Back to Journals » Infection and Drug Resistance » Volume 16
Association Between Proton Pump Inhibitor Use and Extended-Spectrum Beta-Lactamase Urinary Tract Infection in Adults: A Retrospective Study
Authors Purayil NK ![]() , Naushad VA
, Naushad VA ![]() , Chandra P, Joseph P, Khalil Z, Zahid M, Wilson G, Kayakkool MK, Ayari B, Chalihadan S, Elmagboul EBI, Doiphode SH
, Chandra P, Joseph P, Khalil Z, Zahid M, Wilson G, Kayakkool MK, Ayari B, Chalihadan S, Elmagboul EBI, Doiphode SH
Received 12 April 2023
Accepted for publication 21 June 2023
Published 29 June 2023 Volume 2023:16 Pages 4251—4258
DOI https://doi.org/10.2147/IDR.S415096
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Nishan Kunnummal Purayil,1– 3 Vamanjore A Naushad,1– 3 Prem Chandra,4 Prakash Joseph,1,2 Zahida Khalil,1,2 Muhammad Zahid,1,3 Godwin Wilson,3,5 Muhammed Kunhi Kayakkool,1– 3 Basma Ayari,1,3 Sajid Chalihadan,1 Emad Bashier I Elmagboul,5 Sanjay H Doiphode3,5
1General Internal Medicine Department, Hamad General Hospital, Hamad Medical Corporation, Doha, Qatar; 2Clinical Department, College of Medicine-QU Health, Qatar University, Doha, Qatar; 3Department of Clinical Medicine, Weill Cornell Medicine-Qatar, Doha, Qatar; 4Medical Research Center, Hamad Medical Corporation, Doha, Qatar; 5Department of Microbiology, Hamad Medical Corporation, Doha, Qatar
Correspondence: Nishan Kunnummal Purayil, General Internal Medicine Department, Hamad General Hospital, Post Box No-3050, Hamad Medical Corporation, Doha, Qatar, Tel +97455792180, Email [email protected]
Purpose: To study the association between proton pump inhibitor (PPI) use and the risk of urinary tract infection (UTI) caused by extended-spectrum beta-lactamase-producing Enterobacteriaceae (ESBL).
Patients and Methods: A retrospective cross-sectional study was conducted between October 2018 and September 2019. Adults with ESBL-UTIs were compared to adults with UTIs caused by gram-negative bacteria (GNB) and those with UTIs caused by miscellaneous organisms. The association between ESBL infection and PPI use was assessed.
Results: A total of 117 of 277 ESBL cases, 229 of 679 non-ESBL GNB controls, and 57 of 144 non-ESBL miscellaneous controls were exposed to PPIs within 3 months prior to admission. The univariate analysis indicated unadjusted odds ratio for PPI exposure with ESBL infection versus the GNB controls was 1.43 (95% CI 1.07– 1.90, P = 0.015) while the odds ratio for PPI exposure with ESBL infection versus miscellaneous organisms was 1.10 (95% CI 0.73– 1.67, P = 0.633) indicating positive association (PPI exposure increases risk of ESBL infection). Multivariate analysis revealed a positive association between ESBL infection and PPI use versus the GNB controls with an odds ratio of 1.74 (95% CI 0.91– 3.31). While Esomeprazole was positively associated with ESBL infection, particularly compared with the miscellaneous group (adjusted OR 1.35, 95% CI 0.47– 3.88), Lansoprazole was inversely associated (adjusted OR 0.48, 95% CI 0.18– 1.24 and adjusted OR 0.40, 95% CI 0.11– 1.41 for ESBL versus GNB controls and ESBL versus miscellaneous organisms, respectively).
Conclusion: Exposure to PPIs in the preceding 3 months showed an association with increased risk of ESBL-UTI. While Esomeprazole showed a positive association, Lansoprazole had an inverse association for ESBL-UTI. Restricting the use of PPIs may be beneficial in the fight against antimicrobial resistance.
Keywords: proton pump inhibitor, PPI, ESBL, extended-spectrum beta-lactamase, urinary tract infections
Introduction
Beta-lactamases are enzymes that cleave the beta-lactam ring and lead to the inactivation of antibiotics. The first plasmid-mediated beta-lactamase TEM-1 in gram-negative bacteria was discovered in Greece in the 1960s.1 TEM-1 and TEM-2 are the most common beta-lactamases found in gram-negative bacteria such as Enterobacteriaceae, Pseudomonas aeruginosa, Haemophilus influenza (H.influenza), and Neisseria gonorrhea. While TEM variants hydrolyze penicillins and narrow-spectrum cephalosporins, they are ineffective against higher-generation cephalosporins with an oxyimino side chain, such as cefotaxime, ceftriaxone, and cefepime. In later years, oxyimino cephalosporin-resistant Klebsiella ozaena strains, named SHV-2, were discovered in Germany.2 These were called extended-spectrum beta-lactamases (ESBL) due to their increased spectrum of activity, particularly against the oxyimino cephalosporins. Another type of beta-lactamase, called CTX-M, has greater activity against cefotaxime and other oxyimino beta-lactams. More than 220 TEM, 190 SHV, and 160 varieties of CTX-M beta-lactamases have been described.3,4 In 1984 and 1988, TEM-related ESBL-producing organisms were detected in France and the United States, respectively.5 The activity of ESBLs against various oxyimino beta-lactam antibiotics varies. They are ineffective against cephamycins (cefoxitin, cefotetan, cefmetazole) and carbapenems (imipenem, meropenem, ertapenem).
ESBL-producing Enterobacteriaceae infections have a global distribution, particularly in specimens from hospital settings. Infection is also increasingly reported in community settings. The prevalence of ESBL infection varies by country. Community-acquired ESBL infection is being increasingly recognized as an important clinical problem in both the US and Europe, with ESBL-Escherichia coli (E coli) being reported among individuals with no healthcare-associated risk factors.6
Urinary tract infection (UTI) is one of the most common infection caused by ESBL-producing organisms and is associated with increased mortality and morbidity. Several risk factors for ESBL-associated UTI have been identified, including demographic factors such as gender and age,7–11 and co-morbid conditions such as diabetes mellitus,7,12,13 renal disease, chronic obstructive pulmonary disease, and malignancy.9 Recent exposure to antibiotics,12–15 hospitalization in the prior 3 months, presence of a urinary catheter, or receipt of an invasive urological procedure in the preceding 3 months are also considered ESBL-UTI risk factors.8,15
Globally, the prevalence of ESBL-UTI has a wide range of distribution. Developed nations reported a significantly lower rate than developing or underdeveloped nations. Norway (2%) and Australia (2.1%) reported the lowest prevalence of ESBL-UTI among the developed nations. In the state of Qatar, a study by Naushad et al reported a prevalence rate of 25.2% for ESBL-UTI among adults. The prevalence rate in the Middle Eastern countries and Arab world was reported to be higher than that from Qatar. The prevalence of ESBL-UTI was 74% in Iraq, while it was 62% and 52% in Jordan and Syria, respectively.13,15
Proton pump inhibitors (PPIs) reduce gastric acidity and are shown to increase the risk of gastrointestinal infections.16,17 Whether PPIs increase the risk of ESBL-UTI in adults is less clear, and there is scarcity of published literature on the potential association. The current study sought to determine whether PPIs increase the risk of ESBL-UTI in adults.
Materials and Methods
Study Design and Setting
This retrospective cross-sectional study was conducted at Hamad General Hospital, Hamad Medical Corporation in Qatar.
Participants
Adult patients with a UTI caused by ESBL-producing Enterobacteriaceae based on the positive urine culture growth of a single pathogen with more than 105 colony-forming units between October 2018 and September 2019 were identified from medical records. This included in-patients, out-patients, and emergency department patients. Individuals with the signs and symptoms of a UTI with insignificant growth, negative urine culture, or mixed growth in urine culture were excluded from the study. Adult patients with a UTI caused by non-ESBL-producing organisms were used as controls. These individuals were divided into two groups, those with non-ESBL gram-negative bacteria and those with miscellaneous organisms.
Data Collection
Demographic, co-morbidity, laboratory, and PPI use data were extracted from the clinical information system using the health-care numbers of each patient.
Exposure
A documented history or prescription of PPIs in the preceding 3 months was noted.
Sample Size
A statistical power calculation prior to data collection indicated that this sample size (245 cases and 245 controls) was adequate to detect an odds ratio (OR) of 3.2 with 80% power at a 5% level of significance.18
Statistical Analysis
Descriptive statistics were used to summarize the data and determine the sample characteristics and patient distribution. Quantitative data and results were reported using the mean and standard deviation (SD). Categorical data were summarized using frequencies and proportions. Associations between two or more qualitative variables (eg, exposure to PPI, comorbidities and their association with ESBL-UTI) were assessed using the Chi-square (χ2) or Fisher Exact test, as appropriate. Quantitative data between two or more independent groups were analyzed using an unpaired t (Mann Whitney U-test for non-normally distributed data) or one-way analysis of variance (ANOVA) (Kruskal Wallis test for non-normally distributed data) test as appropriate.
Univariate and multivariate logistic regression analyses were used to determine and assess the factors associated with ESBL-UTI while adjusting for variables such as age, gender, comorbidities, and the main exposure variable, PPI use. Predictor variables were included in the multivariate logistic regression models while considering both statistical and clinical significance. The logistic regression analysis results were presented as odds ratios (OR) with their corresponding 95% confidence intervals (CI). Quantification of positive and negative association were determined using values of respective odds ratio (OR) derived using logistic regression method. If the values of OR <1 indicating inverse association (exposure variables decreases risk of ESBL-UTI) and OR >1 indicating positive association (exposure variables increases risk of ESBL-UTI) and OR values closer to 1 indicates no potential statistical association. All P values were two-tailed, and P values <0.05 were considered statistically significant. All statistical analyses were performed using the statistical packages, SPSS version 27.0 (Armonk, NY: IBM Corp) and Epi-info (Centers for Disease Control and Prevention, Atlanta, GA) software.
Results
A total of 277 subjects with ESBL-UTI, 679 subjects with UTI caused by non-ESBL gram-negative bacteria (GNB), and 144 subjects with UTI caused by miscellaneous organisms (controls) were included in this study. While most patients in both the ESBL (61%) and GNB groups (66%) were female, the miscellaneous group had an almost even gender distribution. Most subjects in the three groups were 51–70 years of age. Diabetes was the most common co-morbid condition in all three groups. The basic characteristics and co-morbid conditions of the patients in each group are summarized in Table 1.
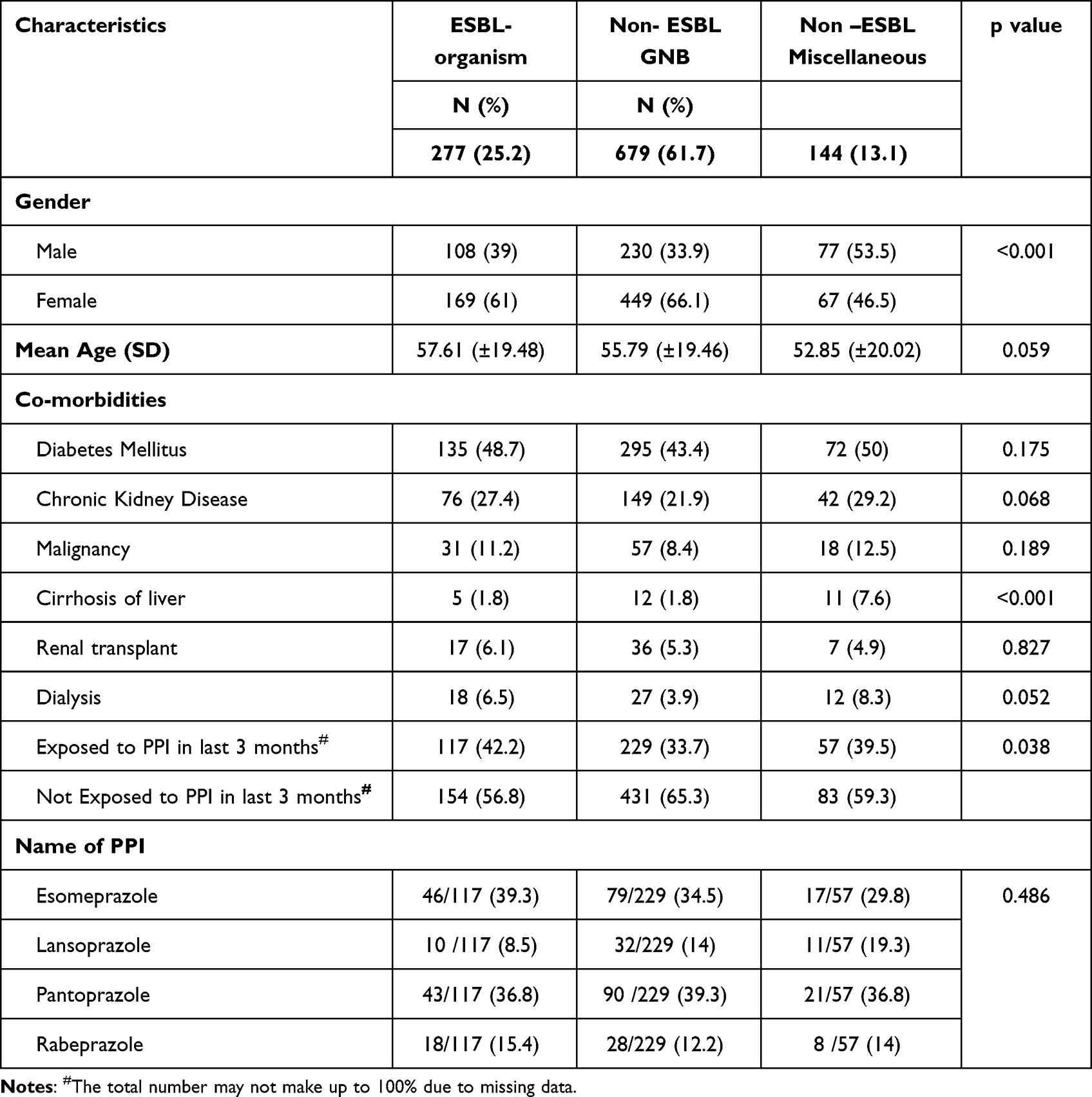 |
Table 1 Demographic Characteristics and PPI Use of the Study Population |
Isolated Organisms
E. coli (79% vs 56%) and Klebsiella pneumonia (18% vs 20%) were the common organisms isolated in the ESBL and GNB groups, respectively. Enterococcus faecalis (33%), Candida species (30%), and Streptococcus agalactiae (20%) were the common isolates in the miscellaneous group. Details of the isolated organisms isolated are summarized in Figure 1A–C.
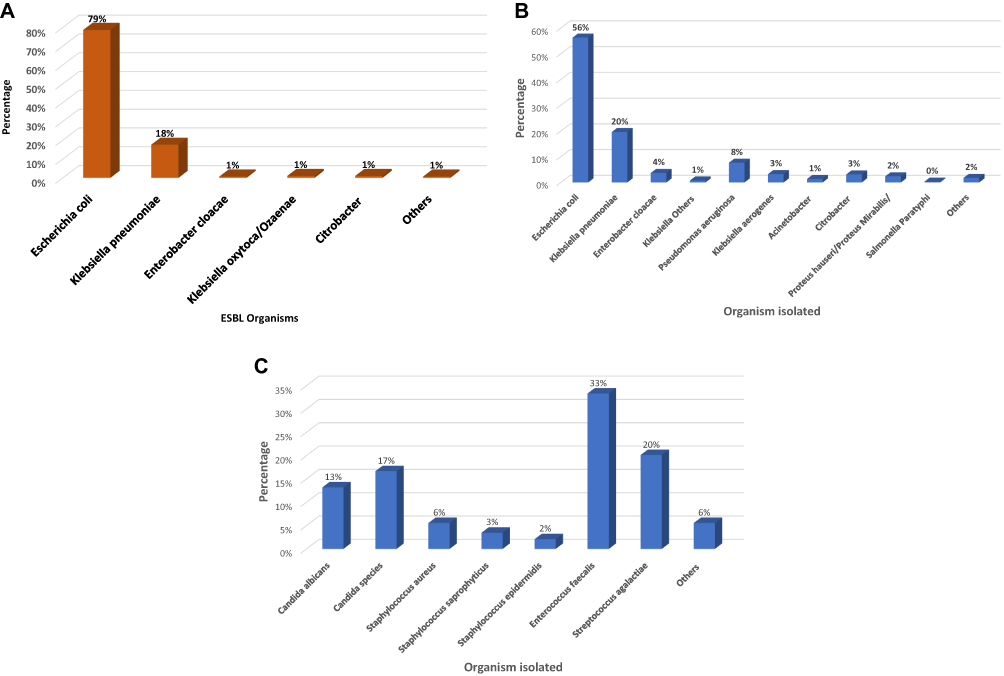 |
Figure 1 (A) Distribution of ESBL organisms (n = 277). (B) Distribution of Non ESBL -GNB organisms (n = 679). (C) Distribution of Non ESBL- Miscellaneous organism (n = 144). |
PPI Exposure
A significantly higher percentage of patients (42.2%) in the ESBL group were exposed to PPI in the preceding 3 months compared to 33.7% and 39.5% in the GNB and miscellaneous groups, respectively (P = 0.038). Esomeprazole and Pantoprazole were the most common PPIs used in all three groups. Use of PPI was found to be higher in patients with comorbid conditions among all the three groups. Details of the PPI exposures are summarized in Table 1 and Table 2.
 |
Table 2 Showing Exposure to PPI in the Various Study Groups |
Association Between PPI Use and ESBL-UTI
Univariate and multivariate logistic regression analyses of potential factors and predictors of PPI use and their possible association with ESBL-UTI are shown in Table 3. Univariate logistic regression identified a significant positive association between ESBL-UTI and PPI use as compared to the GNB (unadjusted OR 1.43, 95% CI 1.07–1.90, P = 0.015). Similarly, a positive association was observed when compared with miscellaneous groups (unadjusted OR 1.10, 95% CI 0.73–1.67); however, this difference did not reach to statistical significance (P = 0.633). Subgroup analysis of individual drugs revealed that Esomeprazole was positively associated with ESBL-UTI as compared with the miscellaneous group (unadjusted OR 1.20, 95% CI 0.44–3.27, P = 0.718) while Lansoprazole was inversely associated with ESBL-UTI (unadjusted OR 0.48, 95% CI 0.19–1.22, P = 0.126 for ESBL versus. GNB and unadjusted OR 0.40 95% CI 0.12–1.33, P = 0.137 for ESBL versus. miscellaneous group).
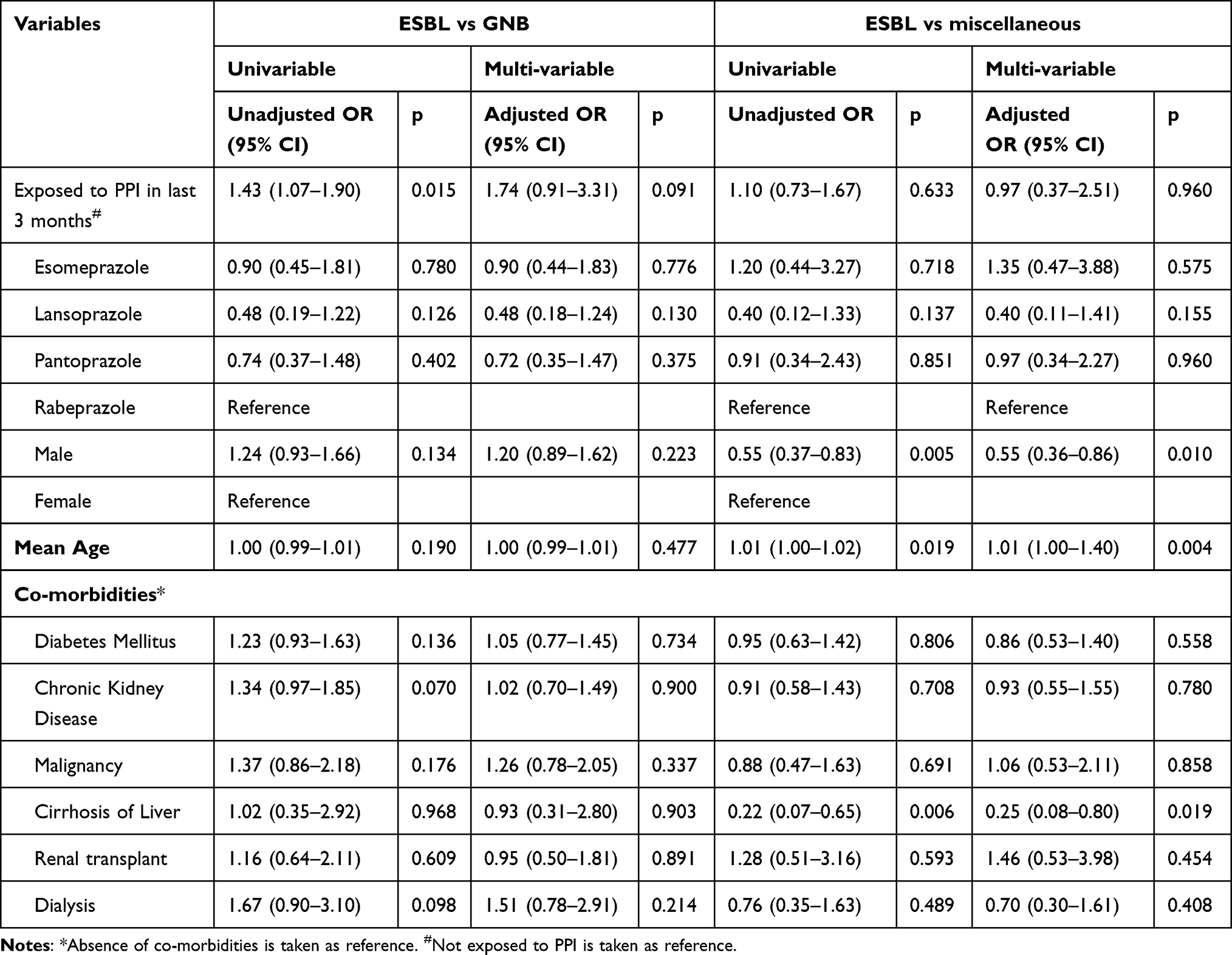 |
Table 3 Univariate and Multivariate Analysis Showing Odds Ratio (95% Confidence Interval) of Variables for ESBL-UTI versus Two Controls |
Multivariate logistic regression analysis showed an increased risk for ESBL-UTI with PPI use as compared to the GNB group (adjusted OR 1.74, 95% CI 0.91–3.31, P = 0.091). Meanwhile, no statistically significant association was observed between ESBL-UTI and the miscellaneous group (adjusted OR 0.97, 95% CI 0.37–2.51, P = 0.960). When individual PPIs were assessed, Esomeprazole was more positively associated with ESBL-UTI than the miscellaneous group (adjusted OR 1.35, 95% CI 0.47–3.88) while Lansoprazole was inversely associated with ESBL-UTI (adjusted OR 0.48, 95% CI 0.18–1.24 for ESBL versus GNB and adjusted OR 0.40, 95% CI 0.11–1.41 for ESBL versus the miscellaneous group, respectively). All these differences noted to be statistically insignificant (P > 0.05).
Discussion
This study showed an association between exposure to PPIs and UTI with ESBL-producing Enterobacteriaceae in adults. This is a salient finding given the widespread use of PPIs and ready over-the-counter availability. Few studies have assessed the relationship between exposure to PPIs and ESBL-UTI in adults. Sogard et al conducted a case-control study on the role of PPI and nitrofurantoin in the development of ESBL-E coli UTI versus non-ESBL-E. coli UTI and population controls. PPI use within the previous year yielded an OR of 1.55 for ESBL-E coli UTI compared with non-ESBL-E. coli UTI. The most recent PPI exposure carried the highest risk of ESBL-E coli UTI.10 The current study showed an OR of 1.43 for PPI exposure by ESBL-UTI patients versus GNB controls, supporting the findings of Sogard et al. Mulder et al found that concomitant use of ciprofloxacin and PPI is a risk factor for ciprofloxacin-resistant E coli UTI in elderly women.19 This may be because PPIs decrease the bioavailability of fluoroquinolones by increasing gastric pH,20,21 however, Washington et al showed no difference in ciprofloxacin bioavailability following PPI use.22
Multiple studies have assessed PPI exposure as a risk factor for Enterobacteriaceae infection. Huizinga et al evaluated the association between PPI use and ESBL-Enterobacteriaceae rectal carriage at hospital admission and found that PPI use was independently associated with ESBL-Enterobacteriaceae carriage. A total of 8.5% of PPI users were rectal carriers of ESBL-Enterobacteriaceae as compared to 2.9% of non-PPI users.23 A study conducted by Cunnigham et al in England found a significant association between PPI exposure and infection with ESBL and non-ESBL-producing Enterobacteriaceae in hospitalized patients.18 No association was identified between histamine-2 receptor blocker or antacid use and ESBL-Enterobacteriaceae infection.
Jackson et al investigated the association between PPI usage and the gut microbiome using 16s ribosomal RNA amplification from the fecal samples of 1827 healthy twins. PPI use was associated with changes in the gut microbiota composition and moderately lower bacterial diversity. PPI use was associated with an increase in the lactobacillus order, particularly the family Streptococcaceae. In PPI users, frequent commensals of the oral, throat, and nasal cavities are found in abundance in the gut. Under normal circumstances, gastric acid acts as a barrier to the progression of oral and nasal commensals and environmental bacteria into the lower GI tract. PPI alters this barrier and allows gut colonization by these organisms.24
Strengths and Limitations of the Study
Simple random sampling was used to select the study sample population which facilitated to reduce the selection bias and ensured true representation of hospital-based population. Hamad medical corporation being the main health-care provider of the country this study sample represent the country population to a greater extent. Exposure to PPIs and the prevalence of UTIs caused by extended-spectrum beta-lactamase-producing Enterobacteriaceae remains poorly studied. To our knowledge, this is the first study to analyze the exposure of individual PPIs and their association for ESBL-UTI in a large cohort.
Due to the retrospective nature of the study, there may be incomplete information about some variables in the data. Some patients may lack information about PPI use prescribed by private health facilities. However, it is unlikely that this was a high enough number to impact the study results.
Conclusions
PPIs use in the preceding 3 months is associated with an increased risk of ESBL-UTI compared to GNB group. Of the individual PPIs, only Esomeprazole showed an association with increased risk of ESBL-UTI compared to miscellaneous group. Lansoprazole, in contrast, demonstrated an inverse association. While this study identified a link between PPI use and ESBL-UTI, it cannot confirm causation. Large case-control studies are recommended to assess the quantification and establish the true risk involved.
Ethical Approval
The study was approved by the ethical committee of the Medical Research Center at Hamad medical corporation in Doha, Qatar (Approval number MRC-01-20-006). The consent was waived due to the retrospective nature of the review. The confidentiality of the included subjects was maintained by not disclosing the identification details and using anonymized data. The study was conducted in full compliance with the principles of “Declaration of Helsinki” Good Clinical Practice (GCP).
Disclosure
The authors declare that they have no financial interest or other conflict of interest to declare in this study.
References
1. Datta N, Kontomichalou P. Penicillinase synthesis controlled by infectious R factors in Enterobacteriaceae. Nature. 1965;208(5007):239–241. doi:10.1038/208239a0
2. Kliebe C, Nies BA, Meyer JF, Tolxdorff-Neutzling RM, Wiedemann B. Evolution of plasmid-coded resistance to broad-spectrum cephalosporins. Antimicrob Agents Chemother. 1985;28(2):302–307. doi:10.1128/AAC.28.2.302
3. Jacoby GA, Munoz-Price LS. The new beta-lactamases. N Engl J Med. 2005;352(4):380–391. doi:10.1056/NEJMra041359
4. Lahey Clinic. ß-lactamase classification and amino acid sequences for TEM, SHV and OXA extended-spectrum and inhibitor resistant enzymes. Available from: http://www.lahey.org/Studies/.
5. Bradford PA. Extended-spectrum beta-lactamases in the 21st century: characterization, epidemiology, and detection of this important resistance threat. Clin Microbiol Rev. 2001;14(4):933–951. doi:10.1128/CMR.14.4.933-951.2001
6. Doi Y, Park YS, Rivera JI, et al. Community-associated extended-spectrum β-lactamase-producing Escherichia coli infection in the United States. Clin Infect Dis. 2013;56(5):641–648. doi:10.1093/cid/cis942
7. Rodríguez-Baño J, Alcalá JC, Cisneros JM, et al. Community infections caused by extended-spectrum beta-lactamase-producing Escherichia coli. Arch Intern Med. 2008;168(17):1897–1902. doi:10.1001/archinte.168.17.1897
8. Tüzün T, Sayın Kutlu S, Kutlu M, Kaleli İ. Risk factors for community-onset urinary tract infections caused by extended-spectrum β-lactamase-producing Escherichia coli. Turk J Med Sci. 2019;49(4):1206–1211. doi:10.3906/sag-1902-24
9. Colodner R, Rock W, Chazan B, et al. Risk factors for the development of extended-spectrum beta-lactamase-producing bacteria in nonhospitalized patients. Eur J Clin Microbiol Infect Dis. 2004;23(3):163–167. doi:10.1007/s10096-003-1084-2
10. Søgaard M, Heide-Jørgensen U, Vandenbroucke JP, Schønheyder HC, Vandenbroucke-Grauls CM. Risk factors for extended-spectrum β-lactamase-producing Escherichia coli urinary tract infection in the community in Denmark: a case-control study. Clin Microbiol Infect. 2017;23(12):952–960. doi:10.1016/j.cmi.2017.03.026
11. Ben-Ami R, Rodríguez-Baño J, Arslan H, et al. A multinational survey of risk factors for infection with extended-spectrum beta-lactamase-producing Enterobacteriaceae in nonhospitalized patients. Clin Infect Dis. 2009;49(5):682–690. doi:10.1086/604713
12. Inns T, Millership S, Teare L, Rice W, Reacher M. Service evaluation of selected risk factors for extended-spectrum beta-lactamase Escherichia coli urinary tract infections: a case-control study. J Hosp Infect. 2014;88(2):116–119. doi:10.1016/j.jhin.2014.07.009
13. Søraas A, Sundsfjord A, Sandven I, Brunborg C, Jenum PA. Risk factors for community-acquired urinary tract infections caused by ESBL-producing Enterobacteriaceae--a case-control study in a low prevalence country. PLoS One. 2013;8(7):e69581. doi:10.1371/journal.pone.0069581
14. Rogers BA, Ingram PR, Runnegar N, et al. Community-onset Escherichia coli infection resistant to expanded-spectrum cephalosporins in low-prevalence countries. Antimicrob Agents Chemother. 2014;58(4):2126–2134. doi:10.1128/AAC.02052-13
15. Naushad VA, Purayil NK, Wilson GJ, et al. Epidemiology of urinary tract infection in adults caused by extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae - a case-control study from Qatar. IJID Reg. 2022;3:278–286. doi:10.1016/j.ijregi.2022.05.001
16. Hassing RJ, Verbon A, de Visser H, Hofman A, Stricker BH. Proton pump inhibitors and gastroenteritis. Eur J Epidemiol. 2016;31(10):1057–1063. doi:10.1007/s10654-016-0136-8
17. Bavishi C, Dupont HL. Systematic review: the use of proton pump inhibitors and increased susceptibility to enteric infection. Aliment Pharmacol Ther. 2011;34(11–12):1269–1281. doi:10.1111/j.1365-2036.2011.04874.x
18. Cunningham R, Jones L, Enki DG, Tischhauser R. Proton pump inhibitor use as a risk factor for Enterobacteriaceal infection: a case-control study. J Hosp Infect. 2018;100(1):60–64. doi:10.1016/j.jhin.2018.05.023
19. Mulder M, Kiefte-de Jong JC, Goessens WH, et al. Risk factors for resistance to ciprofloxacin in community-acquired urinary tract infections due to Escherichia coli in an elderly population. J Antimicrob Chemother. 2017;72(1):281–289. doi:10.1093/jac/dkw399
20. Office of Clinical Pharmacology and Biopharmaceutics Review. CIPRO® XR. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/nda/2002/21-473_Cipro_BioPharmr.pdf.
21. Teng R, Dogolo LC, Willavize SA, Friedman HL, Vincent J. Effect of Maalox and omeprazole on the bioavailability of trovafloxacin. J Antimicrob Chemother. 1997;39:93–97. doi:10.1093/jac/39.suppl_2.93
22. Washington C, Hou E, Hughes N, Berner B. Effect of omeprazole on bioavailability of an oral extended-release formulation of ciprofloxacin. Am J Health Syst Pharm. 2006;63(7):653–656. doi:10.2146/ajhp050355
23. Huizinga P, van den Bergh MK, van Rijen M, Willemsen I, van ‘t Veer N, Kluytmans J. Proton pump inhibitor use is associated with extended-spectrum β-lactamase-producing Enterobacteriaceae rectal carriage at hospital admission: a cross-sectional study. Clin Infect Dis. 2017;64(3):361–363. doi:10.1093/cid/ciw743
24. Jackson MA, Goodrich JK, Maxan ME, et al. Proton pump inhibitors alter the composition of the gut microbiota. Gut. 2016;65(5):749–756. doi:10.1136/gutjnl-2015-310861
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.