Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Association Between Migraine and Gastrointestinal Disease in Pediatric Patients: A Propensity Score Weighting Approach
Authors Rhew K ![]()
Received 24 October 2023
Accepted for publication 23 November 2023
Published 28 November 2023 Volume 2023:19 Pages 2607—2615
DOI https://doi.org/10.2147/NDT.S442635
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Richard J Porter
Kiyon Rhew
College of Pharmacy, Dongduk Women’s University, Seoul, Republic of Korea
Correspondence: Kiyon Rhew, College of Pharmacy, Dongduk Women’s University, 60 Hwarang-ro 13-gil, Seongbuk-gu, Seoul, 02748, Republic of Korea, Tel +82-2-940-4519, Fax +82-2-940-4159, Email [email protected]
Purpose: Migraine is a neurological disorder affecting pediatric patients of all age groups, with a prevalence ranging from approximately 5% to 15%. It significantly impacts the quality of life in children and adolescents, potentially hampering their learning abilities, school performance, and daily activities. This study investigated the association between migraine and several prevalent gastrointestinal (GI) diseases in pediatric patients.
Patients and Methods: We analyzed the Health Insurance Review and Assessment Service Pediatric Patient Sample (HIRA-PPS) dataset from South Korea. Propensity scores based on patient characteristics (age, sex, and insurance type) were employed through the inverse probability of treatment weighting (IPTW) in binary logistic regression. We included gastroesophageal disease (GERD), peptic ulcer disease (PUD), gastritis, dyspepsia, irritable bowel syndrome (IBS), and inflammatory bowel disease (IBD) as GI diseases.
Results: A total of 683,347 patients from the HIRA dataset were included in the study. After IPTW adjustment, the prevalence of GI diseases among pediatric patients with migraine remained significantly increased (OR 4.15; 95% CI 4.12– 4.18). Migraine patients showed higher prevalence rates for all six individual GI diseases, with GERD (OR 4.11; 95% CI 4.05– 4.16) and IBS (OR 3.79; 95% CI 3.74– 3.84) showing the highest associations. We also confirmed a progressively increasing association between the presence of diagnosed migraine and GI diseases.
Conclusion: This study highlights a strong association between pediatric migraine and GI diseases, even after adjusting for patient characteristics. The elevated prevalence of various GI diseases in migraine patients suggests the need for comprehensive approaches to their prevention and treatment.
Keywords: migraine, gastrointestinal disease, pediatric, GERD, IBS
Introduction
Migraine is a neurological disorder that can occur in pediatric patients of all age groups, including infancy, with a prevalence ranging from approximately 5% to 15%.1–3 Migraine can negatively impact the quality of life in children and adolescents, affecting their school and daily activities and potentially reducing their learning abilities.4,5 Esposito’s study reported a high prevalence of harm avoidance and persistence of temperamental domains in pediatric patients with migraine, suggesting a correlation between temperamental domains and migraine.6
Several studies have indicated a higher prevalence of sleep-related problems, depressive mood, anxiety disorders, and attention-deficit hyperactivity disorder (ADHD) in pediatric patients with migraine.7–9 Some studies have also linked childhood and adolescent migraine to parental stress.10,11 Additionally, migraine has been suggested as a risk factor for respiratory conditions like asthma and associated with low income or education levels, increasing the risk of other disorders or symptoms.12,13
Recent studies have presented findings on the association between migraine and several gastrointestinal (GI) conditions. In patients with migraine, H. Pylori infection rates were approximately twice as high, and particularly in Asians, it appeared to be even higher, around 3.5 times.14 The prevalence of irritable bowel syndrome (IBS) in migraine patients was about 2.7 times higher than in those without migraine.15 Furthermore, GI diseases such as dyspepsia, gastroesophageal reflux (GERD), and inflammatory bowel disease (IBD) also showed higher prevalence in migraine patients.16–18
Pediatric migraine patients have been suggested to exhibit correlations with GI diseases distinct from those observed in adults. For instance, infantile colic, affecting approximately 20% of infants, has been reported to be influenced by parental migraine history, infantile GI diseases, and migraine symptoms.19 Abdominal migraine, categorized as a functional abdominal pain disorder, impacts 0.2% to 4.1% of children and is characterized by intermittent, repetitive, and sudden episodes of abdominal pain.20 Accompanied by symptoms such as paleness, nausea, vomiting, loss of appetite, headache, and sensitivity to light, approximately 70% of pediatric patients with abdominal migraine were found to experience migraine symptoms during long-term tracking and observation.21 These studies underscore the correlation between distinctive migraine characteristics in children and adolescents and GI diseases. The International Headache Society formally recognizes specific codes 1.6.1 (recurrent gastrointestinal disorder) and 1.6.1.2 (abdominal migraine) within the International Classification of Headache Disorders, Third Edition (ICHD-3, 2018) as having equivalence to or association with hemicrania.22
However, this study diverges from focusing on migraine and GI symptoms in patients diagnosed with abdominal migraine; instead, it aims to assess the prevalence of several GI diseases in pediatric patients with migraine. Previous studies have also presented associations between migraine and GI disorders in adults.14–18 Nevertheless, comprehensive studies analyzing the overall prevalence and associations between migraine and GI disorders in pediatric patients are yet to be conducted. Therefore, this study aims to establish the association between migraine and several high-prevalence GI diseases in pediatrics. The results of this study could have valuable implications for approaches to treating and preventing both migraine and GI diseases.
Materials and Methods
Study Subjects
In this study, we conducted an analysis using the Health Insurance Review and Assessment Service Pediatric Patient Sample (HIRA-PPS) dataset from South Korea. This dataset was carefully selected by considering age and gender and contains information from medical facilities and pharmacies where patients sought healthcare services over one year.23 It is important to note that the HIRA dataset was provided after removing personally identifiable patient information in compliance with South Korea’s personal information protection regulations. This dataset was deemed appropriate for representing the characteristics of patients in South Korea.24
For this study, all pediatric patients were included in the dataset. However, patients diagnosed with GI diseases only once a year and those diagnosed with headaches other than migraine were excluded from the study. Patients diagnosed with cardiovascular, cerebrovascular, neurological, or psychiatric disorders that could potentially increase the risk of migraine were also excluded (Table 1).25–28
 |
Table 1 The List of ICD-10 Diagnostic Codes of Diseases in the Study |
Definition of Diseases
The ICD-10 codes for GI diseases and migraine included in this study are as follows: GERD [K21, ri K22], peptic ulcer disease (PUD) [K25, K26, K27, K28], gastritis [K29], dyspepsia [K30], IBS [K58], IBD [K50, K51], and migraine [G43]. Abdominal migraine corresponds to the ICD-10 code G43.D. However, this study utilized claims data for analysis, and most of these data report diagnoses using three-digit codes. As a result, the analysis was conducted on all patients diagnosed with migraine, regardless of abdominal migraine. A specific criterion was applied to ensure the clarity of patient diagnoses: a patient was defined as having a particular disorder if they received a diagnosis for that disorder on two or more occasions within a year. We classified pediatric patients diagnosed with one or more of the six conditions mentioned above on two or more occasions within a year as the group with GI disease.
Statistical Analysis
We conducted binary logistic regression utilizing inverse probability of treatment weighting (IPTW) based on propensity scores. The propensity score was computed through a multivariable logistic regression model, taking into account patient characteristics such as age, sex, and insurance type as social status to assess the probability for each patient. We reported odds ratio (OR) and their 95% confidence intervals (CI) to characterize the association between migraine and GI diseases. All statistical analyses were conducted utilizing SAS 9.4 (SAS Institute Inc., Cary, NC, USA). This study received approval from the Institutional Review Board of Dongduk Women’s University (IRB No. DDWU2304-03).
Results
Patient Characteristics
In the HIRA-PPS-2018 dataset, a total of 949,354 patients were included. Among them, 85,806 patients with conditions increasing the risk of migraine and 180,201 patients with a one-time diagnosis of GI diseases were excluded, resulting in a total of 683,347 patients included in the study (Figure 1). Pediatric migraine patients numbered 1984, with 1431 (72.13%) being adolescents aged 12 or older, and 1119 (56.40%) being female. Subsequently, IPTW was applied to match the age group, sex, and insurance type between the migraine-diagnosed and non-migraine groups (Table 2). After the IPTW adjustment, the migraine patient group comprised 695,584 individuals, while the non-migraine group comprised 683,347 individuals.
 |
Table 2 Patient Characteristics Before and After Weighting by Propensity Score |
 |
Figure 1 Flow diagram for study subject inclusion. Abbreviation: GI, Gastrointestinal. |
Association Between Migraine and GI Diseases After Weighting with Propensity Score
Following the adjustment of patient characteristics using propensity scores, the analysis of the association between migraine and GI diseases yielded an OR of 4.15 (95% CI, 4.12–4.18; p<0.001) for the prevalence of GI diseases among migraine patients (Table 3). Upon analyzing the correlation between migraine and individual GI diseases, migraine patients exhibited a higher prevalence of all six GI diseases compared to pediatric individuals without a migraine diagnosis. The association between migraine and individual GI diseases showed the highest OR for GERD at 4.11 (95% CI, 4.05–4.16; p<0.001), followed by IBS with an OR of 3.79 (95% CI, 3.74–3.84; p<0.001). Furthermore, elevated prevalence rates among migraine patients were also observed for gastritis, IBD, PUD, and dyspepsia in descending order for other conditions (Table 3).
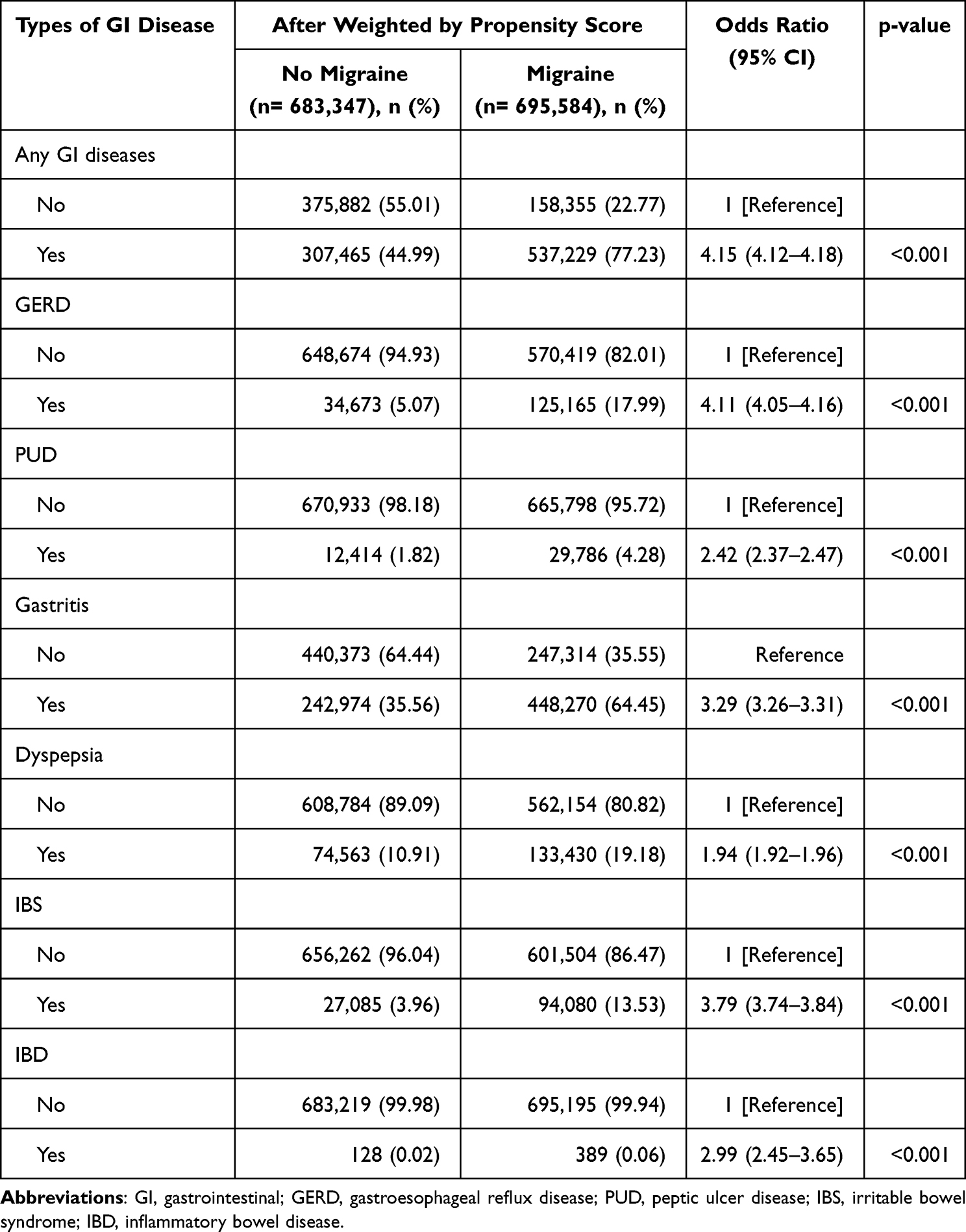 |
Table 3 Association between Gastrointestinal Disease and Migraine After Weighting by Propensity Score |
This study also analyzed the association between migraine and the number of diagnosed GI diseases. We confirmed a progressively increasing association between the presence of diagnosed GI diseases and pediatric migraine patients when compared to those without migraine. The OR for having at least one GI diseases diagnosis was 3.10 (95% CI, 3.07–3.12; p<0.001). However, for two, three, four, and five or more diagnosed GI diseases, the OR values increased to 7.34 (95% CI, 7.26–7.42; p<0.001), 8.89 (95% CI, 8.70–9.09; p<0.001), 13.06 (95% CI, 12.44–13.71; p<0.001), and 21.70 (95% CI, 18.68–25.21; p<0.001), respectively (Table 4).
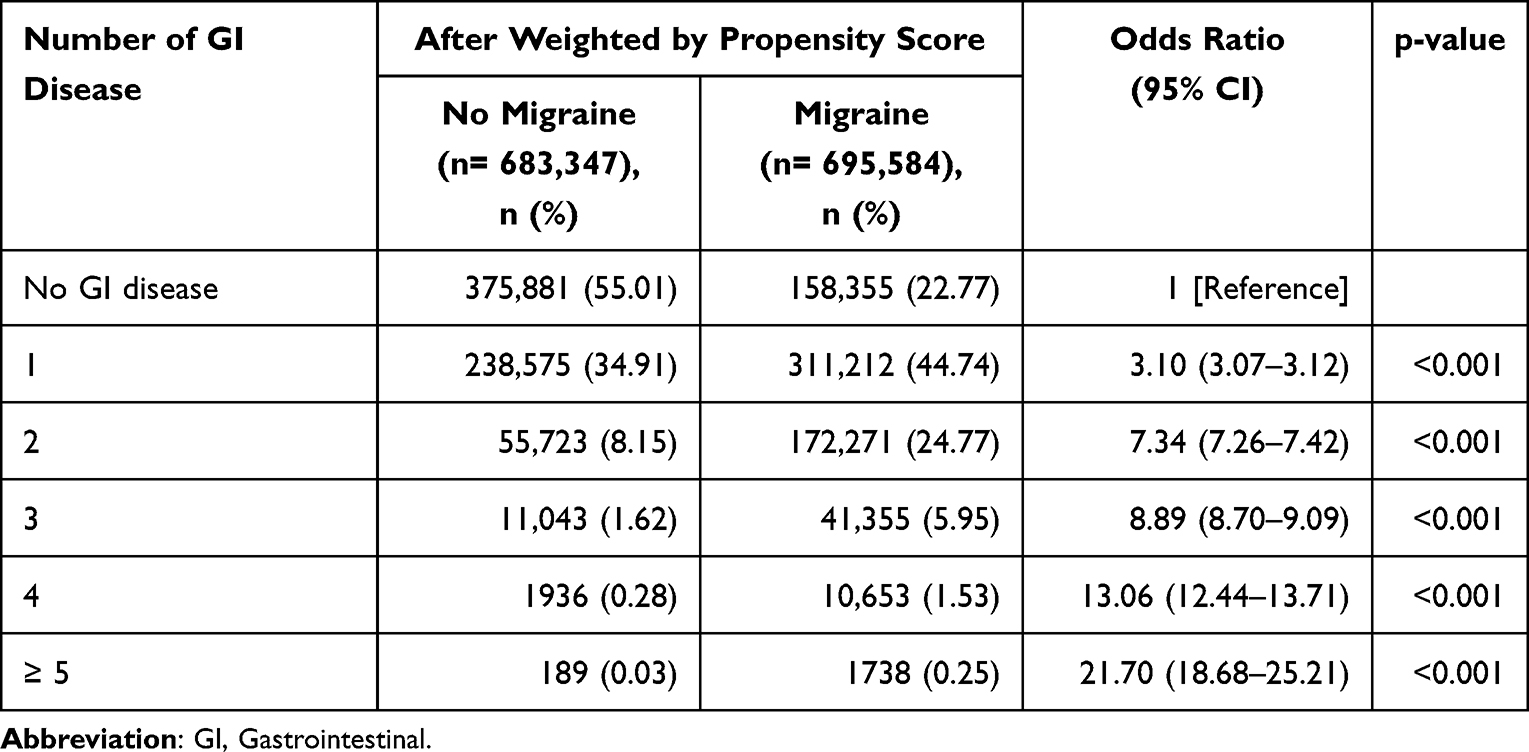 |
Table 4 Odds Ratio of Migraine According to the Number of Gastrointestinal Disease After Weighting by Propensity Score |
Discussion
After adjusting for patient age, gender, and economic status (as represented by the types of health insurance), the prevalence of GI diseases in pediatric patients with migraine was approximately 4.15 times higher. Additionally, the prevalence of all six individual GI diseases in migraine patients was higher compared to those without a migraine diagnosis, and it was observed that the association with migraine increased significantly with the number of diagnosed GI diseases. All of these findings indicate a clear association between migraine and GI diseases.
Several studies conducted on adult patients have reported research findings regarding the correlation between migraine and GI diseases.12,14–16,29 According to the results of a meta-analysis, H. pylori infection appeared to be approximately 1.4 times more prevalent in migraine patients compared to the control group.14 Although this study did not assess the correlation with H. pylori infection, the analysis revealed that migraine patients exhibited an approximately 2.4-fold higher prevalence of PUD, for which H. pylori infection is considered a primary risk factor. The prevalence of IBS in migraine patients was also approximately 3.8 times higher, consistent with similar findings in studies reporting a two to three-fold higher prevalence.30,31 This study, conducted with pediatric patients, showed a stronger association between migraine and GI diseases compared to studies involving adults. Given the elevated occurrence of abdominal migraine in children, gastrointestinal symptoms (eg, nausea, vomiting, or loss of appetite) may frequently coexist with migraine in pediatric patients. However, in this study, we analyzed diagnoses of GI disorders such as GERD, PUD, gastritis, dyspepsia, IBS, and IBD. Therefore, it is considered that such biases were minimized. This more heightened correlation may be attributed to the increased evidence in children, as inflammatory conditions caused by chronic diseases or aging appear less frequently in this population.32,33
Previous studies have proposed several hypotheses concerning the association between these two conditions.34–36 The term “gut-brain axis” explains the close interconnection and mutual influence between the GI tract and the central nervous system (CNS). One of the mechanisms behind this relationship involves the role of gut microbiota and inflammation in migraine. Inflammatory cells and inflammatory mediators can induce visceral pain, and proinflammatory cytokines such as IL-1β, IL-6, IL-8, and TNF-α have been implicated in migraine.37,38 This hypothesis aligns with recent research findings demonstrating no genetic correlation between migraine and IBD.39 The second mechanism in migraine involves the action of neuropeptides such as glutamate, CGRP (calcitonin gene-related peptide), or cholecystokinin. These neuropeptides are also known to be involved in neuronal communication in the brain and have been shown to increase concentration during migraine attacks.40,41 Lastly, there may be a connection between the serotonin pathway and migraine.17,42 The tryptophan-kynurenine pathway suggests that gut microbiota, through synthetic enzymes in specific bacterial strains capable of metabolizing tryptophan, may influence CNS function.
There are study findings indicating that the association between the two conditions and the severity of the diseases or their treatment status can influence each other. H. pylori eradication has been shown to relieve symptoms and reduce disability in migraine positively.18,43 Furthermore, a higher frequency of headache pain in migraine patients was associated with a higher prevalence of IBS.44 The exact mechanisms behind the correlation between these two conditions are still unclear. Although the precise correlation mechanism between migraine and GI diseases remains unclear, it can hold significance for diagnosis, prevention, and treatment approaches if they exhibit clinical linkage in patients. Furthermore, if the prevalence of migraine is associated with disease prevalence, severity, or treatment status, novel approaches to the prevention and treatment of gastrointestinal diseases or migraine are warranted. Particularly in pediatric cases of migraine, there are differences in risk factors and related conditions compared to adult patients, and there are medications for migraine that cannot be used in younger individuals.45 Therefore, exploring methods such as probiotics, appropriate dietary intake, and treating GI diseases may be considered beyond pain relief medications, which could be even more important in the pediatric population than in adults.
This study has several limitations. Firstly, while it has presented a correlation between the two conditions, it is challenging to establish precise mechanisms or causality. Additionally, excluding the influence of migraine treatments and their association with GI diseases is impossible. Lastly, the classification of patients with GI diseases or migraine was based on diagnosis codes from claims data, which may lead to differences from actual prevalence rates. Nevertheless, this study, conducted using healthcare claims data in South Korea, can be considered representative of the characteristics of pediatric patients in the country. Even when considering the interaction between medications and diseases, this study provides evidence that the prevalence of other GI diseases not significantly associated with medication for migraine, such as NSAIDs, increases. Additionally, the risk increases clearly as the number of concurrent GI diseases in migraine patients increases.
Conclusion
The association between migraine and GI diseases remains evident even after adjusting for patient characteristics in pediatric and adolescent populations. The prevalence of the six GI diseases (GERD, PUD, gastritis, dyspepsia, IBS, and IBD) also increased in migraine patients. Furthermore, the association between the two conditions becomes even more distinct, with more concurrent GI diseases in migraine patients. Future research may shed light on the precise mechanisms behind the association and causality between these two conditions, potentially offering new perspectives on treating pediatric migraine patients.
Acknowledgments
This work was supported by the National Research Foundation (NRF) of Korea grant funded by the Korean government (MSIT, Ministry of Science and ICT) (No. 2021R1F1A1059897).
Disclosure
The author reports no conflicts of interest in this work.
References
1. GBD 2016 Headache Collaborators. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016 [published correction appears in Lancet Neurol. 2021 Dec;20(12):e7]. Lancet Neurol. 2018;17(11):954–976. doi:10.1016/S1474-4422(18)30322-3
2. Rho YI, Chung HJ, Lee KH, et al. Prevalence and clinical characteristics of primary headaches among school children in South Korea: a nationwide survey. Headache. 2012;52(4):592–599. doi:10.1111/j.1526-4610.2011.02001.x
3. Onofri A, Pensato U, Rosignoli C, et al. Primary headache epidemiology in children and adolescents: a systematic review and meta-analysis. J Headache Pain. 2023;24(1):8. doi:10.1186/s10194-023-01541-0
4. Arruda MA, Bigal ME. Behavioral and emotional symptoms and primary headaches in children: a population-based study. Cephalalgia. 2012;32(15):1093–1100. doi:10.1177/0333102412454226
5. Onofri A, Olivieri L, Silva P, Bernassola M, Tozzi E. Correlation between primary headaches and learning disabilities in children and adolescents. Minerva Pediatr. 2022;74(1):1–6. doi:10.23736/S2724-5276.21.06191-7
6. Esposito M, Marotta R, Gallai B, et al. Temperamental characteristics in childhood migraine without aura: a multicenter study. Neuropsychiatr Dis Treat. 2013;9:1187–1192. doi:10.2147/NDT.S50458
7. Esposito M, Roccella M, Parisi L, Gallai B, Carotenuto M. Hypersomnia in children affected by migraine without aura: a questionnaire-based case-control study. Neuropsychiatr Dis Treat. 2013;9:289–294. doi:10.2147/NDT.S42182
8. Kafle M, Mirea L, Gage S. Association of psychiatric comorbidities with treatment and outcomes in pediatric migraines. Hosp Pediatr. 2022;12(3):e101–e105. doi:10.1542/hpeds.2021-006085
9. Walter SM, Dai Z, Wang K. Comorbidities of rural children and adolescents with migraine and without migraine. Children. 2023;10(7):1133. doi:10.3390/children10071133
10. Esposito M, Gallai B, Parisi L, et al. Maternal stress and childhood migraine: a new perspective on management. Neuropsychiatr Dis Treat. 2013;9:351–355. doi:10.2147/NDT.S42818
11. Smirni D, Carotenuto M. Pediatric chronic migraine severity and maternal stress. Pediatr Rep. 2021;13(4):576–582. doi:10.3390/pediatric13040068
12. Martin VT, Fanning KM, Serrano D, Buse DC, Reed ML, Lipton RB. Asthma is a risk factor for new onset chronic migraine: results from the American migraine prevalence and prevention study. Headache. 2016;56(1):118–131. doi:10.1111/head.12731
13. Xu J, Kong F, Buse DC. Predictors of episodic migraine transformation to chronic migraine: a systematic review and meta-analysis of observational cohort studies. Cephalalgia. 2020;40(5):503–516. doi:10.1177/0333102419883355
14. Su J, Zhou XY, Zhang GX. Association between Helicobacter pylori infection and migraine: a meta-analysis. World J Gastroenterol. 2014;20(40):14965–14972. doi:10.3748/wjg.v20.i40.14965
15. Chang FY, Lu CL. Irritable bowel syndrome and migraine: bystanders or partners? J Neurogastroenterol Motil. 2013;19(3):301–311. doi:10.5056/jnm.2013.19.3.301
16. Meucci G, Radaelli F, Prada A, et al. Increased prevalence of migraine in patients with uninvestigated dyspepsia referred for open-access upper gastrointestinal endoscopy. Endoscopy. 2005;37(7):622–625. doi:10.1055/s-2005-870251
17. Arzani M, Jahromi SR, Ghorbani Z, et al. Gut-brain axis and migraine headache: a comprehensive review. J Headache Pain. 2020;21(1):15. doi:10.1186/s10194-020-1078-9
18. Savi L, Ribaldone DG, Fagoonee S, Pellicano R. Is Helicobacter pylori the infectious trigger for headache?: a review. Infect Disord Drug Targets. 2013;13(5):313–317. doi:10.2174/1871526513666131201125021
19. Gelfand AA. Infant colic--a baby’s migraine? Cephalalgia. 2015;35(14):1243–1245. doi:10.1177/0333102415576224
20. Azmy DJ, Qualia CM. Review of abdominal migraine in children. Gastroenterol Hepatol. 2020;16(12):632–639.
21. Dignan F, Abu-Arafeh I, Russell G. The prognosis of childhood abdominal migraine. Arch Dis Child. 2001;84(5):415–418. doi:10.1136/adc.84.5.415
22. Olesen J. Headache Classification Committee of the International Headache Society (IHS) the international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
23. Kim L, Kim JA, Kim S. A guide for the utilization of health insurance review and assessment service national patient samples. Epidemiol Health. 2014;36:e2014008. doi:10.4178/epih/e2014008
24. Yoon CY, Ahn JJ, Lee G, et al. Developing the new national patient sample and evaluating representations. HIRA Res. 2021;1(2):166–178. doi:10.52937/hira.21.1.2.166
25. Jahangir S, Adjepong D, Al-Shami HA, Malik BH. Is there an association between migraine and major depressive disorder? A narrative review. Cureus. 2020;12(6):e8551. doi:10.7759/cureus.8551
26. Agostoni E, Rigamonti A. Migraine and cerebrovascular disease. Neurol Sci. 2007;28(Suppl 2):S156–S160. doi:10.1007/s10072-007-0770-8
27. Adelborg K, Szépligeti SK, Holland-Bill L, et al. Migraine and risk of cardiovascular diseases: Danish population based matched cohort study. BMJ. 2018;360:k96. doi:10.1136/bmj.k96
28. Çilliler AE, Güven H, Çomoğlu SS. Epilepsy and headaches: further evidence of a link. Epilepsy Behav. 2017;70(Pt A):161–165. doi:10.1016/j.yebeh.2017.03.009
29. Kim J, Lee S, Rhew K. Association between gastrointestinal diseases and migraine. Int J Environ Res Public Health. 2022;19(7):4018. doi:10.3390/ijerph19074018
30. Cole JA, Rothman KJ, Cabral HJ, Zhang Y, Farraye FA. Migraine, fibromyalgia, and depression among people with IBS: a prevalence study. BMC Gastroenterol. 2006;6:26. doi:10.1186/1471-230X-6-26
31. Vandvik PO, Wilhelmsen I, Ihlebaek C, Farup PG. Comorbidity of irritable bowel syndrome in general practice: a striking feature with clinical implications. Aliment Pharmacol Ther. 2004;20(10):1195–1203. doi:10.1111/j.1365-2036.2004.02250.x
32. Liberale L, Badimon L, Montecucco F, Lüscher TF, Libby P, Camici GG. Inflammation, aging, and cardiovascular disease: JACC review topic of the week. J Am Coll Cardiol. 2022;79(8):837–847. doi:10.1016/j.jacc.2021.12.017
33. Mou Y, Du Y, Zhou L, et al. Gut microbiota interact with the brain through systemic chronic inflammation: implications on neuroinflammation, neurodegeneration, and aging. Front Immunol. 2022;13:796288. doi:10.3389/fimmu.2022.796288
34. Cámara-Lemarroy CR, Rodriguez-Gutierrez R, Monreal-Robles R, Marfil-Rivera A. Gastrointestinal disorders associated with migraine: a comprehensive review. World J Gastroenterol. 2016;22(36):8149–8160. doi:10.3748/wjg.v22.i36.8149
35. Mayer EA, Tillisch K, Gupta A. Gut/brain axis and the microbiota. J Clin Invest. 2015;125(3):926–938. doi:10.1172/JCI76304
36. Hindiyeh N, Aurora SK. What the gut can teach us about migraine. Curr Pain Headache Rep. 2015;19(7):33. doi:10.1007/s11916-015-0501-4
37. Ramachandran R. Neurogenic inflammation and its role in migraine. Semin Immunopathol. 2018;40(3):301–314. doi:10.1007/s00281-018-0676-y
38. Murphy SF, Schaeffer AJ, Thumbikat P. Immune mediators of chronic pelvic pain syndrome. Nat Rev Urol. 2014;11(5):259–269. doi:10.1038/nrurol.2014.63
39. Welander NZ, Rukh G, Rask-Andersen M, et al. Migraine, inflammatory bowel disease and celiac disease: a Mendelian randomization study. Headache. 2023;63(5):642–651. doi:10.1111/head.14470
40. Dodick DW. CGRP ligand and receptor monoclonal antibodies for migraine prevention: evidence review and clinical implications [published correction appears in Cephalalgia. 2019 Jul;39(8):1069]. Cephalalgia. 2019;39(3):445–458. doi:10.1177/0333102418821662
41. Lipton RB, Croop R, Stock EG, et al. Rimegepant, an oral calcitonin gene-related peptide receptor antagonist, for migraine. N Engl J Med. 2019;381(2):142–149. doi:10.1056/NEJMoa1811090
42. Clarke G, Grenham S, Scully P, et al. The microbiome-gut-brain axis during early life regulates the hippocampal serotonergic system in a sex-dependent manner. Mol Psychiatry. 2013;18(6):666–673. doi:10.1038/mp.2012.77
43. Faraji F, Zarinfar N, Zanjani AT, Morteza A. The effect of Helicobacter pylori eradication on migraine: a randomized, double blind, controlled trial. Pain Physician. 2012;15(6):495–498.
44. Li C, Yu S, Li H, et al. Clinical features and risk factors for irritable bowel syndrome in Migraine patients. Pak J Med Sci. 2017;33(3):720–725. doi:10.12669/pjms.333.12379
45. Teleanu RI, Vladacenco O, Teleanu DM, Epure DA. Treatment of pediatric migraine: a review. Maedica. 2016;11(2):136–143.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.