Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Association Between Interleukin-6 Gene Polymorphism and Severity of Coronary Artery Disease in Patients with Diabetes
Authors Yao H ![]() , Pang Y, Chen Y, Si N, Wu C, Wang Z, Ren Y
, Pang Y, Chen Y, Si N, Wu C, Wang Z, Ren Y ![]()
Received 27 June 2023
Accepted for publication 15 October 2023
Published 9 November 2023 Volume 2023:16 Pages 3599—3608
DOI https://doi.org/10.2147/DMSO.S427873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Hongmei Yao,1 Yongqiang Pang,2 Yubin Chen,2 Nilu Si,2 Chao Wu,2 Zijing Wang,2 Yi Ren3
1Department of Cardiology, the First Hospital of Shanxi Medical University, TaiYuan City, 030001, People’s Republic of China; 2Department of Internal Medicine, Shanxi Medical University, TaiYuan City, 030001, People’s Republic of China; 3Department of Endocrinology, the First Hospital of Shanxi Medical University, TaiYuan City, 030001, People’s Republic of China
Correspondence: Yi Ren, Department of Endocrinology, the First Hospital of Shanxi Medical University, No. 85, Jiefang South Road, Yingze District, TaiYuan City, 030001, People’s Republic of China, Tel +86-351-4639756, Email [email protected]
Introduction: Previous studies have identified diabetes as a risk factor for coronary heart disease. This study determined the correlation between the IL-6 gene − 572 G/C polymorphism and the incidence and severity of coronary heart disease in patients with diabetes.
Methods: One hundred four patients with diabetes who were admitted to our hospital from January 2019 to December 2020 were retrospectively enrolled in the current study. These patients were divided into a diabetes only group (group A, 27 patients) and a diabetes complicated by coronary heart disease group (group B, 77 patients). Seventy patients in the latter group were further divided into low, medium, and high Syntax score groups based on coronary angiography results. A correlation analysis between IL-6, blood lipids, and the IL-6 − 572 G/C gene levels was performed.
Results: The serum IL-6 level in patients with the IL-6-572G/C-GG genotype was higher than patients with the GC and CC genotypes. In patients with diabetes, the presence of the IL-6-572G/C-GG and GC genotypes was associated with a significantly increased risk of developing coronary heart disease. Patients with the IL-6-572G/C-GG genotype and diabetes were shown to have more severe coronary artery lesions compared to patients with the CC genotype. Moreover, the G allele of the IL-6-572G/C gene was linked to a higher risk of coronary heart disease and more severe coronary artery lesions in patients with diabetes compared to the C allele.
Conclusion: The IL-6-572G/C gene polymorphism is associated with the incidence and severity of coronary heart disease in patients with diabetes.
Keywords: IL-6, diabetes, coronary heart disease, gene polymorphism, coronary artery lesions
Two Letters to the Editor have been received and published for this article
Introduction
Coronary heart disease (CHD) is a significant threat to human health. Epidemiologic surveys, disease monitoring, and mortality statistics have shown that in the next 20 years the incidence and mortality of CHD will continue to rise worldwide.1
Although previous studies have identified multiple CHD risk factors, approximately 50% of patients with CHD cannot be explained based on known risk factors alone, and primary and secondary prevention trials can only benefit some individuals.2 When the medical history of diabetes, blood glucose control level, and other risk factors are similar, even among patients with diabetes, only a portion of the patients develop CHD, and this group of diabetic patients with concurrent CHD often has diffuse coronary artery disease with severe stenosis.2 The notion that CHD is a complex multi-gene genetic disease has been increasingly accepted, which has opened new avenues for the complete treatment of CHD from a molecular level. The basic pathologic change among patients with CHD is atherosclerosis (AS), which is an inflammatory lesion. Chronic inflammation is involved in and runs through all stages of AS, from the infiltration of cells into the arterial intima to the increased fragility of the plaque fibrous cap, ultimately leading to rupture of the plaque and acute coronary syndrome.3 Inflammation has a crucial role in the occurrence and development of coronary artery disease (CAD). Tumor necrosis factor, interleukins, adhesion molecules, growth factors, and other inflammatory factors produced locally in the vascular wall promote the occurrence of AS through a complex inflammatory factor network, thereby accelerating the occurrence and development of CHD.4 Genetic polymorphisms that affect the production of inflammatory factors or the degree to which inflammatory cells respond to inflammatory stimuli can affect the occurrence of AS and CHD.5 Therefore, studying the impact of inflammatory factor gene polymorphisms on CHD is of great significance.
IL-6 is a multifunctional cytokine belonging to the interleukin family with a molecular weight of 26 kDa. IL-6 has a vital role in the activation of leukocytes and endothelial cells.6,7 The human IL-6 gene, located in chromosome 7p15-21, is approximately 5kb long and has 5 exons and 4 introns. The main causes of polymorphism are promoter regions −597, −572, and −174. These polymorphisms affect the quantity of IL-6 in the body and may be associated with the development of a variety of diseases. Some studies abroad have shown that there is a correlation between the IL-6 gene polymorphism and CHD. IL-6 is an important local and circulating marker of coronary artery plaque inflammation events, and has a more important role than C-reactive protein in the occurrence of CHD. The IL-6 gene is one of the important candidate genes for the onset of CHD.8 The level of IL-6 in the circulation can be used to predict the survival rate of patients with unstable angina and to identify the population that benefits from coronary intervention therapy.9 The IL-6 174G/C mutation and IL-6 plasma levels can be used to predict CHD in first-degree healthy relatives of CHD patients. There have also been reports on the correlation between diabetes and IL-6 gene polymorphisms.10 Prolonged exposure to high levels of glucose in the blood (chronic hyperglycemia) leads to several metabolic and structural changes in the body. These changes include the production of advanced glycation end products, abnormal activation of signaling pathways, such as protein kinase C, increased production of reactive oxygen species, and abnormal stimulation of hemodynamics through the renin-angiotensin system.11 These alterations have detrimental effects on various organs and systems, leading to the development and progression of several chronic diseases, including cardiovascular disease, diabetes, and diabetic complications. As an inflammatory agent, IL-6 is tightly linked to endocrine function, and IL-6 levels are abnormally increased in patients with type 2 diabetes and insulin resistance. Experiments have shown that IL-6, in conjunction with other inflammatory cytokines, causes apoptosis in pancreatic islets and functions as a predictor and pathogenic marker for the course of type 2 diabetes mellitus.12
As a result, experts believe that higher IL-6 levels may relate to the establishment of type 2 diabetes.13 The rs1800795 GC gene polymorphism, which is located in the 572 G/C gene locus promoter of the type 2 diabetes gene in the Chinese population, is strongly associated with the severity of type 2 diabetes and diabetic nephropathy. Additionally, individuals with rs1800795 GC and rs1800796 GG IL-6 genotypes may have a higher risk for proliferative diabetic retinopathy among type 2 diabetes patients. Furthermore, these genotypes are linked to increased expression of IL-6 at the mRNA and protein levels.14 The role of the inflammatory response in the development of type 2 diabetes complications has been confirmed at the genetic level;14–18 however, there is inconsistency among studies with respect to the association between IL-6 gene polymorphisms and CHD, as well as diabetes complications.16–18 Furthermore, no studies have focused on the link between type 2 diabetes patients with co-existing CHD and the IL-6 gene-572 G/C gene polymorphism.
In the current study we determined the relationship between type 2 diabetes patients with co-existing CHD and the IL-6 gene-572 G/C gene polymorphism, as well as the connection with the severity of CAD. This study will contribute new scientific knowledge for the prevention and personalized management of type 2 diabetes complicated by CHD.
Materials and Methods
Research Subjects
This retrospective study selected 104 patients who were diagnosed with diabetes and admitted to our hospital from January 2019 to December 2020. Baseline variables, including age, gender, cigarette smoking history, alcohol consumption history, body mass index, family history of CHD, history of diabetes, and blood glucose control, were analyzed. The exclusion criteria included patients with infectious and non-infectious inflammatory diseases, severe heart failure (New York Heart Association functional class III or higher),19 severe arrhythmias, acute myocardial infarction, abnormal liver function (chronic liver disease [such as cirrhosis] or biochemical evidence of a liver disorder [such as a bilirubin level > 2 times the upper limit of normal combined with alanine aminotransferase/aspartate aminotransferase/alkaline phosphatase levels > 3 times the upper limit of normal]), abnormal kidney function (long-term dialysis, kidney transplantation, or a serum creatinine level ≥ 200 μmol/L), tumors, and hematologic diseases.
The study protocol was approved from the institutional Ethical Review Committee of the First Hospital of Shanxi Medical University. The entire study was conducted in compliance with the Helsinki Declaration. Written informed consent forms were waived by the Ethical Review Committee because this was a retrospective study. Oral informed consent was confirmed by the participants. The study complies with patient data confidentiality, and the patients are in anonymity data in this study, the patient data are protected and will not be used for any other purpose.
Study Groups
The enrolled diabetes patients were split into two groups based on clinical data and coronary angiography results according to the diagnostic criteria for ischemic heart disease developed by the International Society of Cardiology and the World Health Organization,20,21 as follows: diabetes group (group A, 27 patients); and diabetes with CHD group (group B, 77 patients). The severity of coronary artery stenosis was further evaluated for 70 of the 77 patients in the diabetes with CHD group using the Syntax score, which was calculated based on the coronary angiography results (the other 7 patients were diagnosed with CHD based on clinical information and did not undergo coronary angiography) according to the 2014 European Society of Cardiology/European Association of Cardio-Thoracic Surgery myocardial revascularization recommendations.22 All lesions with a lumen diameter of 1.5mm and a stenosis of 50% were considered for calculating the Syntax score. The Syntax score23 was independently calculated by two experienced interventional cardiologists who were unaware of the study protocol and patient characteristics when reviewing all selected patient coronary angiography images. When the results of the two cardiologists were inconsistent, another senior physician was consulted to reach a consensus through discussion among the three cardiologists. Based on the Syntax score, group B was further divided into a low-score group (Syntax score = 0–22 [n=44]), a medium-score group (Syntax score = 23–32 [n=15]), and a high-score group (Syntax score ≥33 [n=11]).
Testing Indicators
Upon admission the morning following a fast, the IL-6, glycated hemoglobin (HbA1c), total cholesterol (TC), triglycerides (TG), low-density lipoprotein-cholesterol (LDL-C), and high-density lipoprotein-cholesterol (HDL-C) levels were measured in all patients.
Serum IL-6 Measurement
Peripheral venous blood (2 m1) was collected from the study subjects after fasting, centrifuged at 3500 rpm for 15 min, and the serum was separated and stored at −20°C. The enzyme-linked immunosorbent assay (ELISA) was used to measure the IL-6 levels following the specific steps provided in the kit.
IL-6 −572G/C Gene Polymorphism Analysis
The polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method was used to analyze the IL-6 −572G/C gene polymorphism. The specific steps were as follows: ①3 mL of peripheral venous blood was collected from all participants with EDTA anticoagulation and the Qiagen DNA extraction kit was used to extract genomic DNA; ② IL-6 primers were designed using Primer Express software (v2.0) based on the reference sequence; ③ restriction enzyme digestion was performed; ④ gel electrophoresis was performed; and ⑤ the allele frequencies were calculated using the Hardy-Weinberg equation.24
Statistical Analysis
The statistical analysis was performed using SPSS (version 26.0). A chi-square test, one-way ANOVA, and Bonferroni test were used to compare the differences in demographic characteristics, lifestyle factors, IL-6 levels, lipid levels, HbA1c, and genotype frequency between the groups. The Mann–Whitney U-test was used to compare quantitative data with and without a normal distribution. Normally distributed data are presented as the mean ± standard deviation, while non-normally distributed data are expressed as the median (P25, P75). Qualitative data, expressed as rates or percentages, were compared using a chi-square or Fisher’s exact test. Logistic regression analysis was used to evaluate the association between the IL-6-572G/C gene polymorphism, susceptibility to CHD, and the degree of coronary stenosis. A significance level of P<0.05 was used for all statistical analyses.
Results
Comparison of Baseline Data Between Groups A and B
There were no significant differences between the two groups with respect to gender (P=0.463), body mass index [BMI] (P=0.133), cigarette smoking history (P=0.154), alcohol consumption history (P=0.594), family history of CHD (P=0.398), the presence or absence of hypertension (P=0.580), duration of diabetes (P=0.340), and blood glucose control vis-A-vis HbA1c (P=0.342), thus confirming comparability between the two groups. The mean age of group B was greater than the simple diabetes group (P=0.006; Table 1).
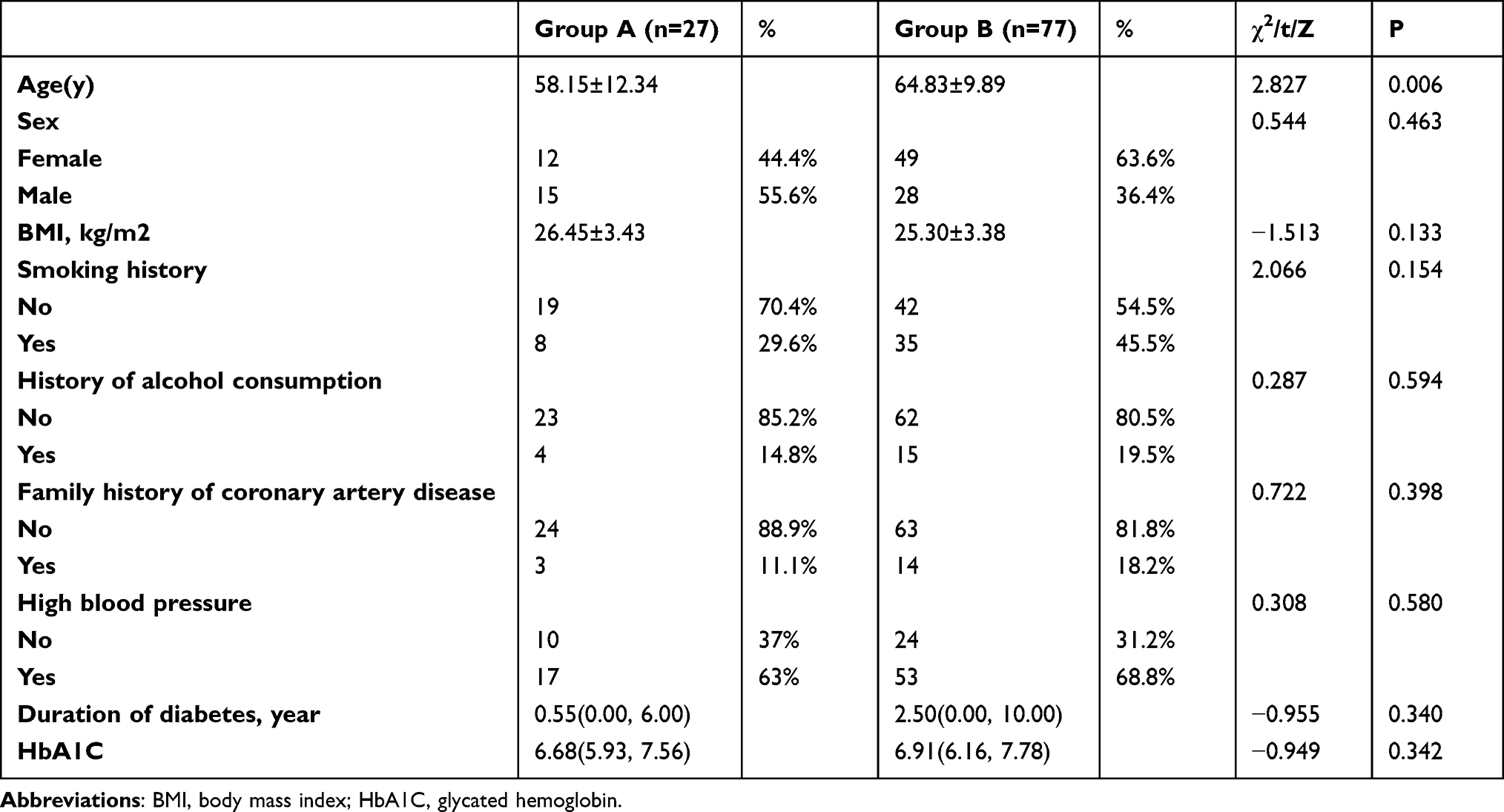 |
Table 1 Comparison of Baseline Information for Group A and Group B |
Comparison of Blood Lipids, IL-6, and HbA1c Levels Between Groups A and B
Group B had lower HDL-C (Z=−2.827, P=0.005) and higher IL-6 levels (Z=−3.510, P<0.001) compared to group A. There was no significant difference in TC (P=0.352), TG (P=0.362), LDL-C (P=0.711), or HbA1c (P=0.342) between the two groups (Table 2).
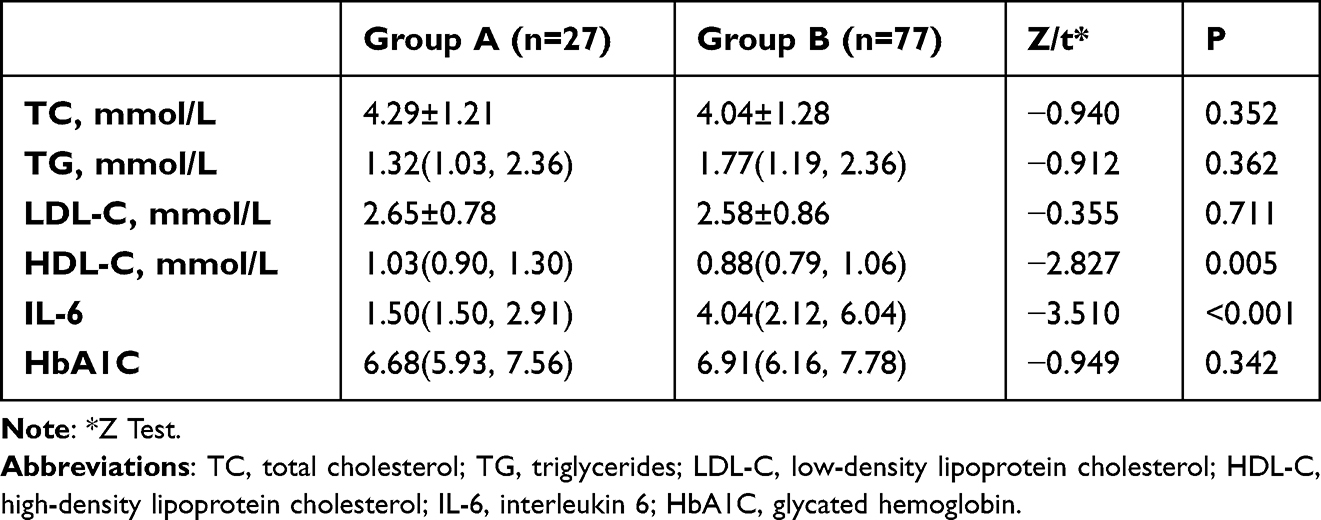 |
Table 2 Comparison of Lipid, IL-6, and HbA1C Levels Between Group A and Group B |
Comparison of IL-6 −572G/C Genotype Frequency Between Groups A and B
The chi-square test showed a significant difference in the distribution of IL-6 −572G/C genotypes between the two groups (χ2=8.682, P=0.013), with the CC genotype frequency being highest in the pure diabetes group and the GC genotype frequency being highest in the diabetes combined with CHD group. There was also a significant difference in the G and C allele frequencies between the two groups (χ2=9.477, P=0.002), with group B having a higher G allele frequency than group A (Table 3).
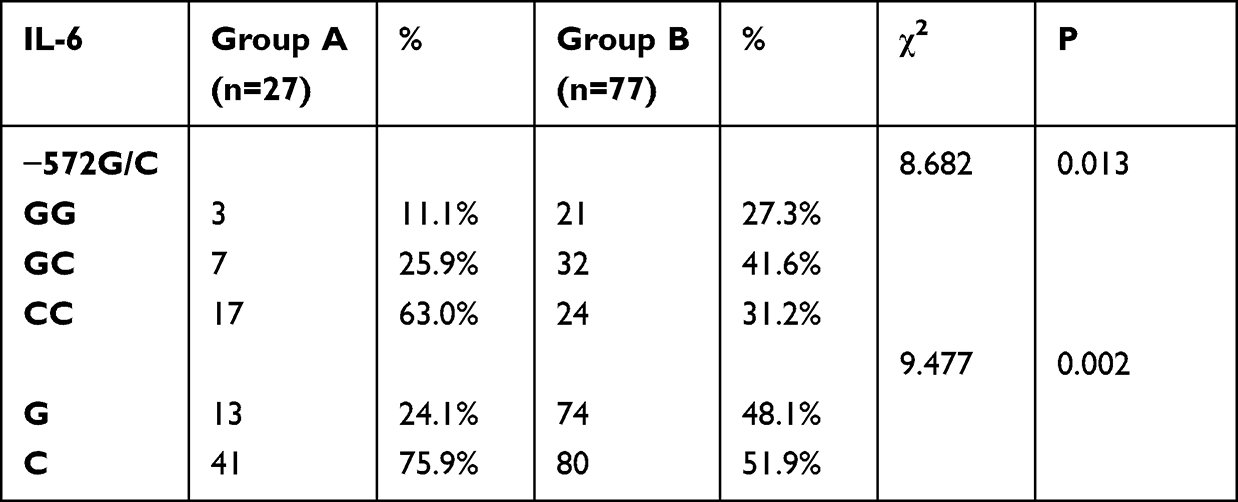 |
Table 3 Comparison of Genotype Frequencies of IL-6 −572G/C in Group A and Group B |
Correlation Between the IL-6 −572G/C Genotype and the Combined Occurrence of Diabetes and CHD
The risk of CHD in the GG genotype was 4.958-fold higher (95% CI: 1.273, 19.318; P=0.021) than the CC genotype and the risk in the GC genotype was 3.238-fold higher (95% CI: 1.159, 9.044; P=0.025). The risk of CHD in the G allele was 2.917-fold higher (95% CI, 1.450, 5.871; P=0.03; Table 4) than the C allele.
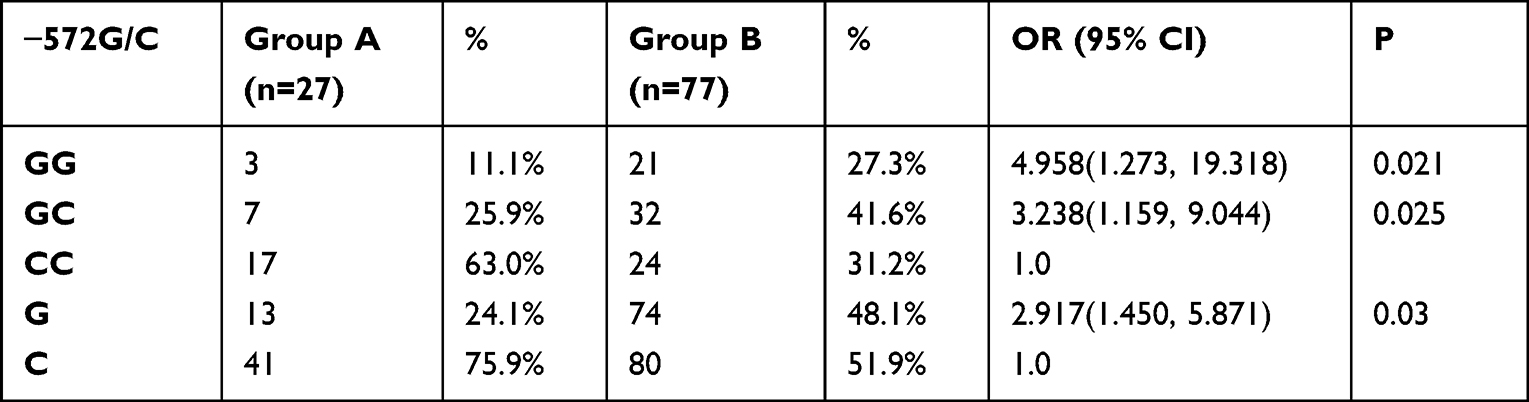 |
Table 4 Genetic Polymorphisms of IL-6 −572 G/C Correlated with the Development of Coronary Heart Disease in Diabetic Patients |
Comparison of Baseline Data Between Different Coronary Artery Lesion Severity Groups in Group B
There were no differences in age (t=1.227, P=0.300), gender (χ2=1.540, P=0.222), BMI (t=1.059, P=0.352), cigarette smoking history (χ2=0.224, P=0.800), alcohol consumption history (χ2=0.380, P=0.685), presence or absence of hypertension (χ2=1.355, P=0.265), duration of diabetes (Z=0.876, P=0.645), and blood glucose control vis-A-vis HbA1c (Z=0.137, P=0.934) among the three groups, indicating comparability. There was a difference in family history of CHD among the three groups, with a higher proportion of the high Syntax score group having a family history than the middle Syntax score group, and the middle Syntax score group having a higher proportion than the low Syntax score group (χ2=3.598, P=0.033; Table 5).
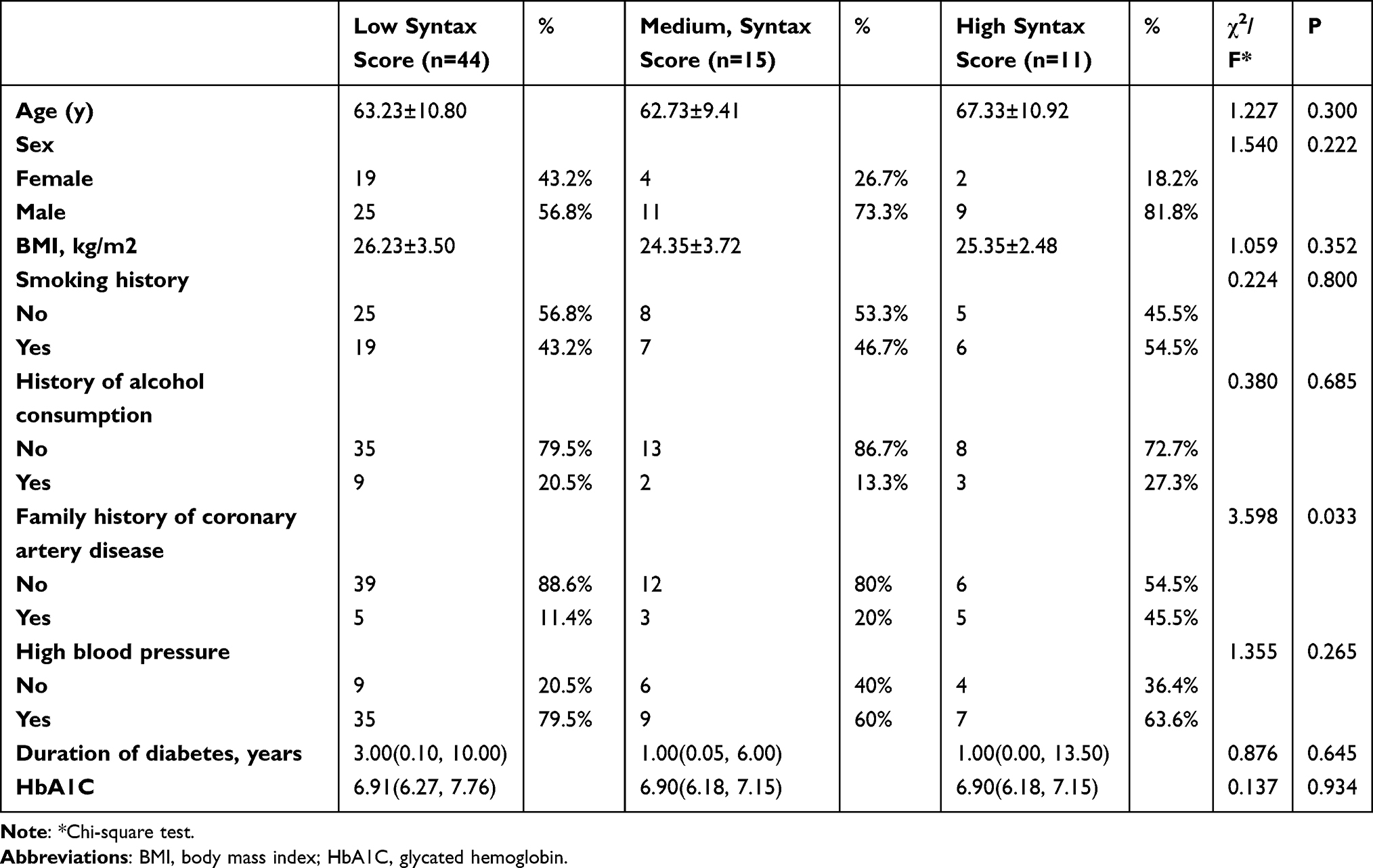 |
Table 5 Comparison of Baseline Information of Different Coronary Lesion Degree Groups in Group B |
Comparison of Blood Lipids, IL-6, and HbA1c Levels as a Function of Coronary Artery Lesion Severity in Group B
The low score group had higher HDL-C levels than the middle- and high-score groups (Z=8.197, P=0.017), indicating differences in HDL-C levels between the three groups. The high-score group had higher levels of IL-6 than the middle- and low-score groups (Z=6.511, P=0.039). The TC (Z=0.282, P=0.244), TG (Z=0.607, P=0.738), LDL-C (t=2.371, P=0.306), and HbA1c (Z=0.137, P=0.934) levels did not differ significantly among the 3 groups (Table 6).
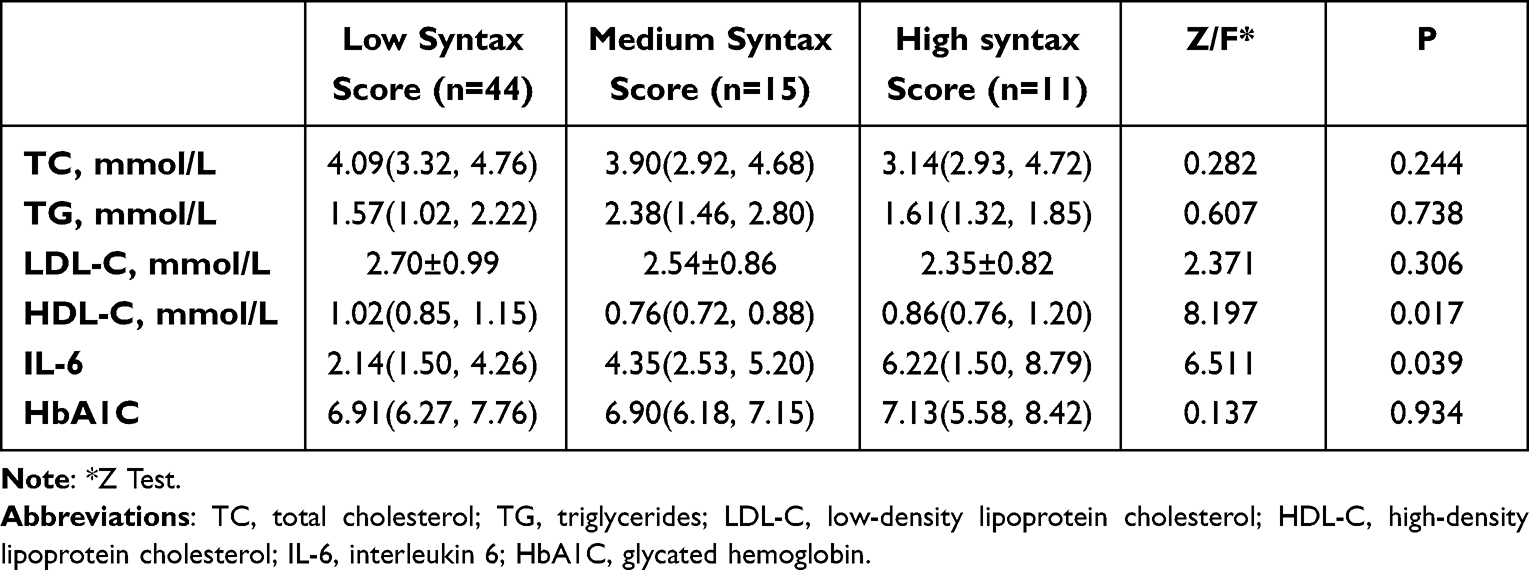 |
Table 6 Comparison of Lipid, IL-6, and HbA1C Levels in Different Coronary Lesion Degree Groups in Group B |
Comparison of IL-6 −572G/C Genotype Distribution as a Function of Coronary Artery Lesion Severity in Group B
There was a significant variation in the distribution of IL-6 −572G/C genotypes among the three groups according to the chi-square test (χ2=1.743, P=0.034). The low-score group had a higher percentage of the CC genotype, while the high-score group had a higher percentage of the GC genotype. There was no significant difference in the G/C allele frequency among the 3 groups (χ2=1.370, P=0.504; Table 7).
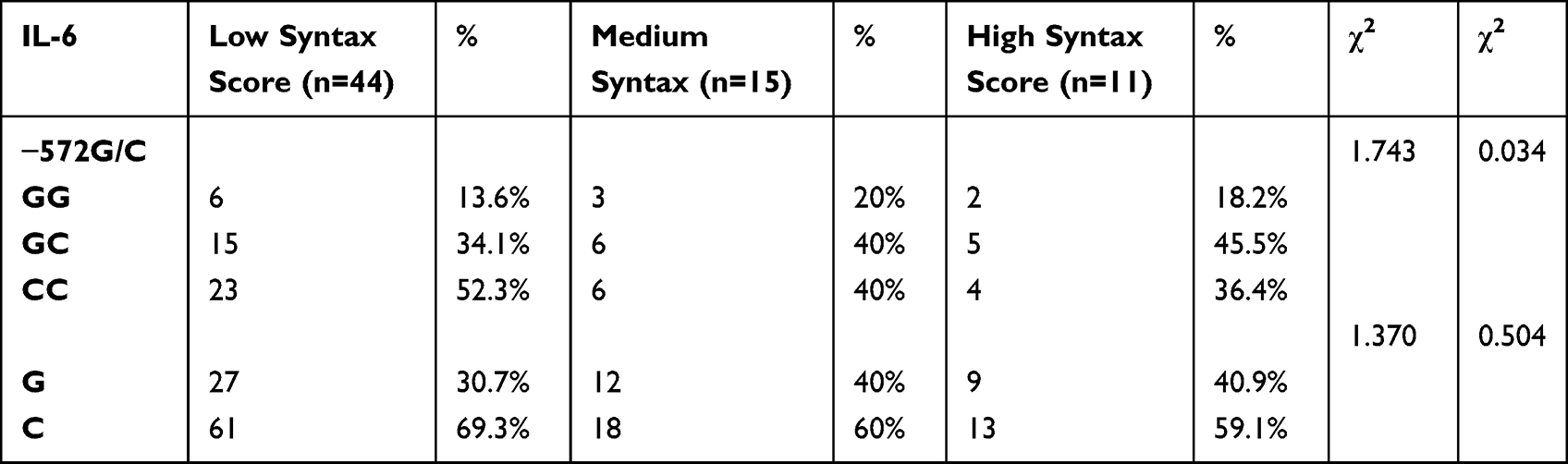 |
Table 7 Genotype Frequencies of IL-6 −572 G/C in Different Coronary Lesion Degree Groups in Group B |
Correlation Between the IL-6 −572G/C Genotype and the Severity of CAD in Group B
The risk ratio for increased severity of CAD in group B with the GG and GC genotypes was 9.346 (95% CI: 2.063, 42.31; P=0.004; Table 8), and 3.589 (95% CI: 0.872, 14.776; P=0.077) compared to the CC genotype, respectively. The G allele increased the risk ratio for increased CAD severity in group B by 2.455 (95% CI: 1.207, 4.993; P<0.001) compared to the C allele.
 |
Table 8 Correlation of Genetic Polymorphisms of IL-6 −572 G/C with the Degree of Coronary Artery Disease in Patients with Diabetes Mellitus Combined with Coronary Artery Disease |
Correlation Between the IL-6 −572G/C Genotype and Blood Lipids, IL-6, and Glycosylated Hemoglobin
According to Table 9, The IL-6 levels were significantly different among the three IL-6 −572G/C genotype groups; the GG group had higher levels than the GC group and the GC group had higher levels than the CC group (Z=12.210, P=0.002; Table 9); however, no significant differences existed with respect to the TC (Z=1.800, P=0.407), TG (Z=1.048, P=0.592), LDL-C (Z=1.285, P=0.526), HDL-C (Z=0.358, P=0.836), and HbA1c levels (Z=0.218, P=0.897) among the three IL-6 −572G/C genotype groups.
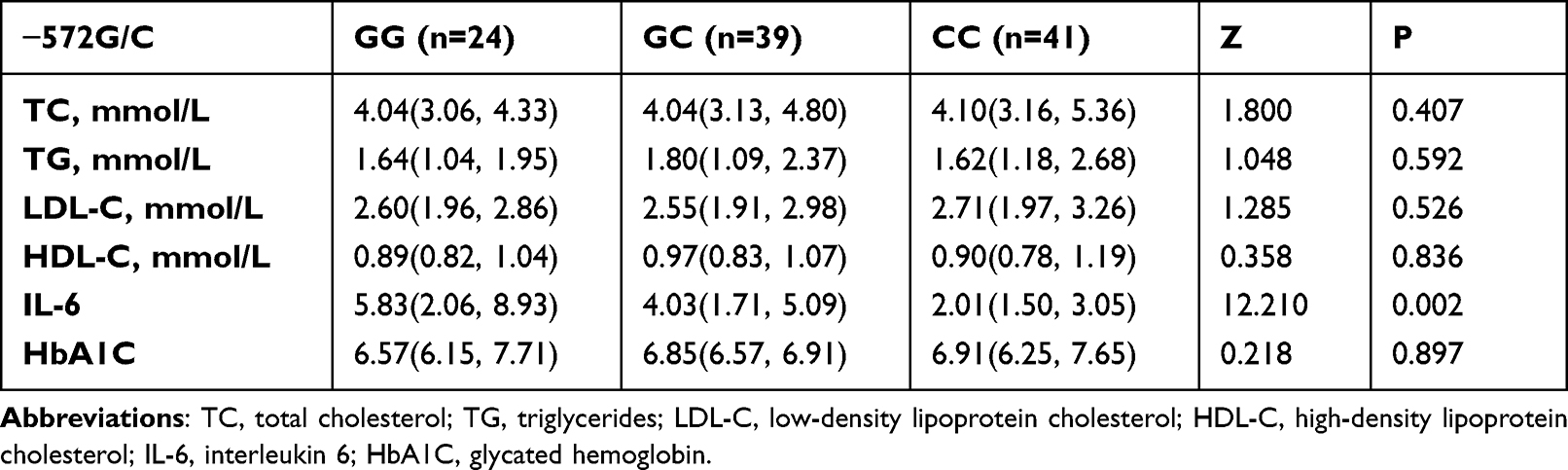 |
Table 9 Comparison of Genotypes of IL-6 −572 G/C with Blood Lipid, IL-6, and Glycated Hemoglobin Levels |
Discussion
Both diabetes and CHD pose significant risks to human health and are major global public health concerns. An independent risk factor for CHD is diabetes. Numerous studies have raised the possibility that chronic inflammation may contribute to the emergence of cardiovascular disease.25–27 Chronic inflammation and some forms of cardiovascular disease are accelerated by persistent inflammatory states.27–29 Human IL-6, a cytokine with pro-inflammatory properties, is encoded by the IL-6 gene; IL-6 was cloned and discovered in 1986.30
The IL-6 gene is found on chromosome 7p15-p21 and has five exons and four introns. A precursor protein with 212 amino acids in length is encoded by the IL-6 gene using a mature peptide of 184 amino acids and a signal sequence of 28 amino acids.31,32 An essential part of the inflammatory response during AS can be attributed to the cytokine, IL-6.30 These data have led to the conclusion that increased IL-6 levels are linked to cardiovascular events.30,33–35
Our study provided evidence that IL-6 gene polymorphism is associated with an increased risk of developing CHD and the severity of coronary artery stenosis in diabetic patients. Specifically, the IL-6-572G/C polymorphism was shown to be associated with a higher risk of CHD in the Chinese population. These findings are in agreement with previous studies that have demonstrated a positive correlation between plasma IL-6 levels and atherosclerotic calcification in patients with chronic renal disease.36 Additionally, our results are consistent with the findings of Elsenberg et al,35 who reported that plasma IL-6 levels were significantly higher in patients with CHD compared to the control group.
The structure and quantity of gene products can be altered by genetic polymorphism, which ultimately affects how the gene products function.37 The expression and functionality of the IL-6 protein may be impacted by IL-6 gene polymorphism, thus changing vulnerability to cardiovascular disease. Contradictory findings have been presented in prior studies that investigated the connection between IL-6 gene polymorphism and the prevalence of cardiovascular disease.27,37–39 The IL-6 −572C/G polymorphism and the risk of cardiovascular events are not linked according to Song et al.27
Li et al37 reported that the GG genotype of IL-6-572C/G was linked to an elevated risk of CAD in a group of Chinese individuals. In their study of 402 CHD patients and 402 controls, Wang et al38 found no association between CHD and the IL-6-572C/G polymorphism, but a strong link between susceptibility to CHD and the IL-6-174G/C polymorphism, in 402 CHD patients and 402 controls. According to one study, the IL-6 gene 572 C/G CC genotype has a protective effect.39 The research also showed that the IL-6 gene 572 C/G genotypes CG and GG enhanced the risk of CHD.39 The Han population in China has much higher levels of the GG/GC genotype and allele G of −572 than the control group according to Fu et al.40 The −572G/C gene polymorphism is linked to vulnerability to CHD by Hongmei et al.41
Our study showed that patients with diabetes and CHD were older and IL-6 levels, and lower HDL-C compared to patients with simple diabetes. In addition, with the increase in CAD severity in patients with diabetes and CHD, IL-6 levels gradually increased and HDL-C gradually decreased. Furthermore, the GG and GC genotypes, and IL-6-572G/C G allele were shown to be associated with an increased risk of susceptibility to CAD and the severity of coronary artery stenosis. Therefore, IL-6-572G/C gene polymorphism is associated with the occurrence of diabetes and CHD and the severity of CAD.
Limitations in the Current Study
The current study had a limited sample size and geographic scope, thus diminishing the generalizability of the study. Therefore, there is a need to increase the sample size and expand the coverage area to enhance the representativeness of the study. The mechanisms underlying how the interleukin-6-572G/C gene polymorphism contributes to CAD, as well as the associations between other interleukin-6 gene polymorphisms and the onset and progression of CAD, both require further study. Additionally, there is a need to investigate other inflammatory factors, such as interleukin-10 and CRP, and the relationship to the incidence of CHD.
Conclusion
In conclusion, the association between IL-6 gene polymorphisms and susceptibility to cardiovascular disorders in individuals with diabetes is discussed herein, thus drawing attention to the conflicting results of other studies and offers novel evidence that the IL-6 −572G/C gene polymorphism increases the risk of CAD and augments the severity of coronary artery stenosis in Chinese patients with diabetes. The study also showed that individuals with diabetes and CAD had lower HDL-C levels and higher IL-6 levels than patients with diabetes alone. Overall, the evidence points to a potential involvement of IL-6 gene polymorphisms in the onset and severity of cardiovascular disease in individuals with diabetes. These specific findings suggest that IL-6 gene polymorphisms may facilitate CHD prevention efforts in a genetic-specific diabetic population.
Data Sharing Statement
Data are available by the corresponding author upon reasonable request.
Funding
This study was supported by Educational Reform Foundation of Shanxi Province(NO.J20220322), Foundation of the First Hospital of Shanxi Medical University (NO.YB161708), and Natural Science Foundation of Shanxi Province (NO.201801D221405).
Disclosure
The authors declare that they have no conflict of interest to report.
References
1. Ralapanawa U, Sivakanesan R. Epidemiology and the magnitude of coronary artery disease and acute coronary syndrome: a narrative review. J Epidemiol Glob Health. 2021;11(2):169–177. doi:10.2991/jegh.k.201217.001
2. Canto JG, Kiefe CI, Rogers WJ, et al. Number of Coronary heart disease risk factors and mortality in patients with first myocardial infarction. JAMA. 2011;306(19):2120–2127. doi:10.1001/jama.2011.1654
3. Badimon L, Padró T, Vilahur G. Atherosclerosis, platelets and thrombosis in acute ischaemic heart disease. Eur Heart J Acute Cardiovasc Care. 2012;1(1):60–74. doi:10.1177/2048872612441582
4. Su JH, Luo MY, Liang N, et al. Interleukin-6: a Novel Target for Cardio-Cerebrovascular Diseases. Front Pharmacol. 2021;12:745061. doi:10.3389/fphar.2021.745061
5. Shanker J, Kakkar VV. Implications of genetic polymorphisms in inflammation-induced atherosclerosis. Open Cardiovasc Med J. 2010;4:30–37.
6. Tanaka T, Narazaki M, Kishimoto T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb Perspect Biol. 2014;6(10):a016295. doi:10.1101/cshperspect.a016295
7. Omoigui S. The Interleukin-6 inflammation pathway from cholesterol to aging--role of statins, bisphosphonates and plant polyphenols in aging and age-related diseases. Immun Ageing. 2007;4:1. doi:10.1186/1742-4933-4-1
8. Fanola CL, Morrow DA, Cannon CP, et al. Interleukin-6 and the risk of adverse outcomes in patients after an acute coronary syndrome: observations from the SOLID-TIMI 52 (Stabilization of Plaque Using Darapladib-Thrombolysis in Myocardial Infarction 52) Trial. J Am Heart Assoc. 2017;6(10):e005637. doi:10.1161/JAHA.117.005637
9. Zheng GH, Chen HY, Xiong SQ. Polymorphisms of −174G>C and −572G>C in the interleukin 6 (IL-6) gene and Coronary heart disease risk: a meta-analysis of 27 research studies. PLoS One. 2012;7(4):e34839. doi:10.1371/journal.pone.0034839
10. Rahman S, Rahman T, Ismail AA, Rashid AR. Diabetes-associated macrovasculopathy: pathophysiology and pathogenesis. Diabetes Obes Metab. 2007;9:767–780. doi:10.1111/j.1463-1326.2006.00655.x
11. Cade WT. Diabetes-related microvascular and macrovascular diseases in the physical therapy setting. Phys Ther. 2008;88(11):1322–1335. doi:10.2522/ptj.20080008
12. Pradhan AD, Manson JE, Rifai N, et al. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA. 2001;286:327–334. doi:10.2174/1874192401004020030
13. Akash MS, Shen Q, Rehman K, Chen S. Interleukin-1 receptor antagonist: a new therapy for type 2 diabetes mellitus. J Pharm Sci. 2012;101:1647–1658. doi:10.1002/jps.23057
14. Lu QK, Zhang JT, Zhao N, Wang HY, Tong QH, Wang SL. Association of IL-6 Gene (−174 and −572 G/C) polymorphisms with proliferative diabetic retinopathy of type 2 diabetes in a Chinese population. Ophthalmic Res. 2017;58(3):162–167. doi:10.1159/000475670
15. Ayelign B, Negash M, Andualem H, et al. Association of IL-10 (− 1082 A/G) and IL-6 (− 174 G/C) gene polymorphism with type 2 diabetes mellitus in Ethiopia population. BMC Endocr Disord. 2021;21:70. doi:10.1186/s12902-021-00738-1
16. Shoily SS, Ahsan T, Fatema K, Sajib AA. Common genetic variants and pathways in diabetes and associated complications and vulnerability of populations with different ethnic origins. Sci Rep. 2021;11(1):7504. doi:10.1038/s41598-021-86801-2
17. Liu K, Xie Y, Zhao Q, et al. Polymorphisms and gene-gene interaction in AGER/IL6 pathway might be associated with diabetic ischemic heart disease. J Pers Med. 2022;12(3):392.
18. Manolio TA, Collins FS, Cox NJ, et al. Finding the missing heritability of complex diseases. Nature. 2009;461:747–753. doi:10.1038/nature08494
19. Caraballo C, Desai NR, Mulder H, et al. Clinical Implications of the New York heart association classification. J Am Heart Assoc. 2019;8(23):e014240. doi:10.1161/JAHA.119.014240
20. Nomenclature and criteria for diagnosis of ischemic heart disease. Report of the Joint International Society and Federation of Cardiology/World Health Organization task force on standardization of clinical nomenclature. Nomenclature and criteria for diagnosis of ischemic heart disease. Circulation. 1979;59(3):607–609. doi:10.1161/01.CIR.59.3.607
21. World Health Organization. Cardiovascular diseases Credits. Available from: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1.
22. Windecker S, Kolh P. 2014 ESC/EACTS Guidelines on myocardial revascularization: the Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014;35(37):2541–2619.
23. Sianos G, Morel M-A, Kappetein AP, et al. The SYNTAX score: an angiographic tool grading the complexity of coronary artery disease. EuroIntervention. 2005;1:219–227.
24. Sen S, Burmeister M. Hardy-Weinberg analysis of a large set of published association studies reveals genotyping error and a deficit of heterozygotes across multiple loci. Hum Genomics. 2008;3(1):36–52. doi:10.1186/1479-7364-3-1-36
25. Mormile R. Multiple sclerosis and susceptibility to cardiovascular diseases: implications of ethnicity-related interleukin-17A gene polymorphism? Med Hypotheses. 2015;85(3):365–366.
26. Qi X, Bai F, You C, Guo X, Shi L, Hu Z. 高分辨率融解曲线技术检测冠心病患者IL-1β和IL-1Ra基因多态性[High-resolution melting technology for detecting genetic polymorphisms of IL-1β and IL-1Ra in patients with coronary artery disease]. Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi. 2015;31(6):816–820. Chinese.
27. Song Y, Gu HD, He Y, Wang JW. Role of IL-6 polymorphism on the development of cardiovascular events and coronary artery disease in patients receiving hemodialysis. Genet Mol Res. 2015;14(1):2631–2637. doi:10.4238/2015.March.30.23
28. Wang S, Dai YX, Chen LL, et al. Effect of IL-1β, IL-8, and IL-10 polymorphisms on the development of myocardial infarction. Genet Mol Res. 2015;14(4):12016–12021. doi:10.4238/2015.October.5.14
29. Zou L, Zhao H, Gong X, et al. The association between three promoter polymorphisms of IL-1 and stroke: a meta-analysis. Gene. 2015;567(1):36–44.
30. Terry CF, Loukaci V, Green FR. Cooperative influence of genetic polymorphisms on interleukin 6 transcriptional regulation. J Biol Chem. 2000;275(24):18138–18144. doi:10.1074/jbc.M000379200
31. Hirano T, Yasukawa K, Harada H, et al. Complementary DNA for a novel human interleukin (BSF-2) that induces B lymphocytes to produce immunoglobulin. Nature. 1986;324(6092):73–76. doi:10.1038/324073a0
32. Simpson RJ, Hammacher A, Smith DK, Matthews JM, Ward LD. Interleukin-6: structure-function relationships. Protein Sci. 1997;6(5):929–955.
33. Batra G, Ghukasyan Lakic T, Lindbäck J, et al. STABILITY Investigators. Interleukin 6 and cardiovascular outcomes in patients with chronic kidney disease and chronic coronary syndrome. JAMA Cardiol. 2021;6(12):1440–1445.
34. Held C, White HD, Stewart RAH, et al. STABILITY Investigators. Inflammatory Biomarkers Interleukin-6 and C-reactive protein and outcomes in stable coronary heart disease: experiences from the STABILITY (Stabilization of Atherosclerotic Plaque by Initiation of Darapladib Therapy) Trial. J Am Heart Assoc. 2017;6(10):e005077. doi:10.1161/JAHA.116.005077
35. Elsenberg EH, Sels JE, Hillaert MA, et al. Increased cytokine response after toll-like receptor stimulation in patients with stable coronary artery disease. Atherosclerosis. 2013;231(2):346–351. doi:10.1016/j.atherosclerosis.2013.09.036
36. Roy N, Rosas SE. IL-6 is associated with progression of coronary artery calcification and mortality in incident dialysis patients. Am J Nephrol. 2021;52(9):745–752. doi:10.1159/000518652
37. Li L, Li E, Zhang LH, Jian LG, Liu HP, Wang T. IL-6-174G/C and IL-6-572C/G polymorphisms are associated with increased risk of coronary artery disease. Genet Mol Res. 2015;14(3):8451–8457.
38. Wang K, Dong PS, Zhang HF, Li ZJ, Yang XM, Liu H. Role of interleukin-6 gene polymorphisms in the risk of coronary artery disease. Genet Mol Res. 2015;14(2):3177–3183. doi:10.4238/2015.April.10.29
39. Salari N, Mansouri K, Hosseinian-Far A, et al. The effect of polymorphisms (174G> C and 572C> G) on the Interleukin-6 gene in coronary artery disease: a systematic review and meta-analysis. Genes Environ. 2021;43(1):1. doi:10.1186/s41021-021-00172-8
40. Fu HX, Zhang JY, Li GS, Li Y, Xu JL, Zhao ZN. Association study of interleukin-6 gene −572C/G polymorphism with susceptibility to myocardial infarction. Chin J Med Genet. 2006;23(3):245–249.
41. Hongmei Y, Yongping J, Jiyuan L. Interleukin-6 polymorphisms and risk of coronary artery diseases in a Chinese population: a case-control study. Pak J Med Sci. 2016;32(4):880–885. doi:10.12669/pjms.324.9908
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Genetic Polymorphism of NQO1 Influences Susceptibility to Coronary Heart Disease in a Chinese Population: A Cross-Sectional Study and Meta-Anaylsis
Zhou YY, Sun JH, Wang L, Cheng YY
Pharmacogenomics and Personalized Medicine 2023, 16:825-833
Published Date: 11 September 2023
Based on the Dual Pathway of Interaction-Mediated NF-κB in Cell Apoptosis and Immune Inflammation to Study the Effect of Danzhi Xiaoyao Powder on the Learning and Cognitive Ability of AD Model Rats
Wang HP, Li MC, Yang J, Zhou J, Meng ZP, Hu YY, Lyu YJ, Chen YQ, Han YM, Pei WL
Degenerative Neurological and Neuromuscular Disease 2025, 15:41-64
Published Date: 14 April 2025
Inflammation Mediates the Relationship Between Serum Uric Acid and New-Onset Diabetes Risk in Patients with Coronary Heart Disease: Results from a Multicenter Cohort Study
Song S, Cai X, Xu T, Cui P, Zou Z, Zhao J, Liu Y, Wang K
Diabetes, Metabolic Syndrome and Obesity 2026, 19:602643
Published Date: 18 June 2026
Obesity-Related Insulin Resistance Indices and CKD Risk in Patients with Diabetes and Coronary Heart Disease: A Multicenter Cohort Analysis
Zhang J, Zhang Z, He Y, Liu S, Zhao J, Ge X
Diabetes, Metabolic Syndrome and Obesity 2026, 19:610602
Published Date: 26 June 2026