Back to Journals » International Journal of General Medicine » Volume 17
Association Between Serum 25-Hydroxyvitamin D Level and Risk of Anemia: An Observational and Mendelian Randomization Study
Authors Bi S, Zhang J, Wei N, Zhou Q, Wang C
Received 17 July 2024
Accepted for publication 30 August 2024
Published 6 September 2024 Volume 2024:17 Pages 3893—3905
DOI https://doi.org/10.2147/IJGM.S479039
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kenneth Adler
Shaojie Bi,1 Juan Zhang,1 Ning Wei,2 Qingbo Zhou,3,4 Chunyan Wang3
1Department of Cardiology, The Second Hospital, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China; 2Department of Information Center, The Second Hospital, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China; 3Department of Geriatrics, The Second Hospital, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China; 4School of Nursing and Rehabilitation, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China
Correspondence: Chunyan Wang, Email [email protected]
Introduction: Anemia, characterized by low hemoglobin or erythrocyte levels, is a significant global health issue with severe implications for public health. Recent studies have explored the potential link between anemia and 25-hydroxyvitamin D [25(OH)D], yet the precise mechanisms remain unclear. This study aims to clarify the possible causal relationship between 25(OH)D levels and anemia risk.
Methods: We conducted a comprehensive investigation combining observational and Mendelian randomization (MR) analyses. The observational study included detailed demographic, comorbidities, and laboratory data collected from 7160 hospitalized patients in China. For the MR analysis, genetic polymorphisms were utilized to assess causal effects.
Results: Observational analysis revealed an inverse relationship between 25(OH)D levels and the risk of anemia, with stratified analysis indicating a nonlinear association and a threshold of 48.716 nmol/L. The MR analysis confirmed a protective causal relationship between higher 25(OH)D levels and a reduced risk of anemia. Bidirectional MR analysis found no evidence that anemia influences 25(OH)D levels.
Discussion: This study provides strong evidence of a causal link between increased 25(OH)D levels and a lower incidence of anemia. The findings highlight the potential role of vitamin D in anemia prevention, supporting the need for further research into vitamin D supplementation as a strategy to reduce anemia risk.
Conclusion: Our findings support the hypothesis that higher 25(OH)D levels are causally associated with a reduced risk of anemia, suggesting vitamin D’s potential role in anemia prevention and public health strategies.
Keywords: anemia, 25-hydroxyvitamin D, Mendelian randomization
Introduction
Anemia is a common health problem worldwide. Low blood erythrocyte count, or hemoglobin deficiency, results in decreased oxygen carrying capacity and an inability to meet metabolic needs. Anemia is generally characterized by hemoglobin (HGB) levels, hematocrit, or red blood cell counts falling below typical age- and sex-adjusted ranges.1 An estimated 1.6 billion people globally suffer from anemia to varied degrees, according to the World Health Organization (WHO). Region, age, gender, and socioeconomic characteristics all affect the specific incidence.2 In 2010, the estimated prevalence of anemia worldwide was 32.9% of the total population. Anemia dramatically affects both the quality of life of persons who are affected and healthcare systems due to its widespread effects on physical and cognitive health.3 In China, the most recent national health survey reported that the prevalence of anemia among the general population is approximately 12.6%, with higher rates observed in elderly populations and women of childbearing age.4 Older adults are considered high-risk for anemia due to age-related changes and the presence of multiple comorbidities, highlighting the importance of further detailed research in this population. The identification of putative causative variables and pathways associated with anemia is critical for developing effective preventive and intervention measures as the globe addresses this health issue. While the WHO Global Nutrition Target 2025 specifically aims to reduce anemia in women of reproductive age by 50%,5 similar targeted efforts are needed to address the growing burden of anemia in the elderly. The involvement of 25-hydroxyvitamin D [25(OH)D] in the development of anemia is one of the novel correlations being investigated by developing research, despite the fact that recognized risk factors for anemia, such as nutritional deficiencies and chronic diseases, have been thoroughly researched.6 25(OH)D, a physiologically active version of vitamin D that may be produced by the skin when exposed to sunlight or can be consumed through food, has drawn interest for its ability to affect the hematological system among other physiological functions in addition to bone health.7 It has been revealed by recent studies to have a wide range of physiological functions, from immunological regulation to heart function. Amidst this growing field, a number of research have suggested that 25(OH)D may have a positive effect on anemia through its inhibitory actions on hepcidin and inflammatory cytokines.8–10 The National Health and Nutrition Examination Survey (NHANES) cross-sectional research conducted between 2001 and 2018 reveals a correlation between the incidence of anemia and serum 25(OH)D concentration.11 Comparable observational research has suggested that there may be a connection between a low level of 25(OH)D and a higher risk of anemia, potentially via immunological response, inflammation, and erythropoiesis regulation.12,13 Nonetheless, the difficulty is separating causation from simple correlation, particularly in light of the complex interactions between multiple variables affecting anemia and 25(OH)D content. Mendelian randomization (MR) analysis was the tool we used to overcome this obstacle and clarify the possible causative relationship between anemia and 25(OH)D. By utilizing the stochastic distribution of genetic variables during meiosis and fertilization, MR uses genetic variants as instrumental variables to infer causation.14 Using summary statistics from extensive genome-wide association studies (GWASs) on 25(OH)D levels and anemia outcomes, our goal is to disentangle the intricate network of confounding variables that frequently mask causal links in conventional observational research. Our work includes a two-sample MR analysis in addition to an observational investigation that uses a local database. Investigating the association between levels of 25(OH)D and the risk of anemia, as well as any possible dose-effect relationship, is our goal. It is possible to discover fresh approaches to anemia prevention and therapy that make use of 25(OH)D supplementation. By means of thorough scientific investigation, we want to offer a more refined comprehension of the complex elements that cause anemia, opening the door to better public health results and higher standards of living.
Materials and Methods
In this work, we employed two-sample bidirectional MR and cross-sectional research methods. The reporting of this study was strengthened through the application of STROBE-MR and STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) recommendations. The study workflow chart is shown in Figure 1.
 |
Figure 1 Study workflow chart. Association and causal effect between anemia and 25(OH)D. |
Data Collection
A local database of 7160 hospitalized patients from January 1, 2021 to June 30, 2023 at the Second Hospital of Shandong University, Shandong, China, was created for the primary observational study. Information about the patient’s age, sex, comorbidities, serum concentration of 25(OH)D, hemoglobin (HGB), white blood cells (WBC), platelets (PLT), albumin (ALB), potassium (K), sodium (Na), chloride (Cl), calcium (Ca), magnesium (Mg), and phosphorus (P), C-reactive protein (CRP), iron (Fe), ferritin, N-terminal pro-brain natriuretic peptide (NT-proBNP), alanine aminotransferase (ALT), aspartate aminotransferase (AST), creatinine (Cr), and uric acid (UA). The medical laboratory at Shandong University’s Second Hospital tested each hematological indicator, and the information system at the hospital collected the results. Hemoglobin levels below 120 g/L for adult males and 110 g/L for adult females were considered anemia.1 The protocol for the study was accepted by the Medical Ethics Committee of Shandong University’s Second Hospital [No. KYLL-2023(KJ)P-1792, 2023–10-20].
Association Analysis for Local Database
Continuous data were presented as median and quartile spacing (Median, IQR) or means and standard deviations (Mean±SD). Case numbers and percentages (n, %) were used to represent categorical data. We carried out a cross-sectional study and a multivariable logistic regression analysis adjusted for demographic variables, comorbidities, and laboratory test findings in association analysis based on local database. We computed 95% confidence intervals (95% CIs) and odds ratios (ORs) to evaluate the connections between the variables. The software package Free Statistics, version 1.8, was used to analyze the data.
Summary Statistics for GWAS
We took the 25(OH)D concentration GWAS summary data from the UK Biobank GWAS and used it as the exposure in the MR research.15 The number of single nucleotide polymorphisms (SNPs) was 16668957, and the sample size was 441291. In the initial analysis, genetic principle components were previously used to adapt GWAS data of the European population and probable population structure. The GWAS anemia summary data came from the FinnGen, comprising 27371 cases and 88536 controls. For each of the initial research, ethical approval was obtained. The Supplementary Table S1 contains a list of GWAS study characteristics.
Selection of Instrumental Variables
Three hypotheses need to be met for MR studies to support causal estimates: (1) genetic variants must exhibit a strong correlation with exposure; (2) genetic variants must not exhibit a correlation with any potential confounder of the exposure-outcome association; and (3) genetic variants must not independently affect the outcome.16 The instrumental variable (IV) was genetic variations linked to the 25(OH)D concentration, as determined by the genome-wide significance of Pvalue ≤5×10−8. In order to preserve independent SNPs, we eliminate the linkage disequilibrium by defining the clumping window size as 10000kb and the r2 threshold as 0.001. Due to their unclear effect direction, palindromic SNPs were eliminated, and pleiotropic SNPs were eliminated using the MR-Egger outlier test with Poutlier<0.05. F statistic ≥10, which measures the strength of IVs, showed a high correlation between the IVs and the exposure.
Two-Sample Bidirectional MR Analysis
The study employed the two-sample bidirectional MR analysis17 to determine the causal relationship between the risk of anemia and 25(OH)D concentration. A meta-analysis technique called inverse-variance weighted (IVW) method was used to aggregate Wald ratio estimates of the causal influence derived from several SNPs. Assuming that every genetic variant met the IV requirements, this approach yielded a consistent estimate of the causal effect of the exposure variable on the outcome variable. The study employed weighted median and MR-Egger regression techniques to investigate and account for horizontal pleiotropy. Tests were deemed statistically significant when P<0.05 was reached. We evaluated SNP heterogeneities using the I2 statistic and Cochran’s Q-statistics. To look into the potential that a single SNP was the cause of the causal connection, “leave-one-out” analysis was done. Regarding reverse MR, the previously described steps were carried out again using the same database, this time swapping the exposure [25(OH)D] and outcome (anemia) in order to evaluate the reverse-causal relationship. We specifically analyzed the causal effect of 25(OH)D on different types of anemia, including iron deficiency anemia, nutritional anemia, hemolytic anemia, aplastic anemia, acute hemorrhagic anemia, vitamin B12 deficiency anemia, and anemia in chronic illness. Each anemia type was treated as a separate outcome, using genetic instruments from GWAS. All MR analyses were performed using R version 4.3.1 with the TwoSampleMR package.
Results
Characteristics of Local Data
The study included 7160 adult hospitalized patients (≥18 years old), of which 3692 (51.6%) were female and 3468 (48.4%) were male.The average age of the participants was 56.5±14.6 years. Among them, the prevalence of anemia was 24.3%. Other comorbidities included hypertension (1.8%), cardiovascular diseases (58.1%), heart failure (0.3%), chronic pulmonary disease (0.3%), diabetes (6.2%), thyroid disorders (0.5%), metabolic disorders (0.5%), liver diseases (2.0%), digestive disorders (0.9%), kidney diseases (0.9%), cerebrovascular diseases (1.9%), neurodegenerative disorders (0.6%), autoimmune diseases (0.5%), infectious diseases (7.1%), cancer (1.1%), electrolyte disturbances (1.7%), and pregnancy-related conditions.We categorized participants into different groups based on their 25(OH)D concentrations as follows: ≥75 nmol/L for the sufficient group, 50–75 nmol/L for the insufficient group, 25–50 nmol/L for the deficient group, and ≤25 nmol/L for the severe deficiency group. These cutoff values were chosen based on widely accepted guidelines and studies that correlate these levels with bone health and overall health outcomes.18 The baseline features for the several groups with varying levels of 25(OH)D are compiled in Table 1. Age, hemoglobin level, WBC, PLT, and comorbidities of cancer, kidney disease, cerebrovascular disease, and metabolic illnesses were all statistically significantly different.
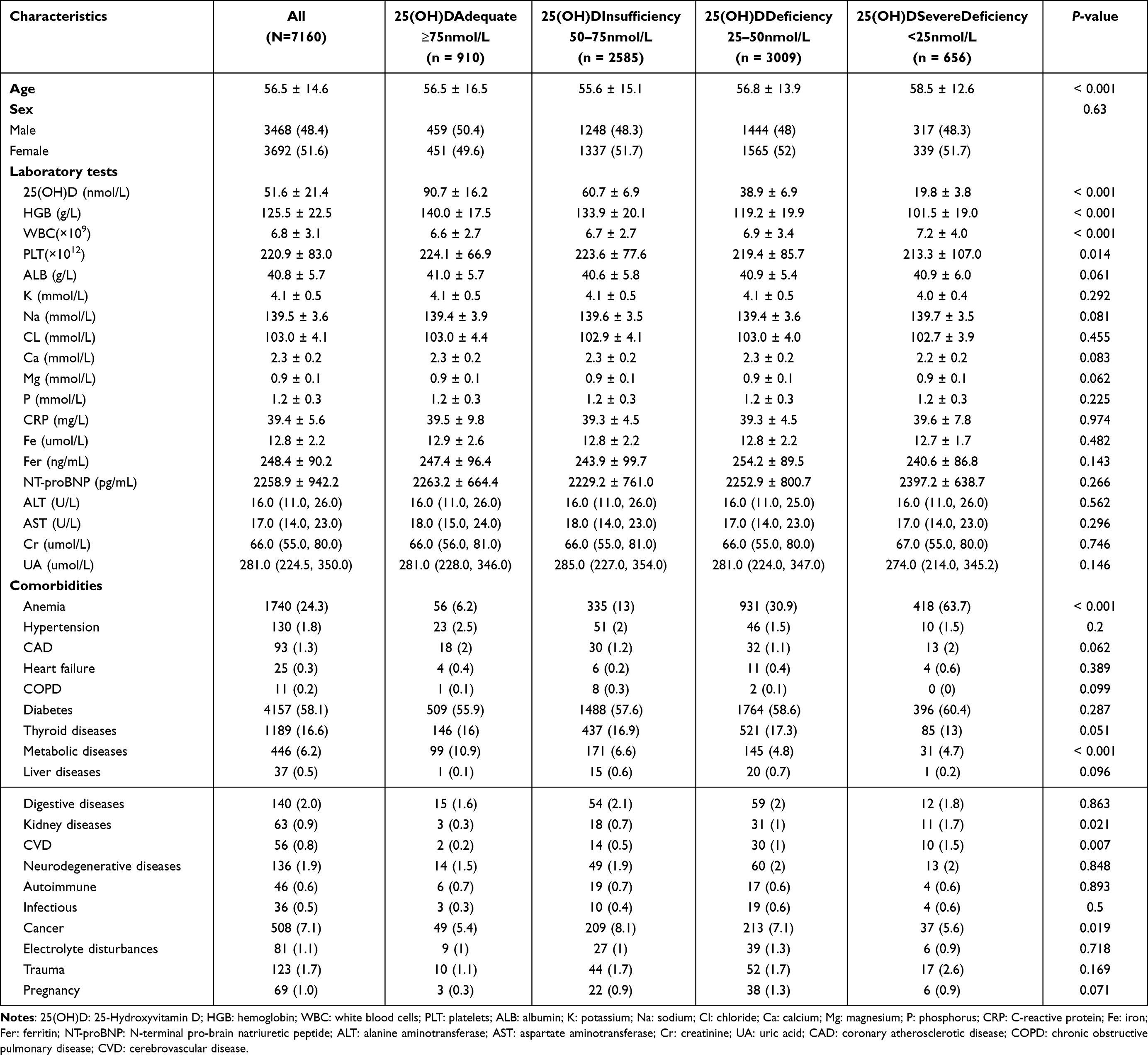 |
Table 1 Baseline Characteristics of the Adult Hospitalized Patients According to Various different 25(OH)Dlevels |
Relationship Between Anemia and 25(OH)D concentration
Serum 25(OH)D concentration and the risk of anemia were found to be significantly inversely correlated by multivariable logistic regression analyses (Table 2). The 25(OH)D concentration was inversely correlated with anemia in both the minimally adjusted Model 2 and the unadjusted Model 1, which were both adjusted for demographic factors and comorbidities (OR 0.95, 95% CI 0.94–0.96, P <0.001, and OR 0.95, 95% CI 0.94–0.97, P <0.001, in Model 2). The outcome of fully adjusting for demographics, comorbidities, and laboratory test findings in model 3 revealed that the risk of anemia decreased by 5% for every unit rise in 25(OH)D (OR 0.95, 95% CI 0.94–0.97, P <0.001). All three statistical models produced reliable results. The trend of the effective value changed differently in each group when the serum 25(OH)D concentration was classified as acceptable (≥75 nmol/L), insufficiency (50–75 nmol/L), deficiency (25–50 nmol/L), and severe deficiency (≤25 nmol/L). The 25(OH)D insufficiency group had a 2.23-fold increased risk of anemia compared to the adequate group (OR 2.23, 95% CI 1.66–3.00, P <0.001), the 25(OH)D deficiency group had a 6.72-fold increased risk of anemia compared to the adequate group (OR 6.72, 95% CI 5.05–8.93, P <0.001), and the 25(OH)D severe deficiency group had a 27.22-fold increased risk of anemia compared to the adequate group (OR 27.22, 95% CI 19.76–37.49, P <0.001). P for trend was less than 0.001.
 |
Table 2 The Correlation Between Anemia and Serum 25(OH)D |
The Nonlinear Relationship and Interaction Analyses Between Anemia and 25(OH)D
After all variables were taken into account, a nonlinear dose-response connection between the risk of anemia and the 25(OH)D concentration was shown (Figure 2). We discovered that the threshold of 25(OH)D concentration was 48.716 nmol/L by employing a two-piecewise linear regression model (Table 3). The incidence of anemia rapidly decreased by 7% below the threshold (OR 0.93, 95% CI 0.922–0.937, P <0.001). The dose-response curve trend was 2.3% gentler above the threshold (OR 0.977, 95% CI 0.969–0.986, P <0.001). Furthermore, after stratification, the interaction analysis in Figure 3 showed that the relationship between 25(OH)D concentration and anemia was stable (P for interaction > 0.05) and that the following variables were not statistically significant: sex, CRP, NT-proBNP, ALB, ALT, Cr, diabetes, coronary heart disease, and cancer. On the other hand, the relationship between anemia and 25(OH)D was interactive with age (P for interaction = 0.02).
 |
Table 3 Inflection Point analysis of 25(OH)D on Anemia |
 |
Figure 2 The fitting curve of 25(OH)D on anemia. The multivariable regression model was adjusted for demographic characteristics, comorbidities, and laboratory test results. The inflection point was 49.42 and P for non-linear was <0.001. |
 |
Figure 3 Forest plot of 25(OH)D on anemia. |
MR Analysis for Causal Relationship between Anemia and 25(OH)D
Selection of Instrumental Variables
We performed Two-Sample MR analyses for the Causal Relationship between 25(OH)D and anemia, employing genetic variations linked to 25(OH)D concentration as the instruments and anemia as the desired outcome. After using the IV selection protocols, we were able to identify 93 distinct SNPs as the IVs, all of which showed a strong correlation with 25(OH)D concentration. After that, MR analyses were performed using these chosen SNPs to determine the causal relationship between exposure and the result.
Two-Sample MR
A protective causal association between 25(OH)D concentration and the incidence of anemia was found by the Two-Sample MR analysis. OR 0.87, 95% CI 0.78 to 0.96 (P=0.009) was obtained using the IVW technique. In particular, there was a 5% decreased incidence of anemia for every one standard deviation increase in 25(OH)D concentration (Table 4). A protective impact of increased 25(OH)D concentration against anemia risk was consistently supported by the MR estimations produced from several approaches, such as IVW, weighted median, weighted mode, and MR robust adjusted profile score (MR-RAPS). Scatter plots showing the relationship between 25(OH)D and the risk of anemia for the instruments are shown in Supplementary Figure S1 (A). The heterogeneity Supplementary Figure S1 (B) was evaluated using a funnel plot. Additionally, forest plots showing the MR estimates of the effects of SNPs linked to 25(OH)D concentration on the incidence of anemia were produced Supplementary Figure S1 (C). The results were consistent and not influenced by a single SNP, according to leave-one-out analyses Supplementary Figure S1 (D).
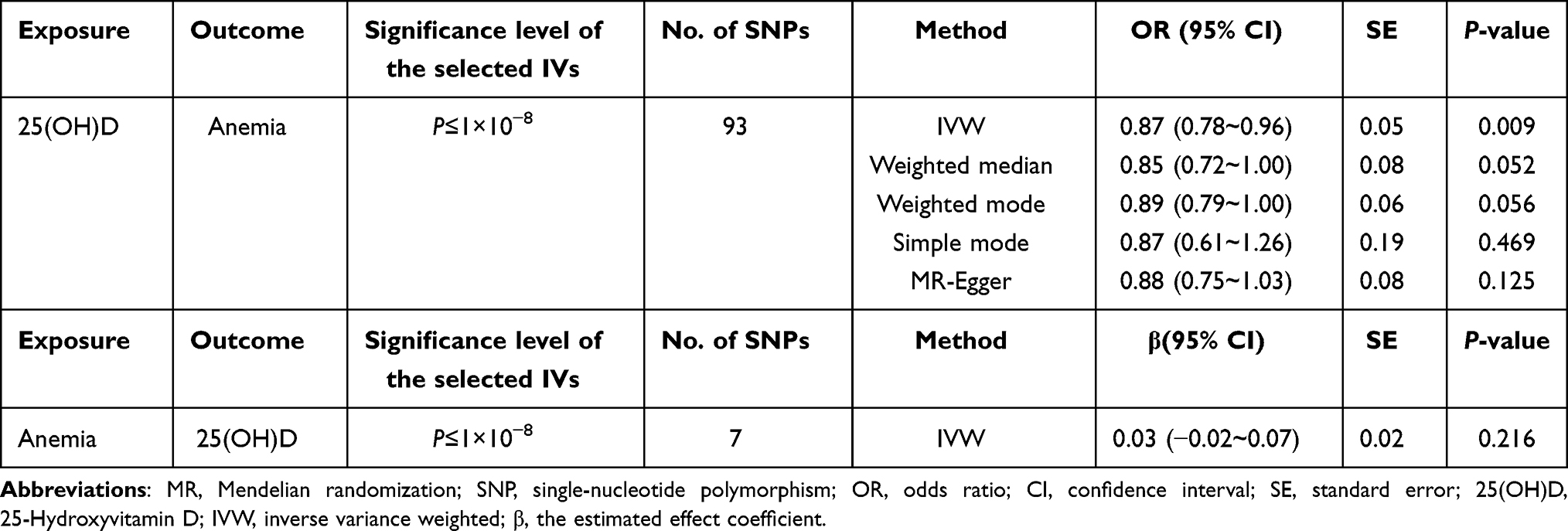 |
Table 4 Bidirectional MR Result of the Causal Effect Between the Risk of Anemia and 25(OH)D |
Bidirectional MR
In order to study the opposite direction of causation, we used genetic liability for anemia as an exposure to examine if anemia risk had a causal effect on 25(OH)D concentration. Nevertheless, no meaningful causal association between the incidence of anemia and 25(OH)D concentration was discovered using any of the MR techniques (IVW β = 0.03; 95% CI, −0.02 to 0.07; P = 0.216). Finally, a protective causal connection between a greater 25(OH)D concentration and a lower incidence of anemia was revealed by the univariable MR analysis. There was, however, insufficient data to support a link between the risk of anemia and 25(OH)D concentration.
MR Analyses of 25(OH)Don Different Types of Anemia
Using MR analyses, we investigated the connection between 25(OH)D and various forms of anemia in further detail. The findings indicated that iron deficiency anemia (IVW OR = 0.79; 95% CI, 0.68 to 0.92; P=0.003) and nutritional anemia (IVW OR = 0.83; 95% CI, 0.72 to 0.95; P=0.006) were causally associated to 25(OH)D concentration. There was no correlation with other forms of anemia, such as hemolytic anemia, aplastic anemia, acute hemorrhagic anemia, vitamin B12 deficiency anemia, and anemia in chronic illness (Supplementary Table S2).
Discussion
Causal Association Between 25(OH)D and Anemia
Our research suggests a reliable causal association between lower anemia risk and higher 25(OH)D levels through the use of MR analysis in conjunction with observational study. This approach provides a deeper understanding of the etiology of anemia, moving beyond simple correlations to identify potential management and preventive strategies. The results provide new insight into the field of anemia and iron deficiency etiology. The results add meaningful contribution to the field by providing the link between anemia and serum 25- Hydroxyvitamin D.
Insights from Previous Studies
Anemia and vitamin D may be related, according to earlier observational research. A cross-sectional study of the US population from 2001 to 2018 was conducted by Yang Zhang et al using data from the NHANES. The general population in the United States has a U-shaped curve in relation to serum 25(OH)D concentration and anemia risk, according to the results. As a result, vigilant observation and suitable vitamin D treatment can lower the risk of anemia.11 Our findings support the validity of the link between greater 25(OH)D levels and a lower incidence of anemia in the adult Chinese population, which is in line with previous research. Additionally, we disclose the dose-effect and nonlinear relationships between the risk of anemia and 25(OH)D. The possible impact of vitamin D on erythropoiesis, inflammation, and immunological responses is highlighted by this alignment.
Focus on Specific Populations
Much of the existing research focuses on specific groups, such as pregnant women and children. For instance, Reagan M. Mogire et al found that children with low 25(OH)D concentrations were more likely to experience iron deficiency compared to those with adequate levels. Individual indicators of iron status were impacted differently by 25(OH)D concentrations.19 Furthermore, Shuting Siet al reported that early- and mid-pregnant women with vitamin D deficit had a higher risk of anemia than did women without vitamin D deficiency. Hemoglobin concentration and plasma 25(OH)D levels correlated favorably during each trimester of pregnancy.20 These studies are important sources of information regarding the connection between anemia and 25(OH)D, but they do not include thorough, stratified population-level research. Our study addresses this gap by examining various stratification criteria, including age, gender, comorbidities, and laboratory tests.
Challenges in Observational Research
Most previous studies were observational and subject to confounding variables, which complicates the determination of causality. Determining causality in the presence of confounding variables is still difficult. Simple causal attributions become more difficult to understand due to the several factors that interact to influence both 25(OH)D levels and anemia outcomes. Therefore, this makes the conclusions of this study less lack of merit. By using genetic tools to investigate possible causation, our study goes one step further. Our study’s use of MR analysis helps to overcome this difficulty.
Strengths of Combining MR and Observational Study
The strength of our study lies in its comprehensive approach, combining MR analysis with observational data.In order to exclude confounding variables and reverse causation on causal inference, MR analysis was used to ascertain the causal relationship between the 25(OH)D level and anemia.21 To ensure the strength of instruments in the MR analysis, the largest known GWAS meta-analysis yielded the genetic instrumental variable of 25(OH)D.22 The MR-PRESSO and MR-Egger regression intercept term tests were used to identify and rule out horizontal pleiotropy. Non-overlapping exposure and outcome summary-level data were employed, together with a bidirectional Two-Sample MR design, to prevent bias. Notably, non-linear connections and subgroup analyses could not be carried out because MR analysis relied on summary statistics rather than raw data. We addressed the shortcomings of MR in evaluating dose-response correlations in this investigation by gathering and compiling a single-center local database, doing corresponding analyses, and supplementing it. We have a deeper grasp of the complex association between 25(OH)D levels and anemia risk thanks to our study design, which combines broad MR analysis across varied populations with observational analysis. This thorough method successfully handles issues with confounding in observational research and supports the validity of our findings.
Potential Molecular Mechanisms
Comprehending the intricate genesis of anemia is crucial due to its extensive occurrence and significant consequences.23 Amid known risk factors, 25(OH)D, has garnered attention recently due to its possible connection to anemia.24 Our research provides insights into fundamental mechanisms and goes beyond association to clarify the possible causative relationship between anemia and 25(OH)D. It’s likely that complex physiological systems play a role in the interaction between vitamin D and anemia. Iron metabolism, inflammation-associated anemia, and immunological regulation are all impacted by vitamin D, as evidenced by the receptors for the hormone found in immune cells and erythroid progenitors.25 Moreover, the role that vitamin D plays in the survival and development of red blood cells offers an additional possible influence on the risk of anemia.26 The basis for comprehending the relationship between 25(OH)D levels and anemia outcomes is provided by these molecular theories.
Limitations and Future Directions
While our local database predominantly includes Asian populations, the regional focus of MR analysis on European populations is a noteworthy constraint, notwithstanding the study’s merits. The lack of Asian-specific MR analysis highlights a weakness in our research and calls for care when extrapolating the results. Comprehensive subgroup exploration and generalizability are hindered by the utilization of summary statistics in MR analysis and the dependence on a single-center local database. Our research sheds light on the possible connection between anemia and 25(OH)D, although it does not fully explain the molecular processes involved. These restrictions highlight the necessity of interpreting data carefully and offer potential directions for further study, particularly in varied groups.
Conclusions
In summary, our research has yielded strong evidence that increased 25(OH)D levels independently lowered the incidence of anemia in the participants under examination, indicating that 25(OH)D may serve as a causative protective factor against anemia. These findings, which suggest that regulating 25(OH)D levels through supplementation or lifestyle modifications may be a useful tactic for reducing the prevalence of anemia, especially in susceptible populations, have significant therapeutic ramifications.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Medical Ethics Committee of the Second Hospital of Shandong University [No. KYLL-2023(KJ)P-1792, 2023-10-20].
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Acknowledgments
We would like to thank all participants for their time and excellent cooperation, especially sincerely thank the Physician Scientist Team for their enthusiastic and meticulous teaching and guidance on Mendelian randomization study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. World Health Organization 2011. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity, Available from: https://www.who.int/publications/i/item/WHO-NMH-NHD-MNM-11.1.
2. Chaparro CM, Suchdev PS. Anemia epidemiology, pathophysiology, and etiology in low- and middle-income countries. Ann N Y Acad Sci. 2019;1450(1):15–31. doi:10.1111/nyas.14092
3. Kassebaum NJ, Jasrasaria R, Naghavi M, et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood. 2014;123(5):615–624. doi:10.1182/blood-2013-06-508325
4. Li M, Hu Y, Mao D, et al. Prevalence of Anemia among Chinese Rural Residents. Nutrients. 2017;9(3):192. doi:10.3390/nu9030192
5. World Health Organization. Global targets 2025. Available from: http://www.who.int/nutrition/topics/nutrition_globaltargets2025/en/.
6. Smith EM, Tangpricha V. Vitamin D and anemia: insights into an emerging association. Curr Opin Endocrinol Diab Obes. 2015;22(6):432–438. doi:10.1097/MED.0000000000000199
7. L Bishop E, Ismailova A, Dimeloe S, Hewison M, White JH. Vitamin D and Immune Regulation: antibacterial, Antiviral, Anti-Inflammatory. JBMR Plus. 2021;5(1):e10405. doi:10.1002/jbm4.10405
8. Soepnel LM, Mabetha K, Draper CE, et al. A Cross-Sectional Study of the Associations between Biomarkers of Vitamin D, Iron Status, and Hemoglobin in South African Women of Reproductive Age: the Healthy Life Trajectories Initiative, South Africa. Curr Dev Nutr. 2023;7(5):100072. doi:10.1016/j.cdnut.2023.100072
9. Stallhofer J, Veith L, Diegelmann J, et al. Iron Deficiency in Inflammatory Bowel Disease Is Associated With Low Levels of Vitamin D Modulating Serum Hepcidin and Intestinal Ceruloplasmin Expression. Clin Transl Gastroenterol. 2022;13(1):e00450. doi:10.14309/ctg.0000000000000450
10. Koren Y, Lubetzky R, Mandel D, et al. Hepcidin, and Vitamin D in Healthy Preterm Infants: a Pilot Study. Am J Perinatol. 2023;40(5):508–512. doi:10.1055/s-0041-1729556
11. Zhang Y, Wang X, Wang J, et al. The Association between Standardized Serum 25-Hydroxyvitamin D Concentration and Risk of Anemia: a Population-Based Cross-Sectional Study. Int J Clin Pract. 2022;2022:8384306. doi:10.1155/2022/8384306
12. De la Cruz-Gongora V, Salinas-Rodriguez A, Flores-Aldana M, Villalpando S. Etiology of Anemia in Older Mexican Adults: the Role of Hepcidin, Vitamin A and Vitamin D. Nutrients. 2021;13:3814. doi:10.3390/nu13113814
13. Zhang C, Wang J, Xie X, Sun D. Low serum vitamin D concentration is correlated with anemia, microinflammation, and oxidative stress in patients with peritoneal dialysis. J Transl Med. 2021;19(1):411. doi:10.1186/s12967-021-03077-w
14. Mountjoy E, Schmidt EM, Carmona M, et al. An open approach to systematically prioritize causal variants and genes at all published human GWAS trait-associated loci. Nat Genet. 2021;53(11):1527–1533. doi:10.1038/s41588-021-00945-5
15. Manousaki D, Mitchell R, Dudding T, et al. Genome-wide Association Study for Vitamin D Levels Reveals 69 Independent Loci. Am J Hum Genet. 2020;106(3):327–337. doi:10.1016/j.ajhg.2020.01.017
16. Mukamal KJ, Stampfer MJ, Rimm EB. Genetic instrumental variable analysis: time to call mendelian randomization what it is. The example of alcohol and cardiovascular disease. Eur J Epidemiol. 2020;35(2):93–97. doi:10.1007/s10654-019-00578-3
17. Bowden J, Holmes MV. Meta-analysis and Mendelian randomization: a review. Res Synth Methods. 2019;10(4):486–496. doi:10.1002/jrsm.1346
18. Lips P, Cashman KD, Lamberg-Allardt C, et al. Current Vitamin D Status in European and Middle East and African Countries and Strategies to Prevent Vitamin D Deficiency: a Position Statement of the European Calcified Tissue Society. Eur J Endocrinol. 2019;180(4):23–54.
19. Mogire RM, Muriuki JM, Morovat A, et al. Vitamin D Deficiency and Its Association with Iron Deficiency in African Children. Nutrients. 2022;14:1372. doi:10.3390/nu14071372
20. Si S, Peng Z, Cheng H, et al. Association of Vitamin D in Different Trimester with Hemoglobin during Pregnancy. Nutrients. 2022;14:2455. doi:10.3390/nu14122455
21. Li P, Wang H, Guo L, et al. Association between gut microbiota and preeclampsia-eclampsia: a two-sample Mendelian randomization study. BMC Med. 2022;20(1):443. doi:10.1186/s12916-022-02657-x
22. Timmer T, Tanck MWT, Huis I, et al. Associations between single nucleotide polymorphisms and erythrocyte parameters in humans: a systematic literature review. Mutat Res Rev Mutat Res. 2019;779:58–67. doi:10.1016/j.mrrev.2019.01.002
23. Debnath A, Rehman T, Ghosh T, Kaur A, Ahamed F. Prevalence of Anemia Among Elderly Population Residing in an Urban Area of West Bengal: A Community-Based Cross-Sectional Analytical Study. Indian J Com Med. 2022;47(4):604–608. doi:10.4103/ijcm.ijcm_522_22
24. Ernst JB, Tomaschitz A, Grubler MR, et al. Vitamin D Supplementation and Hemoglobin Levels in Hypertensive Patients: A Randomized Controlled Trial. Int J Endocrinol. 2016;2016:6836402. doi:10.1155/2016/6836402
25. Thirunavukkarasu R, Chitra A, Asirvatham A, Jayalakshmi M. Association of Vitamin D Deficiency and Vitamin D Receptor Gene Polymorphisms with Type 1 Diabetes Risk: a South Indian Familial Study. J Clin Res Pediatr Endocrinol.
26. Gupta V, Mishra S, Gazala MP, Vandana KL, Ratre MS. Serum Vitamin D level and its association with red blood cell indices in patients with periodontitis. J Indian Soc Periodontol. 2022;26(5):446–450. doi:10.4103/jisp.jisp_443_21
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.