Back to Journals » International Journal of General Medicine » Volume 17
Association Between Pericoronary Fat Attenuation Index as Evaluated by Coronary Artery CT Angiography and Clinical Interventions in Lipid Management Among Patients with Coronary Artery Disease
Authors Feng YS, Sun ZY, Jiang F, Ma PC, Liu XR, Meng YY, Liao CD, Sun GF
Received 23 May 2024
Accepted for publication 24 September 2024
Published 26 October 2024 Volume 2024:17 Pages 4937—4946
DOI https://doi.org/10.2147/IJGM.S468768
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Yu-Sen Feng,1,* Zheng-Yun Sun,2,* Fei Jiang,3 Peng-Cheng Ma,1 Xing-Rui Liu,1 Yuan-Yuan Meng,2 Cheng-De Liao,1 Gui-Fang Sun1
1Department of Radiology, Kunming Yan’an Hospital, Kunming, 650051, People’s Republic of China; 2Department of Radiology, Lincang First People’s Hospital, Lincang, 677000, People’s Republic of China; 3Department of Radiology, Wenshan First People’s Hospital, Wenshan, 663599, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Gui-Fang Sun, Department of Radiology, Kunming Yan’an Hospital, No. 245 Renmin East Road, Panlong District, Kunming, Yunnan, 650051, People’s Republic of China, Tel +86 13759518529, Email [email protected]
Objective: This study aims to evaluate the relationship between the pericoronary fat attenuation index (FAI), derived from coronary artery computed tomography angiography, and post-lipid management levels of low-density lipoprotein cholesterol in patients with coronary artery disease (CAD). Additionally, the study investigates coronary inflammation across different lipid management strategies.
Methods: We selected a cohort comprising 521 CAD patients who met the inclusion criteria. Patients were categorized into well-managed (LDL-C< 2.6 mmol/L) and poorly managed (LDL-C≥ 2.6 mmol/L) groups based on lipid management efficacy. We collected anthropometric measures (height, weight, body mass index, and body surface area) and clinical indicators, including Gensini score, and FAI-related parameters for coronary atherosclerotic lesions. We analyzed the interrelations along these parameters and lipid management using statistical methods and assessed diagnostic value via receiver operating characteristic (ROC) curve analysis of these parameters was assessed through.
Results: The poorly managed group exhibited significantly higher levels of total cholesterol, triglycerides, and lower levels of high-density lipoprotein compared to the well-managed group (P < 0.05). Significant differences were observed between the groups in terms of lesion length in the proximal segment of the left anterior descending artery, FAI value in the proximal segment of lesions in the right coronary artery (RCA), volume thickness in the middle segment of RCA lesions, and lesion length in the distal segment of RCA (P < 0.05). ROC curve analysis revealed areas under the curve ranging from 0.484 to 0.660 for the parameters, indicating limited diagnostic efficacy.
Conclusion: The FAI in the RCA varies with lipid management strategies, suggesting it as a valuable metric for monitoring both perivascular inflammation and lipid status in CAD patients. However, its current diagnostic efficacy is limited, indicating the need for further research to improve its clinical utility.
Keywords: coronary artery CT angiography, coronary atherosclerotic heart disease, coronary inflammation, lipids, low-density lipoprotein cholesterol, pericoronary fat attenuation index
Introduction
Coronary artery disease (CAD) represents a prevalent cardiovascular condition. In urban China, CAD exhibits a mortality rate of 126.91 per 100,000, a concerning trend marked by escalating prevalence and mortality rates, thereby posing substantial health hazards.1 Low-density lipoprotein cholesterol (LDL-C) is a pathogenic risk factor and primary target for intervention in CAD. The mechanism of action of cLDL in coronary heart disease is that the antioxidant content of small and dense low-density lipoprotein in cLDL is low, which is very easy to oxidize, difficult to clear from plasma, and easy to adhere to the vascular wall.2 It has been confirmed that it can be used as an independent risk factor for predicting atherosclerosis, and has been included in the National Cholesterol Education Plan of the United States.3 However, the treatment rate for LDL-C among patients at high risk of atherosclerotic cardiovascular disease (ASCVD) in China stands at a modest 42.9%.4 While lipid-lowering therapies have demonstrated efficacy in slowing and even reversing the progression of coronary atherosclerosis, apprehensions about safety emerge when LDL-C levels are excessively low, potentially resulting in intracranial hemorrhage.5,6 Pericoronary inflammation (referred to as coronary inflammation) plays a key role in different stages of the development of coronary atherosclerotic plaque, affecting the formation and stability of plaque.7,8 Severe inflammation can easily cause significant vascular stenosis and unstable plaques, leading to adverse events. Consequently, there is a critical need to assess the inflammatory status of coronary arteries post LDL-C management. Recently, the quantitative assessment of the pericoronary fat attenuation index (FAI) using coronary artery computed tomography (CT) angiography imaging has gained widespread recognition as a novel surrogate biomarker for coronary inflammation. Previous studies have shown that FAI is a non-invasive examination method that can warn the level of coronary artery inflammation related to CAD in the early stage of disease and provide basis for early clinical treatment. The FAI provides a reliable means to monitor changes in the content and size of pericoronary lipids, providing insight into changes in fat density driven by paracrine mechanisms of coronary inflammation.9–11 In this study, we investigated the correlation between FAI as observed in coronary artery CT angiography and LDL-C levels following lipid management interventions in patients with CAD. The primary objectives are to discern the CAD status and associated FAI under diverse LDL-C management scenarios, as well as to analyze the state of coronary inflammation in the context of varied lipid management strategies.
Data and Methods
Study Participants and Grouping
A retrospective analysis was conducted encompassing 521 patients diagnosed with CAD who received treatment at the cardiology departments of Yan’an Hospital Affiliated to Kunming Medical University, Wenshan Prefecture First People’s Hospital, and The People’s Hospital of Lincang between January and December 2022. Patients were categorized clinically based on lipid management indicators, specifically LDL-C, into two groups: the well-managed group (LDL-C < 2.6 mmol/L) and the poorly managed group (LDL-C ≥ 2.6 mmol/L), including traditional Chinese medicine treatment, Miao medicine, Yi medicine treatment, other nonclinical guideline treatment plans, and comprehensive multiple treatment plans, and patients who refuse treatment. The informed consent was obtained from all participants.
Inclusion and Exclusion Criteria
Inclusion criteria: 1.CAD patients: Coronary atherosclerotic heart disease refers to a common cardiovascular disease caused by coronary artery stenosis or occlusion, resulting in myocardial ischemia, hypoxia or necrosis; 2. Aged 18 years and above; 3. Cardio-gated coronary artery scan was performed with Gensini score greater than 0;12 4. Complete liver function examination (including LDL-C) and have complete clinical data; 5. Clinical manifestations were angina pectoris; 6. Patients who have not undergone coronary stent implantation or DSA, or do not need coronary stent implantation for the time being; 7. Coronary artery CTA examination indicates the presence of stenosis in the coronary artery and the degree is from 50% to 70%.
Exclusion criteria: 1. Diabetic patients; 2. Patients with severe heart, liver and renal insufficiency; 3. Patients who had undergone heart surgery prior to the examination.
Methods
Research Methods
General Data Collection
The collected data included the height, weight, body mass index (BMI), and body surface area of enrolled patients. Liver function tests included total cholesterol (TC), triglycerides (TG), LDL-C, and high-density lipoprotein cholesterol (HDL-C). BMI was calculated as weight (kg) divided by height (m) squared. The formula for body surface area was  .
.
Coronary CT Angiography Enhancement Examination
Imaging procedures were performed using the Siemens Flash 128 dual-source spiral CT scanner, including both plain and enhanced scans. The scan parameters were a tube voltage of 120 kV with automatic milliampere technology. The detector configurations were either 2×128×0.6 mm or 2×64×0.6 mm, with a pitch of 1.5. The reconstruction layer thickness was 1.0 mm, with a 0.6 mm interval. Non-ionic iohexol (350 mgI/mL) was used as the contrast agent, administered via a dual-barrel high-pressure injector into the median cubital vein at a rate of 3–4 mL/s. A total of 60–80 mL of contrast agent was followed by a 20–30 mL saline flush at the same rate. The bolus tracking technique, was employed with the aortic chamber as the target vessel for monitoring. Scanning began when the enhancement threshold CT value of 120 hU was reached, with the patient holding their breath. The scanning range extended from 2 cm above the aortic arch to below the apex of the heart. The acquired images were then transferred to a workstation for reconstruction using multiplanar reconstruction (MPR), curved planar reconstruction (CPR), maximum intensity projection (MIP), and volume rendering (VR). These reconstructed images were analyzed alongside axial images.
FAI Image Analysis
All results from coronary CT enhancement examinations were transferred to the Perivascular Analysis Tool software workstation, developed by Shukun Technology (Shukun (Beijing) Network Technology Co., Ltd.), for post-processing.
The main coronary artery FAI were calculated automatically.13,14 After data import, the system measured the length of the three primary coronary arteries, their respective FAI values, and the volume of pericoronary fat. A fat partition threshold of −190 to −30 hU was used to calculate the target fat within a 40 mm range extending outward from the outer edge of the vessel wall. For the left anterior descending artery (LAD) and the left circumflex artery (LCX), the measurement range began at the origin and extended to 4 mm distally, while for the right coronary artery (RCA), it started 10 mm from the coronary ostium and extended to 50 mm distally (see Figure 1).
 |
Figure 1 Female, 46 years old, localized non-calcified plaque in mid-segment (segment 3) of the right coronary artery causing mild luminal stenosis (approximately 45% narrowing), Gensini score of 2. (A) Proximal section of LAD (start–40 mm), FAI value of −88 hU, volume of 2591 mm³, thickness approximately 4.00 mm; (B) Proximal section of LCX (start–40 mm), FAI value of −82 hU, volume of 2071 mm³, thickness approximately 4.00 mm; (C) Proximal section of RCA (start–40 mm), FAI value of −83 hU, volume of 2693 mm³, thickness approximately 4.00 mm; (D) Localized non-calcified plaque in the mid-segment (segment 3) of the right coronary artery causing mild stenosis around FAI parameters: FAI value of −81 hU, length approximately 7 mm, volume about 402 mm³. |
For the measurement of FAI in areas of coronary atherosclerosis, the measurement region was centered at the plaque site of interest. The radial distance was manually adjusted to match the diameter of the vessel, and the software automatically computed the length of the plaque, the FAI value, and the volume of pericoronary fat surrounding it.
Image Analysis
Image interpretation was independently performed by two physicians, each with over 10 years of experience in cardiovascular imaging diagnosis. In cases of disagreement, a collaborative discussion was conducted to reach a consensus. The analysis focused primarily on lesions within the main coronary artery, with an emphasis on plaque characteristics categorized as non-calcified, calcified, or mixed. Soft plaque, with a CT value < 50 hU, and fibrous plaque with a CT value between 50 and 120 hU, were collectively classified as non-calcified plaques. The analysis also included an assessment of plaque extent, degree of luminal stenosis, identification of vulnerable plaques, and Gensini scoring. The Gensini scoring system assigns scores based on the degree of coronary lumen narrowing: < 25% scored 1 point, 25–50% scored 2 points, 51–75% scored 4 points, 76–90% scored 8 points, 91–99% scored 16 points, and 100% occlusion scored 32 points. Varied weighting coefficients were applied depending on the location of the narrowing, with a coefficient of 5 for the left main coronary artery, 2.5 for the proximal segments of the LAD and left circumflex artery (LCX), 1.5 for the mid-segment of the LAD, 1 for the RCA, posterior descending artery (PDA), distal segments of the LAD, diagonal branch (D1), obtuse marginal artery (OM), and distal segments of the LCX, and 0.5 for the remaining vessels. The Gensini score for each patient was derived as the sum of scores across all branches.
Statistical Methods
Data analysis was performed using SPSS 19.0 statistical software. Quantitative data following a normal distribution are presented as mean ± standard deviation, and inter-group comparisons were conducted using independent sample t-tests. Categorical data are expressed as the number of cases (%) and compared between-group using the chi-squared test and Fisher’s exact test, depending on the distribution characteristics. Non-normally distributed quantitative data are represented as the median (interquartile range) and compared using the non-parametric rank sum test. A P < 0.05 was considered statistically significant. These findings enable clinical physicians to assess pericoronary inflammation in patients without complete lipid status, allowing for appropriate adjustments in medication and the development of more suitable coronary CT follow-up schedule.
Results
General Information
The study included 521 patients with a mean age of (62.98 ± 11.37) years (range: 26 to 97 years). Of these, 204 were females (39.2%) and 317 were males (60.8%). All patients underwent lipid management according to the “Chinese Adult Guidelines for the Prevention and Treatment of Abnormal Blood Lipids (2016 Revised).” The well-managed group consisted of 211 patients (40.5%), while the poorly managed group included 310 patients (59.5%).
In the poorly managed group, levels of TC, TG, and HDL were significantly higher than those in the well-managed group (P < 0.05). However, no statistically significant differences were observed in weight, height, body surface area, or BMI between the two groups (P > 0.05), as revealed in Table 1.
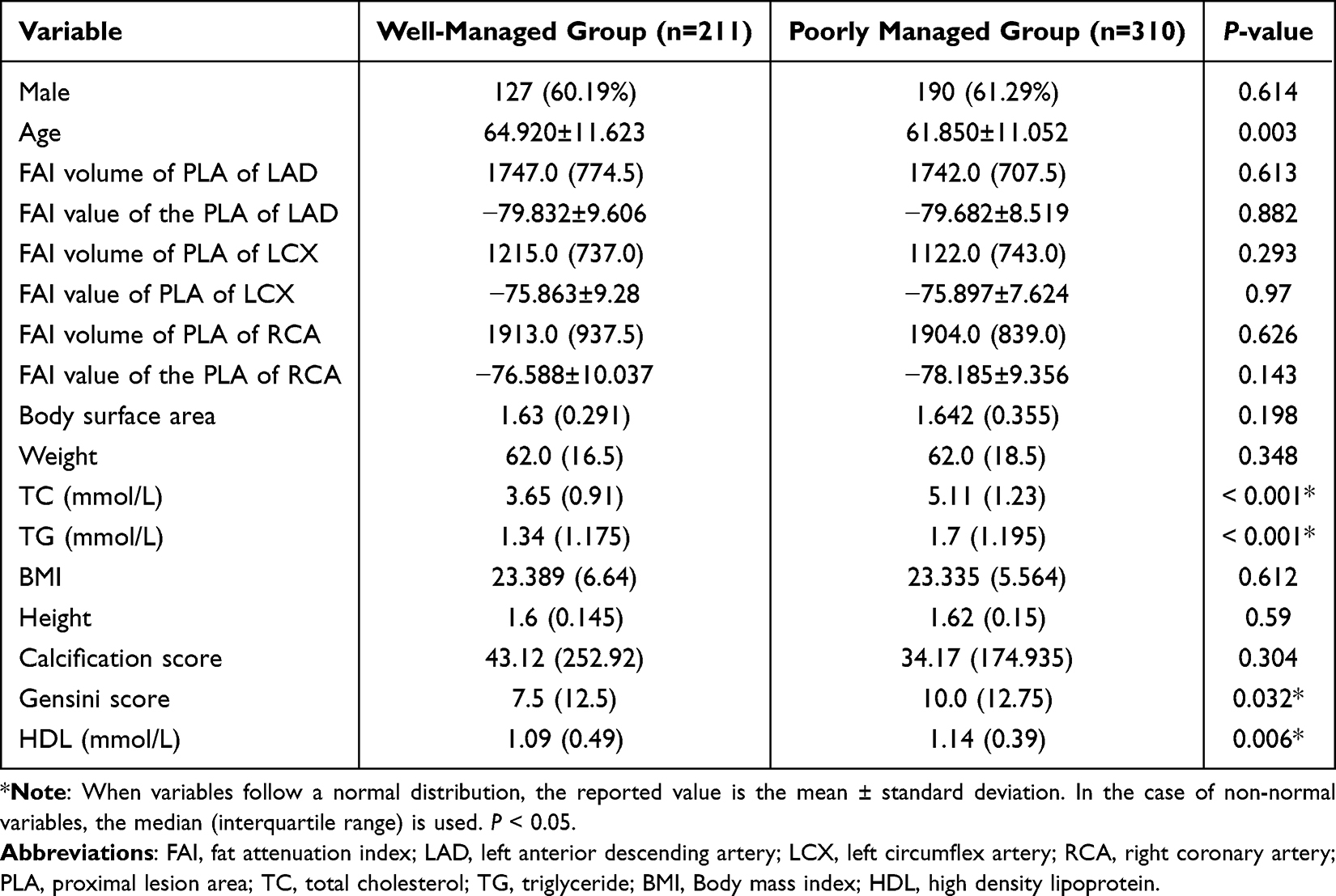 |
Table 1 Differences in Proximal FAI Parameters and General Data Between the Well-Managed and Poorly Managed Groups |
Differences in FAI Between the Well-Managed and Poorly Managed Groups at the LAD, LCX, and RCA Proximal Segments
As shown in Table 1 and Figure 1, there were statistically significant differences between the poorly managed and well-managed groups in terms of the FAI values and volumes in the proximal segments of the LAD, LCX, and RCA (P<0.05).
Differences in FAI in Coronary Atherosclerosis Areas Between the Well-Managed and Poorly-Managed Groups
Table 2 presents statistically significant differences between the groups concerning lesion length in the proximal segment of the LAD, FAI value in the proximal segment of the RCA, volume thickness in the mid-segment of the RCA, and lesion length in the distal segment of the RCA (P < 0.05).
 |
Table 2 Differences in FAI Parameters of Coronary Atherosclerosis Areas Between Well-Managed and Poorly-Managed Groups |
Differences in Coronary Gensini Scores Between the Well-Managed and Poorly Managed Groups
The present research revealed a statistically significant difference (P < 0.05) in the overall distribution of Gensini scores between the well-managed and poorly-managed groups. Regarding the calcification scores, however, no statistically significant distinction existed between the two groups (P > 0.05), as indicated in Table 1.
ROC Curve Analysis of Parameters with Statistical Differences Between the Two Groups
ROC curve analysis was performed using parameters that showed statistically significant differences between the two groups. The AUC for these parameters ranged from 0.484 to 0.660. Specifically, the AUCs for lesion length in the proximal segment of the LAD, volume thickness in the mid-segment of the RCA, lesion length in the distal segment of RCA, FAI value in the proximal segment of RCA, and Gensini score were 0.484, 0.573, 0.685, 0.533, and 0.660, respectively. The optimal cut-off values, along with their corresponding sensitivity and specificity, were as follows: 15.5 (45.20%, 54.80%), 3.5 (58.10%, 41.90%), 21 (22.60%, 77.40%), −78.5 (68.40%, 48.40%), and 20.25 (78.90%, 51.60%). The diagnostic efficacy of these parameters, as indicated by their AUC, was generally below 0.700, as detailed in Table 3 and illustrated in Figure 2.
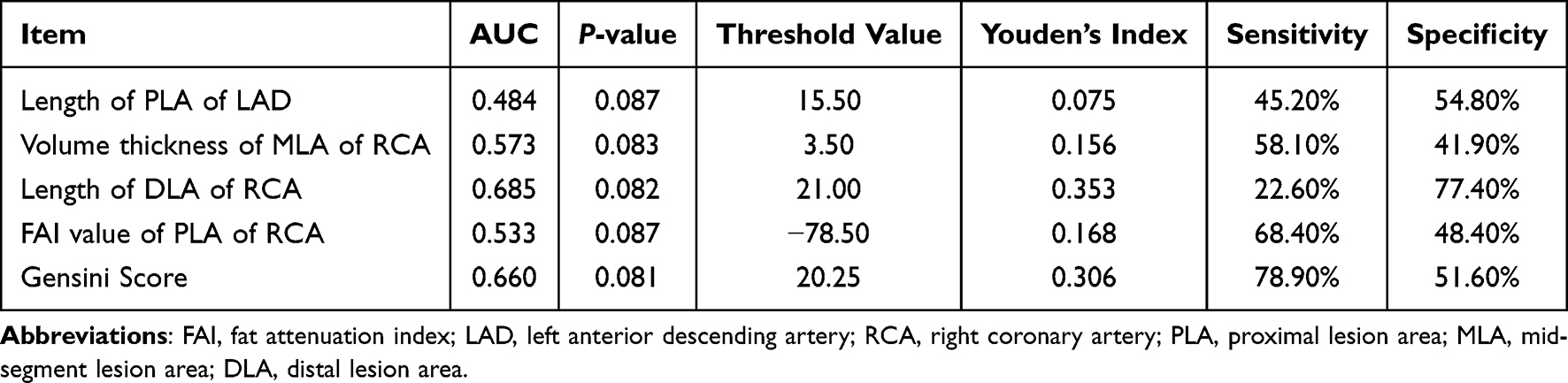 |
Table 3 Diagnostic Efficacy Assessment Using the ROC Curve for Parameters Indicating Statistical Differences Between the Two Groups |
 |
Figure 2 ROC curve analysis for parameters that differ significantly between the two groups. |
Discussion
Differences in General Conditions Between the Well-Managed and Poorly Managed Groups
CAD remains a significant health concern, with increasing prevalence in China. LDL-C stands out as a pathogenic risk factor for CAD. In the United States, a decline in CAD mortality has been largely attributed to improved risk factor control, including a notable 24% reduction in TC.15 Our study highlights a significant disparity in the overall distribution of TC between well-managed and poorly-managed CAD patients, emphasizing the critical role of effective TC management. Consistent with broader literature trends, our findings show an increase in TC, LDL-C, and triglycerides (TG) among Chinese patients, alongside a decrease in HDL-C.16,17 This underscores the urgent need to enhance awareness and management of dyslipidemia in CAD patients. The study supports existing literature that identifies HDL-C and the LDL/HDL ratio as important predictors of CAD, reinforcing the need for comprehensive lipid management.18
Correlation Between Coronary Artery CT Angiography, Gensini Score, and Lipid Management Intervention in Patients with CAD
Cardiovascular diseases, including CAD, are the leading cause of mortality worldwide19 Myocardial ischemia due to coronary artery stenosis is a major concern, and the Gensini score is used to assess the severity of CAD.20 Research indicates that each 1 mmol/L reduction in LDL-C corresponds to a 20–23% decrease in adverse cardiovascular events.21–23 Atherosclerosis is driven by a concentration gradient that results in the deposition and retention of ApoB-containing lipoproteins in the subendothelial space.24 All ApoB-containing lipoprotein particles contribute to atherosclerosis, with 95% of LDL-C comprised of ApoB100. Our study found that Gensini scores varied significantly between well-managed and poorly managed CAD patients, with poorly managed patients exhibiting higher scores. This aligns with previous studies suggesting that severe narrowing is associated with elevated Gensini scores.9 Elevated LDL-C is a primary risk factor for atherosclerosis across genetic, animal, and epidemiological studies,25–29 and reducing LDL-C improves CAD outcomes.26,30,31 Our findings reinforce the importance of LDL-C management in improving CAD prognosis.
Correlation Between Pericoronary FAI Based on Coronary Artery CT Angiography and Lipid Management Intervention in Patients with CAD
Pericoronary adipose tissue, rich in saturated fats, influences the inflammatory environment around coronary vessels.32 The pericoronary FAI, reflecting fat density and inflammation, is a novel marker for coronary inflammation.33 Our study revealed that poorly managed CAD patients had more adverse pericoronary FAI conditions compared to well-managed patients. This suggests that inadequate lipid management accelerates pericoronary inflammation, which is consistent with research indicating RCA-FAI as a potential independent risk factor for atherosclerosis.32 Increased attenuation of pericoronary fat correlates with coronary inflammation and mortality,34 and FAI offers a valuable, non-invasive marker for assessing coronary inflammation.35 Our results support the use of FAI in conjunction with lipid management to better assess and manage CAD.
Research Limitations
The study’s uneven age distribution may introduce bias, highlighting the need for more balanced data in future research. Additionally, the lack of detailed categorization of lipid management interventions and analysis of treatment plans limits the depth of our findings. Future studies should include a more granular classification of treatment and consider the impact of calcified plaques and potential artifacts on coronary assessments. Other confounding factors, such as dyslipidemia duration and ethnic differences, were not addressed. The absence of a healthy control group also underscores the need for additional comparative studies.
Conclusion
In summary, as a novel inflammatory biomarker, FAI may be serve as a valuable tool for assessing the lipid profiles and the state of inflammation of patients around coronary arteries, but its diagnostic efficacy needs to be improved. Subsequent combined diagnosis with other inflammatory factor parameters is expected to improve diagnostic efficacy. Notably, the results of this study indicate that RCA-FAI varies with lipid management strategies. Therefore, FAI may have the potential to be employed in monitoring perivascular inflammation and lipid status in CAD.
Abbreviations
CAD, coronary atherosclerotic heart disease; LDL-C, low-density lipoprotein cholesterol; FAI, fat attenuation index; TC, total cholesterol; TG, triglyceride; HDL-C, high-density lipoprotein cholesterol.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Kunming Yan’an Hospital. This study was conducted by the declaration of Helsinki. Written informed consent was obtained from all participants.
Consent for Publication
All participants signed a document of informed consent.
Funding
This study was funded by the Yunnan Provincial Department of Science and Technology Major Science and Technology Special Program - Biomedical Special Project (Grant No. 202102AA310003-5), and Yunnan Provincial Department of Science and Technology - Kunming Medical University Joint Special Plan (Grant No. 202401AY070001-364). The funding bodies had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The authors declare that they have no competing interests.
References
1. The Writing Committee of the Report on Cardiovascular Health and Diseases in China. Report on cardiovascular health and diseases in China 2022: an updated summary. Chin J Intervent Cardiol. 2023;7:485–508.
2. Sekimoto T, Koba S, Mori H, et al. Small dense low-density lipoprotein cholesterol: a residual risk for rapid progression of non-culprit coronary lesion in patients with acute coronary syndrome. J Atheroscler Thromb. 2021;28(11):1161–1174. doi:10.5551/jat.60152
3. Viktorinova A, Malickova D, Svitekova K, Choudhury S, Krizko M. Low-density lipoprotein cholesterol-to-apolipoprotein B ratio as a potential indicator of LDL particle size and plasma atherogenicity in type 2 diabetes. Diabetes Res Clin Pract. 2021;176:108858. doi:10.1016/j.diabres.2021.108858
4. Chinese Joint Committee for the Revision of Guidelines for the Prevention and Treatment of dyslipidemia in adults. Guidelines for the prevention and treatment of dyslipidemia in adults in China (2016 revision). Chin Circ J. 2016;31:937–950.
5. Shin S, Park HB, Chang HJ, et al. Impact of intensive LDL cholesterol lowering on coronary artery atherosclerosis progression: a serial CT angiography study. JACC. 2017;10(4):437–446. doi:10.1016/j.jcmg.2016.04.013
6. Beijing Hypertension Association, Beijing Diabetes Prevention and Treatment Association, Beijing Research for Chronic Diseases Control and Health Education. Practice guide for integrated management of primary cardiovascular disease 2020. Chin Med Front J. 2020;8:1–73.
7. Shobeiri N, Bendeck MP. Interleukin-1β is a key biomarker and mediator of inflammatory vascular calcification. Arterioscler Thromb Vasc Biol. 2017;37(2):179–180. doi:10.1161/ATVBAHA.116.308724
8. Madonna R, Massaro M, Scoditti E, Pescetelli I, De Caterina R. The epicardial adipose tissue and the coronary arteries: dangerous liaisons. Cardiovasc Res. 2019;115(6):1013–1025. doi:10.1093/cvr/cvz062
9. Zhang R, Ju Z, Li Y, Gao Y, Gu H, Wang X. Pericoronary fat attenuation index is associated with plaque parameters and stenosis severity in patients with acute coronary syndrome: a cross-sectional study. J Thorac Dis. 2022;14(12):4865–4876. doi:10.21037/jtd-22-1536
10. Margaritis M, Antonopoulos AS, Digby J, et al. Interactions between vascular wall and perivascular adipose tissue reveal novel roles for adiponectin in the regulation of endothelial nitric oxide synthase function in human vessels. Circulation. 2013;127(22):2209–2221. doi:10.1161/CIRCULATIONAHA.112.001133
11. Elnabawi YA, Oikonomou EK, Dey AK, et al. Association of biologic therapy with coronary inflammation in patients with psoriasis as assessed by perivascular fat attenuation index. JAMA Cardiol. 2019;4(9):885–891. doi:10.1001/jamacardio.2019.2589
12. Rampidis GP, Benetos G, Benz DC, Giannopoulos AA, Buechel RR. A guide for gensini score calculation. Atherosclerosis. 2019;287:181–183. doi:10.1016/j.atherosclerosis.2019.05.012
13. Antonopoulos AS, Sanna F, Sabharwal N, et al. Detecting human coronary inflammation by imaging perivascular fat. Sci Transl Med. 2017;9(398):eaal2658. doi:10.1126/scitranslmed.aal2658
14. van Griethuysen JJM, Fedorov A, Parmar C, et al. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017;77(21):e104–e107. doi:10.1158/0008-5472.CAN-17-0339
15. Ford ES, Ajani UA, Croft JB, et al. Explaining the decrease in U.S. deaths from coronary disease, 1980-2000. N Engl J Med. 2007;356(23):2388–2398. doi:10.1056/NEJMsa053935
16. Thanassoulis G, Williams K, Ye K, et al. Relations of change in plasma levels of LDL-C, non-HDL-C and apoB with risk reduction from statin therapy: a meta-analysis of randomized trials. J Am Heart Assoc. 2014;3(2):e000759. doi:10.1161/JAHA.113.000759
17. Joint Committee on the Chinese Guidelines for Lipid Management. Chinese guidelines for lipid management (2023). Chin Circ J. 2023;38(3):237–271.
18. Adepu C, Sandeep Kumar Reddy B. Association of serum bilirubin and lipid ratio (total cholesterol/(high-density lipoprotein + bilirubin)) in coronary artery disease: a case-control study at a tertiary care hospital. Cureus. 2023;15(10):e46420. doi:10.7759/cureus.46420
19. Vetter C, Devore EE, Wegrzyn LR, et al. Association between rotating night shift work and risk of coronary heart disease among women. JAMA. 2016;315(16):1726–1734. doi:10.1001/jama.2016.4454
20. Wang J, Xiao M, Li YF, Cai Y. Relationship between blood lipid, blood coagulation indexes and the degree of coronary artery stenosis in patients with coronary atherosclerotic heart disease. China Med. 2023;18(1):11–15.
21. Navarese EP, Robinson JG, Kowalewski M, et al. Association between baseline LDL-C level and total and cardiovascular mortality after LDL-C lowering: a systematic review and meta-analysis. JAMA. 2018;319(15):1566–1579. doi:10.1001/jama.2018.2525
22. Lin LQ, Wu BX, Lin MY, Chen QX, Xu DP. Interim analysis report of kuanxiong aerosol in improving angina and quality of life after percutaneous coronary intervention. World J Tradit Chin Med. 2022;8:87–91. doi:10.4103/wjtcm.wjtcm_26_21
23. Silverman MG, Ference BA, Im K, et al. Association between lowering LDL-C and cardiovascular risk reduction among different therapeutic interventions: a systematic review and meta-analysis. JAMA. 2016;316(12):1289–1297. doi:10.1001/jama.2016.13985
24. Shaya GE, Leucker TM, Jones SR, Martin SS, Toth PP. Coronary heart disease risk: low-density lipoprotein and beyond. Trends Cardiovasc Med. 2022;32(4):181–194. doi:10.1016/j.tcm.2021.04.002
25. Liu Z, Yan Y, Gu S, Lu Y, He H, Ding H. White blood cell count combined with LDL cholesterol as a valuable biomarker for coronary artery disease. Coronary Artery Dis. 2023;34(6):425–431. doi:10.1097/MCA.0000000000001248
26. Packard C, Chapman MJ, Sibartie M, Laufs U, Masana L. Intensive low-density lipoprotein cholesterol lowering in cardiovascular disease prevention: opportunities and challenges. Heart. 2021;107(17):1369–1375. doi:10.1136/heartjnl-2020-318760
27. Zhou R, Stouffer GA, Smith SC. Targeting the cholesterol paradigm in the risk reduction for atherosclerotic cardiovascular disease: does the mechanism of action of pharmacotherapy matter for clinical outcomes? J Cardiovasc Pharmacol Ther. 2021;26(6):533–549. doi:10.1177/10742484211023632
28. Wang CH, Gong B, Meng H, Wu YL, Zhao XS, Wei JH. Dalbergia odorifera essential oil protects against myocardial ischemia through upregulating Nrf2 and inhibiting caspase signaling pathways in isoproterenol-induced rats. World J Tradit Chin Med. 2023;9:338–347. doi:10.4103/2311-8571.372727
29. Chistiakov DA, Myasoedova VA, Revin VV, Orekhov AN, Bobryshev YV. The phenomenon of atherosclerosis reversal and regression: lessons from animal models. Exp Mol Pathol. 2017;102(1):138–145. doi:10.1016/j.yexmp.2017.01.013
30. Vani A, Underberg JA. Lowering LDL-cholesterol and CV benefits: is there a limit to how low LDL-C needs to be for optimal health benefits? Clin Pharmacol Ther. 2018;104(2):290–296. doi:10.1002/cpt.1133
31. Hoogeveen RC, Ballantyne CM. Residual cardiovascular risk at low LDL: remnants, lipoprotein(a), and inflammation. Clin Chem. 2021;67(1):143–153. doi:10.1093/clinchem/hvaa252
32. Liu S, Guan H, Li S. To explore the influencing factors of pericoronary adipose tissue and noninvasive fractional flow reserve on the progression of coronary heart disease based on 320-slice coronary CTA. Anatol J Cardiol. 2023;27(2):100–105. doi:10.14744/AnatolJCardiol.2022.2576
33. Huang Cao ZF, Stoffel E, Cohen P. Role of perivascular adipose tissue in vascular physiology and pathology. Hypertension. 2017;69(5):770–777. doi:10.1161/HYPERTENSIONAHA.116.08451
34. Duncker H, Achenbach S, Moshage M, et al. Computed tomography-derived characterization of pericoronary, epicardial, and paracardial adipose tissue and its association with myocardial ischemia as assessed by computed fractional flow reserve. J Thorac Imaging. 2023;38(1):46–53. doi:10.1097/RTI.0000000000000632
35. Zhao W, Zhang N, Yang S, et al. Analysis of coronary computed tomography angiography-derived pericoronary fat attenuation index characteristics in the diagnostic assessment of patients with Takayasu arteritis. Quant Imaging Med Surg. 2023;13(10):7142–7155. doi:10.21037/qims-23-419
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.