Back to Journals » Journal of Inflammation Research » Volume 16
Association Between Neutrophil-to-Lymphocyte Ratio and Benign Prostatic Hyperplasia: Results from the TCLSIH Cohort Study
Authors Song Y, Gu Y, Guo H, Yang H, Wang X, Wu H, Wang A ![]() , Wang H, Zhang Q, Zhang Q, Liu L, Meng G, Liu B, Niu K
, Wang H, Zhang Q, Zhang Q, Liu L, Meng G, Liu B, Niu K ![]()
Received 14 August 2023
Accepted for publication 18 October 2023
Published 25 October 2023 Volume 2023:16 Pages 4857—4866
DOI https://doi.org/10.2147/JIR.S431049
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Yanqi Song,1 Yeqing Gu,2 Honglei Guo,3 Honghao Yang,4– 6 Xuena Wang,4– 6 Hongmei Wu,4– 6 Aidi Wang,1 Haijin Wang,1 Quan Zhang,1 Qing Zhang,7 Li Liu,7 Ge Meng,6 Baoshan Liu,1 Kaijun Niu4– 6
1Department of Traditional Chinese Medicine, Tianjin Medical University General Hospital, Tianjin, People’s Republic of China; 2Institute of Radiation Medicine, Chinese Academy of Medical Sciences & Peking Union Medical College, Tianjin, People’s Republic of China; 3School of Graduate, Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China; 4School of Public Health, Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China; 5School of Integrative Medicine, Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China; 6Nutritional Epidemiology Institute, Tianjin Medical University, Tianjin, People’s Republic of China; 7Health Management Centre, Tianjin Medical University General Hospital, Tianjin, People’s Republic of China
Correspondence: Kaijun Niu, Nutritional Epidemiology Institute, Tianjin Medical University, 22 Qixiangtai Road, Heping District, Tianjin, 300070, People’s Republic of China, Tel +86-22-83336613, Email [email protected]; [email protected] Baoshan Liu, Department of Traditional Chinese Medicine, Tianjin Medical University General Hospital, 154 Anshan Road, Heping District, Tianjin, 300052, People’s Republic of China, Tel +86-22-60362808, Email [email protected]
Purpose: The prevalence of benign prostatic hyperplasia (BPH) in the general Chinese adult male population has risen sharply over the past few decades. Increasing evidence suggests that inflammation plays an important role in the pathogenesis of BPH. To better understand the role of inflammation in the pathogenesis of BPH, we can use the neutrophil-to-lymphocyte ratio (NLR) because it is a simple and effective marker of inflammation and immunity. This study aims to prospectively investigate the association between NLR levels and the prevalence of BPH in a general Chinese adult male population.
Patients and Methods: This study included a total of 15,783 male participants free from BPH at baseline. NLR was measured according to the complete blood count. BPH was defined as total prostate volume (TPV) ≥ 30 mL, and TPV was determined by transabdominal ultrasonography. Multivariable Cox proportional hazards models were fitted to calculate hazards ratios (HRs) and corresponding 95% confidence intervals (CIs) for BPH risk with NLR levels.
Results: During a median follow-up of 2.7 years, 5078 BPH cases were documented. After adjusting for age, body mass index, smoking, alcohol, education, occupation, income, physical activity, total energy intake, personal and family history of disease, and inflammation markers, the multivariable-adjusted HRs of BPH were 1.00 (reference), 1.08 (95% CIs 0.99, 1.17), 1.10 (95% CIs1.02, 1.19), and 1.12 (95% CIs1.03, 1.21), respectively, for participants with NLR in the first, second, third, and fourth quartiles (P for trend < 0.01).
Conclusion: Higher NLR levels were associated with a higher risk of BPH in Chinese adult male population. Our findings support the notion that NLR levels may be an important target for BPH prevention and intervention.
Keywords: neutrophil to lymphocyte ratio, inflammation, benign prostatic hyperplasia, prospective cohort study
Introduction
Prostate cancer (PCa) is the second most prevalent cancer type diagnosed worldwide and the major cause of cancer-related death among human beings.1 Benign prostatic hyperplasia (BPH) is the most prevalent prostate condition affecting men as they age and a significant risk factor for PCa development.2 Moreover, BPH may cause symptoms of the lower urinary tract (LUTS) due to increased smooth muscle tone and resistance3 and blockage of the proximal urethra.4
Although several theories with empirical support tackle this point, the causes of BPH are multifactorial and not fully understood. A growing body of literature that recognized inflammation of the prostate plays a particularly critical role in the initiation and evolution of BPH and the progression of symptoms,5 and most of the studies underline that it has a causal or predictive role.6 Infections, hormonal changes, nutritional factors, immunological reactions, environmental factors, genetic predisposition, and even urine reflux inside the prostate’s collecting duct are all potential causes of inflammation.7 Meanwhile, a number of growth factors and cytokines may support an inflammatory process in the prostate.
The neutrophil-to-lymphocyte ratio (NLR) has gained popularity as a biomarker for determining the overall level of inflammation in recent years.8 It is also easy to measure and an inexpensive parameter that can be easily calculated from complete blood counts (CBCs).3 Multiple studies have clearly shown that the potential role of NLR in urology has generated considerable attention. For example, evidence suggests that NLR has a role, both in biochemical failure in prostate cancer and the spontaneous passage of ureteral stones.9,10 Extensive research has revealed that NLR is related to severe LUTS and intravesical prostatic protrusion (IPP) in men with BPH.3,11,12 However, small sample sizes limit the findings of all of these studies. Until now, there has been a lack of a well-designed prospective cohort to determine a causal relationship between NLR levels and the prevalence of BPH in the first place.
To address this research gap, the major purpose of the prospective cohort study was to investigate whether NLR levels are associated with the risk of BPH in a large-scale Chinese adult male population.
Methods
Study Design and Participants
The Tianjin Chronic Low-Grade Systemic Inflammation and Health (TCLSIH) cohort study (clinicaltrials.gov UMIN000027174) included this investigation. The cohort had been described in detail in our previous studies.13,14 This is in line with the ethical guidelines of the 1975 Declaration of Helsinki. The Institutional Review Board of Tianjin Medical University approved the study’s protocols and procedures under approval number TMUhMEC 201430, and each participant signed a written informed consent form. Also, this study complies with STROBE guidelines for cohort studies.
From January 2010 to December 2020, 35,238 Chinese adult male participants were enrolled in the TCLSIH cohort study; participants who had received at least one health examination and questionnaire, including physical examination, blood tests, socio-demographic characteristics, and lifestyle questionnaires. Among these individuals, we excluded 4828 participants who were lost to follow-up (follow-up rate: 86.3%). We also excluded participants with other prostate diseases (n=2682) and those with cardiovascular disease (CVD) (n=2875), cancer (n=1618), or did not undergo neutrophil and lymphocyte counts (n=1583), had BPH or a prior history of treatment for BPH (n=5869) at baseline. The final study sample included 15,783 people after these exclusions. Figure 1 displays a flowchart of the participant selection process.
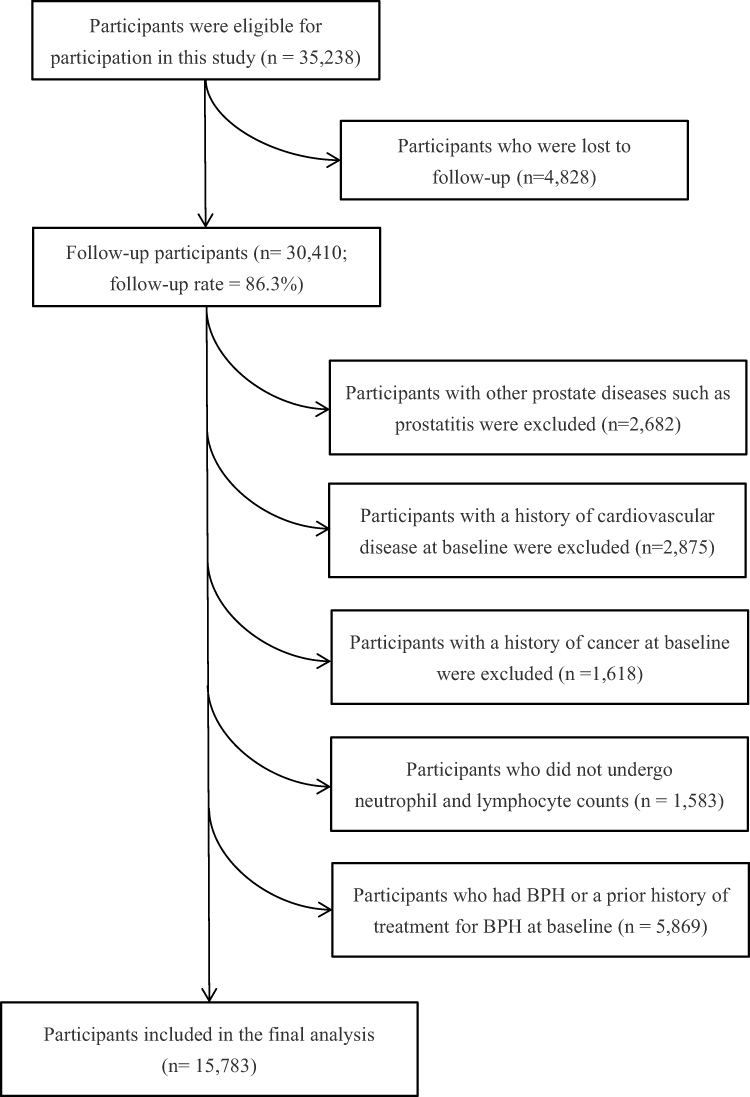 |
Figure 1 Flow diagram of study participant selection. Abbreviation: BPH, benign prostatic hyperplasia. Note: BPH was defined as TPV ≥ 30 mL. |
Definition of Newly Diagnosed BPH
Previous studies have investigated the relative adequacy of transabdominal and transrectal ultrasonography for prostatic measurements, replacing gold-standard transrectal studies with cheaper, easier, and less invasive transabdominal studies in large-scale population screening.15 At both baseline and subsequent follow-up examinations, prostate disease was tested using transabdominal ultrasonography.16 BPH was defined as total prostate volume (TPV) ≥ 30 mL16 according to a previous study. TPV was determined by transabdominal ultrasonography (7–12 MHz, Royal Philips) and calculated as elliptical volume (height× width× length× π/6).17 Using trained professional staff, transabdominal ultrasonography with TPV measurements was performed. A first-time BPH developed as a result of the follow-up period.
Assessment of NLR
Using venipuncture at the elbow, fasting blood samples were taken from each participant in the morning. An automated hematology analyzer was used to measure the leukocyte, neutrophil, and lymphocyte counts, which were expressed as 1000 cells/mm3. The NLR was calculated as the ratio of the neutrophil count to the lymphocyte count. To investigate how the NLR levels are associated with the prevalence of BPH, we divided them into quartiles and continuous variables.
Assessment of Other Variables
Height (m) and weight (kg) were measured using calibrated equipment for anthropometric measurements. Weight/height2 (kg/m2) was used to calculate the body mass index (BMI). Waist circumference was measured according to a standardized protocol (to the closest 0.1 cm).
Fasting blood glucose (FBG), triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), alanine aminotransferase (ALT), and high-sensitivity C-reactive protein (hsCRP) were all measured in fasting blood samples. An FBG level of ≥7.0 mmol/L or a self-reported history of diabetes mellitus were considered indicators of diabetes mellitus.18 TC ≥ 5.17 mmol/Lor TG ≥ 1.7 mmol/L or LDL-C ≥3.37 mmol/L, or the usage of antilipemic medications have been defined as hyperlipidemia.19 Blood pressure (BP) was measured at least twice by trained nurses using automatic BP monitors (A&D Company, Ltd., Tokyo, Japan).20 Prior to taking BP measurements, participants rested for at least 5 min in a calm area, and measurements were then taken in the upper right arm.21 The measurements were separated by at least 1 min. Systolic BP of ≥140 mmHg and/or diastolic BP of ≥90 mmHgor a history of hypertension were both considered to be indicators of hypertension.22
Social and demographic variables were also assessed, including age, smoking and drinking status, educational level, occupation, monthly household income, and individual and family history of disease were obtained from a health status questionnaire. A simplified version of the International Physical Activity Questionnaire (IPAQ), which records the amount of time spent engaging in vigorous-intensity activities, moderate-intensity activities, walking, and sitting during the past 7 days, was used to measure physical activity (PA).23 Total PA was estimated using the formula metabolic equivalent hours per week [Metabolic equivalent (MET)× hours/week].23 To determine the usual dietary intake, a 100 food items validated extended self-administered food frequency questionnaire (FFQ) was employed. Data from the FFQ and the Chinese food composition table were combined to determine each participant’s average daily energy intake.24
Statistical Analysis
The presence of normal distributions for continuous variables is checked using the Kolmogorov–Smirnov test. The clinical characteristics and blood tests taken at baseline on the participants are listed. Descriptive data are presented as the geometric mean (95% confidence intervals, CI) for continuous variables and as a percentage for categorical variables. The person-time of follow-up time for each participant was calculated from the completion of the initial survey to the last time of follow-up, the date of incident BPH occurred, or loss to follow-up, whichever came first.
To determine if NLR levels were associated with the risk of BPH, we used the proportional hazards Cox model. A significant level of interaction terms between quartile categories of NLR and follow-up time was examined to evaluate the proportional hazard assumption. Three progressively multivariable Cox regression models were fitted. In model 1, crude hazard ratios (HRs) with their corresponding 95% confidence intervals (CIs) were calculated. In model 2, the participants adjusted for age and BMI. Model 3, additionally adjusted for smoking status, alcohol drinking status, educational level, occupation, household income, PA, total energy intake, hypertension, hyperlipidemia, family history of the disease (including CVD, hypertension, and diabetes mellitus), and inflammatory markers (hsCRP and ALT). Adjustment for inflammatory markers was performed to assess the effect of inflammation on the associations with the prevalence of BPH. By modeling these quartiles as ordinal variables, tests of linear trends within categories of NLR quartiles were assessed.
All statistical tests were two-tailed, with a P value < 0.05 being statistically significant. The SAS version 9.4 (SAS Institute, Inc., Cary, NC) was used for all analyses.
Results
Characteristics of Study Subjects
The study’s participants had an average age of 44.1 ±10.3 years. Table 1 shows the basic characteristics associated with incident BPH. Males with BPH had a higher average age than men without BPH (P< 0.0001). Participants with BPH tended to have a lower level of ALT, “Animal foods” dietary pattern score, education (P< 0.0001), and household income (P= 0.01), but had a higher level of BMI, waist, TC, TG, LDL, FBG, SBP, DBP, and “Sweets” dietary pattern score (P< 0.0001). They tend to have a history of hypertension and hyperlipidemia and a family history of CVD, hypertension, and diabetes mellitus (P< 0.0001). Men with BPH had a spread between smoking, drinking, and employment status. Otherwise, no significant differences were observed between groups.
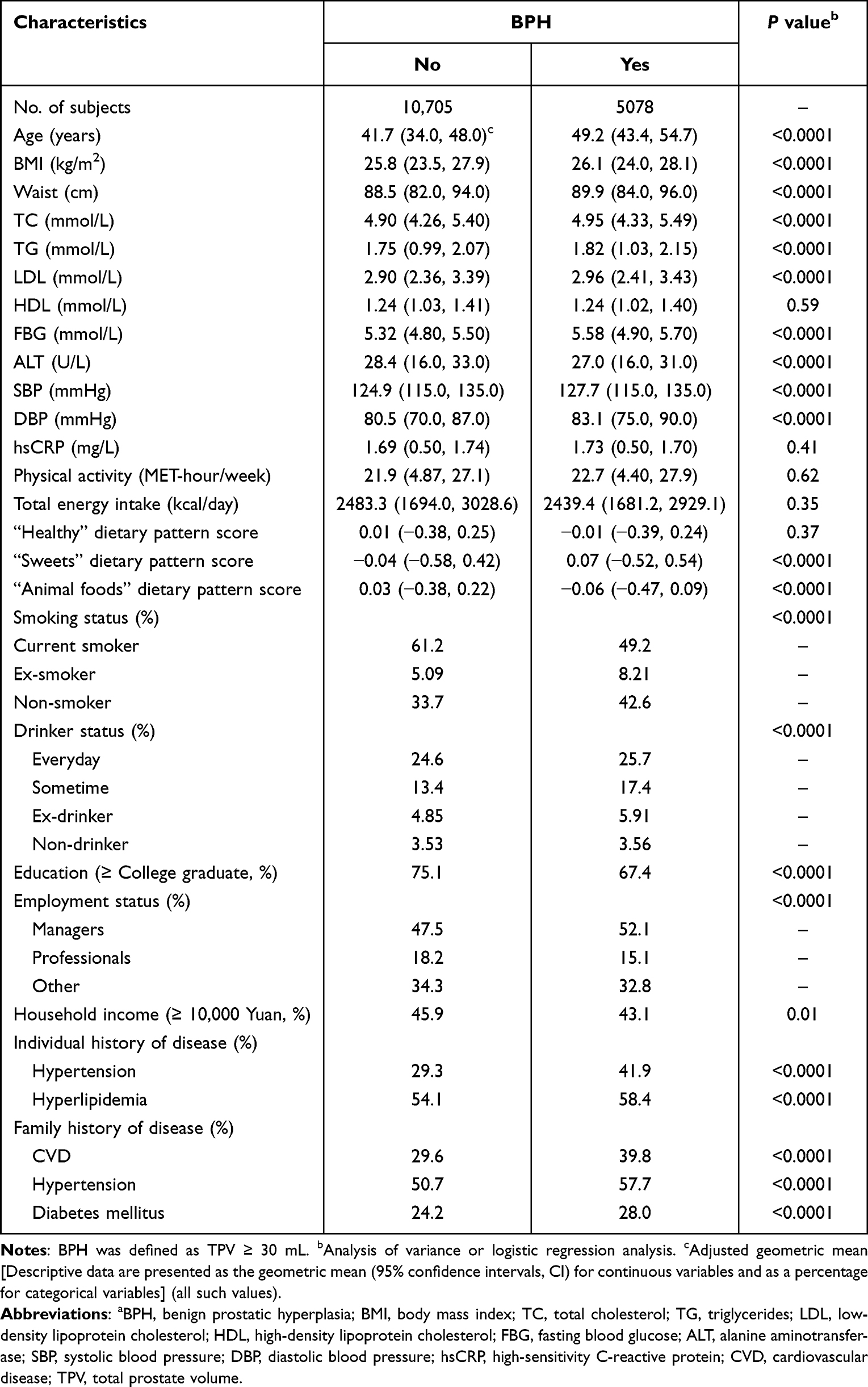 |
Table 1 Participant Baseline Characteristics by BPH Status (n = 15, 783)a |
Association Between NLR Levels and Risk of BPH
During a median follow-up of 2.7 years and 42,517 person-years, we documented a total of 5078 participants with incident BPH. The association between NLR levels and the prevalence of BPH is shown in Table 2. NLR levels were positively associated with the presence of BPH in all models. Following final multiple adjustments, the HRs of BPH were 1.00 (reference), 1.08 (95% CIs 0.99, 1.17), 1.10 (95% CIs1.02, 1.19), and 1.12 (95% CIs1.03, 1.21), respectively, for participants with NLR in the first, second, third, and fourth quartiles (P for trend < 0.01). The data for participant cohort for each NLR quartile are shown in Table 3.
 |
Table 2 Adjusted Relationships of NLR to BPH (n = 15,783) |
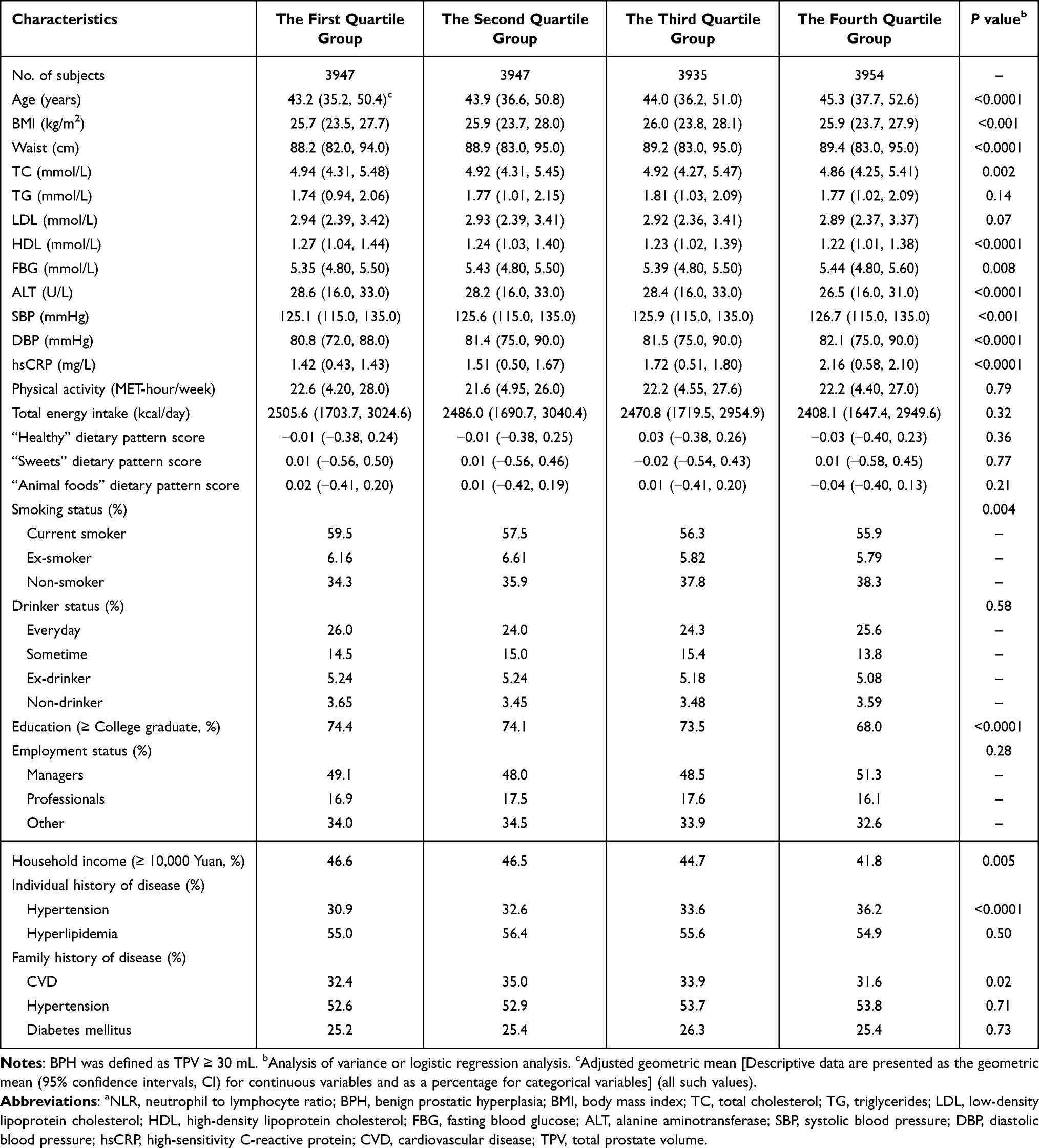 |
Table 3 Participant Baseline Characteristics for Each NLR Quartile (n = 15, 783)a |
In addition, we performed a sensitivity analysis excluding participants with diabetes (n=1030) in the final model. The results are similar to our previous analysis (data not shown).
Discussion
In this large prospective cohort study of adult males in China, we found that higher NLR levels were associated with a higher risk of BPH after adjustment for a wide range of potential confounding variables. We believe that this is the first large-scale population-based study on NLR levels and the risk of BPH to be carried out in Asia.
From the biological view, it is well-known that NLR is a recognized surrogate marker for inflammatory states in the body and can easily be determined from a peripheral blood sample using a complete blood count.25 In the general population, scarce data are available on the association between NLR levels and on the risk of BPH. Kang et al conducted a case–control study using normal controls, with 538 men in the control group and 269 men in the case group, and showed that the prevalence of BPH was substantially correlated with increased NLR levels.26 Similarly, Ozer et al found that NLR was positively associated with severe International Prostate Symptom Score (IPSS), TPV, prostate-specific antigen (PSA), and Maximum urinary flow rate (Qmax) values.3 Furthermore, Chung et al investigated the association between NLR and IPP in male BPH, and their findings demonstrated that NLR might be used as a surrogate marker for IPP with certain morphological abnormalities.12 In our cohort study with 15,783 participants, a positive association between NLR levels and the risk of BPH was observed. Reasons for the discrepancy between these findings remain unclear, which may partly be due to the small sample size, cross-sectional design, particular patient population, and incomplete control of confounding factors.
Epithelial and stromal cell proliferation in the periurethral and transition zone is a symptom of BPH.27 In the past few decades, it has been clear how androgens, growth factors, and inflammation all play a role in the occurrence and progression of BPH.6 BPH is an immune-mediated inflammatory illness characterized by a persistent prostatic inflammatory state (PIS).28 Inflammation was found in 43% of the 3942 surgically generated BPH specimens, 69% of which were chronic inflammation.29 Histological inflammation is commonly found in BPH specimens, and it affects the biological characteristics of BPH, such as patient symptoms, prostate volume, and PSA levels.30 Several studies have shown how immune cell infiltration and pro-inflammatory mediators contribute to the pathophysiology of BPH.31
Important serum indicators for illness diagnosis, prognosis, and treatment evaluation include inflammatory cytokines.8 The most prevalent types of leukocytes, neutrophils, are crucial for starting and controlling innate and adaptive immunity. Another critical component of circulating leukocytes that facilitates adaptive immune response and collaborates closely with innate immunity are lymphocytes. As a measure of systemic inflammation for the current analysis, we used NLR, a ratio that depicts the interaction between two distinct immune pathways. NLR has dramatically associated with prostate tissue inflammation in a recent study with 183 patients who underwent transurethral resection of the prostate.30 Considering the association between NLR and prostatic inflammation and the potential for prostatic inflammation to contribute to the development of BPH, it is plausible to believe that the presence of BPH and NLR is significantly correlated.26 During the study, we also found that participants with BPH tended to have a lower level of ALT. This result is in accordance with a recent study that demonstrates association between development of nonalcoholic fatty liver disease, a metabolic aberration-associated disease, and prostate volume.32,33 In this study, there was no significant difference between the CRP in the groups. The outcome is identical to the previous one, when men with elevated CRP levels were not more likely to experience rapid in creases in prostate volume, obstructive LUTS, or PSA level.34
In comparison to earlier studies, the current study has several significant advantages. Unlike research done in particular clinical populations, the participants in this analysis were selected from a large sample size and are hence more generalizable. In addition, the association between NLR levels and the risk of BPH was also adjusted for a number of potential confounding variables. However, when adjusting for these potential confounders, the results were still statistically significant, indicating that increased NLR levels are independently associated with a higher risk of BPH. It goes without saying that the current study has several limitations. First, in participants with elevated NLR levels, we were unable to explore the pathophysiology of the progression of BPH. BPH is not exclusively caused by inflammation, and several additional causes are probably involved in this morphological alteration. In order to ascertain if the progression of BPH varies with NLR over time in men who first present with BPH, more study on this topic is required. Nevertheless, we believe the current study offers substantial initial information on the association between NLR levels and the risk of BPH. Second, there are still many unidentified variable factors that could affect the association between NLR levels and the risk of BPH, even after we have adjusted for some potentially confounding variables. Finally, the age range in our study is broad (18–90 years). As a result, the relatively brief follow-up period (median: 2.7 years) and youthful participant population may underestimate the association between NLR and the risk of BPH. Although the follow-up period was brief, the sample size of the study was sufficient to increase the statistical validity of our conclusions. To support our findings, additional long-term studies are needed.
Conclusion
In summary, our study demonstrates that, even after adjusting for potential confounding variables, there is a positive association between NLR levels and the risk of BPH in Chinese adult male population. This study highlights the significant association between NLR levels and the risk of BPH, supporting the possibility that NLR levels can be used to predict the risk of BPH. These results back up the notion that inflammation and BPH are related. BPH does not pose a life-threatening hazard, but its symptoms might impair a patient’s quality of life. Further experimental and long-term studies are needed to clarify the biological mechanisms of BPH and ascertain whether the elevated level of NLR is a result of BPH.
Abbreviations
NLR, neutrophil-to-lymphocyte ratio; BPH, benign prostatic hyperplasia; PCa, prostate cancer; LUTS, lower urinary tract symptoms; CBCs, complete blood counts; IPP, intravesical prostatic protrusion; BMI, body mass index; TCLSIH, Tianjin Chronic Low-Grade Systemic Inflammation and Health; CVD, cardiovascular disease; TPV, total prostate volume; Qmax, Maximum urinary flow rate; IPSS, International Prostate Symptom Sore; FBG, fasting blood glucose; TG, triglycerides; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; hsCRP, high-sensitivity C-reactive protein; ALT, alanine aminotransferase; BP, blood pressure; PA, Physical activity; IPAQ, International Physical Activity Questionnaire; MET, Metabolic equivalent; FFQ, food frequency questionnaire; HRs, crude hazard ratios; CIs, confidence intervals; PSA, prostate-specific antigen; PIS, prostatic inflammatory status.
Data Sharing Statement
The raw/processed data required to reproduce these findings cannot be shared at this time as the data also form part of an ongoing study.
Ethics Approval and Informed Consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors. Informed consent was obtained from all individual participants included in the study.
Acknowledgments
The authors thank Health Management Centre of Tianjin Medical University General Hospital for their strong support and help in the field investigation. The authors appreciate the cooperation and participation of teachers, nurses, students, and participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the Study of Diet and Nutrition Assessment and Intervention Technology (No. 2020YFC2006300) from Active Health and Aging Technologic Solutions Major Project of National Key R&D Program—Study on Intervention Strategies of Main Nutrition Problems in China (No. 2020YFC2006305), National Natural Science Foundation of China (Nos. 81941024, 81872611, 82103837, and 81903315), Tianjin Major Public Health Science and Technology Project (No. 21ZXGWSY00090), National Health Commission of China (No. SPSYYC 2020015), Food Science and Technology Foundation of Chinese Institute of Food Science and Technology (No. 2019-12), 2014 and 2016 Chinese Nutrition Society (CNS) Nutrition Research Foundation—DSM Research Fund (Nos. 2016-046, 2014-071, and 2016-023), China.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ferlay J, Colombet M, Soerjomataram I, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries and 25 major cancers in 2018. Eur J Cancer. 2018;103:356–387. doi:10.1016/j.ejca.2018.07.005
2. Ilic D, Misso M. Lycopene for the prevention and treatment of benign prostatic hyperplasia and prostate cancer: a systematic review. Maturitas. 2012;72(4):269–276. doi:10.1016/j.maturitas.2012.04.014
3. Ozer K, Horsanali MO, Gorgel SN, Horsanali BO, Ozbek E. Association between benign prostatic hyperplasia and neutrophil-lymphocyte ratio, an indicator of inflammation and metabolic syndrome. Urol Int. 2017;98(4):466–471. doi:10.1159/000448289
4. McVary KT, Roehrborn CG, Avins AL, et al. Update on AUA guideline on the management of benign prostatic hyperplasia. J Urol. 2011;185(5):1793–1803. doi:10.1016/j.juro.2011.01.074
5. Chughtai B, Lee R, Te A, Kaplan S. Role of inflammation in benign prostatic hyperplasia. Rev Urol. 2011;13(3):147–150.
6. Zlotta AR, Egawa S, Pushkar D, et al. Prevalence of inflammation and benign prostatic hyperplasia on autopsy in Asian and Caucasian men. Eur Urol. 2014;66(4):619–622. doi:10.1016/j.eururo.2014.06.026
7. Ficarra V, Sekulovic S, Zattoni F, Zazzera M, Novara G. Why and how to evaluate chronic prostatic inflammation. Eur Urol Suppl. 2013;12(5):110–115. doi:10.1016/j.eursup.2013.08.002
8. Imtiaz F, Shafique K, Mirza SS, Ayoob Z, Vart P, Rao S. Neutrophil lymphocyte ratio as a measure of systemic inflammation in prevalent chronic diseases in Asian population. Int Arch Med. 2012;5(1):2. doi:10.1186/1755-7682-5-2
9. Lee KS, Ha JS, Koo KC. Significance of neutrophil-to-lymphocyte ratio as a novel indicator of spontaneous ureter stone passage. Yonsei Med J. 2017;58(5):988–993. doi:10.3349/ymj.2017.58.5.988
10. Tanik S, Albayrak S, Zengin K, et al. Is the neutrophil-lymphocyte ratio an indicator of progression in patients with benign prostatic hyperplasia? Asian Pac J Cancer Prev. 2014;15(15):6375–6379.
11. Jang WS, Cho KS, Kim MS, et al. The prognostic significance of postoperative neutrophil-to-lymphocyte ratio after radical prostatectomy for localized prostate cancer. Oncotarget. 2017;8(7):11778–11787. doi:10.18632/oncotarget.14349
12. Chung MS, Yang YJ, Lee SH, Yoon BI. Association between the neutrophil-to-lymphocyte ratio and intravesical prostatic protrusion in men with benign prostatic hyperplasia. Low Urin Tract Symptoms. 2020;12(1):62–67. doi:10.1111/luts.12287
13. Yu B, He H, Zhang Q, et al. Soft drink consumption is associated with depressive symptoms among adults in China. J Affect Disord. 2015;172:422–427. doi:10.1016/j.jad.2014.10.026
14. Song K, Du H, Zhang Q, et al. Serum immunoglobulin M concentration is positively related to metabolic syndrome in an adult population: Tianjin Chronic Low-Grade Systemic Inflammation and Health (TCLSIH) Cohort Study. PLoS One. 2014;9(2):e88701. doi:10.1371/journal.pone.0088701
15. Blanc M, Sacrini A, Avogadro A, et al. Prostatic volume: suprapubic versus transrectal ultrasonography in the control of benign prostatic hyperplasia. Radiol Med. 1998;95(3):182–187.
16. Huh JS, Kim YJ, Kim SD. Prevalence of Benign Prostatic Hyperplasia on Jeju Island: analysis from a Cross-sectional Community-based Survey. World J Mens Health. 2012;30(2):131–137. doi:10.5534/wjmh.2012.30.2.131
17. Zhao SC, Xia M, Tang JC, Yan Y. Associations between metabolic syndrome and clinical benign prostatic hyperplasia in a northern urban Han Chinese population: a prospective cohort study. Sci Rep. 2016;6:33933. doi:10.1038/srep33933
18. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
19. Expert Panel on Detection E, Treatment of High Blood Cholesterol in A. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA. 2001;285(19):2486–2497. doi:10.1001/jama.285.19.2486
20. Kobalava ZD, Kotovskaya YV, Babaeva LA, Moiseev VS. Validation of TM-2655 oscillometric device for blood pressure measurement. Blood Press Monit. 2006;11(2):87–90. doi:10.1097/01.mbp.0000200484.49540.12
21. Mancia G, De Backer G, Dominiczak A, et al. 2007 guidelines for the management of arterial hypertension: the task force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2007;25(6):1105–1187. doi:10.1097/HJH.0b013e3281fc975a
22. Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA. 2003;289(19):2560–2572. doi:10.1001/jama.289.19.2560
23. Craig CL, Marshall AL, Sjostrom M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–1395. doi:10.1249/01.MSS.0000078924.61453.FB
24. Yang Y, Wang G, Pan X. China Food Composition. Beijing: Peking University Medical Press; 2002.
25. Guthrie GJ, Charles KA, Roxburgh CS, Horgan PG, McMillan DC, Clarke SJ. The systemic inflammation-based neutrophil-lymphocyte ratio: experience in patients with cancer. Crit Rev Oncol Hematol. 2013;88(1):218–230. doi:10.1016/j.critrevonc.2013.03.010
26. Kang JY, Choi JD, Cho JM, Yoo TK, Park YW, Lee JH. Association of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and lymphocyte-to-monocyte ratio with benign prostatic hyperplasia: a propensity score-matched analysis. Urol Int. 2021;105(9–10):811–816. doi:10.1159/000512894
27. Roehrborn CG. BPH progression: concept and key learning from MTOPS, ALTESS, COMBAT, and ALF-ONE. BJU Int. 2008;101(Suppl 3):17–21. doi:10.1111/j.1464-410X.2008.07497.x
28. De Nunzio C, Salonia A, Gacci M, Ficarra V. Inflammation is a target of medical treatment for lower urinary tract symptoms associated with benign prostatic hyperplasia. World J Urol. 2020;38(11):2771–2779. doi:10.1007/s00345-020-03106-1
29. Di Silverio F, Gentile V, De Matteis A. Distribution of inflammation, pre-malignant lesions, incidental carcinoma in histologically confirmed benign prostatic hyperplasia: a retrospective analysis. Eur Urol. 2003;43(2):164–175. doi:10.1016/S0302-2838(02)00548-1
30. Zhang Q, Pang S, Zhang Y, Jiang K, Guo X. Association between inflammation and lower urinary tract symptoms of benign prostatic hyperplasia. Urol J. 2020;17(5):505–511. doi:10.22037/uj.v0i0.5462
31. Melissa M, Norström ER, Sundberg B, et al. Progression of benign prostatic hyperplasia is associated with pro-inflammatory mediators and chronic activation of prostate-infiltrating lymphocytes. Oncotarget. 2016;7(17):23581–23593. doi:10.18632/oncotarget.8051
32. Nagakura Y, Hayashi M, Kajioka S. Lifestyle habits to prevent the development of benign prostatic hyperplasia: analysis of Japanese nationwide datasets. Prostate Int. 2022;10(4):200–206. doi:10.1016/j.prnil.2022.06.004
33. Chung GE, Yim JY, Kim D, et al. Nonalcoholic fatty liver disease is associated with benign prostate hyperplasia. J Korean Med Sci. 2020;35(22):e164. doi:10.3346/jkms.2020.35.e164
34. St Sauver JL, Sarma AV, Jacobson DJ, et al. Associations between C-reactive protein and benign prostatic hyperplasia/lower urinary tract symptom outcomes in a population-based cohort. Am J Epidemiol. 2009;169(11):1281–1290. doi:10.1093/aje/kwp085
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Eriochloa villosa Alleviates Progression of Benign Prostatic Hyperplasia in vitro and in vivo
Baek EB, Hwang YH, Park S, Hong EJ, Won YS, Kwun HJ
Research and Reports in Urology 2022, 14:313-326
Published Date: 24 September 2022
Association Between Mean Platelet Volume and Benign Prostatic Hyperplasia: A Population Study from the TCLSIH Cohort Study
Song Y, Gu Y, Guo H, Yang H, Wang X, Wu H, Wang A, Wang M, Wang H, Zhang Q, Liu L, Meng G, Liu B, Niu K
Journal of Inflammation Research 2023, 16:3259-3269
Published Date: 5 August 2023
Discordance Between Neutrophil to Lymphocyte Ratio and High Sensitivity C-Reactive Protein to Predict Clinical Events in Patients with Stable Coronary Artery Disease: A Large-Scale Cohort Study
He J, Song C, Zhang R, Yuan S, Li J, Dou K
Journal of Inflammation Research 2023, 16:5439-5450
Published Date: 20 November 2023