")
Back to Journals » International Journal of Women's Health » Volume 15
Association Between Serum Ferritin Levels in Early Pregnancy and Thyroid Function and Pregnancy Outcomes in Chinese Population
Authors Li X, Zhang Z, Cai W, Zhou X, Zhang Y, Wu C, Xu X, Wu H
Received 23 August 2023
Accepted for publication 22 November 2023
Published 11 December 2023 Volume 2023:15 Pages 1951—1957
DOI https://doi.org/10.2147/IJWH.S436651
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Xing Li, Zhuyuan Zhang, Wen Cai, Xuexin Zhou, Yan Zhang, Cailiang Wu, Xianming Xu, Hao Wu
Department of Obstetrics and Gynecology, Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200080, People’s Republic of China
Correspondence: Hao Wu; Xianming Xu, Email [email protected]; [email protected]
Background: The relationship of iron deficiency and thyroid hormone has been researched a lot among pregnant or other healthy population. However, invisible iron deficiency, namely shortage of serum ferritin (sFer) level, has been barely investigated among Chinese pregnant women. This study aimed to explore the effects of sFer status on thyroid function and pregnancy outcomes in a population-based upper first-class hospital.
Methods: A total of 781 singleton pregnant women of gestation in Shanghai General Hospital took part in this retrospective cohort study. The participants were divided into four groups by quartiles of serum ferritin levels (Q1– 4). Binary logistic regressions were used to examine the strength of association between the different traits and the serum ferritin (sFer) quartiles separately, where Q1 (lowest ferritin quartile) was taken as the base reference. One-way ANOVA was adopted to compare the averages of the different variables across sFer quartiles. Categorical measures were compared by Fisher exact test or chi-square test.
Results: As the sFer concentration rises, incidence of premature birth (15.8%vs 12.3% vs 9.20% vs 6.20% p = 0.016) as well as threatened miscarriage (14.8% vs 7.2% vs 8.70% vs 6.70% p = 0.021) presented a downward trend. Compared with the other sFer group, subjects of the low sFer group were older, more often to be found to have lower serum γT3 and FT4 levels in early pregnancy but not in middle pregnancy.
Conclusion: sFer concentration in the first trimester can affect thyroid function. The correction of invisible iron deficiency with inadequate sFer status prior to pregnancy or during early pregnancy is imperative, not only to prevent anemia, but also for maintaining optimum thyroid function and normal fetal development. For clinicians, sFer status of pregnant women should be attached great importance apart from attention to iron level.
Keywords: serum ferritin, thyroid hormone, subclinical hypothyroidism, thyroid-stimulating hormone, pregnant women
Introduction
Subclinical hypothyroidism (SCH) occurs when one individual still has normal range of serum thyroid hormone, but serum thyroid-stimulating hormone (TSH) levels jump outside the reference range. In most cases, the condition is so mild that a person barely notices it until hypothyroidism is present. However, emerging studies have discovered that thyroid hormone during pregnancy has been associated with various physiological processes related to a higher risk of pre-eclampsia, preterm birth, placental development and function, fetal growth, impaired cognitive function of offspring and spontaneous abortion.1–4 The maintenance of normal function of thyroid gland requires a diversity of trace elements, among which iron is an essential one.5,6 Iron deficiency remains a global problem, affecting roughly 20% of the world’s population.7 Iron deficiency undermines the synthesis and metabolism of thyroid hormones, including impairing plasma concentrations of T3 and T4 and increasing hepatic reverse T3 deiodination, which indicates that population deficient in iron is likely to metabolize thyroid hormone via a deactivating pathway.8 Pregnant women are much more prone to develop thyroid disorders, which probably lie in poor adaptation to changes in the physiology of the thyroid gland during pregnancy, including increased microelement demands. Data show that 0.2% to 0.6% of pregnant women develop overt hypothyroidism (elevated concentrations of TSH with low concentrations of free T4)9,10; however, maternal SCH (elevated concentrations of TSH with normal concentrations of free T4) occurs in 3.5% to ~18% of all pregnancies,11–13 suggesting a higher prevalence.
Serum ferritin is a major iron storage protein, a widely used marker for total body Fe stores, with a nano-sized core of hydrated iron oxide and a cage-shaped protein shell, containing 20% iron. Several studies reported that concentrations of serum ferritin are altered in patients with thyroid disease, denoting that ferritin levels in blood reflect thyroid function. Iron supplementation improves some indices of thyroid function in iron-deficient adolescent girls.
The relationship of iron deficiency and thyroid hormone has been researched a lot among pregnant or other healthy population. However, the relationship between different status of serum ferritin and SCH has not been well investigated in the Chinese pregnant population. Hence, our purpose was to assess the relationship between sFer levels and SCH in pregnant women during the first and second trimester. We also explored the effects of sFer levels on the pregnancy outcomes.
Methods and Materials
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Shanghai General Hospital. As this is a retrospective research, informed written consent was exempted but oral permission was obtained from all individual participants before embarking on this study.
Subjects
This retrospective study obtained obstetrical parameters and biological data through electronic medical records system from Department of obstetrics in Shanghai General Hospital on 781 singleton pregnant women aged 21–44 years hospitalized for delivery during January 2021 to Oct 2021.
Recruitment criteria of the study population included: 1) live-birth singleton pregnancy; 2) women’s age ≥18 years old; 3) had their first antenatal care visit between 10 and 20 weeks of gestation. Patients were excluded if they were complicated by 1) stillbirths, 2) congenital fetus malformation, 3) a prior history of thyroid diseases including thyroid dysfunction and thyroid autoimmunity, any other chronic disorders such as hypertension, dyslipidemia, diabetes mellitus, acute or chronic liver diseases, taking oral contraceptive medicine or any other medical agents that might influence thyroid function at the beginning of enrolment, 4) multiple gestations and 5) incomplete medical records.
Among 800 women who met these criteria, 5 refused to participate orally, 6 had abortions before 24 weeks of gestation, and 4 did not undergo an assessment for GDM diagnosis and 4 were excluded for not performing serum lipid tests. Ultimately, a total of 781 pregnant women were included in this analysis.
In the very first antenatal examination, all pregnant women were asked to complete the questionnaires relevant personal history of pro-gestational medical information, such as age, height, weight, gravidity and parity history, husbands’ personal data, personal history of thyroid diseases, chronic diseases such as hypertension, dyslipidemia, diabetes mellitus, acute or chronic liver diseases, and if taken oral contraceptive medicine.
Clinical Measurements
All measurements and the sample collections were performed in the morning after an overnight fast. Blood samples was extracted in gestation 10–14 weeks for early pregnancy and 24–28 weeks for middle pregnancy. Pre-pregnancy body mass index (P-BMI) (kg/m2) was calculated through weight (kg)/height2 (m2). Given the currently available evidence, we adopted the definition of SCH as pregnant women with serum levels of TSH that are above than pregnancy-specific reference ranges or >4 mIU/l, regardless of TPO antibody status.14
Laboratory Examinations
Serum TSH, fT4, and TPOAb levels were measured at a clinical analysis laboratory by using an automated two-step chemiluminescent immunoassay on an ARCHITECT analyzer (Roche Cobas e602, Germany).
Statistical Analyses
Statistical analyses were performed using IBM SPSS version 25.0 (IBM Corp., Armonk, NY, USA). The participants were stratified by SFer levels. They are grouped as Q1, Q2, Q3 and Q4. Normality of the data distribution was tested by the Kolmogorov–Smirnov method. Data with normal distribution were presented as mean ± standard deviation. Categorical data were presented as percentages (cases/absolute numbers). One-way ANOVA tests were used to analyze statistical differences among the study participant’s characteristics in relation to serum ferritin quartile (Q1-4) groups. Binary logistic regressions were used to examine the strength of association between the different traits and the SFer quartiles separately in the first trimester, while Q1 (lowest ferritin quartile) was taken as the base reference.
Results
The participants were divided into four groups based on their serum ferritin quartile (Q1: 13.98 ± 5.78μg/L, N = 196; Q2: 31.40 ± 5.01μg/L, N = 195; Q3: 53.58 ± 8.18μg/L, N = 195; and Q4: 116.61 ± 59.33μg/L, N = 195) at the beginning of the study, and their characteristics are presented in Table 1. Compared with the other sFer group, subjects of the low sFer group were older, more often to be found to have lower serum γT3 and FT4 levels. By contrast, blood glucose data presented an opposite trend. Starting with 5.14 ± 0.38, this number reached 5.24 ± 0.32 with an increase trend, which has been discussed in our previous published paper.15 BMI levels, serum lipid concentrations were comparable between these study groups but yielded non-statistical results. Similar trend from Hb levels showed analogous patterns as sFer status.
 |
Table 1 Association Between sFer Levels in the First Trimester and Thyroid Function |
Database of follow-up was also conducted based on the subjects of early pregnancy. As displayed in Table 2, data of thyroid function failed to reach statistical significance among comparison of these groups. A similar non-statistically significant result was as well reflected in the status of TG, TC, LDL, and HDL, whereas, accompanied by climbing levels of sFer, Hb concentration also took on the same trend. HbA1c value, as in early pregnancy, is significant negative correlation with sFer levels.
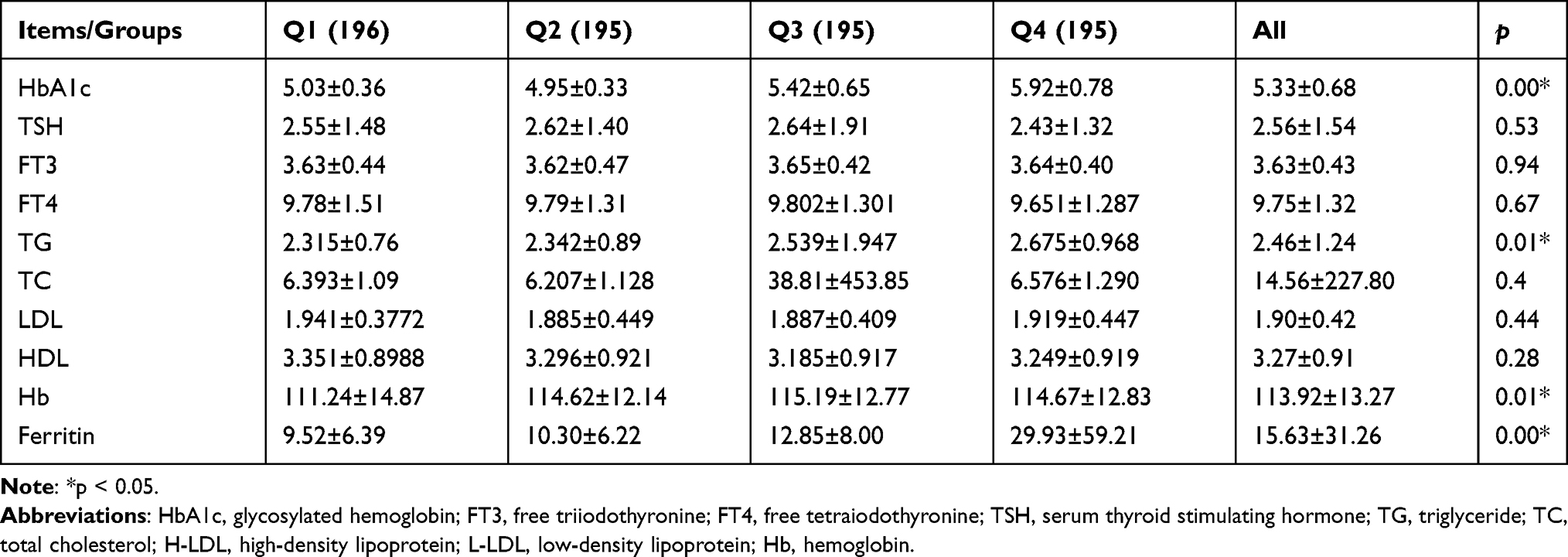 |
Table 2 Association Between sFer Levels in the Second Trimester and Thyroid Function |
For further elaboration, the relationship between sFer levels and SCH, OR and aOR for the association of serum ferritin with SCH in early pregnancy are listed in Table 3. As presented above (Table 3), negative correlations between SCH in early pregnancy and serum ferritin levels were found for Q4 (aOR = 0.367, P = 0.042).
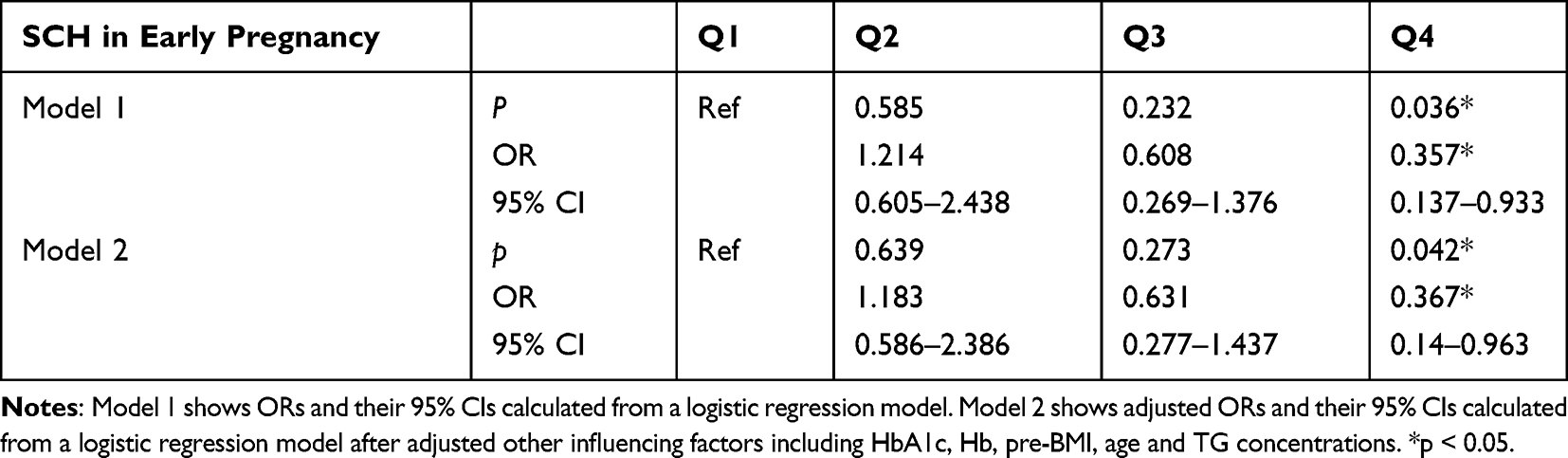 |
Table 3 Odds Ratios and Adjusted Odds Ratios for the Association of Serum Ferritin in Early Gestation with SCH in Early Gestation by Serum Ferritin Quartile (Reference Group = Q1) |
As Table 4 indicates, with the serum ferritin level increasing, the incidence of SCH in middle pregnancy otherwise statistically decreased, with relative risks of 0.593 (OR = 0.575, 95% CI = 0.312–0.987, P = 0.048). After adjusting for potential confounding parameters (Pre-BMI, maternal age), similar results (OR = 0.593, 95% CI = 0.321–0.976, P = 0.05) were still obtained, although the results changed slightly after the additional adjustment.
 |
Table 4 Odds Ratios and Adjusted Odds Ratios for the Association of Serum Ferritin in Early Gestation with SCH in Middle Pregnancy by Serum Ferritin Quartile (Reference Group = Q1) |
For a further elucidation of association between sFer levels in the first trimester and pregnancy outcomes, the clinical pregnancy prognosis for each cohort was compared. As presented in Table 5, the four group (Q1, Q2, Q3 and Q4) in the incidence rate of premature birth, threatened miscarriage was significantly different (p<0.05). As the sFer concentration rises, incidence of premature birth (15.8% vs 12.3% vs 9.20% vs 6.20% p = 0.016) as well as threatened miscarriage (14.8% vs 7.2% vs 8.70% vs 6.70% p = 0.021) presented a downward trend. The prevalence of gestational hypertensive disorders and low birth weight also declined but without statistical significance (p > 0.05).
 |
Table 5 Association Between sFer Levels in the First Trimester and Pregnancy Outcomes |
Discussion
Although the fetal thyroid gland is formed and functional in the first trimester, it is not mature enough until second trimester (18–20 weeks).16 Thus, maternal thyroid hormone crosses the placenta to the fetus depending on maternal thyroid hormone during a crucial period of development in early gestation.17 Consequently, in early pregnancy maternal thyroid disorders can spell adverse pregnancy and child neurodevelopmental outcomes. In our present study, we investigated the relationship between sFer levels in early pregnancy and SCH in early and middle pregnancy. Based on our research, the SCH incidence shows a positive correlation with sFer level variables. We also further demonstrate that the incidence rate of premature birth and threatened miscarriage in pregnancy posed a negative correlation with sFer status of the first trimester.
Previous studies have revealed that during pregnancy elevated TSH concentration was in accordance with higher risks of prematurity and neonatal respiratory distress syndrome (RDS) in offspring. Higher maternal serum TSH was also related to elevated chance of spontaneous abortion, premature birth, threatened miscarriage, gestational hypertension disorders, and low birth weight.18 Our results are almost in line with earlier various studies done on the correlation between thyroid hormones and sFer metabolism studies.19 According to our results, with the sFer status increasing, incidence of premature birth (15.8%vs 12.3% vs 9.20% vs 6.20% p = 0.016) as well as threatened miscarriage (14.8% vs 7.2% vs 8.70% vs 6.70% p = 0.021) presented a downward trend. The prevalence of gestational hypertensive disorders and low birth weight also declined but without statistical significance (p>0.05). Iron deficiency may be the underlying cause of hypothyroidism in the form of thyroid peroxidase; the key enzyme in thyroid hormone biosynthesis depends on iron.20 A meta-analysis of 18 cohort studies involving nearly 4000 women revealed that, compared to euthyroidism, the mother’s subclinical hyperthyroidism is associated with increased risks of abortion, premature rupture of membranes, preterm birth and neonatal death.1 Moreover, the risks of these adverse reactions were even more pronounced if subclinical hypothyroidism was present during the first trimester.18 Though evidence is mounting that maternal subclinical hypothyroidism is associated with low birth weight and preterm birth. The pathological physio-mechanisms of our findings are largely speculative and remain unclear.
In a study of the relationship between hemoglobin and SCH during pregnancy, hemoglobin were found elevated after left thyroid hormone supplementation in pregnant women, suggesting a negative correlation between TSH and hemoglobin.21 It is suggested that low dose of L-T4 should be added to iron therapy in patients with anemia and subclinical hypothyroidism T4, showed greater improvement in hematological parameters than iron supplementation alone. On the other hand, the study also found that patients with hypothyroidism and reduced iron reserve may benefit from supplementing L-T4 with iron.21 In this Chinese pregnancy population-oriented study, we demonstrated this conclusion again. We found that deficiency of Sfer has been linked to an increased risk of subclinical hypothyroxinemia in the first trimester of pregnancy but not in the second trimester, which is different from a previous study. An earlier research performed in Switzerland indicated that among middle and late pregnancy the state of iron has been proved to be a decisive factor for serum T4 and TSH.22 However, in another study conducted in Belgium,23 they demonstrated that iron deficiency, is a determinant of serum fT4 and T4 in pregnant women in the first trimester, and our findings almost consist with this result. Few other regional and hospital studies have been conducted about the state of iron and thyroid function during pregnancy. Significant association between iron condition and fT4 was found but not with TSH.24,25
In this population-based study, we demonstrate that sFer deficiency is a significant determinant of TSH and fT4 in pregnant women. These findings matter a lot since sFer deficiency frequently happens in an invisible way and because hypothyroxinemia during pregnancy can negatively hinder the neurodevelopment of offspring and prematurity or preterm birth.3,26 To our knowledge, this is the first population-based study showing such a relation between sFer status and SCH in pregnant women.
As the limited sample size of our investigation and the retrospective type of the present study, the findings with regard to the relation between thyroid hormones need to be confirmed through further prospective researches with larger sample size.
Conclusions
Our results support the correction of invisible iron deficiency with inadequate sFer status prior to pregnancy or during early pregnancy, not only to prevent anemia, but also for maintaining optimum thyroid function and normal fetal development. For clinicians, sFer status of pregnant women should be attached great importance apart from attention to iron level.
Data Sharing Statement
The data used to support the findings of this study are included in the article. Also, if readers need detailed information, he/she can email the corresponding author.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Shanghai General Hospital. As this is a retrospective research, informed written consent was exempted but oral permission was obtained from all individual participants before embarking on this study.
Acknowledgments
The authors are grateful for Department of Obstetrics and Gynecology, Shanghai General Hospital Affiliated to Shanghai Jiaotong University for collecting health information data.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Korevaar TIM, Derakhshan A, Taylor PN, et al. Association of thyroid function test abnormalities and thyroid autoimmunity with preterm birth: a systematic review and meta-analysis. JAMA. 2019;322(7):632–641. doi:10.1001/jama.2019.10931
2. Barjaktarovic M, Korevaar TI, Chaker L, et al. The association of maternal thyroid function with placental hemodynamics. Hum Reprod. 2017;32(3):653–661. doi:10.1093/humrep/dew357
3. Finken MJ, van Eijsden M, Loomans EM, Vrijkotte TG, Rotteveel J. Maternal hypothyroxinemia in early pregnancy predicts reduced performance in reaction time tests in 5- to 6-year-old offspring. J Clin Endocrinol Metab. 2013;98(4):1417–1426. doi:10.1210/jc.2012-3389
4. Toloza FJK, Derakhshan A, Männistö T, et al. Association between maternal thyroid function and risk of gestational hypertension and pre-eclampsia: a systematic review and individual-participant data meta-analysis. Lancet Diabetes Endocrinol. 2022;10(4):243–252. doi:10.1016/S2213-8587(22)00007-9
5. Eftekhari MH, Eshraghian MR, Mozaffari-Khosravi H, Saadat N, Shidfar F. Effect of iron repletion and correction of iron deficiency on thyroid function in iron-deficient Iranian adolescent girls. Pak J Biol Sci. 2007;10(2):255–260. doi:10.3923/pjbs.2007.255.260
6. Eftekhari MH, Simondon KB, Jalali M, et al. Effects of administration of iron, iodine and simultaneous iron-plus-iodine on the thyroid hormone profile in iron-deficient adolescent Iranian girls. Eur J Clin Nutr. 2006;60(4):545–552. doi:10.1038/sj.ejcn.1602349
7. Veltri F, Decaillet S, Kleynen P, et al. Prevalence of thyroid autoimmunity and dysfunction in women with iron deficiency during early pregnancy: is it altered? Eur J Endocrinol. 2016;175(3):191–199. doi:10.1530/EJE-16-0288
8. Smith SM, Johnson PE, Lukaski HC. In vitro hepatic thyroid hormone deiodination in iron-deficient rats: effect of dietary fat. Life Sci. 1993;53(8):603–609. doi:10.1016/0024-3205(93)90268-8
9. Krassas GE, Poppe K, Glinoer D. Thyroid function and human reproductive health. Endocr Rev. 2010;31(5):702–755. doi:10.1210/er.2009-0041
10. Pop V, Broeren M, Wiersinga W. The attitude toward hypothyroidism during early gestation: time for a change of mind? Thyroid. 2014;24(10):1541–1546. doi:10.1089/thy.2014.0007
11. Lazarus J, Brown RS, Daumerie C, Hubalewska-Dydejczyk A, Negro R, Vaidya B. European thyroid association guidelines for the management of subclinical hypothyroidism in pregnancy and in children. Eur Thyroid J. 2014;3(2):76–94. doi:10.1159/000362597
12. Abalovich M, Amino N, Barbour LA, et al. Management of thyroid dysfunction during pregnancy and postpartum: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2007;92(8 Suppl):s1–s7. doi:10.1210/jc.2007-0141
13. Korevaar TIM, Medici M, Visser TJ, Peeters RP. Thyroid disease in pregnancy: new insights in diagnosis and clinical management. Nat Rev Endocrinol. 2017;13(10):610–622. doi:10.1038/nrendo.2017.93
14. Casey BM, Metz TD, Quinlan J Thyroid disease in pregnancy: acog practice bulletin, number 223. Obstet Gynecol. 2020;135(6):e261–e74. doi:10.1097/AOG.0000000000003893
15. Zhang Z, Li X, Zhou X, et al. Association of gestational hypertriglyceridemia, diabetes with serum ferritin levels in early pregnancy: a retrospective cohort study. Front Endocrinol. 2023;14:1067655. doi:10.3389/fendo.2023.1067655
16. Lee SY, Pearce EN. Assessment and treatment of thyroid disorders in pregnancy and the postpartum period. Nat Rev Endocrinol. 2022;18(3):158–171. doi:10.1038/s41574-021-00604-z
17. LaFranchi SH. Thyroid function in preterm/low birth weight infants: impact on diagnosis and management of thyroid dysfunction. Front Endocrinol. 2021;12:666207. doi:10.3389/fendo.2021.666207
18. Lee SY, Cabral HJ, Aschengrau A, Pearce EN. Associations between maternal thyroid function in pregnancy and obstetric and perinatal outcomes. J Clin Endocrinol Metab. 2020;105(5):e2015–23. doi:10.1210/clinem/dgz275
19. Wang F, Zhang Y, Yuan Z, et al. The association between iron status and thyroid hormone levels during pregnancy. J Trace Elem Med Biol. 2022;74:127047. doi:10.1016/j.jtemb.2022.127047
20. Tiwari R, Saharia GK, Mangaraj M. Evaluation of serum ferritin and anti-thyroid peroxidase antibody status in newly diagnosed subclinical cases of hypothyroidism. Endocr Metab Immune Disord Drug Targets. 2021;21(8):1453–1458. doi:10.2174/1871530320666200925125404
21. Soliman AT, De Sanctis V, Yassin M, Wagdy M, Soliman N. Chronic anemia and thyroid function. Acta Biomed Ateneo Parmense. 2017;88(1):119–127. doi:10.23750/abm.v88i1.6048
22. Zimmermann MB, Burgi H, Hurrell RF. Iron deficiency predicts poor maternal thyroid status during pregnancy. J Clin Endocrinol Metab. 2007;92(9):3436–3440. doi:10.1210/jc.2007-1082
23. Moreno-Reyes R, Corvilain B, Daelemans C, Wolff F, Fuentes Peña C, Vandevijvere S. Iron deficiency is a risk factor for thyroid dysfunction during pregnancy: a population-based study in Belgium. Thyroid. 2021;31(12):1868–1877. doi:10.1089/thy.2021.0286
24. Teng X, Shan Z, Li C, et al. Iron deficiency may predict greater risk for hypothyroxinemia: a retrospective cohort study of pregnant women in china. Thyroid. 2018;28(8):968–975. doi:10.1089/thy.2017.0491
25. Yu X, Shan Z, Li C, et al. Iron deficiency, an independent risk factor for isolated hypothyroxinemia in pregnant and nonpregnant women of childbearing age in China. J Clin Endocrinol Metab. 2015;100(4):1594–1601. doi:10.1210/jc.2014-3887
26. Liu H, Shan Z, Li C, et al. Maternal subclinical hypothyroidism, thyroid autoimmunity, and the risk of miscarriage: a prospective cohort study. Thyroid. 2014;24(11):1642–1649. doi:10.1089/thy.2014.0029
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.