Back to Journals » Patient Preference and Adherence » Volume 19
Association Between Receiving Medication Information and Adherence to Antihypertensive Medication: Findings from the 2023 Indonesian Health Survey
Authors Alfian SD ![]() , Candradewi-SF, Griselda M
, Candradewi-SF, Griselda M ![]() , Insani WN
, Insani WN ![]() , Sweileh W
, Sweileh W ![]() , Abdulah R
, Abdulah R
Received 1 August 2025
Accepted for publication 21 November 2025
Published 19 December 2025 Volume 2025:19 Pages 4141—4151
DOI https://doi.org/10.2147/PPA.S557301
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ramón Morillo-Verdugo
Sofa D Alfian,1– 3 Susan F Candradewi,1 Meliana Griselda,1 Widya Norma Insani,1,2 Waleed Sweileh,4 Rizky Abdulah1,2
1Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jatinangor, Indonesia; 2Center of Excellence for Pharmaceutical Care Innovation, Universitas Padjadjaran, Jatinangor, Indonesia; 3Center for Health Technology Assessment, Universitas Padjadjaran, Jatinangor, Indonesia; 4Department of Physiology, Pharmacology and Toxicology, College of Medicine and Health Sciences, An-Najah National University, Nablus, Palestine
Correspondence: Sofa D Alfian, Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, Indonesia, Tel +62 22 84288888, Email [email protected]
Purpose: Effective management of hypertension requires consistent and long-term therapy. In Indonesia, the association between medication information from healthcare providers and adherence to antihypertensive therapy has not been examined. This study aimed to analyze the relationship between receiving antihypertensive medication information and medication adherence among adults with hypertension in Indonesia.
Methods: A cross-sectional analysis was conducted using secondary data from the 2023 Indonesian Health Survey. Baseline characteristics were described using descriptive statistics. Medication non-adherence, receipt of antihypertensive medication information, and potential confounders such as gender, age, education level, marital status, occupation, and island of residence were assessed through self-reported single-item measures. The association between lack of information and medication non-adherence was examined using binary logistic regression adjusted for confounders. Both Crude (COR) and Adjusted Odds ratios (AORs) with corresponding 95% confidence intervals (CIs) were reported.
Results: Among 53,668 patients, most were female (66.3%), married (77.4%), aged over 35 years (95.3%), and unemployed (40.9%). The majority (68.1%) had received information emphasizing the need for regular antihypertensive medication. A lack of information about the necessity of long-term antihypertensive treatment was significantly associated with medication non-adherence (AOR=5.05; 95% CI=4.84– 5.26).
Conclusion: This study demonstrates a strong association between a lack of information regarding long-term antihypertensive medication and non-adherence among hypertensive patients in Indonesia. Therefore, there is a need for improved communication strategies between patients and healthcare providers to improve long-term medication adherence.
Keywords: hypertension, antihypertensive, medication adherence, Indonesian Health Survey
Introduction
Hypertension is a major modifiable risk factor for cardiovascular disease and stroke, accounting for 1.16 million deaths and 21.5 million disability-adjusted life-years lost globally in 2019.1–3 The World Health Organization reports that 1.28 billion people globally suffer from hypertension, with two-thirds of them living in low and middle-income country (LMICs).4 Effective management for hypertensive patients requires a combination of long-term treatment and lifestyle modifications.4
Although various sociodemographic factors may influence the incidence of hypertension,5 medication adherence remains a critical component in managing the condition and reducing the risk of complications. Medication adherence refers to the extent to which a person’s behavior in taking medication corresponds with agreed recommendations from a healthcare provider.6 Adherence rates are often suboptimal, particularly in LMICs.7 A meta-analysis conducted in Asia estimated that 48% of patients do not adhere to their prescribed antihypertensive medications.8 Similarly, non-adherence rates are typically higher in LMICs compared to high-income countries.8 Non-adherence is a complex, multifactorial behavior influenced by various factors, including the side effects of medications, inadequate understanding of the disease and medications, lack of social support, and socioeconomic status.8–12
Studies indicate that a lack of information regarding medication can lead to non-adherence, whereas sufficient knowledge is positively associated with adherence.13–15 Medication information refers to essential communication provided to patients about their prescribed drugs, including the purpose, dosing, side effects, warnings, as well as risk and benefit to ensure safe and appropriate use16. A study in Ethiopia found that patients with higher knowledge and health literacy levels were more likely to adhere to their medication regimen compared to those with limited understanding.17 A prior study in Indonesia involving 7,920 respondents across various regions found that 87.1% lacked awareness of hypertension treatment, which was attributed to older age, irregular blood pressure monitoring, and low healthcare satisfaction.18 Examining the relationship between receipt of medication information and adherence to antihypertensive therapy is important for identifying key factors that can inform strategies to reduce medication non-adherence.
Previous studies in Indonesia assessing the relationship between receiving information regarding regular antihypertensive medication use and non-adherence were limited and involved relatively small populations.19–21 Thus, the relationship between exposure to medication information and adherence among hypertensive patients in Indonesia warrants further investigation. Poor adherence to antihypertensive therapy exacerbates the burden of uncontrolled hypertension and related non-communicable diseases (NCDs).22 Moreover, medication non-adherence could create a barrier to the advancement of medicine by limiting the benefits of evidence-based medicine.23 Medication non-adherence can lead to poor clinical outcomes, increased morbidity and mortality, and a significant rise in healthcare costs24–27 This directly undermines progress toward Sustainable Development Goals (SDG) 3.4, which targets the reduction of premature mortality from NCDs. Integrating these strategies into national health agendas can significantly enhance patient outcomes and accelerate progress toward the SDG. This study aimed to evaluate the association between receiving medication information and adherence to antihypertensive medication within the broader Indonesian population of hypertensive patients.
Materials and Methods
This study is presented following the cross-sectional studies guidelines: Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)28 (Table S1).
Study Design and Data Source
The study employed an observational cross-sectional design using nationwide secondary data from the 2023 Indonesian Health Survey. Ethical approval for the 2023 Indonesian Health Survey was obtained from the Health Research Ethics Committee of Health Polytechnic Jakarta, Ministry of Health, Indonesia (Approval Number LB.02.01/I/KE/287/2023).29 The Indonesian Ministry of Health conducted the survey as an integrated study encompassing basic health research, child nutritional status, biomedical assessments, and dental and oral health. The resulting data were made publicly accessible through their official website.30 Data collection involved face-to-face interviews conducted across 34,500 census blocks in all 38 provinces of Indonesia.30 The survey instrument was structured into three sections: place introduction, individual interview, and personal information. The personal information interview consists of ten sections, including one dedicated to non-communicable diseases.
Study Population and Data Collection
The survey employed a stratified multi-stage cluster sampling technique. From a total sample size of 877,531 in the survey, the selection process was as follows:
Stage 1: Census Block Selection
Census blocks were selected proportionally to size (PPS) based on the number of families recorded in the 2020 population census. The selection process adhered to an allocation table specific to each urban/rural stratum within each district/municipality. Standard census results from the 2020 population census served as the foundation for selecting these census block samples.
Stage 2: Household Selection
From an updated list of households, two distinct samples were drawn: (1) a sample of non-infant households, designated as n1, and (2) a sample of infant households, designated as n2. To ensure a representative sample, systematic sampling was employed, incorporating implicit stratification based on the educational level of the household head.
The 2023 Indonesian Health Survey underwent both internal and external validation. Internal validation was conducted through structured training, supervision, monitoring, evaluation, and direct discussions involving provincial and city technical officers, as well as enumerators. Additionally, the survey incorporated external validation by independent parties unaffiliated with the Ministry of Health. This involved observation and assessment of both the training sessions and the data collection processes during the survey.
Sample Selection
Individuals were included in this study if they were at least 15 years old, had a prior diagnosis of hypertension from a general practitioner confirmed by blood pressure measurements exceeding 140/90 mmHg,31 and had resided within the selected cluster for a minimum of one month to ensure familiarity with the local context and health services. Respondents who declined to participate or had incomplete data on their hypertension status or medication adherence were excluded. Respondents’ selection process is presented in the Figure 1.
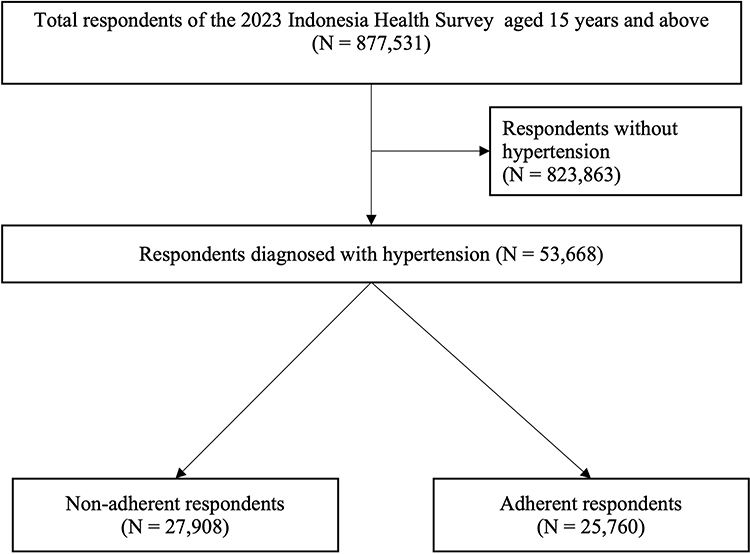 |
Figure 1 Respondents’ selection process. |
Dependent Variable: Medication Adherence
Medication adherence was assessed using a single self-reported item using a structured questionnaire. The question included “Do you take antihypertensive medication?” with response options of “Yes, regularly”, “Yes, but not regularly”, and “No”. Respondents who reported not taking their medication regularly and not taking their medicine were classified as non-adherent. Conversely, those who consistently took their medication were classified as adherent. Responses were interpreted as reflecting the respondent’s typical medication-taking behaviour at the time of the survey. The use of single-item self-report measures for medication adherence has been reported in previous studies, with evidence showing that a single adherence question can predict clinical outcomes.32,33
Main Independent Variable: Exposure to Information Regarding Antihypertensive Medication
Exposure to information about antihypertensive medication was assessed through the question “Have you ever received information or explanation regarding antihypertensive medication should be taken continuously?”. Responses were classified as either “Yes” or “No”. Respondents who answered “No” were classified as having no exposure to information about antihypertensive medication. Studies specifically evaluating medication information are scarce. However, the use of a single-item self report question to assess unmet medication information needs has been reported in prior research.34
Potential Confounders
Socio-demographic factors such as gender (male, female), age (15–35 years, over 35 years), education level (no formal education to primary school, high school to higher degree), marital status (not married, married), occupation (unemployed, government/private sector employee, self-employed, farmer/fisherman, laborer/driver/helper, other), and island of residence (Sumatra, Java and Bali, Kalimantan, Nusa Tenggara, Maluku, Papua) were considered as potential confounders according to previous studies.13,35–37 These variables were selected to adjust for potential socio-demographic influences on adherence behavior and access to medication-related information.
Data Analysis
The baseline characteristics of patients were analyzed using descriptive statistics, represented as percentages and proportions. Missing data were handled using complete case analysis. This bivariate analysis was performed using a chi-square test to explore the association between independent and dependent variables. The first multivariate model included potential covariates associated with the outcome at a significance level of p < 0.25 in the bivariate analysis to avoid excluding potentially relevant predictors. Given the large sample size, statistical significance in chi-square tests may reflect small differences. Therefore, interpretation focused on the adjusted models, which provide a more accurate estimation of the associations. Multivariate binary logistic regression was utilized to assess the relationship between receiving information regarding antihypertensive medications and covariate factors related to patient non-adherence. Both Crude (COR) and Adjusted Odds ratios (AORs) with corresponding 95% confidence intervals (CIs) were reported. SPSS version 27 was used for all data analyses.
Ethics Statement
Ethical approval for the 2023 Indonesian Health Survey was obtained from the Health Research Ethics Committee at Health Polytechnics Jakarta (Approval Number LB.02.01/I/KE/287/2023). Informed consent was obtained from all respondents prior to participation. Ethical considerations, including anonymity and confidentiality, were meticulously addressed. These measures were implemented in accordance with the Law of the Republic of Indonesia No. 27 of 2022 concerning Personal Data Protection.38 According to the 2022 Standard Operating Procedures of the Research Ethics Committee at Universitas Padjadjaran, Indonesia (No. POB/08/KEP), research involving existing data, publicly available documents, or pathological and diagnostic specimens that protect participants’ identities is exempt from ethical review requirements.
Results
Respondents’ Sociodemographic Characteristics
The 2023 Indonesian Health Survey included 877,531 individuals aged 15 years and above (Figure 1). However, 823,863 of these individuals did not have hypertension and were therefore excluded, resulting in a final sample of 53,668 patients with hypertension for this study. According to Table 1, over half of the respondents—27,908 (52%)—were non-adherent. Most of respondents were female (66.3%), married (77.4%), over 35 years old (95.2%), had attained only a primary school education or no formal education (65.4%), were unemployed (40.9%), resided in Java and Bali Island (35.2%), had been diagnosed with hypertension for 0–3 years (32.1%), and had received information emphasizing the importance of regular use of antihypertensive medication (68.1%). Table 2 outlines major reasons for non-adherence, including feeling healthy (58.9%), lack of motivation or forgetfulness (21.2%), and the use of traditional medicine (10.7%).
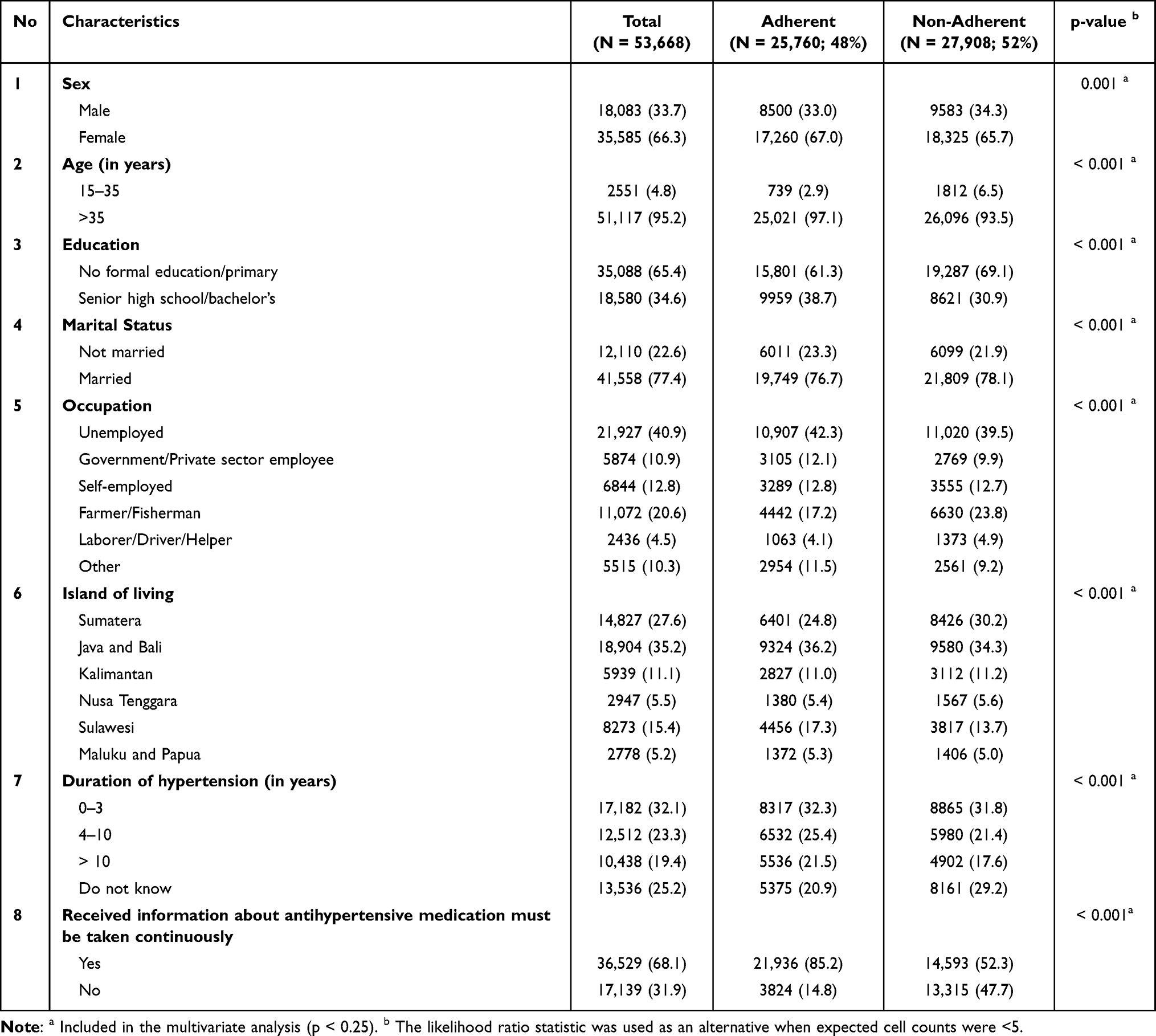 |
Table 1 Respondents’ Characteristics |
 |
Table 2 Reasons for Medication Non-Adherence Among Respondents (N=27,908) |
Association Between the Reception of Information About Antihypertensive Medication and Medication Non-Adherence
After adjusting for age, education, marital status, occupation, islands of residence, and duration of hypertension (Table 1), not receiving information about the continuous use of antihypertensive medication was significantly associated with medication non-adherence (AOR=5.05; 95% CI=4.84–5.26; p-value = 0.000) (Table 3). The Hosmer–Lemeshow test indicated good model calibration (p = 0.063), suggesting that the model fit the data adequately. The pseudo R2 value was relatively low (0.1111), indicating that only a modest proportion of the variability in medication adherence was explained by the observed independent variables. The area under the receiver operating characteristic curve (AUC) was 0.713, demonstrating acceptable discriminative ability of the model in distinguishing between adherent and non-adherent respondents.
 |
Table 3 Multivariate Binary Logistic Regression Analysis of Association Between Exposure to Antihypertensive Information with Medication Non-Adherence |
Discussion
We observed that more than half of the respondents (52.0%) exhibited non-adherence to antihypertensive medication. This proportion aligns with findings from previous Indonesian studies, which reported non-adherence to antihypertensive medication ranging from 45.5% to 93.6%.39,40 After adjusting for confounding variables, a lack of information about the importance of regular antihypertensive medication use was significantly associated with non-adherence. This study extends previous evidence by employing nationally representative data, offering new insights into how medication information influences adherence to antihypertensive therapy.
Limited exposure to information about the importance of long-term antihypertensive medication use is consistently associated with the persistent issue of medication non-adherence.41–43 Our findings revealed that although 68.1% of respondents reported being exposed to information about the long-term use of antihypertensive medication, the prevalence of non-adherence remained high. This aligns with broader national trends, as demonstrated by a nationwide study in Indonesia reported that 87.1% of 7,920 patients with hypertension had low awareness of treatment-related information.18
Our findings confirm earlier studies37,44 that identified a lack of information as a key factor in medication non-adherence, and extend this evidence using a large, nationally representative dataset. Furthermore, previous research highlighted the relationship between patients’ knowledge and adherence, revealing that a moderate level of knowledge was associated with full adherence.45 Knowledge reflects patients’ awareness and understanding of their medication, while health literacy encompasses the broader capacity to access, comprehend, and apply such information in daily health decisions.46 The significant association found in this study indicates that inadequate medication information strongly contributes to non-adherence, underscoring the importance of effective patient education aimed not only at improving knowledge but also at enhancing health literacy.
This aligns with the World Health Organization (WHO) framework, which identifies low health literacy, such as a limited understanding of therapy goals, proper medication administration, and general medication knowledge, as a significant contributor to non-adherence.47, Patients’ medication beliefs, as a result of information exposure, were reported to have a significant association with disease perception, knowledge, and medication adherence.40 Receiving information about the importance of long-term antihypertensive medication is a crucial step in raising awareness of one’s condition, improving perceptions of the necessity and benefits of medication, reducing misconceptions, and ultimately fostering more consistent adherence.21,48 Strengthening medication literacy particularly through community-based education and digital health interventions not only improves adherence but also promotes health equity (SDG 10) by addressing disparities in access to information across socioeconomic and geographic groups. In line with SDG 17’s emphasis on strengthening partnerships, multi-sectoral collaboration is considered essential for implementing scalable, culturally adapted adherence programs in LMICs.49
A lack of information regarding antihypertensive medication may be attributed to various factors, including older age, depressive symptoms, sleep disturbances, inadequate engagement in blood pressure management, and dissatisfaction with health care services.18 In the recent study, respondents cited primary reasons for medication non-adherence, including a feeling of well-being, lack of motivation, forgetfulness, and concurrent use of traditional medicine. These align with the Health Belief Model, where perceived barriers and low perceived susceptibility play a key role in treatment non-adherence.50
Our findings are also consistent with previous qualitative studies in Congo, where patients with hypertension often take antihypertensives only when symptoms arise, discontinuing treatment upon symptom relief.9 This may be rooted in a misunderstanding of hypertension, in which patients mistakenly believe a lack of symptoms equates to controlled blood pressure51 or a mistaken positive self-perception of their health.52 Similarly, studies in Cairo and Pakistan found that a significant proportion of participants were non-adherent due to being asymptomatic.51,53 Patients who seek knowledge about hypertension, including its risks and the benefits of treatment, are generally more aware of the importance of medication adherence.54,55 Healthcare providers are on the frontline to provide medication information for patients. Previous studies have identified various strategies to improve patients’ medication knowledge, including daily educational materials delivered via WhatsApp groups56 and pharmacist-led interventions provided through counselling sessions that focus on treatment goals, the importance of adherence, and strategies for managing potential side effects.57 These interventions may also incorporate the teach-back method, which involves assessing patients’ comprehension of the information provided.58 A customized and tailored approach based on patients’ backgrounds (e.g., age, gender, education level) also plays a key role in the success rate of interventions.59 One study reported that most patients in the intervention group preferred accessing educational materials through digital platforms,56 highlighting the potential of telepharmacy as an effective tool.60 In Indonesia, digital health literacy among the older population remains modest. While 87% of adults aged 60 years and older reported using a mobile phone monthly, only 16% accessed health applications, and 51% experienced difficulties using mobile apps.61 Therefore, digital interventions for medication adherence should utilize accessible platforms with simplified designs tailored to the target population.61
This study also underscores the urgent need for targeted interventions, such as communication skills training for healthcare providers and behavior change communication strategies directed at the community,62 to effectively address the underlying factors of medication non-adherence due to a lack of exposure to information. These interventions must focus on improving the perception and awareness of hypertension, not only among patients but also among healthcare providers.63 These efforts should be integrated into national health policies by strengthening primary care communication protocols and adding structured patient education programs within the public health system, for example, using incentives for enhanced pharmacist service as in the new medication service (NMS) and medication use review program to support adherence for patients with long-term conditions in the United Kingdom.64
Digital health interventions, including telemedicine platforms, digital devices, and mHealth applications, have shown promising results in providing patients with sufficient information and improving adherence.65–67 For instance, telepharmacy can facilitate consistent medication reminders and online counseling with a pharmacist, even at a distance.60 In offline settings, healthcare providers can provide both brief and extended interviews as interventions to enhance patient involvement in medication decision-making and address concerns regarding medication use.68,69 Furthermore, healthcare providers should prioritize modifiable factors when developing strategies and implementing personalized approaches. This includes fostering two-way communication to educate patients and assessing their understanding of treatment plans.18,70 Education and counselling have been shown to be effective in clarifying misunderstandings and enhancing patients’ knowledge of hypertension treatment, whether delivered in direct or indirect settings.71
The strength of this study is its use of a nationally representative dataset, which enhances the generalisability and external validity of the findings. It provides valuable insights into the association between a lack of information regarding the need for regular antihypertensive medication use and medication non-adherence across a wide age range, from young adolescents to older adults with hypertension. These findings have the potential to address knowledge gaps among patients that may be hindering medication adherence.
However, this study has several limitations. First, medication adherence was assessed using a single self-reported item, which may have introduced recall and social desirability bias compared with clinical records maintained by healthcare providers. Second, the use of a binary yes/no variable to capture information receipt may have underestimated the extent or frequency of information actually received by patients. Third, the cross-sectional design limits the ability to establish causality or determine the direction of associations. Fourth, the analysis did not apply sampling weights, which may slightly affect the accuracy of the estimated associations. Nevertheless, as the data were derived from a nationally representative survey, this limitation is unlikely to substantially compromise the representativeness of the findings. Lastly, the database lacked information on other potentially relevant factors, including comorbidities,72,73 false belief regarding antihypertensive medications,74 patient-provider relationship,75 prevention type,76 type of antihypertensive regiments (monotherapy vs combination therapy),77 adverse drug reaction,78 and the level of family and friends support,37 all of which might have been associated with non-adherence to antihypertensive medications.
Future longitudinal studies examining the relationship between information exposure and medication adherence should incorporate sampling weights, include larger and more diverse population samples, and include blood pressure as an important clinical indicator of treatment effectiveness. Furthermore, future studies are needed to develop tailored strategies for improving medication information exposure, e.g., digital health interventions such as mobile-based reminders, telepharmacy, or online patient education platforms which may serve as potential tools to enhance information delivery and support adherence.
Conclusion
This study demonstrates a strong association between lack of information about long-term antihypertensive medication use and non-adherence among hypertensive patients in Indonesia. These findings highlight the importance of effective information dissemination to support adherence to antihypertensive therapy. Enhancing patients’ access to and understanding of medication information is essential to reduce the burden of uncontrolled hypertension, which remains a major contributor to complications and mortality.
Abbreviations
LMIC, Low- to Middle-Income Country; NCD, Non-communicable Disease; NMS, New Medication Service; PPS, Probability Proportional to Size; SKI, Indonesian Health Survey; SDG, Sustainable Development Goal; SPSS, Statistical Package for Social Sciences; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; WHO, World Health Organization.
Data Sharing Statement
The data used in this study are publicly available from the 2023 Indonesian Health Survey (SKI). The data can be accessed at https://www.badankebijakan.kemkes.go.id/hasil-ski-2023/.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16(4):223–237. doi:10.1038/s41581-019-0244-2
2. Roth GA, Johnson C, Abajobir A, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70(1):1–25. doi:10.1016/j.jacc.2017.04.052
3. Abegaz TM, Shehab A, Gebreyohannes EA, Bhagavathula AS, Elnour AA. Nonadherence to antihypertensive drugs. Medicine. 2017;96(4):e5641. doi:10.1097/MD.0000000000005641
4. World Health Organization. Hypertension [Internet]; 2023 [cited May 3, 2025]. Available from: https://www.who.int/news-room/fact-sheets/detail/hypertension.
5. Alfaqeeh M, Alfian S, Abdulah R. Factors associated with hypertension among adults: a cross-sectional analysis of the Indonesian family life survey. Vasc Health Risk Manag. 2023;19:827–836. doi:10.2147/VHRM.S438180
6. Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. Geneva, Switzerland: World Health Organization; 2003.
7. Osamor PE, Owumi BE. Factors associated with treatment compliance in hypertension in Southwest Nigeria. J Health Popul Nutr. 2012;29(6). doi:10.3329/jhpn.v29i6.9899
8. Mahmood S, Jalal Z, Hadi MA, Khan TM, Haque MS, Shah KU. Prevalence of non-adherence to antihypertensive medication in Asia: a systematic review and meta-analysis. Int J Clin Pharm. 2021;43(3):486–501. doi:10.1007/s11096-021-01236-z
9. Fina Lubaki JP, Mabuza L, Malete N, Maduna P, Ndimande JV. Reasons for non-compliance among patients with hypertension at Vanga Hospital, Bandundu Province, Democratic Republic of Congo: a qualitative study. Afr J Prim Health Care Fam Med. 2009;1(1). doi:10.4102/phcfm.v1i1.68
10. Neiman AB, Ruppar T, Ho M, et al. CDC grand rounds: improving medication adherence for chronic disease management — innovations and opportunities. MMWR Morb Mortal Wkly Rep. 2017;66(45):1248–1251. doi:10.15585/mmwr.mm6645a2
11. Yang C, Hui Z, Zeng D, Liu L, Lee DTF. Examining and adapting the information–motivation–behavioural skills model of medication adherence among community-dwelling older patients with multimorbidity: protocol for a cross-sectional study. BMJ Open. 2020;10(3):e033431. doi:10.1136/bmjopen-2019-033431
12. Gikunda CN, Gitonga L. Patients Related Factors Associated with Non-Adherence to Antihypertensive Medication among Patients at Chuka Referral Hospital, Kenya. Open J Clin Diagn. 2019;09(03):90–113. doi:10.4236/ojcd.2019.93007
13. Abbas H, Kurdi M, de Vries F, et al. Factors associated with antihypertensive medication non-adherence: a cross-sectional study among Lebanese hypertensive adults. Patient Prefer Adherence. 2020;14:663–673. doi:10.2147/PPA.S238751
14. Boima V, Ademola AD, Odusola AO, et al. Factors associated with medication nonadherence among hypertensives in Ghana and Nigeria. Int J Hypertens. 2015;2015:1–8. doi:10.1155/2015/205716
15. Mekonnen GB, Gelayee DA. Low medication knowledge and adherence to oral chronic medications among patients attending community pharmacies: a cross‐sectional study in a low‐income country. Biomed Res Int. 2020;2020(1). doi:10.1155/2020/4392058
16. Russell AM, Lovett R, Vogeley A, et al. Evidence-based design of prescription medication information: an updated scoping review. Drug Saf. 2025;48(6):607–641. doi:10.1007/s40264-025-01527-8
17. Teshome DF, Bantie Bekele K, Habitu Y, Addis Gelagay A. Medication adherence and its associated factors among hypertensive patients attending the Debre Tabor General Hospital, northwest Ethiopia. Integr Blood Press Control. 2017;10:1–7. doi:10.2147/IBPC.S128914
18. Khoiry QA, Alfian SD, Abdulah R. Modifiable and non-modifiable factors associated with low awareness of hypertension treatment in Indonesia: a cross-sectional population-based national survey. Glob Heart. 2022;17(1). doi:10.5334/gh.1143
19. Ardiansyah R, Zukhruf Saputri G, Supadmi W, Candradewi SF, Hastuti D, Ardhiani M. The relationship between level of knowledge and adherence therapy in hypertensive patients at Ramadhan Pharmacy in Yogyakarta City. Int J Health Sci Technol. 2023;5(2):166–173. doi:10.31101/ijhst.v5i2.3411
20. Tania T, Yunivita V, Afiatin A. Adherence to antihypertensive medication in patients with hypertension in Indonesia. Int J Integrat Health Sci. 2019;7(2):74–80. doi:10.15850/ijihs.v7n2.1588
21. Tursina H, Sya’id A, Fatarona A. Factors Associated with Medication Adherence in Hypertensive Patients in Rural Areas. Jurnal Kesehatan Dr Soebandi. 2024;12(2):125–134. doi:10.36858/jkds.v12i2.773
22. Guo A, Jin H, Mao J, et al. Impact of health literacy and social support on medication adherence in patients with hypertension: a cross-sectional community-based study. BMC Cardiovasc Disord. 2023;23(1):93. doi:10.1186/s12872-023-03117-x
23. Kardas P, Bennett B, Borah B, et al. Medication non-adherence: reflecting on two decades since WHO adherence report and setting goals for the next twenty years. Front Pharmacol. 2024;15. doi:10.3389/fphar.2024.1444012
24. Burnier M. The role of adherence in patients with chronic diseases. Eur J Intern Med. 2024;119:1–5. doi:10.1016/j.ejim.2023.07.008
25. Burnier M, Egan BM. Adherence in Hypertension. Circ Res. 2019;124(7):1124–1140. doi:10.1161/CIRCRESAHA.118.313220
26. Hamrahian SM, Maarouf OH, Fülöp T. A critical review of medication adherence in hypertension: barriers and facilitators clinicians should consider. Patient Prefer Adherence. 2022;16:2749–2757. doi:10.2147/PPA.S368784
27. Farah R, Alawwa I, Khateeb D, et al. Factors affecting the level of adherence to hypertension medications: a cross-sectional study using the Hill-Bone Questionnaire. Patient Prefer Adherence. 2024;18:893–904. doi:10.2147/PPA.S457026
28. Cuschieri S. The STROBE guidelines. Saudi J Anaesth. 2019;13(Suppl 1):S31–4. doi:10.4103/sja.SJA_543_18
29. Titaley CR, Tjandrarini DH, Malakauseya MLV, et al. Determinants of non-use of antenatal care services in eastern Indonesia: analysis of the 2023 Indonesia health survey. Front Glob Womens Health. 2025;6:1649276. doi:10.3389/fgwh.2025.1649276
30. Indonesian Ministry of Health. Laporan Survei Kesehatan Indonesia (SKI) 2023 [Internet]; 2023 [cited October 12, 2024]. Available from: https://layanandata.kemkes.go.id/katalog-data/ski/ketersediaan-data/ski-2023.
31. Mulyanto J, Kringos DS, Kunst AE. Socioeconomic inequalities in the utilisation of hypertension and type 2 diabetes management services in Indonesia. Trop Med Int Health. 2019;24(11):1301–1310. doi:10.1111/tmi.13303
32. Feldman BJ, Fredericksen RJ, Crane PK, et al. Evaluation of the single-item self-rating adherence scale for use in routine clinical care of people living with HIV. AIDS Behav. 2013;17(1):307–318. doi:10.1007/s10461-012-0326-7
33. Wu JR, DeWalt DA, Baker DW, et al. A single-item self-report medication adherence question predicts hospitalisation and death in patients with heart failure. J Clin Nurs. 2014;23(17–18):2554–2564. doi:10.1111/jocn.12471
34. Walquist MJ, Svendsen K, Garcia BH, et al. Self-reported medication information needs among medication users in a general population aged 40 years and above - the Tromsø study. BMC Public Health. 2022;22(1):2182. doi:10.1186/s12889-022-14573-z
35. Pal B, Dutta A, Chaudhary V, Kumari S, Meenakshi S, Murti K. Prevalence of antihypertensive medication adherence and associated factors in India: a systematic review and meta-analysis. Hipertens Riesgo Vasc. 2024 doi:10.1016/j.hipert.2024.11.005.
36. Andala S, Sofyan H, Hasballah K, Marthoenis. Knowledge and acceptance associated with medication adherence among hypertension individuals in Aceh province, Indonesia. Heliyon. 2024;10(7):e29303. doi:10.1016/j.heliyon.2024.e29303
37. Soesanto E, Ramadlan I, Setyawati D, Aisah S, Pawestri P. Factors affecting medication adherence in hypertension patients: a literature review. Bali Med J. 2021;10(3):1364–1370. doi:10.15562/bmj.v10i3.3038
38. Indonesian Ministry of Health. Frequently asked question SKI 2023 [Internet]; 2024 [cited November 20, 2024]. Available from: https://www.badankebijakan.kemkes.go.id/daftar-frequently-asked-question-seputar-hasil-utama-ski-2023/.
39. Puspitasari IM, Azizah LN, Sinuraya RK, Alfian SD, Abdulah R. Measuring medication adherence of hypertensive patients with monotherapy treatment in a community health center by utilizing medication possession ratio. Pharmacia. 2022;69(2):345–350. doi:10.3897/pharmacia.69.e82330
40. Alfian SD, Annisa N, Fajriansyah F, et al. Modifiable factors associated with non-adherence to antihypertensive or antihyperlipidemic drugs are dissimilar: a multicenter study among patients with diabetes in Indonesia. J Gen Intern Med. 2020;35(10):2897–2906. doi:10.1007/s11606-020-05809-y
41. World Health Organization. First WHO report details devastating impact of hypertension and ways to stop it [Internet]; 2023 [cited May 3, 2025]. Available from: https://www.who.int/news/item/19-09-2023-first-who-report-details-devastating-impact-of-hypertension-and-ways-to-stop-it.
42. Alfian SD, van Boven JFM, Abdulah R, Sukandar H, Denig P, Hak E. Effectiveness of a targeted and tailored pharmacist‐led intervention to improve adherence to antihypertensive drugs among patients with type 2 diabetes in Indonesia: a cluster randomised controlled trial. Br J Clin Pharmacol. 2021;87(4):2032–2042. doi:10.1111/bcp.14610
43. Alfian SD, Annisa N, Perwitasari DA, Coelho A, Abdulah R. The role of illness perceptions on medication nonadherence among patients with hypertension: a multicenter study in Indonesia. Front Pharmacol. 2022;13. doi:10.3389/fphar.2022.985293
44. Listiana D, Effendi S, Saputra YE. Faktor-Faktor yang Berhubungan dengan Kepatuhan Penderita Hipertensi dalam Menjalani Pengobatan di Puskesmas Karang Dapo Kabupaten Muratara (Factors associated with medication adherence among hypertensive patients at Karang Dapo Community Health Center, Muratara Regency). J Nurs Public Health. 2020;8(1):11–22 doi:10.37676/jnph.v8i1.1005.
45. Pristianty L, Hingis ES, Priyandani Y, Rahem A. Relationship between knowledge and adherence to hypertension treatment. J Public Health Afr. 2023;14(1):4. doi:10.4081/jphia.2023.2502
46. WHO. Health literacy [Internet]. Geneva: World Health Organization; 2024 [cited October 14, 2025]. Available from: https://www.who.int/news-room/fact-sheets/detail/health-literacy.
47. Choudhry NK, Kronish IM, Vongpatanasin W, et al. Medication adherence and blood pressure control: a scientific statement from the American heart association. Hypertension. 2022;79(1):E1–14. doi:10.1161/HYP.0000000000000203
48. Jo S, Kim S, Park K, Kim H, Han S, Park W. Self‐blood pressure monitoring is associated with improved awareness, adherence, and attainment of target blood pressure goals: prospective observational study of 7751 patients. J Clin Hypertens. 2019;21(9):1298–1304. doi:10.1111/jch.13647
49. Pedersen AB, Hickmann T, Renn O, et al. SDGs at the halfway point: how the 17 global goals address risks and wicked problems. Ambio. 2023;52(4):679–682. doi:10.1007/s13280-023-01837-0
50. Joho AA. Using the health belief model to explain the patient’s compliance to anti-hypertensive treatment in three district hospitals - Dar es Salaam, Tanzania: a cross section study. East Afr Health Res J. 2021;5(1):50–58. doi:10.24248/eahrj.v5i1.651
51. Youssef G, Mohamed M, Abdel Hamid M, El Remisy D. Reasons behind high rate of non-compliance to scheduled office visits in hypertensive patients: results from the Egyptian registry of specialized hypertension clinics. Egyptian Heart Jl. 2022;74(1):45. doi:10.1186/s43044-022-00285-7
52. Pradipta I, Aprilio K, Ningsih Y, et al. How does indonesian chronic disease patient adhere to their treatment? A cross-sectional analysis of 11,408 subjects. Patient Prefer Adherence. 2025;19:173–184. doi:10.2147/PPA.S503601
53. Yousuf FS, Khan MAA, Bibi R, Arif A, Arshad A, Almas A. Medication adherence in patients with uncontrolled hypertension & hypertensive crisis presenting to a hospital setting in Karachi, Pakistan. Cureus. 2023. doi:10.7759/cureus.33995
54. Ismail M, El-Nayal M, Domiati S. Exploring the impact of subjective well-being on medication adherence: a cross-sectional study among individuals with multiple chronic diseases. Exploratory Res Clin Soc Pharm. 2024;15:100496. doi:10.1016/j.rcsop.2024.100496
55. Tri Wijayanti Y, Sasarari ZA, Sumiyati S, Prasetyowati P, Rusli R. Motivation can improve medication adherence in hypertension patients. Jurnal Edukasi Ilmiah Kesehatan. 2024;2(3):78–85. doi:10.61099/junedik.v2i3.58
56. Atolagbe ET, Sivanandy P, Ingle PV. Effectiveness of educational intervention in improving medication adherence among patients with diabetes in Klang Valley, Malaysia. Front Clin Diabetes Healthcare. 2023;4. doi:10.3389/fcdhc.2023.1132489
57. Alfian SD, Abdulah R, Denig P, van Boven JFM, Hak E. Targeted and tailored pharmacist-led intervention to improve adherence to antihypertensive drugs among patients with type 2 diabetes in Indonesia: study protocol of a cluster randomised controlled trial. BMJ Open. 2020;10(1):e034507. doi:10.1136/bmjopen-2019-034507
58. Ha Dinh TT, Bonner A, Clark R, Ramsbotham J, Hines S. The effectiveness of the teach-back method on adherence and self-management in health education for people with chronic disease: a systematic review. JBI Database Syst Rev Implement Rep. 2016;14(1):210–247. doi:10.11124/jbisrir-2016-2296
59. D’Amore C, Zama B, Salotti R, et al. Improving knowledge on safe medication management of inpatient children and adolescents: a pre-post study. Patient Educ Couns. 2022;105(7):2234–2239. doi:10.1016/j.pec.2022.02.010
60. Alfian SD, Sania JA, Aini DQ, et al. Evaluation of usability and user feedback to guide telepharmacy application development in Indonesia: a mixed-methods study. BMC Med Inform Decis Mak. 2024;24(1):130. doi:10.1186/s12911-024-02494-3
61. Laksmi PW, Dinakrisma AA, Abdiel T, et al. Digital divide: knowledge, attitudes and practices toward mobile phone and apps use among Indonesian older adults residing in a megapolitan city. Gerontechnology. 2024;23(1):1–13. doi:10.4017/gt.2024.23.1.845.03
62. Al-Hazmi AH, Alanazi ADM, Thirunavukkarasu A, et al. Evaluation of hypertension knowledge and its association with medication adherence among hypertensive patients attending primary health centers: a cross-sectional study from eastern Saudi Arabia. Front Public Health. 2025;12. doi:10.3389/fpubh.2024.1378561
63. Sudarman, Dioso R, Harun Z, Hassan HC. Interventions to improve medication adherence in hypertensive patients: a bibliometric analysis. Malaysian J Nurs. 2024;16(Suppl 1):178–191. doi:10.31674/mjn.2024.v16isupp1.017
64. Elliott RA, Boyd MJ, Tanajewski L, et al. “New Medicine Service”: supporting adherence in people starting a new medication for a long-term condition: 26-week follow-up of a pragmatic randomised controlled trial. BMJ Qual Saf. 2020;29(4):286–295. doi:10.1136/bmjqs-2018-009177
65. Avegno KS, Roberson KB, Onsomu EO, Edwards MF, Dean EL, Bertoni AG. Evaluating a telephone and home blood pressure monitoring intervention to improve blood pressure control and self-care behaviors in adults with low-socioeconomic status. Int J Environ Res Public Health. 2023;20(7):5287. doi:10.3390/ijerph20075287
66. Kappes M, Espinoza P, Jara V, Hall A. Nurse-led telehealth intervention effectiveness on reducing hypertension: a systematic review. BMC Nurs. 2023;22(1):19. doi:10.1186/s12912-022-01170-z
67. Yilmaz E, Uzuner A, Bajgora M, et al. Effect of eTansiyon smartphone application on hypertension control. Prim Health Care Res Dev. 2022;23. doi:10.1017/S146342362100058X
68. Huang X, Xu N, Wang Y, Sun Y, Guo A. The effects of motivational interviewing on hypertension management: a systematic review and meta-analysis. Patient Educ Couns. 2023;112:107760. doi:10.1016/j.pec.2023.107760
69. Donovan G, Hall N, Ling J, Smith F, Wilkes S. Influencing medication taking behaviors using automated two‐way digital communication: a narrative synthesis systematic review informed by the Behavior Change Wheel. Br J Health Psychol. 2022;27(3):861–890. doi:10.1111/bjhp.12580
70. Romain M, Sprung CL. Approaches to patients and families with strong religious beliefs regarding end-of-life care. Curr Opin Crit Care. 2014;20(6):668–672. doi:10.1097/MCC.0000000000000148
71. Aulia G, Halimah E, Lestari K. Pharmaceutical counseling has a positive impact on quality of life of hypertension patients. Pharmacol Clin Pharm Res. 2018;3(1). doi:10.15416/pcpr.v3i1.16449
72. Saadat Z, Nikdoust F, Aerab-Sheibani H, et al. Adherence to antihypertensives in patients with comorbid condition. Nephrourol Mon. 2015;7(4). doi:10.5812/numonthly.29863
73. Arukala P. Impact of comorbidities on medication adherence in hypertensive patients. Value Health. 2016;19(7):A615. doi:10.1016/j.jval.2016.09.1546
74. Gebreyohannes EA, Bhagavathula AS, Abebe TB, Tefera YG, Abegaz TM. Adverse effects and non-adherence to antihypertensive medications in University of Gondar Comprehensive Specialized Hospital. Clin Hypertens. 2019;25(1):1. doi:10.1186/s40885-018-0104-6
75. van der Laan DM, Elders PJM, Boons CCLM, Beckeringh JJ, Nijpels G, Hugtenburg JG. Factors associated with antihypertensive medication non-adherence: a systematic review. J Hum Hypertens. 2017;31(11):687–694. doi:10.1038/jhh.2017.48
76. Alfian SD, Denig P, Coelho A, Hak E. Pharmacy-based predictors of non-adherence, non-persistence and reinitiation of antihypertensive drugs among patients on oral diabetes drugs in the Netherlands. PLoS One. 2019;14(11):e0225390. doi:10.1371/journal.pone.0225390
77. Wawruch M, Petrova M, Tesar T, et al. Factors associated with non-adherence to angiotensin-converting enzyme inhibitors and angiotensin receptor blockers in older patients with peripheral arterial disease. Front Pharmacol. 2023;14. doi:10.3389/fphar.2023.1199669
78. Insani WN, Wei L, Abdulah R, et al. Exploring the association of adverse drug reactions with medication adherence and quality of life among hypertensive patients: a cross-sectional study. Int J Clin Pharm. 2025;47(2):354–364. doi:10.1007/s11096-024-01832-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Medication Adherence and Blood Pressure Control Among Hypertensive Outpatients Attending a Tertiary Cardiovascular Hospital in Tanzania: A Cross-Sectional Study
Pallangyo P, Komba M, Mkojera ZS, Kisenge PR, Bhalia S, Mayala H, Kifai E, Richard MK, Khanbhai K, Wibonela S, Millinga J, Yeyeye R, Njau NF, Odemary TK, Janabi M
Integrated Blood Pressure Control 2022, 15:97-112
Published Date: 10 August 2022
A Critical Review of Medication Adherence in Hypertension: Barriers and Facilitators Clinicians Should Consider
Hamrahian SM, Maarouf OH, Fülöp T
Patient Preference and Adherence 2022, 16:2749-2757
Published Date: 7 October 2022
Interventions Incorporating Therapeutic Alliance to Improve Medication Adherence in Black Patients with Diabetes, Hypertension and Kidney Disease: A Systematic Review
Desta R, Blumrosen C, Laferriere HE, Saluja A, Bruce MA, Elasy TA, Griffith DM, Norris KC, Cavanaugh KL, Umeukeje EM
Patient Preference and Adherence 2022, 16:3095-3110
Published Date: 14 November 2022
Patient Pill Organization Strategies and Adherence Measured in a Cross-Sectional Study of Hypertension
Genelin MP, Helmkamp LJ, Steiner JF, Maertens JA, Hanratty R, Vupputuri S, Havranek EP, Dickinson LM, Blair IV, Daugherty SL
Patient Preference and Adherence 2023, 17:817-826
Published Date: 23 March 2023
A Systematic Review of the Hill-Bone Compliance to Blood Pressure Therapy Scale
Commodore-Mensah Y, Delva S, Ogungbe O, Smulcer LA, Rives S, Dennison Himmelfarb CR, Kim MT, Bone L, Levine D, Hill MN
Patient Preference and Adherence 2023, 17:2401-2420
Published Date: 28 September 2023