Back to Journals » International Journal of General Medicine » Volume 18
Association Between Heparin-Binding Protein and Extubation Outcomes in ARDS: A Retrospective Cohort Study
Received 9 August 2025
Accepted for publication 28 November 2025
Published 9 December 2025 Volume 2025:18 Pages 7371—7380
DOI https://doi.org/10.2147/IJGM.S559258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Yinchao Zhou,1 Wei Li,2 Zhouzhou Dong1,3
1Department of Critical Care Medicine, Ningbo Medical Center Lihuili Hospital, Ningbo, Zhejiang, 315000, People’s Republic of China; 2School of Life Sciences, Westlake University, Hangzhou, Zhejiang, 310030, People’s Republic of China; 3Health Science Center, Ningbo University, Ningbo, Zhejiang, 315211, People’s Republic of China
Correspondence: Zhouzhou Dong, Department of Critical Care Medicine, Ningbo Medical Center Lihuili Hospital, Ningbo, Zhejiang, 315000, People’s Republic of China, Tel +86 13858287868, Email [email protected]
Background: Extubating from mechanical ventilation is crucial in acute respiratory distress syndrome (ARDS). Heparin-binding protein (HBP) has been closely linked to ARDS development. We aimed to evaluate the association between HBP trajectories and extubation outcomes in ARDS patients.
Patients and Methods: This was a retrospective study of ARDS patients who were ready for extubation. Group-based trajectory modeling was applied to identify subgroups with similar HBP trajectories in this cohort. Logistic regression was used to elucidate the relationship between different trajectories and extubation success.
Results: Overall, this study enrolled 267 patients from September 2023 to March 2025. Five HBP trajectories were identified including traj1 (HBP stable at extremely low level), traj2 (HBP stable at low level), traj3 (HBP descending from a high level to a low level), traj4 (HBP stable at moderate level), and traj5 (HBP stable at high level). The rates of successful extubation were 86.27%, 61.91%, 71.11%, 50.00%, and 40.98% respectively (P < 0.001). In addition, Logistic regression indicated that patients in traj2, traj3, traj4, and traj5 was associated with significantly decreased extubation success compared to those in traj1 group (odd ratio [OR] = 0.239, 95% confidence interval [CI]: 0.091– 0.630; OR = 0.195, 95% CI: 0.054– 0.706; OR = 0.143, 95% CI: 0.056– 0.368; OR = 0.081, 95% CI: 0.030– 0.220, respectively).
Conclusion: In mechanically ventilated ARDS patients, distinct HBP trajectories demonstrate significant associations with extubation outcomes, suggesting their potential utility in refining extubation protocols in critical care settings.
Keywords: acute respiratory syndrome, heparin-binding protein, group-based trajectory modeling, extubation outcome
Introduction
Acute respiratory distress syndrome (ARDS) is an acute respiratory illness characterized by bilateral chest radiographical opacities with severe hypoxemia due to non-cardiogenic pulmonary oedema. It represents a critical condition in intensive care unit (ICU) with mortality rates as high as 43%.1–3 Mechanical ventilation is a critical lifesaving intervention for ARDS;4 however, 10–20% of patients experience difficult extubation,5 and extubation failure is strongly associated with adverse clinical outcomes.6 Accurate prediction of extubation success in ARDS patients is therefore paramount.7
The pathophysiology of ARDS is complex and is characterized by injury to pulmonary vascular endothelial cells and alveolar epithelia.8 This pathological process leads to increased capillary permeability, facilitating the leakage of fluid and proteins into the alveolar and interstitial spaces, which ultimately impairs pulmonary function.9 In conclusion, pulmonary vascular permeability constitutes the pivotal mechanism underlying the severity of pulmonary injury in ARDS, serving as a critical determinant of both disease progression and clinical prognosis.10 Consequently, it is essential to evaluate the dynamics of pulmonary vascular permeability before extubation for ARDS.
Heparin-binding protein (HBP), a neutrophil-derived granular protein, is stored within secretory vesicles and azurophilic granules (primary granules) and is rapidly released upon cellular activation.11 HBP is an emerging clinical biomarker which plays a pivotal role in the vascular leakage and pulmonary edema characteristic of ARDS by mediating proinflammatory cytokine release, immune cell chemotaxis, and endothelial damage.12–14 Clinical investigations have validated that ARDS exhibit significantly elevated HBP, with this biomarker elevation demonstrating strong correlations with both the development and pathophysiological severity of the disorder.15 However, research investigating the relationship between the dynamic changes in the HBP and extubation outcome among ARDS patients remain limited.16
In summary, our study will conduct longitudinal HBP monitoring and leveraged group-based trajectory modeling (GBTM) to investigate associations between different HBP trajectories and extubation outcomes in ARDS patients. The findings aim to establish a predictive tool to guide ventilator weaning strategies and optimize clinical decision-making.
Material and Methods
Study Design and Participants
In this study, ARDS patients who were admitted to the ICU of Ningbo Medical Center Lihuli Hospital between September 2023 to March 2025 were enrolled. The diagnosis of ARDS was established in accordance with the new global criteria.17 The details of diagnostic criteria for ARDS are shown in the Supplementary Material. This study was approved by the ethics of Ningbo Medical Center Lihuli Hospital (KY2025SL228-01). Informed consent was waived for this retrospective study in accordance with institutional/ethics committee guidelines.
We hypothesized that different patterns of change in HBP were associated with the extubation outcomes of ARDS. The inclusion criteria were as follow: (a) stayed in ICU for more than six days; (b) complete clinical data; (c) age > 18 years. The exclusion criteria were as follow: (a) extubation within 6 days after enrolled; (b) patients with tracheostomy; (c) patients requesting discharge during treatment.
Date Collection
All data were extracted from the critical care electronic database. The baseline characteristics including age, gender, body mass index (BMI), chronic disease, Acute Physiology and Chronic Health Evaluation II (APACHE II) score,18 Sequential Organ Failure Assessment (SOFA) score,19 PaO2/FiO2 at enrolled, and primary disease of ARDS. HBP levels were measured daily from 1–6 days after enrolled.
Clinical Outcomes
The primary outcome was extubation success, which was defined as sustained spontaneous breathing for more than 48 h following extubation without mechanical ventilation (invasive or noninvasive). The secondary outcomes included ventilator-free days through 28 days, length of ICU stays, length of hospital stays, and ICU mortality.
Statistical Analysis
The Kolmogorov–Smirnov test examined the normality of continuous variables. For normally distributed, continuous variables, data are expressed as the means ± standard deviations and were compared with the t test. For non-normally distributed, continuous variables, data are presented as [M (P25, P75)] medians (interquartile ranges) and were compared using the Mann−Whitney U-test. For categorical variables, data are presented as numbers (%), and the Chi-square test was used for comparisons.
Trajectories of HBP were categorized using GBTM, implemented in R (version 4.3.3) with the “gbmt” package. GBTM predicted trajectories for each group, estimated each individual’s probability of group membership, and assigned individuals to groups based on their highest probabilities, which were modeled by a finite set of different polynomial time functions. Then, we identified the optimal number of trajectory classes using Bayesian Information Criterion (BIC) values and Akaike Information Criterion (AIC), average posterior probability of assignment (AvePP) (> 70%), odds of correct classification (OCC) (> 5), minimal class sizes (> 5% of sample size) and clinical experience.20
We conducted a two-step regression analysis to identify factors associated with extubation success. First, we conducted univariate logistic regression for different patterns of change in HBP and other clinical variables (including age, gender, BMI, SOFA score, primary disease of ARDS, PaO2/FiO2 at enrolled, and number of chronic diseases) to screen for potential associations with extubation success. We then introduced potential confounders (P < 0.1) into the multivariate logistic regression model to assess the relationship between the relationships between HBP trajectories and the extubation success. We performed a prespecified subgroup analysis for extubation success by the age and SOFA score, using the median values of the cohort ([Median] years for age and [Median] points for SOFA score) as the cut-offs.
Statistical tests were two-sided, and a P value < 0.05 was considered significant. The analysis was performed using R (version 4.3.3) software and GraphPad Prism 9.3 software.
Results
Characteristics of the Study Population
Between September 2023 to March 2025, 267 patients were included in the analysis. A total of 156 patients were ultimately successfully extubated. The flowchart is shown in Figure 1. The cohort is predominately male (73.78%), with a median age of 72 years old [interquartile range (IQR): 63–80] and a median APACHE II score of 21 (IQR:16.00–24.00). The primary disease of ARDS was pulmonary disease. The baseline characteristics of the patients are summarized in Table 1. The HBP of first day was lower in patients who were successfully extubated compared with those with extubation failure (P < 0.05). No statistically significant differences were observed in other indicators between the successful and failed groups (all P > 0.05).
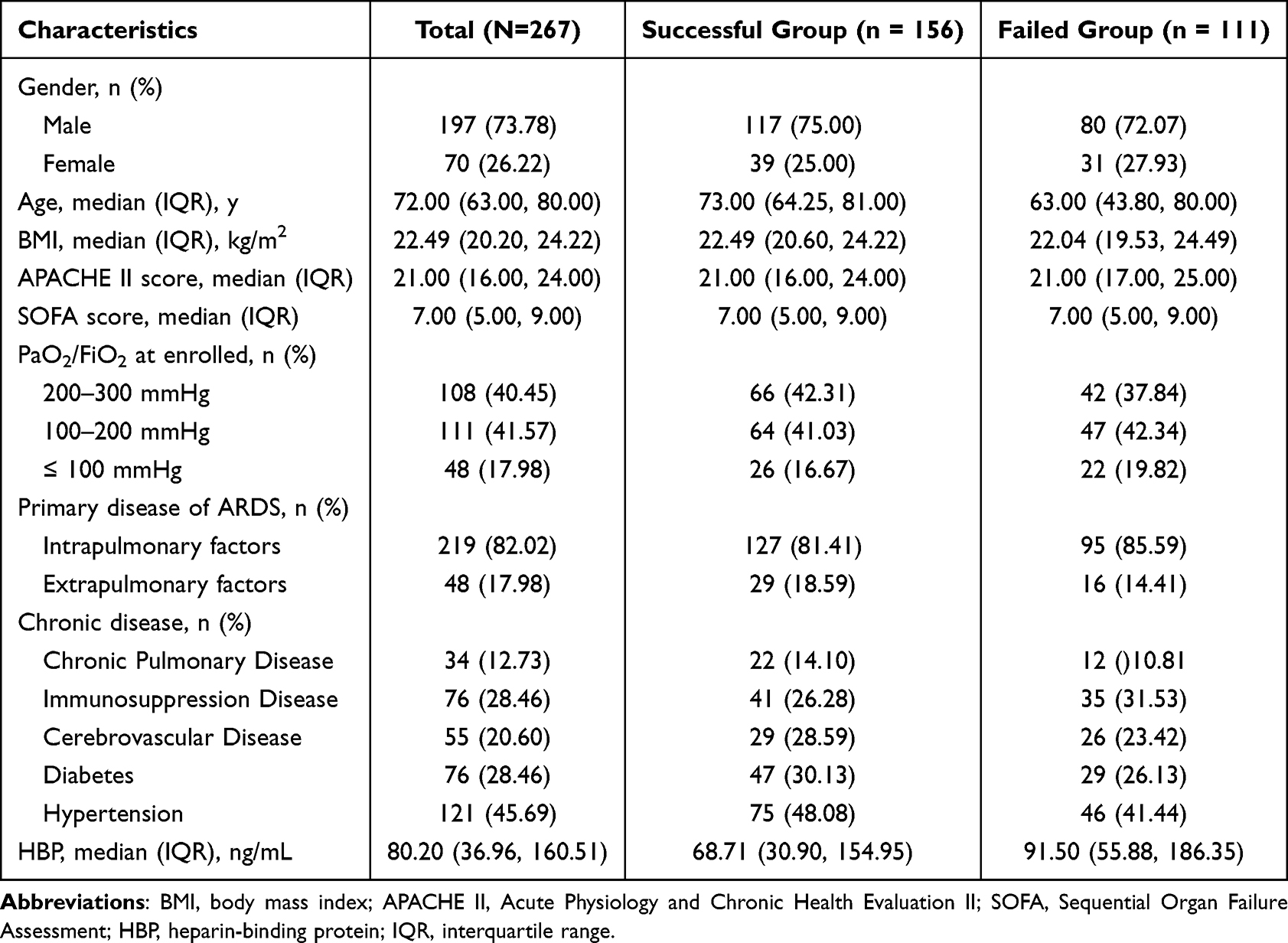 |
Table 1 Baseline Characteristics of the Study Subjects |
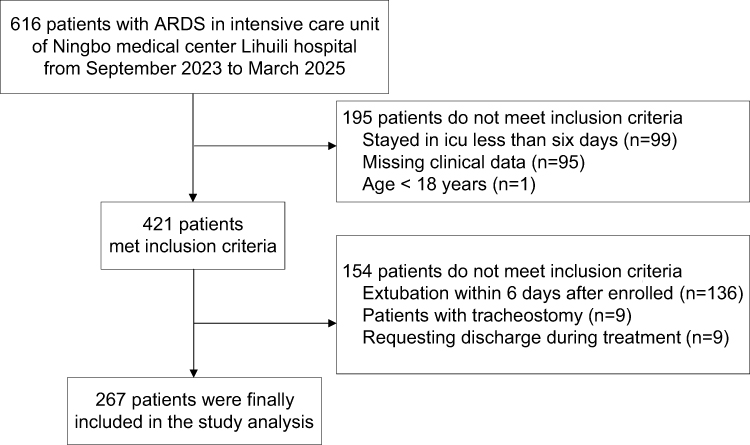 |
Figure 1 Flowchart of the study. |
Group-Based Trajectory Modeling
With the polynomial order fixed at three, we explored group-based trajectory models with 1 to 6 subgroups. Model fit indices are detailed in Table 2. The results demonstrated that both BIC and AIC values progressively decreased with an increasing number of subgroups. After comprehensive consideration of clinical relevance and model parsimony, a 5-subgroup trajectory configuration was ultimately determined to be optimal for this study. After setting the number of trajectory groups to five, parameter estimation results for different polynomial orders in each trajectory group are presented in Table S1. The results demonstrated that when the polynomial order was set to 3 in all trajectory groups, the associated P-values were consistently less than 0.05. For internal validation, all HBP trajectory groups demonstrated robust classification accuracy with AvePP > 70%, OCC > 5, and strong concordance between posterior probabilities of group membership (Pj) and estimated prior probabilities (πj), indicating satisfactory model fit as detailed in Table S2.
 |
Table 2 Objective Criteria for Determining the Number of HBP Trajectory Groups Using GBTM in ARDS Patients |
Characteristics and Clinical Outcomes of Various HBP Trajectories
Based on the HBP trajectory, ARDS patients were classified into five distinct groups, including traj1 (persistently extremely low HBP, n = 51), traj2 (persistently low HBP, n = 63), traj3 (high-to-low transitional HBP, n = 18), traj4 (persistently moderate HBP, n = 74), and traj5 (persistently high HBP, n = 61). All trajectories were shown in Figure 2, and the daily HBP of five groups are detailed in Table S3.
 |
Figure 2 Identification of heparin-binding protein trajectories. Abbreviation: HBP, Heparin-binding protein. Notes: traj1, stable at extremely low level; traj2, stable at low level; traj3, descending from a high level to a low level; traj4, stable at moderate level; traj5, stable at high level. |
The extubation success rate progressively decreased from group traj1 to traj5, with statistically significant differences observed between groups (P < 0.001). Moreover, ventilator-free days through 28 days and ICU mortality showed statistically significant differences among the five groups (all P < 0.05). Detailed comparative data are presented in Table 3.
 |
Table 3 Clinical Outcomes Among the Five Trajectory Groups |
Association Between HBP Trajectories and Extubation Success
Logistic regression analysis illustrated that extubation success was significantly different among the five groups. The relationship of different HBP trajectories with extubation success is presented in Table 4. The traj2, traj3, trje4, and traj5 was associated with decreased extubation success rate when compared with the traj1 (odd ratio [OR] = 0.239, 95% confidence interval [CI]: 0.091–0.630; OR = 0.195, 95% CI: 0.054–0.706; OR = 0.143, 95% CI: 0.056–0.368, OR = 0.081, 95% CI: 0.030–0.220, respectively). The observed associations persisted after adjustment for potential confounders, including age, gender, BMI, SOFA score, primary disease of ARDS, PaO2/FiO2 at enrolled, and number of chronic diseases.
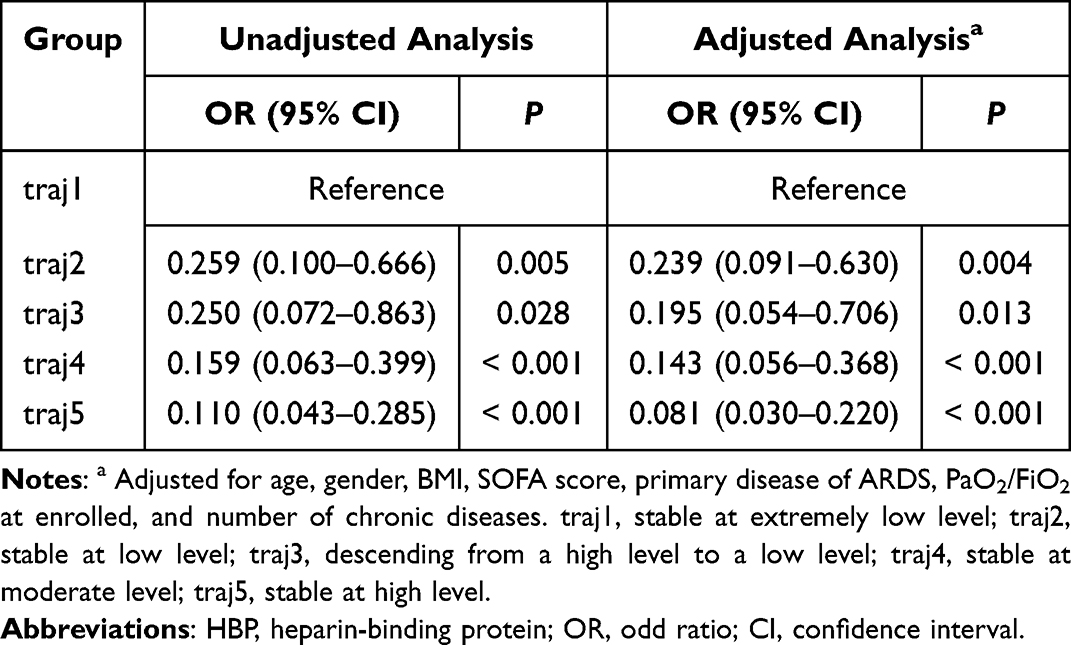 |
Table 4 Relationship of HBP Trajectories and Extubation Success |
Subgroup Analysis
The prespecified subgroup analysis by age and SOFA score revealed non-significant interaction effects (all P > 0.05) between these variables and HBP trajectories. However, robust associations between distinct HBP trajectories and extubation outcomes were observed in patients aged ≥ 72 years, and SOFA scores < 7 or ≥ 7 (Figure 3).
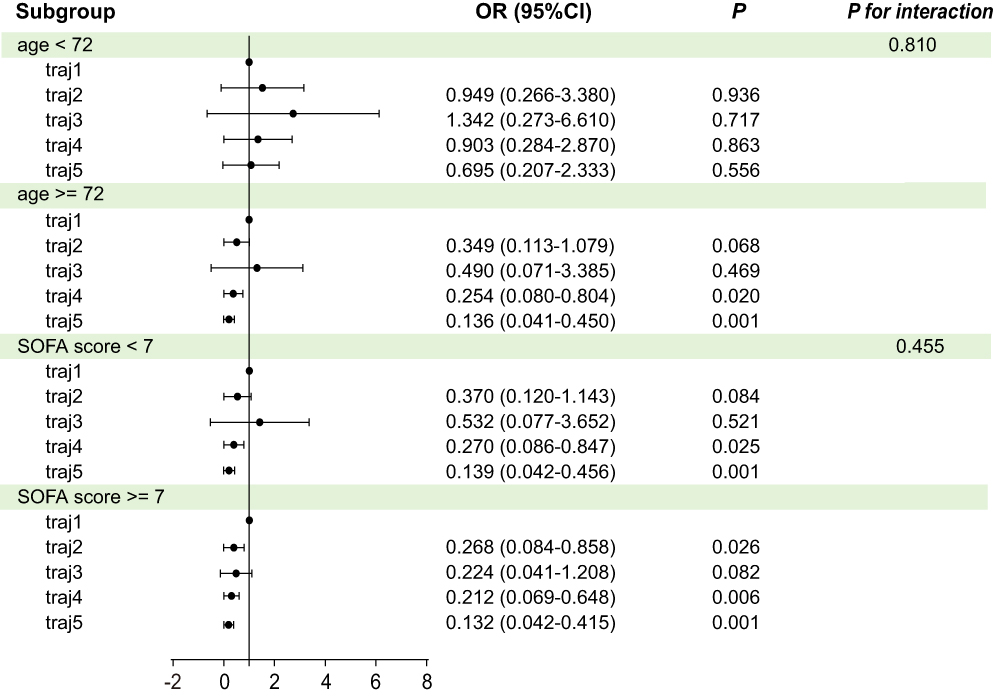 |
Figure 3 Subgroup analysis of the association between heparin-binding protein trajectories and extubation success. Abbreviations: SOFA, Sequential Organ Failure Assessment; OR, odd ratio; CI, confidence interval. Notes: traj1, stable at extremely low level; traj2, stable at low level; traj3, descending from a high level to a low level; traj4, stable at moderate level; traj5, stable at high level. |
Discussion
In this study, five distinct HBP trajectories were identified in a cohort of ARDS patients. Those patients with higher HBP were associated with a higher risk of failed extubation compared with patients whose HBP stained at a lower level. This association remained significant after adjusting potential confounding factors. These findings may assist clinicians in identifying high-risk populations for extubation failure and provide clinical guidelines for extubation decision.
Although the pathophysiology of ARDS is complex and not fully elucidated, it is widely accepted that ARDS represents a severe pulmonary manifestation of systemic inflammatory response syndrome (SIRS).21 The activation of inflammatory cells (particularly polymorphonuclear leukocytes, PMNs), arachidonic acid metabolic byproducts, and other inflammatory mediators have been identified as pivotal drivers in the progression of SIRS and ARDS.22,23 This cellular mechanism predominantly manifests through PMN-induced structural damage to the alveolar-capillary membrane via pro-inflammatory cytokine release, facilitates the leakage of fluid and protein into the interstitial spaces and alveoli, culminating in ARDS.24,25 Thus, PMNs play a central role in the pathogenesis of ARDS.
HBP, a key component of granules in PMNs, plays a pivotal role in initiating the cascade of inflammation and enhancing vascular permeability.26,27 Bentzer et al demonstrated that HBP binds to glycosaminoglycans on endothelial cell surfaces, subsequently activating protein kinase C and Rho kinase pathways. This cascade triggers Ca2⁺ influx, induces cytoskeletal rearrangement and endothelial cell contraction, and disrupts intercellular junctions between pulmonary capillary endothelial cells, collectively leading to increased vascular permeability.12,28 Furthermore, HBP exhibits chemoattractant activity, promoting the recruitment of monocytes, macrophages, and other inflammatory cells to pulmonary inflammatory sites. Upon accumulation in the lungs, these cells release proinflammatory mediators that exacerbate local inflammation and further amplify pulmonary capillary hyperpermeability.29 Collectively, these mechanisms underscore the pivotal role of HBP in modulating the permeability of pulmonary microvascular endothelial barriers.
Recent evidence demonstrates significantly elevated plasma HBP levels in ARDS patients compared to those with cardiogenic pulmonary edema, with a strong correlation observed between HBP and the severity of lung injury.30 Furthermore, Xue et al validated the utility of HBP as a predictive biomarker for clinical deterioration in respiratory failure patients.31 Notably, our findings revealed that successful extubation group exhibited significantly lower HBP levels of first day than failed group. These collective data support the role of HBP as a robust indicator for evaluating alteration in pulmonary microvascular permeability and stratifying lung injury severity in ARDS. Nevertheless, a critical knowledge gap remains regarding the longitudinal dynamicsof HBP and their relationship with extubation outcomes of ARDS.
In this study, we identified five groups of HBP trajectory groups based on GBTM. We observed that patients in the persistent moderate or high level HBP trajectory groups exhibited significantly lower extubation success rates compared to the persistent extremely low level HBP group. Logistic regression analyses confirmed that this inverse association remained significant after adjusting for confounding variables. These findings suggest that sustained moderate or high HBP levels in ARDS patients may perpetuate alveolar-capillary barrier dysfunction, driving progressive pulmonary edema, unresolved inflammatory infiltration, and consequently more severe lung injury. Clinically, this biological persistence correlates with prolonged mechanical ventilation dependence, higher risks of extubation failure and ICU mortality, and serve as an indicator of critical disease progression requiring vigilant monitoring. Notably, patients demonstrating a descending HBP trajectory (from a high level to a low level) achieved superior extubation outcomes and lower ICU mortality compared to those with static elevated HBP levels, which is a critical distinction unattainable through single-point HBP assessments. Although these preliminary observations are consistent with Sun et al, who reported that rapid HBP reduction was associated with improved survival in multiorgan dysfunction syndrome, large-scale prospective studies are needed for validation.32 Collectively, dynamic HBP trajectory monitoring provides enhanced prognostic utility over static measurements for guiding extubation decision-making in ARDS management.
Subgroup analyses stratified by age and SOFA scores demonstrated persistent associations between HBP trajectory patterns and extubation outcomes, with particularly robust correlations observed in patients aged ≥ 72 years and across SOFA score subpopulations. These findings align with Wang et al’s cohort study, which showed that patients exhibiting extreme HBP elevation typically present with advanced age, compromised immunity, multiple comorbidities, and elevated mortality risk.16 Clinically, these data suggest that ARDS patients aged ≥72 years with sustained moderate-to-high HBP levels warrant prioritized clinical attention and early targeted therapeutic interventions.
HBP trajectories could help clinicians stratify patients at high risk for extubation failure, enabling closer monitoring and timely interventions. Future research should focus on establishing specific HBP cut-off values to guide clinical decision-making.
This study has several limitations. Firstly, the sample size of our study was moderate, and all participants were recruited from a single center. Secondly, as a retrospective study, we cannot verify a causal relationship between HBP trajectories and extubation outcomes. Therefore, a larger, multi-centre study is needed to further validate our results.
Conclusion
In conclusion, our study identifies distinct HBP trajectories that are strongly associated with extubation success in ARDS, providing a potential tool for risk stratification. This suggests that monitoring HBP dynamics could help clinicians identify patients at high risk for extubation failure, who may benefit from more vigilant monitoring and tailored weaning protocols. Future research should focus on validating these trajectories prospectively and establishing specific HBP cut-off values to guide clinical decision-making.
Abbreviations
ARDS, acute respiratory distress syndrome; HBP, heparin-binding protein; ICU, intensive care unit; GBTM, group-based trajectory modeling; BMI, body mass index; APACHE II, acute physiology and chronic health evaluation II; SOFA, sequential organ failure assessment; BIC, Bayesian Information Criterion; AIC, Akaike Information Criterion; AvePP, average posterior probability of assignment; OCC, odds of correct classification; SIRS, systemic inflammatory response syndrome; PMNs, polymorphonuclear leukocytes; IQR, interquartile range; OR, odd ratio; CI, confidence interval.
Data Sharing Statement
The data that support the findings of this study are available upon reasonable request from the corresponding author (Zhouzhou Dong) and with permission from Ningbo Medical Center Lihuili Hospital.
Institutional Review Board Statement
This study was approved by the ethics of Ningbo Medical Center Lihuili Hospital (approval number: KY2025SL228-01; approval date: June 19, 2025).
Ethics Approval and Consent to Participate
This retrospective study was approved by the Ethics Committee of Ningbo Medical Center Lihuili Hospital, which waived the requirement for obtaining individual patient informed consent due to the retrospective nature of the study and the use of anonymized data. All patient data were anonymized and de-identified prior to analysis to protect patient privacy and confidentiality, and the study complied with the ethical principles of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Zhejiang Provincial Natural Science Foundation of China under Grant No. LTGY24H150001.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Meyer NJ, Gattinoni L, Calfee CS. Acute respiratory distress syndrome. Lancet. 2021;398(10300):622–637. doi:10.1016/S0140-6736(21)00439-6
2. Sakr Y, François B, Sole-Violan J, et al. Temporal changes in the epidemiology, management, and outcome from acute respiratory distress syndrome in European intensive care units: a comparison of two large cohorts. Crit Care. 2021;25(1):87. doi:10.1186/s13054-020-03455-8
3. Gorman EA, CM O, McAuley DF. Acute respiratory distress syndrome in adults: diagnosis, outcomes, long-term sequelae, and management. Lancet. 2022;400(10358):1157–1170. doi:10.1016/S0140-6736(22)01439-8
4. Wick KD, Ware LB, Matthay MA. Acute respiratory distress syndrome. BMJ. 2024;387:e076612. doi:10.1136/bmj-2023-076612
5. De Jong A, Talmor D, Jaber S. How to optimize extubation? Intensive Care Med. 2023;49(3):337–340. doi:10.1007/s00134-022-06964-y
6. Jaber S, Quintard H, Cinotti R, et al. Risk factors and outcomes for airway failure versus non-airway failure in the intensive care unit: a multicenter observational study of 1514 extubation procedures. Crit Care. 2018;22(1):236. doi:10.1186/s13054-018-2150-6
7. Liu Y, Zhou Y, Liu P, Ying W, Wu H, Dong Z. Combined lung and diaphragm ultrasound predicts extubation outcomes in ARDS: a prospective study. Eur J Med Res. 2024;29(1):510. doi:10.1186/s40001-024-02103-z
8. Al-Husinat L, Azzam S, Al Sharie S, et al. A narrative review on the future of ARDS: evolving definitions, pathophysiology, and tailored management. Crit Care. 2025;29(1):88. doi:10.1186/s13054-025-05291-0
9. Bos LDJ, Ware LB. Acute respiratory distress syndrome: causes, pathophysiology, and phenotypes. Lancet. 2022;400(10358):1145–1156. doi:10.1016/S0140-6736(22)01485-4
10. Xu P, He Y, Cao Y. Research progress of biomarkers of pulmonary microvascular endothelial cells in acute respiratory distress syndrome. Chin J Emerg Med. 2022;31. doi:10.3760/cma.j.issn.1671-0282.2022.04.026
11. Wu YL, Yo CH, Hsu WT, et al. Accuracy of Heparin-Binding Protein in Diagnosing Sepsis: a Systematic Review and Meta-Analysis. Crit Care Med. 2021;49(1):e80–e90. doi:10.1097/CCM.0000000000004738
12. Bentzer P, Fisher J, Kong HJ, et al. Heparin-binding protein is important for vascular leak in sepsis. Intensive Care Med Exp. 2016;4(1):33. doi:10.1186/s40635-016-0104-3
13. Kaukonen KM, Linko R, Herwald H, et al. Heparin-binding protein (HBP) in critically ill patients with influenza A(H1N1) infection. Clin Microbiol Infect. 2013;19(12):1122–1128. doi:10.1111/1469-0691.12156
14. Liu Y, Ma S, Wang X, et al. The role of β2 integrin associated heparin-binding protein release in ARDS. Life Sci. 2018;203:92–98. doi:10.1016/j.lfs.2018.04.029
15. Lin Q, Shen J, Shen L, Zhang Z, Fu F. Increased plasma levels of heparin-binding protein in patients with acute respiratory distress syndrome. Crit Care. 2013;17(4):R155. doi:10.1186/cc12834
16. Wang K, Jiang Y, Yang X. Clinical Observation of Extremely Elevated Hepstatin-Binding Protein. Chin J Emerg Med. 2022;31(9):1270–1274. doi:10.3760/cma.j.issn.1671-0282.2022.09.020
17. Matthay MA, Arabi Y, Arroliga AC, et al. A New Global Definition of Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2024;209(1):37–47. doi:10.1164/rccm.202303-0558WS
18. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. Apache II: a severity of disease classification system. Crit Care Med. 1985;13:818e29.
19. Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22(7):707–710. doi:10.1007/BF01709751
20. Nagin DS, Jones BL, Elmer J. Recent Advances in Group-Based Trajectory Modeling for Clinical Research. Annu Rev Clin Psychol. 2024;20(1):285–305. doi:10.1146/annurev-clinpsy-081122-012416
21. Nie J, Zhou L, Tian W, et al. Deep insight into cytokine storm: from pathogenesis to treatment. Signal Transduct Target Ther. 2025;10(1):112. doi:10.1038/s41392-025-02178-y
22. Flower L, Vozza EG, Bryant CE, Summers C. Role of inflammasomes in acute respiratory distress syndrome. Thorax. 2025;80(4):255–263. doi:10.1136/thorax-2024-222596
23. Ma W, Tang S, Yao P, et al. Advances in acute respiratory distress syndrome: focusing on heterogeneity, pathophysiology, and therapeutic strategies. Signal Transduct Target Ther. 2025;10(1):75. doi:10.1038/s41392-025-02127-9
24. Burkard P, Schonhart C, Vögtle T, et al. A key role for platelet GPVI in neutrophil recruitment, migration, and NETosis in the early stages of acute lung injury. Blood. 2023;142(17):1463–1477. doi:10.1182/blood.2023019940
25. Grégoire M, Uhel F, Lesouhaitier M, et al. Impaired efferocytosis and neutrophil extracellular trap clearance by macrophages in ARDS. Eur Respir J. 2018;52(2):1702590. doi:10.1183/13993003.02590-2017
26. Tapper H, Karlsson A, Mörgelin M, Flodgaard H, Herwald H. Secretion of heparin-binding protein from human neutrophils is determined by its localization in azurophilic granules and secretory vesicles. Blood. 2002;99(5):1785–1793. doi:10.1182/blood.v99.5.1785
27. Liu L, Shao Y, Zhang Y, et al. Neutrophil-derived heparin binding protein triggers vascular leakage and synergizes with myeloperoxidase at the early stage of severe burns (With video). Burns Trauma. 2021;9:tkab030. doi:10.1093/burnst/tkab030
28. Linder A, Soehnlein O, Akesson P. Roles of heparin-binding protein in bacterial infections. J Innate Immun. 2010;2(5):431–438. doi:10.1159/000314853
29. Fisher J, Linder A. Heparin-binding protein: a key player in the pathophysiology of organ dysfunction in sepsis. J Intern Med. 2017;281(6):562–574. doi:10.1111/joim.12604
30. Liu Y, Zhou W, Xu W, et al. The value of heparin-binding protein in bronchoalveolar lavage fluid in acute respiratory distress syndrome. Front Med Lausanne. 2025;12:1537680. doi:10.3389/fmed.2025.1537680
31. Xue M, Zeng Y, Qu HQ, et al. Heparin-binding protein levels correlate with aggravation and multiorgan damage in severe COVID-19. ERJ Open Res. 2021;7(1):00741–2020. doi:10.1183/23120541.00741-2020
32. Sun J, Xu D, Zeng Z, et al. Predictive value of dynamic changes of heparin-binding protein in patients with MODS. Guangdong Med J. 2025;46(3). doi:10.13820/j.cnki.gdyx.20242249
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.