Back to Journals » Journal of Pain Research » Volume 19
Association Between Pain Subtypes and Cognitive Impairment in Parkinson’s Disease
Authors Gao L, Li Z, Cai L ![]() , Xu W, Liu Y
, Xu W, Liu Y
Received 5 September 2025
Accepted for publication 27 February 2026
Published 23 March 2026 Volume 2026:19 559348
DOI https://doi.org/10.2147/JPR.S559348
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Rocío de la Vega
Liang Gao, Zhichang Li, Laisheng Cai, Wenyuan Xu, Yi Liu
Department of Neurology, the First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China
Correspondence: Yi Liu, Department of Neurology, the First Affiliated Hospital of Nanchang University, No. 17 Yongwai zheng Street, Nanchang City, Jiangxi Province, 330006, People’s Republic of China, Tel +86-0791-88692511, Email [email protected] Wenyuan Xu, Department of Neurology, the First Affiliated Hospital of Nanchang University, No. 17 Yongwai zheng Street, Nanchang City, Jiangxi Province, 330006, People’s Republic of China, Tel +86-0791-88692511, Email [email protected]
Purpose: To investigate the impact of different pain subtypes on cognitive function in patients with Parkinson’s disease (PD).
Patients and Methods: A total of 344 patients with PD were enrolled in this cross-sectional study, comprising 187 males (54.4%) and 157 females (45.6%), with ages ranging from 32 to 84 years old. Demographic and clinical data were collected, including age, disease duration, levodopa equivalent daily dose (LEDD), and scores on the Unified Parkinson’s Disease Rating Scale part III (UPDRS-III), Hoehn and Yahr (H&Y) scale, Pittsburgh Sleep Quality Index (PSQI), King’s Parkinson’s Disease Pain Scale (KPPS), Visual Analogue Scale (VAS), Mini-Mental State Examination (MMSE), Activities of Daily Living (ADL) scale, Hamilton Depression Rating Scale (HAMD), and Hamilton Anxiety Rating Scale (HAMA).
Results: Cognitive impairment was present in 56.4% of patients with PD. Compared with those with normal cognition, patients with cognitive impairment were older, had a later age at onset, more severe motor symptoms, higher levels of anxiety and depression, and greater pain severity. Specifically, they reported more chronic pain, central pain, visceral pain, “off” period dystonia, discoloration/swelling, and generalized lower abdominal pain (p < 0.05). Moreover, MMSE scores were positively correlated with chronic pain, radicular pain, and visceral pain (p < 0.05).
Conclusion: Cognitive impairment in PD is closely associated with pain severity, with certain pain subtypes exerting a stronger influence on cognition.
Keywords: parkinson’s disease, pain, cognitive impairment, mini-mental state examination, king’s parkinson’s disease pain scale
Introduction
Parkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder characterized by both motor symptoms (resting tremor, rigidity, bradykinesia, and postural instability) and a wide range of non-motor symptoms (cognitive impairment, pain, sleep disturbances, anxiety, depression, autonomic dysfunction, behavioral abnormalities, and fatigue).1 Among these, pain and cognitive impairment are increasingly recognized as prevalent and disabling non-motor symptoms that significantly reduce the quality of life in patients with PD.2,3
Approximately 40–85% of patients with PD experience different types of pain, including musculoskeletal pain, chronic pain, fluctuation-related pain, nocturnal pain, orofacial pain, discoloration/swelling, and radicular pain.2 However, appropriate management is often lacking because PD-related pain remains poorly understood. To address this gap, the King’s Parkinson’s Disease Pain Scale (KPPS) was developed as the first disease-specific tool for assessing pain in PD and demonstrates greater validity across various PD-related pain types compared with the Visual Analogue Scale (VAS). KPPS not only enables characterization, scoring, and longitudinal monitoring of pain but also allows discrimination between different levels of pain severity.4 Known clinical risk factors for PD-related pain include female sex, greater disease severity, and sleep disturbances.2
Cognitive impairment is also common in PD. At diagnosis, 15–35% of PD patients meet the criteria for mild cognitive impairment (PD-MCI), and longitudinal studies suggest that up to 80% of PD patients eventually progress to Parkinson’s disease dementia (PDD).5 Risk factors for cognitive decline include older age, later age at disease onset, greater disease severity, postural instability-gait disorder subtype, and the presence of features such as rapid eye movement sleep behavior disorder (RBD), psychosis, depression, and anxiety.6
Pain and cognitive impairment frequently co-occur in PD. Increasing evidence suggests that pain is closely associated with cognitive dysfunction, particularly impairments in memory, attention, executive function, and decision-making. These two conditions may interact bidirectionally, exacerbating one another.7–10 The potential neurobiological mechanisms linking pain and cognition may involve shared neurotransmitter systems (including dopamine and acetylcholine) as well as overlapping anatomical structures, such as the limbic system and thalamus.
Studies examining the association between pain and cognition in PD patients have produced inconsistent findings. While two studies reported no significant relationship, a more recent investigation showed that PD patients with poorer executive function experienced greater pain interference.11–13 Another study demonstrated that reduced amplitudes of pain-related somatosensory evoked potentials (SEPs) were associated with impairments in attention and memory.14 Nevertheless, few studies have investigated the relationship between different pain subtypes and cognitive impairment in PD. Moreover, our previous research demonstrated that PD-related pain is associated with sleep, which may in turn influences cognitive function.15 Therefore, using the Mini-Mental State Examination (MMSE) and the KPPS, the present study aimed to examine the association between specific pain subtypes and cognitive function, and to identify pain-related predictors of cognitive impairment in patients with PD.
Materials and Methods
Participants
This cross-sectional observational study enrolled 344 patients with PD who attended the Department of Neurology at the First Affiliated Hospital of Nanchang University between March 2019 and March 2024, comprising 187 males (54.4%) and 157 females (45.6%), with ages ranging from 32 to 84 years old. All participants, recruited from both outpatient clinics and inpatient wards, were evaluated by experienced neurologists and met the Movement Disorder Society (MDS) Clinical Diagnostic Criteria for Parkinson’s Disease (MDS-PD Criteria).16 Patients with atypical or secondary parkinsonism, pain of known etiology, or a history of neurosurgery were excluded. Individuals diagnosed with other parkinsonian syndromes, including progressive supranuclear palsy, multiple system atrophy, and corticobasal degeneration, as well as those with severe systemic diseases or psychiatric disorders, were also excluded. Written informed consent was obtained from all subjects before participation in the study. This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the First Affiliated Hospital of Nanchang University (2020956).
Clinical Assessment Protocol
Demographic and clinical data, including age, sex, disease duration, and use of antiparkinsonian medications, were collected by movement disorder specialists through standardized face-to-face interviews. Motor disability was assessed using the Unified Parkinson’s Disease Rating Scale part III (UPDRS-III), and disease severity was staged with the Hoehn and Yahr (H&Y) scale. Pain was evaluated using the KPPS and the VAS. Global cognitive function was assessed using the MMSE. Depression and anxiety symptoms were evaluated with the Hamilton Depression Rating Scale (HAMD) and Hamilton Anxiety Rating Scale (HAMA), respectively. Sleep quality was assessed with the Pittsburgh Sleep Quality Index (PSQI), and functional status in activities of daily living was measured with the activities of daily life (ADL) scale. Participants were divided into two groups based on cognitive status: normal cognition (MMSE score 27–30) and cognitive impairment (MMSE score 0–26).
Statistical Analysis
All statistical analyses were performed using SPSS version 25.0 (SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as mean ± standard deviation (SD). Homogeneity of variance was assessed using Levene’s test. Between-group differences in demographic and clinical characteristics were analyzed using independent two-tailed t-tests. The magnitude of differences between groups was quantified using Cohen’s d, with thresholds of 0.2 (small), 0.5 (medium), and 0.8 (large). Categorical variables were presented as frequencies and percentages, and comparisons between groups were made using the chi-square test. Correlations between MMSE and KPPS scores were evaluated using Pearson’s correlation coefficient. Generalized linear regression was applied to identify potential risk factors for cognitive impairment. A two-tailed p-value of <0.05 was considered statistically significant.
Results
Clinical Characteristics
Table 1 summarizes the demographic and clinical characteristics of PD patients enrolled in this study. The mean MMSE score was 24.75 ± 4.02. Among them, 150 patients (43.6%) had normal cognition, while 194 patients (56.4%) exhibited cognitive impairment. There were no significant between-group differences in disease duration, levodopa equivalent daily dose (LEDD), or ADL scores. However, cognitive impairment was more common in females (p < 0.001). Patients with cognitive impairment were significantly older (t = 3.127, p = 0.001) and had a higher age at disease onset (t = 2.630, p = 0.009) compared with the normal cognition group. Motor disability, as measured by UPDRS-III (t = 4.148, p < 0.001) and H&Y scale (t = 2.934, p = 0.004), was more severe in patients with cognitive impairment. Furthermore, patients with cognitive impairment scored significantly higher on the HAMA (t = 4.665, p < 0.001), HAMD (t = 3.002, p = 0.003), and PSQI (t = 2.254, p = 0.025). A medium effect size was observed for HAMA (Cohen’s d = 0.507), whereas small effect sizes were found for all other measures (Cohen’s d < 0.5).
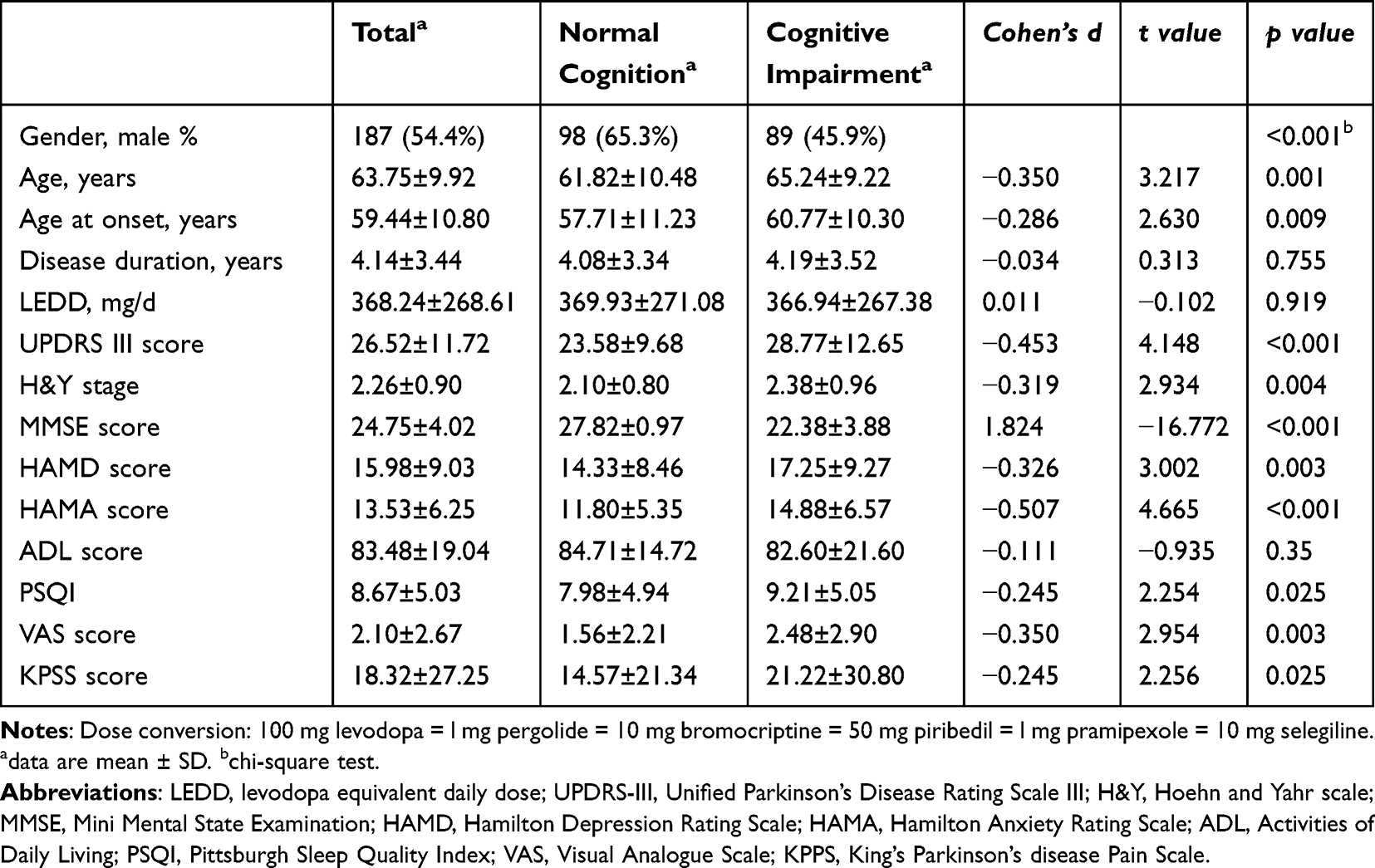 |
Table 1 Demographic and Clinical Features of Patients with Parkinson’s Disease Related Pain in the Total Sample and Stratified by Cognition |
Effects of Pain Subtypes on Cognition
Pain assessment with the KPPS (t = 2.256, p = 0.025) and VAS (t = 2.954, p = 0.003) revealed higher overall pain scores in PD patients with cognitive impairment (Table 1). Among the seven KPPS domains, patients with cognitive impairment had significantly higher scores for chronic pain (t = 3.192, p = 0.002) and discoloration/swelling (t = 1.992, p = 0.047). At the item level (14 KPPS items), patients with cognitive impairment showed higher scores for central pain (t = 2.695, p = 0.007), visceral pain (t = 2.317, p = 0.021), “off” period dystonia (t = 2.114, p = 0.035), and generalized lower abdominal pain (t = 2.013, p = 0.045) compared with patients with normal cognition (Table 2). However, the effect sizes were all small (Cohen’s d < 0.5).
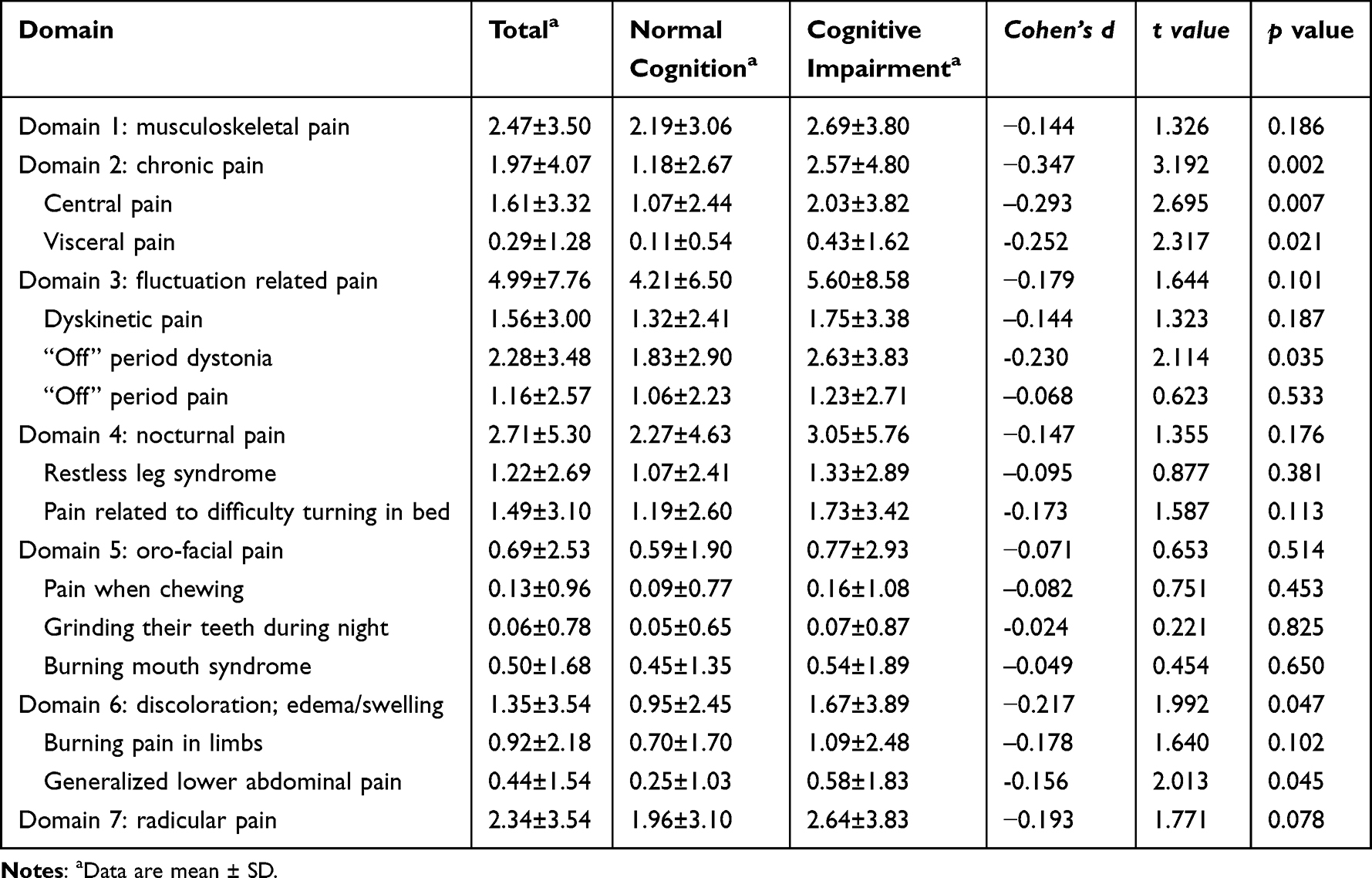 |
Table 2 King’s Parkinson’s Disease Pain Scale Scores of Patients with Parkinson’s Disease Related Pain in the Total Sample and Stratified by Cognition |
Association Between KPPS Subtypes and MMSE Scores
Pearson’s correlation analysis showed that MMSE scores were correlated with both total KPPS (r = 0.128, p = 0.018) and VAS scores (r = 0.176, p = 0.003). Among the KPPS domains, MMSE scores were correlated with chronic pain (r = 0.182, p = 0.001) and radicular pain (r = 0.138, p = 0.010). At the item level, MMSE scores were positively correlated with visceral pain (r = 0.213, p < 0.001) (Table 3).
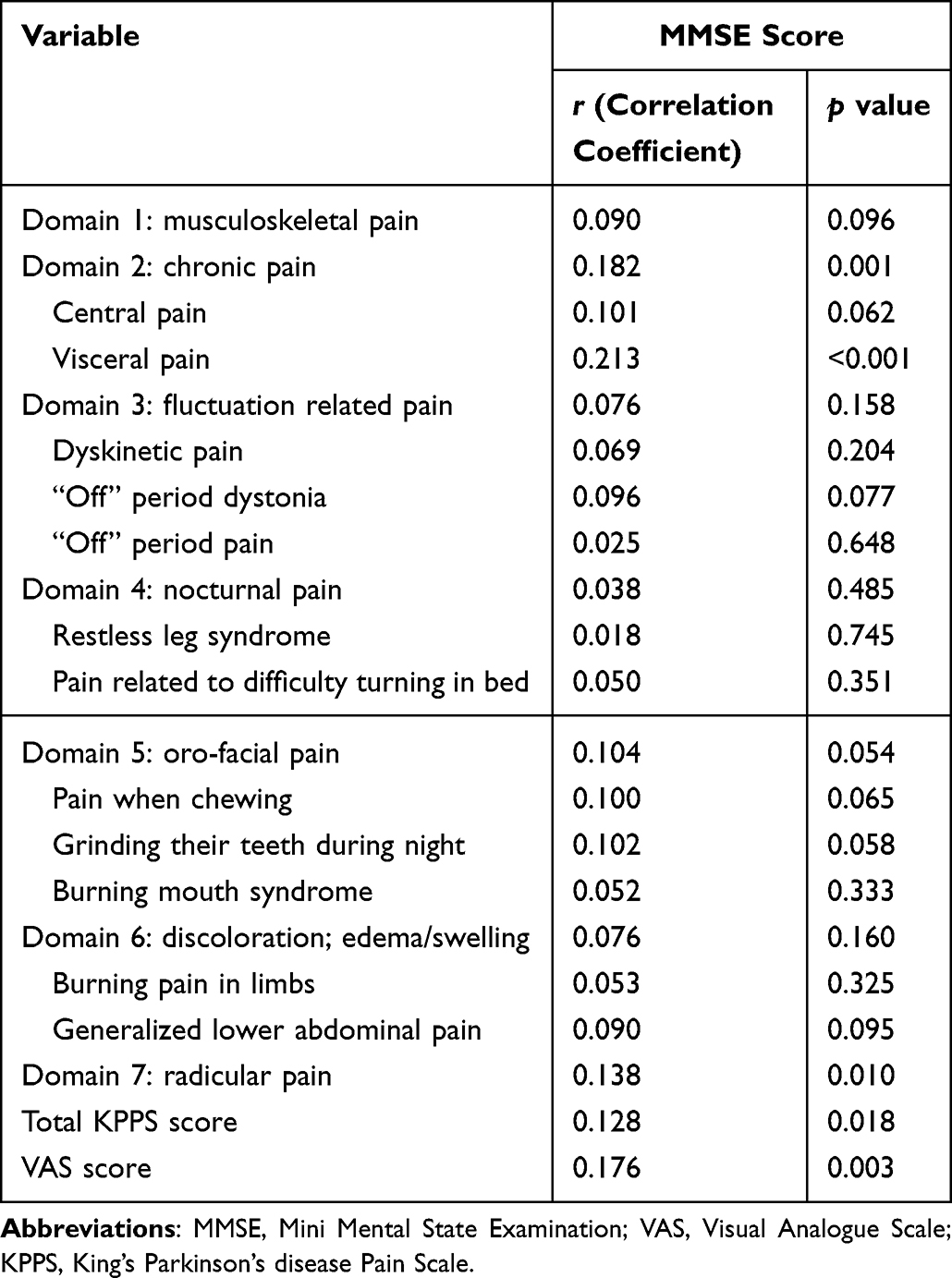 |
Table 3 Correlation of Mini Mental State Examination Scores with King’s Parkinson’s Disease Pain Scale Scores |
Risk Factors for Cognitive Impairment
Regression analysis identified UPDRS III score (β = −0.348, p < 0.001), HAMA score (β = −0.247, p < 0.001), and disease duration (β = 0.221, p < 0.001) as independent predictors of cognitive impairment in PD (Tables 4 and 5).
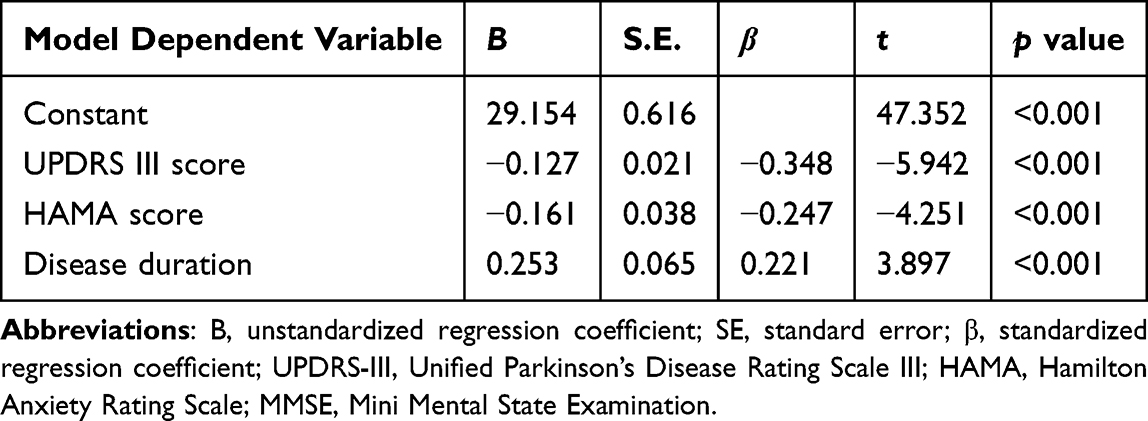 |
Table 4 Generalized Linear Regression Analysis of Risk Factors for Cognitive Impairment in Parkinson’s Disease |
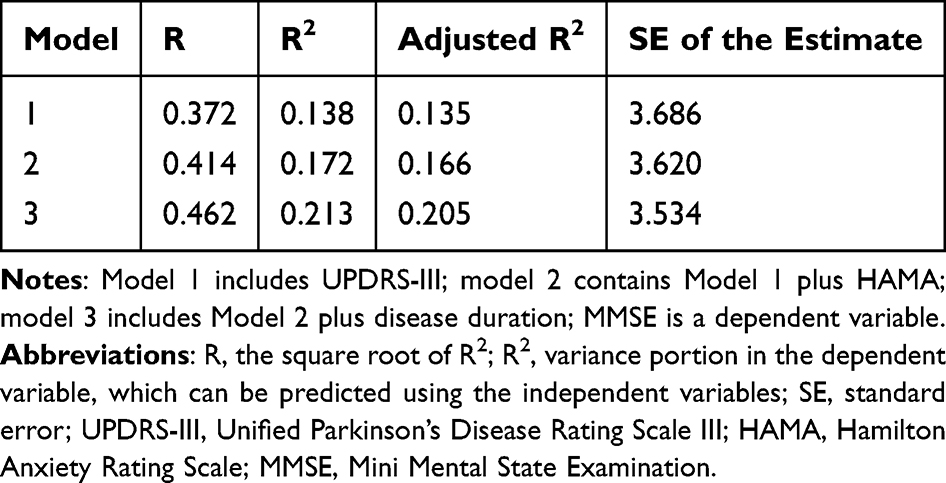 |
Table 5 Summary Results of Generalized Linear Models (Stepwise Including Method) Assessing the Effect of UPDRS III Score, HAMA Score and Disease Duration on MMSE Score |
Discussion
This is the first study to investigate the association between specific pain subtypes and cognitive impairment in PD using the KPPS. Our findings demonstrate that patients with cognitive impairment experience greater pain severity than those with normal cognition, and patients with cognitive impairment are more prone to develop chronic pain, central pain, visceral pain, “off” period dystonia, discoloration/swelling, and generalized lower abdominal pain in PD.
In line with previous studies,5,17 the prevalence of cognitive impairment in our cohort was 56.4%, and female patients were more likely to develop cognitive deficits. Additionally, patients with cognitive impairment were older, had a higher age at disease onset, more severe motor symptoms, and higher levels of anxiety, depression, and sleep disturbances, which is also consistent with prior reports.6
Pain severity was significantly higher in patients with cognitive impairment. Neurophysiological studies support this finding; for instance, Okada et al reported reduced amplitudes of pain-related somatosensory evoked potentials and impaired attention and memory in PD patients.13 Cruz-Almeida et al found that deficits in working memory and inhibitory function were associated with higher pain interference, possibly due to altered frontal lobe integrity.14 However, other studies, such as that by Engels et al, found no direct relationship between cognition and pain, instead attributing variance in pain perception primarily to depression and anxiety symptoms.12
In our study, chronic pain including central and visceral pain was more common in patients with cognitive impairment. Epidemiological data suggest that over half of individuals with chronic pain also experience cognitive deficits.18 Several mechanisms may explain this relationship. The neural resource hypothesis posits that persistent pain consumes neural resources, limiting capacity for cognitive processing.10 Chronic pain also alters activity in the dorsolateral prefrontal cortex, medial prefrontal cortex, and default mode network.19 The gate control theory proposed by Melzack and Wall further suggests that persistent activation of pain “gates” amplifies nociceptive input, increasing cognitive load.20 Neuroimaging studies have shown cortical thinning and disrupted connectivity in chronic pain-related networks, particularly in the insula and anterior cingulate cortex.8 Finally, chronic pain and PD share mechanisms of neuroinflammation and dopaminergic dysfunction, potentially accelerating neuronal decline in regions involved in both pain modulation and cognition.21
We also observed that “off” period dystonia was more severe in patients with cognitive impairment, likely reflecting overlapping dopaminergic dysfunction contributing to motor, cognitive, and pain-related symptoms.3 Similarly, generalized lower abdominal pain was more frequent in cognitively impaired patients. Emerging evidence implicates the gut-brain-microbiota axis in PD pathogenesis.22 For example, Shen et al reported altered gut microbiota composition in PD patients with cognitive impairment, including reduced short-chain fatty acid-producing bacteria and increased pathogenic species.23 Microbiome dysbiosis may exacerbate pain and cognitive decline through systemic inflammation and altered neurotransmitter regulation.24,25
Additionally, we observed that MMSE scores were positively correlated with radicular pain, a neuropathic pain subtype. Previous studies have demonstrated that neuropathic pain progressively impairs both working and long-term memory, accompanied by hippocampal remodeling and microglial activation.26 Huang et al identified circuitry abnormalities in patients with neuropathic pain using transcranial magnetic stimulation (TMS) combined with electroencephalogram co-registration (TMS-EEG), and reported increased activity within attentional-cognitive regions, including the anterior insula and supracallosal anterior cingulate cortex, compared with healthy controls.27 Furthermore, neuropathic pain has been shown to disrupt glutamatergic and GABAergic neurotransmission as well as brain-derived neurotrophic factor (BDNF) expression in the hippocampus.28 In addition, CXCL12-mediated monocyte recruitment into the perivascular space has been identified as a critical mechanism underlying neuroinflammation and the associated cognitive impairment observed in neuropathic pain.29
While our study identified a statistically significant association between pain and cognitive impairment in patients with PD, the effect size was relatively small, suggesting a modest strength of association.30,31 Further analysis of the risk factors for cognitive impairment indicated that the UPDRS Part III score, the HAMA score, and disease duration were the primary factors influencing cognitive function in these patients. Therefore, caution is warranted when interpreting the relationship between pain and cognitive function in PD, and any overinterpretation or exaggeration of their association should be avoided.
Moreover, our study has several limitations. First, the cohort predominantly comprised patients at moderate disease stages, and the use of analgesic medications was not recorded, which may have influenced the results. Second, the MMSE, while widely used, is not disease-specific and may underestimate certain cognitive domains. Future studies should incorporate Montreal Cognitive Assessment (MoCA) and PD-specific cognitive scales such as the Parkinson’s Disease Cognitive Rating Scale (PD-CRS). Third, our study found that PD patients with cognitive impairment had higher levels of anxiety, depression, sleep disturbances and disease severity. Therefore, when evaluating the relationship between pain and cognition, the potential mediating effects of mood disorders and disease severity should be taken into account. Finally, this study is a cross-sectional observational design; therefore, it cannot establish a causal relationship between pain and cognitive function in PD patients. Future larger cohort studies are needed to further clarify this association and improve the statistical power of these findings.
Conclusion
Cognitive impairment is highly prevalent in PD and is associated with increased overall pain severity. Crucially, our findings suggest a specific association between cognitive impairment and certain PD-related pain subtypes, particularly chronic pain (including central and visceral pain), “off” period dystonia, discoloration/swelling, generalized lower abdominal pain, and radicular pain. These associations may arise from shared pathophysiological mechanisms involving neural resource competition, structural and functional brain alterations, dopaminergic dysfunction, neuroinflammation, and gut-brain axis dysregulation. Future longitudinal studies utilizing PD-specific cognitive assessments and larger cohorts are needed to elucidate causal relationships and underlying mechanisms.
Acknowledgments
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (https://www.parinc.com). The authors thank the patients and their families for their participation in the study.
Funding
This work was supported by the Key Laboratory Project of Neurological Diseases in Jiangxi Province (2024SSY06072) and the Science and Technology Project of Jiangxi Provincial Health Commission (202410176; 202310282).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Goldman JG. Non-motor symptoms and treatments in parkinson’s disease. Neurol Clin. 2025;43(2):291–8. doi:10.1016/j.ncl.2024.12.008
2. Gao L, Huang W, Cai L, Peng Y. Pain assessment in chinese parkinson’s disease patients using king’s parkinson’s disease pain scale. J Pain Res. 2022;15:715–722. doi:10.2147/JPR.S353249
3. Patrick K, Cousins E, Spitznagel MB. Associations between cognitive screening performance and motor symptoms in Parkinson’s disease: A systematic review and meta-analysis. Dement Neuropsychol. 2024;18:e20230102. doi:10.1590/1980-5764-dn-2023-0102
4. Chaudhuri KR, Rizos A, Trenkwalder C, et al. King’s Parkinson’s disease pain scale, the first scale for pain in PD: an international validation. Mov Disord. 2015;30(12):1623–1631. doi:10.1002/mds.26270
5. Carceles-Cordon M, Weintraub D, Chen-Plotkin AS. Cognitive heterogeneity in Parkinson’s disease: a mechanistic view. Neuron. 2023;111(10):1531–1546. doi:10.1016/j.neuron.2023.03.021
6. Guo Y, Liu FT, Hou XH, et al. Predictors of cognitive impairment in Parkinson’s disease: a systematic review and meta-analysis of prospective cohort studies. J Neurol. 2021;268(8):2713–2722. doi:10.1007/s00415-020-09757-9
7. Patel M, Hasoon J, Diez Tafur R, Lo Bianco G, Abd-Elsayed A. The impact of chronic pain on cognitive function. Brain Sci. 2025;15(6):559. doi:10.3390/brainsci15060559
8. Chen J, Wang X, Xu Z. The relationship between chronic pain and cognitive impairment in the elderly: a review of current evidence. J Pain Res. 2023;16:2309–2319. doi:10.2147/JPR.S416253
9. Zhao LY, Zhang GF, Yang JJ, Diao YG, Hashimoto K. Knowledge mapping and emerging trends in cognitive impairment associated with chronic pain: a 2000-2024 bibliometric study. Brain Res Bull. 2025;220:111175. doi:10.1016/j.brainresbull.2024.111175
10. Gonzalez-Roldan AM, Delgado-Bitata M, Dorado A, Costa da Silva I, Montoya P. Chronic pain and its association with cognitive decline and brain function abnormalities in older adults: insights from EEG and neuropsychological assessment. Neurobiol Aging. 2025;150:172–181. doi:10.1016/j.neurobiolaging.2025.03.009
11. Defazio G, Antonini A, Tinazzi M, et al. Relationship between pain and motor and non-motor symptoms in Parkinson’s disease. Eur J Neurol. 2017;24(7):974–980. doi:10.1111/ene.13323
12. Engels G, Weeda WD, Vlaar AM, Weinstein HC, Scherder EJ. Clinical pain and neuropsychological functioning in parkinson’s disease: are they related? Parkinsons Dis. 2016;2016:8675930. doi:10.1155/2016/8675930
13. Okada A, Nakamura T, Suzuki J, et al. Impaired pain processing correlates with cognitive impairment in parkinson’s disease. Intern Med. 2016;55(21):3113–3118. doi:10.2169/internalmedicine.55.7067
14. Cruz-Almeida Y, Crowley SJ, Tanner J, Price CC. Pain severity and interference in different parkinson’s disease cognitive phenotypes. J Pain Res. 2020;13:3493–3497. doi:10.2147/JPR.S270669
15. Gao L, Huang W, Cai L, Li H. Association between sleep disturbances and pain subtypes in Parkinson’s disease. Neurol Sci. 2022;43(8):4785–4790. doi:10.1007/s10072-022-06030-x
16. Postuma RB, Berg D, Stern M, et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov Disord. 2015;30(12):1591–1601. doi:10.1002/mds.26424
17. Gao L, Nie K, Tang H, et al. Sex differences in cognition among Chinese people with Parkinson’s disease. J Clin Neurosci. 2015;22(3):488–492. doi:10.1016/j.jocn.2014.08.032
18. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
19. Zhou Z, Hui ES, Kranz GS, et al. Potential mechanisms underlying the accelerated cognitive decline in people with chronic low back pain: a scoping review. Ageing Res Rev. 2022;82:101767. doi:10.1016/j.arr.2022.101767
20. Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965;150(3699):971–979. doi:10.1126/science.150.3699.971
21. Vazirian F, Tian J, Jane A, et al. Chronic musculoskeletal pain and risk of incident parkinson’s disease: a 13-year longitudinal study. Mov Disord. 2025;40(1):87–96. doi:10.1002/mds.30046
22. Yadav S, Raj RG. Parkinson’s disease and the gut microbiota connection: unveiling dysbiosis and exploring therapeutic horizons. Neuroscience. 2025;581:1–15. doi:10.1016/j.neuroscience.2025.07.003
23. Shen X, Leng B, Zhang S, et al. Secondary analysis reveals gut microbiota differences in patients with Parkinson’s disease and/or cognitive impairment. Microbiome Res Rep. 2024;3(4):42. doi:10.20517/mrr.2024.35
24. Gonzalez-Alvarez ME, Sanchez-Romero EA, Turroni S, Fernandez-Carnero J, Villafane JH. Correlation between the altered gut microbiome and lifestyle interventions in chronic widespread pain patients: a systematic review. Medicina. 2023;59(2). doi:10.3390/medicina59020256
25. Freidin MB, Stalteri MA, Wells PM, et al. An association between chronic widespread pain and the gut microbiome. Rheumatology. 2021;60(8):3727–3737. doi:10.1093/rheumatology/keaa847
26. Tyrtyshnaia A, Manzhulo I, Egoraeva A, Ivashkevich D. Cognitive and affective dysregulation in neuropathic pain: associated hippocampal remodeling and microglial activation. Int J Mol Sci. 2025;26(13). doi:10.3390/ijms26136460
27. Huang Z, Wang Y, Yan Y, et al. Identifying neural circuitry abnormalities in neuropathic pain with transcranial magnetic stimulation and electroencephalogram co-registration. Neurotherapeutics. 2025;22(2):e00496. doi:10.1016/j.neurot.2024.e00496
28. Saffarpour S, Shaabani M, Naghdi N, Farahmandfar M, Janzadeh A, Nasirinezhad F. In vivo evaluation of the hippocampal glutamate, GABA and the BDNF levels associated with spatial memory performance in a rodent model of neuropathic pain. Physiol Behav. 2017;175:97–103. doi:10.1016/j.physbeh.2017.03.025
29. Mai CL, Tan Z, Xu YN, et al. CXCL12-mediated monocyte transmigration into brain perivascular space leads to neuroinflammation and memory deficit in neuropathic pain. Theranostics. 2021;11(3):1059–1078. doi:10.7150/thno.44364
30. Zieliński G. Effect size guidelines for individual and group differences in physiotherapy. Arch Phys Med Rehabil. 2025;106(12):1844–1849. doi:10.1016/j.apmr.2025.05.013
31. Sullivan GM, Feinn R. Using effect size-or why the p value is not enough. J Grad Med Educ. 2012;4(3):279–282. doi:10.4300/JGME-D-12-00156.1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.