Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Association Between FAM134B and Diabetic Peripheral Neuropathy in Type 2 Diabetes: A Double-Center Case-Control Study
Authors Hu X ![]() , Peng J, Li Q, Chen Y
, Peng J, Li Q, Chen Y ![]() , Zeng Y, Li P, Yang C
, Zeng Y, Li P, Yang C
Received 26 November 2024
Accepted for publication 26 February 2025
Published 11 March 2025 Volume 2025:18 Pages 729—742
DOI https://doi.org/10.2147/DMSO.S508698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Xingyun Hu,1,* Jie Peng,2,* Qingxian Li,3 Yuying Chen,4 Yingjuan Zeng,5 Peishan Li,4 Chuan Yang4
1Department of General Practice, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China; 2Department of Emergency, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China; 3Department of Endocrinology, Shenzhen Longhua District Central Hospital, Shenzhen, People’s Republic of China; 4Department of Endocrinology, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China; 5Department of Endocrinology, The Fifth Affiliated Hospital, Sun Yat-sen University, Zhuhai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Peishan Li; Chuan Yang, Department of Endocrinology, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Yanjiang West Road No. 107, Guangzhou, 510120, People’s Republic of China, Email [email protected]; [email protected]
Purpose: The role of FAM134B in neurological diseases has received significant attention; however, its role in diabetic peripheral neuropathy (DPN) remains unexplored. This study investigated the association between plasma FAM134B levels and DPN while assessing its diagnostic value.
Methods: The study included 128 inpatients with type 2 diabetes divided into DPN (n = 68) and non-DPN (n = 60) groups. FAM134B expression was determined via qRT-PCR analysis of plasma FAM134B mRNA level. All clinical data were retrieved from the Hospital Information System. SPSS and R were used for statistical analyses.
Results: Plasma FAM134B mRNA levels were significantly higher in the DPN than in the non-DPN group (p < 0.001). Increased FAM134B mRNA levels were strongly linked to increased odds of DPN, with the highest quartile showing a significant risk elevation (Odds Ratio [OR] = 21.42, 95% Confidence Interval: 4.86– 96.46, p < 0.001). Restricted cubic spline analysis confirmed a non-linear relationship, thereby identifying a critical threshold of FAM134B mRNA levels at 2.53, above which the risk sharply increased (adjusted OR = 3.11, p = 0.006). Subgroup analysis showed consistent associations across most subgroups, with a notable difference in males (p = 0.038). The diagnostic performance was moderate (Area Under the Curve [AUC] = 0.756). While adding FAM134B mRNA to the model did not dramatically improve the AUC, it significantly enhanced reclassification metrics (Net Reclassification Improvement = 0.165, Integrated Discrimination Improvement = 0.095, p < 0.05), thereby highlighting its clinical value.
Conclusion: Increased FAM134B expression positively correlated with the odds of DPN, and may act as a promising target for diagnostic and therapeutic interventions.
Plain Language Summary: Diabetic peripheral neuropathy (DPN) is a common diabetic complication without effective treatment to block or reverse its progression currently. FAM134B is thought to be closely linked with neurological disease in previous studies, potentially playing a pivotal role in DPN.Plasma FAM134B mRNA levels were significantly increased in individuals with DPN and markedly associated with increased odds of DPN. Different statistical models demonstrated that FAM134B had an excellent diagnostic predictive value for DPN.Our findings provide a theoretical foundation for the development of FAM134B as a potential target for diagnostic and therapeutic interventions of DPN.
Keywords: FAM134B, type 2 diabetes, diabetic peripheral neuropathy, clinical value
Introduction
In 2021, the International Diabetes Federation’s 10th edition of the Global Diabetes Atlas, revealed that 537 million adults aged 20–79 years (10.5% of the worldwide population within this age range) have diabetes mellitus. Projections estimate a rise to 643 million (11.3%) by 2030 and up to 783 million (12.2%) by 2045.1 Diabetic neuropathy, most prevalent chronic complication of diabetes, affects more than half of individuals with diabetes.
The predominant form of diabetic neuropathy, peripheral sensorimotor neuropathy, typically presents with tingling, numbness, and pain, especially in the lower extremities.2 Individuals with diabetic peripheral neuropathy (DPN) are at a higher risk of falls and fractures due to impaired limb sensation,3 and difficult-to-heal foot ulcers, which can lead to Charcot neuroarthropathy and poor prognosis in the context of hyperglycemia. The high incidence and disability rates of DPN severely compromise patients’ quality of life and impose significant financial and psychological burdens on families and society.4
The precise pathogenesis of DPN remains unclear. However, several risk factors have been identified, including hyperglycemia, hypertension, hyperlipidemia, smoking, and certain nonmodifiable factors such as age and race. FAM134B, also known as RETREG1 (JK-1), is a member of the family with sequence similarity 134. FAM134B primarily expressed in sensory and autonomic nerves. Evidence suggests that FAM134B mutations and aberrant expression are closely linked to hereditary sensory and autonomic neuropathy (HSAN) type IIB.5 HSAN type IIB is primarily characterized by sensory neuropathy, with clinical features including progressive hyperalgesia and hyperesthesia, and peripheral nerve demyelination—hallmarks closely resembling DPN. Our previous studies demonstrated that FAM134B-knockout mice exhibit dysmyelination, hypomyelination, and demyelination phenotypes that mirror those observed in wild-type diabetic mice.6 The expression of FAM134B may be a critical initiating factor in DPN, potentially contributing to its onset and progression.
This study evaluated plasma FAM134B mRNA levels in individuals with type 2 diabetes, comparing those with DPN to those without (non-DPN). Additionally, we explored the potential relationship between plasma FAM134B levels and DPN, and constructed statistical models to assess the diagnostic value of FAM134B in identifying DPN in type 2 diabetes.
Methods
Study Design and Participants
This double-center case-control study was approved by the ethics committees of the participating hospitals (Approval No. SYSKY-2022-042-03). Between September 2022 and May 2024, a total of 128 inpatients with type 2 diabetes mellitus, diagnosed according to the latest Chinese clinical guidelines7 and who had previously provided informed consent for voluntary participation, were screened by the Department of Endocrinology at Sun Yat-sen Memorial Hospital and Shenzhen Longhua District Central Hospital. The exclusion criteria included: (1) acquired inflammatory demyelinating peripheral neuropathy, including Guillain–Barré Syndrome; (2) peripheral neuropathy from non-diabetic causes, such as tumors, connective tissue disease, alcohol abuse, or drug use; (3) inability to perform nerve conduction tests (NCT) due to diabetic foot, gouty arthritis, or mental disease; and (4) pregnancy or lactation.
Data Collection
Each patient underwent a comprehensive clinical assessment, with clinical data retrieved from the Hospital Information System (HIS) at Sun Yat-sen Memorial Hospital and Shenzhen Longhua District Central Hospital. The collected data included demographic data, metabolic indicators, liver and kidney function, cardiac evaluation, and diabetes related history (details in Table 1). FAM134B expression was measured using quantitative real-time polymerase chain reaction (qRT-PCR) to express plasma FAM134B mRNA levels. The detailed procedure of qRT-PCR and the primer sequences for target genes were presented in Appendix 1. β-Actin served as the housekeeping reference gene for normalization.
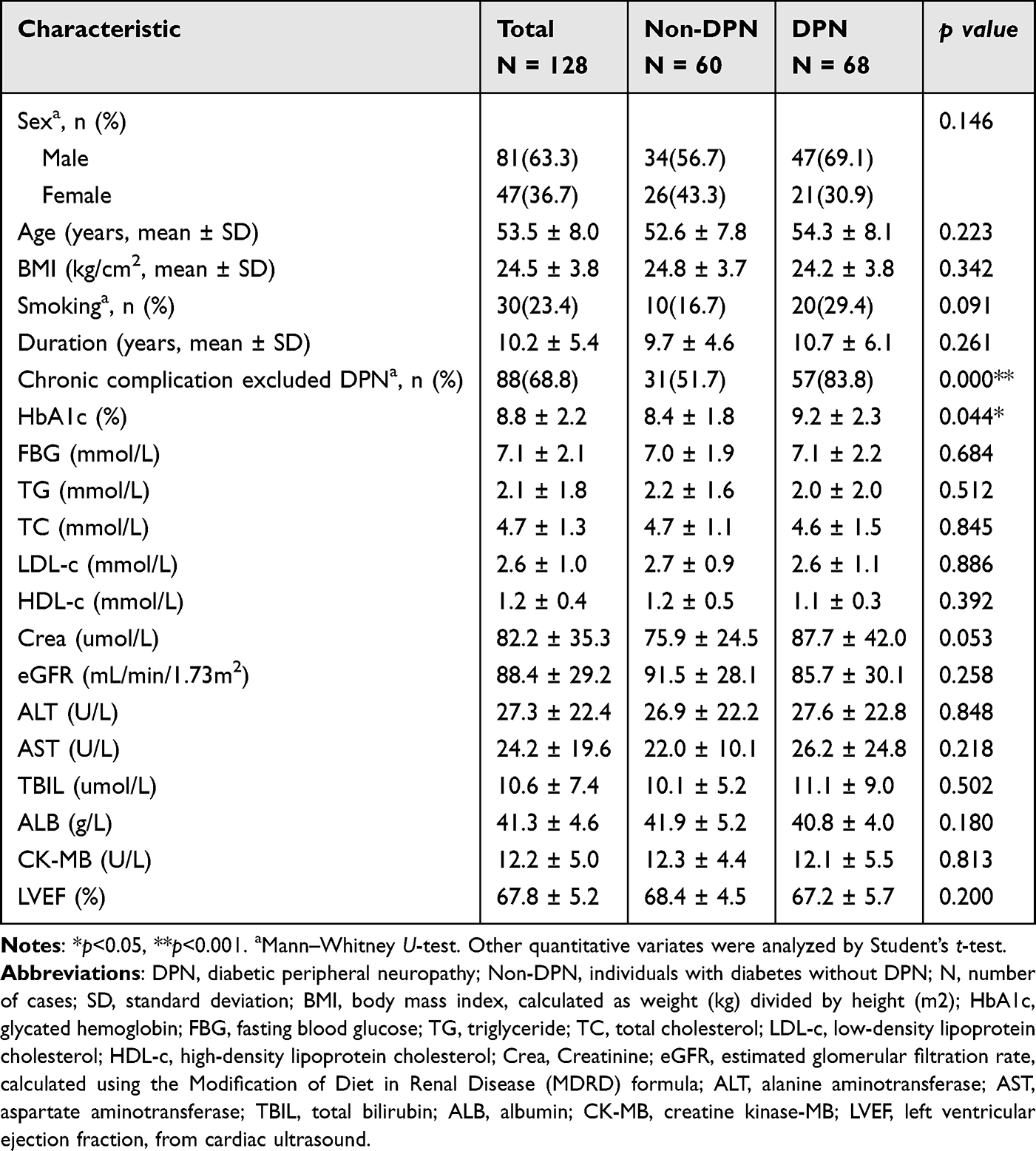 |
Table 1 Baseline Characteristics of All Participants with and without DPN |
Assessment and Definition of Diabetic Peripheral Neuropathy
Owing to the lack of unified diagnostic criteria for DPN, NCT abnormalities served a the primary objective measure for this condition.8 In this study, DPN was defined based on NCT values from both upper and lower extremities, including assessments of the median, ulnar, sural, peroneal, and superficial peroneal nerves. DPN was confirmed electro-physiologically based on the presence of abnormalities in any nerve conduction index of at least two separate nerves.9 The Toronto Clinical Scoring System (TCSS) was utilized for evaluating the clinical features of DPN based on clinical signs and symptoms. Participants were assessed using the TCSS, which includes a six-item symptom score evaluating lower extremity symptoms (numbness, tingling, pain, weakness, imbalance) and any upper extremity symptoms; a five-item physical examination score assessing light touch, temperature sensation, pinprick sensation, vibration, and positional sensation; and an eight-item reflex score examining ankle, knee, and bilateral reflexes, each graded as absent, diminished, or normal. The combined total score has a maximum of 19 points.10
Statistical Analysis
Statistical analyses were performed using SPSS version 18.0 and R version 4.4.1. Demographic data, clinical features, and plasma FAM134B mRNA levels were compared using Student’s t-test or the Mann–Whitney U-test for continuous and categorical data, respectively. Pearson’s correlation analysis was performed to evaluate the relevance of plasma FAM134B mRNA levels to the TCSS score and the different indices of NCT. The association between plasma FAM134B mRNA levels and DPN risk was assessed using logistic regression models. Subgroup analyses were also performed to investigate potential effect modifications by various demographic and clinical factors. A two-piecewise linear regression model was employed to investigate the relationship between plasma FAM134B mRNA levels and DPN risk. Various statistical models and algorithms were applied to evaluate the diagnostic effectiveness of FAM134B mRNA in predicting DPN in multiple dimensions. Statistical significance was defined as p < 0.05 in all analyses. The specifics of statistical methodologies are presented in Appendix 2.
Results
Baseline Characteristics of Participants
The elementary characteristics of all participants are shown in Table 1. Overall, 128 individuals with type 2 diabetes mellitus were enrolled, with 68 (53%) diagnosed with DPN. The DPN group exhibited a higher mean glycated hemoglobin (HbA1c) level (9.2 ± 2.3% vs 8.4 ± 1.8%, p = 0.044) and a greater prevalence of chronic diabetic complications history (excluding DPN) compared to the non-DPN group (83.8% vs 51.7%, p < 0.001). Differences in sex, age, body mass index (BMI), smoking history, diabetes duration, fasting blood glucose, blood lipid, liver function, kidney function, and cardiac indicators across the groups were not statistically significant.
Plasma FAM134B mRNA Level Between DPN and Non-DPN Group
The data on plasma FAM134B mRNA levels were consistent with non-normal distribution. Mann–Whitney U-test showed that the median plasma FAM134B mRNA level in the DPN group was markedly higher than that in the non-DPN control group (3.09 ± 3.56 vs 1.76 ± 1.57, p < 0.001) (Figure 1A). All participants were divided into four groups based on the quartiles of plasma FAM134B mRNA levels. Chi-square test results showed that the proportion of DPN increased progressively with higher plasma FAM134B mRNA levels (p < 0.001) (Figure 1B).
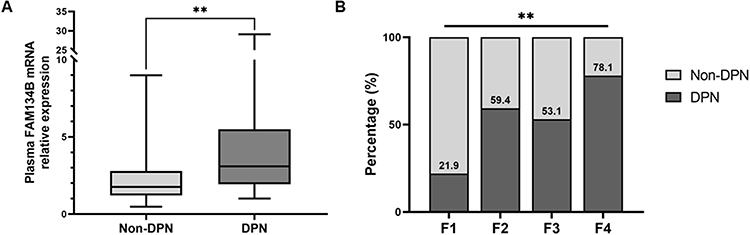 |
Figure 1 (A) Differential expression of plasma FAM134B mRNA between the non-DPN group and DPN group. (B) Percentage of DPN across plasma FAM134B mRNA levels. All participants were divided into four groups according to quartiles of plasma FAM134B mRNA level (F1 [first quartile]: <1.507; F2 [second quartile]: 1.507–2.326; F3 [third quartile]: 2.326–3.977; F4 [4th quartile]: ≥3.977). **p < 0.001. Abbreviations: DPN, diabetic peripheral neuropathy; Non-DPN, individuals with diabetes without DPN. |
Correlation of Plasma FAM134B mRNA Level with TCSS Score
The TCSS score represents the typical clinical signs and symptoms of DPN. Pearson’s correlation coefficient test showed a statistically significant positive correlation between plasma FAM134B mRNA levels and TCSS scores (r = 0.182, p = 0.041) (Figure 2A). Similarly, all participants were divided into four groups based on the quartiles of plasma FAM134B mRNA levels, and the one-way analysis of variance (ANOVA) results indicated that the TCSS score in F4 group (the highest quartile) was markedly higher than that in F1 group (the lowest quartile) (p = 0.021) (Figure 2B).
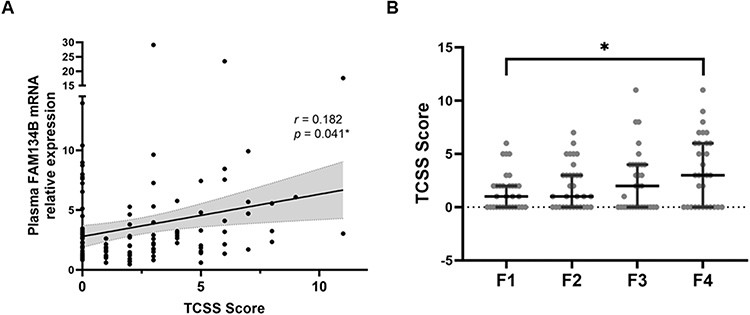 |
Figure 2 (A) Correlation between plasma FAM134B mRNA level and TCSS score. (B) Comparison of TCSS scores across plasma FAM134B mRNA levels. All participants were divided into four groups according to quartiles of plasma FAM134B mRNA level (F1 [first quartile]: < 1.507; F2 [second quartile]: 1.507–2.326; F3 [third quartile]: 2.326–3.977; F4 [fourth quartile]: ≥ 3.977). *p < 0.05. r represents Pearson correlation coefficients. Abbreviation: TCSS, Toronto clinical scoring system. |
Correlation of Plasma FAM134B mRNA Level with NCT
The NCT values for the median, ulnar, sural, peroneal, and superficial peroneal nerves, including conduction velocity, distal latency, and amplitude, are presented in Table 2. The heatmap directly displayed a general trend of decreasing conduction velocity and amplitude accompanied by increasing levels of plasma FAM134B mRNA, while distal latency increased (Figure 3).
 |
Table 2 Values of Nerve Conduction Tests |
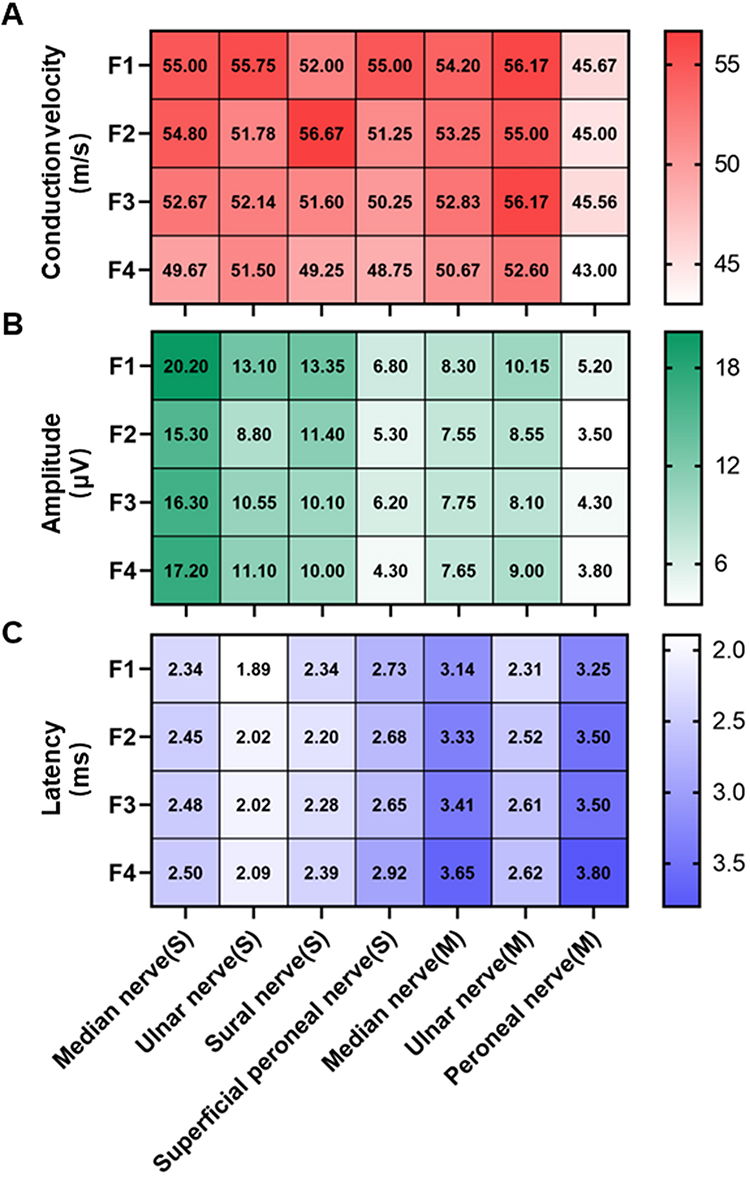 |
Figure 3 Descriptive analysis of nerve conduction tests across different plasma FAM134B mRNA levels. (A) Conduction velocity heatmap. (B) Amplitude heatmap. (C) Latency heatmap. All participants were divided into four groups according to quartiles of plasma FAM134B mRNA level (F1 [first quartile]: < 1.507; F2 [second quartile]: 1.507 ~ 2.326; F3 [third quartile]: 2.326 ~ 3.977; F4 [fourth quartile]: ≥ 3.977). Abbreviations: S, sensory nerve; M, motor nerve. |
We further performed a Pearson’s correlation coefficient test to explore the relationship between plasma FAM134B mRNA levels and different NCT indices. The results showed significant negative correlations between plasma FAM134B mRNA levels and conduction velocities of the median (sensory and motor branches), ulnar (sensory), peroneal (motor), and superficial peroneal (sensory) nerves. Additionally, the amplitude of the sural nerve (sensory branch) was negatively correlated with plasma FAM134B mRNA levels. A statistically significant positive correlation was identified between plasma FAM134B mRNA levels and the distal latencies of the median nerve (motor branch), sensory nerve (sensory and motor branches), and common peroneal nerve (motor branch). Other NCT indices showed weak or no correlation with plasma FAM134B mRNA levels (Figure 4).
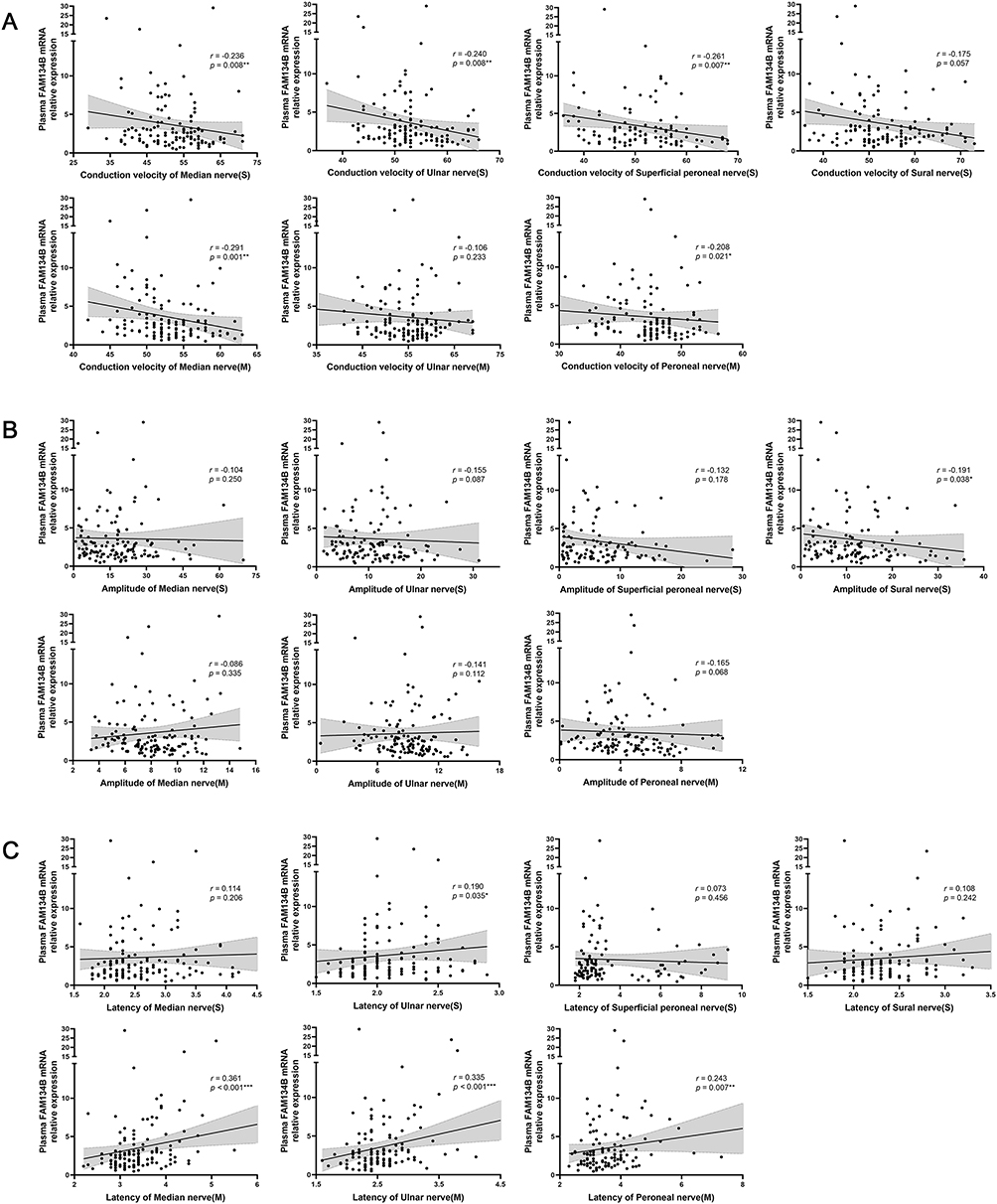 |
Figure 4 Correlation between plasma FAM134B mRNA level and conduction velocity (A), amplitude (B), and distal latency (C) of peripheral sensory and motor nerves. *p < 0.05. r represents Pearson correlation coefficients. Unit: conduction velocity: m/s; amplitude: uV; distal latency: ms. |
Multivariate-Adjusted Odds Ratio (OR) for the Association Between Plasma FAM134B mRNA Levels and DPN Risk
In the multivariate analysis, the relationship between plasma FAM134B mRNA levels and the prevalence of DPN was evaluated across the three models (Figure 5). Higher plasma FAM134B mRNA levels were consistently associated with increased odds of developing DPN. In Model 1, participants in the highest quartile of plasma FAM134B mRNA levels (F4, ≥3.977) had a markedly elevated risk of DPN (OR = 12.76, 95% CI: 3.90–41.73) than those in the reference group (F1, <1.507). This association strengthened in Models 2 and 3, with Model 3 showing an OR of 21.42 (95% CI: 4.86–96.46), highlighting the robustness of this relationship across different model adjustments. The p-trend across all models was statistically significant (p < 0.001), indicating a clear dose-response relationship between increasing plasma FAM134B mRNA levels and DPN risk.
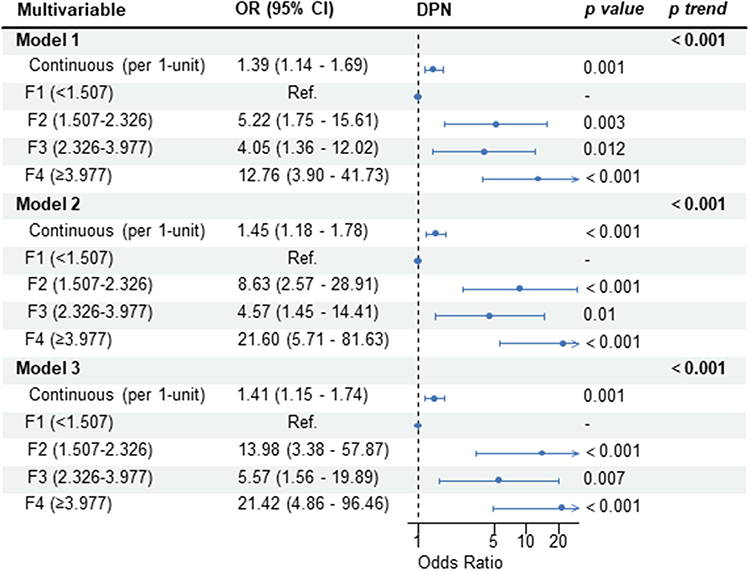 |
Figure 5 Forest plot of the binary logistic regression analysis for plasma FAM134B mRNA level as a risk factor for DPN in individuals with diabetes. Model 1 was unadjusted; Model 2 was adjusted by Model 1+ age + sex + BMI; Model 3 was adjusted by Model 2+ smoking + diabetes duration + chronic complication excluded DPN + HbA1c. (F1 [first quartile]: < 1.507; F2 [second quartile]: 1.507–2.326; F3 [third quartile]: 2.326–3.977; F4 [fourth quartile]: ≥ 3.977). Abbreviations: DPN, diabetic peripheral neuropathy; BMI, body mass index; HbA1c, glycosylated hemoglobin; OR, odds ratio; CI, confidence interval. |
These findings were further supported by the restricted cubic spline (RCS) analysis, which demonstrated a significant non-linear relationship between plasma FAM134B mRNA levels and DPN risk (p < 0.05, Figure 6), revealing a sharp increase in the odds of developing DPN when FAM134B mRNA levels exceeded 2.53, corroborating the threshold effect identified in the two-piecewise model (Table 3). Below this threshold, the adjusted OR for DPN was substantially higher (adjusted OR = 3.11, 95% CI: 1.42–7.28, p = 0.006). In contrast, above 2.53, the risk increase was less pronounced (adjusted OR = 1.21, 95% CI: 0.99–1.56, p = 0.113). The two-piecewise model demonstrated a better fit than the linear model (p = 0.040).
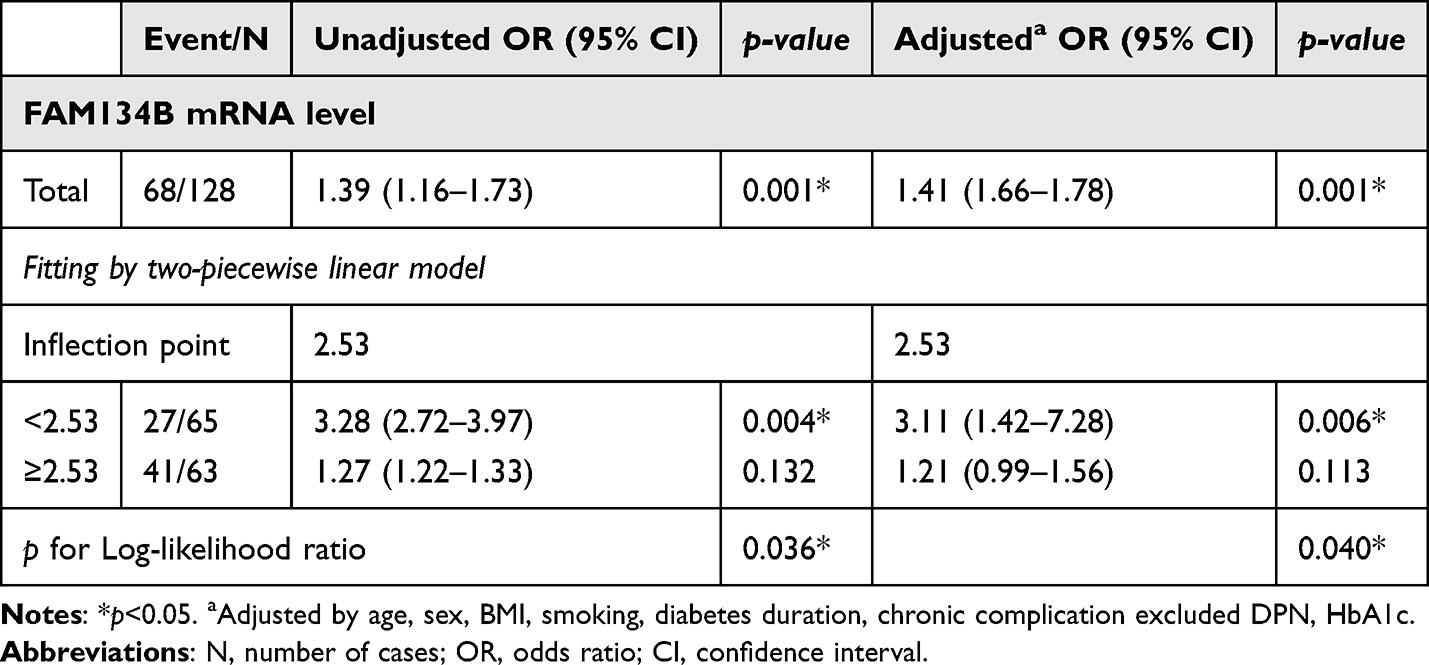 |
Table 3 Segmented Regression Analysis |
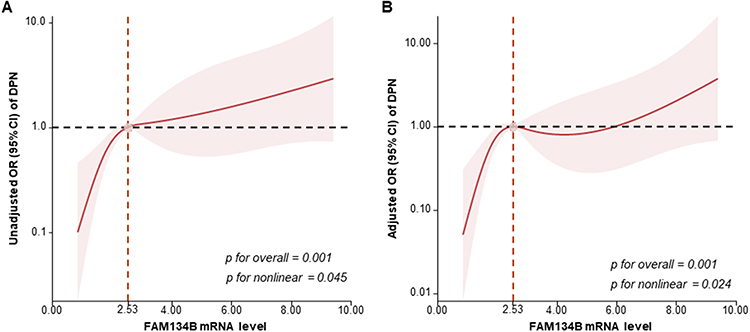 |
Figure 6 Association between plasma FAM134B mRNA levels and DPN using unadjusted (A) and adjusted (B) restricted cubic spline regression model. Adjusted for sex, age, smoking, diabetes duration, and chronic complication excluded DPN, HbA1c, and BMI. Data were analyzed using a logistic regression model, with four knots at the 5th, 35th, 65th, and 95th percentiles of FAM134B. The reference value, based on the inflection point of the curve, was set at 2.53. Solid lines represent odds ratios (OR), while shaded areas denote 95% confidence intervals (CI). Abbreviations: DPN, diabetic peripheral neuropathy; HbA1c, glycosylated hemoglobin; BMI, body mass index. |
Further subgroup analyses (Figure 7) clarified the effects of various demographic and clinical factors on the relationship between FAM134B mRNA levels and DPN. This association remained consistent across subgroups. Notably, the association was stronger in males (OR = 2.23, 95% CI: 1.35–3.67, p-interaction = 0.038), indicating a potential sex-specific vulnerability. Other factors, including age, smoking status, BMI, HbA1c level, and diabetes duration, did not significantly affect this relationship (p > 0.05).
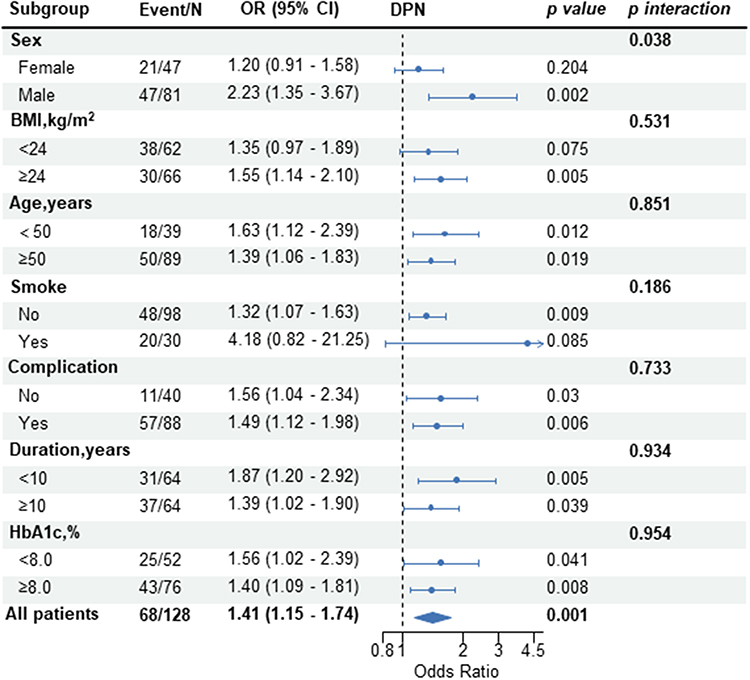 |
Figure 7 Subgroup analysis of plasma FAM134B mRNA levels with DPN. Adjusted by sex, BMI, age, smoking, chronic complication (excluding DPN), diabetes duration, and HbA1c. Abbreviations: DPN, diabetic peripheral neuropathy; BMI, body mass index; HbA1c, glycosylated hemoglobin; OR, odds ratio; CI, confidence interval. |
Diagnostic Value of Plasma FAM134B mRNA Level in Detecting DPN
Receiver operating characteristic (ROC) curves showed plasma FAM134B mRNA levels exhibited moderate diagnostic performance for DPN, with the area under the curve (AUC) of 0.756 (95% CI: 0.549–0.822) (Figure 8A). When incorporated into the multivariate model, the AUC increased to 0.82; however, this improvement did not achieve statistical significance (p = 0.156) (Figure 8B). Boruta feature selection (Figure 8C) highlighted plasma FAM134B mRNA as the most influential factor, surpassing traditional clinical variables, such as comorbidities and HbA1c. The decision curve analysis (DCA) (Figure 8D) demonstrated that the inclusion of FAM134B mRNA provided a greater net benefit across various thresholds. Calibration plots (Figure 8E) confirmed that the FAM134B-enhanced model showed better alignment between predicted and observed risks. While the incorporation of FAM134B mRNA resulted in only a marginal increase in the C-index (from 0.772 to 0.816, p = 0.156), it significantly enhanced the reclassification measures, with notable gains in both integrated discrimination improvement (IDI = 0.095, p < 0.001) and net reclassification improvement (NRI = 0.165, p = 0.022) (Figure 8F).
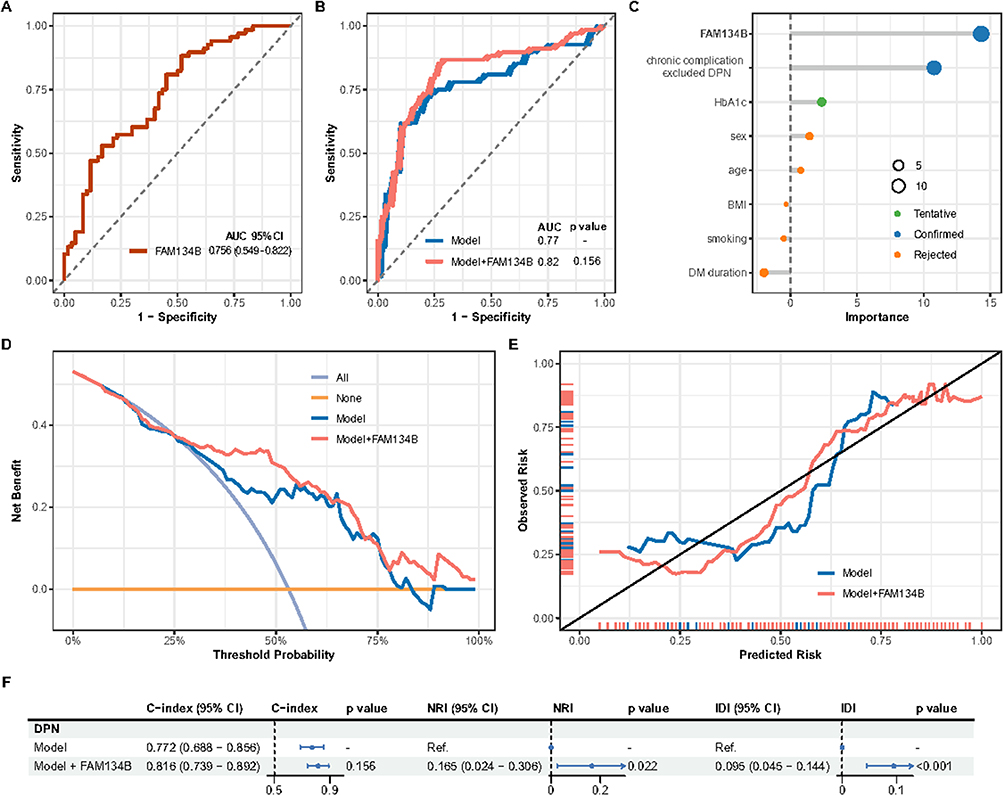 |
Figure 8 (A) ROC curve for plasma FAM134B mRNA levels to indicate DPN among individuals with type 2 diabetes mellitus. (B) ROC curve comparison for the model with or without FAM134B. (C) Feature importance assessment via Boruta analysis for clinical variables associated with DPN. (D) Decision curve analysis for the model with or without FAM134B. (E) Calibration curve analysis for the model with or without FAM134B. (F) Evaluation of model improvement with and without FAM134B for the diagnostic prediction of DPN. The model includes age, sex, BMI, smoking, diabetes duration, chronic complication excluded DPN, and HbA1c. Abbreviations: DPN, diabetic peripheral neuropathy; ROC, Receiver operating characteristic; BMI, body mass index; HbA1c, glycosylated hemoglobin; Ref, reference; C index, Harrell’s concordance statistic; NRI, net reclassification improvement; IDI, integrated discrimination improvement. |
Discussion
In this study, FAM134B mRNA expression levels were significantly higher in type 2 diabetes individuals with DPN than in those without peripheral neuropathy, which may highlight the critical role of FAM134B in the pathophysiology of DPN. The human FAM134B gene, located at position 15.1 on the short arm of chromosome 5, encodes a 479-amino acid protein whose function remains unclear.11 Initially, FAM134B was reported to be associated with esophageal and colon cancers.11,12 Since the identification of nonsense mutations in FAM134B as a primary trigger for HSAN IIB in 2009,13 its function has received widespread attention in neurological diseases such as vascular dementia,14 epilepsy,15 and Parkinson’s disease.16 Our findings suggest that FAM134B may be an important independent influencing factor for DPN, which has not been extensively investigated in the existing literature.
Clinical signs and symptoms are the primary criteria used for assessing peripheral neuropathy. Various rating scales, such as the TCSS, MNSI, and NSC, have been widely applied in clinical evaluations. The TCSS is a comprehensive scoring system based on the clinical characteristics of DPN, which assesses the function of myelinated and tiny unmyelinated nerve fibers. Owing to its simplicity and comprehensiveness, it is suitable for clinical screening for DPN and for conducting large-scale epidemiological investigations. In our study, we observed statistically significant positive correlations between TCSS score and plasma FAM134B levels, although the strength of these associations was weak. This may be attributable to the limited sample size and the inherent subjectivity of the TCSS rating scale.
Electrophysiology can be regarded as an extension of clinical neurological measurement. Owing to the objective nature of its measurements and independence from the individual subjective responses, electrophysiological techniques currently represent the most reliable assessment of peripheral neuromuscular function.
The NCT, a classical electrophysiological examination, is the gold standard for identifying peripheral neuropathy. It can differentiate neuropathy from mimics (radiculopathy and distal myopathy), assess disease severity, reveal subclinical involvement of neurons and fibers in the absence of clinical manifestations, and identify major pathophysiological alterations (axonal vs demyelinating).17 In contrast to axonal neuropathies, which show a loss of amplitude and relative preservation of conduction velocity, demyelinating polyneuropathies show a decline in nerve conduction velocity while maintaining nerve potential amplitudes.18 The findings of the present study show that increased FAM134B levels correlate strongly with slowed conduction velocity, prolonged distal latency, and flattened amplitude of the peripheral sensory and motor nerves. All these indicators are critical measures for evaluating myelinated axonal function of peripheral nerves. These data indicate that FAM134B may be involved in the pathological changes associated with peripheral neuropathy, especially demyelination.
Currently, NCT is a universally accepted diagnostic criterion for DPN;19 however, its application in primary healthcare settings is limited due to being time-consuming, labor-intensive, and expensive. Although TCSS can be used for early detection of DPN, its accuracy is implicitly limited by its subjectivity. Therefore, a relatively easy-to-perform and objective examination is urgently needed to identify early DPN. FAM134B expression in peripheral blood could serve as an objective outcome to address deficiency.
Previous studies have suggested that risk factors such as age, sex, BMI, smoking, diabetes duration, and HbA1c are demonstrably associated with DPN.20–23 In this study, after adjusting for confounding factors using binary logistic regression analysis, FAM134B was identified as an independent risk indicator for DPN. Notably, subgroup and interaction analyses showed that FAM134B had a stronger impact on DPN in males. However, no similar studies have been conducted to date. These sex differences may be linked to the protective benefit of estrogen in females, which could be counteracted by the negative effects of FAM134B. Male sex is considered a risk factor for DPN; however, it should be noted that the study cohort had an imbalanced sex ratio (male: female ≈ 2:1), which may affect the objectivity of the statistical analysis. The interaction between sex and increased expression of FAM134B in diabetic populations, especially those with DPN, remains unclear and warrants further investigation. Nevertheless, this finding supports our hypothesis that FAM134B might be a significant risk factor influencing the occurrence and progression of DPN.
Most studies have shown that FAM134B contributes to the development, survival, and repair of the nervous system; however, the definite mechanisms involved in DPN remain incompletely elucidated. The increased expression of FAM134B in our study suggests that its role in the pathogenesis of DPN is different from that in HSAN type IIB.
A report published in Nature indicates that FAM134B functions as an autophagy receptor for the endoplasmic reticulum (ER), promoting ER fragmentation and facilitating its entry into the autophagosome to ensure the decomposition and removal of damaged ER components.5
Appropriate autophagy is crucial for cell homeostasis; however, dysregulated autophagy can lead to various disease presentations, including inflammation, metabolic disturbances, and neurodegenerative alterations.24 Numerous studies indicate that severe toxicity of glucose and oxidative stress can result in dysregulated autophagy.25–27 Furthermore, excessive autophagy may contribute to the excessive degradation of myelin-associated proteins and the death of glial cells. Therefore, the driving effect of FAM134B on DPN progression may be mediated through the modulation of ER-phagy.
ROC curve analysis suggested that plasma FAM134B mRNA levels have diagnostic value for DPN. Furthermore, our study showed that adding FAM134B expression to the diagnostic model enhanced the identification of DPN. The Plus model exhibited satisfactory clinical value across different indices, such as Boruta feature importance, IDI, and NRI. These findings indicate the necessity of further mechanistic research into the pathogenic effects of FAM134B and its role in the formation and advancement of DPN.
This study had several limitations. As this study was retrospective and cross-sectional, determining a causal relationship between the expression of FAM134B and the risk of developing DPN could not be established. Additionally, no commercial kit exists for detecting FAM134B protein expression in peripheral blood; therefore, we could only detect mRNA levels via PCR to indirectly reflect FAM134B expression. The cutoff values derived from the Jordon index represent relative expression values applied to the current study population; nonetheless, these shortcomings could be addressed by employing standardized controls if future clinical applications are pursued. Finally, the study included only individuals with type 2 diabetes and lacked non-diabetic control data, making it difficult to confirm the association between FAM134B expression levels and DPN across populations.
Conclusion
This study revealed that plasma FAM134B mRNA levels were significantly elevated in individuals with DPN in the type 2 diabetes mellitus population and were an independent factor influencing the presence of DPN. Additionally, different statistical models demonstrated that FAM134B had significant diagnostic predictive value for DPN. To our best knowledge, this is the first study to comprehensively assess the association between FAM134B and DPN. Further well-designed prospective longitudinal studies are needed to validate these findings and clarify the precise role of FAM134B in the etiology of DPN. Thus, FAM134B may emerge as a promising target for both diagnostic and therapeutic management strategies for DPN.
Data Sharing Statement
All data are available on reasonable request from corresponding authors.
Ethics Approval and Informed Consent
This study was conducted in accordance with the declaration of Helsinki and approved by the Ethics Committee of Sun Yat-sen Memorial Hospital, Sun Yat-sen University (Approval No. SYSKY-2022-042-03). All participants have signed the informed consent.
Acknowledgment
We sincerely express our gratitude to all the individuals who participated in this research endeavor.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the National Natural Science Foundation of China under Grant (Chuan Yang, 81670764; Yingjuan Zeng, 81700716); the Basic and Applied Basic Research Foundation of Guangdong Province of China under Grant (Chuan Yang, 2020B1515120076); and the Medical Scientific Research Foundation of Guangdong Province of China under Grant (Chuan Yang, A2019040).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabet Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
2. Pop-Busui R, Boulton AJ, Feldman EL, et al. Diabetic neuropathy: a position statement by the American Diabetes Association. Diabetes Care. 2017;40(1):136–154. doi:10.2337/dc16-2042
3. Lalli P, Chan A, Garven A, et al. Increased gait variability in diabetes mellitus patients with neuropathic pain. J Diabetes Complications. 2013;27(3):248–254. doi:10.1016/j.jdiacomp.2012.10.013
4. Tavakoli M, Klingelhofer D, Fadavi H, Groneberg DA. The landscape of global research on diabetic neuropathy. Front Endocrinol. 2023;14:1220896. doi:10.3389/fendo.2023.1220896
5. Khaminets A, Heinrich T, Mari M, et al. Regulation of endoplasmic reticulum turnover by selective autophagy. Nature. 2015;522(7556):354–358. doi:10.1038/nature14498
6. Chen B, Hu X, Chen M, et al. Identification of sensory dysfunction and nervous structure changes in Fam134b knockout mice. Neurol Res. 2023;45(1):41–48. doi:10.1080/01616412.2022.2117947
7. Chinese Elderly Type 2 Diabetes P, Treatment of Clinical Guidelines Writing G, Geriatric E, et al. [Clinical guidelines for prevention and treatment of type 2 diabetes mellitus in the elderly in China (2022 edition)]. Zhonghua Nei Ke Za Zhi. 2022;61(1):12–50. Polish. doi:10.3760/cma.j.cn112138-20211027-00751
8. Tesfaye S, Boulton AJ, Dyck PJ, et al. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care. 2010;33(10):2285–2293. doi:10.2337/dc10-1303
9. England JD, Gronseth GS, Franklin G, et al. Distal symmetrical polyneuropathy: a definition for clinical research. A report of the American Academy of Neurology, the American Association of Electrodiagnostic Medicine, and the American Academy of Physical Medicine and Rehabilitation. Arch Phys Med Rehabil. 2005;86(1):167–174. doi:10.1016/j.apmr.2004.09.011
10. Perkins BA, Olaleye D, Zinman B, Bril V. Simple screening tests for peripheral neuropathy in the diabetes clinic. Diabetes Care. 2001;24(2):250–256. doi:10.2337/diacare.24.2.250
11. Tang WK, Chui CH, Fatima S, et al. Oncogenic properties of a novel gene JK-1 located in chromosome 5p and its overexpression in human esophageal squamous cell carcinoma. Int J Mol Med. 2007;19(6):915–923.
12. Kasem K, Sullivan E, Gopalan V, Salajegheh A, Smith RA, Lam AK. JK1 (FAM134B) represses cell migration in colon cancer: a functional study of a novel gene. Exp Mol Pathol. 2014;97(1):99–104. doi:10.1016/j.yexmp.2014.06.002
13. Kurth I, Pamminger T, Hennings JC, et al. Mutations in FAM134B, encoding a newly identified Golgi protein, cause severe sensory and autonomic neuropathy. Nat Genet. 2009;41(11):1179–1181. doi:10.1038/ng.464
14. Kong M, Kim Y, Lee C. A strong synergistic epistasis between FAM134B and TNFRSF19 on the susceptibility to vascular dementia. Psychiatr Genet. 2011;21(1):37–41. doi:10.1097/YPG.0b013e3283413496
15. Wang C, Li Y, Li Y, et al. FAM134B-Mediated ER-Phagy in Mg(2+)-Free Solution-Induced Mitochondrial Calcium Homeostasis and Cell Death in Epileptic Hippocampal Neurons. Neurochem Res. 2021;46(9):2485–2494. doi:10.1007/s11064-021-03389-9
16. Kim DY, Shin JY, Lee JE, et al. A selective ER-phagy exerts neuroprotective effects via modulation of alpha-synuclein clearance in parkinsonian models. Proc Natl Acad Sci U S A. 2023;120(37):e2221929120. doi:10.1073/pnas.2221929120
17. Lehmann HC, Wunderlich G, Fink GR, Sommer C. Diagnosis of peripheral neuropathy. Neurol Res Pract. 2020;2:20. doi:10.1186/s42466-020-00064-2
18. Perkins B, Bril V. Electrophysiologic testing in diabetic neuropathy. Handb Clin Neurol. 2014;126:235–248.
19. Selvarajah D, Kar D, Khunti K, et al. Diabetic peripheral neuropathy: advances in diagnosis and strategies for screening and early intervention. Lancet Diabetes Endocrinol. 2019;7(12):938–948. doi:10.1016/S2213-8587(19)30081-6
20. Abdissa D, Hamba N, Kene K, et al. Prevalence and determinants of peripheral neuropathy among type 2 adult diabetes patients attending Jimma University Medical Center, Southwest Ethiopia, 2019, an institutional-based cross-sectional study. J Diabetes Res. 2020;2020:9562920. doi:10.1155/2020/9562920
21. Tesfaye S, Chaturvedi N, Eaton SE, et al. Vascular risk factors and diabetic neuropathy. N Engl J Med. 2005;352(4):341–350. doi:10.1056/NEJMoa032782
22. Jember G, Melsew YA, Fisseha B, Sany K, Gelaw AY, Janakiraman B. Peripheral Sensory Neuropathy and associated factors among adult diabetes mellitus patients in Bahr Dar, Ethiopia. J Diabetes Metab Disord. 2017;16:16. doi:10.1186/s40200-017-0295-5
23. Kiani J, Moghimbeigi A, Azizkhani H, Kosarifard S. The prevalence and associated risk factors of peripheral diabetic neuropathy in Hamedan, Iran. Arch Iran Med. 2013;16(1):17–19.
24. Chen Y, Shi J, Liu H, et al. Plasma microRNA array analysis identifies overexpressed miR-19b-3p as a biomarker of bipolar depression distinguishing from unipolar depression. Front Psychiatry. 2020;11:757. doi:10.3389/fpsyt.2020.00757
25. Liu L, Li Z, Liu X, Guo S, Guo L, Liu X. Bacterial distribution, changes of drug susceptibility and clinical characteristics in patients with diabetic foot infection. Exp Ther Med. 2018;16(4):3094–3098. doi:10.3892/etm.2018.6530
26. Tang Y, Chen Y, Jiang H, Nie D. Short-chain fatty acids induced autophagy serves as an adaptive strategy for retarding mitochondria-mediated apoptotic cell death. Cell Death Differ. 2011;18(4):602–618. doi:10.1038/cdd.2010.117
27. Wei X, Zheng Y, Ai Y, Li B. Regulatory effects of astragaloside IV on hyperglycemia-induced mitophagy in Schwann cells. Evid Based Complement Alternat Med. 2022;2022:7864308. doi:10.1155/2022/7864308
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.