Back to Journals » International Journal of General Medicine » Volume 16
Association Between Serum Irisin Levels and ST-Segment Elevation Myocardial Infarction
Authors Ozturk D, Melekoglu A ![]() , Altinbilek E, Calik M
, Altinbilek E, Calik M ![]() , Kosem A, Kilci H, Misirlioglu NF, Uzun H
, Kosem A, Kilci H, Misirlioglu NF, Uzun H ![]()
Received 20 January 2023
Accepted for publication 12 April 2023
Published 17 April 2023 Volume 2023:16 Pages 1355—1362
DOI https://doi.org/10.2147/IJGM.S403564
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Derya Ozturk,1 Adem Melekoglu,1 Ertugrul Altinbilek,1 Mustafa Calik,2 Arzu Kosem,3 Hakan Kilci,4 Naile Fevziye Misirlioglu,5 Hafize Uzun6
1Sisli Hamidiye Etfal Education and Research Hospital, Department of Emergency, İstanbul, Turkey; 2Gaziosmanpasa Education and Research Hospital, Department of Emergency, İstanbul, Turkey; 3Ministry of Health Ankara City Hospital, Clinical Biochemistry Laboratory, Ankara, Turkey; 4Sisli Hamidiye Etfal Education and Research Hospital, Department of Cardiology, Istanbul, Turkey; 5University of Health Sciences, Gaziosmanpaşa Training and Research Hospital, Department of Biochemistry, Istanbul, Turkey; 6Istanbul Atlas University, Faculty of Medicine, Department of Medical Biochemistry, Istanbul, Turkey
Correspondence: Mustafa Calik, Gaziosmanpasa Education and Research Hospital, Emergency Department, İstanbul, 34255, Turkey, Email [email protected]
Background: An acute ST-elevation myocardial infarction (STEMI) is a serious cardiovascular condition with a high risk of morbidity and mortality. Irisin is adipomyokine that is associated with various health conditions. In post-STEMI, elevated serum irisin levels are associated with more adverse cardiovascular events.
Objective: The purpose of this study was to investigate associations between the serum irisin levels and acute MI (AMI) and whether irisin may be a useful biomarker for severity of AMI in patients with STEMI. Possible correlations between serum irisin and cardiac troponin-I (cTi) levels were investigated.
Methods: A total of 90 subjects (46 control subjects and 44 STEMI patients) were included in the study. Besides demographic data, presence of diabetes mellitus and hypertension, electrocardiography (ECG) findings, blood biochemistry, cardiac biomarkers (cTi) and serum irisin levels were examined.
Results: Significantly lower heart rate (HR) and significantly higher ST-elevation and QTc interval were detected in ECG recordings in STEMI patients (p < 0.05). Serum irisin levels were significantly lower in STEMI patients compared to the control subjects (p < 0.001). The decrease in the serum irisin levels was significantly correlated with the increase in cTi levels, as well as increased QTc (p < 0.05). The sensitivity and specificity of irisin were found to be 93% and 78%, respectively.
Conclusion: Decreased irisin levels were found to be highly predictive in STEMI. In patients with STEMI, the serum irisin levels were associated with cTi levels and QTc, suggesting that irisin is a promising biomarker for AMI cases.
Keywords: myocardial infarction, cardiovascular diseases, irisin, troponin-I, QT interval, biomarker
Introduction
Myocardial infarction (MI) is among the main risk factors for heart failure.1,2 Acute ST-elevation MI (STEMI) occurs when one or more coronary arteries are occluded that leads to transmural myocardial ischemia resulting in myocardial injury or necrosis.3 Regardless of the advances in the management of STEMI including pharmacological and surgical approaches, there are still areas to be clarified and improved.4
Irisin, a 112 amino acid-long peptide, is an adipomyokine that is cleaved from a plasma membrane protein, fibronectin type III domain containing protein 5 (FNDC-5).5 Previous studies have reported that irisin exerts beneficial effects such as exerting anti-inflammatory6 and anti-oxidant activities,7 as well as improving glucose and lipid metabolism.8 On the other hand, higher levels of irisin were found to be associated with obesity and metabolic syndrome, suggesting muscular resistance to irisin,9,10 the fact of which is similar to the conditions of leptin resistance in obesity and insulin resistance in diabetes.11
Irisin has been shown to play different roles in cardiovascular conditions. Irisin was shown to be protective against pressure-overload cardiac hypertrophy via induction of autophagy.12 Moreover, irisin is beneficial against ischemia/reperfusion injury both in vitro and in vivo.13 Endothelial dysfunction and endothelial cell apoptosis were found to be alleviated by irisin.7,14 Infarct size was reduced, and cardiac function was improved by irisin treatment in post-MI mouse hearts via increased angiogenesis.15 Skeletal and myocardial irisin levels are elevated in rats after MI,16 while in humans, serum and saliva levels of irisin are diminished after acute MI (AMI).17
The above-mentioned effects and functions of irisin and the potential relationship between irisin and atherosclerotic cardiovascular disease are insufficient and controversial.12–21 Therefore, this study aimed to investigate associations between the circulating irisin levels and MI and whether irisin levels may be a useful biomarker for the severity of MI in patients with STEMI.
Materials and Methods
Subjects and Study Design
The protocol for sample collection was prospectively approved by the University of Health Sciences, Sisli Hamidiye Etfal Education and Research Hospital, Clinical Research Ethics Committee (date: 28.01.2020, no: 2648). We conducted in this single center cross-sectional study between February 2020 and June 2020. The study was performed in accordance with the 1975 Helsinki Declaration, updated in 2013. All participants were informed of the study protocol, and their written informed consents were obtained.
A total of 90 subjects (healthy control = 46 and STEMI = 44) were included in the study. STEMI diagnosis was made according to the third universal definition of MI document.22
Inclusion Criteria
Patients with STEMI were admitted to the emergency room and healthy volunteers who were 18 years old or older were included. The healthy volunteers consisted of hospital personnel who were subjected to annual routine control examinations. Patients with STEMI were required to have (1) continuous chest pain upon presentation, refractory to nitrates, and lasting >30 min; (2) ST-segment elevation of >0.2 mV in >2 contiguous precordial leads, or >0.1 mV in >2 contiguous limb leads, or new (or presumably new) left bundle branch block on admission electrocardiogram; (3) presentation within the first 12 h from index pain. Patients with NSTEMI were required to have angina-like chest pain at rest in the last 24 h lasting >5 min, with associated ST-segment depression of >0.1 mV in >2 contiguous leads upon presentation.
Exclusion Criteria
Patients were younger than 18 years, with a known history of heart failure or left ventricular diastolic dysfunction, coronary artery disease, atrial fibrillation and/or cerebrovascular disease, peripheral artery disease, chronic renal failure, and malignancy, and had ongoing infectious disease, and chronic inflammatory disease were excluded from the study.
Demographic data (age, gender and body weight), presence of diabetes mellitus (DM), hypertension (HT), and smoking status of the subjects were recorded on admission. Blood pressure (BP), heart rate (HR), time to onset of chest pain, elevation in electrocardiography (ECG), QT interval was measured. The vein that was involved and angiography were performed on were also recorded in STEMI patients.
Laboratory Tests
Venous blood was drawn from each patient in the biochemistry tube within the first 24 hours of the emergency department admission. Serum samples were obtained after at least 30 min of clotting by centrifugation at 2.500g for 15 min and were stored at −80 C until assayed for determination of irisin concentrations. All icteric or hemolyzed blood samples were discarded. All parameters were analyzed in all samples together in a single batch.
Fasting blood sugar, urea, creatinine, cardiac troponin-I (cTi), total cholesterol (TC), high-density lipoprotein (HDL), low-density lipoprotein (LDL), total glyceride (TG), levels were measured with an automated analyzer (COBAS 8000, ROCHE-2007, Tokyo, Japan).
Measurement of Serum Irisin Levels
Serum irisin levels were measured according to manufacturer’s instructions (Human Irisin ELISA Kit, Cat. No: YLA1361HU; YL Biont). The coefficients of intra and inter-assay variation were 7.6% (n = 25) and 9.5% (n = 25), respectively.
Statistical Analysis
The Statistical Package for Social Sciences (SPSS) for Windows, Version 22 (IBM, Armonk, NY, USA) was used for the statistical analyses. The Kolmogorov–Smirnov test was used to analyze the distribution of the variables. Data with were either expressed as mean ± standard deviation (SD) or median, minimum and maximum. Unpaired Student’s t-test was used for parameters that were normally distributed and the data without normal distribution were evaluated with Mann–Whitney U-test. Associations between the groups were investigated by Fisher’s exact test. Correlations between numerical data were investigated by using Pearson correlation coefficient test for parameters that were normally distributed, while Spearman correlation coefficient test was used for the analysis of the data that were not normally distributed. The diagnostic values of irisin, cTi and QTc variables in diagnosing AMI were determined by ROC analysis. Logistic regression analysis was performed for clinical factors and biochemical parameters thought to be associated with STEMI, and the OR and 95% confidence interval were calculated. A p < 0.05 was considered statistically significant.
Results
Age, gender, body weights and smoking status of the subjects did not differ between the STEMI patients and control subjects (Table 1). There were no differences in the number of patients with systemic HT between the groups, while the number of patients with DM was higher in STEMI patients (p = 0.034; Table 1). The number of patients who developed angina pectoris was significantly higher in STEMI patients (p = 0.031) Table 1). Most of the patients underwent prior percutaneous coronary intervention in STEMI group (Table 1). On the other hand, none of the subjects had a history of coronary artery bypass graft.
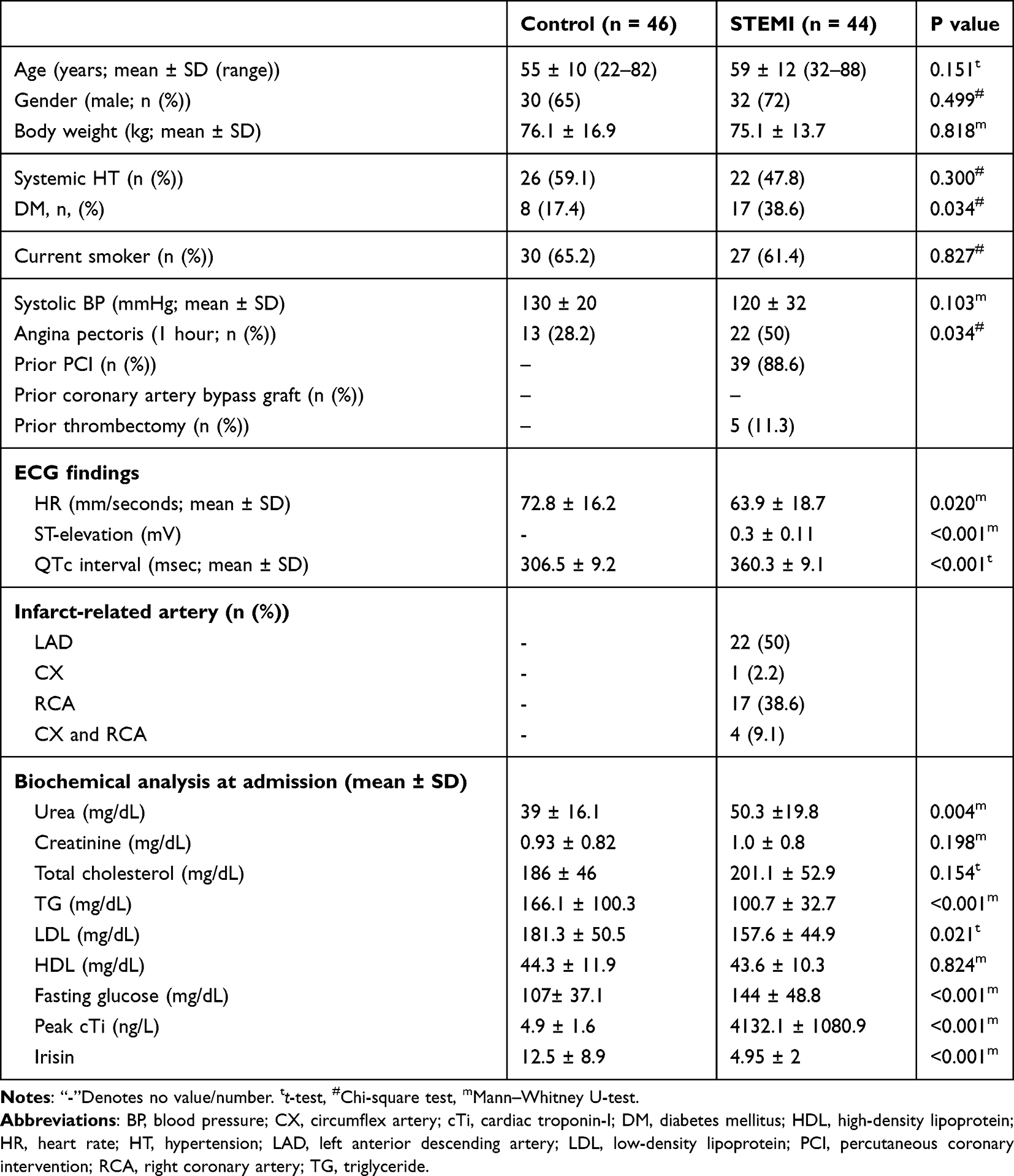 |
Table 1 Baseline Demographics, Characteristics, and Comorbidities of the Subjects |
ECG findings revealed significantly lower HR and significantly higher ST-elevation and QTc interval in STEMI patients (p < 0.05) (Table 1). Most of the infarct-related artery was found as left anterior descending artery (LAD) followed by right coronary artery (RAC) (Table 1).
Urea, fasting glucose and peak cTi levels were significantly higher (p < 0.01), while TG, LDL levels were significantly lower in STEMI patients compared to control subjects (p < 0.05) (Table 1).
Serum irisin levels were found to be significantly lower in the AMI patients compared to control subjects (p < 0.001; Figure 1). Moreover, when there are correlations between irisin levels, peak cTi levels and QTc intervals, there is a moderately negative correlation between serum irisin levels with cTi levels (p < 0.001) and QTc interval (p < 0.05) in AMI patients (Table 2).
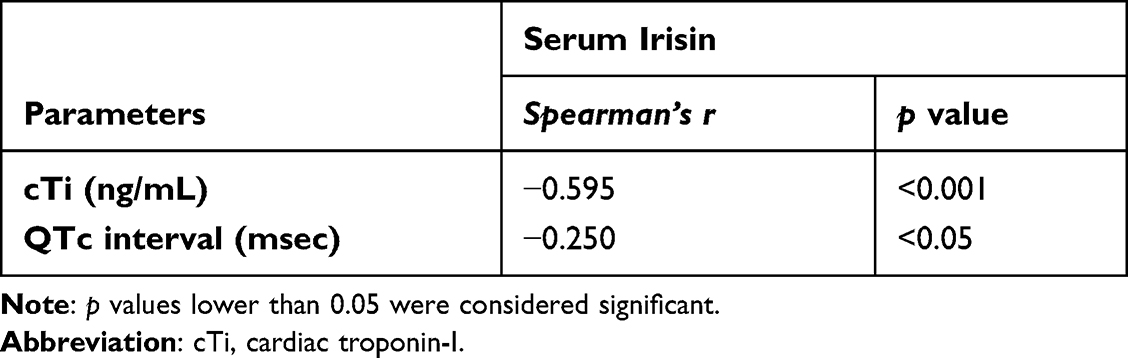 |
Table 2 Correlations Between Serum Irisin, cTi Levels and QTc Interval |
 |
Figure 1 Serum irisin levels in control subjects and AMI patients (****p<0.0001m). |
In the ROC analysis of peak cTi level for STEMI and control groups, the AUC value of 0.98 (95% CI 0.969–0.1000 and Cut off >16.5) was found to be statistically significant (p < 0.05). In the ROC analysis of QTc interval for STEMI and control groups, the AUC value of 0.71 (95% CI 0.609–0.820 and Cut off >16.5) was found to be statistically significant (p < 0.05). In the ROC analysis of the irisin level for STEMI and control groups, the AUC value of 0.93 (95% CI 0.881–0.980 and Cut off <6.71) was found to be statistically significant (p < 0.05). Decreased irisin levels were found to be highly predictive in STEMI. The sensitivity and specificity were found to be 93% and 78%, respectively (Figure 2, Table 3).
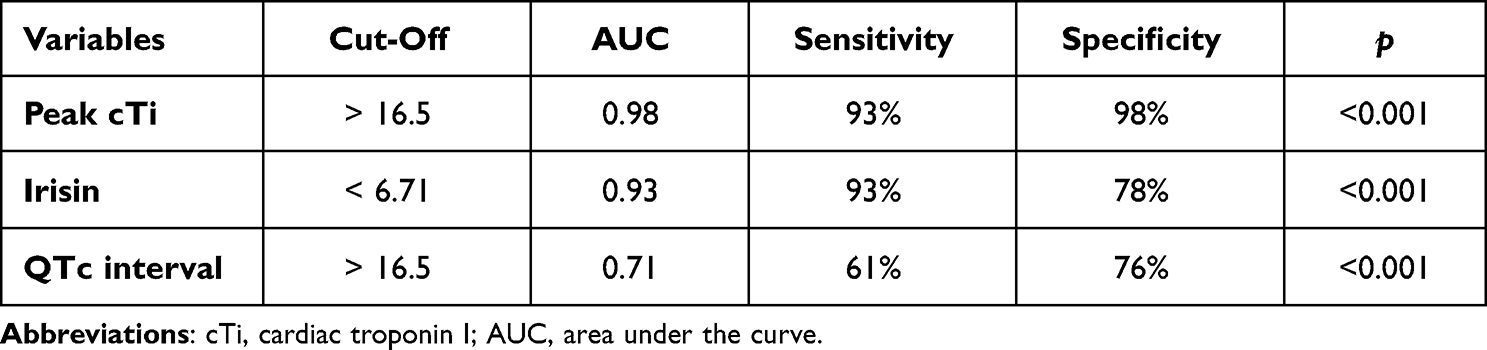 |
Table 3 Diagnostic Values of Irisin and Other Variables in All Groups |
 |
Figure 2 ROC analysis of irisin, peak cTi and QTc interval for STEMI variables and control groups. |
In the regression analysis of independent variables for the STEMI patient group, irisin, peak cTi, urea, LDL and TG variables showed significant differences in the univariate model. However, no parameter showed significant difference in the multivariate model (Table 4). cTi peaked at 0.283 (0.627–0.905). In univariate regression analysis; irisin (odds ratio [OR]: 1.047; 95% confidence interval [CI]: 1.756–4.619; p < 0.001), urea (OR: 0.037; 95% CI: 0.940–0.990; p = 0.008), LDL (OR: 0.011, 95% CI: 1.001–1.020; p = 0.011), and TG (OR: 0.022; 95% CI: 1.010–1.035; p = 0.001) were found to be factors associated with a peak cTi (STEMI patient group).
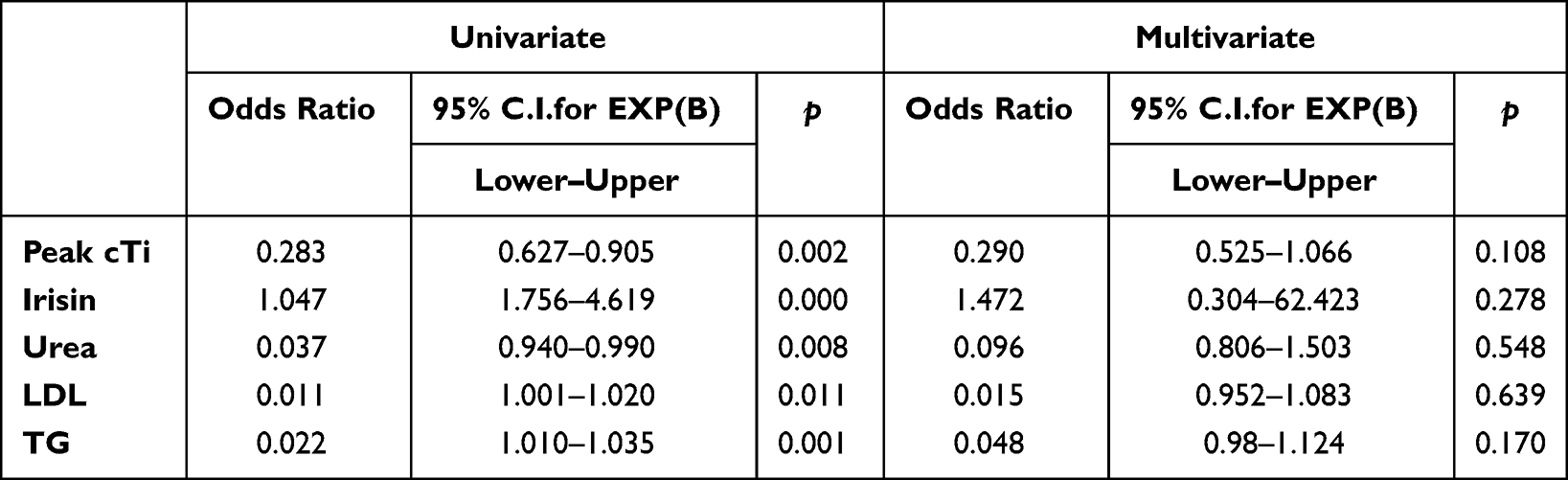 |
Table 4 Regression Analysis of Variables for STEMI |
Discussion
In this study, we demonstrated that serum irisin levels are significantly lower in STEMI patients compared to healthy control subjects and reduced irisin levels are significantly correlated with increased AMI biomarkers and cTi levels, as well as with increased QTc interval. In the differential diagnosis of AMI, cTi and irisin were found to have high sensitivity and specificity. There was also a moderate relationship between cTi and irisin in patients with STEMI. This study demonstrated a potential relationship between irisin levels and prognostic markers in patients with STEMI.
Irisin was discovered as a muscle derived hormone in response to exercise,21 while further studies reported several other tissues also produce irisin.23–25 Although irisin has been reported to be beneficial against cardiovascular events,7,12–15 elevated irisin levels were reported to be associated with adverse cardiovascular events in patients.18–20 A study reported that circulating irisin levels are not associated with acute coronary syndrome (ACS) development in healthy individuals, while elevated irisin levels are associated with major adverse cardiovascular events in patients with established coronary artery disease (CAD).18 Moreover, an inverse relation between serum irisin levels in CAD patients with stable angina was found.19 In post-STEMI patients, elevated serum irisin levels are found to be associated with adverse cardiovascular events.20 Another recent study reported reduced serum irisin levels after AMI.17
Previous studies have also shown that the potential relationship between irisin and atherosclerotic cardiovascular disease is insufficient and controversial.12–21 In current study, serum irisin levels were significantly lower in AMI patients. Irisin is also produced by cardiomyocytes at a higher amount than muscles.17 Reduced irisin levels may be explained by the fact that irisin is released into the circulation after cardiomyocyte damage from the intracellular pool, similar to the CK-MB and cTi.26 However, why irisin levels decrease after AMI still remains elusive. Another reason might be that irisin levels are decreased to limit the heat production and increase ATP synthesis in the damaged tissue. In order to repair the damaged tissue, cells require more energy than the steady state conditions.16 Irisin was previously found to induce mitochondrial thermogenesis via heat production27 and reduce ATP production.28 Heat is associated with elevated incidence of various cardiovascular diseases and may worsen the conditions related to AMI.29,30 Therefore, it is suggested that limiting irisin production may provide more energy in the damaged tissue. Moreover, reduced levels of irisin might be a protective mechanism against additional myocardial damage. Results of the experimental study of Bashar et al31 revealed a significant decrease in serum irisin in the infarct rats as compared to the control rats. Their results also showed a significant positive correlation between serum irisin level and QRS duration. Similarly, to our study, there is a negative correlation between serum irisin and troponin. They recommend regular exercise or taking recombinant irisin as a supplement to protect at-risk individuals against AMI. However, additional studies are required to clarify this issue.
cTi and CK-MB are two well-known biomarkers for the AMI diagnosis.32 Higher CK-MB levels are associated with adverse outcomes after MI.33 Elevation in cTi is also associated with adverse outcomes after MI.34,35 In our study, cTi levels were found to be significantly higher in STEMI patients compared to control subjects. Moreover, the increase in the serum irisin levels was associated with the decrease in serum cTi levels in STEMI patients. Similar to our study, decreased levels of irisin were found in association with cTi in AMI models of animals16,31 and AMI patients.17
The sensitivity of peak cTi was 93%, and the specificity was 98%; the sensitivity of irisin was 93%, specificity 78%; QTc had a sensitivity of 61% and a specificity of 76%. It was determined that serum irisin could statistically significantly distinguish patients with AMI from healthy individuals. QTc are not valuable in the diagnosis of AMI. Serum irisin performed well in distinguishing AMI from healthy volunteers, even in patients with normal QTc. The serum irisin level also appears to be a statistically strong and independent protective factor against STEMI risk and severity, according to univariate regression analysis.
Smoking is an important risk factor for heart diseases. The current study found that smoking was not statistically significant between the two groups. It is well known that smoking is an important risk factor for heart attacks. Many prospective studies show that both male and female smokers have a higher risk of myocardial infarction, recurrent heart attacks, and sudden death due to coronary artery disease. The incidence of coronary artery disease is 2–4 times higher in smokers. The risk of death from coronary artery disease is related to the number of cigarettes smoked per day, depth of inhalation, age at onset of smoking, and number of years smoked. In addition, smoking greatly affects other risk factors of coronary artery disease such as hypercholesterolemia and diabetes.36
Our study also had some limitations. First of all, the sample size was small, and studies investigating the associations between serum irisin levels in with a larger population of STEMI patients are relevant. Moreover, the patients were not followed up after discharge, and their baseline irisin levels and their association with other cardiac biomarkers were investigated.
In conclusion, this study provides evidence of a reduction in serum irisin levels in patients with STEMI. Serum irisin also maintained a higher discriminatory ability for AMI. Circulating irisin levels were found to be correlated with cTi levels. Our data indicate that irisin may be a good candidate as a biomarker for STEMI besides cTi levels.
Data Sharing Statement
The primary author must be contacted with a valid request in order to provide the data sets used in this study. The email address is [email protected].
Funding
There is no funding to report.
Disclosure
No potential conflict of interest relevant to this article was reported.
References
1. Anderson JL, Morrow DA. Acute myocardial infarction. N Engl J Med. 2017;376:2053–2064. doi:10.1056/NEJMra1606915
2. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction. J Am Coll Cardiol. 2018;72:2231–2264. doi:10.1016/j.jacc.2018.08.1038
3. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined – a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36:959–969. doi:10.1016/S0735-1097(00)00804-4
4. Ibanez B, James S, Agewall S, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2017;2018(39):119–177.
5. Arhire LI, Mihalache L, Covasa M. Irisin: a hope in understanding and managing obesity and metabolic syndrome. Front Endocrinol. 2019;10:524. doi:10.3389/fendo.2019.00524
6. Mazur-Bialy AI, Pocheć E, Anti-Inflammatory ZM. Properties of Irisin, mediator of physical activity, are connected with TLR4/MyD88 signaling pathway activation. Int J Mol Sci. 2017;18:701. doi:10.3390/ijms18040701
7. Zhu D, Wang H, Zhang J, et al. Irisin improves endothelial function in type 2 diabetes through reducing oxidative/nitrative stresses. J Mol Cell Cardiol. 2015;87:138–147. doi:10.1016/j.yjmcc.2015.07.015
8. Mo L, Shen J, Liu Q, et al. Irisin Is Regulated by CAR in liver and is a mediator of hepatic glucose and lipid metabolism. Mol Endocrinol. 2016;30:533–542. doi:10.1210/me.2015-1292
9. Park KH, Zaichenko L, Brinkoetter M, et al. Circulating irisin in relation to insulin resistance and the metabolic syndrome. J Clin Endocrinol Metab. 2013;98:4899–4907. doi:10.1210/jc.2013-2373
10. Polyzos SA, Kountouras J, Shields K, Mantzoros CS. Irisin: a renaissance in metabolism? Metabolism. 2013;62:1037–1044. doi:10.1016/j.metabol.2013.04.008
11. Moon HS, Dalamaga M, Kim SY, et al. Leptin’s role in lipodystrophic and nonlipodystrophic insulin-resistant and diabetic individuals. Endocr Rev. 2013;34:377–412. doi:10.1210/er.2012-1053
12. Li RL, Wu SS, Wu Y, et al. Irisin alleviates pressure overload-induced cardiac hypertrophy by inducing protective autophagy via mTOR-independent activation of the AMPK-ULK1 pathway. J Mol Cell Cardiol. 2018;121:242–255. doi:10.1016/j.yjmcc.2018.07.250
13. Wang H, Zhao YT, Zhang S, et al. Irisin plays a pivotal role to protect the heart against ischemia and reperfusion injury. J Cell Physiol. 2017;232:3775–3785. doi:10.1002/jcp.25857
14. Lu J, Xiang G, Liu M, Mei W, Xiang L, Dong J. Irisin protects against endothelial injury and ameliorates atherosclerosis in apolipoprotein E-Null diabetic mice. Atherosclerosis. 2015;243:438–448. doi:10.1016/j.atherosclerosis.2015.10.020
15. Liao Q, Qu S, Tang LX, et al. Irisin exerts a therapeutic effect against myocardial infarction via promoting angiogenesis. Acta Pharmacol Sin. 2019;40:1314–1321. doi:10.1038/s41401-019-0230-z
16. Kuloglu T, Aydin S, Eren MN, et al. Irisin: a potentially candidate marker for myocardial infarction. Peptides. 2014;55:85–91. doi:10.1016/j.peptides.2014.02.008
17. Aydin S, Aydin S, Kobat MA, et al. Decreased saliva/serum irisin concentrations in the acute myocardial infarction promising for being a new candidate biomarker for diagnosis of this pathology. Peptides. 2014;56:141–145. doi:10.1016/j.peptides.2014.04.002
18. Aronis KN, Moreno M, Polyzos SA, et al. Circulating irisin levels and coronary heart disease: association with future acute coronary syndrome and major adverse cardiovascular events. Int J Obes. 2015;39:156–161. doi:10.1038/ijo.2014.101
19. Efe TH, Açar B, Ertem AG, et al. Serum irisin level can predict the severity of coronary artery disease in patients with stable angina. Korean Circ J. 2017;47:44–49. doi:10.4070/kcj.2016.0079
20. Hsieh IC, Ho MY, Wen MS, et al. Serum irisin levels are associated with adverse cardiovascular outcomes in patients with acute myocardial infarction. Int J Cardiol. 2018;261:12–17. doi:10.1016/j.ijcard.2017.11.072
21. Boström P, Wu J, Jedrychowski MP, et al. A PGC1-α-dependent myokine that drives brown-fat-like development of white fat and thermogenesis. Nature. 2012;481:463–468. doi:10.1038/nature10777
22. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Eur Heart J. 2012;33:2551–2567. doi:10.1093/eurheartj/ehs184
23. Huh JY, Panagiotou G, Mougios V, et al. FNDC5 and irisin in humans: I predictors of circulating concentrations in serum and plasma and II mRNA expression and circulating concentrations in response to weight loss and exercise. Metabolism. 2012;61(12):1725–1738.
24. Liu JJ, Wong MD, Toy WC, et al. Lower circulating irisin is associated with type 2 diabetes mellitus. J Diabetes Complications. 2013;27:365–369. doi:10.1016/j.jdiacomp.2013.03.002
25. Roca-Rivada A, Castelao C, Senin LL, et al. FNDC5/irisin is not only a myokine but also an adipokine. PLoS One. 2013;8:e60563. doi:10.1371/journal.pone.0060563
26. Lewandrowski K, Chen A, Januzzi J. Cardiac markers for myocardial infarction. A Brief Review Am J Clin Pathol. 2002;118(Suppl):S93–S99.
27. Xie C, Zhang Y, Tran TD, et al. Irisin controls growth, intracellular Ca2+ signals, and mitochondrial thermogenesis in cardiomyoblasts. PLoS One. 2015;10:e0136816. doi:10.1371/journal.pone.0136816
28. Waseem R, Shamsi A, Mohammad T, et al. FNDC5/irisin: physiology and pathophysiology. Molecules. 2022;27:1118. doi:10.3390/molecules27031118
29. Abd El-Mottaleb NA, Galal HM, El Maghraby KM, Gadallah AI. Serum irisin level in myocardial infarction patients with or without heart failure. Can J Physiol Pharmacol. 2019;97:932–938. doi:10.1139/cjpp-2018-0736
30. Wang JC, Chien WC, Chu P, Chung CH, Lin CY, Tsai SH. The association between heat stroke and subsequent cardiovascular diseases. PLoS One. 2019;14:e0211386. doi:10.1371/journal.pone.0211386
31. Bashar SM, Samir El-Sherbeiny SM, Boraie MZ. Correlation between the blood level of irisin and the severity of acute myocardial infarction in exercise-trained rats. J Basic Clin Physiol Pharmacol. 2018;30:59–71. doi:10.1515/jbcpp-2018-0090
32. Aydin S, Ugur K, Aydin S, Sahin İ, Yardim M. Biomarkers in acute myocardial infarction: current perspectives. Vasc Health Risk Manag. 2019;15:1–10. doi:10.2147/VHRM.S166157
33. Ramsay J, Shernan S, Fitch J, et al. Increased creatine kinase MB level predicts postoperative mortality after cardiac surgery independent of new Q waves. J Thorac Cardiovasc Surg. 2005;129:300–306. doi:10.1016/j.jtcvs.2004.06.005
34. Polanczyk CA, Lee TH, Cook EF, et al. Cardiac troponin I as a predictor of major cardiac events in emergency department patients with acute chest pain. J Am Coll Cardiol. 1998;32:8–14. doi:10.1016/S0735-1097(98)00176-4
35. Javed F, Khan SA, Aziz EF, Abbasi T, Suryadevara R, Herzog E. Unusual towering elevation of troponin I after ST-elevation myocardial infarction and intensive monitoring with echocardiography post-percutaneous coronary intervention: a case report. J Med Case Rep. 2010;4:137. doi:10.1186/1752-1947-4-137
36. Jia S, Liu Y, Yuan J. Evidence in guidelines for treatment of coronary artery disease. Adv Exp Med Biol. 2020;1177:37–73.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
High Urine Albumin-to-Creatinine Ratio is Associated with Increased Arterial Stiffness in Diabetes: A Chinese Cross-Sectional Study
Guo K, Zhu Y, Yu Q, Chen H, Cheng W, Zhang X, Zhang X, Liu B, Zhou Z, Kuang X
Diabetes, Metabolic Syndrome and Obesity 2024, 17:2121-2133
Published Date: 23 May 2024
Impact of High Troponin Level on the Outcome in COVID-19 Positive Patients
Abohamr SI, Kattea MO, Abazid RM, Aldossari MA, Al Asiri N, Alhussini AU, Al Hussaini KI, Alasiri GA, Ali A, Elsheikh E
Journal of Multidisciplinary Healthcare 2024, 17:4989-5000
Published Date: 1 November 2024