")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Association Between Serum Thyroid Measurements and Hyperhomocysteinemia in Euthyroid Subjects: A Retrospective Cross-Sectional Study
Received 21 August 2023
Accepted for publication 24 October 2023
Published 30 October 2023 Volume 2023:16 Pages 3425—3433
DOI https://doi.org/10.2147/DMSO.S436381
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Jiayun Zou,1 Yuhan Wang2
1Department of Thyroid Surgery, The First Hospital of China Medical University, Shenyang, Liaoning, People’s Republic of China; 2Department of Cardiovascular, The First Hospital of China Medical University, Shenyang, Liaoning, People’s Republic of China
Correspondence: Yuhan Wang, Department of Thyroid Surgery, The First Hospital of China Medical University, No. 155, Nanjing North Street, Heping District, Shenyang, Liaoning, People’s Republic of China, Email [email protected]
Objective: The objective of this study was to investigate the association between serum thyroid measurements and homocysteine (HCy) in euthyroid participants.
Methods: This retrospective study was based on Hospital Information Systems. After excluding participants with thyroid dysfunction and those who had recently taken medications that affected serum HCy, 775 participants were enrolled. We compared the serum thyroid function measurements of patients with or without hyperhomocysteinemia (HHCy) and analyzed the effect of thyroid indicators on HHCy prevalence and HCy levels. Multivariate regression analysis was utilized to analyze the association of thyroid-stimulating hormone (TSH) and thyroid peroxidase (TPOAb) with HCy.
Results: The serum TSH level (2.10 ± 1.06 mIU/L) of HHCy patients (n = 98) was significantly higher than controls (n = 677) (1.65 ± 0.90 mIU/L) (p < 0.05), as was the positive rate of TPOAb (19.4% vs 10.0%, p < 0.05). The serum HCy levels in subjects with TSH within the highest quartile were significantly higher than those in the lowest quartile (13.49 ± 7.78 vs 9.81 ± 3.59 μmol/L, p < 0.05). HCy was also significantly higher in TPOAb-positive patients than in negative subjects (14.06 ± 8.89 vs 11.48 ± 5.47 μmol/L, p < 0.05). Among the TSH quartiles, the prevalence of HHCy showed a similar significant upward trend to that described above. The prevalence of HHCy was also significantly higher in TPOAb-positive patients. The results of multivariate regression analysis suggested that both TSH elevation and TPOAb positivity were independent risk factors for HCy elevation and HHCy prevalence. However, we found no definitive association between linear increases in TPOAb titers and HCy concentrations or HHCy prevalence.
Conclusion: Patients with HHCy had significantly higher TSH levels and positive rates of TPOAb. Elevated TSH and positive TPOAb levels were independent risk factors for elevated HCy concentrations and HHCy risk.
Keywords: thyroid stimulating hormone, thyroid peroxidase antibody, hyperhomocysteinemia, retrospective study
Introduction
Residents of mainland China have a high prevalence of thyroid diseases. According to a recent nationwide cross-sectional survey, subclinical hypothyroidism (SCH) has the highest prevalence among various thyroid disorders, reaching 12.93%.1 At present, serum thyroid-stimulating hormone (TSH) is the most sensitive indicator to diagnose thyroid dysfunction. Over the past few decades, abnormal serum TSH levels have been associated with a variety of cardiovascular and metabolic diseases, including stroke, atrial fibrillation (AF), dyslipidemia, non-alcoholic fatty liver disease (NAFLD), and type 2 diabetes mellitus (T2DM).2–6 Elevated serum TSH may also lead to a significantly increased risk of cardiovascular and all-cause mortality.7,8 Many studies have suggested that even if thyroid function is within the reference interval, an increase or decrease in TSH levels may induce cardiometabolic diseases.9,10 The serum TSH levels and free thyroxine (FT4) levels in individuals are known to be narrower than the reference interval calculated based on population studies. An individual’s TSH setting point is largely determined by genetic background.11 In a previous national cross-sectional study, a significant effect of ethnicity on the TSH reference interval was confirmed.12 As the feedback relationship between pituitary TSH secretion and serum FT4 levels is exquisitely sensitive, an individual’s TSH level is likely to remain within the population-based TSH reference interval, even though the TSH level may be higher or lower than the individual-based reference interval.13 According to clinical experience, even if patients with euthyroid Hashimoto thyroiditis (HT) are positive for thyroid autoantibodies, they still have a higher risk of cardiovascular and metabolic diseases, and even have manifestations associated with thyroid dysfunction.14 Therefore, it is necessary to explore the correlation between the fluctuation of thyroid function within the reference interval and the risk of related diseases.
Hyperhomocysteinemia (HHCy) is a common metabolic disorder, which can be divided into two categories according to its etiology: inherited and non-inherited types. Among inherited HHCy, cystathionine β-synthase deficiency, methylenetetrahydrofolate reductase deficiency, and methionine adenosyltransferase deficiency manifest as isolated homocysteinemia, whereas cobalamin metabolic disorders can lead to methylmalonic acidemia combined with homocysteinemia. Non-inherited diseases, such as deficiencies of cobalamin, folic acid, vitamin B6, and betaine, can also cause HHCy.15 A previous meta-analysis, which included 36 independent studies, revealed that the overall pooled prevalence of HHCy is 27.5% in mainland China.16 The HHCy prevalence was generally higher in northern cities (34.3%) and inland cities (31.5%), as well as in older (35.2%) and male subjects (34.8%). Studies have suggested that homocysteine (HCy) may cause damage to vascular endothelial cells by promoting the oxidative stress response and the proliferation or migration of vascular smooth muscle cells, thus leading to their dysfunction. HCy may also promote platelet aggregation and deteriorate the coagulation state of blood. The association between HCy level and glycemic regulation has also been demonstrated. HHCy may induce insulin resistance and decrease the efficiency of glucose uptake by surrounding tissues, leading to hyperglycemia. In summary, HCy is currently a recognized risk marker for cardiovascular and metabolic diseases.17 Previous studies have suggested that hyperthyroidism and hypothyroidism were related to the decrease and increased in HCy, respectively,18,19 and that HCy also decreased significantly after the administration of levothyroxine to patients with hypothyroidism.20
Given that fluctuations in thyroid function within the reference range may be independent risk factors for cardiovascular and metabolic diseases, we sought to explore the association between changes in thyroid function within the reference interval and HHCy. As no previous studies have investigated the fluctuation in thyroid function measurements within the reference range and HHCy, our results may serve to fill the current research gaps.
Methods
Study Population
Beginning from February 2019, potential study subjects were screened from the Hospital Information System (HIS) of the First Affiliated Hospital of China Medical University. The inclusion criteria for this study were as follows, subjects had a record of visiting the outpatient clinic or ward of the Department of Thyroid Surgery or Cardiovascular Medicine of China Medical University from February 2019 to the present. All enrolled subjects agreed to participate in the study and signed informed consent forms. The ethics committee of China Medical University approved the study (Approval No. 2023-2022-385-6).
The exclusion criteria were as follows: 1) subjects with missing necessary information or who were unwilling to sign informed consent; 2) children and adolescents < 18 years; 3) participants with a prior personal history of thyroid dysfunction (defined as abnormal serum TSH), recent use of thyroid medications, or thyroid surgery; 4) participants who had recently taken medications (eg, folic acid and multivitamins) that affected serum HCy levels; and 5) subjects with severe hepatic and kidney diseases, autoimmune diseases, malignant tumors, acute infections, and pregnant.
A total of 775 eligible participants were finally enrolled in the study.
Data Collection and Diagnostic Criteria
The height and weight of the subjects were measured by trained nurses. The body mass index (BMI) was obtained by dividing the weight (kg) by the square of the height (m2). Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured using an Omron electronic sphygmomanometer (Omron HEM-7430, Omron Corporation, Kyoto, Japan). All subjects were asked to rest for at least 5 min before the BP measurements. Two BP measurements were taken at least 10 min apart, and the average of the two measurements was considered the final SBP or DBP measurement.
All laboratory test indices used in this study could be queried from the HIS. The levels of serum TSH, FT4-free triiodothyronine (FT3), thyroid peroxidase antibody (TPOAb), and thyroglobulin antibody (TgAb) were measured via a supersensitive chemiluminescence immunoassay (ARCHITECT system i2000SR, Abbott, Chicago, US). Serum HCy levels were detected using an autoanalyzer (Hitachi 747, Roche Diagnostics, Germany). The concentrations of total cholesterol (TC), triglyceride (TG), high-density lipoprotein (HDL), low-density lipoprotein (LDL), and fasting plasma glucose (FPG) were measured using a calibrated Roche Cobas c701 automatic biochemical analyzer (Roche Diagnostics, Mannheim, Germany). The performances of all of the test instruments were optimal and the quality control was under good control.
Hypertension was diagnosed if the SBP exceeded 140 mmHg or the DBP exceeded 90 mmHg. The reference intervals for biochemical indicators were derived from the kit instructions. The reference intervals of serum TSH, FT4, FT3, TPOAb, and TgAb were 0.35–4.94 mIU/L, 9.01–19.05 pmol/L, 2.43–6.01 pmol/L, 0–5.61 IU/mL, and 0–4.11 IU/mL, respectively. HHCy was defined as a serum HCy level >15 μmol/L. The reference intervals for glycemic and lipid indicators were as follows: FPG at 3.9–6.1 mmol/L, TC at 0–5.72 mmol/L, TG at 0–1.70 mmol/L, HDL at 0.91–1.92 mmol/L, and LDL at 0–3.64 mmol/L.
Statistical Analysis
All of the data in this study were entered into the Statistical Package for Social Science version 25 (SPSS Inc., Chicago, IL, USA). All of the p-values were based on a two-tailed test with a significance cutoff set at the 0.05 level. For descriptive analysis, continuous variables are described as the means ± standard deviations, whereas dichotomous variables are described as numbers and frequencies. One-sample t-tests or chi-square tests were used to assess the magnitude of the differences between groups for continuous or dichotomous variables. Additionally, univariate or multivariate logistic regression analysis was employed to assess the association between different levels of thyroid function measurements and the corresponding risk of HHCy.
Results
General Characteristics of the Subjects
This retrospective study included 775 participants, of whom 98 had serum HCy levels greater than the reference value. The general profile of subjects with or without HHCy was analyzed. As shown in Table 1, the age of the patients with HHCy was significantly higher than that of the control group, and the frequency of smoking and drinking was also significantly higher in the HHCy group. Additionally, patients with HHCy generally had significantly higher BMI and BP values, as well as a higher prevalence of dyslipidemia and blood lipid concentrations.
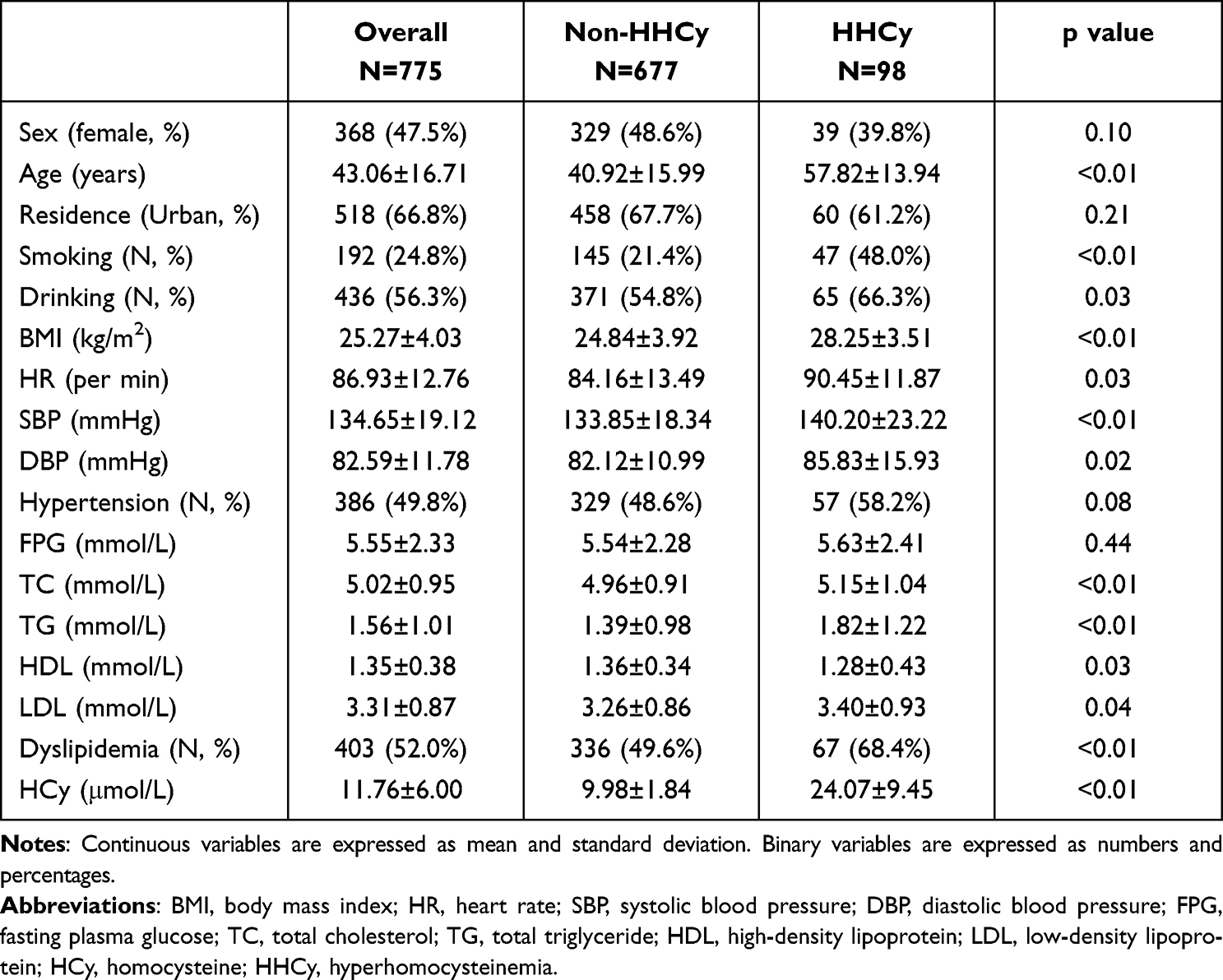 |
Table 1 General Characteristics of the Subjects |
Thyroid Function Measurements in HHCy and Non-HHCy Subjects
As shown in Table 2, we compared the serum thyroid function test results between patients with and without HHCy. The serum TSH levels of patients with HHCy were significantly higher than those without (1.65 ± 0.90 vs 2.10 ± 1.06 mIU/L, p < 0.01). Moreover, the serum TPOAb-positive rate was significantly higher in patients with HHCy (10.0% vs 19.4%, p < 0.01). However, there was no significant difference in serum FT3 and FT4 levels and TgAb-positive rates between the two groups.
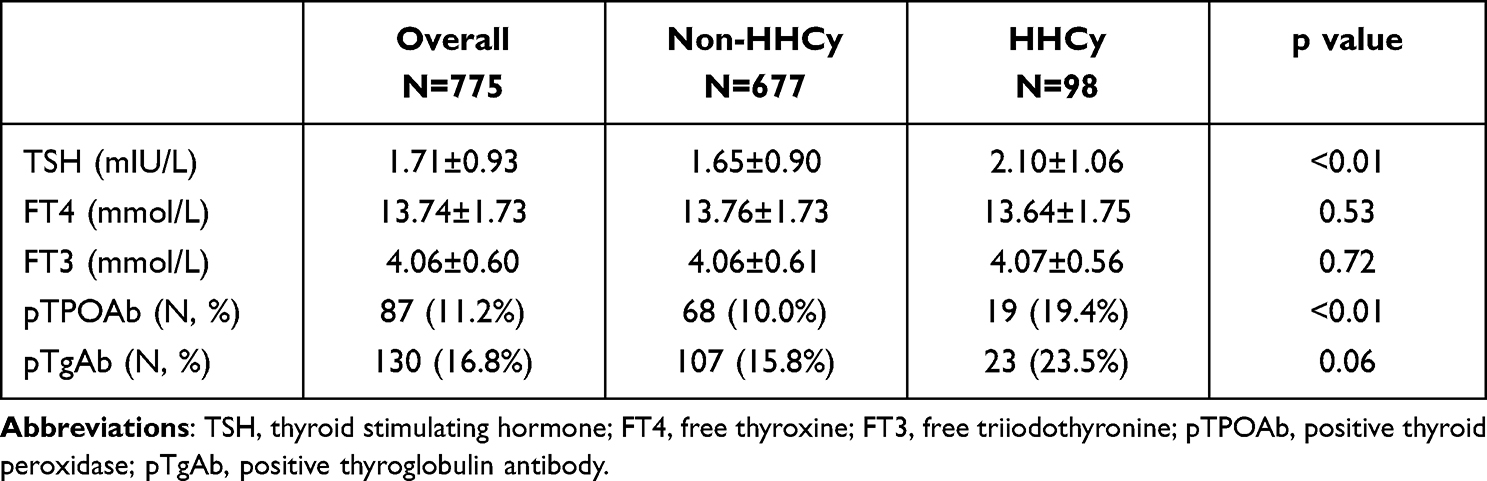 |
Table 2 Thyroid Indicators Corresponding to Subjects with or without HHCy |
Serum HCy Levels and HHCy Prevalence Corresponding to Different Levels of Thyroid Function
Serum TSH, FT4, and FT3 were divided into four quartiles, and the serum HCy levels were compared among the four subgroups. As shown in Table 3, the HCy level showed a significant increasing trend with increasing serum TSH within the reference interval among the four subgroups (p for trend < 0.01). Moreover, comparing the serum HCy concentrations between the TPOAb- and TgAb-positive and -negative groups, the HCy level of TPOAb-positive subjects was significantly higher than that of TPOAb-negative subjects (14.06 ± 8.89 vs 11.48 ± 5.47, p < 0.01). However, HCy showed no significant increasing or decreasing trend with the increase in serum FT4 or FT3. The HCy levels were also comparable between the TgAb-positive and -negative subgroups.
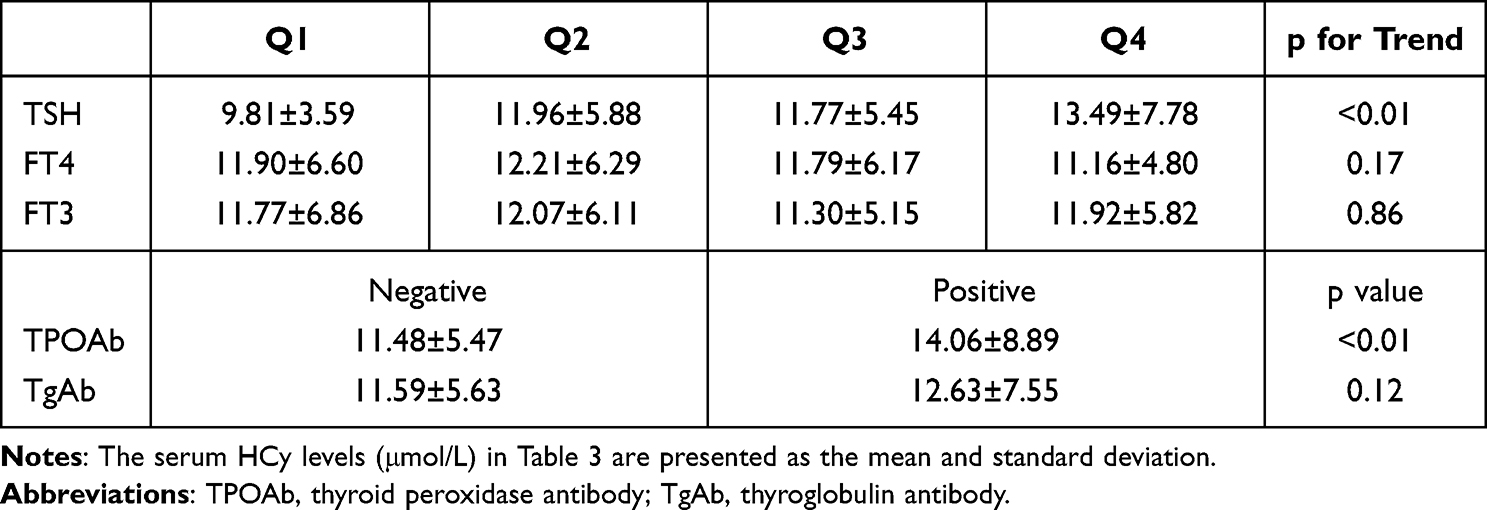 |
Table 3 HCy Levels in Subgroups with Different Quartiles of TSH, FT4, FT3, and Positive or Negative TPOAb and TgAb |
Similarly, as shown in Table 4, with the gradual increase in serum TSH within the reference interval, the prevalence of HHCy also showed a significant increasing trend, from 5.7% in the Q1 subgroup to 19.1% in the Q4 subgroup (p for trend < 0.01). Additionally, the prevalence of HHCy was significantly higher in TPOAb-positive patients (21.8% vs 11.5%, p < 0.01).
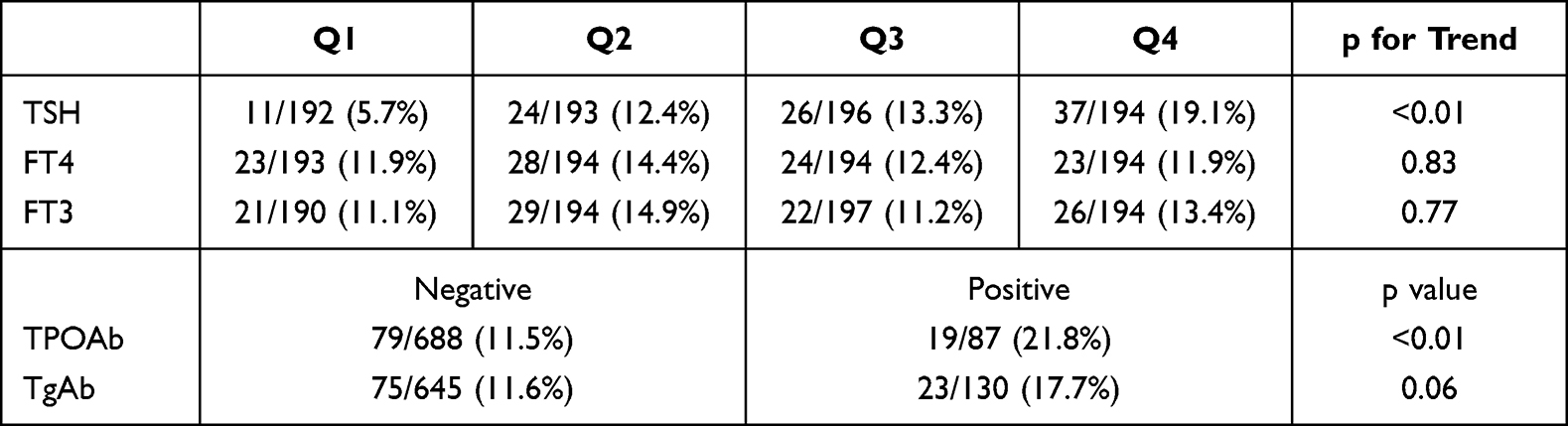 |
Table 4 HHCy Prevalence in Subgroups with Different Quartiles of TSH, FT4, FT3, and Positive or Negative TPOAb and TgAb |
Association of Serum TSH and TPOAb Changes with HCy Levels and HHCy Prevalence
The above results suggested that HCy levels and HHCy risk may be related to variations in serum TSH and TPOAb. As shown in Table 5, we used univariate and multivariate regression analyses to explore the association of TSH and TPOAb with HCy levels and HHCy risk. After adjusting for confounding factors, we found that the serum TSH levels in the Q2, Q3, and Q4 intervals were independent risk factors for elevated HCy levels compared to those in Q1. Moreover, TSH within the Q4 interval was an independent risk factor for increased HHCy risk [OR: 3.440, 95% CI (1.511, 7.832), p < 0.05]. After adjusting for confounding factors, the results of regression analysis suggested that TSH (with per SD increase) was also significantly positively correlated with HCy levels (1.414 ± 0.199, p < 0.05) and HHCy prevalence [OR: 1.706, 95% CI (1.315, 2.214), p < 0.05].
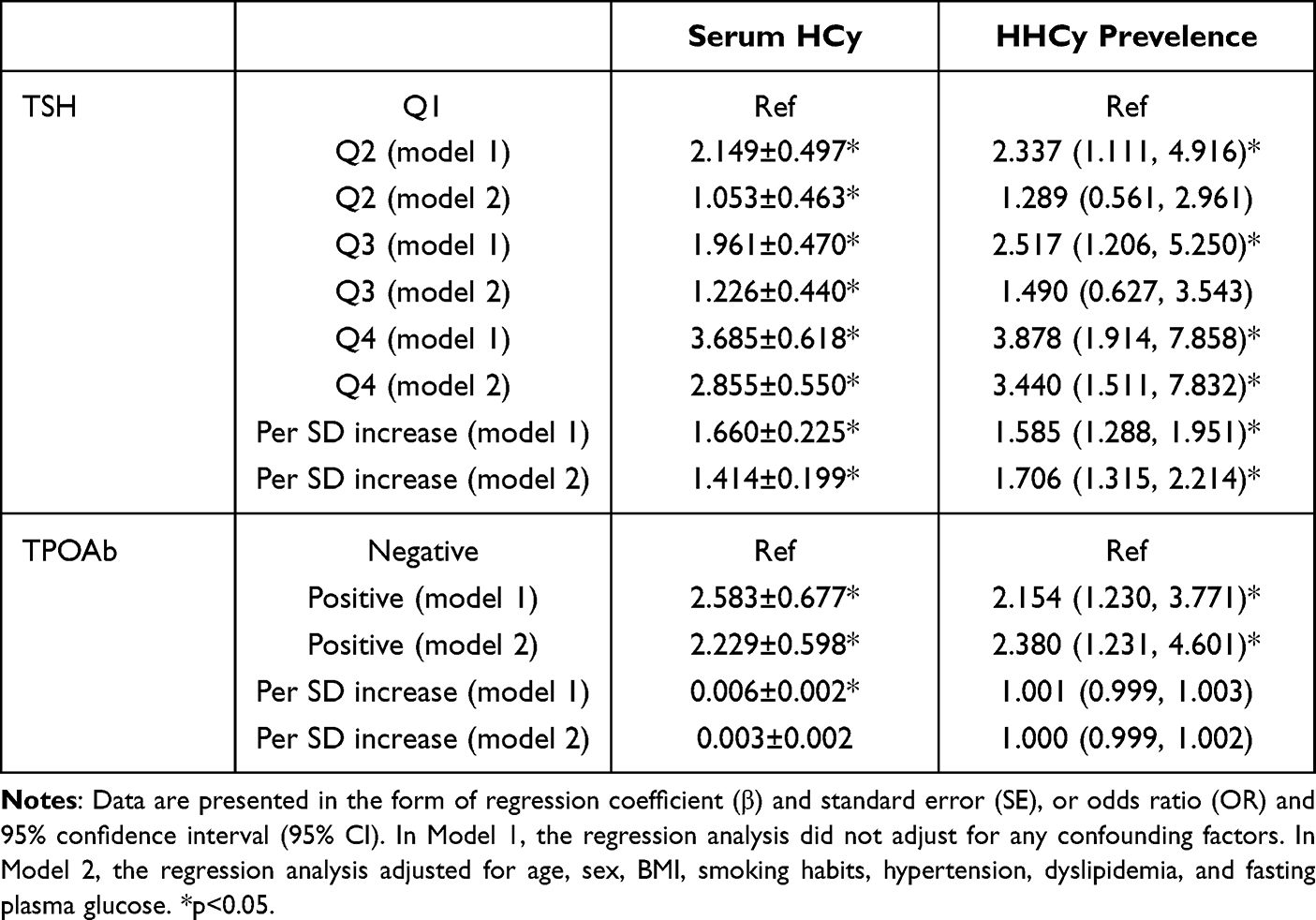 |
Table 5 Regression Analysis Between Serum TSH and TPOAb Measurements and Serum HCy Level or HHCy Prevalence |
The effects of positive TPOAb and linear elevation of TPOAb on HCy were also analyzed. After adjusting for confounders, TPOAb positivity was found to be an independent risk factor for elevated HCy (2.229 ± 0.598, p < 0.05) and HHCy risk [OR: 2.380, 95% CI (1.231, 4.601), p < 0.05]. However, as the TPOAb titers increased, we found no significant association with HCy levels or HHCy risk.
Discussion
This retrospective study based on a HIS found that patients with HHCy had significantly higher TSH levels and positive rates of TPOAb compared to non-HHCy subjects in a population with euthyroid function. Additionally, the HCy level and HHCy prevalence showed a significant upward trend with the increase in TSH in the reference interval. HCy levels and HHCy prevalence were also significantly higher in TPOAb-positive patients than in TPOAb-negative subjects. Multivariate regression analyses confirmed that higher TSH levels were an independent risk factor for elevated HCy levels and HHCy risk compared to subjects with lower TSH, and that TPOAb positivity was also an independent risk factor for elevated HCy levels and HHCy risk. However, we found no significant association between a linear increase in TPOAb titers and HCy levels or HHCy risk. Based on the above results, we speculate that there is a permissibility relationship between TPOAb and HCy. In other words, only when the titer of TPOAb reaches a certain degree, will the correlation between it and HCy show a significant effect. However, more prospective cohort studies are required to confirm this conjecture.
Despite many previous studies on thyroid function and HCy or HHCy, few have been conducted in euthyroid subjects. The association between overt thyroid dysfunction and HCy is expected given that overt thyroid dysfunction is a recognized risk factor for cardiometabolic abnormalities. It has long been known that overt hyperthyroidism decreases HCy and overt hypothyroidism (OH) increases HCy. Indeed, Zhou et al reported in a meta-analysis that plasma HCy concentrations were significantly higher in patients with OH than in healthy controls and SCH. Moreover, HCy levels decreased significantly after levothyroxine treatment in patients with OH or SCH.21 In another meta-analysis, Zhang et al found significantly higher HCy levels in patients with SCH compared to euthyroid subjects. Moreover, these results remained significant after subgroup analysis based on age, sex, and the magnitude of serum TSH elevation.19 Some basic studies have revealed the underlying mechanisms responsible for the association between serum HCy levels and thyroid dysfunction. The expression and activity of methylene tetrahydrofolate reductase (MTHFR), a key enzyme in folate-dependent re-methylation, has been shown to be significantly decreased in thyroidectomy rats, suggesting dysregulation of HCy metabolism in individuals with hypothyroidism.22–24 In comparison, the number of studies on hyperthyroidism and HCy is relatively small, and no secondary studies have been reported at present. Several European case-control studies with small samples have found that HCy levels in patients with hyperthyroidism were significantly lower than those in healthy controls. Moreover, HCy levels have been shown to increase after treatment with antithyroid drugs.18,25–27 These results go some way to explain our finding that changes in thyroid function are risk factors for HCy abnormalities and that HCy levels or HHCy risk increase significantly with the increase of TSH. However, previous studies on thyroid function within the reference interval and HCy levels are rare, and no previous studies have explored the association between thyroid function test results and HCy or HHCy levels. A recent cross-sectional study in China analyzed the association between central sensitivity parameters of thyroid hormone and HCy. After excluding patients with known thyroid abnormalities, the researchers found that the thyroid feedback quantile-based index (TFQI), Chinese-referenced parametric TFQI (PTFQI), TSH index (TSHI), and thyrotropin thyroxine resistance index (TT4RI) were independent risk factors for the increase in HCy. These results suggest that the decreased central sensitivity of thyroid hormone leads to an increase in HCy.28 Individuals with elevated TSH with no, or slightly reduced FT4 are common in clinical practice, which is in fact a manifestation of decreased central sensitivity to thyroid hormone. Our results showed that the TSH levels in the HHCy group were significantly higher than those in the control group, while the FT4 and FT3 levels were comparable to those in the control group. Moreover, HHCy was significantly correlated with TSH but not with FT4 or FT3, which explained Ding et al’s finding that the increase in HCy caused by the increase in TSH may be due to the impaired central sensitivity of thyroid hormone. As we found no clear association between FT4 or FT3 and HCy in this study, we hypothesize that the increased TSH in the HHCy group of subjects with euthyroid function is more due to impaired central thyroid hormone sensitivity than to reduced thyroid function. However, more basic research is needed to confirm this hypothesis.
As thyroid autoimmunity is the most common cause of elevated serum TSH, and given that our results suggested a significant positive association between TSH and HCy, it is reasonable to suspect that thyroid autoantibodies may also be associated with HCy. In addition to patients with HT, many patients with autoimmune diseases, such as systemic lupus erythematosus (SLE), Behcet’s disease, and rheumatoid arthritis (RA), whose pathogenic mechanisms are diverse, have a significantly increased risk of cardiovascular events, manifested by elevated HCy.29–31 HCy may be used as an indicator of dyslipidemia, kidney damage, and skin involvement in patients with SLE.32 Moreover, a previous study found significantly higher levels of HCy in patients with active Behcet’s disease than in healthy controls, and HCy was positively correlated with the degree of disease activity in multiple organs, such as uveitis.33 Furthermore, patients with RA with a long course of disease, high range of motion, severe joint destruction, treatment with metrediol, and the elderly should be closely monitored for HCy changes and their damaging effects on the cardiovascular system.34 Additionally, if thyroid autoantibodies are positive for either hyperthyroidism or hypothyroidism, the subject will have a significantly higher risk of cardiometabolic disease and high HCy levels. A recent cross-sectional study revealed that TPOAb is independently and positively associated with HCy levels in patients with Graves’ disease (GD). TPOAb may also be associated with the cardiovascular risk of patients with GD through its effect on HCy.35 Similar to hyperthyroidism, the results of an Italian cross-sectional study suggested that patients with iatrogenic hypothyroidism combined with HT had significantly higher serum HCy levels than non-HT patients.36 Moreover, in a cross-sectional study in Taiwan, where participants were not screened for serum TSH beforehand, the researchers evaluated the association between thyroid autoantibodies and HCy. The results suggested that serum HCy levels were significantly higher in TPOAb-positive patients, which is similar to the findings of the current study.37 We also found that patients with HHCy had a higher positive rate of TPOAb, and that positive TPOAb was an independent risk factor for elevated HCy or HHCy. However, neither the HCy levels nor HHCy risk strictly increased with TPOAb titers, indicating that there was no linear association between the two. Linear increases in TPOAb may not accurately predict HHCy risk. We hypothesize that it is only when TPOAb reaches a certain level that it is necessary to monitor the risk of HT in a timely manner. However, due to the lack of relevant previous evidence, the above hypothesis needs to be confirmed by more prospective cohort studies with large samples.
The current study has some shortcomings that warrant discussion. First, cross-sectional studies do not produce causal associations between individual variables. Second, as all of the included subjects were from a HIS, the results may have some level of selection bias. Third, many changes in lifestyle habits may have a significant impact on diet, which in turn affects serum homocysteine. Since this study is a retrospective study based on HIS, we did not have access to more demographic information, such as family income, education level, and ethnicity.
Conclusion
The serum TSH level and TPOAb-positive rate were significantly higher in patients with HHCy. Serum TSH and positive TPOAb levels were independent risk factors for elevated HCy levels and elevated HHCy risk. As there may not be a linear association between TPOAb and HCy, we consider it valuable to monitor subjects’ HT risk only when TPOAb is elevated to a certain level.
Data Sharing Statement
The data used during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was performed following the approval of the institutional review board at the Medical Science Research Ethics Committee of the First Hospital of China Medical University and the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent for Publication
The authors hereby confirm that neither the manuscript nor any part of it has been published or is being considered for publication elsewhere. We acknowledge that all authors participated sufficiently in the work and take public responsibility for its content.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflict of interests.
References
1. Li Y, Teng D, Ba J, et al. Efficacy and safety of long-term universal salt iodization on thyroid disorders: epidemiological evidence from 31 Provinces of Mainland China. Thyroid. 2020;30(4):568–579. doi:10.1089/thy.2019.0067
2. Baumgartner C, da Costa BR, Collet TH, et al. Thyroid function within the normal range, subclinical hypothyroidism, and the risk of atrial fibrillation. Circulation. 2017;136(22):2100–2116. doi:10.1161/CIRCULATIONAHA.117.028753
3. Chaker L, Baumgartner C, Ikram MA, et al. Subclinical thyroid dysfunction and the risk of stroke: a systematic review and meta-analysis. Eur J Epidemiol. 2014;29(11):791–800. doi:10.1007/s10654-014-9946-8
4. Denicoff KD, Joffe RT, Lakshmanan MC, Robbins J, Rubinow DR. Neuropsychiatric manifestations of altered thyroid state. Am J Psychiatry. 1990;147(1):94–99.
5. Kotwal A, Cortes T, Genere N, et al. Treatment of thyroid dysfunction and serum lipids: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2020;105(12):12. doi:10.1210/clinem/dgaa672
6. Rong F, Dai H, Wu Y, et al. Association between thyroid dysfunction and type 2 diabetes: a meta-analysis of prospective observational studies. BMC Med. 2021;19(1):257. doi:10.1186/s12916-021-02121-2
7. Chubb SAP, Peters KE, Bruce DG, Davis WA, Davis TME. The relationship between thyroid dysfunction, cardiovascular morbidity and mortality in type 2 diabetes: the Fremantle Diabetes Study Phase II. Acta Diabetol. 2022;59(12):1615–1624. doi:10.1007/s00592-022-01969-x
8. Laulund AS, Nybo M, Brix TH, Abrahamsen B, Jorgensen HL, Hegedus L. Duration of thyroid dysfunction correlates with all-cause mortality. the OPENTHYRO Register Cohort. PLoS One. 2014;9(10):e110437. doi:10.1371/journal.pone.0110437
9. Wang Y, Guo P, Liu L, Zhang Y, Zeng P, Yuan Z. Mendelian randomization highlights the causal role of normal thyroid function on blood lipid profiles. Endocrinology. 2021;162(5):bqab037. doi:10.1210/endocr/bqab037
10. Dalila N, Frikke-Schmidt R, Nordestgaard BG, Tybjaerg-Hansen A. Plasma TSH and cardiovascular disease in the general population: a Mendelian randomization study of 105,224 individuals. Atherosclerosis. 2023;376:26–33. doi:10.1016/j.atherosclerosis.2023.05.018
11. Zhou W, Brumpton B, Kabil O, et al. GWAS of thyroid stimulating hormone highlights pleiotropic effects and inverse association with thyroid cancer. Nat Commun. 2020;11(1):3981. doi:10.1038/s41467-020-17718-z
12. Zhao L, Teng D, Shi X, et al. The effect of increased iodine intake on serum thyrotropin: a cross-sectional, Chinese nationwide study. Thyroid. 2020;30(12):1810–1819. doi:10.1089/thy.2019.0842
13. Biondi B, Cappola AR, Cooper DS. Subclinical hypothyroidism: a review. JAMA. 2019;322(2):153–160. doi:10.1001/jama.2019.9052
14. Kim HJ, Park SJ, Park HK, Byun DW, Suh K, Yoo MH. Thyroid autoimmunity and metabolic syndrome: a nationwide population-based study. Eur J Endocrinol. 2021;185(5):707–715. doi:10.1530/EJE-21-0634
15. Han L, Liu Y, Wang C, et al. Determinants of hyperhomocysteinemia in healthy and hypertensive subjects: a population-based study and systematic review. Clin Nutr. 2017;36(5):1215–1230. doi:10.1016/j.clnu.2016.11.011
16. Yang B, Fan S, Zhi X, et al. Prevalence of hyperhomocysteinemia in China: a systematic review and meta-analysis. Nutrients. 2014;7(1):74–90. doi:10.3390/nu7010074
17. Hermann A, Sitdikova G. Homocysteine: biochemistry, molecular biology and role in disease. Biomolecules. 2021;11(5):737. doi:10.3390/biom11050737
18. Orzechowska-Pawilojc A, Siekierska-Hellmann M, Syrenicz A, Sworczak K. Homocysteine, folate, and cobalamin levels in hyperthyroid women before and after treatment. Endokrynol Pol. 2009;60(6):443–448.
19. Zhang SF, Li LZ, Zhang W, et al. Association between plasma homocysteine levels and subclinical hypothyroidism in adult subjects: a meta-analysis. Horm Metab Res. 2020;52(9):625–638. doi:10.1055/a-1199-2633
20. Yang N, Yao Z, Miao L, et al. Novel clinical evidence of an association between homocysteine and insulin resistance in patients with hypothyroidism or subclinical hypothyroidism. PLoS One. 2015;10(5):e0125922. doi:10.1371/journal.pone.0125922
21. Zhou Y, Chen Y, Cao X, Liu C, Xie Y. Association between plasma homocysteine status and hypothyroidism: a meta-analysis. Int J Clin Exp Med. 2014;7(11):4544–4553.
22. Ayav A, Alberto JM, Barbe F, et al. Defective remethylation of homocysteine is related to decreased synthesis of coenzymes B2 in thyroidectomized rats. Amino Acids. 2005;28(1):37–43. doi:10.1007/s00726-004-0151-z
23. Nair CP, Viswanathan G, Noronha JM. Folate-mediated incorporation of ring-2-carbon of histidine into nucleic acids: influence of thyroid hormone. Metabolism. 1994;43(12):1575–1578. doi:10.1016/0026-0495(94)90019-1
24. Chan MM, Stokstad EL. Metabolic responses of folic acid and related compounds to thyroxine in rats. Biochim Biophys Acta. 1980;632(2):244–253. doi:10.1016/0304-4165(80)90082-3
25. Demirbas B, Ozkaya M, Cakal E, et al. Plasma homocysteine levels in hyperthyroid patients. Endocr J. 2004;51(1):121–125. doi:10.1507/endocrj.51.121
26. Nedrebo BG, Hustad S, Schneede J, et al. Homocysteine and its relation to B-vitamins in Graves’ disease before and after treatment: effect modification by smoking. J Intern Med. 2003;254(5):504–512. doi:10.1046/j.1365-2796.2003.01222.x
27. Diekman MJ, van der Put NM, Blom HJ, Tijssen JG, Wiersinga WM. Determinants of changes in plasma homocysteine in hyperthyroidism and hypothyroidism. Clin Endocrinol. 2001;54(2):197–204. doi:10.1046/j.1365-2265.2001.01170.x
28. Ding X, Wang Y, Liu J, Wang G. Impaired sensitivity to thyroid hormones is associated with elevated homocysteine levels in the euthyroid population. J Clin Endocrinol Metab. 2022;107(9):e3731–e3737. doi:10.1210/clinem/dgac371
29. van Ede AE, Laan RF, Blom HJ, et al. Homocysteine and folate status in methotrexate-treated patients with rheumatoid arthritis. Rheumatology. 2002;41(6):658–665. doi:10.1093/rheumatology/41.6.658
30. Merashli M, Bucci T, Pastori D, et al. Plasma homocysteine in Behcet’s disease: a systematic review and meta-analysis. Thromb Haemost. 2022;122(7):1209–1220. doi:10.1055/s-0041-1740637
31. Stojan G, Li J, Liu T, Kane MA, Petri MA. Intracellular homocysteine metabolites in SLE: plasma S-adenosylhomocysteine correlates with coronary plaque burden. Lupus Sci Med. 2021;8(1):e000453. doi:10.1136/lupus-2020-000453
32. Tsai TY, Lee TH, Wang HH, Yang TH, Chang IJ, Huang YC. Serum homocysteine, folate, and vitamin B(12) levels in patients with systemic lupus erythematosus: a meta-analysis and meta-regression. J Am Coll Nutr. 2021;40(5):443–453. doi:10.1080/07315724.2020.1788472
33. Shadmanfar S, Shahram F, Nadji A, et al. The relationship between plasma homocysteine level and HLA-B51 in patients with Behcet’s disease: a case-control study. Int J Rheum Dis. 2014;17(4):466–470. doi:10.1111/1756-185X.12271
34. Figus FA, Piga M, Azzolin I, McConnell R, Iagnocco A. Rheumatoid arthritis: extra-articular manifestations and comorbidities. Autoimmun Rev. 2021;20(4):102776. doi:10.1016/j.autrev.2021.102776
35. Li F, Aji G, Wang Y, Lu Z, Ling Y. Thyroid peroxidase antibody is associated with plasma homocysteine levels in patients with Graves’ disease. Exp Clin Endocrinol Diabetes. 2020;128(1):8–14. doi:10.1055/a-0643-4692
36. Cicone F, Santaguida MG, My G, et al. Hyperhomocysteinemia in acute iatrogenic hypothyroidism: the relevance of thyroid autoimmunity. J Endocrinol Invest. 2018;41(7):831–837. doi:10.1007/s40618-017-0811-y
37. Wang YP, Lin HP, Chen HM, Kuo YS, Lang MJ, Sun A. Hemoglobin, iron, and vitamin B12 deficiencies and high blood homocysteine levels in patients with anti-thyroid autoantibodies. J Formos Med Assoc. 2014;113(3):155–160. doi:10.1016/j.jfma.2012.04.003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.