosis, and interstitial lung diseases), which can affect SUA levels.
Initially, a total of 3160 study subjects were considered as eligible subjects and included in our study. After excluding those without a laboratory examination (n=118), without a complete questionnaire (n=62) and lacking available spirometry data (n=183), 2797 participants were enrolled in our study (Figure 1). Invited participants were required to undergo anthropometric measurement, the spirometer examination, laboratory assessment, and also answered COPD related-questionnaires. The study protocol was approved by the Ethics Committee of the First Affiliated Hospital of Guangzhou Medical University (No.2018–53). All participants gave written informed consent. This present study was in line with the principles of the Declaration of Helsinki.
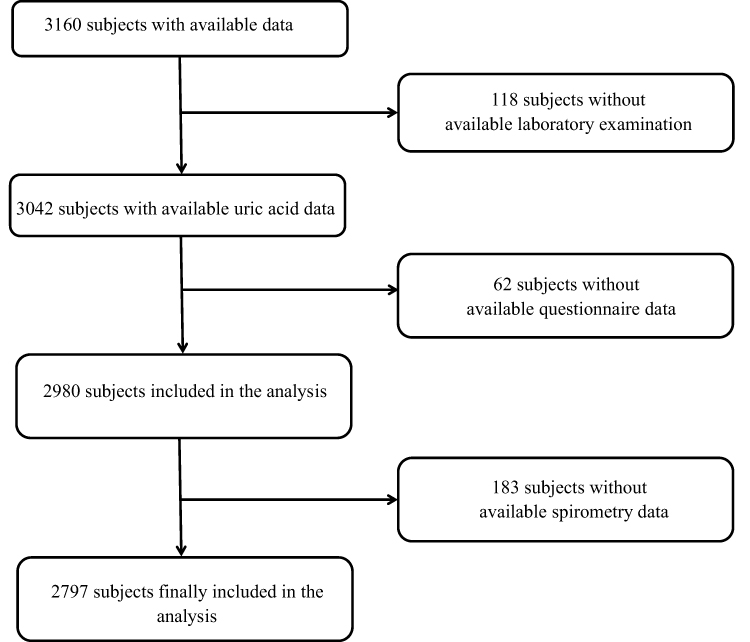 |
Figure 1 Study flow chart. |
Blood samples were obtained from invited participants after 12 h of fasting. SUA levels were determined by the uricase-peroxidase method and by the creatinase-peroxidase method, respectively.16
Outcome Definitions
Invited participants were required to complete a questionnaire based on the questionnaires from the International Burden of Obstructive Lung Disease Study17 and a 2007 Chinese epidemiological study,18 that included potential risk factors for COPD and also chronic respiratory symptoms (such as cough, phlegm production, and dyspnoea). The technicians who were responsible for administering this questionnaire had been strictly trained and also passed a training test. The presence of cough was assessed with “Do you usually cough for three consecutive months or more per year for two years? ” Phlegm production was assessed with “Do you usually bring up phlegm for three consecutive months or more per year for two years?” Dyspnoea was assessed with “Have you had shortness of breath either when walking up a slight hill or brisk walking on the level?”
Lung Function Measures
Participants aged over 30 years were required to finish standardized spirometry. Participants who were physically incapable of taking standardized spirometry (ie, thoracic, abdominal, or eye surgery, retinal detachment or myocardial infarction in past three months; pregnant or breastfeeding; antibacterial chemotherapy for tuberculosis) were excluded.19 Before and after bronchodilator spirometries were performed by using a portable spirometer (CareFusion MasterScreen Pneumo, Germany) according to the European Respiratory Society/American Thoracic Society standards (ERS/ATS 2005).19 Manoeuvre of American Thoracic Society quality grade C or above were acceptable for analysis.20 Standardized spirometry was conducted during the summer, from 2019 to 2020. The diagnosis of COPD is defined by post-bronchodilator (Salbutamol Sulfate Aerosol, 400 μg, 20 min later) FEV1/FVC ratio of less than 0.70.21 The predicted value for FVC and FEV1 is calculated according to the Report Working Party Standardization of lung function tests,22 adjusted by an equation obtained in a representative Chinese population.23
Covariate Definitions
We collected demographic data, including sex, age, and also body index mass (BMI). Never smokers were defined as adults who reported having smoked less than 100 cigarettes in their lifetime. Current smokers were defined as adults who reported having smoked more than 100 cigarettes in their lifetime and also currently smoke some days or every day. Former smokers were defined as adults who reported having smoked more than 100 cigarettes in their lifetime but quit smoking more than three months.
Statistical Analyses
The normality of distribution of variables was evaluated with the Kolmogorov–Smirnov test. Continuous variables were exhibited as the mean ± SD when in a normal distribution, and as medians (interquartile ranges) when in a skewed distribution. Student’s t-test was applied to compare differences among individuals with and without COPD. Categorical variables were expressed as numbers (percentages), and the Chi-square test or Fisher’s exact test were used to assess the inter-group difference. Continuous SUA values were also transformed into categorical variables according to their terciles. The ANOVA test was applied to investigate the significant differences between different SUA- levels groups.
Binary logistic models were applied to investigate the relationships between the SUA levels, the presence of COPD, and the chronic respiratory symptoms (cough, phlegm production, and dyspnea), either adjusted or unadjusted sex, age, smoking status, cumulative tobacco smoking, and body mass index (BMI). To investigate the different effects of SUA on lung function, we also conducted a multivariate analysis among individuals with or without COPD. Odds ratios (ORs) and 95% confidence intervals (95% CIs) were calculated to estimate the strength of this association.
Multivariable adjustment linear models were implied to estimate the effect of SUA levels on FEV1%, FVC%, and FEV1/FVC. We also tested the assumptions of normality, linearity, and homoscedasticity graphically by using plots of observed versus predicted values as well as also plots of residuals versus predicted values or the observed exposure values. No major violations were found.
In the sensitivity analysis, the same analyses were performed in the different groups by smoking statuses to explore any differential effects of SUA based on smoking status. Analyses of the gender subgroups were also conducted. The relationship between SUA and spirometer measurement after bronchodilators was also estimated.
All tests were two-sided, and p-values less than 0.05 were considered statistically significant. Data were analyzed using R statistical software (version 4.1.0).
Results
Study Population
A total of 2797 participants who met inclusion criteria and had available data were enrolled in our study, including 1410 (50.41%) non-COPD subjects and 1387 (49.58%) COPD patients. The clinical characteristics and biochemical biomarkers of invited participants are presented in Table 1. Participants were divided into two groups based on their current status of COPD. Significant differences between the two groups were found, such as sex, age, BMI, smoking status, pre-bronchodilator spirometric values, and also chronic respiratory symptoms. Additionally, overall SUA levels were higher in individuals with COPD, as 4.17 ± 1.10 mg/dl, versus 3.79 ± 1.14 mg/dl in the non-COPD group (Table 1; Figure 2). Individuals with high SUA levels were older, with higher values of BMI, and more likely to be current smokers compared to individuals in the lowest SUA group. Those in the highest terciles were also more likely to have lower FEV1% predicted, lower FVC % predicted, and low FEV1/FVC. Compared to the lowest SUA tertiles, individuals in the two highest terciles were more likely to report a risk of cough, phlegm production, and also dyspnoea.
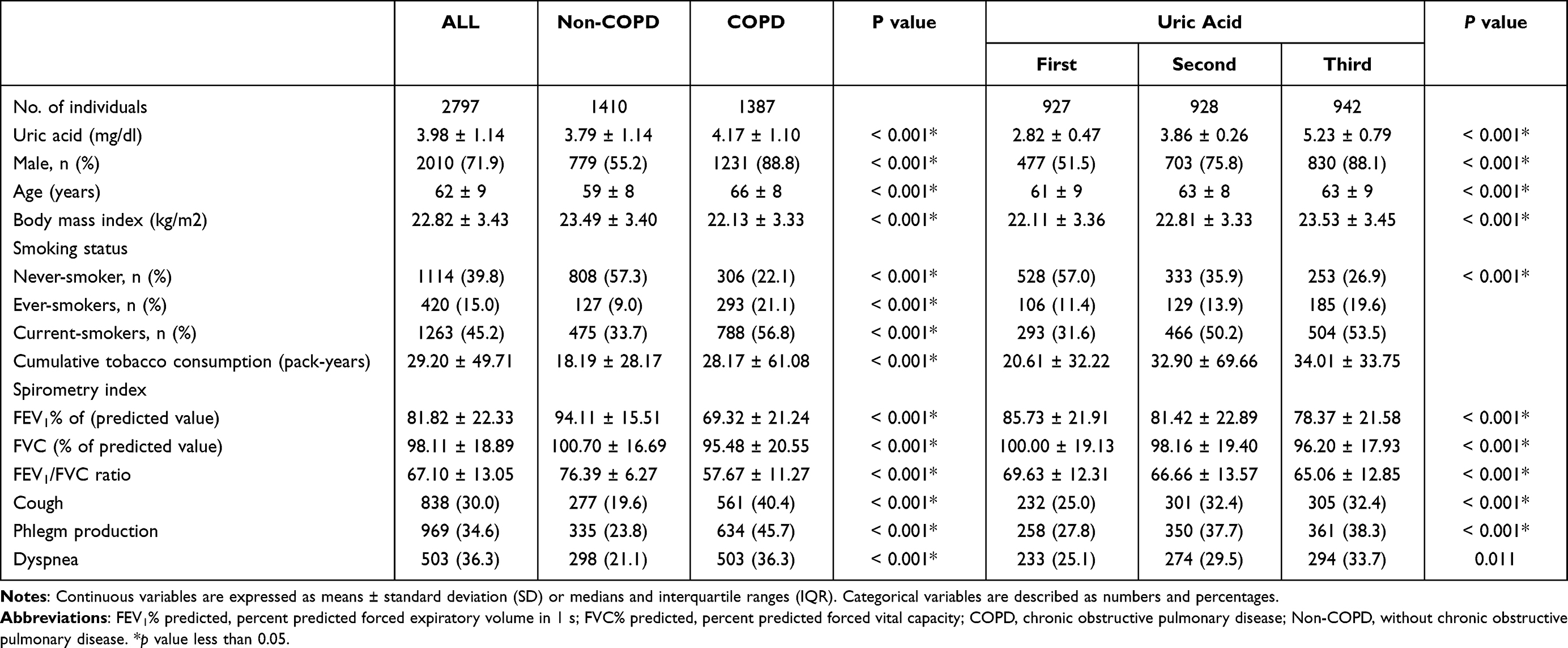 |
Table 1 The Association of Baseline Participant Characteristics with SUA and COPD (N=2797) |
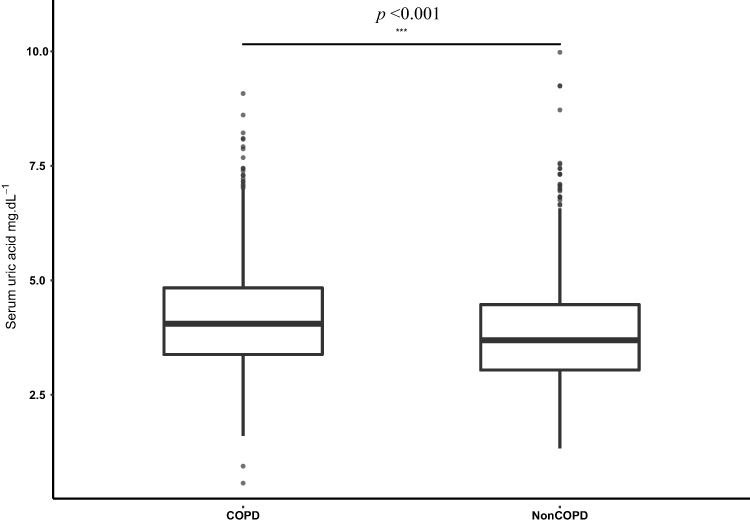 |
Figure 2 Serum uric acid levels in people with and without chronic obstructive pulmonary disease. ***p value less than 0.001. Abbreviations: COPD, chronic obstructive pulmonary disease; Non-COPD, without chronic obstructive pulmonary disease. |
Uric Acid and COPD
Unadjusted logistic regression analysis showed no significant effect of SUA on the prevalence of COPD (unadjusted OR,1.33; 95% CI 1.25 to 1.44) (Table 2). After multivariable adjustment, the OR (95% CI) of the prevalence of COPD was 1.15 (95% CI 1.06 to 1.25) with p-value less than 0.001 per 1 mg/dL increase of SUA (Table 2; Figure 3). Similar results were also found both in the never-smoker and ever-smoker groups (online supplementary Figure A1), but not in the female population (online supplementary Figure A2).
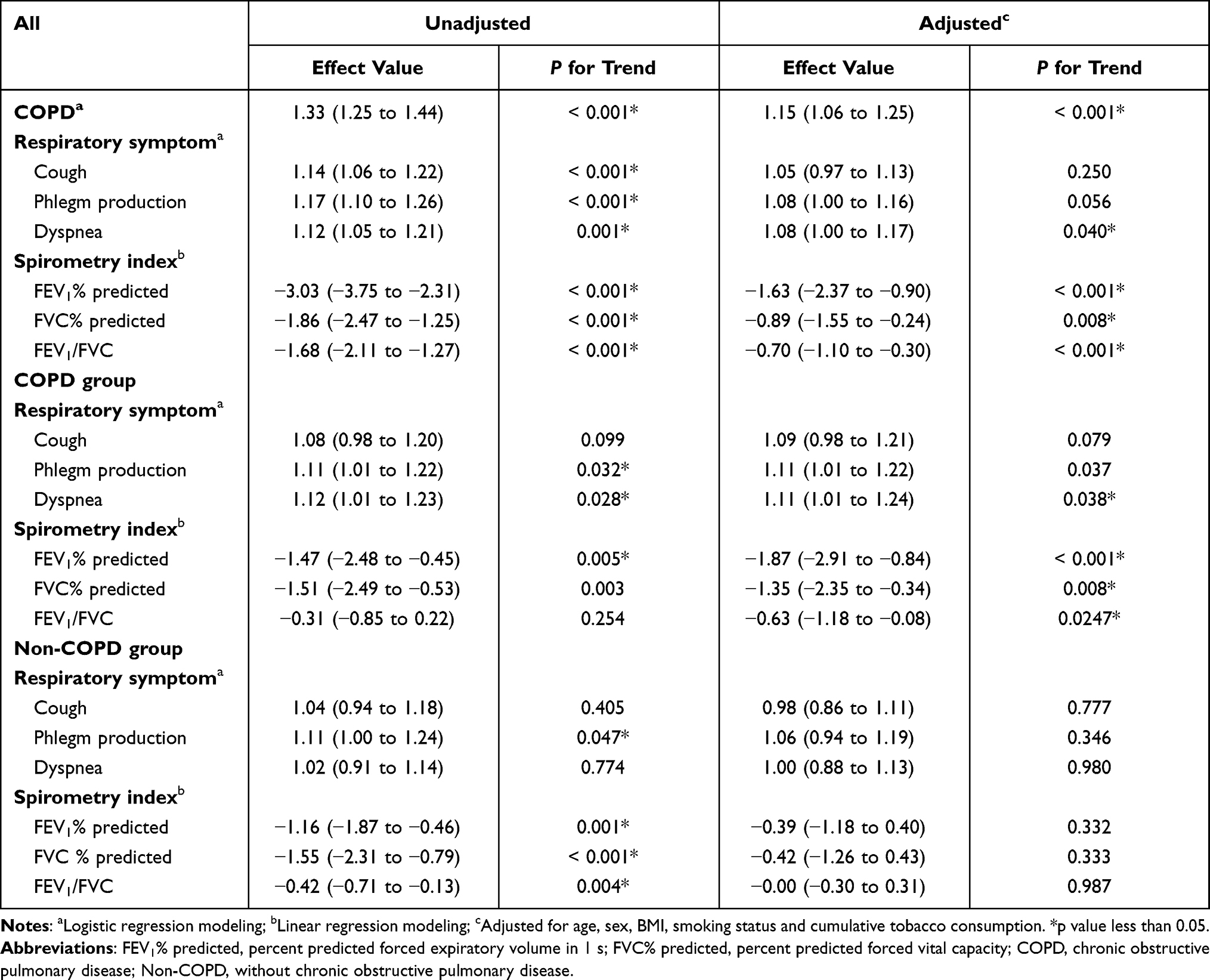 |
Table 2 Association Between SUA, Lung Function and Chronic Respiratory Symptom in People with or Without COPD |
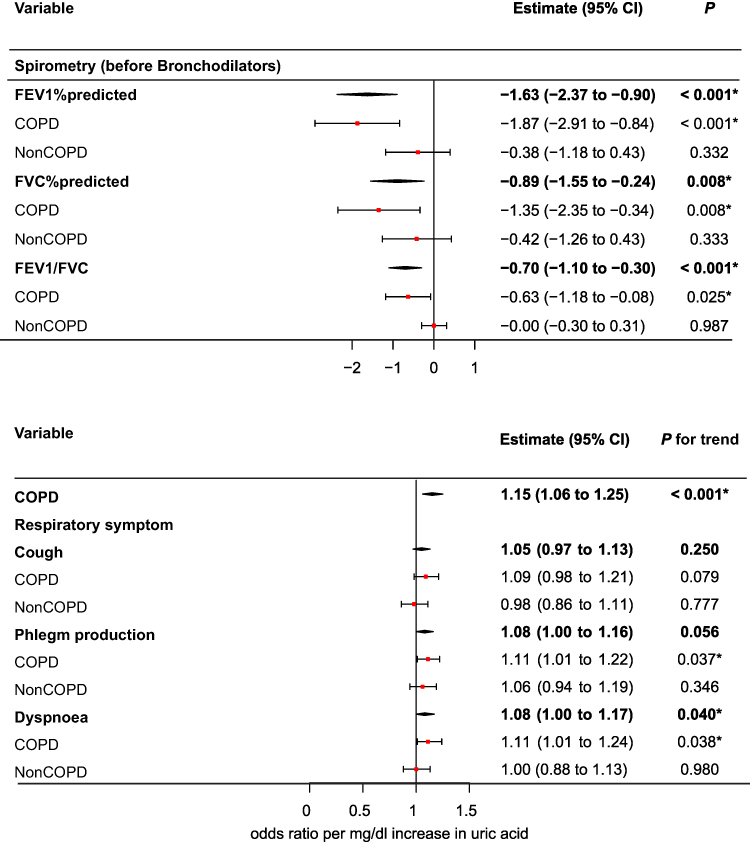 |
Figure 3 Association of SUA levels with study outcomes. Shown are odds ratio or estimate effect for each outcome for each 1 mg/dl increase in serum uric acid, adjusted for age, sex, BMI, smoking status, and cumulative tobacco consumption. Bold values means that all participants were in the analysis. *p value less than 0.05. Abbreviations: COPD, chronic obstructive pulmonary disease; Non-COPD, without chronic obstructive pulmonary disease; FEV1% predicted, percent predicted forced expiratory volume in 1 s; FVC% predicted, percent predicted forced vital capacity; 95% CI, 95% confidence interval. |
Uric Acid and Lung Function
After multivariable adjustment, each 1 mg/dl increase of SUA was associated with a 1.63% decrease in FEV1% predicted (95% CI −2.37 to −0.90) (Table 2; Figure 3; Figure 4). Each 1 mg/dl increase of SUA was significantly associated with a 1.87% (95% CI −2.91 to −0.84) decrease in FEV1% predicted, but no significant relationship was found in the non-COPD group (0.39%,95% CI −1.18 to 0.40). After multivariable adjustment, each 1 mg/dl increase of SUA levels was associated with a −0.89% decrease (95% CI −1.55 to−0.24) in FVC % predicted. Similar results were found in the COPD group, (−1.35% [95% CI −2.35 to −0.34]) but not in the non-COPD group (−0.42% [95% CI −1.26 to 0.43]). Additionally, after multivariable adjustment, each 1 mg/dL increase in SUA levels was associated with a −0.7% (95% CI −1.10 to −0.30) decrease in FEV1 /FVC. Each 1 mg/dl increase in SUA was associated with a 0.63% decrease in FEV1 /FVC in the COPD group, while no significant association between SUA levels and FEV1 /FVC was found in the Non-COPD group (p-value 0.987). The associations between SUA levels and lung function after using bronchodilators were also evaluated, with similar results were found (online supplementary Figure A3.).
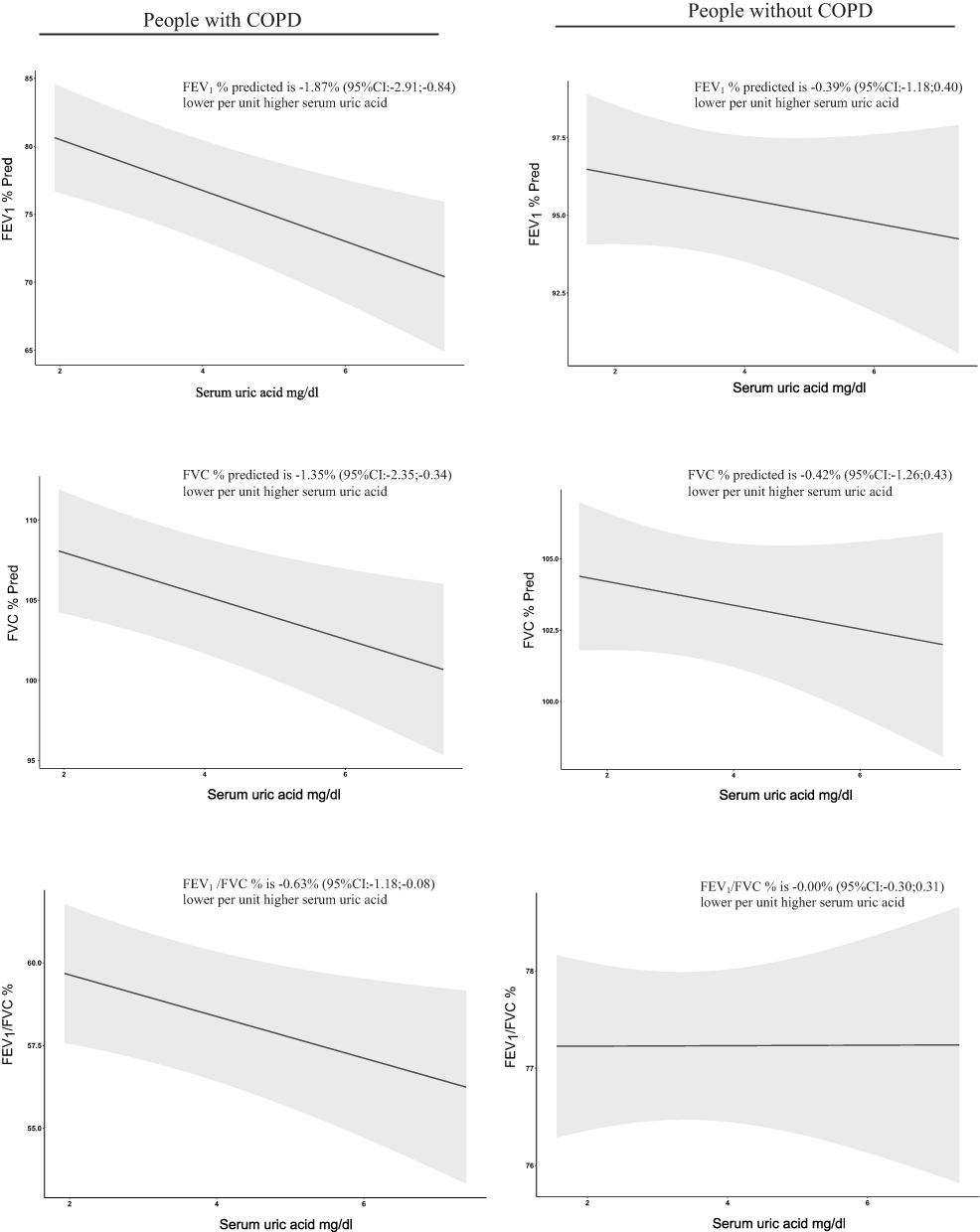 |
Figure 4 Regression of lung function on SUA in people with or without COPD. The analysis was multi-variable adjusted for age, sex, BMI, smoking status, and cumulative tobacco consumption. Regression values in the top and 95% CIs were shown as the shaded area around the regression line. Abbreviations: COPD, chronic obstructive pulmonary disease; Non-COPD, without chronic obstructive pulmonary disease; FEV1% predicted, percent predicted forced expiratory volume in 1 s; FVC% predicted, percent predicted forced vital capacity. |
Uric Acid and Symptoms of Airway Disease
The OR of dyspnea was 1.12 (95% CI 1.05 to 1.21) with each 1 mg/dl higher SUA (Table 2; Figure 3). This association remained significant after adjustment for potential confounders. People with COPD had a higher risk of dyspnea than did those without COPD (adjusted ORs, 1.11 in the COPD group and 1.07 in the non-COPD group). No significant effect of SUA on dyspnoea was found in the non-COPD group (adjusted OR,1.00; 95% CI 0.88 to 1.13).
Discussion
This observational study analyzed 1387 individuals (49.58%) with COPD. Individuals with COPD had significantly higher SUA levels than did individuals without COPD (4.17 ± 1.10 vs 3.79 ± 1.14, respectively). In addition, we found that increased SUA levels were significantly associated with decreased in FEV1% predicted, FVC% predicted, and FEV1/FVC, and with increased risk of COPD as well as chronic respiratory symptoms. Negative associations between SUA and FEV1% predicted, FVC% predicted, and FEV1/FVC were found in the COPD group, but no significant association between lung function and SUA levels was found in the non-COPD group. To the best of our knowledge, this is the first epidemiological study focusing on the different effects of SUA on lung function based on individuals with or without COPD.
Cross-sectional studies have estimated that higher SUA levels were positively6 and inversely24 associated with lung function. Previous epidemiological results have been rather inconsistent whether in COPD populations or healthy populations. Two studies found that increased SUA levels accelerated lung function decline in COPD patients,12,25 while another found no significant effect of SUA on lung function in individuals with COPD.12 Similarly, the contradictory effect of SUA on lung function was found in individuals without COPD. In comparison, a positive effect was observed in a large Korean population (n=69,928) of healthy subjects,6 a negative effect was reported in the Korean National Health and Nutrition Examination Survey,13 and another analysis of young adults aged 22–29 years found no significant effect.14 With the heterogeneity of the above studies, such as in term of demographic data and statistical analysis, and so on, it is difficult to draw a clear relationship between SUA and lung function and to explore potential mechanisms, which may explain the discrepancy in current epidemiological studies.
The potentially different effects of SUA on lung function may depend on differential mechanisms. Shaheen suggested that interpretation of previous studies need to be careful26 and provided several possible mechanisms, such as the pro-oxidant and pro-inflammatory properties of SUA, a poor proxy for epithelial lining fluid concentrations, and also potential for confounding. Previous studies have demonstrated that SUA levels were inversely correlated with lung function in the female general population but not the male population.13,24 Though the cause of these sex differences between SUA and lung function remain uncertain, one study has suggested that sex hormones may affect SUA metabolism, making the relative health effect of SUA may be stronger in female generations.27 Further, our study provides a new insight to explain the contradictory relationship between SUA and lung function, the health effect of SUA levels on lung function, which is that health effect of SUA levels on lung function could be influenced by COPD status.
Previous experimental studies have estimated that high SUA levels do not affect reactive oxygen species levels, which can initiate inflammation or airway remodeling26,28–30 under normal conditions, and do not affect lung function under the same condition.9 Experimentally induced hypoxia models found that SUA levels were higher in hypoxia status compared to normal status in lung tissue,31 which means that hypoxia may promote purine catabolism,32,33 which could increase the levels of SUA, and those elevated SUA levels can cause systemic inflammation, potentially damaging lung function. A previous epidemiological study revealed that SUA levels were higher in people with more severe airflow limitation, and were also increased in the presence of hypoxia and systemic inflammation.25 Braghiroli et al suggested that compared to the healthy population, SUA levels were significantly increased in individuals with COPD in hypoxia status but not in those without.32 In a cross-sectional study, Nicks et al found that lower SUA levels were associated with COPD severity in the cross-sectional study.7
This is consistent with our findings; high SUA levels impaired the lung function in the COPD patients but not in non-COPD people with normal oxygen saturation.34,35 Although oxygen saturation values were not collected in our studies, we identified the positive correlation between the high SUA levels and the risk of dyspnoea. As people with the symptom of dyspnoea have different levels of hypoxia,36 that may support our assumptions. Meanwhile, further research is needed to explore the relationships among SUA, lung function, and oxygen saturation in respiratory disease, especially in COPD patients.
A variety of factors such as air pollution and smoking are suggested to have more influence on lung function in COPD patients and therefore have attracted significant attention. Quitting smoking and avoiding air pollution are important suggestions to prevent decreased lung function in COPD patients, but blood biomarkers such as higher SUA levels cannot be ignored. A meta-analysis demonstrated that SUA levels might be a useful biomarker for COPD,37 and an independent predictor of mortality, and are associated with a higher risk of acute exacerbation of COPD.25,38 For better management of COPD, further research about the effect of SUA on lung function, especially in COPD patients, is required.
The strengths of this study include its large sample size and also the amount of data available. Subjects in our study were enrolled from the community but not the clinic, without any severity underlying disease except COPD. Additionally, we were also able to analyze the effect of SUA on lung function after bronchodilation, which could not observed in the previous studies. Similar results were found when compared to SUA levels and lung function before bronchodilation.
Some limitations in our study should be considered. First, the population in our study consisted mostly of males (71.9%), and the percentage of females (28.1%) was lower than in other studies,6,39 which may have influenced the overall results. Nonetheless, the observed association between SUA and lung function persisted in a gender-adjusted model. Second, several possible factors that may influence SUA levels were not completely ruled out, including chronic kidney disorders, alcohol consumption, food intake, metabolic syndrome, and also cardiovascular disease. However, after adjustment for major confounders (age, gender, BMI, smoking status, and cumulative tobacco consumption), logistic regression analysis showed that SUA levels continued to be a significant predictor of COPD risk. Similar results were seen in the linear regression model. Based on this, we believe that the influence of biases from unknown confounding that the model did not adjust for did not significantly affect the outcome. Thirdly, though SUA levels have been suggested to be an imperfect proxy for epithelial lining fluid concentration,1 SUA from epithelial lining fluid concentration is thought to be secreted by submucosal nasal glands after uptake from plasma.3 Lastly, because the design of our study was retrospective and cross-sectional, the causal relationship between uric acid and lung function could not be determined.
Conclusion
In conclusion, the high SUA level was associated with a higher risk of COPD and chronic respiratory symptoms, and lower lung function. What’s more, significant effects of SUA on lung function were found in individuals with COPD, but not individuals without COPD.
Abbreviations
SUA, serum uric acid; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; BMI, body mass index; ORs, odds ratios.
Data Sharing Statement
With the permission of the corresponding authors, we can provide participant data without names and identifiers. The corresponding authors have the right to decide whether to share the data based on the research objectives and plan provided. Data will be immediately available after publication. No end date. Please contact correspondence author for data requests.
Ethics Approval and Informed Consent
The study protocol was approved by the Ethics Committee of the First Affiliated Hospital of Guangzhou Medical University. All participants gave written informed consent.
Consent for Publication
This article has not been published elsewhere in whole or in part. All authors have read and approved the content, and agree to submit it for consideration for publication in your journal. There are no ethical/legal conflicts involved in the article.
Acknowledgments
We thank all the participants who contributed to this study. Thanks are due to Zhishan Deng, Youlan Zheng, Lifei Lu, Ningning Zhao, Jianwu Xu, Peiyu Huang, Xiaopeng Ling, Shaodan Wei, Qiaoyi He, Wenjun Lai and Yunsong Chen (National Center for Respiratory Medicine, State Key Laboratory of Respiratory Disease, National Clinical Research Center for Respiratory Disease, Guangzhou. Institute of Respiratory Health, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou Medical University, Nan shan Medical Development Foundation of Guangdong Province) for Data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The present study was supported by The National Key Research and Development Program of China (Grant number 2016YFC1304101), the Local Innovative and Research Teams Project of Guangdong Pearl River Talents Program (2017BT01S155), the National Natural Science Foundation of China (81970045), Zhongnanshan Medical Foundation of Guangdong Province (ZNSA2020003, ZNSA-2021012, and ZNSA-2020013) Basic and Applied Basic Research Fund of Guangdong Province (2020A 1515110915) and National Natural Science Foundation of China (82000044).
Disclosure
We declare that there are no financial or personal competing interests associated with the study.
References
1. van der Vliet A, Neill O, Cross CE, et al. Determination of low-molecular-mass antioxidant concentrations in human respiratory tract lining fluids. Am J Physiol. 1999;276(2):L289–L296. doi:10.1152/ajplung.1999.276.2.L289
2. Kelly FJ, Blomberg A, Frew A, et al. Antioxidant kinetics in lung lavage fluid following exposure of humans to nitrogen dioxide. Am J Respir Crit Care Med. 1996;154:1700–1705. doi:10.1164/ajrccm.154.6.8970358
3. Peden DB, Hohman R, Brown ME, et al. Uric acid is a major antioxidant in human nasal airway secretions. Proc Natl Acad Sci U S A. 1990;87:7638–7642. doi:10.1073/pnas.87.19.7638
4. So A, Thorens B. Uric acid transport and disease. J Clin Invest. 2010;120(6):1791–1799. doi:10.1172/JCI42344
5. Lyngdoh T, Marques-Vidal P, Paccaud F, et al. Elevated serum uric acid is associated with high circulating inflammatory cytokines in the population-based Colaus study. PLoS One. 2011;6(5):e19901. doi:10.1371/journal.pone.0019901
6. Song JU, Hwang J, Ahn JK. Serum uric acid is positively associated with pulmonary function in Korean health screening examinees. Mod Rheumatol. 2017;27:1057–1065. doi:10.1080/14397595.2017.1285981
7. Nicks NE, O’Brien MM, Bowler RP. Plasma antioxidants are associated with impaired lung function and COPD exacerbations in smokers. COPD. 2011;8:264–269. doi:10.3109/15412555.2011.579202
8. Kobylecki CJ, Vedel-Krogh S, Afzal S, et al. Nordestgaard, Plasma urate, lung function and chronic obstructive pulmonary disease: a Mendelian randomisation study in 114 979 individuals from the general population. Thorax. 2018;73(8):748–757. doi:10.1136/thoraxjnl-2017-210273
9. Fujikawa H, Sakamoto Y, Masuda N, et al. Higher blood uric acid in female humans and mice as a protective factor against pathophysiological decline of lung function. Antioxidants. 2020;9(5):387. doi:10.3390/antiox9050387
10. Elsayed NE, Nakashima JM, Postlethwait EM. Measurement of uric acid as a marker of oxygen tension in the lung. Arch Biochem Biophys. 1993;302(1):228–232. doi:10.1006/abbi.1993.1204
11. Kahnert K, Alter P, Welte T, et al. Uric acid, lung function, physical capacity and exacerbation frequency in patients with COPD: a multi-dimensional approach. Respir Res. 2018;19(1):110. doi:10.1186/s12931-018-0815-y
12. Garcia-Pachon E, Padilla-Navas I, Shum C. Serum uric acid to creatinine ratio in patients with chronic obstructive pulmonary disease. Lung. 2007;185(1):21–24. doi:10.1007/s00408-006-0076-2
13. Jeong H, Baek SY, Kim SW, et al. Gender-specific association of serum uric acid and pulmonary function: data from the Korea National Health and Nutrition Examination Survey. Medicine. 2021;57:953.
14. Garcia-Larsen V, Chinn S, Rodrigo R, et al. Relationship between oxidative stress-related biomarkers and antioxidant status with asthma and atopy in young adults: a population-based study. Clin Exp Allergy. 2009;39(3):379–386. doi:10.1111/j.1365-2222.2008.03163.x
15. Horsfall LJ, Nazareth I, Petersen I. Serum uric acid and the risk of respiratory disease: a population-based cohort study. Thorax. 2014;69(11):1021–1026. doi:10.1136/thoraxjnl-2014-205271
16. Domagk GF, Schlicke HH. A colorimetric method using uricase and peroxidase for the determination of uric acid. Anal Biochem. 1968;22(2):219–224. doi:10.1016/0003-2697(68)90309-6
17. Buist AS, McBurnie MA, Vollmer WM, et al. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370(9589):741–750. doi:10.1016/S0140-6736(07)61377-4
18. Zhou Y, Hu G, Wang D, et al. Community based integrated intervention for prevention and management of chronic obstructive pulmonary disease (COPD) in Guangdong, China: cluster randomised controlled trial. BMJ. 2010;341(2):c6387. doi:10.1136/bmj.c6387
19. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26:319–338. doi:10.1183/09031936.05.00034805
20. Enright PL, Studnicka M, Zielinski J. Spirometry to detect and manage chronic obstructive pulmonary disease and asthma in the primary care setting. Eur Respir Mon. 2005;31:1–14.
21. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 Report: GOLD executive summary. Am J Respir Crit Care Med. 2017;195:557–582. doi:10.1164/rccm.201701-0218PP
22. Quanjer PH, Tammeling GJ, Cotes JE, et al. Lung volumes and forced ventilatory flows. Eur Respir J. 1993;16:5–40.
23. Zheng J, Zhong N. Normative values of pulmonary function testing in Chinese adults. Chin Med J. 2002;115(1):5054.
24. Aida Y, Shibata Y, Osaka D, et al. The relationship between serum uric acid and spirometric values in participants in a health check: the Takahata study. Int J Med Sci. 2011;8(6):470–478. doi:10.7150/ijms.8.470
25. Bartziokas K, Papaioannou AI, Loukides S, et al. serum uric acid as a predictor of mortality and future exacerbations of COPD. Eur Respir J. 2014;43(1):43–53. doi:10.1183/09031936.00209212
26. Shaheen SO. Uric acid, lung function and COPD: a causal link is unlikely. Thorax. 2018;73(8):697–698. doi:10.1136/thoraxjnl-2017-211230
27. De Vera MA, Rahman MM, Bhole V, et al. The independent impact of gout on the risk of acute myocardial infarction among elderly women: a population-based study. Ann Rheum Dis. 2010;69:1162–1164. doi:10.1136/ard.2009.122770
28. McNeil JD, Wiebkin OW, Betts WH, et al. Depolymerisation products of hyaluronic acid after exposure to oxygen-derived free radicals. Ann Rheum Dis. 1985;44:780–789. doi:10.1136/ard.44.11.780
29. Uchiyama H, Dobashi Y, Ohkouchi K, et al. Chemical change involved in the oxidative reductive depolymerization of hyaluronic acid. J Biol Chem. 1990;265:7753–7759. doi:10.1016/S0021-9258(19)38993-8
30. McKee CM, Penno MB, Cowman M, et al. Hyaluronan (HA) fragments induce chemokine gene expression in alveolar macrophages. The role of HA size and CD44. J Clin Invest. 1996;98:2403. doi:10.1172/JCI119054
31. Ozanturk E, Ucar ZZ, Varol Y, et al. Urinary uric acid excretion as an indicator of severe hypoxia and mortality in patients with obstructive sleep apnea and chronic obstructive pulmonary disease. Rev Port Pneumol. 2016;22:18–26. doi:10.1016/j.rppnen.2015.06.002
32. Braghiroli A, Sacco C, Erbetta M, et al. Overnight urinary uric acid: creatinine ratio for detection of sleep hypoxemia. Validation study in chronic obstructive pulmonary disease and obstructive sleep apnea before and after treatment with nasal continuous positive airway pressure. Am Rev Respir Dis. 1993;148:173–178. doi:10.1164/ajrccm/148.1.173
33. Saito H, Nishimura M, Shibuya E, et al. Tissue hypoxia in sleep apnea syndrome assessed by uric acid and adenosine. Chest. 2002;122(5):1686–1694. doi:10.1378/chest.122.5.1686
34. Sundh J, Ekström M. Risk factors for developing hypoxic respiratory failure in COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:2095–2100. doi:10.2147/COPD.S140299
35. Wells JM, Estepar RS, McDonald MN, et al. Clinical, physiologic, and radiographic factors contributing to development of hypoxemia in moderate to severe COPD: a cohort study. BMC Pulm Med. 2016;16:169. doi:10.1186/s12890-016-0331-0
36. Higashimoto Y, Honda N, Yamagata T, et al. Exertional dyspnoea and cortical oxygenation in patients with COPD. Eur Respir J. 2015;46(6):1615–1624.
37. Li H, Chen Y. Serum uric acid level as a biomarker for chronic obstructive pulmonary disease: a meta-analysis. J Int Med Res. 2021;49(1):300060520983705. doi:10.1177/0300060520983705
38. Zhang X, Liu L, Liang R, Jin S. Hyperuricemia is a biomarker of early mortality in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2015;10:2519–2523. doi:10.2147/COPD.S87202
39. Fukuhara A, Saito J, Sato S, et al. The association between risk of airflow limitation and serum uric acid measured at medical health check-ups. Int J Chron Obstruct Pulmon Dis. 2017;12:1213–1219. doi:10.2147/COPD.S126249
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.