Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Association Between Metabolic Dysfunction-Associated Fatty Liver Disease and MACCEs in Patients with Diabetic Foot Ulcers: An Ambispective Longitudinal Cohort Study
Authors Huang X, Li Z ![]() , Zhai Z, Wang Q, Wei R, Mo J
, Zhai Z, Wang Q, Wei R, Mo J ![]() , Huang J, Lu W
, Huang J, Lu W ![]()
Received 14 November 2023
Accepted for publication 28 February 2024
Published 6 March 2024 Volume 2024:17 Pages 1119—1130
DOI https://doi.org/10.2147/DMSO.S447897
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Xiuxian Huang,1,* Zhengming Li,1,* Zhenwei Zhai,1,* Qiu Wang,1 Rongyan Wei,1 Jiacheng Mo,2 Jianhao Huang,1 Wensheng Lu1,*
1Department of Endocrinology and Metabolism of Guangxi Academy of Medical Sciences, People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, Guangxi, 530021, People’s Republic of China; 2Information Network Center of Guangxi Academy of Medical Sciences, People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, Guangxi, 530021, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wensheng Lu, Email [email protected]
Aim: Metabolic dysfunction-related fatty liver disease (MAFLD) is closely related to metabolic disorders. However, the relationship between MAFLD and the prognosis in diabetic foot ulcers (DFUs) remains unclear. This study aimed to explore the association between MAFLD and the risk of major adverse cardiac and cerebral events (MACCEs) in patients with DFUs.
Methods: 889 inpatients with DFUs (PEDIS/TEXAS mild and above) were included in this study from 2013 to 2023. All participants were placed into non-MAFLD (n = 643) and MAFLD (n = 246) groups and followed up every 6 months for 10.9 years with a median of 63 months through in-person outpatient interviews and family fixed-line telephone visits. The association between MAFLD and the risk of MACCEs was evaluated through Multivariate Cox regression analyses, Stratified analyses and Kaplan-Meier survival analyses.
Results: Of the 889 subjects, 214 (24.07%) experienced MACCEs. Multivariate Cox regression analysis showed that MAFLD was independently associated with MACCEs (P < 0.001), of which with non-fatal myocardial infarction (P = 0.04), non-fatal stroke (P = 0.047), coronary artery revascularization (P = 0.002), heart failure (P = 0.029), and all-cause mortality (P = 0.021), respectively. The stratified analysis revealed that compared with non-MAFLD (HR=1), DFUs with MAFLD had a 2.64-fold increased risk for MACCEs (P < 0.001; P for interaction = 0.001) in peripheral arterial disease (PAD) subgroup. Kaplan-Meier analysis evidenced that the MAFLD group had a higher cumulative incidence of MACCEs (log-rank, all P < 0.05).
Conclusion: MAFLD is a high-risk factor for MACCEs in patients with DFUs. The findings will remind clinicians to pay more attention to MAFLD in patients with DFUs, especially in patients with DFUs combined with PAD as early as possible in clinical practice and adopt timely effective intervention strategies to prevent the occurrence of MACCEs to improve the clinical prognosis in patients with DFUs.
Keywords: diabetic foot ulcers, peripheral arterial disease, metabolic dysfunction-associated fatty liver disease, major adverse cardiac and cerebral events
Introduction
At present, China has the highest incidence rate of diabetes in the world, with a prevalence rate of 12.4%, of which about 30% will eventually suffer from diabetes foot ulcers (DFUs).1 DFUs refer to a foot ulcer, infection, or profound tissue destruction caused by peripheral arterial disease (PAD), lower extremity arterial ischemia, peripheral neuropathy, and deep tissue infection.2 DFUs are characterized by high morbidity, disability, and mortality caused by severe infection, pulmonary embolism, myocardial infarction, cerebral infarction, heart failure, and surgical amputation.3 The recurrence rates of DFUs are 40% within a year, 60% within three years, and 65% within five years worldwide.4 Patients with DFUs have a 2.5 times higher mortality risk than those without DFUs,5 and the 5-year mortality rate is nearly identical to malignancy.6 DFUs with a prevalence rate of 8.1%, 31.6% recurrence rate, 5.1% amputation rate, and 14.4% mortality rate in China have seriously threatened public health and brought a huge economic burden to society.1
Approximately 25% of adults worldwide suffer from metabolic dysfunction-associated fatty liver disease (MAFLD), formerly known as non-alcoholic fatty liver disease (NAFLD), which has a significant negative impact on public health and economic development.7 Recently, an international expert group from 22 countries reached a consensus on naming NAFLD as MAFLD and the diagnostic criteria for MAFLD. The criteria are based on evidence of hepatic steatosis and one of the three conditions listed below: existing overweight or obesity, T2DM or metabolic dysregulation.7 With this newly revised classification, most DM can be categorized as MAFLD, indicating a strong association between diabetes and MAFLD.8,9 MAFLD, characterized by insulin resistance, obesity, and type 2 diabetes, may associated with a dysbiosis of the gut microbiota, in which toxic chemicals, including LPS from Gram-negative bacteria, can enter the liver through the portal vein due to the increased permeability of the intestinal barrier, also referred to as “leaky gut”, formation of insulin resistance in the liver.10 Even though obesity and MAFLD are commonly linked, there is growing evidence that not everyone who is overweight or obese goes on to develop fatty liver disease. However, a sizable fraction of MAFLD patients have normal weight, demonstrating the significance of metabolic health in the disease’s pathophysiology independent of body mass index.11 Multidisciplinary efforts to manage the complex condition can be enhanced by focusing more on managing concurrent metabolic disease in MAFLD patients.12 The change in the term and description of NAFLD to MAFLD is a noteworthy turning point that shows a great deal of concrete progress in the direction of a patient-centered, egalitarian, and inclusive approach to tackling the severe obstacles associated with this disease. A growing body of research has demonstrated the specific and larger settings that can significantly impact the diagnosis and course of treatment. The momentum behind this nomenclature change has also drawn extensive public attention to the distinctive burden of this hitherto unappreciated disease, especially adverse clinical outcomes in diabetes complications such as DFUS.13
Recent studies revealed that MAFLD patients had a higher risk of all-cause mortality, cardiovascular disease-related mortality, and cancer-associated mortality.14,15 Global epidemiological data show that the comorbidity incidence of T2DM in patients with MAFLD is 22.5%, while 43.6% are in the non-alcoholic steatohepatitis (NASH) stage.16 With an exceeding 15% prevalence incidence in the population, MAFLD has nearly doubled with the rapidly rising rate of obesity over the last ten years in China.17 Given the fragility of pancreatic islet function in the elderly, the impact of MAFLD on the elderly is far more significant than that of young individuals.18 Therefore, the management strategy for patients with T2DM should address the coexistence of MAFLD and T2DM to achieve ideal goals, especially in the elderly patients.18
To sum up, DFUs and MAFLD have increasingly become a massive threat to public health and quality of life. In light of this, exploring the association between MAFLD and MACCEs in patients with DFUs is particularly urgent. To date, no evidence-based literature has been published on the association between MAFLD and the risk of MACCEs in patients with DFUs. This study aimed to explore the relationship between MAFLD and the risk factors for MACCEs in patients with DFUs for the first time, which aided in stopping or delaying the occurrence of MACCEs to improve the clinical outcomes and quality of life in patients with DFUs.
Methods
Study Design and Subjects
The data of this study originated from the Foot Care Database of the Foot Disease Center of the People’s Hospital of Guangxi Zhuang Autonomous Region. The screening strategy for participants is listed in Figure 1. Finally, 889 inpatients with DFUs were enrolled in the current study. The average age of participants in this study was 63 years old, of which 68.2% were male. The infection severity of DFUs was evaluated as PEDIS level 2 or above.19 The ischemia severity of DFUs was assessed as TEXAS 1C or above.20 None of the subjects had a history of amputation surgery. The inclusion criteria were as follows: (1) aged over 18 years old; (2) T2DM diagnosed according to WHO criteria in 1999;21 and (3) DFUs diagnosed and classified based on IWGDF criteria in 2019.22 The exclusion criteria were as follows: (1) foot ulcers without T2DM; (2) malignant tumors; (3) rheumatoid arthritis, osteoporosis, thyroid dysfunction, vitamin D deficiency, hypoproteinemia, and malnutritional anemia; (4) specific drug treatment: glucocorticoids, immunosuppressants, or immunomodulators; (5) hemodialysis therapeutic regimes; (6) missing liver ultrasound data for identifying MAFLD; and (7) missing complete hospitalization data, loss to follow-up or follow-up time of less than 1 year. Additionally, it should be illustrated that surgical amputation in DFUs is an extreme situation that is affected by many factors, such as infection, nutritional status, Wound debridement technology, etc. To eliminate the influence of confounding factors, this study did not include patients who have undergone surgical amputation.
 |
Figure 1 Flow chart for selecting patients with DFUs. |
All participants receiving standardized anti-hyperglycemia, anti-hyperlipidemia, anti-hyperuricemia, anti-hypertension, and anticoagulant therapeutic schedules according to the requirements of the Chinese Diabetes Guidelines, were divided into two groups: non-MAFLD (n = 643, 72.33%) and MAFLD (n = 246, 27.67%). All subjects were followed up every 6 months for 10.9 years with a median of 63 months through in-person outpatient interviews or family fixed-line telephone visits by trained professional medical staff. All participants agreed to participate in the study and signed written informed consent. The principles of the Declaration of Helsinki were followed. All experiments were performed with approval from the Ethics Committee of the Guangxi Academy of Medical Sciences and Guangxi People’s Hospital.
Related Definitions
MAFLD was diagnosed following the international expert consensus statement mentioned above,7 based on the combined evidence of fatty liver identified through ultrasound imaging in patients with T2DM. The other relevant definitions in this study were as follows: (1) MACCEs referred to non-fatal myocardial infarction, coronary artery revascularization, heart failure, non-fatal stroke, and all-cause mortality. Coronary artery revascularization was defined as blood flow recovery through percutaneous intervention or coronary-artery-bypass-grafting (CABG) of the target vessels. Non-fatal stroke, consisting of ischemic and hemorrhagic stroke, was defined as a neurological dysfunction caused by sudden cerebral vascular rupture or occlusion, according to computed tomography or magnetic resonance imaging. (2) DFUs were defined as infection and ischemic ulcers on the lower extremity below the ankle. (3) PEDIS (Perfusion, Extent, Depth, Infection, and Sensation) infection classification standards of DFUs include grade 1-uninfected; grade 2-mild infection (with at least two symptoms: suppuration, erythema, pain, warmth, or sclerosis; cellulitis ≤ 2cm around the ulcer; mild skin infection; no other complications); grade-3: moderate infection (if there are symptoms described as mild infection and at least one cellulitis > 2 cm, with deep tissue abscess formation, gangrene, and some life-threatening symptoms; involving muscles, tendons, joints, or bones); grade-4: severe infection (infection accompanied by systemic toxicity or metabolic instability; fever, chills, tachycardia, hypotension, unclear consciousness, vomiting, severe hyperglycemia, acidosis, or azotemia).22 (4) TEXAS ischemic classification standards of DFUs include Grade 0A: unruptured epidermis, 0B: infection, 0C: ischemia, 0D: infection and ischemia; Grade 1A: skin damage only, 1B: infection, 1C: ischemia, 1D: infection and ischemia. Grade 2A: damage involving tendons, 2B: infection, 2C: ischemia, 2D: infection and ischemia; Grade 3A: damage involving bones, 3B: infection, 3C: ischemia, 3D: infection and ischemia.22 (5) Peripheral arterial disease (PAD) was defined as an ankle-brachial index (ABI) ≤ 0.9 with the presence of decreased pulsation of the dorsal pedal artery and intermittent claudication based on the recommendations of IWGDF in 2019.22
Data Collection
Demographic data, anthropometric data, laboratory biochemical index data, inpatient medical records information, and follow-up data were collected from the Foot Care Database of the Foot Disease Center of the People’s Hospital of Guangxi Zhuang Autonomous Region. Every participant in the study had accessible and traceable clinical data, including medical records and ongoing follow-up information. Data collection and analysis follow the principles of confidentiality. Data collection was approved by the Ethics Committee of the Guangxi Academy of Medical Sciences and the People’s Hospital of Guangxi Zhuang Autonomous Region.
Outcomes
The primary endpoint events of this study were MACCEs consisting of non-fatal myocardial infarction, coronary artery revascularization, heart failure, non-fatal stroke, and all-cause death. The trained professional medical staff gathered the endpoint events through in-person outpatient interviews and family fixed-line telephone visits. All individuals were continuously followed up every 6 months with a median of 63 months for 10.9 years. On September 30, 2023, the last follow-up data were gathered.
Statistical Analysis
Nonnormally distributed continuous variables are displayed as medians (interquartile ranges). The classification variables are represented as frequencies. The nonparametric Mann‒Whitney U-test was used to compare continuous variables with nonnormal intergroup distribution. The chi-square test was used for intergroup comparisons of categorical variables. Cox regression analysis evaluated the hazard ratios and 95% confidence intervals for the association between MAFLD and MACCEs in patients with DFUs. Three multivariate regression models were built and used to adjust for potential confounding factors of MACCEs gradually. Model I was adjusted for none. Model II was additionally adjusted for gender and age with Model I. Model III was further adjusted for hyperlipidemia, hypertension, PAD, CHD, CVD, DN, duration of diabetes, SBP, and TC with Model II. The stratified analysis results of the subgroup are presented in forest plots through GraphPad Prism 9.3 (GraphPad Software, San Diego, CA). Kaplan‒Meier survival curve analysis was used to calculate the cumulative incidence of MACCEs and differences between the two groups were assessed through the Log rank test. The study sample size and power analysis were calculated using PASS 11.0 (https://www.ncss.com/download/pass/updates/pass11/) to ensure that the minimum cases met a high testing power of over 90%. Data analyses were performed using the SPSS 23.0 statistical software package (IBM Corp., Armonk, NY, USA). Statistical significance was set at the P < 0.05 level.
Results
Baseline Characteristics
A total of 889 patients with DFUs were included in this longitudinal cohort analysis. The baseline characteristics of the subjects are detailed in Table 1. All subjects were divided into two groups: non-MAFLD (n = 643, 72.33%) and MAFLD (n = 246, 27.67%). The average age of the study population was 63 years old, and 68.2% were males. SBP, DBP, Hb, TC, TG, LDL-c, Alb, ALT, Cr., and UA showed significant differences between the two groups (all P < 0.05). Gender, age, hypertension, CHD, CVD, PAD, DR, DPN, DN, smoking history, drinking history, diabetes course, WBC, HDL-c, AST, and HbA1c were not significantly different between the groups (all P > 0.05).
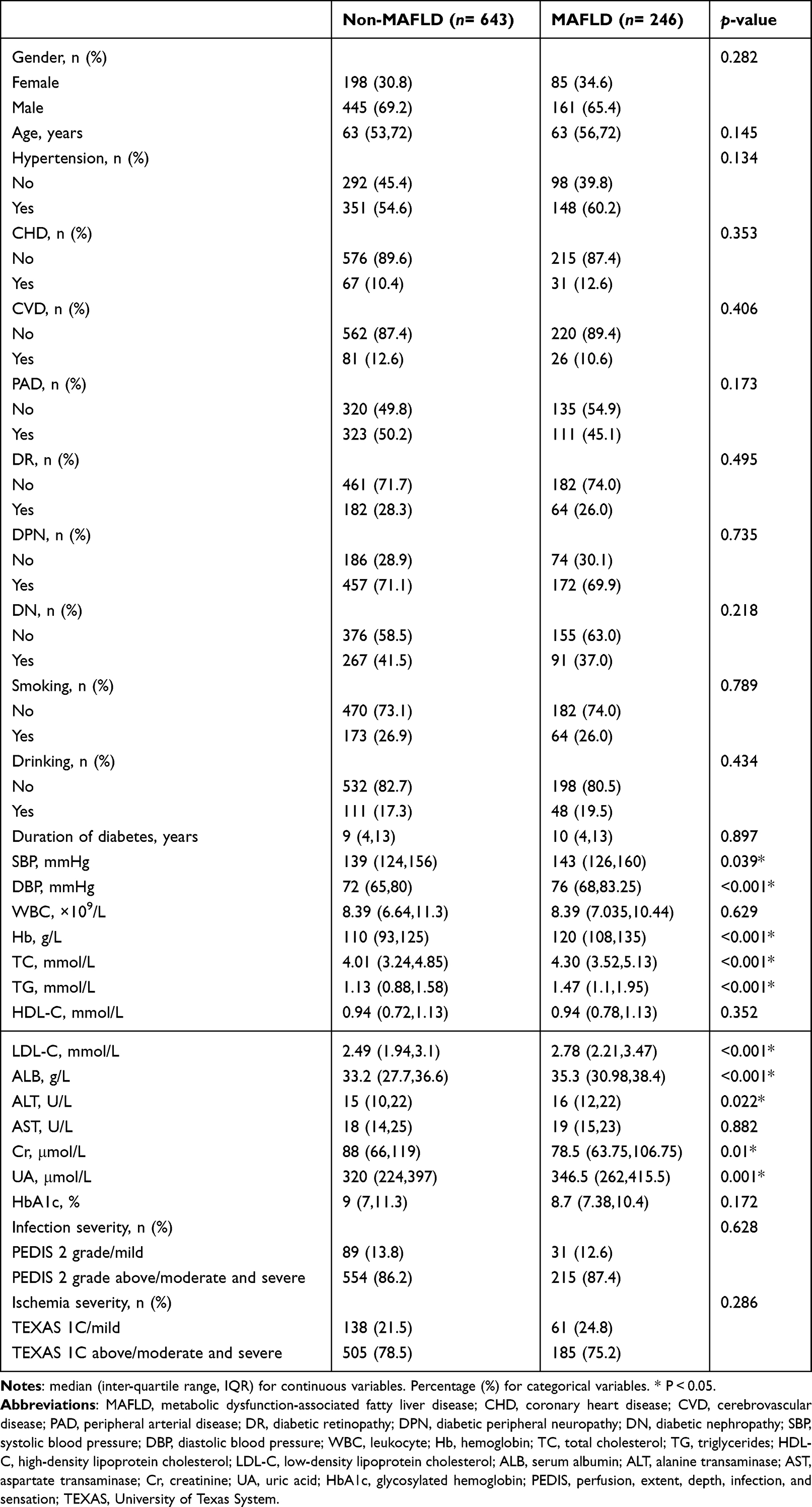 |
Table 1 Baseline Characteristics of the Subjects |
Cox Regression Analysis
The incidence rates of MACCEs (19.4% and 36.2%) including all-cause mortality (5.0% and 9.3%), non-fatal myocardial infarction (2.5% and 5.7%), coronary artery revascularization (3.0% and 8.5%), non-fatal stroke (10.6% and 17.1%), and heart failure (2.6% and 6.1%) are listed in detail in Figure 2 for the non-MAFLD and MAFLD groups. Then, variables with P <0.1 in univariate Cox regression analysis were included in multivariate Cox regression analysis (Table 2). Cox regression analysis showed that MAFLD was independently related to the incidence of MACCEs in patients with DFUs in Model I (unadjusted) (HR = 1.993, 95% CI = 1.518–2.615, P <0.001), Model II (Model I adjusted for gender and age) (HR=1.977, 95% CI = 1.506–2.596, P <0.001), and Model III (Model II adjusted for was further adjusted for hyperlipidemia, hypertension, PAD, CHD, CVD, DN, duration of diabetes, SBP, and TC) (HR = 1.94, 95% CI = 1.474–2.553, P < 0.001). Additionally, MAFLD is also an independent risk factor in the specific disease components of MACCEs such as all-cause mortality (Model I: HR = 1.856, 95% CI = 1.086–3.172, P = 0.024; Model II: HR = 1.822, 95% CI = 1.066–3.116, P = 0.028; Model III: HR = 1.902, 95% CI = 1.103–3.279, P = 0.021), non-fatal myocardial infarction (Model I: HR = 2.215, 95% CI = 1.081–4.54, P = 0.03; Model II: HR = 2.165, 95% CI = 1.056–4.442, P = 0.035; Model III: HR = 2.148, 95% CI = 1.036–4.452, P = 0.04), coronary artery revascularization (Model I: HR = 2.868, 95% CI = 1.541–5.335, P = 0.001; Model II: HR = 2.846, 95% CI = 1.527–5.303, P = 0.001; Model III: HR = 2.73, 95% CI = 1.46–5.104, P = 0.002), non-fatal stroke (Model I: HR = 1.59, 95% CI = 1.082–2.336, P = 0.018; Model II: HR = 1.564, 95% CI = 1.064–2.298, P = 0.023; Model III: HR = 1.487, 95% CI = 1.006–2.199, P = 0.047), and heart failure (Model I: HR = 2.223, 95% CI = 1.11–4.451, P = 0.024; Model II: HR = 2.196, 95% CI = 1.095–4.403, P = 0.027; Model III: HR = 2.197, 95% CI = 1.085–4.452, P = 0.029), respectively. The results of Cox regression analysis suggested that MAFLD was a high-risk factor for MACCEs in patients with DFUs.
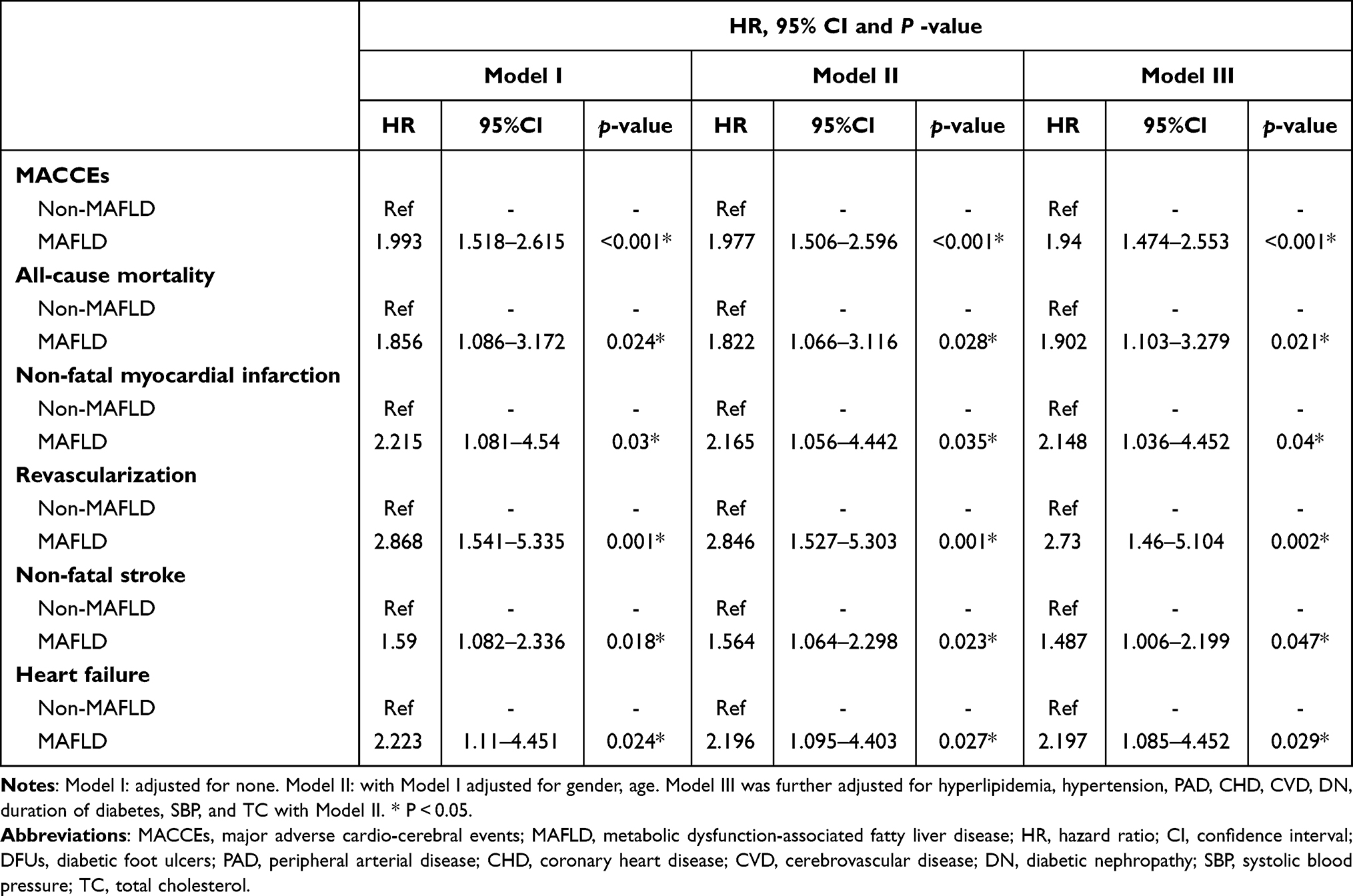 |
Table 2 Risk of MACCEs in Subjects with DFUs Between Two Groups Through Multivariate Cox Regression Analyses |
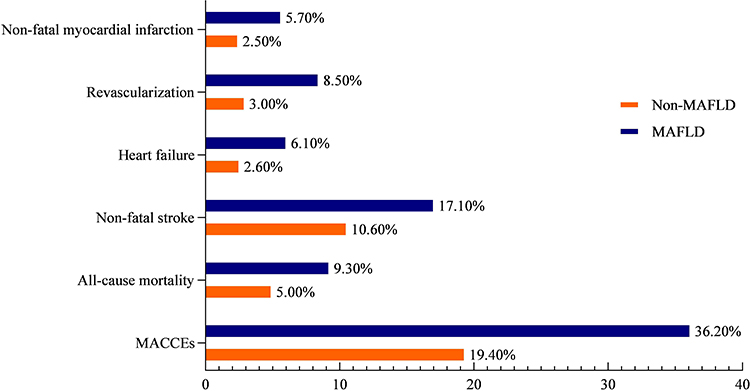 |
Figure 2 The incidence of MACCEs in patients with DFUs between MAFLD and non-MAFLD groups. Abbreviations: MACCEs, major adverse cardiac and cerebral events; MAFLD, metabolic dysfunction-associated fatty liver disease. Notes: During the follow-up period with a median of 63 months for 10.9 years, the incidence rate of MACCEs, including non-fatal myocardial infarction, coronary artery revascularization, heart failure, non-fatal stroke, and all-cause mortality, was listed in detail between the MAFLD and non-MAFLD groups. |
Stratified Analysis in Subgroups
Stratified analysis by age, gender, LDL-c, SBP, CHD, PAD, and DN is shown in the forest plots (Figure 3). Except for the stratification factors themselves, each stratification was adjusted for all factors, including all independent variables in the Cox regression analysis. The stratified analysis revealed that in peripheral arterial disease (PAD) subgroup, MAFLD was a high-risk factor for MACCEs. Compared with non-MAFLD (HR=1), DFUs with MAFLD combined with PAD had a 2.64-fold increased risk for MACCEs (HR = 3.64, 95% CI = 2.358–5.62, P <0.001; P for interaction = 0.001). However, there were not relationship between MAFLD and age (HR = 2.094, 95% CI = 1.417–3.096, P < 0.001, P for interaction= 0.755), sex (HR = 2.249, 95% CI = 1.61–3.141, P < 0.001, P for interaction= 0.128), LDL-C ≥ 2.6 mmol/L (HR =2.346, 95% CI = 1.62–3.398, P < 0.001, P for interaction=0.107), SBP ≥ 140 mmHg (HR =2.204, 95% CI = 1.541–3.154, P < 0.001, P for interaction=0.331), with CHD (HR = 2.969, 95% CI = 1.447–6.09, P = 0.003, P for interaction=0.241), without CHD (HR =1.84, 95% CI = 1.36–2.489, P < 0.001, P for interaction=0.241), with DN (HR = 2.019, 95% CI = 1.331–3.062, P = 0.001, P for interaction=0.884), without DN (HR = 1.983, 95% CI = 1.371–2.868, P < 0.001, P for interaction=0.884), respectively. The results of stratified analysis confirmed that MAFLD was a high-risk factor for MACCEs in patients with DFUs combined with PAD.
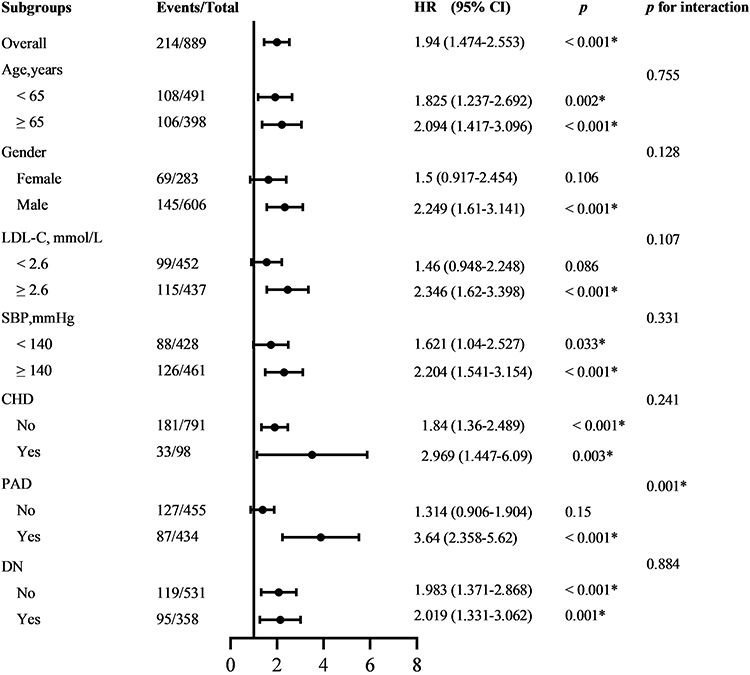 |
Figure 3 Subgroup stratified analysis for the association between MAFLD and MACCEs in the forest plots. Abbreviations: MAFLD, metabolic dysfunction-associated fatty liver disease; MACCEs, major adverse cardiac and cerebral events; HR, hazard ratio; CI, confidence interval; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; CHD, coronary heart disease; PAD, peripheral arterial disease; DN, diabetic nephropathy. Notes: Except for the stratification factors themselves, each stratification was adjusted for all factors, including all independent variables in the Cox regression analysis. *P < 0.05. |
Kaplan‒Meier Survival Curve Analysis
During the follow-up period, out of 889 patients with DFUs, 214 (24.07%) developed MACCEs. Kaplan‒Meier survival curve analysis showed that compared with the non-MAFLD group, the MAFLD group had a higher cumulative incidence of MACCEs (Figure 4), including all-cause mortality (A), non-fatal myocardial infarction (B), coronary artery revascularization (C), non-fatal stroke (D), heart failure (E) in patients with DFUs (log-rank, all P < 0.05). The Kaplan‒Meier survival analysis results further revealed that MAFLD was a high-risk factor for MACCEs in patients with DFUs.
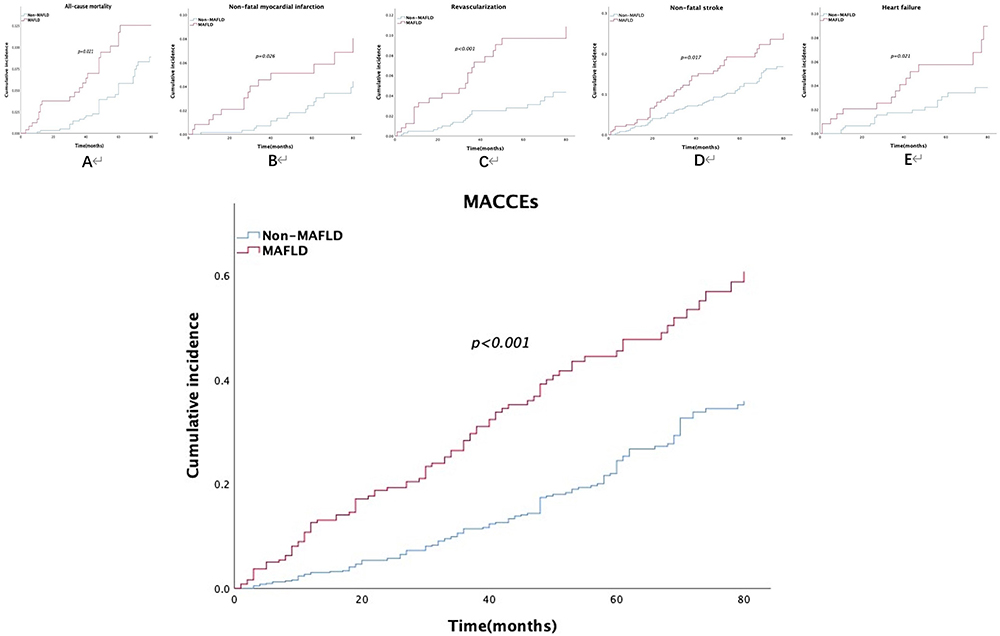 |
Figure 4 The cumulative incidence of MACCEs between MAFLD and non-MAFLD groups. Abbreviations: MACCEs, major adverse cardiac and cerebral events; MAFLD, metabolic dysfunction-associated fatty liver disease. Notes: Kaplan‒Meier analysis showed that compared with the non-MAFLD group, the MAFLD group had a higher cumulative incidence of MACCEs consisting of all-cause mortality (A), non-fatal myocardial infarction (B), coronary artery revascularization (C), and non-fatal stroke (D), and heart failure (E) in patients with DFUs (log-rank, p < 0.05). |
Discussion
MAFLD, formerly known as NAFLD, affects roughly a quarter of adults and approximately 50% of T2DM patients, which has put nearly all nations globally, whether developed or underdeveloped, under tremendous financial and health burdens.16,23–25 Since introducing the new definition highlighting metabolic dysfunction issues, MAFLD has quickly become a research hotspot.26 Theoretically, metabolic dysfunction should be related to the clinical prognosis in patients with DFUs. However, whether MAFLD is associated with MACCEs in patients with diabetic foot ulcers (DFUs) remains unclear. To our knowledge, this is the first study to evaluate the relationship between MAFLD and the primary adverse clinical outcomes in patients with DFUs.
This cohort study suggested that the prevalence of MAFLD in the study population was 27.67%, and MAFLD patients were more likely to exhibit hypertension, metabolic liver dysfunction, abnormal blood lipids, and a more significant impact on cardiovascular risk in patients with T2DM, which was consistent with previous research findings.27–32 In our study, Of the 889 subjects, 214 experienced MACCEs. Multivariate Cox regression analysis, stratified analysis, and Kaplan-Meier survival analysis showed that MAFLD was independently associated with MACCEs consisting of non-fatal myocardial infarction, non-fatal stroke, coronary artery revascularization, heart failure, and all-cause mortality in patients with DFUs. The findings clearly show that MAFLD plays an essential role in the prognosis of patients with DFUs.
According to the latest definition, obesity, hypertension, and dyslipidemia all fall under the umbrella of MAFLD, particularly type 2 diabetes characterized by glycotoxicity and lipotoxicity.24,33 The primary pathogenesis of MAFLD is still hepatic insulin resistance.34 An international cohort of patients with NASH and Child-Pugh A cirrhosis confirmed by biopsy evidenced that MAFLD-related type 2 diabetes increased the risk of mortality and liver-related outcomes, including hepatocellular carcinoma (HCC), in which taking metformin, an insulin sensitizer, has a higher survival rate, lower rates of decompensation and HCC.35 MAFLD disrupts the natural equilibrium between energy intake and expenditure in the body, causing fat to accumulate in the liver and vascular walls and ultimately leading to fatty liver, liver insulin resistance, and atherosclerotic cardiovascular disease (ASCVD).36–42 When hepatic steatosis modifies hepatocytokine secretion, it creates a complementary reciprocal condition that affects fatty acid metabolism and insulin resistance in various tissues, including skeletal muscle, cardiovascular smooth muscle, adipose tissue, and the liver.43 Previous studies have shown that NAFLD is independently associated with chronic macrovascular and microvascular complications, especially with PAD in T2DM situations,44,45 and its mechanism may involve dyslipidemia, increased insulin resistance, modifications in hemostatic-fibrinolytic factors, elevated proinflammatory cytokines, and dysbiosis.39 Evidence suggests that DFUs are the inevitable outcome of the comprehensive combined effect of chronic macrovascular and microvascular complications in diabetic situations.46,47 Obviously, as the most typical complication of T2DM, DFUs characterized by macrovascular and microvascular pathological changes are inevitably related to the core pathological mechanism of insulin resistance.48,49 Our prior research also supported the finding about the fundamental mechanism of insulin resistance in cardiovascular adverse events of DFUs.50 Given this, MAFLD causes several clinical adverse vascular outcomes in patients with DFUs through the mediation of insulin resistance. Additionally, establishing a patient-centered multidisciplinary management framework is essential due to the global prevalence of chronic diseases like MAFLD, type 2 diabetes mellitus, chronic kidney disease, hypertension, stroke, cardiovascular disease, osteoporosis, cancer, and cognitive impairment. Conducting clinical care for MAFLD and related clinical experimental research is especially critical.51
Through a longitudinal cohort study, this project conducted the first preliminary evaluation of the association between MAFLD and the risk of MACCEs in patients with DFUs. This provides crucial guidance information for clinical practice. However, there are still some limitations. First, despite tissue biopsy being the most accurate approach for identifying fatty liver, ultrasonography is the typical inspection method in our hospital clinical practices owing to its noninvasive nature. Second, the severity of liver steatosis was not considered. Third, given that metabolic anomalies are dynamic, ongoing follow-up is still required for our cohort investigations. Finally, our study is a single-center study, and the research conclusion still needs to be confirmed by a large sample size, multicenter, and prospective cohort study.
In conclusion, MAFLD is a high-risk factor for MACCEs in patients with DFUs. The findings will remind clinicians to pay more attention to MAFLD in patients with DFUs, especially in patients with DFUs combined with PAD as early as possible in routine clinical practice and adopt timely effective intervention strategies to prevent the occurrence of MACCEs to improve the clinical prognosis in patients with DFUs.
Acknowledgments
We are grateful to all the patients and colleagues who gave their time and effort to the study.
Funding
The study was funded by the National Natural Science Foundation of China (82160052, 81560044, 30860113).
Disclosure
No potential conflicts of interest relevant to this article were reported.
References
1. Wang L, Peng W, Zhao Z, et al. Prevalence and treatment of diabetes in china, 2013–2018. JAMA. 2021;326(24):2498–2506. doi:10.1001/jama.2021.22208
2. Kirsner RS, Vivas AC. Lower-extremity ulcers: diagnosis and management. Br J Dermatol. 2015;173(2):379–390. doi:10.1111/bjd.13953
3. Kimura T, Watanabe Y, Tokuoka S, et al. Utility of skin perfusion pressure values with the society for vascular surgery wound, ischemia, and foot infection classification system. J Vasc Surg. 2019;70(4):1308–1317. doi:10.1016/j.jvs.2019.01.045
4. Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017;376(24):2367–2375. doi:10.1056/NEJMra1615439
5. Walsh JW, Hoffstad OJ, Sullivan MO, Margolis DJ. Association of diabetic foot ulcer and death in a population-based cohort from the United Kingdom. Diabet Med. 2016;33(11):1493–1498. doi:10.1111/dme.13054
6. Armstrong DG, Swerdlow MA, Armstrong AA, et al. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J Foot Ankle Res. 2020;13(1):16. doi:10.1186/s13047-020-00383-2
7. Eslam M, Newsome PN, Sarin SK, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73(1):202–209. doi:10.1016/j.jhep.2020.03.039
8. Tang M, Wei X-H, Cao H, et al. Association between Chinese visceral adiposity index and metabolic-associated fatty liver disease in Chinese adults with type 2 diabetes mellitus. Front Endocrinol. 2022;13:935980. doi:10.3389/fendo.2022.935980
9. Guan C, Fu S, Zhen D, et al. Metabolic (dysfunction)-associated fatty liver disease in Chinese patients with type 2 diabetes from a subcenter of the national metabolic management center. J Diabetes Res. 2022;2022:8429847. doi:10.1155/2022/8429847
10. Abenavoli L, Guido Maria Scarlata G, Scarpellini E, et al. Metabolic-dysfunction-associated fatty liver disease and gut microbiota: from fatty liver to dysmetabolic Syndrome. Medicina. 2023;59(3):594. doi:10.3390/medicina59030594
11. Eslam M, El-Serag HB, Francque S, et al. Metabolic (dysfunction)-associated fatty liver disease in individuals of normal weight. Nat Rev Gastroenterol Hepatol. 2022;19(10):638–651. doi:10.1038/s41575-022-00635-5
12. En Chan K, Jia Ling Koh T, Shao Pin Tang A, et al. Global prevalence and clinical characteristics of metabolic-associated fatty liver disease: a meta-analysis and systematic review of 10 739 607 individuals. J Clin Endocrinol Metab. 2022;107(9):2691–2700. doi:10.1210/clinem/dgac321
13. Alharthi J, Gastaldelli A, Homer Cua I, et al. Metabolic dysfunction-associated fatty liver disease: a year in review. Curr Opin Gastroenterol. 2022;38(3):251–260. doi:10.1097/MOG.0000000000000823
14. Meyersohn NM, Mayrhofer T, Corey KE, et al. Association of hepatic steatosis with major adverse cardiovascular events, independent of coronary artery disease. Clin Gastroenterol Hepatol. 2021;19(7):1480–1488.e14. doi:10.1016/j.cgh.2020.07.030
15. Le MH, Yeo YH, Li X, et al. 2019 Global NAFLD prevalence: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2022;20(12):2809–2817.e28. doi:10.1016/j.cgh.2021.12.002
16. Younossi ZM, Koenig AB, Abdelatif D, et al. Global epidemiology of non-alcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–84. doi:10.1002/hep.28431
17. Fan J-G, Farrell GC. Epidemiology of non-alcoholic fatty liver disease in China. J Hepatol. 2009;50(1):204–210. doi:10.1016/j.jhep.2008.10.010
18. Jeeyavudeen MS, Khan SKA, Fouda S, et al. Management of metabolic-associated fatty liver disease: the diabetology perspective. World J Gastroenterol. 2023;29(1):126–143. doi:10.3748/wjg.v29.i1.126
19. Schaper NC. Diabetic foot ulcer classification system for research purposes: a progress report on criteria for including patients in research studies. Diabetes Metab Res Rev. 2004;20(Suppl 1):S90–5. doi:10.1002/dmrr.464
20. Jeon B-J, Jun Choi H, Kang JS, et al. Comparison of five systems of classification of diabetic foot ulcers and predictive factors for amputation. Int Wound J. 2017;14(3):537–545. doi:10.1111/iwj.12642
21. Alberti KGMM, Zimmet PZ. Diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabetic Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
22. Lipsky BA, Senneville É, Abbas ZG, et al. Guidelines on the diagnosis and treatment of foot infection in persons with diabetes (IWGDF 2019 update). Diabetes Metab Res Rev. 2020;36(Suppl 1):e3280. doi:10.1002/dmrr.3280
23. Eslam M, Sanyal AJ, George J, et al. MAFLD: a consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology. 2020;158(7):1999–2014.e1. doi:10.1053/j.gastro.2019.11.312
24. Younossi ZM, Golabi P, de Avila L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol. 2019;71(4):793–801. doi:10.1016/j.jhep.2019.06.021
25. Xiaojun G, Zheng L, Wang M, et al. Prevalence trends in non-alcoholic fatty liver disease at the global, regional and national levels, 1990–2017: a population-based observational study. BMJ Open. 2020;10(8):e036663. doi:10.1136/bmjopen-2019-036663
26. Liao Y, Wang L, Liu F, et al. Emerging trends and hotspots in metabolic dysfunction-associated fatty liver disease (MAFLD) research from 2012 to 2021: a bibliometric analysis. Front Endocrinol. 2023;14:1078149. doi:10.3389/fendo.2023.1078149
27. Zhu XP, Han GC, Chen Q, et al. Fatty liver is a sensitive early warning for hypertension and its complication in the Chinese population. Clin Exp Hypertens. 2022;44(4):306–312. doi:10.1080/10641963.2022.2029469
28. Tokushige K, Ikejima K, Ono M, et al. Evidence-based clinical practice guidelines for non-alcoholic fatty liver disease/non-alcoholic steatohepatitis 2020. J Gastroenterol. 2021;56(11):951–963. doi:10.1007/s00535-021-01796-x
29. Youwen Y, Kangli L, Fei T, et al. Leukemia inhibitory factor protects against liver steatosis in non-alcoholic fatty liver disease patients and obese mice. J Biol Chem. 2022;298(6):101946. doi:10.1016/j.jbc.2022.101946
30. Matsubayashi Y, Fujihara K, Yamada-Harada M, et al. Impact of metabolic syndrome and metabolic dysfunction-associated fatty liver disease on cardiovascular risk by the presence or absence of type 2 diabetes and according to sex. Cardiovasc Diabetol. 2022;21(1):90. doi:10.1186/s12933-022-01518-4
31. Alexander M, KatrinaLoomis A, van der Lei J, et al. Non-alcoholic fatty liver disease and risk of incident acute myocardial infarction and stroke: findings from matched cohort study of 18 million European adults. BMJ. 2019;367:l5367. doi:10.1136/bmj.l5367
32. Baratta F, Pastori D, Angelico F, et al. Non-alcoholic fatty liver disease and fibrosis associated with increased risk of cardiovascular events in a prospective study. Clin Gastroenterol Hepatol. 2020;18(10):2324–2331.e4. doi:10.1016/j.cgh.2019.12.026
33. Lim GEH, Tang A, Ng CH, et al. An observational data meta-analysis on the differences in prevalence and risk factors between MAFLD vs NAFLD. Clin Gastroenterol Hepatol. 2023;21(3):619–629.e7. doi:10.1016/j.cgh.2021.11.038
34. Sakurai Y, Kubota N, Yamauchi T, et al. Role of insulin resistance in MAFLD. Int J Mol Sci. 2021;22(8):4156. doi:10.3390/ijms22084156
35. Vilar-Gomez E, Calzadilla-Bertot L, Wai-Sun Wong V, et al. Type 2 diabetes and metformin use associate with outcomes of patients with nonalcoholic steatohepatitis-related, child-pugh a cirrhosis. Clin Gastroenterol Hepatol. 2021;19(1):136–145.e6. doi:10.1016/j.cgh.2020.04.083
36. Shimabukuro M. MAFLD and ASCVD: plasma heparin cofactor ii activity as an anti-liver fibrosis biomarker. J Atheroscler Thromb. 2023;30(8):853–854. doi:10.5551/jat.ED227
37. Stols-Gonçalves D, Hovingh GK, Nieuwdorp M, et al. NAFLD and atherosclerosis: two sides of the same dysmetabolic coin? Trends Endocrinol Metab. 2019;30(12):891–902. doi:10.1016/j.tem.2019.08.008
38. Cholongitas E, Tsilingiris D, Diamantopoulou P, et al. Association of cardiovascular factors in diabetic patients with non-alcoholic fatty liver disease. Hormones. 2022;21(1):133–145. doi:10.1007/s42000-021-00334-x
39. Targher G, Lonardo A, Byrne CD. Non-alcoholic fatty liver disease and chronic vascular complications of diabetes mellitus. Nat Rev Endocrinol. 2018;14(2):99–114. doi:10.1038/nrendo.2017.173
40. Pal SC, Méndez-Sánchez N. Insulin resistance and adipose tissue interactions as the cornerstone of metabolic (dysfunction)-associated fatty liver disease pathogenesis. World J Gastroenterol. 2023;29(25):3999–4008. doi:10.3748/wjg.v29.i25.3999
41. Xiaoling L, Fengxia S, Zimeng S, et al. Effect of dangfei liganning capsule on liver X receptor α/steroid regulatory element binding protein-1/fatty acid synthase signal pathway in rats with metabolic- associated fatty liver disease. J Tradit Chin Med. 2022;42(6):940–947. doi:10.19852/j.cnki.jtcm.2022.06.007
42. Samuel VT, Shulman GI. The pathogenesis of insulin resistance: integrating signaling pathways and substrate flux. J Clin Invest. 2016;126(1):12–22. doi:10.1172/JCI77812
43. Zhang L, She Z-G, Hongliang L, et al. Non-alcoholic fatty liver disease: a metabolic burden promoting atherosclerosis. Clin Sci. 2020;134(13):1775–1799. doi:10.1042/CS20200446
44. Zhu W, Juan Deng C, Ping Xuan L, et al. Peripheral artery disease and risk of fibrosis deterioration in nonalcoholic fatty liver disease: a prospective investigation. Biomed Environ Sci. 2020;33(4):217–226. doi:10.3967/bes2020.031
45. Ebert T, Widman L, Stenvinkel P, et al. Increased risk for microvascular outcomes in NAFLD-A nationwide, population-based cohort study. J Intern Med. 2023;294(2):216–227. doi:10.1111/joim.13673
46. Megallaa MH, Ismail AA, Zeitoun MH, et al. Association of diabetic foot ulcers with chronic vascular diabetic complications in patients with type 2 diabetes. Diabetes Metab Syndr. 2019;13(2):1287–1292. doi:10.1016/j.dsx.2019.01.048
47. Zhang L, Fu G, Deng Y, et al. Risk factors for foot ulcer recurrence in patients with comorbid diabetic foot osteomyelitis and diabetic nephropathy: a 3-year follow-up study. Int Wound J. 2023;20(1):173–182. doi:10.1111/iwj.13861
48. Awasthi A, Corrie L, Vishwas S, et al. Gut dysbiosis and diabetic foot ulcer: role of probiotics. Pharmaceutics. 2022;14(11):2543. doi:10.3390/pharmaceutics14112543
49. Vita T, Murphy DJ, Osborne MT, et al. Association between non-alcoholic fatty liver disease at CT and coronary microvascular dysfunction at myocardial perfusion PET/CT. Radiology. 2019;291(2):330–337. doi:10.1148/radiol.2019181793
50. Huang X, Han J, Nong Y, et al. Triglyceride-glucose index is strongly associated with all‐cause mortality in elderly females with diabetic foot ulcers: a 9-year follow-up study. Int Wound J. 2024;21(1):e14344. doi:10.1111/iwj.14344
51. Eslam M, Ahmed A, Després J-P, et al. Incorporating fatty liver disease in multidisciplinary care and novel clinical trial designs for patients with metabolic diseases. Lancet Gastroenterol Hepatol. 2021;6(9):743–753. doi:10.1016/S2468-1253(21)00132-1
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.