Back to Journals » International Journal of Women's Health » Volume 18
Association Between Educational Attainment and the Risk of Gynecological Malignancies: A Mediation Mendelian Randomization Study
Authors Miao M, Huang B, Hua Y, Gu M, Guo F ![]() , Zhou H
, Zhou H ![]()
Received 17 December 2025
Accepted for publication 25 April 2026
Published 22 May 2026 Volume 2026:18 589613
DOI https://doi.org/10.2147/IJWH.S589613
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matteo Frigerio
Mengdan Miao,1 Bingna Huang,2 Yue Hua,1 Mengzhe Gu,1 Feifei Guo,1– 3,* Huaijun Zhou1– 3,*
1Department of Gynecology, Nanjing Drum Tower Hospital Clinical College of Nanjing Medical University, Nanjing, People’s Republic of China; 2Department of Gynecology, Nanjing Drum Tower Hospital Clinical College of Nanjing University of Chinese Medicine, Nanjing, People’s Republic of China; 3Department of Gynecology, Affiliated Drum Tower Hospital, Medical School, Nanjing University, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huaijun Zhou; Feifei Guo, Department of Gynecology, Nanjing Drum Tower Hospital Clinical College of Nanjing Medical University, Nanjing, Jiangsu, 210000, People’s Republic of China, Email [email protected]; [email protected]
Purpose: Gynecological malignancies are a significant burden for women, yet the causal link between educational attainment and gynecological cancer risk, along with the mediators, remains unclear. Therefore, the mendelian randomization method was employed to investigate the association between educational attainment and endometrial cancer, ovarian cancer, cervical cancer, and vulvar cancer, and quantified the proportion of the relationship potentially mediated by intermediate risk factors.
Patients and Methods: Genetic variants (single nucleotide polymorphisms) were employed as tools, primarily employing the inverse-variance weighted method, supplemented by four other sensi-tivity methods. Mediation proportion (β1×β2/β) was calculated via bootstrapped 95% confidence interval.
Results: Higher educational attainment (per SD) was associated with reduced risk of endometrial cancer (OR 0.71, 0.61– 0.83), ovarian cancer (OR 0.84, 0.73– 0.97), and cervical cancer (OR 0.60, 0.38– 0.95). Education causally influenced 18 potential mediators. Body mass index (OR 1.89; 95% CI: 1.69– 2.11), body fat percentage (OR 2.11; 95% CI: 1.48– 3.00), age at menopause (OR 1.23; 95% CI: 1.10– 1.38), fasting insulin (OR 2.07; 95% CI: 1.13– 3.83), testosterone (OR 1.58; 95% CI: 1.38– 1.82), and sex hormone-binding globulin (OR 0.83; 95% CI: 0.75– 0.91) causally influenced endometrial cancer, explaining 42.23%, 41.67%, − 11.05%, 35.84%, 8.80%, and 9.82% of education’s total effect, respectively. Body mass index (OR 1.12; 95% CI: 1.02– 1.24) and age at menopause (OR 1.12; 95% CI: 1.02– 1.24) also had causal effects on ovarian cancer, mediating 15.16% and − 12.03% of education’s effect.
Conclusion: The mendelian randomization analysis reveals the potential causal mechanisms underlying the association between education and the risk of endometrial cancer and ovarian cancer. Interventions targeting obesity (body mass index and body fat percentage), age at menopause, fasting insulin, testosterone, and SHBG may reduce the incidence of endometrial cancer associated with lower educational levels. For ovarian cancer, intervention strategies targeting body mass index and age at menopause could be key to help prevent ovarian cancer. These public health interventions could help mitigate health disparities caused by social inequality.
Keywords: Mendelian randomization, educational attainment, gynecological malignancies, genome-wide association study, mediation analysis
Introduction
The causal relationship between educational attainment and various gynecological malignancies remains unclear. Although low educational level has been established as a risk factor for endometrial cancer (EC),1 its potential etiological role in ovarian, cervical, and vulvar cancers warrants further investigation.
Since educational opportunities are primarily established in early life, altering educational attainment is often impractical. Instead, targeting modifiable intermediary risk factors may offer a viable approach to mitigating education-associated risks of gynecological malignancies. Previous research has demonstrated that educational attainment is closely associated with multiple risk factors, including smoking,2 obesity (as measured via body mass index (BMI)),3 and hypertension.3 Conventional observational studies have identified several established contributors to gynecologic oncogenesis. For instance, elevated estrogen and testosterone levels are associated with increased risk of EC;4 obesity (as measured via BMI) has been causally linked to EC;5 genetic predisposition to smoking correlates with a higher incidence of cervical cancer (CC);6 and coffee consumption has been implicated as a risk factor for endometrioid ovarian cancer (OC).7 However, these observational studies are prone to be influenced by confounding factors, measurement errors, and reverse causality, thereby undermining reliable causal inference.
Moreover, most studies focus solely on a single cancer type, which limits the understanding of common mechanisms in cancer. Gynecological malignancies exhibit biological diversity with distinct subtypes determined by different etiologies and hormone dependence. This further highlights the necessity for mechanistic research among different cancer types.
Previously, some studies have explored the relationship between multiple variables and the risk of gynecological malignancies. For instance, dietary factors,8 hormonal, metabolic and inflammatory markers9,10 had an impact on gynecological malignancies. Furthermore, educational attainment may influence women’s BMI, insulin levels, and estrogen levels through factors such as exercise and diet, thereby affecting the age at menarche, age at menopause, or parity. This could subsequently increase the risk of estrogen exposure and modulate the risk of gynecological malignancies.11,12 However, whether and to what extent these risk factors explain the effect of educational level on gynecological malignancies remains unclear. Therefore, it is necessary to conduct a systematic, targeted assessment of these risk factors. Identifying various risk factors related to educational attainment, further analyzing their relationship with gynecological malignancies, screening for possible mediators, and quantifying the roles of these mediators may help reduce the negative impact of gynecological malignancies due to socioeconomic inequality.
Mendelian randomization (MR) uses randomly allocated genetic variants as instrumental variables to estimate causal exposure-outcome relationships while minimizing confounders, measurement errors, and reverse causation bias.13,14 Because genetic variations occur randomly during conception and are independent of confounding factors, compared to conventional mediation analyses, MR-based approaches are uniquely resistant to exposure-mediator-outcome confounding and measurement bias.15
Therefore, this study aims to evaluate the causal effect of educational attainment on major gynecological malignancies and their subtypes using MR, as well as to identify potential mediating factors while quantifying their contributions to the overall effect. Using two-sample MR, we examined the causal effects of educational attainment on four gynecological cancers (i.e., endometrial, ovarian, cervical, and vulvar cancers, including their subtypes). Given the insufficient evidence regarding molecular characteristics in carcinogenesis, we systematically evaluated 24 cardiometabolic, hormonal, and reproductive factors as mediators and quantified the mediation proportions. Our findings may provide a reference basis for targeted interventions aimed at reducing the burden of gynecological malignancies among women with lower educational attainment.
Material and Methods
Study Design
The analysis consisted of two stages: first, a two-sample MR approach was utilized to assess the potential causal association between educational attainment and gynecological cancers (including endometrial, ovarian, cervical and vulvar cancers, both overall and per their histological subtypes). This was followed by an examination of the causal links between educational attainment and previously reported molecular factors and their subsequent associations with gynecological cancer risks. In the second stage, a two-step MR mediation analysis was performed to quantify the proportion of the association between educational attainment and EC/OC risk that was mediated by these identified factors (Figures 1 and 2). All the analyses adhered to the Strengthening the Reporting of Observational Studies in Epidemiology using MR (STROBE-MR) checklist.16,17
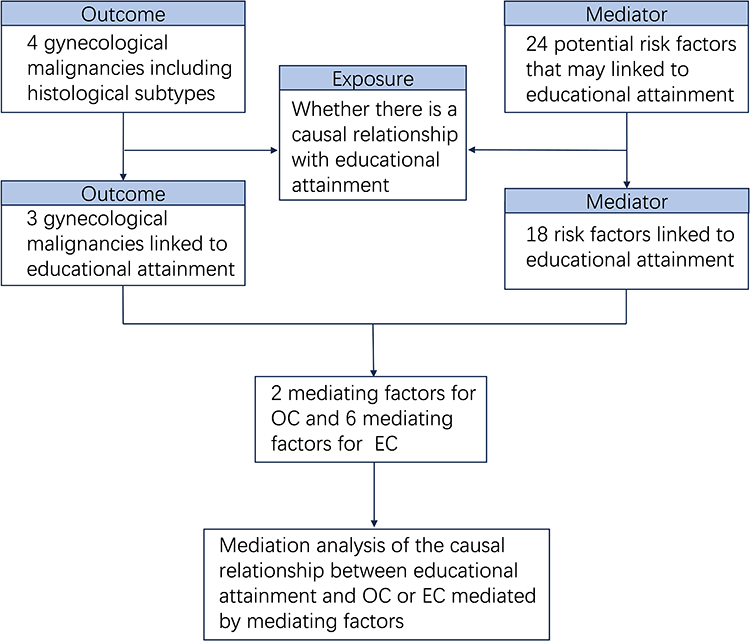 |
Figure 1 A flow diagram reported the variables screening at each stage included in the study. Abbreviations: EC, endometrial cancer; OC, ovarian cancer. |
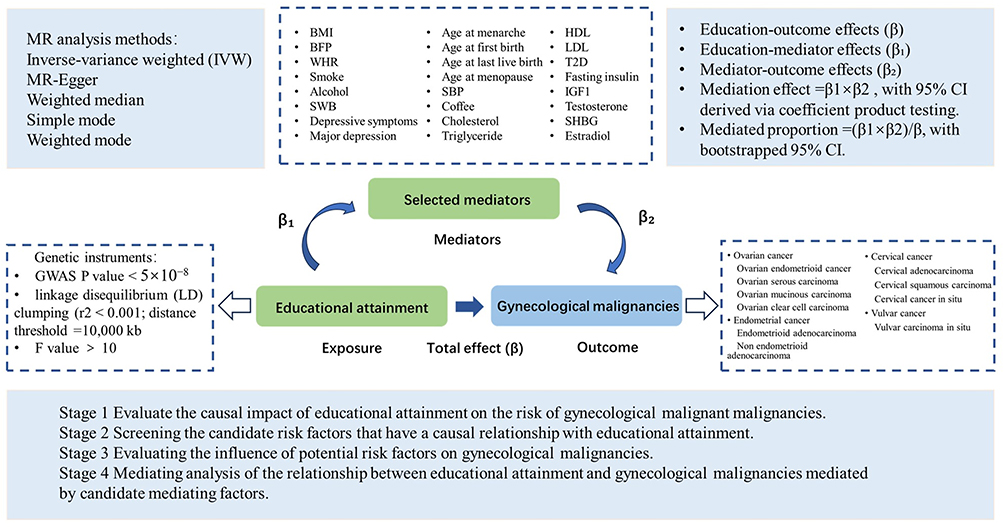 |
Figure 2 Overview of the Mendelian randomization (MR) study design. Through the selection of instrumental SNPs for educational attainment, the selection of candidate mediators, and the selection of outcomes, a two-step MR analysis was conducted. Firstly, univariable MR was used to separately assess the causal relationships between education and gynecological malignancies (β) and the relationships between education and mediating variables (β1), screening for candidate mediators. Subsequently, the causal effect of each candidate mediator on the outcome was evaluated (β2). In the second stage, the mediating effects were calculated using the results from the two-step MR. |
Data Source
The data used in this MR study came from publicly available summary statistics on genome-wide association studies (GWAS), primarily from populations of European ancestry. All the source studies had received proper ethical approval, thus eliminating the need for additional approval from an institutional review board or informed consent measures. Data were obtained from publicly available GWAS and large consortia, comprising studies conducted over varying periods (approximately from 2012 to 2024). For some datasets derived from meta-analyses, detailed timeframe information for individual contributing studies cannot be obtained; therefore, the reported timeframe reflects the data sources that were directly cited. To avoid potential sample overlap between the data sets of GWAS for exposure, mediators, and outcomes, we preferentially select data sets from independent collaborative organizations. Moreover, the outcome data uses databases such as individual organizations, OC Association Consortium, and Finngen, which are different from those for exposure and mediators, to avoid sample overlap.
Selected Genetic Correlation Tools for Educational Attainment
The genetic instruments for educational attainment were derived from a large-scale GWAS meta-analysis conducted by the Social Science Genetic Association Consortium (SSGAC), which examined schooling years in 1,131,881 individuals of European ancestry (N=766,345 after excluding 23andMe participants),18 with each SD representing 4.2 years of additional education. Following strict threshold (P<5×10−8) and linkage disequilibrium (LD) clumping (r2<0.001; distance threshold =10,000 kb), 317 independent genome-wide significant single-nucleotide polymorphisms (SNPs) were selected as primary genetic instruments for educational attainment. These SNPs were confirmed not to overlap with potential mediator-associated variants. To assess the strength of the genetic instruments, we calculated the F-statistic for each SNP using the standard formula. The F-statistic for all the selected SNPs was greater than 10.
Outcomes
The EC outcome data comprised three binary subtypes (overall, endometrioid adenocarcinoma (EEC), and non-endometrioid adenocarcinoma (NEEC)) sourced from a study by O’Mara et al19. The OC data included five binary subtypes (overall, endometrioid, serous, mucinous, and clear cell carcinoma) obtained from a study by Phelan et al20. The CC (overall, squamous carcinoma, adenocarcinoma, and CC in situ) and vulvar cancer data (invasive and in situ carcinoma), analyzed as binary outcomes, were sourced from the FinnGen consortium’s publicly available GWAS summary statistics.21
Mediators
Based on previous epidemiological evidence, 24 potential risk factors associated with educational attainment were selected for verification, mainly divided into the following three categories. Firstly, metabolic factors: BMI data was obtained from a study by Yengo et al;22 body fat percentage (BFP) data was derived from a study by Lu et al;23 waist-hip ratio (WHR) data was taken from Shungin et al;24 data on systolic blood pressure (SBP) was sourced from Evangelou et al;25 data on cholesterol was obtained from Neale labs; data on triglycerides, high-density lipoproteins, and low-density lipoproteins came from Willer.26 Secondly, behavioral, emotional and lifestyle-related factors: smoking and drinking behavioral data were sourced from Liu et al27 and Schumann et al,28 respectively; data on subjective well-being (SWB) and depressive symptoms were extracted from the SSGAC website, based on a study by Okbay et al;29 major depression data were obtained from Howard et al;30 data on coffee was obtained from Ben labs; data on SNP effects related to type 2 diabetes risk came from a study by Mahajan;31 data on fasting insulin,32 insulin like growth factor 1(IGF-1) came from Manning et al32 and Neale labs. Thirdly, reproductive and sex-stratified hormone factors: data on age at menarche, first or last birth, and menopause were obtained from Day,33 Howe, and Ben’s studies; and data on testosterone, sex hormone-binding globulin (SHBG), estradiol were obtained from UK Biobank (via IEU)34 (Table 1 and Supplementary Tables S1–S20).
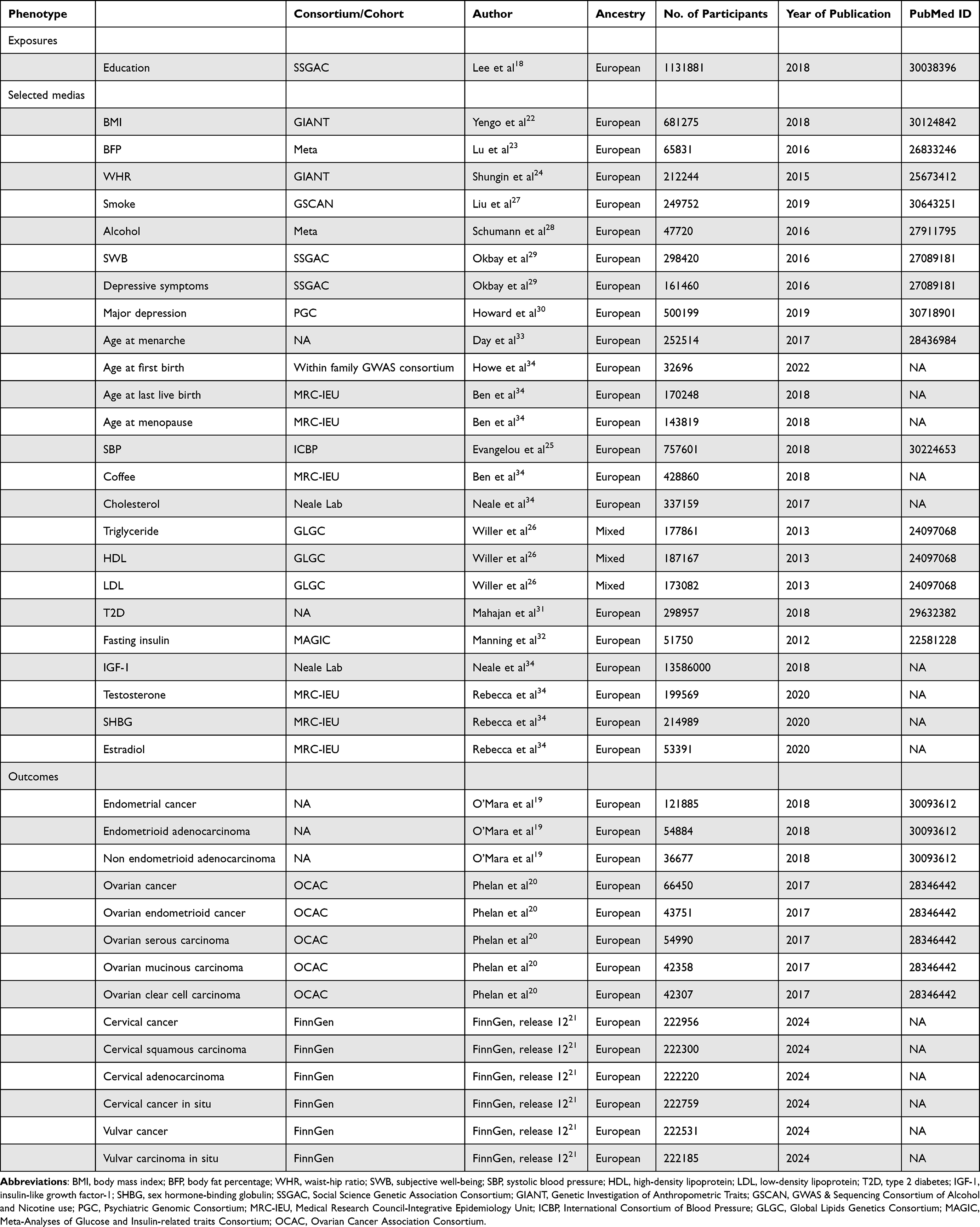 |
Table 1 Summary of the GWAS Data Used for Two-Sample Mendelian Randomization Analyses |
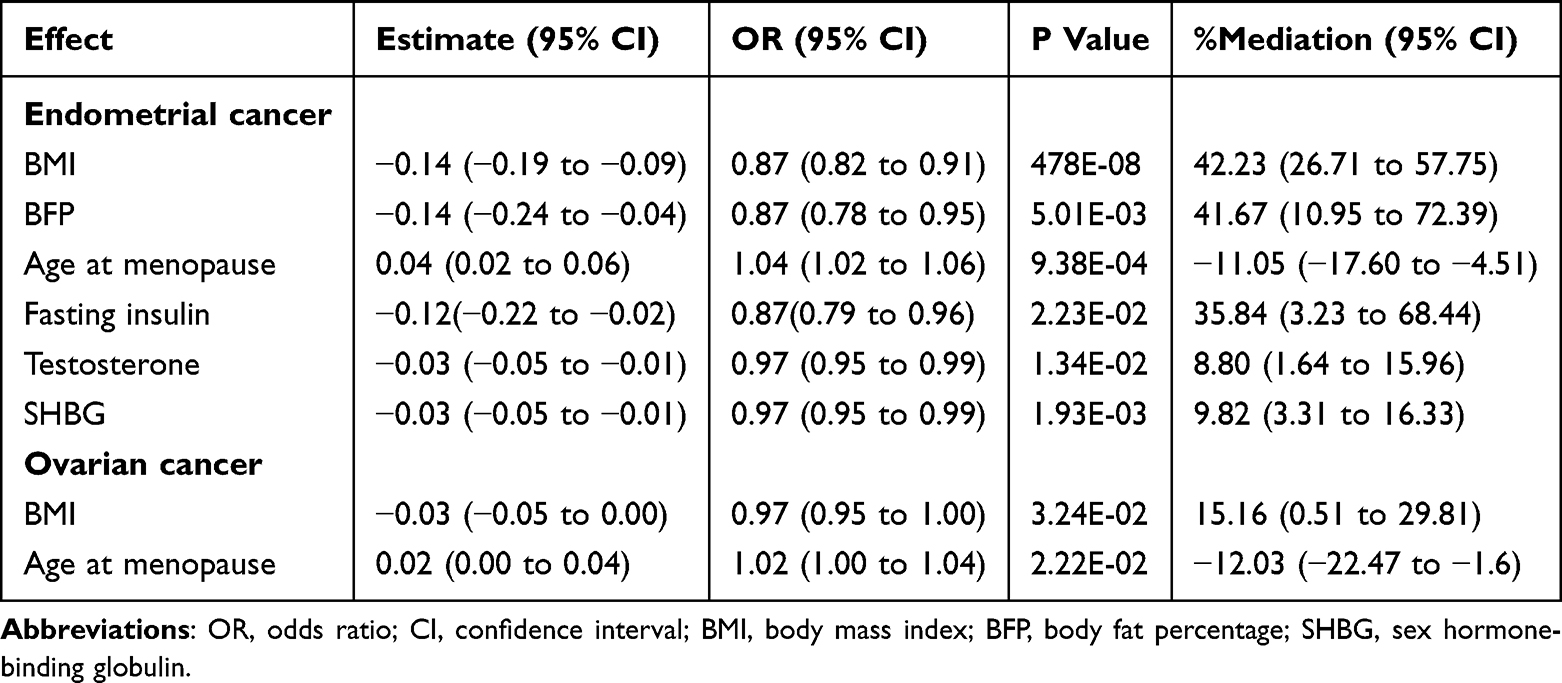 |
Table 2 Results of the Mediation Analysis Examining the Proportions Mediated by mediators in the Causal Association Between Education and Gynecological Malignancies |
Univariable MR Analysis
To investigate the causal effects of exposure on gynecological malignancies, a two-sample MR was implemented. The inverse-variance weighted (IVW) method35 (which combines individual SNP effects using multiplicative random-effects meta-analysis) served as the primary univariable MR (UVMR) method. Additional sensitivity analyses were conducted using the MR-Egger,36 weighted median,37 simple mode,38 and weighted mode38 estimation methods. All the MR analyses satisfied three key criteria: (1) the genetic variants must be strongly associated with the exposure; (2) the genetic variants must not be associated with any known or unknown confounders; and (3) the instrumental variables should influence the outcome exclusively through the exposure, with no direct causal pathways between the genetic variants and the outcome. Two SNPs that were duplicated between the instrumental SNPs for the mediators and for educational attainment were removed.
The MR analyses were executed in R (v4.4.2), using dedicated genetic analysis packages including TwoSampleMR, MendelianRandomization, MR-PRESSO, and VariantAnnotation. A P-value threshold of 0.05 was applied for significance testing, and pleiotropic effects were deemed acceptable when P > 0.05.
Mediation Analysis
Mediators for the association between education and gynecological malignancies were selected based on the following selection criteria: (1) evidence of causal effects between education and potential mediators,39 and (2) significant causal associations between the mediators and EC/OC. The final mediation analysis incorporated six mediators for EC and two mediators for OC, all of which satisfied these criteria. To estimate the proportion of the effect of education on EC or OC that was mediated, a two-step MR analysis was performed.40 First, IVW was used to estimate the effect of educational attainment on the mediators (β1). Second, IVW was used to assess the effect of the mediators on EC or OC (β2). The mediation effect was calculated (via coefficient product testing) as β1×β241 with a 95% CI. The total effect (β) was derived from the IVW estimate of the effect of educational attainment on EC or OC.42 The mediated proportion was calculated as (β1×β2)/β with a bootstrapped 95% CI.
Results
Genetic Estimation of the Impact of Educational Attainment on Gynecological Malignancy Risk
The GWAS on educational attainment included a sample size of 1,131,881 individuals.18 The MR analysis revealed a strong protective association between educational attainment and gynecological malignancies, with odds ratios (ORs) of 0.71 (95% CI: 0.61–0.83) for overall EC, 0.65 (95% CI: 0.54–0.77) for EEC, 0.84 (95% CI: 0.73–0.97) for overall OC, 0.78 (95% CI: 0.66–0.92) for ovarian serous carcinoma (OSC), 0.60 (95% CI: 0.38–0.95) for CC, and 0.61 (95% CI: 0.48–0.77) for cervical cancer in situ. However, educational attainment was not causally associated with NEEC, ovarian endometrioid cancer, ovarian mucinous carcinoma, ovarian clear cell carcinoma, cervical squamous carcinoma, cervical adenocarcinoma, or vulvar cancer (Figure 3). Sensitivity analyses assessing potential bias arising from genetic pleiotropy confirmed the robustness of these associations (Supplementary Table S21), except for CC where only the IVW result was statistically significant.
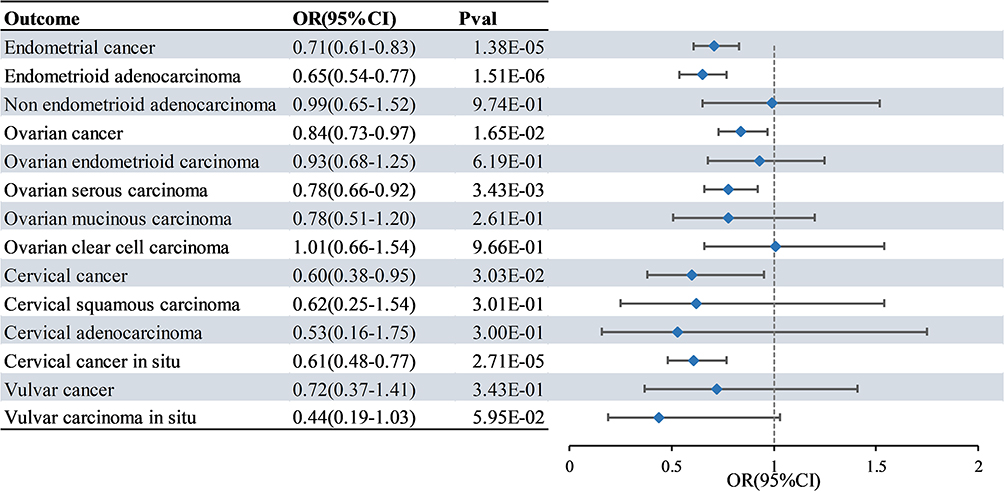 |
Figure 3 Mendelian randomization estimates of associations between educational attainment and gynecological malignancies. The forest plot depicts the causal relationship between educational attainment and gynecological cancers revealed by the inverse variance–weighted two-sample mendelian randomization analysis, with educational attainment as the exposure event and gynecological cancer as the outcome event. Abbreviations: OR, odds ratio; CI, confidence interval. |
The Association Between Genetically Estimated Educational Attainment and Previously Reported Risk Factors
The UVMR analysis revealed significant associations between educational attainment and the 18 selected potential mediators. More years of formal education were associated with lower BMI (95% CI: 0.74–0.86), reduced BFP (95% CI: 0.75–0.91), decreased WHR (95% CI: 0.84–0.96), lower smoking frequency (95% CI: 0.65–0.76), higher SWB (95% CI: 1.06–1.17), fewer depressive symptoms (95% CI: 0.77–0.84), and reduced risk of major depression (95% CI: 0.73–0.85). Education also showed positive associations with reproductive mediators including age at first birth (95% CI: 6.03–12.23), age at last live birth (95% CI: 1.64–1.77), and age at menopause (95% CI: 1.14–1.25). Higher educational attainment was linked to favorable metabolic profiles, including lower SBP (95% CI: 0.07–0.25), increased coffee consumption (95% CI: 1.08–1.13), higher cholesterol levels (95% CI: 1.02–1.04), reduced triglycerides (95% CI: 0.80–0.93), decreased fasting insulin (95% CI: 0.90–0.99), elevated IGF-1 levels (95% CI: 1.48–2.72), lower testosterone (95% CI: 0.89–0.98), and higher SHBG concentrations (95% CI: 1.11–1.28) (Figure 4). These IVW estimates were robustly supported by other sensitivity analyses, and the effect directions remained consistent across multiple modeling approaches (Supplementary Table S22).
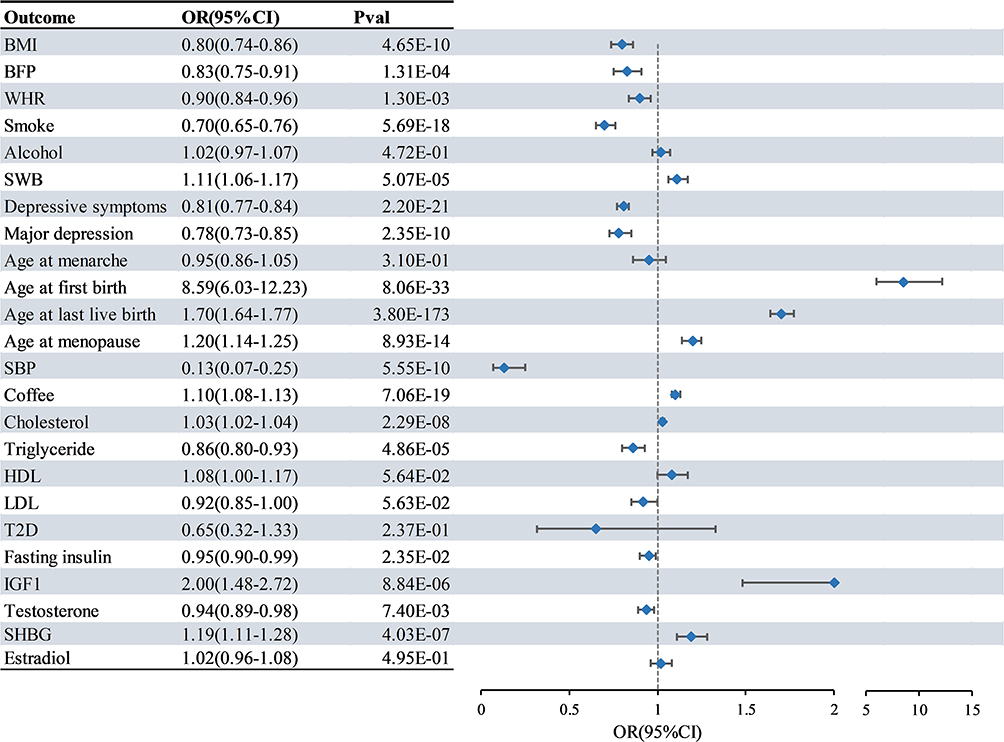 |
Figure 4 Mendelian randomization estimates of associations between educational attainment and mediators. The forest plot depicts the causal estimates between educational attainment and candidate mediators revealed by the inverse variance–weighted two-sample mendelian randomization analysis, with educational attainment as the exposure event and candidate mediators as the outcome event. Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index; BFP, body fat percentage; WHR, waist-hip ratio; SWB, subjective well-being; SBP, systolic blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein; T2D, type 2 diabetes; IGF-1, insulin-like growth factor-1; SHBG, sex hormone-binding globulin. |
Evaluating the Influences of Potential Risk Factors on Gynecological Malignancies
Among the 24 candidate mediators, 18 were shown to have a causal relationship with educational attainment and were thus included in the MR analysis of gynecological malignancies. The IVW analysis results showed that higher BMI (OR 1.89; 95% CI: 1.69–2.11, p < 0.001), BFP (OR 2.11; 95% CI: 1.48–3.00, p < 0.001), age at menopause (OR 1.23; 95% CI: 1.10–1.38, p < 0.001), fasting insulin (OR 2.07; 95% CI: 1.13–3.83, p = 0.019), and testosterone (OR 1.58, 95% CI: 1.38–1.82, p < 0.001) were all significantly associated with an increased risk of EC. Higher SHBG (OR 0.83; 95% CI: 0.75–0.91, p < 0.001) was associated with a reduced risk of EC. Higher BMI (OR 1.12; 95% CI: 1.02–1.24, p = 0.023) and age at menopause (OR 1.12; 95% CI: 1.02–1.24, p = 0.016) were associated with an increased risk of OC. None of these 18 factors showed any significant relationship with CC (Figure 5). Further information is provided in Supplementary Tables S23–S25.
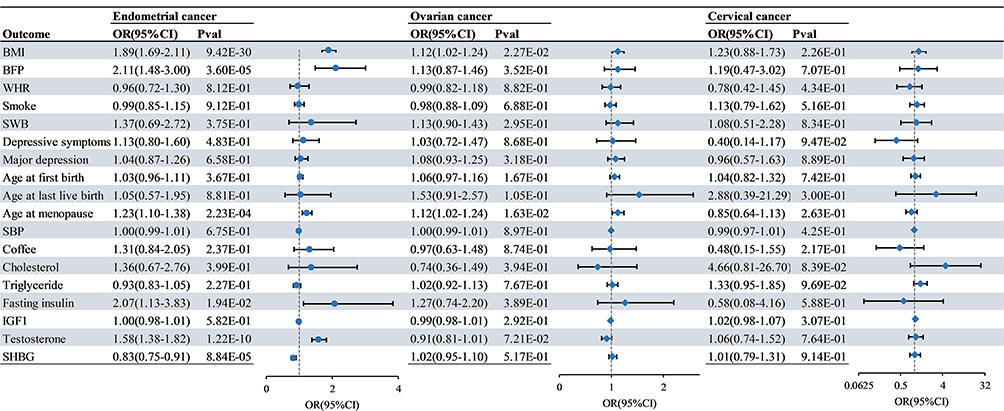 |
Figure 5 Associations between genetically estimated mediators and gynecological malignancies. The forest plot depicts the causal relationship between candidate mediators and gynecological malignancies revealed by the inverse variance–weighted two-sample mendelian randomization analysis, with mediators as the exposure event and gynecological malignancies as the outcome event. Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index; BFP, body fat percentage; WHR, waist-hip ratio; SWB, subjective well-being; SBP, systolic blood pressure; IGF-1, insulin-like growth factor-1; SHBG, sex hormone-binding globulin. |
Mendelian-Randomized Mediation Analysis of Mediators in the Association Between Educational Attainment and Gynecological Malignancies
The total effect of educational attainment on EC was β = −0.34 (95% CI: −0.49, −0.19). The mediation analysis revealed that six factors mediated the relationship between educational attainment and overall EC risk, namely: BMI (42.23% mediated, 95% CI: 26.71–57.75%, p < 0.001), BFP (41.67% mediated, 95% CI: 10.95–72.39%, p = 0.005), age at menopause (−11.05% mediated, 95% CI: −17.60 to −4.51%, p < 0.001), fasting insulin (35.84% mediated, 95% CI: 3.23–68.44%, p= 0.022), testosterone (8.80% mediated, 95% CI: 1.64–15.96%, p = 0.013), and SHBG (9.82% mediated, 95% CI: 3.31–16.33%, p = 0.002). The evidence also shows that BMI (15.16% mediated, 95% CI: 0.51–29.81%, p = 0.032) and age at menopause (−12.03% mediated, 95% CI: −22.47 to −1.6%, p = 0.022) mediated the association between educational attainment and OC risk (Table 2).
Discussion
This two-sample MR study demonstrated that genetically predicted higher educational attainment confers protective effects against the assessed gynecological malignancies (i.e., EC, OC, and CC).
Previous findings on the relationship between educational attainment and EC have been inconsistent. Mouw et al suggested that women with lower levels of educational attainment had a lower risk of EC,43 whereas Wang et al found that lower educational attainment was a causal risk factor for EC, particularly in EEC patients.1 In our study, low educational attainment was identified as a risk factor for EC. We also demonstrated that low educational attainment is also a risk factor for both OC and CC. Histological subtype analysis revealed that educational attainment primarily had a causal association with EEC and OSC, but not with other subtypes. This discrepancy may be attributable to the differences in clinical and pathological characteristics among these different histological subtypes.
Consistent with previous research findings, educational attainment demonstrated causal relationships with numerous factors, including cardiometabolic risk factors. A genetically predicted 1-SD (4.2 years) increase in higher education was associated with higher high-density lipoprotein, lower SBP, lower BMI, lower WHR, lower BFP, lower triglycerides, and reduced risk of major depressive disorder.44 Our study confirms the causal associations between education and multiple factors, namely: obesity-related markers (BMI, BFP, WHR); smoking; emotional factors (SWB, depressive symptoms, major depression); reproductive factors (age at first birth, age at last live birth, age at menopause); cardiovascular markers (SBP, cholesterol, triglycerides); and glucose or hormone-related factors (fasting insulin, IGF-1, testosterone, SHBG).
Obesity,45 diabetes, early menarche, nulliparity, late menopause, advanced age (≥55 years old), and tamoxifen use are typically regarded as common risk factors for EC.46 The substantial impact of obesity is particularly noteworthy. Laaksonen et al estimated that overweight and obesity can account for 41.9% (95% CI 32.3–50.1) of EC cases. Obesity alone contributed 34.5% (95% CI 27.5–40.9) while also increasing OC risk.47 Notably, obesity demonstrates subtype-specific effects, with a strong association with earlier diagnosis of EEC but no significant association with non-endometrioid subtypes, thus reflecting distinct pathogenic pathways.48 Mediation analysis quantified the central role of obesity in the relationship between educational attainment and cancer. BMI mediated 42.23% of the protective effect of education against EC and 15.16% of its protective effect against OC, whereas BFP mediated 41.67% of the association between education and EC risk. Our findings corroborate the findings of previous MR-based studies.1 Wang et al suggested that low educational attainment influences EC risk through potential mediators such as obesity, WHR, and diabetes. We also confirmed that the mediating effect of testosterone, fasting insulin, and SHBG also mediate the causal effect of education on EC risk.
The results support previous findings that women with late menopause have an increased risk of OC and EC.49 Studies have shown that women with lower educational levels are at a greater risk of undergoing natural menopause at a younger age.50 Crucially, our MR analysis establishes that higher educational attainment causally delays menopause, and this delay attenuated the benefit of education on EC and OC. This reveals a complex mediation pathway whereby the protective effect of education against cancer is counterbalanced by its effect on menopausal timing. Our results also align with existing evidence, showing no causal relationship between coffee consumption/IGF-1 and EC/OC.51,52 In addition, circulating lipid levels did not exhibit any strong association with OC risk.53 Both observational studies and Mendelian randomization studies have demonstrated a causal association between elevated circulating testosterone levels, decreased SHBG levels, and an increased risk of EC.54 And educational attainment may influence women’s BMI, insulin levels, and hormone levels through factors such as exercise, diet,12 thereby regulating the risk of gynecological malignancies. Surprisingly, while hypertension is associated with higher overall risk of EC in observational studies,55 our UVMR analysis found no causal relationship between hypertension and EC, suggesting that certain conventionally recognized risk factors may not play direct mediating roles in the association between education and cancer risk.
These findings highlight the extensive influence that education has across diverse aspects of health, establishing it as a valuable exposure factor for future research. Although direct modification of educational attainment may be challenging, later-life knowledge acquisition could potentially replicate its protective benefits.56 Importantly, the identified mediators serve as actionable targets for interventions aimed at mitigating gynecological cancer risk. This offers a practical approach to leveraging the health benefits of education, even in populations with limited formal schooling. The results of this study indicate that obesity is the predominant modifiable factor in EC/OC pathogenesis and underscore the need for targeted weight management strategies—particularly among populations with lower educational attainment—to reduce the substantial burden of obesity-driven gynecological malignancies.
This study has several limitations. First, Some datasets are derived from meta-analyses or combined cohort studies, and a certain degree of sample overlap cannot be completely ruled out, while the use of powerful genetic tools and the consistency of the results of each sensitivity analysis have all proved the reliability of our research findings. Secondly, although we examined numerous potential mediators, our analyses could not fully elucidate the mechanisms underlying the associations between education and gynecological cancer risk. The results related to CC should be interpreted with caution and regarded as exploratory. Further validation using datasets with larger sample sizes, diverse populations, and additional GWAS data is required to determine the stability of the association between education attainment and CC, as well as whether it reflects a causal relationship. Further verification can be conducted by investigating the association with HPV-related pathways. Notably, while genetically predicted higher educational attainment showed a protective effect against CC, this relationship appears to be mediated through pathways beyond the factors we investigated. This warrants the exploration of additional targets (eg., age at first sexual intercourse). Also, persistent SNP heterogeneity may have introduced potential bias and affected the robustness of our MR findings. Moreover, although both BMI and BFP serve as significant mediators in the causal pathway between educational attainment and EC risk, their close correlation may lead to collinearity issues. This could potentially inflate the reported mediation effects, necessitating cautious interpretation. Nevertheless, both mediators consistently reflect that obesity is the key mediating factor. Finally, since the GWAS data used in this study were primarily derived from European populations, and given that different populations have distinct genetic backgrounds, socioeconomic structures, and health determinants, the observed associations and causal inferences might differ in other populations. Therefore, these findings may not necessarily apply to other ethnic groups.
Our research findings provide insight into the value of prioritizing educational policies and reducing educational inequality as effective preventive measures against the burden of gynecological malignancies such as EC and OC.
Conclusion
By employing a causal genetic epidemiological model, our MR cohort study findings indicated that higher educational attainment was associated with a reduced risk of EC, OC, and CC. The mediation analysis further revealed that BMI and the age of natural menopause were important mediating factors in the association between educational attainment and EC/OC. In addition, BFP, testosterone, fasting insulin, and SHBG levels also mediated part of the effect of educational attainment on EC.
Therefore, interventions aimed at reducing BMI and non-delayed age at natural menopause would lead to a decrease in EC and OC attributable to lower educational attainment. Additionally, reductions in testosterone, fasting insulin, and SHBG would also lower the risk of EC associated with lower educational levels. The majority of the associations between genetically estimated educational attainment and EC, OC, and CC are mediated through pathways other than these risk factors, necessitating further research into other targetable mediators.
Data Sharing Statement
Analysis in this study was conducted using datasets that are publicly available.
Ethics Statement
The study was conducted in accordance with the Declaration of Helsinki. This work utilized the results of published GWAS summary statistics, and thus ethical approval was not required. According to Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Beings (2023, China), no additional ethical approval was required.
Acknowledgments
We sincerely thank all the websites, authors and participants that provided the GWAS summary statistics.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by the National Natural Science Foundation of China (NSFC 82172819) to H.Z., and the Natural Science Foundation of Jiangsu Province (BK20220187) to F.G.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang Q, Wang R, Chen C. et al. Educational attainment and endometrial cancer: a Mendelian randomization study. Front Genet. 2022;13:993731. doi:10.3389/fgene.2022.993731
2. Zhao SS, Holmes MV, Zheng J, Sanderson E, Carter AR. The impact of education inequality on rheumatoid arthritis risk is mediated by smoking and body mass index: mendelian randomization study. Rheumatology. 2022;61(5):2167–14. doi:10.1093/rheumatology/keab654
3. Rogne T, Gill D, Liew Z, et al. Mediating Factors in the Association of Maternal Educational Level With Pregnancy Outcomes. JAMA Network Open. 2024;7(1):e2351166. doi:10.1001/jamanetworkopen.2023.51166
4. Zhu P, Ren J, Sun J, et al. The association of endogenous sex hormones with endometrial cancer risk: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2025;310:113997. doi:10.1016/j.ejogrb.2025.113997
5. Dalmartello M, Vermunt J, Negri E, Levi F, La Vecchia C. Adult lifetime body mass index trajectories and endometrial cancer risk. Bjog. 2022;129(9):1521–1529. doi:10.1111/1471-0528.17087
6. Larsson SC, Carter P, Kar S, et al. Smoking, alcohol consumption, and cancer: a mendelian randomisation study in UK Biobank and international genetic consortia participants. PLoS Med. 2020;17(7):e1003178. doi:10.1371/journal.pmed.1003178
7. Liu S, Feng S, Du F, Zhang K, Shen Y. Association of smoking, alcohol, and coffee consumption with the risk of ovarian cancer and prognosis: a mendelian randomization study. BMC Cancer. 2023;23(1):256. doi:10.1186/s12885-023-10737-1
8. Wang X, Glubb DM, O’Mara TA. Dietary Factors and Endometrial Cancer Risk: a Mendelian Randomization Study. Nutrients. 2023;15(3). doi:10.3390/nu15030603
9. Hazelwood E, Sanderson E, Tan VY, et al. Identifying molecular mediators of the relationship between body mass index and endometrial cancer risk: a Mendelian randomization analysis. BMC Med. 2022;20(1):125. doi:10.1186/s12916-022-02322-3
10. Guo J-Z, Xiao Q, Gao S, et al. Review of Mendelian Randomization Studies on Ovarian Cancer. Front Oncol. 2021;11:681396. doi:10.3389/fonc.2021.681396
11. Qian H, Liu Y, Choi H, Lee S. Exploring the causal effects of physical activity, diet, and nutrition on hypertension and hyperlipidemia: a multivariable Mendelian randomization analysis. BMC Cardiovasc Disord. 2025;25(1):196. doi:10.1186/s12872-025-04539-5
12. Ruiz-González D, Cavero-Redondo I, Hernández-Martínez A, et al. Comparative efficacy of exercise, diet and/or pharmacological interventions on BMI, ovulation, and hormonal profile in reproductive-aged women with overweight or obesity: a systematic review and network meta-analysis. Hum Reprod Update. 2024;30(4):472–487. doi:10.1093/humupd/dmae008
13. Davies NM, Holmes MV, Davey Smith G. Reading Mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ. 2018;362:k601. doi:10.1136/bmj.k601
14. Relton CL, Davey Smith G. Two-step epigenetic Mendelian randomization: a strategy for establishing the causal role of epigenetic processes in pathways to disease. Int J Epidemiol. 2012;41(1):161–176. doi:10.1093/ije/dyr233
15. Carter AR, Sanderson E, Hammerton G, et al. Mendelian randomisation for mediation analysis: current methods and challenges for implementation. Eur J Epidemiol. 2021;36(5):465–478. doi:10.1007/s10654-021-00757-1
16. Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the Reporting of Observational Studies in Epidemiology Using Mendelian Randomization: the STROBE-MR Statement. JAMA. 2021;326(16):1614–1621. doi:10.1001/jama.2021.18236
17. Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the reporting of observational studies in epidemiology using mendelian randomisation (STROBE-MR): explanation and elaboration. BMJ. 2021;375:n2233. doi:10.1136/bmj.n2233
18. Lee JJ, Wedow R, Okbay A, et al. Gene discovery and polygenic prediction from a genome-wide association study of educational attainment in 1.1 million individuals. Nat Genet. 2018;50(8):1112–1121. doi:10.1038/s41588-018-0147-3
19. O’Mara TA, Glubb DM, Amant F, et al. Identification of nine new susceptibility loci for endometrial cancer. Nat Commun. 2018;9(1):3166. doi:10.1038/s41467-018-05427-7
20. Phelan CM, Kuchenbaecker KB, Tyrer JP, et al. Identification of 12 new susceptibility loci for different histotypes of epithelial ovarian cancer. Nat Genet. 2017;49(5):680–691. doi:10.1038/ng.3826
21. Kurki MI, Karjalainen J, Palta P, et al. FinnGen provides genetic insights from a well-phenotyped isolated population. Nature. 2023;613(7944):508–518. doi:10.1038/s41586-022-05473-8
22. Yengo L, Sidorenko J, Kemper KE, et al. Meta-analysis of genome-wide association studies for height and body mass index in ∼700000 individuals of European ancestry. Hum Mol Genet. 2018;27(20):3641–3649. doi:10.1093/hmg/ddy271
23. Lu Y, Day FR, Gustafsson S, et al. New loci for body fat percentage reveal link between adiposity and cardiometabolic disease risk. Nat Commun. 2016;7:10495. doi:10.1038/ncomms10495
24. Shungin D, Winkler TW, Croteau-Chonka DC, et al. New genetic loci link adipose and insulin biology to body fat distribution. Nature. 2015;518(7538):187–196. doi:10.1038/nature14132
25. Evangelou E, Warren HR, Mosen-Ansorena D, et al. Genetic analysis of over 1 million people identifies 535 new loci associated with blood pressure traits. Nat Genet. 2018;50(10):1412–1425. doi:10.1038/s41588-018-0205-x
26. Willer CJ, Schmidt EM, Sengupta S, et al. Discovery and refinement of loci associated with lipid levels. Nat Genet. 2013;45(11):1274–1283. doi:10.1038/ng.2797
27. Liu M, Jiang Y, Wedow R, et al. Association studies of up to 1.2 million individuals yield new insights into the genetic etiology of tobacco and alcohol use. Nat Genet. 2019;51(2):237–244. doi:10.1038/s41588-018-0307-5
28. Schumann G, Liu C, O’Reilly P, et al. KLB is associated with alcohol drinking, and its gene product β-Klotho is necessary for FGF21 regulation of alcohol preference. Proc Natl Acad Sci U S A. 2016;113(50):14372–14377. doi:10.1073/pnas.1611243113
29. Okbay A, Baselmans BM, De Neve JE, et al. Genetic variants associated with subjective well-being, depressive symptoms, and neuroticism identified through genome-wide analyses. Nat Genet. 2016;48(6):624–633. doi:10.1038/ng.3552
30. Howard DM, Adams MJ, Clarke TK, et al. Genome-wide meta-analysis of depression identifies 102 independent variants and highlights the importance of the prefrontal brain regions. Nat Neurosci. 2019;22(3):343–352. doi:10.1038/s41593-018-0326-7
31. Mahajan A, Wessel J, Willems SM, et al. Refining the accuracy of validated target identification through coding variant fine-mapping in type 2 diabetes. Nat Genet. 2018;50(4):559–571. doi:10.1038/s41588-018-0084-1
32. Manning AK, Hivert MF, Scott RA, et al. A genome-wide approach accounting for body mass index identifies genetic variants influencing fasting glycemic traits and insulin resistance. Nat Genet. 2012;44(6):659–669. doi:10.1038/ng.2274
33. Day FR, Thompson DJ, Helgason H, et al. Genomic analyses identify hundreds of variants associated with age at menarche and support a role for puberty timing in cancer risk. Nat Genet. 2017;49(6):834–841. doi:10.1038/ng.3841
34. MRC Integrative Epidemiology Unit. The Integrative Epidemiology Unit OpenGWAS project. Available from: https://gwas.mrcieu.ac.uk/.
35. Burgess S, Butterworth A, Thompson SG. Mendelian randomization analysis with multiple genetic variants using summarized data. Genet Epidemiol. 2013;37(7):658–665. doi:10.1002/gepi.21758
36. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–525. doi:10.1093/ije/dyv080
37. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent Estimation in Mendelian Randomization with Some Invalid Instruments Using a Weighted Median Estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
38. Hartwig FP, Davey Smith G, Bowden J. Robust inference in summary data Mendelian randomization via the zero modal pleiotropy assumption. Int J Epidemiol. 2017;46(6):1985–1998. doi:10.1093/ije/dyx102
39. Zhang J, Chen Z, Pärna K, et al. Mediators of the association between educational attainment and type 2 diabetes mellitus: a two-step multivariable Mendelian randomisation study. Diabetologia. 2022;65(8):1364–1374. doi:10.1007/s00125-022-05705-6
40. Burgess S, Daniel RM, Butterworth AS, Thompson SG. Network Mendelian randomization: using genetic variants as instrumental variables to investigate mediation in causal pathways. Int J Epidemiol. 2015;44(2):484–495. doi:10.1093/ije/dyu176
41. VanderWeele TJ. Mediation Analysis: a Practitioner’s Guide. Annu Rev Public Health. 2016;37:17–32. doi:10.1146/annurev-publhealth-032315-021402
42. Carter AR, Gill D, Davies NM, et al. Understanding the consequences of education inequality on cardiovascular disease: mendelian randomisation study. BMJ. 2019;365:I1855. doi:10.1136/bmj.l1855
43. Mouw T, Koster A, Wright ME, et al. Education and risk of cancer in a large cohort of men and women in the United States. PLoS One. 2008;3(11):e3639. doi:10.1371/journal.pone.0003639
44. Wang Y, Ye C, Kong L, et al. Independent Associations of Education, Intelligence, and Cognition With Hypertension and the Mediating Effects of Cardiometabolic Risk Factors: a Mendelian Randomization Study. Hypertension. 2023;80(1):192–203. doi:10.1161/hypertensionaha.122.20286
45. Tong Y, Zhou T, Kong Y, Liu Z, Lai Z. Causal impact of obesity class stratification and endometrial cancer subtypes: an integrated Mendelian randomization and Global Burden of Disease Study 2021 analysis. Int J Surg. 2025;111(10):6783–6801. doi:10.1097/js9.0000000000002883
46. Guo JZ, Wu QJ, Liu FH, et al. Review of Mendelian Randomization Studies on Endometrial Cancer. Front Endocrinol. 2022;13:783150. doi:10.3389/fendo.2022.783150
47. Laaksonen MA, Arriaga ME, Canfell K, et al. The preventable burden of endometrial and ovarian cancers in Australia: a pooled cohort study. Gynecol Oncol. 2019;153(3):580–588. doi:10.1016/j.ygyno.2019.03.102
48. Freuer D, Linseisen J, O’Mara TA, et al. Body Fat Distribution and Risk of Breast, Endometrial, and Ovarian Cancer: a Two-Sample Mendelian Randomization Study. Cancers. 2021;13(20). doi:10.3390/cancers13205053
49. Li Z, Peng Q, Lin Y, et al. Female Reproductive Traits and Late-Life Hormone-Sensitive Cancer Risk: a Mendelian Randomization Study. Cancer Prev Res. 2026;19(4):219–228. doi:10.1158/1940-6207.capr-25-0176
50. Ding X, Tang R, Zhu J, et al. An Appraisal of the Role of Previously Reported Risk Factors in the Age at Menopause Using Mendelian Randomization. Front Genet. 2020;11:507. doi:10.3389/fgene.2020.00507
51. Huang C, Bu H, Wang Y, et al. Association between coffee and tea consumption and ovarian cancer incidence: a prospective analysis in the PLCO dataset. Int J Cancer. 2024;155(6):1033–1044. doi:10.1002/ijc.34982
52. Larsson SC, Carter P, Vithayathil M, et al. Insulin-like growth factor-1 and site-specific cancers: a Mendelian randomization study. Cancer Med. 2020;9(18):6836–6842. doi:10.1002/cam4.3345
53. Trabert B, Hathaway CA, Rice MS, et al. Ovarian Cancer Risk in Relation to Blood Cholesterol and Triglycerides. Cancer Epidemiol Biomarkers Prev. 2021;30(11):2044–2051. doi:10.1158/1055-9965.epi-21-0443
54. Mullee A, Dimou N, Allen N, et al. Testosterone, sex hormone-binding globulin, insulin-like growth factor-1 and endometrial cancer risk: observational and Mendelian randomization analyses. Br J Cancer. 2021;125(9):1308–1317. doi:10.1038/s41416-021-01518-3
55. Drab A, Kanadys W, Malm M, et al. Association of endometrial cancer risk with hypertension- an updated meta-analysis of observational studies. Sci Rep. 2024;14(1):24884. doi:10.1038/s41598-024-76896-8
56. García-Mayor J, Moreno-Llamas A, la Cruz-Sánchez E. High educational attainment redresses the effect of occupational social class on health-related lifestyle: findings from four Spanish national health surveys. Ann Epidemiol. 2021;58:29–37. doi:10.1016/j.annepidem.2021.02.010
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Genetically Predicted Serum Albumin and Risk of Colorectal Cancer: A Bidirectional Mendelian Randomization Study
Lv L, Sun X, Liu B, Song J, Wu DJH, Gao Y, Li A, Hu X, Mao Y, Ye D
Clinical Epidemiology 2022, 14:771-778
Published Date: 21 June 2022
Causal Relationship Between Endometriosis and Pelvic Inflammatory Diseases: Mendelian Randomization Study
Liu K, Liu X, Cao T, Cui X, Sun P, Zhang L, Wu X
International Journal of Women's Health 2024, 16:727-735
Published Date: 24 April 2024
Exploring the Causal Relationship Between Frailty and Chronic Obstructive Pulmonary Disease: Insights From Bidirectional Mendelian Randomization and Mediation Analysis
Cheng Z, Wu J, Xu C, Yan X
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:193-205
Published Date: 25 January 2025
Assessing Causality Between Androgenetic Alopecia with Depression: A Bidirectional Mendelian Randomization Study
Li H, Cai H, Li P, Zeng Y, Zhang Y
Clinical, Cosmetic and Investigational Dermatology 2025, 18:445-451
Published Date: 22 February 2025
The Mediation Role of Insulin Resistance and Chronic Systemic Inflammation in the Association Between Obesity and NAFLD: Two Cross-Sectional and a Mendelian Randomization Study
Huang X, Chen Q, Su Q, Gong J, Wu L, Xiang L, Li W, Chen J, Zhao H, Huang W, Du S, Ye W
Clinical Epidemiology 2025, 17:287-302
Published Date: 24 March 2025