Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Association Between Improvement in Institutional COPD Quality Assessment Grade and Risk of Acute Exacerbations in Primary and Secondary Care: A Nationwide Claims-Based Study
Authors Moon SW ![]() , Lee H
, Lee H ![]() , Kim Y
, Kim Y ![]() , Kim K
, Kim K ![]() , Rhee CK
, Rhee CK ![]() , Moon JY
, Moon JY ![]()
Received 2 April 2026
Accepted for publication 29 May 2026
Published 19 June 2026 Volume 2026:21 613969
DOI https://doi.org/10.2147/COPD.S613969
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Sung Woo Moon,1 Hyun Lee,2 Youlim Kim,1 Kyungjoo Kim,3 Chin Kook Rhee,1 Ji-Yong Moon1
1Division of Pulmonary, Allergy, and Critical Care Medicine, Department of Internal Medicine, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea; 2Department of Internal Medicine, College of Medicine, Hanyang University, Seoul, Korea; 3Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Seoul St Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
Correspondence: Ji-Yong Moon, Division of Pulmonary, Allergy, and Critical Care Medicine, Department of Internal Medicine, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea, Tel +82-2-2030-7615, Email [email protected]
Background: The Health Insurance Review and Assessment Service (HIRA) in South Korea assesses and grades primary and secondary healthcare institutions according to their management of chronic obstructive pulmonary disease (COPD). This study examined whether changes in institutional quality assessment grades were associated with variations in the concurrent risk of acute COPD exacerbations.
Methods: Using national HIRA claims data, we identified 36,218 patients with COPD treated at 873 non-tertiary medical institutions between May 2016 and April 2018. Institutions were stratified into three groups based on their grade trajectories from the 3rd (May 2016–April 2017) to the 4th (May 2017–April 2018) assessment periods: the 158 improved-grade (n=5,118), 526 maintained-grade (n=25,286), and 189 declined-grade (n=5,814) institution groups. We compared the incidence and severity of exacerbations among these groups during the 4th assessment period. Incidence rate ratios (IRRs) for exacerbations were estimated using multivariable negative binomial regression models to adjust for potential confounders.
Results: At baseline, improved-grade institutions exhibited significantly higher rates of pulmonary function testing (56.3% vs. 41.9%) and greater prescription of long-acting muscarinic antagonists (29.0% vs. 14.6%) compared with declined-grade institutions (p< 0.001). During the 1-year outcome period (May 2017–April 2018), the incidence of moderate-to-severe COPD exacerbations was considerably higher in the declined-grade group (29.2%) than in the improved-grade group (26.1%) (p=0.008). In the negative binomial regression analyses using the maintained-grade group as the reference category, patients treated at improved-grade institutions had a significantly lower risk of exacerbations (adjusted IRR 0.864, 95% CI 0.795– 0.939, p< 0.001).
Conclusion: This analysis of nationwide real-world claims data demonstrated that institutional improvement in COPD quality assessment grades was associated with a reduced concurrent risk of acute exacerbations in both primary and secondary care settings. These findings indicate that institutional indicators of guideline-aligned COPD care may correspond to clinically meaningful differences in patient-level outcomes.
Keywords: chronic obstructive pulmonary disease, quality indicators, health care, primary health care, treatment outcome
Introduction
Chronic obstructive pulmonary disease (COPD) is recognized as the fourth leading cause of death worldwide and poses a substantial global health and economic burden.1,2 In South Korea, its prevalence is 13.4% among adults aged >40 years, underscoring its significance as a major chronic respiratory disease.3 Effective COPD management requires sustained adherence to treatment through regular outpatient follow-up and appropriate use of maintenance inhalers.1 Such consistent management is essential to prevent disease progression, reduce the risk of acute exacerbations, and alleviate the associated socioeconomic burden.4,5
As a chronic ambulatory care-sensitive condition, effective COPD management largely depends on outpatient-based care, emphasizing the central role of primary and secondary medical institutions.6 However, variability in care quality persists across healthcare settings. Adherence to guideline-recommended management strategies, including the use of pulmonary function testing (PFT) and maintenance inhalers, has been reported to be lower in non-tertiary institutions than in tertiary hospitals.7 These differences suggest heterogeneity in the delivery of COPD care and raise important questions regarding the clinical impact of variations in institutional performance.8
To address this issue, the Health Insurance Review and Assessment Service (HIRA) has employed nationwide quality assessment programs for COPD management.9 These evaluations generate annual institutional grades based on predefined performance indicators. Because grades are recalculated annually using absolute performance thresholds, changes in grade reflect shifts in institutional adherence to recommended management practices.
Although national trends have demonstrated improvements in certain process indicators,10 the degree to which changes in institutional grade are associated with patient-level clinical outcomes, such as the concurrent risk of acute COPD exacerbations, remains unclear. Therefore, this study aimed to examine the association between longitudinal changes in HIRA assessment grades and the concurrent incidence of acute COPD exacerbations using nationwide claims data.
Materials and Methods
Study Participants and Design
We selected patients with COPD from the HIRA database and designated May 2016 to April 2017 (third assessment) as the baseline period. Using International Classification of Diseases, 10th Revision (ICD-10) codes, COPD was identified when recorded as a principal or secondary diagnosis. Patients with COPD were defined as those who satisfied all of the following criteria: (1) age ≥40 years; (2) an ICD-10 code for COPD (J43.x–J44.x, except J43.0) listed as the principal diagnosis or as a secondary diagnosis within the first four diagnostic positions; and (3) receipt of at least one COPD-related medication prescription on at least two occasions within the baseline period, including long-acting muscarinic antagonists (LAMAs), long-acting beta-2 agonists (LABAs), inhaled corticosteroids (ICS), ICS plus LABA (ICS+LABA), LABA plus LAMA (LABA+LAMA), short-acting beta-2 agonists (SABAs), phosphodiesterase-4 inhibitors, systemic bronchodilators, or theophylline.10 The age threshold of ≥40 years was adopted in accordance with the case definition used by the HIRA COPD Quality Assessment Program.7,9
Comorbidities were ascertained using ICD-10 codes as follows: ischemic heart disease (including angina pectoris, I20.x), congestive heart failure (I50.x), hypertension (I10.x–I15.x), hyperlipidemia (E78.x), diabetes mellitus (E10.x–E14.x), osteoporosis (M80.x–M81.x), gastroesophageal reflux disease (GERD; K21.x), arthritis (osteoarthritis, M15.x–M19.x; rheumatoid arthritis, M05.x and M06.x), and anemia (D50.x).
Patients treated at tertiary hospitals were excluded. Furthermore, to reduce potential confounding from severe comorbid illnesses, we excluded patients with more than one reimbursement claim per year for cancer (C00.x–C97.x), renal failure (N17.x–N19.x), or cerebrovascular disease (I60.x–I69.x) during the study period.
For the analysis of medication use, each drug class was evaluated independently according to prescription claims recorded during the baseline period. Because the HIRA database reflects real-world prescribing practices, medication categories were allowed to overlap and were therefore not mutually exclusive. Individual patients could receive more than one class of COPD-related medication during the same assessment period, either sequentially due to treatment modification or concurrently as combination therapy. For example, some patients may have changed their inhaler regimens over time, whereas others may have been prescribed separate ICS and LABA components rather than fixed-dose combination products (ICS+LABA). Therefore, the proportions reported for each medication class represent the percentage of patients who received at least one prescription for that class during the baseline period, and these percentages were not expected to total 100%.
The primary outcome was the occurrence of moderate-to-severe acute exacerbations of COPD during the fourth assessment period (May 2017 to April 2018), corresponding to the same evaluation period where institutional grade was determined.
Moderate exacerbation was defined as an outpatient visit with an ICD-10 code for COPD (J43.x–J44.x, except J43.0) listed as the principal or secondary diagnosis within the first four diagnostic positions, accompanied by a prescription for systemic corticosteroids and antibiotics. Severe exacerbation was defined as an event requiring hospitalization or an emergency room (ER) visit with a prescription for systemic corticosteroids and antibiotics.
Regarding outpatient services, only visits with COPD (J43.x–J44.x, except J43.0) recorded as the principal or secondary diagnosis (within the first four positions) were included in the analysis. For hospitalization, admissions were included when the principal or secondary (within the first four positions) diagnosis was COPD (J43.x–J44.x, except J43.0) or a COPD-related condition.
Moreover, we collected demographic and clinical variables, including age, sex, type of insurance (medical aid vs. non-medical aid), Charlson Comorbidity Index (CCI), comorbid asthma, prior hospitalizations, ER visits, and medication use.
Grading of Healthcare Institutions
Healthcare institutions were assessed and categorized based on their performance in the national COPD quality assessments conducted by HIRA.11,12 The evaluation system employs a composite score based on three key performance indicators: (1) the PFT execution rate, (2) the proportion of regular outpatient visits, and (3) the prescription rate of inhaled bronchodilators. Based on the weighted total of these indicators, medical facilities are annually assigned one of the five grades, where grades 1 and 5 represent the highest and lowest quality of care, respectively. The detailed scoring thresholds, indicator definitions, and weights used in the grading process are summarized in Supplementary Table S1. As HIRA quality assessments are conducted each year independently based on absolute scoring thresholds, a change in grade reflects a substantial shift in the institutions’ actual adherence to COPD management guidelines during that specific period. Patient–institution linkage in this study followed the HIRA COPD Quality Assessment Program methodology, under which each institution’s grade is derived from its own assessed COPD patients during the relevant assessment period.13
In this study, we evaluated the grade trajectories of institutions between the third (May 2016 to April 2017) and fourth (May 2017 to April 2018) assessment periods. Based on these changes, non-tertiary institutions were classified into the following three groups: the improved-grade group, consisting of institutions that upgraded to a higher clinical grade (eg., from grade 3 to grade 2); the maintained-grade group, including institutions with no change in their assigned grade; and the declined-grade group, comprising institutions that experienced a downgrade (eg., from grade 3 to grade 4).
Statistical Analysis
The selected patients were classified into three institutional groups according to changes in assessment grade (improved, maintained, or declined). Baseline characteristics were compared across groups using the chi-square test and one-way analysis of variance for categorical and continuous variables, respectively.
The primary outcome was the incidence of moderate-to-severe COPD exacerbations during the fourth assessment period. Given that exacerbation counts exhibited overdispersion, incidence rate ratios (IRRs) were estimated using negative binomial regression models. Unadjusted models were first constructed to estimate crude associations between institutional grade trajectory and exacerbation risk. Subsequently, to adjust for potential confounders, including age, sex, type of insurance (medical aid vs. non-medical aid), CCI, comorbid asthma, long-term roflumilast use (defined as use for ≥3 consecutive months), and long-term macrolide use (defined as use for ≥3 consecutive months), multivariable negative binomial regression analyses14 were conducted. Prior hospitalizations and ER visits were not included as adjustment variables in the primary model; given that the analytic plan was pre-specified under HIRA’s closed remote-analysis environment, the adjustment variable set was deliberately maintained conservative at the planning stage.
Results are presented as IRRs with 95% confidence intervals (CIs). All tests were two-sided, and statistical significance was set at p < 0.05. Continuous and categorical variables are presented as mean ± standard deviation and numbers (percentages), respectively. All statistical analyses were conducted using SAS Enterprise Guide version 7.1 (SAS Institute Inc., Cary, NC, USA). Figures were generated using R software version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria) with the ggplot2 and patchwork packages.
Results
Baseline Characteristics of the Study Population
Overall, 36,218 patients with COPD treated at 873 non-tertiary institutions were included (Table 1). According to changes in institutional assessment grade between the third and fourth periods, patients were classified into improved-grade (n=5,118), maintained-grade (n=25,286), and declined-grade (n=5,814) groups.
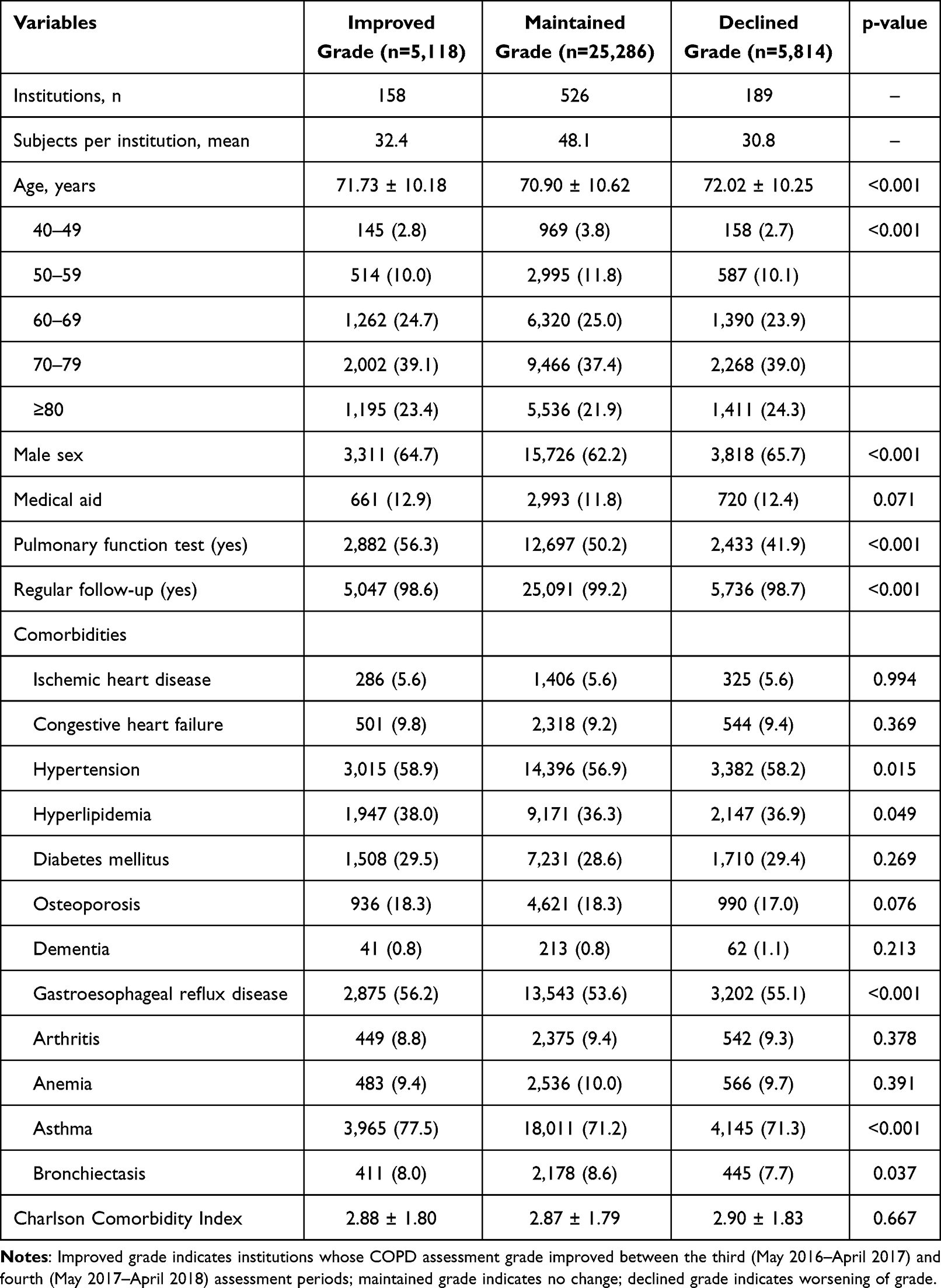 |
Table 1 Baseline Characteristics of Patients According to Changes in Institutional COPD Assessment Grade |
The mean age differed significantly across groups (p<0.001), with patients in declined-grade institutions being slightly older (72.02 ± 10.25 years) than those in improved-grade (71.73 ± 10.18 years) and maintained-grade (70.90 ± 10.62 years) institutions. Male patients comprised 64.7%, 62.2%, and 65.7% of the improved-, maintained-, and declined-grade groups, respectively. The proportion of patients aged ≥80 years was highest in the declined-grade group (24.3%).
PFTs were conducted more frequently in improved-grade institutions (56.3%) than in maintained-grade (50.2%) and declined-grade (41.9%) institutions (p<0.001). Regular outpatient follow-up exceeded 98% in all groups. Asthma was more prevalent in the improved-grade group (77.5%) than in the maintained- (71.2%) and declined-grade groups (71.3%) (p<0.001), whereas the CCI did not differ significantly (p=0.667).
Regarding COPD-related medication use, long-acting bronchodilators were prescribed more frequently in improved-grade institutions, including LAMA (29.0% vs. 22.6% vs. 14.6%, p<0.001) and ICS+LABA (41.0% vs. 34.1% vs. 34.5%, p<0.001). LABA+LAMA combination therapy was also more common in improved-grade institutions (16.6%) than in maintained- (13.9%) and declined-grade institutions (13.6%) (p<0.001) (Table 2).
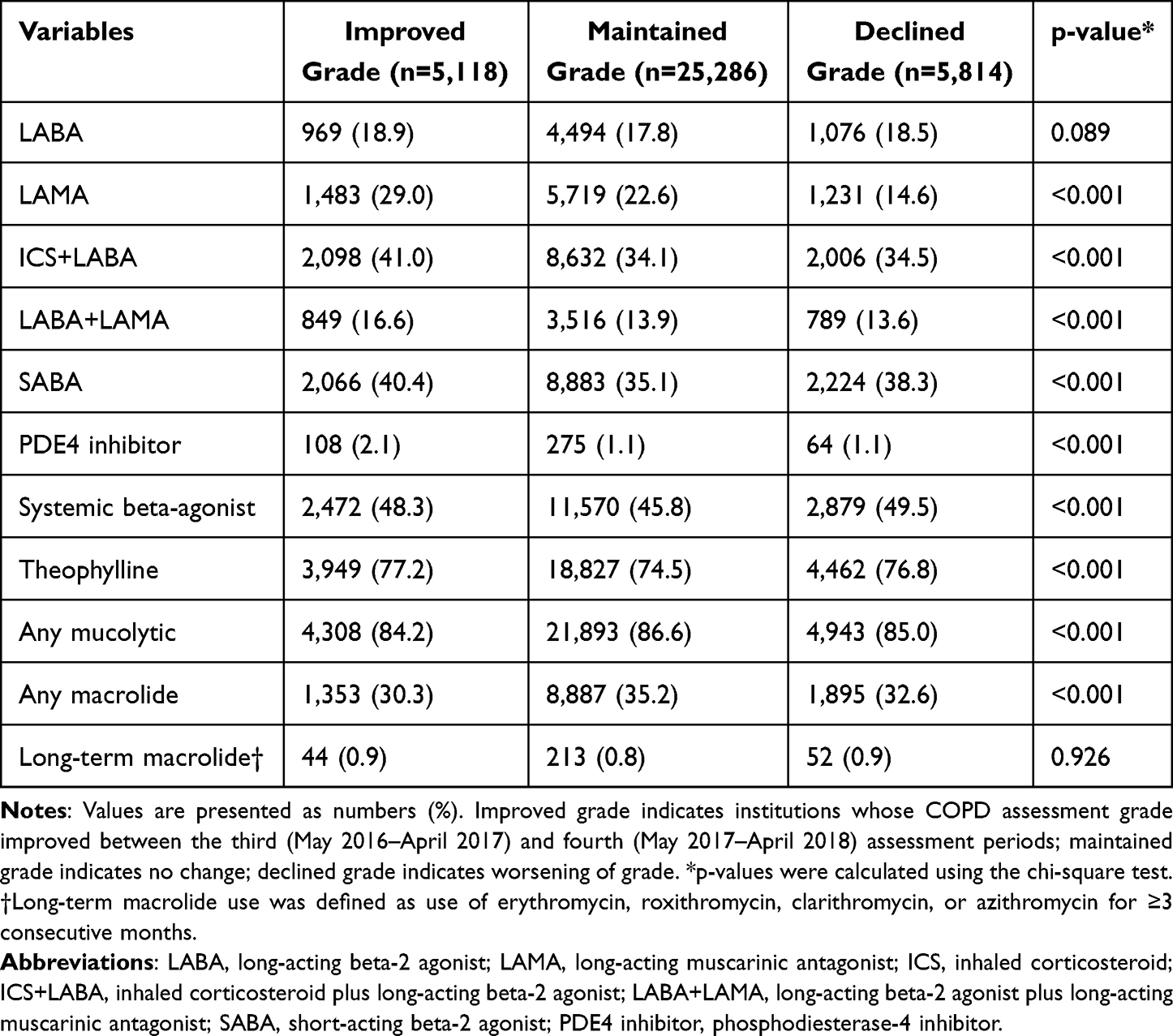 |
Table 2 COPD-Related Medication Use During the Baseline Period According to Changes in Institutional Assessment Grade |
COPD Exacerbation Outcomes
During the fourth assessment period, moderate-to-severe exacerbation outcomes differed according to changes in institutional grade (Table 3). Moderate exacerbations occurred in 21.5% of patients treated at improved-grade institutions, compared with 23.0% and 23.3% in maintained- and declined-grade institutions, respectively (p=0.050). Severe exacerbations were observed in 10.0%, 9.7%, and 11.1% of patients in the improved-, maintained-, and declined-grade groups, respectively (p=0.005). When moderate and severe exacerbations were combined, 26.1% of patients in improved-grade institutions experienced at least one moderate-to-severe exacerbation, compared with 27.8% and 29.2% in maintained- and declined-grade institutions, respectively (p=0.008). The mean number of moderate-to-severe exacerbation events per patient was 1.17 ± 3.63, 1.29 ± 4.24, and 1.32 ± 4.51 in improved-, maintained-, and declined-grade institutions, respectively (p=0.128).
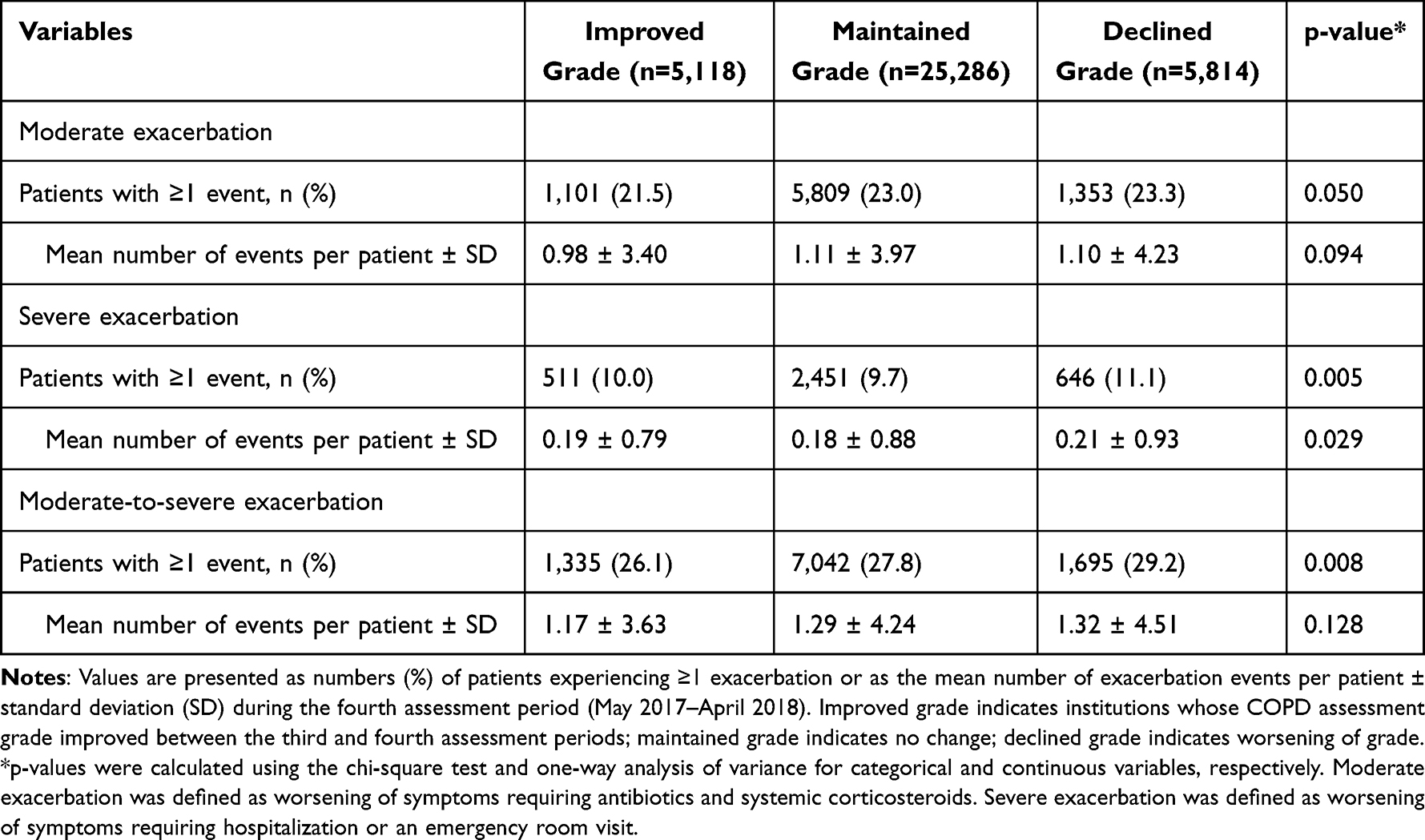 |
Table 3 Moderate-to-Severe COPD Exacerbation Outcomes During the Fourth Assessment Period According to Changes in Institutional Assessment Grade |
Factors Associated with Exacerbations
In negative binomial regression analyses (Figure 1), several factors were independently associated with moderate-to-severe exacerbations. In the adjusted model, older age (adjusted IRR 1.004 per year, 95% CI 1.001–1.006, p=0.015), male sex (adjusted IRR 1.409, 95% CI 1.328–1.495, p<0.001), medical aid status (adjusted IRR 1.588, 95% CI 1.457–1.731, p<0.001), and asthma (adjusted IRR 2.764, 95% CI 2.588–2.951, p<0.001) were significantly associated with increased exacerbation risk. Furthermore, long-term use of roflumilast and macrolides was linked to higher exacerbation risk.
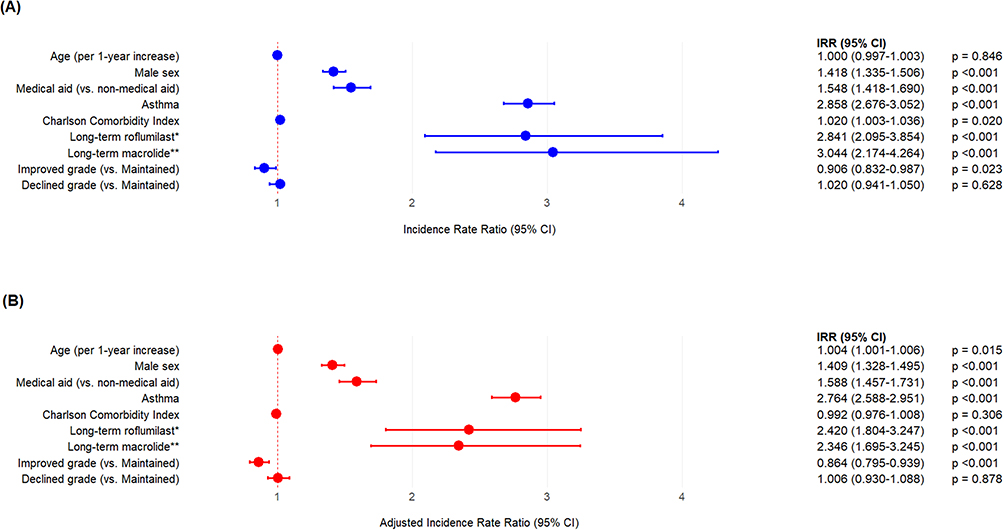 |
Figure 1 Factors associated with moderate-to-severe COPD exacerbations during the fourth assessment period (A) unadjusted analysis; (B), multivariable-adjusted analysis. Abbreviations: IRR, incidence rate ratio; CI, confidence interval. Notes: Improved grade indicates institutions whose COPD assessment grade improved between the third (May 2016–April 2017) and fourth (May 2017–April 2018) assessment periods; declined grade indicates worsening of grade. *Long-term roflumilast use was defined as use for ≥3 consecutive months. **Long-term macrolide use was defined as use of erythromycin, roxithromycin, clarithromycin, or azithromycin for ≥3 consecutive months. |
Using maintained-grade institutions as the reference, treatment at improved-grade institutions was independently associated with a lower risk of moderate-to-severe exacerbations (adjusted IRR 0.864, 95% CI 0.795–0.939, p<0.001), whereas declined-grade institutions revealed no significant difference after adjustment (adjusted IRR 1.006, 95% CI 0.930–1.088, p=0.878).
Discussion
Our analysis of nationwide HIRA claims data investigated whether longitudinal changes in institutional COPD quality assessment grades were associated with the concurrent risk of moderate-to-severe exacerbations in primary and secondary care settings in Korea. We observed that patients treated at institutions with improved assessment grades had a lower risk of exacerbations. This association persisted after adjusting for demographic characteristics, comorbidities, and differences in medication use. Notably, improved-grade institutions demonstrated higher rates of PFT and greater use of long-acting bronchodilators at baseline, indicating that enhanced adherence to guideline-recommended management practices partly accounts for the observed differences in exacerbation risk. In South Korea, all COPD medications are covered by national insurance and dispensed at community pharmacies. Thus, variations in prescription rates reflect physician practices rather than drug availability. Collectively, these findings indicate that institutional performance in national COPD quality assessments aligns with clinically meaningful differences in outpatient COPD outcomes.
Our findings should be interpreted with caution. The observed association is concurrent rather than causal, as both exposure and outcome were evaluated within overlapping time periods. Additionally, residual confounding due to unmeasured severity-related factors and the lack of explicit adjustment for clustering may have influenced the magnitude and precision of our estimates, respectively.
Tertiary hospitals were excluded because of their structural advantages, including specialist availability and widespread access to PFT,15 making it easier to maintain high performance under the process-based national COPD quality assessment system. Indeed, the gap in PFT implementation and inhaled bronchodilator prescription rates is consistently most pronounced between tertiary and non-tertiary institutions in Korea.7 Consequently, grade changes over time are relatively limited in these institutions, reducing the variability required for trajectory-based comparisons. Therefore, we focused on primary and secondary care institutions, where grade trajectories were more heterogeneous and thus more appropriate for evaluating their association with exacerbation risk.
Long-term use of roflumilast and macrolides was associated with a higher risk of exacerbations in the adjusted analysis. However, these agents are typically prescribed for patients with more severe disease or frequent exacerbations.16 Thus, this finding likely reflects confounding by indication rather than a harmful effect of the medications themselves. Specifically, patients receiving these therapies may have had intrinsically higher baseline exacerbation risk despite undergoing preventive treatment.
In this study, exacerbations were identified using a claims-based definition requiring a COPD diagnostic code accompanied by concurrent prescriptions of systemic corticosteroids and antibiotics. Given that systemic corticosteroids and antibiotics may be prescribed for conditions other than COPD, we applied this combined criterion to improve diagnostic specificity and reduce outcome misclassification.17,18 Although this stricter definition may have led to a lower observed prevalence of exacerbations than broader algorithms based on single-agent prescriptions, it reduces the likelihood of false-positive classification and strengthens the internal validity of inter-institutional comparisons. Accordingly, the associations observed in this study are more likely to reflect clinically meaningful moderate-to-severe exacerbations rather than non-specific medication use.
Several considerations qualify the use of exacerbation risk as the outcome of this institutional-level analysis. The HIRA COPD Quality Assessment Program also incorporates COPD-related hospitalization and emergency department visit rates as official indicators for monitoring program performance, in addition to the three process-based indicators used to determine institutional grade (Supplementary Table S1).11 Nevertheless, improvement in institutional grade is unlikely to independently reduce exacerbation risk; it likely reflects more consistent guideline-aligned prescribing, more regular outpatient follow-up, and increased opportunities for inhaler technique education and risk-factor counseling, all of which have been associated with lower exacerbation risk in previous Korean and international COPD cohort studies.4,19 Patient-level behaviors known to strongly influence exacerbation risk, including actual inhaler adherence, inhaler technique, and smoking cessation,20,21 could not be directly measured in our claims-based dataset, and their contribution to the observed associations should be recognized when interpreting these findings.
International real-world studies have consistently demonstrated variability in COPD maintenance treatment patterns across healthcare systems. In a large US administrative cohort, only 37.7% of patients used a controller medication before their first exacerbation and 48.2% during follow-up, with 27.5% receiving any ICS, LABA, or LAMA class medication pre-exacerbation.22 In Chinese primary care cohorts, 33.4% of patients did not receive inhaled therapy, whereas the most commonly prescribed regimens were LABA/ICS (29.9%) and LABA/LAMA/ICS (26.0%), despite recommendations favoring dual long-acting bronchodilator therapy as first-line treatment.23 These observations suggest that the translation of guideline-based COPD management into routine practice remains inconsistent in many settings. In this context, our findings, that improvement in institutional assessment grade was associated with lower exacerbation risk, underscore the potential importance of reinforcing structured, guideline-aligned management strategies in primary and secondary care.
While nationwide administrative claims provide a powerful tool for evaluating real-world clinical practices across a massive population, these data are fundamentally collected for reimbursement purposes rather than clinical research. Consequently, detailed clinical information, including lung function parameters, symptom burden scores, smoking status, inhaler adherence, and blood eosinophil levels, was inherently unavailable. Furthermore, important severity-related proxies, including prior exacerbation history, previous acute-care utilization, baseline controller medication use, and institution-level case mix, were not incorporated as adjustment variables in the primary multivariable model. Although the inclusion of long-term roflumilast and macrolide use in our model served as implicit surrogate markers to partially account for the frequent-exacerbator phenotype, reliance on billing codes inherently limits comprehensive adjustment for baseline disease severity; therefore, residual confounding from unmeasured clinical factors cannot be completely excluded. Furthermore, because these analyses were confined to the pre-approved analytic plans within the closed HIRA Customized Research Database, post-hoc re-extraction of additional severity variables or re-definition of the analytic cohort was unfeasible due to the conclusion of the data access period. Future studies conducted under revised data use agreements will be necessary to directly incorporate individual-level measures of disease severity.
This study had some limitations. First, institutional grade trajectory was defined at the institutional level, and due to the analytic constraints described above, clustering effects within institutions were not explicitly modeled. In the presence of positive intra-cluster correlation, this may lead to underestimation of the variance of the regression coefficients and overestimation of the precision of the point estimates, although the point estimates themselves are not inherently biased by this omission. Nevertheless, considering the large nationwide sample size (n=36,218) and the robust effect size (adjusted IRR, 0.864), the directional association appears to be generally conserved, though precision should be interpreted cautiously. Second, institutional grades were derived from limited process indicators and recalculated annually using absolute thresholds, which may not fully capture the magnitude of quality improvement; finer stratification of exposure by baseline grade, magnitude of change, or care level (primary vs. secondary care) was not undertaken under the analytic constraints described above. Third, we excluded patients with more than one annual reimbursement claim for cancer, renal failure, or cerebrovascular disease to minimize confounding and outcome misclassification. However, this restriction may limit the generalizability of our findings to patients with COPD and these severe comorbid conditions. Furthermore, the possibility of residual outcome misclassification inherent to claims-based ascertainment cannot be fully excluded. Finally, because grade trajectory and exacerbation outcomes were assessed within overlapping periods, the causal direction cannot be definitively established; therefore, our findings should be interpreted as associative rather than causal.
Conclusion
Our nationwide claims-based analysis suggests that improvement in institutional COPD quality assessment grade is associated with a lower concurrent risk of moderate-to-severe exacerbations in primary and secondary care settings. These findings are consistent with the view that institutional indicators of guideline-aligned COPD care may correspond to clinically meaningful differences in patient-level outcomes, supporting continued attention to consistent, guideline-based management.
Use of AI
The draft was initially written in Korean and translated into English with the assistance of ChatGPT, but the English text was subsequently proofread by the English editing service “Editage (www.editage.co.kr).”
Abbreviations
CCI, Charlson Comorbidity Index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; ER, emergency room; GERD, gastroesophageal reflux disease; HIRA, Health Insurance Review and Assessment Service; ICD-10, International Classification of Diseases, 10th Revision; ICS, inhaled corticosteroid; IRR, incidence rate ratio; LABA, long-acting beta-2 agonist; LAMA, long-acting muscarinic antagonist; PDE4, phosphodiesterase-4; PFT, pulmonary function test; SABA, short-acting beta-2 agonist; SD, standard deviation.
Data Sharing Statement
The data that support the findings of this study are available from the Health Insurance Review and Assessment Service (HIRA) of South Korea. Restrictions apply to the availability of these data, which were used under license for the current study and are not publicly available. Data are available from the authors upon reasonable request and with permission of HIRA.
Ethics Approval and Informed Consent
This study conformed to the principles of the Declaration of Helsinki. The Ethics and Review Board of Hanyang University Guri Hospital approved this study (2021-01-013) and waived the requirement for informed consent since it was based on anonymous health claim data.
Consent for Publication
Not applicable. This study used anonymous health insurance claim data and does not contain any individual person’s data in any form (including any individual details, images, or videos).
Acknowledgments
This study was supported by Konkuk University in 2025. The authors thank the Health Insurance Review and Assessment Service (HIRA) for providing access to the national claims database used in this study.
Author Contributions
Conceived and designed the study: Youlim Kim, Hyun Lee, and Ji-Yong Moon. Collected the data: Kyungjoo Kim. Contributed data and analytical tools: Kyungjoo Kim. Performed the analyses: Kyungjoo Kim. Wrote this paper: Sung Woo Moon, Youlim Kim, Hyun Lee, and Ji-Yong Moon. Provided study supervision: Chin Kook Rhee and Ji-Yong Moon. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; provided final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant for its conduct.
Disclosure
Dr Youlim Kim reports lecture fees from AstraZeneca, Sanofi, GlaxoSmithKline, Kolon, Organon Korea, Daewon, Boryung, Hanlim, SAMJIN, Dongkook Pharmaceutical and Han Wha Pharma. She also serves as an Editorial Board Member and a Multimedia Liaison Member for the journal CHEST. In addition, she also serves as an editorial board member for the BMC pulmonary medicine. The authors report no other conflicts of interest in this article.
References
1. Venkatesan P. GOLD COPD report: 2025 update. Lancet Respir Med. 2025;13(1):e7–11. doi:10.1016/S2213-2600(24)00413-2
2. Kim SH, Park JE, Yang B, Kim SY, Kim YY, Park JH. National trend in the prevalence and mortality of COPD in South Korea from 2008 to 2017. BMJ Open Respir Res. 2024;11(1):e002391. doi:10.1136/bmjresp-2024-002391
3. Lee EG, Rhee CK. Epidemiology, burden, and policy of chronic obstructive pulmonary disease in South Korea: a narrative review. J Thorac Dis. 2021;13(6):3888–3897. doi:10.21037/jtd-20-2100
4. Bollmeier SG, Hartmann AP. Management of chronic obstructive pulmonary disease: a review focusing on exacerbations. Am J Health Syst Pharm. 2020;77(4):259–268. doi:10.1093/ajhp/zxz306
5. Blasi F, Cesana G, Conti S, et al. The clinical and economic impact of exacerbations of chronic obstructive pulmonary disease: a cohort of hospitalized patients. PLoS One. 2014;9(6):e101228. doi:10.1371/journal.pone.0101228
6. Chinai B, Hunter K, Roy S. Outpatient management of chronic obstructive pulmonary disease: physician adherence to the 2017 Global Initiative for Chronic Obstructive Lung Disease guidelines and its effect on patient outcomes. J Clin Med Res. 2019;11(8):556–562. doi:10.14740/jocmr3888
7. Kim KY, Yoo KH, Choi HS, et al. Nationwide quality assessment of treatment for chronic obstructive pulmonary disease. J Thorac Dis. 2020;12(12):7174–7181. doi:10.21037/jtd-20-905
8. de Klein MM, Peters JB, van ‘t Hul AJ, et al. Comparing health status between patients with COPD in primary, secondary and tertiary care. NPJ Prim Care Respir Med. 2020;30(1):39. doi:10.1038/s41533-020-00196-7
9. Chung SM, Lee SY. Evaluation of Appropriate Management of Chronic Obstructive Pulmonary Disease in Korea: based on Health Insurance Review and Assessment Service (HIRA) Claims. Tuberc Respir Dis. 2017;80(3):241–246. doi:10.4046/trd.2017.80.3.241
10. Choi JY, Kim KU, Kim DK, et al. Pulmonary rehabilitation is associated with decreased exacerbation and mortality in patients with COPD: a nationwide Korean study. Chest. 2024;165(2):313–322. doi:10.1016/j.chest.2023.09.026
11. Koo HK, Rhee CK, Min KH, et al. A decade of healthcare quality assessment for chronic obstructive pulmonary disease in South Korea: trends and implications (2014-2023). Tuberc Respir Dis. 2025;88(4):615–621. doi:10.4046/trd.2025.0030
12. Health Insurance Review and Assessment Service (HIRA). 2021 (8th) Quality Assessment Report for Chronic Obstructive Pulmonary Disease. Health Insurance Review and Assessment Service; 2023.
13. Park HJ, Kim SR, Kim S, et al. Influence of government-driven quality assessment program on patients with chronic obstructive pulmonary disease. Respir Res. 2021;22(1):87. doi:10.1186/s12931-021-01684-1
14. Hilbe JM. Negative Binomial Regression. Cambridge University Press; 2011.
15. Park HJ, Byun MK, Kim HJ, et al. Asthma-COPD overlap shows favorable clinical outcomes compared to pure COPD in a Korean COPD cohort. Allergy Asthma Immunol Res. 2017;9(5):431–437. doi:10.4168/aair.2017.9.5.431
16. Yawn BP, Mintz ML, Doherty DE. GOLD in practice: chronic obstructive pulmonary disease treatment and management in the primary care setting. Int J Chron Obstruct Pulmon Dis. 2021;16:289–299. doi:10.2147/COPD.S222664
17. Salwan AA, Spigt M, Laue J, Melbye H. Predictors of treatment with antibiotics and systemic corticosteroids for acute exacerbations of asthma and chronic obstructive pulmonary disease in primary care. BMC Fam Pract. 2015;16:40. doi:10.1186/s12875-015-0256-3
18. Dragonieri S, Carratu P, Ranieri T, Carpagnano GE, Resta O. Criteria of prescription of antibiotics and systemic corticosteroids among pulmonologists and general practitioners during asthma and COPD exacerbations: a southern Italian survey. Acta Biomed. 2021;92(3):e2021165. doi:10.23750/abm.v92i3.9909
19. Park HJ, Byun MK, Kim T, et al. Frequent outpatient visits prevent exacerbation of chronic obstructive pulmonary disease. Sci Rep. 2020;10(1):6049. doi:10.1038/s41598-020-63064-x
20. Suh HS, Chang MS, Yu I, et al. Adherence to long-acting inhaler use for initial treatment and acute exacerbation of chronic obstructive pulmonary disease: a retrospective cohort study. J Pers Med. 2022;12(12):2073. doi:10.3390/jpm12122073
21. Vauterin D, Van Vaerenbergh F, Grymonprez M, Vanoverschelde A, Lahousse L. Medication adherence to inhalation therapy and the risk of COPD exacerbations: a systematic review with meta-analysis. BMJ Open Respir Res. 2024;11(1):e001964. doi:10.1136/bmjresp-2023-001964
22. Bogart M, Germain G, Laliberté F, Lejeune D, Duh MS. Real-world treatment patterns and switching following moderate/severe chronic obstructive pulmonary disease exacerbation in patients with commercial or Medicare insurance in the United States. Int J Chron Obstruct Pulmon Dis. 2023;18:1575–1586. doi:10.2147/COPD.S398816
23. Pei H, Su Y, Jing G, et al. Patterns and adherence to GOLD-recommended inhaled therapy in chronic obstructive pulmonary disease (COPD) patients with acute exacerbation history in primary care in China. Int J Chron Obstruct Pulmon Dis. 2026;21:566724. doi:10.2147/COPD.S566724
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.