Back to Journals » Journal of Inflammation Research » Volume 17
Association Between Number of Missing Teeth and Hyperlipidemia: The TCLSIH Cohort Study
Authors Qiao F, Guo H, Zhang J, Zhang Q, Liu L, Meng G, Wu H, Gu Y, Song K, Li C, Niu K ![]()
Received 22 November 2023
Accepted for publication 1 February 2024
Published 17 February 2024 Volume 2024:17 Pages 1095—1104
DOI https://doi.org/10.2147/JIR.S443940
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Feng Qiao,1,2 Hong Guo,1,2 Jing Zhang,1,2 Qing Zhang,3 Li Liu,3 Ge Meng,2 Hongmei Wu,2 Yeqing Gu,2 Kun Song,3 Changyi Li,1 Kaijun Niu2,3
1School of Dentistry, Stomatological Hospital, Tianjin Medical University, Tianjin, People’s Republic of China; 2Nutritional Epidemiology Institute and School of Public Health, Tianjin Medical University, Tianjin, People’s Republic of China; 3Health Management Centre, Tianjin Medical University General Hospital, Tianjin, People’s Republic of China
Correspondence: Kaijun Niu, Nutritional Epidemiology Institute and School of Public Health, Tianjin Medical University, 22 Qixiangtai Road, Heping District, Tianjin, People’s Republic of China, Email [email protected]; [email protected] Changyi Li, School of Dentistry, Stomatological Hospital, Tianjin Medical University, No. 12, Qixiangtai Road, Heping District, Tianjin, 300070, People’s Republic of China, Email [email protected]
Background: To explore the association between the number of missing teeth and the prevalence of hyperlipidemia in a Chinese adult population.
Methods: 13,932 adults were investigated in the TCLSIH cohort study. The number of missing teeth was determined at baseline through a self-reported questionnaire, and then classified into three categories: 0, 1– 2, and ≥ 3. We defined hyperlipidemia as total cholesterol (TC) ≥ 5.17 mmol/L or triglycerides (TG) ≥ 1.7 mmol/L or low-density lipoprotein (LDL) cholesterol ≥ 3.37 mmol/L or a self-report of physician-diagnosed hyperlipidemia during follow-up visits. Cox proportional-hazards regression models were employed to assess the relationship between the number of missing teeth and incident hyperlipidemia.
Results: A total of 6756 first-incident cases of hyperlipidemia occurred during 42,048 person-years of follow-up (median follow-up, 4.2 years). After adjusted confounders, multivariable HRs and 95% CI for incident of hyperlipidemia across the categories of missing teeth were as follows: in male participants, 1.00 (reference), 1.10 (0.98, 1.22), and 1.03 (0.91, 1.16) (P for trend = 0.30); in female participants, 1.00 (reference), 1.09 (0.99, 1.19), and 1.18 (1.04, 1.33) (P for trend < 0.01).
Conclusion: The number of missing teeth is associated with an increased risk of hyperlipidemia in female participants but not in male participants. Systemic chronic inflammation may potentially mediate this association.
Keywords: tooth loss, dyslipidemia, epidemiological studies, population health, inflammation
Introduction
Hyperlipidemia, characterized by an imbalance in cholesterol levels, is strongly linked to the development of stroke, myocardial infarction, and other cardiovascular diseases.1–3 It plays a significant role in the pathogenesis of cardiovascular diseases (CVD), contributing to increased morbidity and mortality rates.4 Meanwhile, it has a high global prevalence and imposes great challenges on public health and healthcare systems worldwide.5 Understanding the risk factors underlying hyperlipidemia has significant public health implications for disease prevention.
Tooth loss is the final consequence of prevalent oral diseases like periodontitis and caries, both of which are considered as oral bacterial infections that give rise to inflammatory processes in the oral cavity.6,7 Previous studies have shown that the cumulative oral inflammation promotes systemic inflammation level.8 There is compelling evidence that periodontitis raises the burden of cumulative systemic inflammation and adds to cardiovascular disease risk factors.9–11 Moreover, Streptococcus mutans (S. mutans), which is widely recognized as the primary causative pathogen for dental caries, has been identified in atheromatous plaque specimens12 and cardiovascular specimens,13 suggesting a potential association with CVD.
The cumulative inflammatory status of oral health, as indicated by the number of missing teeth, is widely recognized as a crucial factor in assessing overall oral health.14,15 Self-reported count of absent teeth has previously been validated as reliable indicator for assessing oral health in large-scale population surveys.16 The presence of multiple missing teeth can suggest that the individual has a history of periodontitis.14 The association between periodontitis and inflammation is well-established and supported by extensive scientific evidence.17,18 The systemic inflammation is thought to be a result of the chronic inflammatory burden imposed by periodontal disease. Tooth loss may then reflect the past inflammatory and infectious state of oral health.15
Several studies suggest a link between oral health, specifically tooth loss, and CVD.19–21 Subjects with missing teeth were more likely to suffer from metabolic syndrome (MetS), whereas dyslipidemia is a key component of MetS. These lipid metabolism abnormalities are a major risk factor for CVD. In addition, a recent systematic review also documented that periodontitis was linked to hyperlipidemia in humans.22 All these data imply that the number of missing teeth may also be related to hyperlipidemia, mediated by systemic chronic inflammation. Despite previous findings, no long-term prospective cohort investigations have reported the correlation between the number of missing teeth and hyperlipidemia within the general adult population of China.
Therefore, this research premise aimed to explore if the baseline number of missing teeth was linked to the incidence of hyperlipidemia in a prospective cohort investigation in the Chinese general adult population.
Methods
Study Design and Sample
The cohort examined in this analysis consisted of individuals belonging to the Tianjin Chronic Low-Grade Systemic Inflammation and Health (TCLSIH) cohort. This particular study, TCLSIH cohort, is an ongoing and prospective investigation into dynamic cohort trends. The cohort was established in August 2012 and officially launched in May 2013. Participants were selected from multiple hospitals’ affiliated health examination centers (or health management centers), urban/suburban/rural communities, and different levels of nursing homes that agreed to participate in the survey.
The inclusion criteria for this study consisted of adults aged 18 years and above who had been residents of Tianjin for a minimum of 5 years. The study randomly selected adults who underwent annual medical health examinations (including routine health checks such as height, weight, waist circumference, blood pressure, blood routine, blood biochemistry, etc.) to complete a structured lifestyle questionnaire at baseline. Participants who had undergone health examinations, such as a blood test, were recruited for the study and given a detailed questionnaire about tooth loss, smoking and drinking habits, disease history, education, physical activity, socioeconomic status, lifestyle factors, as well as dietary intake. The cohort achieved an overall response rate of 97.1%, excluding individuals with disabilities, severe mental illness, severe cognitive impairment, hearing impairment, pregnancy, and other factors.
The implementation of this investigation adheres to the principles stated in the Helsinki Declaration, with all participants explicitly granting their consent through written informed documentation. The TCLSIH cohort study obtained approval from the Ethics Committee of Tianjin Medical University (No.: TMUhMEC201430).
Our study included 20,155 participants initially. The exclusion criteria were as follows: (1) invalid questionnaires (n = 959), (2) baseline hyperlipidemia (n = 2135), (3) a history of cardiovascular disease (n = 837), (4) a history of cancer (n = 167), and people taking lipid-lowering agents (n = 403). In addition, we further exclude those failure to follow up during the study (n = 1722, follow-up rate = 89.0%). Following the application of the criteria for participation, there were a total of 13,932 participants who participated in the final cohort analyses. A flowchart is shown in Figure 1.
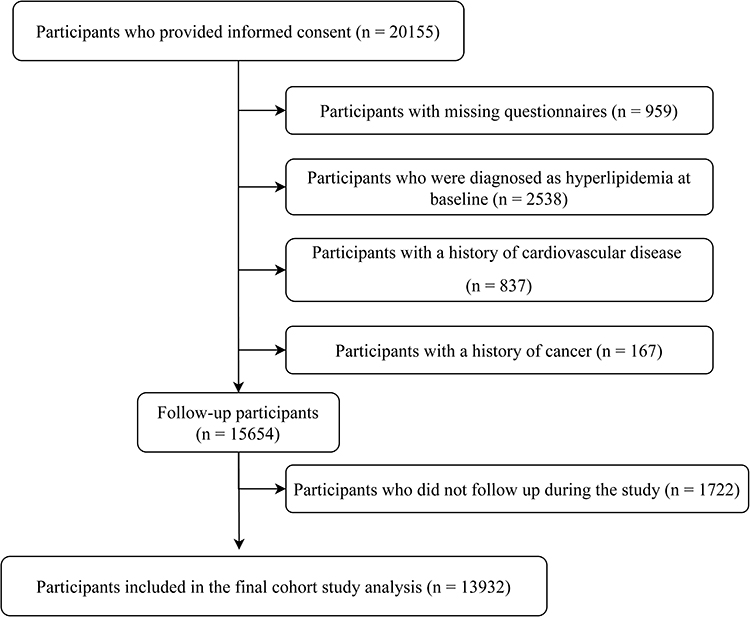 |
Figure 1 Flow diagram showing the selection of the study population. |
Determination of the Number of Missing Teeth
In the survey, participants were asked to recall and document the number of teeth they were missing (excluding wisdom teeth). For those who had difficulty remembering, healthcare professionals provided assistance during the examination. In accordance with the National Health and Nutrition Survey’s findings on adult tooth loss, the average number of permanent teeth among individuals aged 20 to 64 was 24.9 teeth.23 Consequently, we categorized the number of missing teeth into three groups: 0, 1–2, and ≥3. The first group, consisting of individuals with 0 missing teeth, represents subjects with periodontal health (controls). The second group, with 1 to 2 missing teeth, is likely attributed to localized periodontal or caries disease affecting individual teeth. Individuals missing ≥3 teeth may have experienced long-term moderate chronic periodontitis or other minor reasons leading to additional tooth loss.
Assessment of Hyperlipidemia
The definition of hyperlipidemia was determined by considering the onset date as the midpoint between the last checkup where the values were within normal range and the checkup date, which was based on the results obtained from analyzing fasting blood samples. These blood samples were drawn from the antecubital area after an overnight fast of 8–12 hours and collected in silicone-coated vacuum plastic tubes for the purpose of analyzing blood lipid levels. The enzymatic methods were used to assess the levels of triglycerides (TG) and total cholesterol (TC), while the precipitation method involving polyvinyl sulfuric acid was employed to measure LDL cholesterol (LDL-C), and the chemical precipitation method was used to determine HDL cholesterol (HDL-C). Hyperlipidemia was defined as TG levels equal to or above 1.7 mmol/L, TC levels equal to or above 5.17 mmol/L, LDL-C levels equal to or above 3.37 mmol/L, or a self-reported diagnosis of hyperlipidemia by a physician during follow-up visits.24
Assessment of Other Variables
Demographic factors (gender, education level, employment status, age, and income level), level of physical activity, family medical history, smoking habits, and personal medical records were obtained via completion of a comprehensive questionnaire.25 Trained professionals adhering to standardized protocols carried out the measurement and recording of participants’ height and weight. Body mass index (BMI) was computed by dividing weight (in kilograms) by the square of height (in meters), providing a measure of overall body composition. Waist circumference (WC) was assessed using a measuring tape placed near the navel, while participants stood upright and breathed normally (in centimeters). To evaluate dietary habits, a modified version of the food frequency questionnaire (FFQ) was employed. Lastly, physical activity levels during the previous week were assessed utilizing the International Physical Activity Questionnaire (IPAQ).
Serum fasting blood glucose (FBG) contents were determined via the glucose oxidase approach. Type 2 diabetes was defined according to the World Health Organization26 as a fasting blood glucose level of ≥ 7 mmol/L or a history of diabetes. Blood pressure was measured using an electronic blood pressure monitor (TM-2655, A&D Company, Japan). Before measuring blood pressure, participants were asked to rest for five minutes and then position their right upper arm at heart level to begin the measurement. The average of two measurements was taken as the final recorded blood pressure value. If the systolic blood pressure was ≥140 mmHg, the diastolic blood pressure was ≥90 mmHg or the participant self-reported a history of hypertension, it was defined as having hypertension. All protocols were completed in the same environment to address potential sources of bias.
Statistical Analysis
Statistical analyses were conducted using SAS version 9.3 (SAS Institute Inc., Cary, NC, USA). Geometric means (95% CI) are used to present continuous variables, while percentages are used to present categorical variables. The number of missing teeth was considered the independent variable, whilst hyperlipidemia incidence was the dependent variable. Calculation of the follow-up time was done from the date of completion of the baseline FFQ survey to the date of the first diagnosis of hyperlipidemia, the end of follow-up (December 31, 2019), or loss to follow-up, whichever was earliest. Due to significant differences in the prevalence of hyperlipidemia between males and females, we conducted a stratified analysis by gender. We adopted four Cox proportional-hazards regression models to determine the relationship between the number of missing teeth with hyperlipidemia risk. Model 1 was a crude model. In model 2, we adjusted only for age and BMI, and in model 3, we additionally adjusted for smoking status, family history of disease (including cardiovascular disease, hypertension, hyperlipidemia, and diabetes), drinking status, hypertension, diabetes, education level, depressive symptoms, working status, healthy pattern score, total energy intake, household income, physical activity, sweet pattern score, and animal pattern score. Model 4 was additionally adjusted for the baseline values of serum lipids including LDL, TG, and HDL. The linear trend test was determined by including the categories of tooth loss (0, 1–2, and ≥3) as continuous variables in the model. The hazard ratios and 95% CIs were determined. Two-tailed p-values were used for all statistical tests, and a significance level of P < 0.05 was considered statistically significant.
Results
Baseline Characteristic of Participants
From May 2013 to December 2019, a total of 13,932 subjects ultimately completed the study. Tables 1 and 2 display the statistics of the male and female participants at baseline, respectively. In this cohort study, 49.6% (6914 of 13,932) of participants were male, and 50.4% (7018 of 13,932) were female. Male participants with more missing teeth were older; had higher BMI, LDL-C, WC, SBP, TC, TG, FBG, DBP, as well as physical activity (PA); consumed more alcohol (“every day”); exhibited higher smoking status rates (“current smoker”, “ex-smoker”); and had diabetes as well as a family history of cardiovascular and hypertension but had lower total energy intake, healthy intake, education level, or household income. Furthermore, female participants with more missing teeth were older; harbored higher LDL-C, DBP, WC, TC, BMI, TG, SBP, FBG, and PA; harbored higher smoking status rates (“current smoker”); and had diabetes as well as a family history of cardiovascular and hypertension but lower healthy intake, education level, as well as household income. Other indicators were not remarkably different.
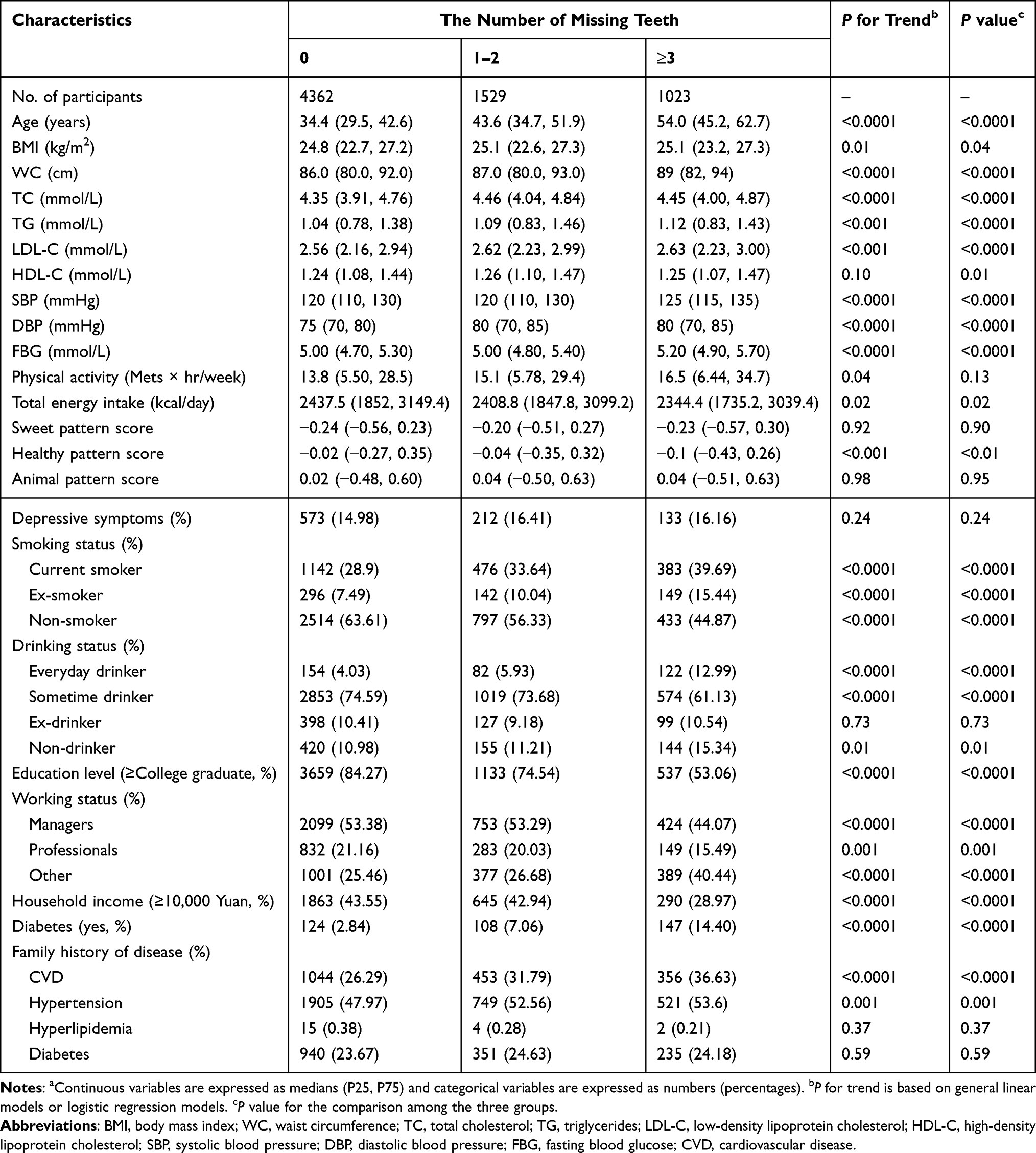 |
Table 1 Baseline Characteristics of Participants According to the Number of Missing Teeth in Male (n=6914)a |
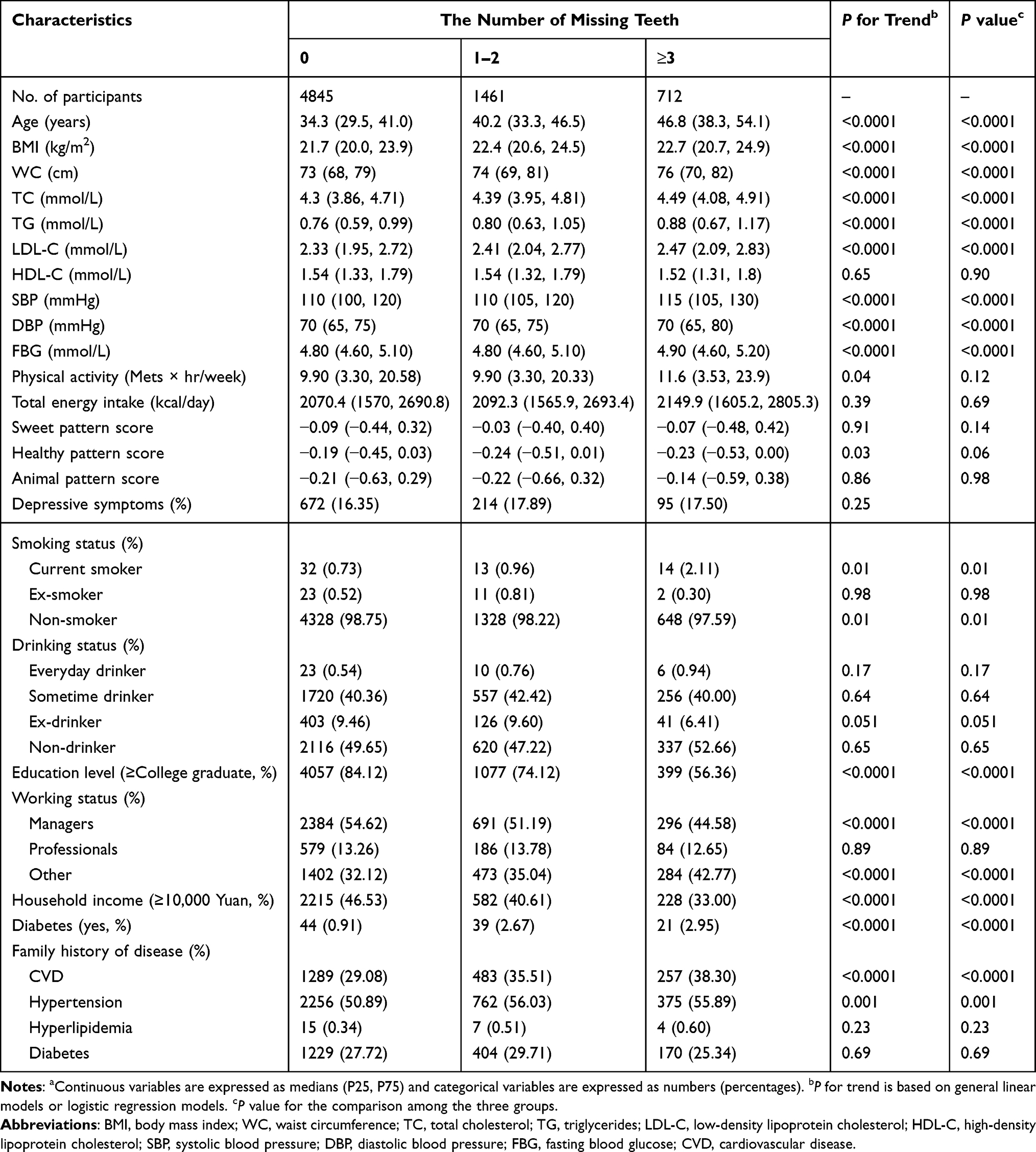 |
Table 2 Baseline Characteristics of Participants According to the Number of Missing Teeth in Females (n=7018)a |
Relationship of the Number of Missing Teeth with Hyperlipidemia
During a median follow-up of 4.2 years (range, 1.0–6.0 years), we identified 6756 incident hyperlipidemia cases during 42,048 person-years of follow-up. Table 3 provides the relationship of the number of missing teeth with hyperlipidemia after adjusting for confounding factors. In model 3, the multivariable hazard ratios (95% CI) of hyperlipidemia across the categories of missing teeth were as follows: in male participants, 1.00 (reference), 1.04 (0.96, 1.13), and 1.01 (0.91, 1.11) (P for trend = 0.63); in female participants, 1.00 (reference), 1.08 (0.99, 1.18), and 1.23 (1.09, 1.38) (P for trend < 0.001), respectively. In model 4, the results showed that the association between the number of missing teeth and hyperlipidemia remained in females, but the effect size was weakened from 23% to 18% after adjusting for baseline blood lipid levels. There was a remarkable connection between the number of missing teeth and hyperlipidemia only in female participants. P for the trend test across the three categories (0, 1–2, and ≥3) was significant.
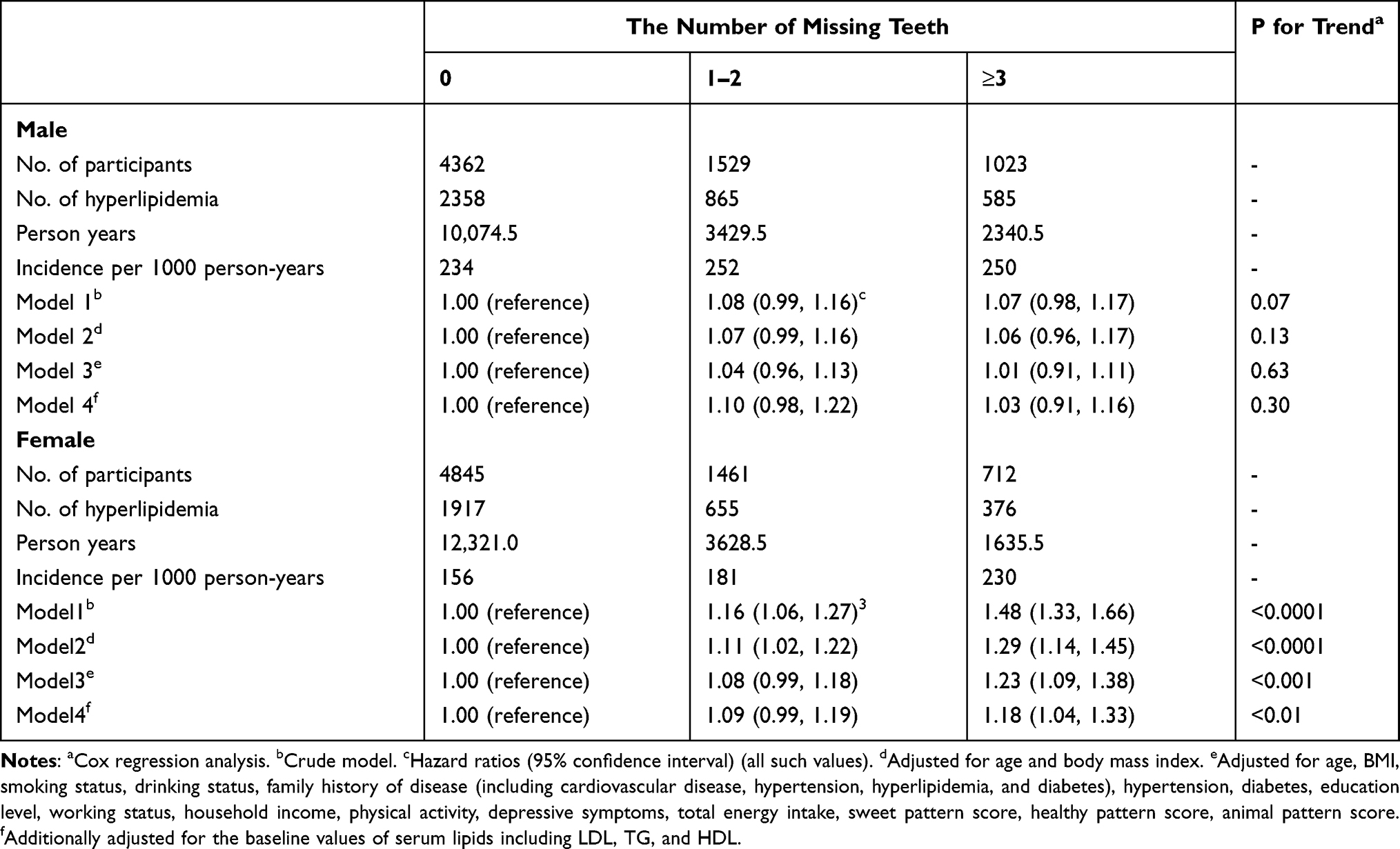 |
Table 3 Adjusted Hazard Ratios (95% Confidence Intervals) for Associations of the Number of Missing Teeth with the Incidence of Hyperlipidemia |
Discussion
After adjusting for potential confounders, female subjects who had ≥3 missing teeth had an 18% increased risk of hyperlipidemia, in comparison with those with no missing teeth. The primary finding of this prospective cohort study is an association between the incidence of hyperlipidemia and the number of missing teeth in females.
It is reported that the missing teeth and periodontal disease may increase the rate of prevalence of several chronic noncommunicable diseases.27 Accumulated evidence has indicated a correlation between the number of missing teeth and various CVD.19,20,28,29 Meanwhile, periodontitis is associated with abnormal lipid profiles.30,31 Meanwhile, studies have also found that women harboring low contents of HDL cholesterol had a remarkably higher risk of periodontitis32 and that high serum total cholesterol was linked with periodontitis.33 As an important measure for oral health, a national cohort investigation also showed that frequent brushing of teeth could reduce blood TG contents and increase HDL-C contents.34 Our study has contributed to the existing body of evidence in this field, enhancing both the content and strength of the evidence to a certain degree.
The number of missing teeth is often used as a surrogate marker of periodontitis for some studies.14 Numerous studies have investigated the relationship between the number of missing teeth and periodontitis. The association between periodontitis and inflammation is well-established and supported by extensive scientific evidence. Hence, the number of missing teeth may then reflect the past inflammatory and infectious state of oral health.35
The potential mechanisms and biological foundations of this association may be as follows. First, chronic oral infections such as periodontitis and dental caries often lead to tooth loss which can trigger systemic low-grade inflammation, as well as insulin resistance. This inflammation may disrupt and affect lipid metabolism, leading to increased lipid levels in the blood. Second, the oral microbiome is strongly associated with the gut microbiome. The loss of teeth can alter the composition of the oral microbiota, which may subsequently impact the gut microbiota. Several studies have suggested that dysbiosis of the gut microbiota may affect lipid metabolism, resulting in the development of hyperlipidemia.36 Third, tooth loss can have an impact on an individual’s dietary habits. Difficulties with chewing and oral discomfort resulting from tooth loss can limit food choices and intake, leading to an imbalanced diet that is high in fat, sugar, and cholesterol. This can increase the risk of hyperlipidemia.37 Fourth, both tooth loss and hyperlipidemia may be influenced by socioeconomic factors. Individuals from lower socioeconomic backgrounds may have poorer access to dental care and a higher likelihood of consuming a diet high in unhealthy fats, both of which could contribute to tooth loss and hyperlipidemia. The socioeconomic status differences and hormonal level disparities in gender could potentially explain the relationship between tooth loss and hyperlipidemia in part. Further study is required to elucidate these potential mechanisms and to understand the extent to which they contribute to the association between missing teeth and hyperlipidemia.
The strengths of this study are the use of longitudinal data and the long-term cohort study, with a higher level of evidence, we adjusted for many confounders, with evidence suggesting a causal relationship to some extent, which has rarely been reported in previous studies. In addition, this study directly explored the relationship between missing teeth and hyperlipidemia in the large Chinese adult population. Such information could inform strategies for preventing and managing both conditions, potentially improving cardiovascular health outcomes.
A limitation of this research work was that the number of missing teeth was recalled by participants and the reasons for tooth loss were not recorded, making it more subjective and prone to recall bias. The number of missing teeth was assessed once at baseline, therefore, the changes in the number of missing teeth over time were not considered. Future research warrants investigating the association with repeated measures data. Finally, it cannot establish a causal relationship and the likelihood of residual confounding may remain.
Conclusion
The number of missing teeth was independently associated with the incidence of hyperlipidemia in females. Therefore, incorporating oral health maintenance into primary prevention of hyperlipidemia holds significant public health significance.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The research protocol was granted approval by the Institutional Review Board of Tianjin Medical University (No: TMUhMEC201430), and all subjects participated voluntarily in the research work and provided written informed consent.
Acknowledgments
We would like to thank the authors Tingjing Zhang, Huiping Li, Xuena Wang, Juanjuan Zhang, Shaomei Sun, Xing Wang, Ming Zhou, Qiyu Jia who have contributed to this scientific literature. We are truly grateful for their unwavering support and collaboration throughout the research process.
Funding
This study was supported by grants from the National Natural Science Foundation of China (No. 81673166, 81372118, 81372467 and81302422); the key technologies R&D program of Tianjin (Key Project: No. 11ZCGYSY05700, 12ZCZDSY20400, 13ZCZDSY20200, and 15YFYZSY00020); The Science and Technology Project of Tianjin Health Commission (ZC20134).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Holmes MV, Millwood IY, Kartsonaki C, et al. Lipids, lipoproteins, and metabolites and risk of myocardial infarction and stroke. J Am Coll Cardiol. 2018;71(6):620–632 doi:10.1016/j.jacc.2017.12.006.
2. Hindy G, Engström G, Larsson SC, et al. Role of blood lipids in the development of ischemic stroke and its subtypes: a Mendelian randomization study. Stroke. 2018;49(4):820–827. doi:10.1161/STROKEAHA.117.019653
3. Allara E, Morani G, Carter P, et al. Genetic determinants of lipids and cardiovascular disease outcomes: a wide-angled Mendelian randomization investigation. Circ Genomic Precis Med. 2019;12(12):e002711. doi:10.1161/CIRCGEN.119.002711
4. Karr S. Epidemiology and management of hyperlipidemia. Am J Manag Care. 2017;23(9 Suppl):S139–S148. PMID: 28978219.
5. Smith DG. Epidemiology of dyslipidemia and economic burden on the healthcare system. Am J Manag Care. 2007;13 Suppl 3(3):S68–71. PMID: 17596114.
6. Richards W, Ameen J, Coll AM, Higgs G. Reasons for tooth extraction in four general dental practices in South Wales. Br Dent J. 2005;198(5):275–278. doi:10.1038/sj.bdj.4812119
7. Reich E, Hiller KA. Reasons for tooth extraction in the western states of Germany. Oral Epidemiol. 1993;21(6):379–383. doi:10.1111/j.1600-0528.1993.tb01103.x
8. Pizzo G, Guiglia R, Russo LL, Campisi G. Dentistry and internal medicine: from the focal infection theory to the periodontal medicine concept. Eur J Internal Med. 2010;21(6):496–502. doi:10.1016/j.ejim.2010.07.011
9. Arimatsu K, Yamada H, Miyazawa H, et al. Oral pathobiont induces systemic inflammation and metabolic changes associated with alteration of gut microbiota. Sci Rep. 2014;4(1):4828. doi:10.1038/srep04828
10. Paraskevas S, Huizinga JD, Loos BG. A systematic review and meta-analyses on C-reactive protein in relation to periodontitis. J Clin Periodontol. 2008;35(4):277–290. doi:10.1111/j.1600-051X.2007.01173.x
11. Winning L, Patterson CC, Cullen KM, et al. The association between subgingival periodontal pathogens and systemic inflammation. J Clin Periodontol. 2015;42(9):799–806. doi:10.1111/jcpe.12450
12. Nakano K, Inaba H, Nomura R, et al. Detection of cariogenic Streptococcus mutans in extirpated heart valve and atheromatous plaque specimens. J Clin Microbiol. 2006;44(9):3313–3317. doi:10.1128/JCM.00377-06
13. Nakano K, Nemoto H, Nomura R, et al. Detection of oral bacteria in cardiovascular specimens. Oral Microbiol Immunol. 2009;24(1):64–68. doi:10.1111/j.1399-302X.2008.00479.x
14. Furuta M, Liu A, Shinagawa T, et al. Tooth loss and metabolic syndrome in middle‐aged Japanese adults. J Clin Periodontol. 2016;43(6):482–491. doi:10.1111/jcpe.12523
15. Kassebaum N, Bernabé E, Dahiya M, Bhandari B, Murray C, Marcenes W. Global burden of severe tooth loss: a systematic review and meta-analysis. J Dent Res. 2014;93(7_suppl):20S–28S. doi:10.1177/0022034514537828
16. Matsui D, Yamamoto T, Nishigaki M, et al. Validity of self-reported number of teeth and oral health variables. BMC Oral Health. 2017;17(1):1–8. doi:10.1186/s12903-016-0248-2
17. Hajishengallis G. Periodontitis: from microbial immune subversion to systemic inflammation. Nat Rev Immunol. 2015;15(1):30–44. doi:10.1038/nri3785
18. Golub LM, Lee HM. Periodontal therapeutics: current host‐modulation agents and future directions. Periodontology. 2020;82(1):186–204. doi:10.1111/prd.12315
19. Aoyama N, Suzuki JI, Kobayashi N, et al. Associations among tooth loss, systemic inflammation and antibody titers to periodontal pathogens in Japanese patients with cardiovascular disease. J Periodontal Res. 2018;53(1):117–122. doi:10.1111/jre.12494
20. Lee H, Choi E, Park J, Han K, Oh S. Tooth loss predicts myocardial infarction, heart failure, stroke, and death. J Dent Res. 2019;98(2):164–170. doi:10.1177/0022034518814829
21. Peng J, Song J, Han J, et al. The relationship between tooth loss and mortality from all causes, cardiovascular diseases, and coronary heart disease in the general population: systematic review and dose–response meta-analysis of prospective cohort studies. Biosci Rep. 2019;39(1):BSR20181773. doi:10.1042/BSR20181773
22. Xu J, Duan X. Association between periodontitis and hyperlipidaemia: a systematic review and meta-analysis. Clin Exp Pharmacol Physiol. 2020;47(11):1861–1873. doi:10.1111/1440-1681.13372
23. NIDCR. Tooth Loss Statistics for Adults Age 20 to 64. Tooth Loss Statistics for Adults Age 20 to 64 Blog. NIDCR; 2018.
24. Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults, E. Expert Panel on Detection E. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA. 2001;285(19):2486–2497. doi:10.1001/jama.285.19.2486
25. Gu Y, Li H, Bao X, et al. The relationship between thyroid function and the prevalence of type 2 diabetes mellitus in euthyroid subjects. J Clin Endocrinol Metab. 2017;102(2):434–442. doi:10.1210/jc.2016-2965
26. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
27. Cheon HW, Yu, MS, Choi, MH. The association of oral diseases and chronic diseases in Korean adult population. J Korean Soc Dent Hyg. 2012;12(2):235–249. doi:10.13065/jksdh.2012.12.2.235
28. Vedin O, Hagström E, Östlund O, et al. Associations between tooth loss and prognostic biomarkers and the risk for cardiovascular events in patients with stable coronary heart disease. Int J Cardiol. 2017;245:271–276. doi:10.1016/j.ijcard.2017.07.036
29. Cheng F, Zhang M, Wang Q, et al. Tooth loss and risk of cardiovascular disease and stroke: a dose-response meta analysis of prospective cohort studies. PLoS One. 2018;13(3):e0194563. doi:10.1371/journal.pone.0194563
30. Nepomuceno R, Pigossi SC, Finoti LS, et al. Serum lipid levels in patients with periodontal disease: a meta-analysis and meta-regression. J Clin Periodontol. 2017;44(12):1192–1207. doi:10.1111/jcpe.12792
31. Duzagac E, Cifcibasi E, Erdem M, et al. Is obesity associated with healing after non‐surgical periodontal therapy? A local vs. systemic evaluation. J Periodontal Res. 2016;51(5):604–612. doi:10.1111/jre.12340
32. Lee S, Im A, Burm E, Ha M. Association between periodontitis and blood lipid levels in a Korean population. J Periodontol. 2018;89(1):28–35. doi:10.1902/jop.2017.170111
33. Thapa S, Wei F. Association between high serum total cholesterol and periodontitis: national health and nutrition examination survey 2011 to 2012 study of American adults. J Periodontol. 2016;87(11):1286–1294. doi:10.1902/jop.2016.150648
34. Song TJ, Kim JW, Kim J. Oral health and changes in lipid profile: a nationwide cohort study. J Clin Periodontol. 2020;47(12):1437–1445. doi:10.1111/jcpe.13373
35. Kassebaum N, Bernabé E, Dahiya M, Bhandari B, Murray C, Marcenes W. Global burden of severe periodontitis in 1990–2010: a systematic review and meta-regression. J Dent Res. 2014;93(11):1045–1053. doi:10.1177/0022034514552491
36. Benguigui C, Bongard V, Ruidavets JB, et al. Metabolic syndrome, insulin resistance, and periodontitis: a cross-sectional study in a middle-aged French population. J Clin Periodontol. 2010;37(7):601–608. doi:10.1111/j.1600-051X.2010.01571.x
37. Zelig R, Goldstein S, Touger-Decker R, et al. Tooth loss and nutritional status in older adults: a systematic review and meta-analysis. JDR Clin Trans Res. 2022;7(1):4–15. doi:10.1177/2380084420981016
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Manifestations and Risk Factors of Osteoporosis in Patients with Type 2 Diabetes Mellitus
Wang Y, Du Y, Zuo J, He L, Shi Y, Yuan Y, Liu Y, Zheng H, Wang H
Journal of Inflammation Research 2026, 19:575474
Published Date: 17 March 2026