Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Association Between Plasma Asprosin Levels and Gestational Diabetes Mellitus
Authors Boz İB, Aytürk Salt S, Salt Ö, Sayın NC, Dibirdik İ
Received 6 June 2023
Accepted for publication 10 August 2023
Published 23 August 2023 Volume 2023:16 Pages 2515—2521
DOI https://doi.org/10.2147/DMSO.S424651
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
İbrahim Bekir Boz,1 Semra Aytürk Salt,2 Ömer Salt,3 Niyazi Cenk Sayın,4 İlker Dibirdik5
1Department of Internal Disease, Akdeniz University, Antalya, Turkey; 2Department of Endocrinology and Metabolic Diseases, Kayseri City Hospital, Kayseri, Turkey; 3Department of Emergency Medicine, Kayseri City Hospital, Kayseri, Turkey; 4Department of Department of Obstetrics and Gynecology, Trakya University, Edirne, Turkey; 5Department of Clinical Biochemistry, Trakya University, Edirne, Turkey
Correspondence: Semra Aytürk Salt, Kayseri City Hospital, Department of Endocrinology and Metabolic Diseases, Şeker Mah. Muhsin Yazıcıoğlu Bulvarı No: 77, Kocasinan, Kayseri, 38080, Turkey, Tel +90 505 780 57 20, Email [email protected]
Purpose: This study sought to investigate whether asprosin can be used in the diagnosis of GDM or for diagnostic purposes in high-risk pregnancies, along with a review of other parameters that may be associated with serum asprosin levels.
Patients and Methods: The study investigated the association between gestational diabetes mellitus (GDM) and asprosin levels. A total of 93 participants; 30 patients with GDM, 33 healthy pregnant women with normal glucose tolerance (NGT), and 30 healthy non-diabetic women (control group) at the Endocrinology and Metabolic Diseases outpatient clinic of a tertiary care university hospital were enrolled in the study. Patients with GDM and NGT were examined in terms of GDM between the 24th and 28th week of pregnancy (2nd trimester). Patient data were collected during routine examinations, and asprosin levels were measured using the ELISA method. All participants underwent testing for measurements of serum hemoglobin, insulin, C-peptide, fasting plasma glucose, and glycated hemoglobin (HbA1c) levels following a fasting period of at least eight hours.
Results: Asprosin levels were higher in pregnant women with NGT and with GDM versus controls (Control–NGT asprosin, p = 0.001; Control–GDM asprosin, p = 0.001). Pregnant women with GDM had higher asprosin levels than those with NGT (p = 0.001). In detecting GDM in pregnant women, an asprosin cutoff value of > 31.709 ng/mL yielded a sensitivity of 93.3%, specificity of 90.9%, positive predictive value of 90.3%, and negative predictive value of 93.75% (p < 0.001).
Conclusion: Serum asprosin levels can potentially be used as a marker in the diagnosis of GDM.
Keywords: asprosin, diabetes mellitus, insulin resistance, pregnancy
Introduction
Gestational diabetes mellitus (GDM) refers to glucose metabolism disorders that occur during pregnancy in healthy women without preexisting diabetes.1 The diagnosis of GDM is made if there is at least one abnormal value (≥92, 180 and 153 mg/dl for fasting, one-hour and two-hour plasma glucose concentrations, respectively), after a 75 g oral glucose tolerance test (OGTT). Type 2 diabetes mellitus (T2DM) is characterized by disorders of carbohydrate, protein, and fat metabolism caused by normal or even higher-than-normal secretion of insulin produced by the beta cells of the pancreas and/or peripheral insulin resistance.
The children of mothers with GDM have a higher body mass index (BMI), fasting plasma glucose levels, abdominal fat ratio, and HOMA-IR scores later in life compared to the children of mothers without GDM.2 Since GDM affects maternal–fetal health and the future health of the unborn child, the early diagnosis and prevention of its associated complications is critical.3 Because gestational diabetes screening varies between countries, Turkey has adopted a screening program based on an oral glucose tolerance test (OGTT) in line with risk factors.4 This test is performed on the second trimester of the pregnancy.
Asprosin is a glucogenic hormone produced by adipose tissue from the C-terminal end of profibrillin. It is involved in regulating adipose tissue distribution and blood glucose levels. Plasma asprosin levels were found to be pathologically elevated in rats and humans with insulin resistance compared with the normal population.5 Asprosin triggers beta cell apoptosis in the pancreas and stimulates glucose release from the liver into the bloodstream via the Janus kinase pathway (JAK).6 Studies conducted on rats with insulin resistance found that injection of monoclonal anti-asprosin antibodies did affect plasma glucose levels but rather decreased both plasma insulin levels and insulin resistance. Plasma asprosin levels were found to be considerably higher in rats and humans with impaired glucose tolerance and diabetes mellitus.5 However, to our knowledge, there is only one study has investigated asprosin levels in pregnant women with GDM with the goal of revealing its utility in determining the risk of developing GDM.6
This study sought to investigate the differences in asprosin levels between healthy individuals (healthy pregnant women and control groups) and those with GDM. To achieve this, we compared plasma asprosin levels among patients with established or newly diagnosed GDM, healthy pregnant women, and healthy non-pregnant women of childbearing age seen by the General Internal Medicine, Endocrinology, and Obstetrics outpatient clinics of a tertiary university hospital. This study aimed to explore the utility of plasma asprosin level in the diagnosis of GDM.
Materials and Methods
The study received approval from the Ethics Committee of Trakya University: the School of Medicine Ethics Committee (dated 30.09.2019 and no. 2019/368). This study was performed by the Declaration of Helsinki. All participants provided written informed consent.
Study Design
A total of 93 women who were admitted to the outpatient clinics of Endocrinology and Metabolic Diseases and Obstetrics and Gynecology and Internal Diseases outpatient clinics at Trakya University School of Medicine between October 01, 2019, and November 15, 2020, were included in the study. These patients read and signed an informed consent form.
Study Population
Participants were divided into three groups: Non-diabetic, non-pregnant controls (Group I), pregnant women with normal glucose tolerance (NGT) (Group II), and pregnant women with GDM (Group III). Group I; the control group consisted of 30 healthy non-pregnant volunteers with normal glucose levels between 18 and 49 years old. Group II consisted of 30 healthy pregnant women >18 years of age without GDM or diabetes, without any chronic comorbidity, and with normal blood glucose levels as detected on tests and OGTT screening. Group III included 33 pregnant women >18 years of age with no known history of chronic disease or pregestational diabetes but were found to have GDM on OGTT. The upper age limit of the participants was 49 years.
Inclusion and Exclusion Criteria
Participants had no known chronic disease and were either diagnosed with GDM during follow-up or were healthy subjects at the outpatient clinic for routine screening. The following were excluded: patients <18 years of age, currently breastfeeding, current smokers, and those with pregestational diabetes mellitus and other acute (acute heart failure, cerebrovascular disease, trauma, myocardial infarction, pulmonary embolism, etc) or chronic diseases (cancer, thyroid disorder, renal failure, etc).
Outcome Measures and Methods
All participants underwent testing for measurements of serum hemoglobin, insulin, C-peptide, fasting plasma glucose, and glycated hemoglobin (HbA1c) levels following a fasting period of at least eight hours. The HOMA-IR scores of the participants were calculated by the formula of fasting glucose (mg/dL) × Fasting insulin (mU/L)/405.7 All laboratory measurements were performed on the second trimester of the pregnancy.
In addition to the parameters, checked at the time of initial presentation to our hospital, the participants were tested for serum asprosin levels using approximately 3 cc of blood that was collected from them, placed in serum-separating tubes with a gel, and centrifuged at 1000 rpm for 15 min at +4°C in the biochemistry laboratory, after which the plasma portion was separated and placed into Eppendorf tubes and stored in a −80°C cooler until the analysis. A total of 10 cc blood collected from the participants for all other biochemical parameters.
Asprosin levels were measured using sandwich ELISA kits manufactured by the Bioassay Technology Laboratory. After delivery to our unit, the kit was stored in a +4°C cabinet until the analysis. The kit is indicated to have a sensitivity of 0.23 ng/mL, a standard curve range of 0.5–100 ng/mL, an intra-assay coefficient of variation (CV) of <8%, and inter-assay CV of >10%.
Methods of Statistical Analysis
Continuous variables were checked for normality of the distribution using the Shapiro–Wilk test. Data related to three or more groups were compared using one-way analysis of variance (Post-Hoc: Tukey’s and Tamhane’s T2 tests) when normally distributed and using the Kruskal–Wallis test (Post-Hoc: Dunn–Bonferroni test) when non-normally distributed. The correlation between two continuous variables was analyzed using Spearman’s rank correlation coefficient. The cutoff value was determined using receiver operating characteristic (ROC) analysis. Sensitivity, specificity, positive predictive value, and negative predictive value were calculated. Continuous variables were expressed in mean and standard deviation (Mean ± SD), median and minimum–maximum (med [min–max]). The analysis was performed using the statistical software SPSS version 23 (SPSS Inc., Armonk, NY). The ROC analysis was performed using the R (version 4.1.0) program pROC (version 1.17.0.1) suite. Statistical significance was set at p < 0.05.
Results
A total of 93 volunteers participated in the study. The mean age of the Groups I, II, and III was 29 ± 3.9 years (median, min–max: 29, 25–39), 27.6 ± 4.6 years (28, 18–38), and 33.6 ± 5.6 years (34, 23–45), respectively. The women in Group III were older than the women in Group I (p = 0.008) and Group II (p < 0.001). There was no significant difference between Group I and Group II in terms of age (p = 0.858).
There was no significant difference in gestational weeks between Group II (25.6 ± 6.2) and Group III (27.1 ± 3.1) (p = 0.226).
Among the subjects included in the study, HOMA-IR and asprosin levels were highest in Group III (6.219 ± 4.4 and 44.2 ± 8.4 ng/mL, respectively). The laboratory parameters of the groups are shown in Table 1.
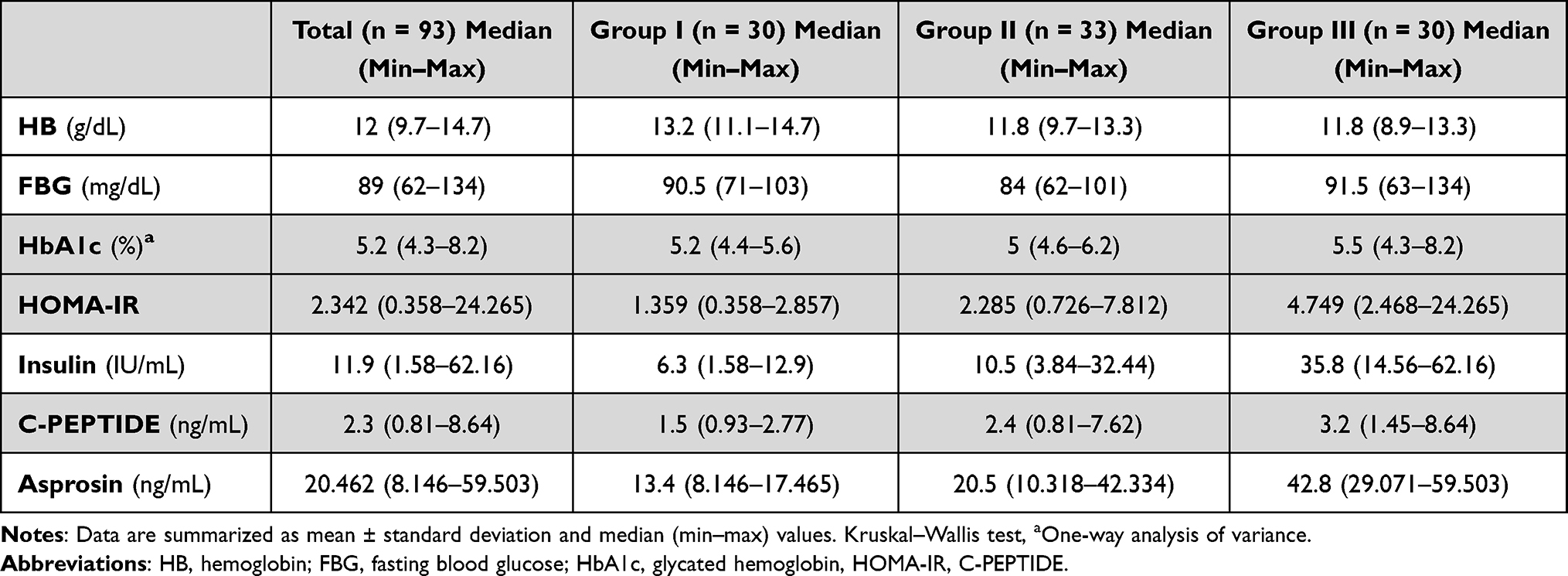 |
Table 1 Laboratory Parameters of the Groups |
In terms of laboratory parameters, Group III had significantly higher HOMA-IR, insulin, C-peptide, and asprosin levels than those in the other two groups (p < 0.001 for both). Fasting blood glucose levels were also significantly higher in Group III than those in Group II (p = 0.007). Glycated hemoglobin levels were significantly higher in Group III than those in Groups I and II (Group I vs III: p = 0.019, Group II vs III: p = 0.001). The results of multiple comparisons between the study groups are shown in Table 2.
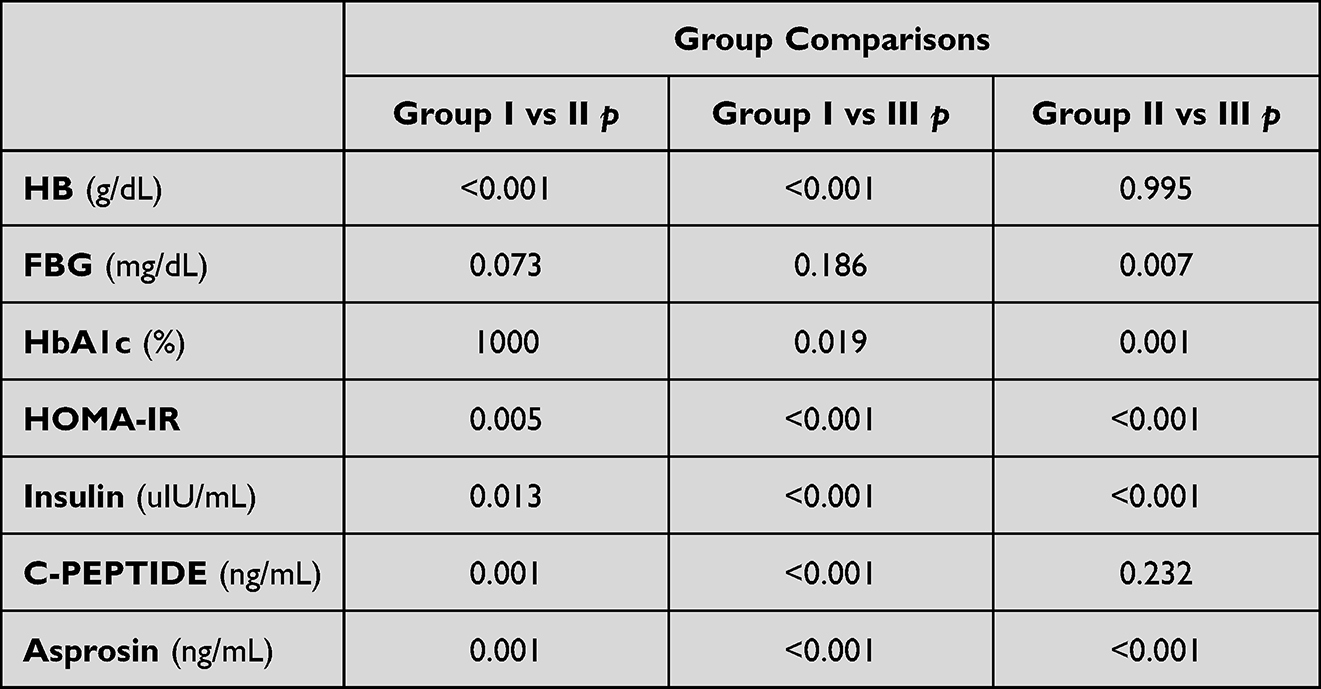 |
Table 2 Results of Pairwise Comparisons |
Association Between Asprosin and HOMA-IR
The linear association between asprosin levels and HOMA-IR was analyzed in each group. Among healthy pregnant women with NGT (Group II), there was a weak negative linear association between asprosin and HOMA-IR levels (r = −0.398, p = 0.022). In Groups I and III, there was no significant linear association between asprosin and HOMA-IR levels (Group I: r = 0.016, p = 0.932; Group III: r = 0.123, p = 0.517).
ROC Analysis for Asprosin Levels
During the analysis of asprosin levels for use in detecting GDM in pregnant women, the area under the curve was 0.970. The calculated cutoff value of >31.709 ng/mL yielded a sensitivity of 93.3%, specificity of 90.9%, positive predictive value of 90.3%, and negative predictive value of 93.75% (p < 0.001, Figure 1).
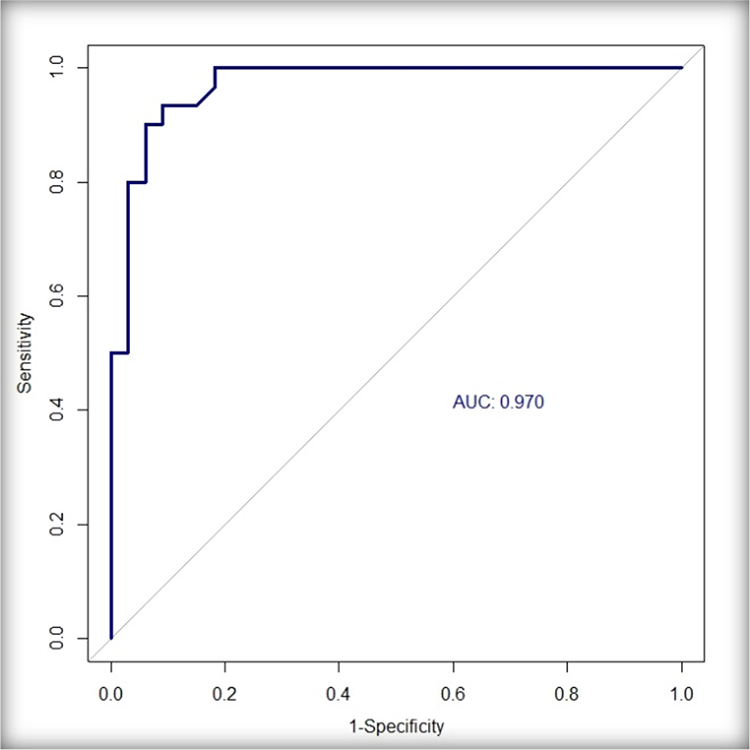 |
Figure 1 ROC curve for asprosin levels in pregnant women. |
Discussion
Although GDM tends to resolve spontaneously after delivery, it is known to contribute to the long-term risk of T2DM, obesity, and cardiovascular disease in both the mother and fetus.3 Although the exact pathophysiology behind GDM is yet to be elucidated, the risk seems to increase with advanced age, obesity, family, or individual history of GDM.8
GDM is detected in approximately 7% of all pregnancies (range, 1–14%) and leads to a number of risks for the mother and fetus during and after pregnancy.9 The pathogenesis of GDM is thought to involve abnormal changes in the insulin signaling pathways of the adipose tissue and skeletal muscle system that occur during pregnancy and the resulting excessive insulin resistance.10 GDM is diagnosed using OGTT in the second trimester, but in order to minimize potential risks, it might be useful to identify and closely follow pregnant women at risk before the second trimester.11 Currently, the HOMA-IR scoring method is widely used for measuring insulin resistance,12 and it reportedly has predictive utility for GDM in the first trimester.9
In the study of Endo et al,13 they compared HOMA-IR scores among pregnant women with normal BMI and NGT, pregnant women with elevated BMI and with NGT, and pregnant women with GDM, and found significantly higher HOMA-IR scores among the obese NGT and GDM groups compared with the NGT group with normal BMI (p < 0.01), but found no significant difference between the GDM and obese NGT groups \1 >\2.05). But this study did not evaluate the asprosin levels of the patients. In our study, we have evaluated asprosin, hemoglobin, insulin, C-peptide and HBA1C levels of the participants to find out the diagnostic role of asprosin in the gestational diabetes. In terms of this point of view, our study is more comprehensive compared to the previous studies.
Sonagra et al14 reported that pregnant women with NGT in the second and third trimesters of their pregnancy had higher HOMA-IR scores than healthy women (p < 0.05 for the second trimester and p < 0.001 for the third trimester). In line with the literature, the present study found significantly higher HOMA-IR scores in the NGT and GDM groups compared with healthy controls (Control–NGT, p = 0.005; Control–GDM, p < 0.001).
During pregnancy, be it healthy or complicated, insulin levels increase.15 Increased insulin is thought to support the anabolic process that occurs during pregnancy.16 These are confirmed by the present study; insulin levels were higher in the NGT and GDM groups compared to those in the control group (NGT–control, p = 0.013; GDM–control, p < 0.001).
Lui et al17 found that C-peptide levels were higher in pregnant women with GDM and impaired glucose tolerance than those with NGT (p < 0.01). Another study comparing C-peptide levels found that pregnant women with impaired glucose tolerance had significantly higher C-peptide levels than those with GDM (p < 0.05), but there was no significant difference between pregnant women with GDM and those with NGT.18 The present study found no significant difference in C-peptide levels between pregnant women with NGT and those with GDM (p = 0.232). We think that; it could be related to pancreatic destruction levels. On the other hand, pregnant women with GDM and NGT had higher C-peptide levels than controls, and it could be related to increased pancreatic secretion of C-peptide (Control–NGT, p = 0.001; Control–GDM, p < 0.001).
According to these results, we think that; we cannot use C-peptide levels alone in the diagnosis of gestational diabetes. But it could be helpful, if it is used in conjunction with asprosin levels.
Asprosin was first introduced in 2016 by Romere et al5 in the literature. It is thought to be produced by white adipose tissue from the C-terminal end of profibrillin and released into circulation. Asprosin secreted in fasting triggers glucose release from the liver and is involved in blood glucose regulation and insulin resistance.5 It has also been found to inhibit insulin secretion from pancreatic beta cells.6
Asprosin crosses the blood–brain barrier and stimulates appetite via the cAMP pathway in the brain. As a result, this increases the amount of adipose tissue in the body and body weight. Experiments found that obese rats had higher asprosin levels compared with healthy rats, and when asprosin levels decreased after injection of monoclonal anti-asprosin antibodies, rats lost weight and their glycemic index improved.19 In line with rat models, studies with humans found elevated asprosin levels in subjects with T2DM compared to healthy controls.17
In the study of Zhang et al20 it was found that increased levels of circulating asprosin in patients with impaired glucose regulation (with high insulin resistance and with high HOMA-IR scores) and those with T2DM versus healthy individuals. Another study found elevated plasma asprosin levels in women with insulin resistance and PCOS (polycystic ovary syndrome) compared to healthy controls.21
One study measured asprosin levels in blood collected from the peripheral circulation and umbilical cord blood in women with GDM, preeclampsia, and eclampsia; the women with complicated pregnancies had higher asprosin levels than those with uncomplicated pregnancy.22
Another study conducted by Wang et al23 that included patients with T2DM found that asprosin levels were higher in individuals with impaired glucose tolerance, insulin resistance, and T2DM versus healthy controls and that plasma asprosin levels were positively correlated with HOMA-IR scores and fasting plasma glucose (p < 0.05). Our study, on the other hand, found a weak negative linear correlation between HOMA-IR scores and asprosin levels (p = 0.022). We think that it is important to diagnose T2DM. Because according to our study, although with a lower HOMA-IR score, patients could be diabetic.
Zhong et al6 compared pregnant women with GDM and NGT at 18–20 weeks of gestation, 24–28 weeks of gestation, and during the prenatal period. Asprosin levels were found to be higher in pregnant women with GDM than in those with NGT at 18–20 weeks and during the prenatal period (18–20 weeks, p < 0.001; prenatal, p = 0.014) but had no significant difference between the two groups at 24–28 weeks (p = 0.118). They concluded that asprosin can be used for the detection and early diagnosis of pregnant women at risk of GDM before the use of the gold standard OGTT test.21 However, since no comparison was made between pregnant women with NGT and healthy controls, no conclusions were made regarding a diagnostic cutoff value for asprosin.
Baykuş et al22 found increased plasma asprosin levels in pregnant women with GDM, preeclampsia, and severe preeclampsia, as well as in those with macrosomic fetuses compared to healthy pregnant women at 37–39 weeks of gestation (p < 0.05). Asprosin was suggested to play a role in the pathophysiology of conditions such as GDM, preeclampsia, and macrosomic fetus. Our study is in line with those findings since significantly higher asprosin levels were seen in the GDM versus the NGT groups (Asprosin NGT–GDM, p < 0.001).
Based on a review of the literature, limited studies have compared asprosin levels in healthy pregnant women with those having NGT and healthy non-pregnant women. In this study, asprosin levels were higher in the NGT group than controls (p < 0.001). Since healthy pregnant women have some degree of insulin resistance, which is known to cause an increase in asprosin, we believe that an increase in asprosin up to a certain level may be physiologic.14,23
On ROC analysis, the calculated cutoff asprosin level of ≥31.709 ng/mL yielded a sensitivity of 93.3%, specificity of 90.9%, positive predictive value of 90.3%, and negative predictive value of 93.75% (p < 0.001).
Limitations of the Study
This study has some limitations. First, our sample size is relatively small, as fewer patients sought consult at the hospital due to COVID-19. Second, in the GDM group, assessments were done using 75-g OGTT, thus precluding comparisons of blood glucose levels and asprosin levels at the time of diagnosis. Studies with a larger population and a larger number of measurements are necessary, which can yield more conclusive results.
Conclusion
Although there is only a partially small sample size in our study, we belive that asprosin levels may have diagnostic value for GDM, and its pathologic and physiologic levels can be determined in appropriate testing settings. Future studies with bigger sample size on the utility of asprosin in the diagnosis of GDM can further elucidate its role in the early detection of the GDM risk and in diagnosing GDM without OGTT.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Buchanan TA, Xiang AH. Gestational diabetes mellitus. J Clin Invest. 2005;115(3):485–491. doi:10.1172/JCI200524531
2. Grunnet LG, Hansen S, Hjort L, et al. Adiposity, dysmetabolic traits, and earlier onset of female puberty in adolescent offspring of women with gestational diabetes mellitus: a clinical study within the Danish national birth cohort. Diabetes Care. 2017;40(12):1746–1755. doi:10.2337/dc17-0514
3. Bartha JL, Martinez-Del-Fresno P, Comino-Delgado R. Early diagnosis of gestational diabetes mellitus and prevention of diabetes-related complications. Eur J Obstet Gynecol Reprod Biol. 2003;109(1):41–44. doi:10.1016/S0301-2115(02)00480-3
4. Grubu DMCv E. Diabetes Mellitus ve Komplikasyonlarının Tanı, Tedavi ve İzlem Kılavuzu [Diagnosis, Treatment and Follow-up Guidelines for Diabetes Mellitus and Its Complications 14th ed]. Grubu DMCv E; 2020.
5. Romere C, Duerrschmid C, Bournat J, et al. Asprosin, a fasting-induced glucogenic protein hormone. Cell. 2016;165(3):566–579. doi:10.1016/j.cell.2016.02.063
6. Zhong L, Long Y, Wang S, et al. Continuous elevation of plasma asprosin in pregnant women complicated with gestational diabetes mellitus: a nested case-control study. Placenta. 2020;93:17–22. doi:10.1016/j.placenta.2020.02.004
7. Mari A, Ahrén B, Pacini G. Assessment of insulin secretion in relation to insulin resistance. Curr Opin Clin Nutr Metab Care. 2005;8(5):529–533. doi:10.1097/01.mco.0000171130.23441.59
8. Lee T, Yun S, Jeong JH, Jung TW. Asprosin impairs insulin secretion in response to glucose and viability through TLR4/JNK-mediated inflammation. Mol Cell Endocrinol. 2019;486:96–104. doi:10.1016/j.mce.2019.03.001
9. Plows JF, Stanley JL, Baker PN, Reynolds CM, Vickers MH. The pathophysiology of gestational diabetes mellitus. Int J Mol Sci. 2018;19(11):3342. doi:10.3390/ijms19113342
10. Alptekin H, Çizmecioğlu A, Işık H, Cengiz T, Yildiz M, Iyisoy MS. Predicting gestational diabetes mellitus during the first trimester using anthropometric measurements and HOMA-IR. Journal of Endocrinological Investigation. 2016;39(5):577–583. doi:10.1007/s40618-015-0427-z
11. Colomiere M, Permezel M, Lappas M. Diabetes and obesity during pregnancy alter insulin signalling and glucose transporter expression in maternal skeletal muscle and subcutaneous adipose tissue. J Mol Endocrinol. 2010;44(4):213–223. doi:10.1677/JME-09-0091
12. Women’s NCCf, Health Cs. Diabetes in Pregnancy: Management of Diabetes and Its Complications from Preconception to the Postnatal Period. Women’s NCCf, Health Cs; 2008.
13. Gutch M, Kumar S, Razi SM, Gupta KK, Gupta A. Assessment of insulin sensitivity/resistance. Indian J Endocrinol Metab. 2015;19(1):160–164. doi:10.4103/2230-8210.146874
14. Endo S, Maeda K, Suto M, et al. Differences in insulin sensitivity in pregnant women with overweight and gestational diabetes mellitus. Gynecol Endocrinol. 2006;22(6):343–349. doi:10.1080/09513590600724836
15. Sonagra AD, Biradar SM, D K, Murthy DSJ. Normal pregnancy – a state of insulin resistance. J Clin Diagnost Res. 2014;8(11):CC01–CC3. doi:10.7860/JCDR/2014/10068.5081
16. Ryan EA, O’ Sullivan MJ, Skyler JS. Insulin action during pregnancy: studies with the euglycemic clamp technique. Diabetes. 1985;34(4):380–389. doi:10.2337/diab.34.4.380
17. Duerrschmid C, He Y, Wang C, et al. Asprosin is a centrally acting orexigenic hormone. Nat Med. 2017;23(12):1444. doi:10.1038/nm.4432
18. Stanley K, Fraser R, Bruce C. Physiological changes in insulin resistance in human pregnancy: longitudinal study with the hyperinsulinaemic euglycaemic clamp technique. Br J Obstet Gynaecol. 1998;105(7):756–759. doi:10.1111/j.1471-0528.1998.tb10207.x
19. Valensise H, Larciprete G, Vasapollo B, et al. C-peptide and insulin levels at 24–30 weeks’ gestation: an increased risk of adverse pregnancy outcomes? Eur J Obstet Gynecol Reprod Biol. 2002;103(2):130–135. doi:10.1016/S0301-2115(02)00048-9
20. Zhang L, Chen C, Zhou N, Fu Y, Cheng X. Circulating asprosin concentrations are increased in type 2 diabetes mellitus and independently associated with fasting glucose and triglyceride. Clin Chim Acta. 2019;489:183–188. doi:10.1016/j.cca.2017.10.034
21. Wang Y, Qu H, Xiong X, et al. Plasma asprosin concentrations are increased in individuals with glucose dysregulation and correlated with insulin resistance and first-phase insulin secretion. Mediators Inflamm. 2018;2018:9471583. doi:10.1155/2018/9471583
22. Alan M, Gurlek B, Yilmaz A, et al. Asprosin: a novel peptide hormone related to insulin resistance in women with polycystic ovary syndrome. Gynecol Endocrinol. 2019;35(3):220–223. doi:10.1080/09513590.2018.1512967
23. Baykus Y, Yavuzkir S, Ustebay S, Ugur K, Deniz R, Aydin S. Asprosin in umbilical cord of newborns and maternal blood of gestational diabetes, preeclampsia, severe preeclampsia, intrauterine growth retardation and macrosemic fetus. Peptides. 2019;120:170132. doi:10.1016/j.peptides.2019.170132
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Decreased Serum Osteocalcin is an Independent Risk Factor for Metabolic Dysfunction-Associated Fatty Liver Disease in Type 2 Diabetes
Wang YJ, Jin CH, Ke JF, Wang JW, Ma YL, Lu JX, Li MF, Li LX
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3717-3728
Published Date: 29 November 2022
Prevention of Hepatalin-Dependent Insulin Resistance Induced by a High Sucrose Diet Using a Synergistic Combination of S-Adenosyl Methionine, Vitamin E and Vitamin C (SAMEC) in Virgin and Pregnant Sprague Dawley Rats
Lovat NEJ, Chowdhury K, Legare DJ, Lautt WW
Journal of Experimental Pharmacology 2025, 17:193-205
Published Date: 15 May 2025
The Effects of the Ethanol Extract of Allium Ascalonicum L. in High-Fat-High-Fructose-Induced Insulin Resistance Swiss-Webster Male Mice
Elkanawati RY, Sumiwi SA, Levita J
Journal of Experimental Pharmacology 2025, 17:207-221
Published Date: 16 May 2025
Asprosin Levels in Adults with Type 2 Diabetes Mellitus and Diabetic Kidney Disease: A Systematic Review and Meta-Analysis
Ristic J, Kodalak S, Peralta-Jiménez GA, Moura de Lima MF, Kovacevic M, Masic S, Nikolic T
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2493-2506
Published Date: 23 July 2025
Association of Fasting C-Peptide to High Density Lipoprotein Cholesterol Ratio with Non-Alcoholic Fatty Liver Disease in Chinese Type 2 Diabetes Mellitus Patients: A Cross-Sectional Study
Liang Q, Hu H, Chen X, Yang S, Zhang Y, Wu Y, Wang X, Chen H
Diabetes, Metabolic Syndrome and Obesity 2025, 18:4507-4522
Published Date: 11 December 2025