Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Association Between Maternal Mood Disorders and Schizophrenia and the Risk of Type 1 Diabetes in Offspring: A Nationwide Cohort Study
Authors Liu YC, Liao YT ![]() , Chen VCH, Chen YL
, Chen VCH, Chen YL ![]()
Received 27 August 2023
Accepted for publication 16 November 2023
Published 20 November 2023 Volume 2023:19 Pages 2511—2518
DOI https://doi.org/10.2147/NDT.S437430
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Yi-Chun Liu,1– 4 Yin-To Liao,5,6 Vincent Chin-Hung Chen,7,8,* Yi-Lung Chen3,9,*
1Department of Psychiatry, Changhua Christian Children’s Hospital, Changhua, 500, Taiwan; 2Department of Psychiatry, Changhua Christian Hospital, Changhua, 500, Taiwan; 3Department of Healthcare Administration, Asia University, Taichung, 413, Taiwan; 4Department of Eldercare, Central Taiwan University of Science and Technology, Taichung, Taiwan; 5Department of Psychiatry, China Medical University Hospital, Taichung, 404, Taiwan; 6China Medical University, Taichung, 406, Taiwan; 7School of Medicine, Chang Gung University, Taoyuan, 333, Taiwan; 8Department of Psychiatry, Chiayi Chang Gung Memorial Hospital, Chiayi, 613, Taiwan; 9Department of Psychology, Asia University, Taichung, 413, Taiwan
*These authors contributed equally to this work
Correspondence: Yi-Lung Chen, Department of Healthcare Administration, Asia University, No. 500, Lioufeng Road, Wufeng, Taichung, 41354, Taiwan, Tel +886-4-23323456 (ext. 20106), Fax +886-4-2331669, Email [email protected]
Objective: Our study aimed to determine whether mothers with bipolar disorder, major depressive disorder, schizophrenia, or schizoaffective disorder affected the risk of type 1 diabetes (T1D) in their offspring.
Methods: We conducted a nationwide cohort study by using data from Taiwan’s National Health Insurance Research Database and the Maternal and Child Health Database from 2004 to 2018. A total of 2,556,640 mother-child pairs were identified. Cox proportional hazards models were used to compare the risk of T1D between children born to mothers with mood disorders and schizophrenia and those without.
Results: No significant difference in risk of T1D was observed between the offspring of mothers with major psychiatric disorders and those without (adjusted hazard ratio (aHR) of 0.86 with a 95% confidence interval (CI) of 0.58– 1.24). In subgroup analysis, we found an aHR of 1.81 with a 95% CI of 0.83– 3.82 in the maternal bipolar disorder on the risk of T1D in offspring and an aHR of 0.87 (95% CI: 0.59– 1.25) in maternal major depressive disorder. In the schizophrenia/schizoaffective disorder group, aHR cannot be obtained due to lesser than three events in the analysis.
Conclusion: The risk of T1D in offspring of mothers with mood disorders and schizophrenia was not significant. However, children born to mothers with bipolar disorder may have a tendency to develop T1D. The relationship between maternal psychiatric disorders and the risk of T1D in offspring warrants further investigation in studies with longer follow-up periods.
Keywords: type 1 diabetes mellitus, schizophrenia, major depressive disorder, bipolar disorder
Introduction
Type 1 diabetes mellitus (T1D) is a chronic multifactorial disease with onset in early childhood.1,2 T1D symptoms include hypoglycemia, weight loss, and ketoacidosis, which require continuous treatment and therefore impose a substantial burden on patients’ mental health and quality of life.1,2 Children with T1D are vulnerable to ketoacidosis, which can further impair their cognitive function and school performance.3 Globally, the incidence of T1D is 15 per 100,000 people, with a prevalence of 0.07–0.12%.4 Although pathogenesis of T1D is complex and remains to be elucidated, a widely recognized pathology involves the autoimmune destruction of islet β-cells, such as that caused by the aberrant pro-inflammatory pathway induced by T-helper 17 (Th17) cells.5–7 Due to the young age of T1D onset and lower familial clustering than type 2 diabetes, pathogenesis other than gene should be considered in T1D.8 As known, maternal immune or cytokine changes can be transferred to the fetus through the placenta, thereby affecting fetal development.9–11 Thus, maternal immune related diseases could be important in the cause of T1D.
Major psychiatric disorders, namely schizophrenia, bipolar disorder, and major depressive disorder, have gradually been recognized as disorders of immune and inflammatory dysregulation. Several studies have reported that the Th17 pathway is involved in the pathogenesis of major psychiatric disorders; therefore, this pathway is common in both T1D and major psychiatric disorder pathogenesis.12–17 Few observational studies evaluating the linkage between psychiatric disorders and T1D risks. Two population-based studies have reported a high prevalence of T1D in patients with schizophrenia or schizoaffective disorder.18,19 Another population-based cohort study explored the risk of T1D in patients with schizophrenia, and the results revealed an elevated risk with adjusted hazard ratio (HR) of 2.84 (95% confidence interval (CI): 1.18–6.82).20 Studies on the mood disorders and subsequent T1D risks are scant. A recent Danish nationwide study demonstrated that patients with T1D have an elevated risk of overall psychiatric disorders, including schizophrenia, bipolar disorder, affective disorder, autistic spectrum disorder, and attention deficit/hyperactivity disorder.21 Despite the use of Danish population-based case-cohort sample, the low sample size of T1D limited the further analysis for stratifying by specific psychiatric disorder. The potential causal relationship between major psychiatric disorders and T1D within individual remains unclear.
During pregnancy, maternal immune changes can have a direct effect on the fetal immune system through the placenta and this effect can persist into the newborn.9,22 As above mentioned, major psychiatric disorders and T1D share a common immune-related pathogenesis. Thus, the aberrant Th17 immune changes in mothers with major psychiatric disorders may penetrate the placenta and affect Th17 immune pathway in their offspring.
Mothers with major psychiatric disorders might be prescribed antipsychotic medications during pregnancy and antipsychotic medications can also penetrate the placenta.23 Maternal antipsychotic exposure was found increasing the risk of gestational diabetes (relative risk of 1.30, 95% CI: 1.023–1.660) in a recent systematic review and meta-analysis.24 There is considerable evidence that intrauterine exposure to diabetes, regardless of the maternal diabetes type, was associated with insulin resistance in offspring. However, the insulin resistance was the core pathogenesis of type 2 diabetes, but not of T1D.25 Studies have also shown that antipsychotics are associated with type 2 diabetes,26 but not with T1D. A study by Polcwiartek showed null association between antipsychotic exposure and T1D (odds ratio of 1.38, 95% CI: 0.84–2.29) in the Danish National Patient Register database.27 Briefly, antipsychotic exposure during pregnancy or gestational diabetes related to antipsychotics did not seem to affect the risk of T1D in offspring. Therefore, our study examined the risk of T1D in the offspring related to maternal major psychiatric disorders, regardless of maternal antipsychotic exposure during pregnancy.
In our review, no studies investigated maternal major psychiatric disorders and their impact on the risk of T1D in offspring. Besides, reverse causality is difficult to avoid in the general population-based cohort study due to the delay of the diagnosis of psychiatric disorders. Mother–infant dyad study can potentially help prevent this reverse causation. Thus, we conducted a nationwide mother–infant dyad study to investigate the association between maternal major psychiatric disorder and the risk of T1D in offspring.
Methods
Data Source
Taiwan’s single-payer National Health Insurance (NHI) program was launched on March 1, 1995. The program had enrolled 99.9% of the Taiwan population, according to the official statement in December 2021. Our study used deidentified insurance claim information from the NHI Research Database (NHIRD) between January 1, 2004, and December 31, 2018. We included data on inpatient and outpatient ambulatory services, drug prescriptions, prescription time, and diagnosis codes. We linked the NHIRD data with data from the Taiwan Birth Certificate Registration from January 1, 2004, to December 31, 2017. This registration database provided confirmation of data on live birth, birth date, and gestational age. The linkages between the data sets were utilized to explore the association between maternal major psychiatric disorders and the risk of T1D in offspring. We also retrieved data from the Taiwan Maternal and Child Health Database to obtain complete information on offspring, fathers, and biological mothers from 2004 to 2017.28
The NHIRD processed and stored all medical claims as anonymous and encrypted dataset. The data are de-identified and cannot be accessed without proper application for research purposes. To secure the privacy further, the NHIRD database is only accessible inside a single location, the Data Science Centre, and the raw data are not allowed to be transferred to any portable storage device. This study was approved by the Research Ethics Committee of the Chang Gung Medical Foundation (IRB number: 202000880B0). There was no informed consent required because the dataset was de-identified and anonymous.
Inclusion Criteria for the Study Population and Controls
We included mothers with major psychiatric disorders diagnosed before gestation.29 The disorders were defined as schizophrenia, schizoaffective disorder, bipolar disorder and major depressive disorder (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] codes 295.*296.00, 296.01–06, 296.10–16, 296.81, 296.40–46, 296.50–56, 296.60–62, 296.20–26, and 296.30–36* and ICD-10 codes F20.*F25.*F30.*F31.*F32.*and F33.*). The diagnoses were ascertained by at least having two times outpatient or one-time inpatient diagnosis.30–32 We included mothers without major psychiatric disorder before pregnancy as controls.
Outcome Measures
Data on children born to mothers with and without major psychiatric disorders were collected and followed up from birth to December 31, 2018, or death. The primary outcomes were index diagnoses of T1D, which was defined as at least one inpatient or one outpatient diagnosis (ICD-9-CM codes 250.01, 250.03, 250.11, 250.13, 250.21, 250.23, 250.31, 250.33, 250.41, 250.43, 250.51, 250.53, 250.61, 250.63, 250.71, 250.73, 250.81, 250.83, 250.91, and 250.93 and ICD-10 code E10 at any age or E13 before the age of 10 years).33,34
Covariates
We included offspring’s sex, age, and birth weight, T1D in the father or mother, maternal age, gestational age, enterovirus and cytomegalovirus infection during pregnancy, and maternal smoking status as covariates related to T1D, as described in studies and reviews.34–36
Statistical Analysis
We used descriptive analyses to compare the baseline characteristics of the study population, that is, children born to mothers with major psychiatric disorders and those born to mothers without major psychiatric disorders. We also examined the characteristics of children born to mothers with schizophrenia, bipolar disorder, and major depressive disorder individually. The Cox proportional hazard model was applied to estimate the adjusted hazard ratios (aHR) and their 95% confidence intervals for the risk of T1D between children born to mothers with major psychiatric disorders and those born to mothers without any psychiatric disorders. We used child age as the timescale. We also adjusted delivery mode, birth weight, gestational age, maternal viral infection (enterovirus and cytomegalovirus infection), maternal and paternal age at childbirth, maternal thyroid disease history, maternal smoking during pregnancy, and parental history of T1D. Considering the correlation between the outcomes of different children from the same mother, we applied the robust estimation in our Cox proportional hazard model.
In the subgroup analyses, we categorized the exposure cohort on the basis of three different major psychiatric disorders and repeated the analyses. Because the same mother may have more than two major mental illnesses, the three classifications of the mother group in our study are not mutually exclusive. All statistical analyses and processing were performed using the Statistical Analysis Software (SAS) version 9.4.
Results
Characteristics of Children Born to Mothers with or without Major Psychiatric Disorders
There were 2,556,640 mother-child pairings and a total of 76,239 children were born to mothers with major psychiatric disorders, of whom 8322 were classified in the bipolar disorder group, 4014 in the schizophrenia/schizoaffective disorder group, and 71,170 in the major depressive disorder group (Table 1). The total number of distinct or unduplicated mothers and fathers was 1,695,832 and 1,694,879, respectively. The control group included 2,480,401 children whose mothers had never been diagnosed with any psychiatric disorder (Table 1). Approximately 52% of the children in the exposure and control groups were boys. The mean age with standard deviation (SD) was 7.1 ± 3.8 and 8.1 ± 4.1 years for the exposure and control groups, respectively (Table 1). In the exposure group, the age at T1D diagnosis was less than that of the control group, with a mean age and SD of 5.8 ± 3.5 and 6.5 ± 3.5 years, respectively (Table 1). No difference in the incidence of T1D was observed between the exposure and control groups, with the incidence being approximately 0.04%–0.05%; however, a higher incidence of 0.1% was observed in the subgroup of bipolar disorder (Table 1).
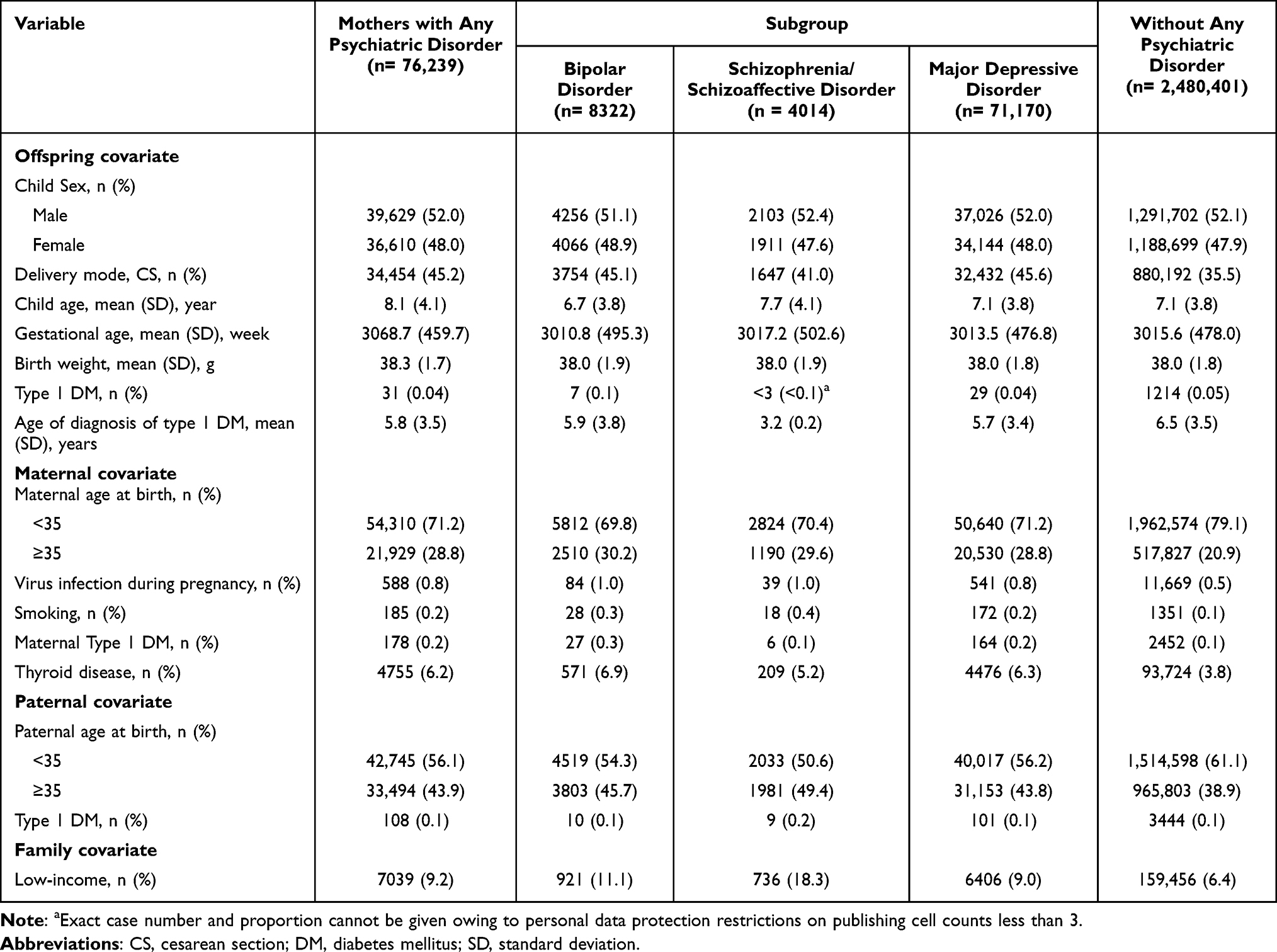 |
Table 1 Characteristics of Mothers with or without Psychiatric Disorders and Their Offspring |
Association Between Maternal Major Psychiatric Disorders and the Risk of T1D in Offspring
In the Cox proportional hazard model adjusted for the mode of delivery of the child, birth weight, gestational age, maternal viral infection, maternal and paternal age in childbirth, maternal thyroid disease history, maternal smoking during pregnancy, and parental history of T1D, there was no significant risk (aHR = 0.86 with 95% CI of 0.58–1.24) of developing T1D in offspring with maternal major psychiatric disorders compared to controls (Table 2). In the subgroup analysis, the major depressive disorder group had an aHR of 0.87 (95% CI: 0.59–1.25). The bipolar disorder group had an aHR of 1.81 (95% CI: 0.83–3.82). Both presented with a broader 95% CI covering a null value of 1 due to the rarity of T1D events (prevalence of 0.05%). In the schizophrenia/schizoaffective disorder group, less than three T1D cases were identified and therefore we could not obtain reliable HR estimates in the adjusted Cox proportional-hazards model.
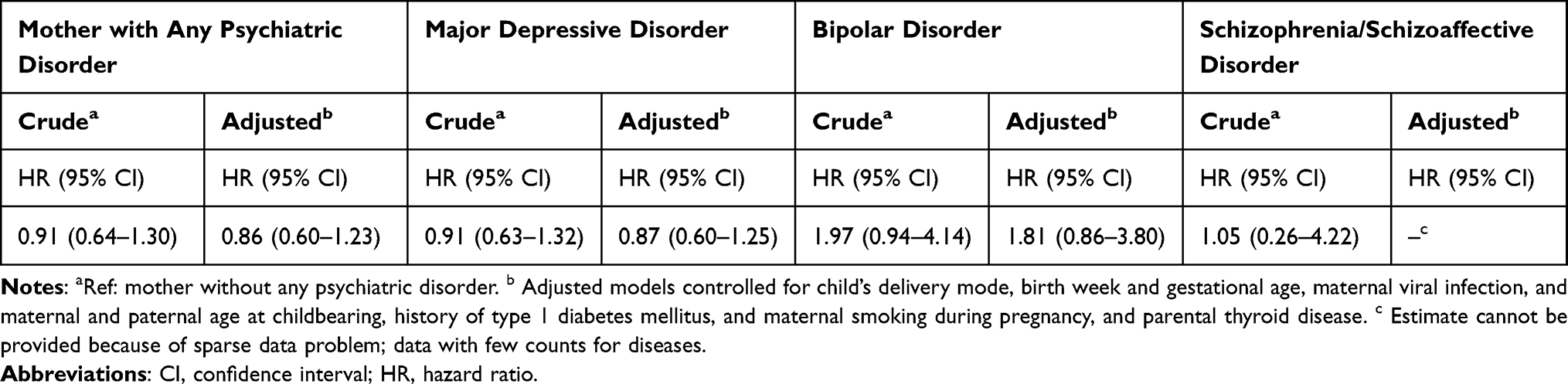 |
Table 2 Baseline and Adjusted Associations Between Maternal Psychiatric Disorder and Type 1 Diabetes Mellitus Outcomes in Offspring |
Discussion
To the best of our knowledge, this study is the first to examine the risk of T1D in children born to mothers with major psychiatric disorders. We observed no significant associations between different maternal major psychiatric disorders and the risk of T1D in offspring. In subgroup analysis, the point estimate of HR of T1D in children born to mothers with bipolar disorder was clinically meaningful (aHR: 1.81), although not statistically significant. The relatively low prevalence of T1D (ie, 0.05%) in our study population and the low fertility rate in mother with bipolar disorders may result in a wide CI and statistically insignificant association between maternal bipolar disorder and the risk of T1D in offspring.1,3,37,38 On the other hand, no association was observed between maternal major depressive disorder and the risk of T1D in offspring. It was difficult to estimate whether the risk of T1D in offspring was associated with the presence of schizophrenia/schizoaffective disorder in the mother because of the rare event of T1D and the limited sample size of this subgroup.
To our knowledge, only a few studies have investigated the association between bipolar disorder and T1D. Cremaschi et al examined the prevalence of T1D in patients with bipolar disorder by using the case–control study design in Sweden.39 Their study indicated no difference in the prevalence of T1D between the bipolar disorder and control groups. As mentioned above, we used the mother-child cohort database to avoid reverse causality. Besides, recall bias and lack of adjustment for crucial confounders could have interfered with the results. Their study first identified patients with bipolar disorder from a previous genetic study and contacted them to collect information on T1D. The accuracy of the T1D diagnosis may be thus limited by recall bias and was not confirmed by any physician or laboratory tests. In addition, some crucial confounding factors (eg, gestational week, birth weight, and family history of T1D) were not adjusted for. Another population-based cohort study by Silva et al reported that maternal T1D was not associated with mood disorders in offspring in either an unadjusted or adjusted model.40 However, the use of less precise bipolar diagnoses, such as the mood disorder, can lead to biased results. As known, depression accounts for a large proportion of mood disorders.41,42 Moreover, the directionality of their research purpose is different from our research. To fill a gap in knowledge about maternal mood disorders and the risk of T1D in offspring, we conducted a unique mother–infant dyad study to examine the potential causal relationship between bipolar disorder, major depression and T1D in our study.
In contrast, some studies with within-individual association study design, that is, the association between the occurrence of the two disorders during a person’s lifetime, have reported high co-occurrence of T1D and depression.43–45 As known, people with T1D often suffer great emotional stress from enduring chronic illness, which may be one of the important factors leading to depression.46 Previous within-individual studies reflected the possible association between two disorders, which is often best explained by stress diathesis model. The null association between major depressive disorder and T1D from our results is explained by the different study design. It was not our aim to explore whether emotional stress caused by chronic medical illness could lead to mental illness within individual.
Based on the rare event of the outcome, the point estimate of HR for T1D in children with maternal bipolar disorder was relatively meaningful. Some studies revealed association between bipolar disorder, cognitive impairment, rapid cycling course and insulin-related problems.47 In our study, the results suggested that children born to mothers with bipolar disorder may have a tendency to develop T1D, which may be explained by some common immune-related pathogenic mechanisms between T1D and major psychiatric disorders.5–7,16,17 For example, Th17-mediated inflammation has been observed in major psychiatric disorders.13,48–52 In stressful environments, IL-17 can cause or accelerate the breakdown of the blood–brain barrier, infiltrate the central nervous system, and cause neuroinflammation.9 Also, Th17 cells are detected in the placenta, endometrial layer, and maternal peripheral blood during pregnancy and play an essential role in placenta formation and pregnancy maintenance.10 Therefore, apart from genetic factors, mothers with major psychiatric disorders may have an impact on the fetal immune system through the placenta during pregnancy. On the other hand, Th17 or its surrogate marker IL-17 is highly associated with insulitis.6,53 The pathogenesis of T1D is characterized by an autoimmune attack on pancreatic islets, which in turn causes insulitis and destroys insulin secretion.1,2 Our findings, however, did not find significant association between major psychiatric disorders and the risk of T1D. In addition to the rarity of the outcome in our study population, another possible explanation is that the high heterogeneity of mood disorder diagnoses also limits the investigation of exact associations.54
Our study has some limitations. First, too few mothers (n = 4014) with schizophrenia and offspring with T1D (n < 3) were identified in the NHIRD; therefore, an analysis could not be performed. Given the low marriage rate of women with schizophrenia and the low birth rate of them, it is understandable that very few mothers with schizophrenia were included despite the use of a nationwide population database.55 The peaks in T1D onset were 5 to 7 years old and near puberty, that is age 10 to 14 for girls and 12 to 16 for boys.56 The follow-up duration was 13 years and might not include the T1D patients with their onset near puberty. Underestimation of T1D incidence and results toward null were possible. The future long-term studies may address data scarcity. Second, according to the medical claim database, the diagnoses of major psychiatric disorders and T1D were performed by board-certified psychiatrists and pediatricians. However, because of the nature of the medical claim data, only patients who seek medical help are identified in the NHIRD. Some psychiatric disorders, such as schizophrenia, patients often did not seek help due to stigmatization, lack of insight, poverty, or being homeless.57,58 Such misclassification may lead to an underestimation of the association between maternal psychiatric disorders and risk of T1D in offspring. In addition, some crucial covariates, such as maternal disease severity, living environment, and stress, cannot be identified in our national databases. Further studies are warranted to examine the effect of these covariates on the risk of T1D in children.
Conclusion
We did not find an association between maternal major psychiatric disorders and the risk of T1D in offspring. Further biological studies or cohort studies with longer follow-up time may be needed to examine the association.
Ethics Approval
This study was approved by the Research Ethics Committee of the Chang Gung Medical Foundation (IRB number: 202000880B0).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no financial or non-financial conflicts of interests for this work.
References
1. Lu CL, Shen HN, Chen HF, Li CY. Epidemiology of childhood Type 1 diabetes in Taiwan, 2003 to 2008. Diabet Med. 2014;31(6):666–673. doi:10.1111/dme.12407
2. Lin SY, Lin CL, Lin CC, Hsu WH, Hsu CY, Kao CH. Risk of Urticaria in Children with Type 1 Diabetes Mellitus: a Nationwide Cohort Study. Int J Environ Res Public Health. 2019;17(1):176. doi:10.3390/ijerph17010176
3. Patterson CC, Karuranga S, Salpea P, et al. Worldwide estimates of incidence, prevalence and mortality of type 1 diabetes in children and adolescents: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Research and Clinical Practice. 2019;157:107842. doi:10.1016/j.diabres.2019.107842
4. Mobasseri M, Shirmohammadi M, Amiri T, Vahed N, Hosseini Fard H, Ghojazadeh M. Prevalence and incidence of type 1 diabetes in the world: a systematic review and meta-analysis. Health Promot Perspect. 2020;10(2):98–115. doi:10.34172/hpp.2020.18
5. Grieco FA, Moore F, Vigneron F, et al. IL-17A increases the expression of proinflammatory chemokines in human pancreatic islets. Diabetologia. 2014;57(3):502–511. doi:10.1007/s00125-013-3135-2
6. Arif S, Moore F, Marks K, et al. Peripheral and islet interleukin-17 pathway activation characterizes human autoimmune diabetes and promotes cytokine-mediated beta-cell death. Diabetes. 2011;60(8):2112–2119. doi:10.2337/db10-1643
7. Honkanen J, Nieminen JK, Gao R, et al. IL-17 immunity in human type 1 diabetes. J Immunol. 2010;185(3):1959–1967. doi:10.4049/jimmunol.1000788
8. Hari Kumar KV, Modi KD. Twins and endocrinology. Indian j Endocrinol Metab. 2014;18(Suppl 1):48. doi:10.4103/2230-8210.145074
9. PrabhuDas M, Bonney E, Caron K, et al. Immune mechanisms at the maternal-fetal interface: perspectives and challenges. Nat Immunol Apr. 2015;16(4):328–334. doi:10.1038/ni.3131
10. Chucri TM, Monteiro JM, Lima AR, Salvadori ML, Kfoury JR Jr, Miglino MA. A review of immune transfer by the placenta. J Reprod Immunol. 2010;87(1–2):14–20. doi:10.1016/j.jri.2010.08.062
11. Yockey LJ, Iwasaki A. Interferons and Proinflammatory Cytokines in Pregnancy and Fetal Development. Immunity. 2018;49(3):397–412. doi:10.1016/j.immuni.2018.07.017
12. Cui M, Dai W, Kong J, Chen H. Th17 Cells in Depression: are They Crucial for the Antidepressant Effect of Ketamine? Front Pharmacol. 2021;12:649144. doi:10.3389/fphar.2021.649144
13. Niu Z, Yang L, Wu X, Zhu Y, Chen J, Fang Y. The Relationship Between Neuroimmunity and Bipolar Disorder: mechanism and Translational Application. Neurosci Bull. 2019;35(4):595–607. doi:10.1007/s12264-019-00403-7
14. Debnath M, Berk M. Th17 Pathway-Mediated Immunopathogenesis of Schizophrenia: mechanisms and Implications. Schizophrenia Bulletin. 2014;40(6):1412–1421. doi:10.1093/schbul/sbu049
15. Abdel-Moneim A, Bakery HH, Allam G. The potential pathogenic role of IL-17/Th17 cells in both type 1 and type 2 diabetes mellitus. Biomed Pharmacother. 2018;101:287–292. doi:10.1016/j.biopha.2018.02.103
16. Bradshaw EM, Raddassi K, Elyaman W, et al. Monocytes from patients with type 1 diabetes spontaneously secrete proinflammatory cytokines inducing Th17 cells. J Immunol. 2009;183(7):4432–4439. doi:10.4049/jimmunol.0900576
17. Emamaullee JA, Davis J, Merani S, et al. Inhibition of Th17 cells regulates autoimmune diabetes in NOD mice. Diabetes. 2009;58(6):1302–1311. doi:10.2337/db08-1113
18. Eaton WW, Byrne M, Ewald H, et al. Association of schizophrenia and autoimmune diseases: linkage of Danish national registers. Am J Psychiatry. 2006;163(3):521–528. doi:10.1176/appi.ajp.163.3.521
19. Chen SJ, Chao YL, Chen CY, et al. Prevalence of autoimmune diseases in in-patients with schizophrenia: nationwide population-based study. Br J Psychiatry. 2012;200(5):374–380. doi:10.1192/bjp.bp.111.092098
20. Melkersson K. Schizophrenia- or schizoaffective disorder diagnosis and the risk for subsequent type 1- or type 2 diabetes mellitus: a Swedish nationwide register-based cohort study. Neuro Endocrinol Lett. 2020;41(5):245–254.
21. Chen MH, Tsai SJ, Bai YM, et al. Type 1 diabetes mellitus and risks of major psychiatric disorders: a nationwide population-based cohort study. Diabetes Metab. 2022;48(1):101319. doi:10.1016/j.diabet.2022.101319
22. Jennewein MF, Abu-Raya B, Jiang Y, Alter G, Marchant A. Transfer of maternal immunity and programming of the newborn immune system. Semin Immunopathol. 2017;39(6):605–613. doi:10.1007/s00281-017-0653-x
23. Tosato S, Albert U, Tomassi S, et al. A Systematized Review of Atypical Antipsychotics in Pregnant Women: balancing Between Risks of Untreated Illness and Risks of Drug-Related Adverse Effects. J Clin Psychiatry. 2017;78(5):e477–e489. doi:10.4088/JCP.15r10483
24. Kucukgoncu S, Guloksuz S, Celik K, et al. Antipsychotic Exposure in Pregnancy and the Risk of Gestational Diabetes: a Systematic Review and Meta-analysis. Schizophr Bull. 2020;46(2):311–318. doi:10.1093/schbul/sbz058
25. Dabelea D. The predisposition to obesity and diabetes in offspring of diabetic mothers. Diabetes Care. 2007;30(Suppl 2):S169–174. doi:10.2337/dc07-s211
26. Stubbs B, Vancampfort D, De Hert M, Mitchell AJ. The prevalence and predictors of type two diabetes mellitus in people with schizophrenia: a systematic review and comparative meta-analysis. Acta Psychiatr Scand. 2015;132(2):144–157. doi:10.1111/acps.12439
27. Polcwiartek C, Kragholm K, Rohde C, Hashemi N, Vang T, Nielsen J. Diabetic ketoacidosis and diabetes associated with antipsychotic exposure among a previously diabetes-naive population with schizophrenia: a nationwide nested case-control study. Diabetologia. 2017;60(9):1678–1690. doi:10.1007/s00125-017-4320-5
28. Liu YC, Chen VC, Liao YT, Chen YL. Association of Prenatal Maternal Anemia with Tics and Tourette’s Syndrome in Offspring. J Pers Med. 2021;11(10):1038. doi:10.3390/jpm11101038
29. Chen LC, Chen MH, Hsu JW, et al. Association of parental depression with offspring attention deficit hyperactivity disorder and autism spectrum disorder: a nationwide birth cohort study. b. 2020;277:109–114. doi:10.1016/j.jad.2020.07.059
30. Ma KS, Wu MC, Thota E, Wang YH, Alqaderi HE, Wei JC. Tonsillectomy as a risk factor of periodontitis: a population-based cohort study. J Periodontol. 2022;93(5):721–731. doi:10.1002/JPER.21-0215
31. Kim D, Yang PS, Yu HT, et al. Risk of dementia in stroke-free patients diagnosed with atrial fibrillation: data from a population-based cohort. Eur Heart J. 2019;40(28):2313–2323. doi:10.1093/eurheartj/ehz386
32. Hou HA, Tang CH, Goh CH, et al. A population-based cohort study of the epidemiology of light-chain amyloidosis in Taiwan. Sci Rep. 2022;12(1):15736. doi:10.1038/s41598-022-18990-3
33. Dabelea D, Bell RA, D’Agostino RB Jr, et al. Incidence of diabetes in youth in the United States. JAMA. 2007;297(24):2716–2724. doi:10.1001/jama.297.24.2716
34. Cardwell CR, Stene LC, Joner G, et al. Birthweight and the risk of childhood-onset type 1 diabetes: a meta-analysis of observational studies using individual patient data. Diabetologia. 2010;53(4):641–651. doi:10.1007/s00125-009-1648-5
35. Pociot F, Lernmark A. Genetic risk factors for type 1 diabetes. Lancet. 2016;387(10035):2331–2339. doi:10.1016/S0140-6736(16)30582-7
36. Allen DW, Kim KW, Rawlinson WD, Craig ME. Maternal virus infections in pregnancy and type 1 diabetes in their offspring: systematic review and meta-analysis of observational studies. Rev Med Virol. 2018;28(3):e1974. doi:10.1002/rmv.1974
37. Williams KE, Marsh WK, Rasgon NL. Mood disorders and fertility in women: a critical review of the literature and implications for future research. Hum Reprod Update. 2007;13(6):607–616. doi:10.1093/humupd/dmm019
38. Grover S, Sahoo S, Chaudhary S, Chakrabarti S, Nehra R, Avasthi A. Gender differences, family size and fertility rate among patients with bipolar disorder: a study from India. Psychiatry Res. 2019;272:562–568. doi:10.1016/j.psychres.2018.12.156
39. Cremaschi L, Kardell M, Johansson V, et al. Prevalences of autoimmune diseases in schizophrenia, bipolar I and II disorder, and controls. Psychiatry Res. 2017;258:9–14. doi:10.1016/j.psychres.2017.09.071
40. Nogueira Avelar ESR, Yu Y, Liew Z, Vested A, Sorensen HT, Li J. Associations of Maternal Diabetes During Pregnancy With Psychiatric Disorders in Offspring During the First 4 Decades of Life in a Population-Based Danish Birth Cohort. JAMA Netw Open. 2021;4(10):e2128005. doi:10.1001/jamanetworkopen.2021.28005
41. Clemente AS, Diniz BS, Nicolato R, et al. Bipolar disorder prevalence: a systematic review and meta-analysis of the literature. Braz J Psychiatry. 2015;37(2):155–161. doi:10.1590/1516-4446-2012-1693
42. Kessler RC, Bromet EJ. The epidemiology of depression across cultures. Annu Rev Public Health. 2013;34:119–138. doi:10.1146/annurev-publhealth-031912-114409
43. Akbarizadeh M, Naderi Far M, Ghaljaei F. Prevalence of depression and anxiety among children with type 1 and type 2 diabetes: a systematic review and meta-analysis. World J Pediatr. 2022;18(1):16–26. doi:10.1007/s12519-021-00485-2
44. Buchberger B, Huppertz H, Krabbe L, Lux B, Mattivi JT, Siafarikas A. Symptoms of depression and anxiety in youth with type 1 diabetes: a systematic review and meta-analysis. Psychoneuroendocrinology. 2016;70:70–84. doi:10.1016/j.psyneuen.2016.04.019
45. Roy T, Lloyd CE. Epidemiology of depression and diabetes: a systematic review. b. 2012;142(Suppl):S8–21. doi:10.1016/S0165-0327(12)70004-6
46. Fisher L, Hessler DM, Polonsky WH, et al. Prevalence of depression in Type 1 diabetes and the problem of over-diagnosis. Diabet Med. 2016;33(11):1590–1597. doi:10.1111/dme.12973
47. Miola A, Alvarez-Villalobos NA, Ruiz-Hernandez FG, et al. Insulin resistance in bipolar disorder: a systematic review of illness course and clinical correlates. J Affect Disord. 2023;334:1–11. doi:10.1016/j.jad.2023.04.068
48. Varun CN, Venkataswamy MM, Ravikumar R, et al. Th17 and MAIT cell mediated inflammation in antipsychotic free schizophrenia patients. Schizophrenia Res. 2019;212:47–53. doi:10.1016/j.schres.2019.08.013
49. Beurel E, Lowell JA. Th17 cells in depression. Brain Behav Immun. 2018;69:28–34. doi:10.1016/j.bbi.2017.08.001
50. El Kissi Y, Samoud S, Mtiraoui A, et al. Increased Interleukin-17 and decreased BAFF serum levels in drug-free acute schizophrenia. Psychiatry Res. 2015;225(1–2):58–63. doi:10.1016/j.psychres.2014.10.007
51. Ding M, Song X, Zhao J, et al. Activation of Th17 cells in drug naive, first episode schizophrenia. Prog Neuro Psychopharmacol Biol Psychiatry. 2014;51:78–82. doi:10.1016/j.pnpbp.2014.01.001
52. Waisman A, Hauptmann J, Regen T. The role of IL-17 in CNS diseases. Acta Neuropathol. 2015;129(5):625–637. doi:10.1007/s00401-015-1402-7
53. Martin-Orozco N, Chung Y, Chang SH, Wang YH, Dong C. Th17 cells promote pancreatic inflammation but only induce diabetes efficiently in lymphopenic hosts after conversion into Th1 cells. Eur J Immunol. 2009;39(1):216–224. doi:10.1002/eji.200838475
54. Lynch CJ, Gunning FM, Liston C. Causes and Consequences of Diagnostic Heterogeneity in Depression: paths to Discovering Novel Biological Depression Subtypes. Biol. Psychiatry. 2020;88(1):83–94. doi:10.1016/j.biopsych.2020.01.012
55. Thara R, Kamath S. Women and schizophrenia. Indian Journal of Psychiatry. 2015;57(Suppl 2):246. doi:10.4103/0019-5545.161487
56. Atkinson MA, Eisenbarth GS, Michels AW. Type 1 diabetes. Lancet. 2014;383(9911):69–82. doi:10.1016/S0140-6736(13)60591-7
57. Cohen CI. Poverty and the course of schizophrenia: implications for research and policy. Hosp Community Psychiatry. 1993;44(10):951–958. doi:10.1176/ps.44.10.951
58. Ayano G, Tesfaw G, Shumet S. The prevalence of schizophrenia and other psychotic disorders among homeless people: a systematic review and meta-analysis. BMC Psychiatry. 2019;19(1):370. doi:10.1186/s12888-019-2361-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.