Back to Journals » International Journal of Women's Health » Volume 18
Association Between Daily Sitting Time and Urinary Leakage and the Double Mediation Effects of Inflammation and Physical Activity: A Cross-Sectional Study
Authors Huang C, Wang L, Hu H, Li X ![]()
Received 30 October 2025
Accepted for publication 4 February 2026
Published 23 February 2026 Volume 2026:18 577871
DOI https://doi.org/10.2147/IJWH.S577871
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Chunling Huang,* Li Wang,* Huiwen Hu, Xia Li
Changzhou Maternal and Child Health Care Hospital, Changzhou Medical Center, Nanjing Medical University, Changzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xia Li; Huiwen Hu, Changzhou Maternal and Child Health Care Hospital, Changzhou Medical Center, Nanjing Medical University, No. 16 Dingxiang Road, Changzhou, Jiangsu, 213000, People’s Republic of China, Email [email protected]; [email protected]
Background: Sedentary behavior (SB), recognized as a health risk, may contribute to urinary leakage (UL). This study examined the association between daily sitting time (DST) and UL risk, investigating inflammatory markers as potential mediators and leisure-time physical activity (LTPA) as a mediator.
Methods: We conducted a cross-sectional analysis of data from the National Health and Nutrition Examination Survey (NHANES) spanning 2007 to 2020, involving 20,168 adult participants. Information on UL, DST, Dietary Inflammatory Index (DII), Body Mass Index (BMI), and Neutrophil-to-Lymphocyte Ratio (NLR) was collected through standardized questionnaires and 24-hour recall interviews. Logistic regression models assessed DST, LTPA, and UL relationships, adjusting for relevant covariates. Mediation analysis evaluated DII, BMI, and NLR’s mediating roles in the DST-UL association.
Results: The overall prevalence of UL among participants was 29.19%. Our findings revealed a significant positive association between longer DST and UL risk. Notably, individuals engaging in adequate LTPA demonstrated an attenuated association between DST and UL. Furthermore, mediation analysis identified significant parallel double mediating effects of DII-BMI and BMI-NLR on the relationship between DST and UL. However, no significant mediating effect was observed for DII-NLR, this suggests that DII, BMI, and NLR might jointly mediate the relationship of DST on UL risk.
Conclusion: These findings suggest that prolonged sitting may be associated with higher UL risk through inflammatory mechanisms, and that LTPA may mitigate this risk. Further research is needed to validate these results and explore the underlying biological pathways.
Keywords: urinary leakage, daily sitting time, inflammation, National Health and Nutrition Examination Survey
A Letter to the Editor has been published for this article.
Introduction
Urinary leakage (UL), also known as urinary incontinence (UI), is a widespread health concern characterized by the involuntary loss of urine. In the United States, this condition affects a substantial portion of the population.1 According to estimates, the prevalence ranges from 9.3% to 30.8% among women and 2.6% to 20.9% among men, with a notable increase in prevalence observed with advancing age.2 UL can have a profound impact on an individual’s life, leading to compromised psychosocial well-being, diminished self-confidence, and reduced social interactions and interpersonal relationships.3 Therefore, it is essential to identify the risk factors and mechanisms underlying UL in order to provide comprehensive disease management.
Sedentary behavior (SB) is recognized as an independent risk factor for numerous health-related issues. SB refers to any waking activity performed while sitting, reclining, or lying down that expends no more than 1.5 metabolic equivalents (METs).4 SB has been identified as a risk factor for various conditions, including diabetes, obesity, cardiovascular disease, cancer, and dementia. A cross-sectional study involving 150 women at a urology center revealed a link between SB and the occurrence of UI in postmenopausal women.5,6 Additionally, an analysis by Roig et al of women aged 60 years and older from the NHANES database demonstrated a significant association between increased sedentary time and UI in older women, suggesting that reducing prolonged sitting time may be an effective intervention for lowering UI risk.7 These studies indicate a potential association between SB and UI. However, the specific reasons and key factors behind prolonged sitting leading to UL are unclear, and elucidating its specific mechanism is particularly important.
Sedentary behavior is strongly associated with the development of systemic low-grade inflammation,8,9 potentially mediated by metabolic dysregulation such as hypertriglyceridemia and insulin resistance.10,11 To capture the inflammatory mechanism linking SB to health outcomes, selecting an appropriate marker is crucial. While blood-based markers (eg, NLR) capture the current systemic inflammatory state, the Dietary Inflammatory Index (DII) offers a unique perspective by quantifying the inflammatory potential of an individual’s long-term diet.12,13 SB is frequently accompanied by unhealthy dietary patterns, such as increased consumption of ultra-processed foods and lower intake of anti-inflammatory nutrients.14 These dietary habits elevate the DII, creating a chronic pro-inflammatory environment. Unlike direct bladder irritants, a high-DII diet may contribute to UL pathology through systemic pathways, including oxidative stress and microvascular damage, which can impair pelvic floor neuromuscular function.15,16
In addition to dietary factors, leisure-time physical activity (LTPA) is another critical factor. Research shows that LTPA can improve chronic inflammatory status by reducing cytokine production and downregulating TLR4 expression on monocytes.17 However, there is a lack of systematic research on the complex interplay between prolonged sitting, dietary inflammation (DII), and LTPA in the context of UL.
Based on this background, we hypothesize that inflammation may serve as a crucial link between SB and UL. The NHANES is an ongoing, nationally representative survey designed to assess the health and nutritional status of the US population. This survey encompasses a broad range of health-related aspects, including demographics, socioeconomic factors, dietary and health-related behaviors, and utilizes interviews, physical examinations, and laboratory tests to collect data.18 This study aims to utilize the NHANES database to investigate the relationship between DST and UL in US adults, with a particular focus on exploring the mediating role of inflammation. We believe that the findings of this study will provide valuable insights and guidance for the prevention of UL.
Materials and Methods
Study Design and Participants
The NHANES database is a population-based cross-sectional survey program conducted by the Centers for Disease Control and Prevention in the United States. It aims to assess the health and nutritional status of the American population, estimate the distribution of certain diseases and risk factors within the US population and specific subgroups, monitor trends in risk behaviors and environmental exposures, and explore emerging public health issues and new technologies. This study utilized data from the NHANES database from 2007 to 2020. Initially, 66,148 people were included, after excluding demographic data with missing values (n = 42,731), questionnaire data with missing values (n = 1,921), and variable data with missing values (n = 1,328), our final analysis included 20,168 participants who met the conditions, as shown in Figure 1. All NHANES protocols received approval from the Ethics Review Board of the National Center for Health Statistics, and written informed consent was obtained from each participant.
 |
Figure 1 Flowchart of participant selection in NHANES 2007–2020. |
Main Variables
Daily Sitting Time (DST)
The term “daily sitting time (DST)” was defined in the Questionnaire Data of Physical Activity (PAQ) survey as “Daily sitting time (Question number: PAD680): How much time do you usually spend sitting on a typical day?” The question is about sitting at work, at home, getting to and from places, or with friends, including time spent sitting at a desk, traveling in a car or bus, reading, playing cards, watching television, or using a computer. Do not include time spent sleeping. For further analysis, the time was converted into hours. According to the method by Li et al, DST was categorized into four groups: G1 (less than 4 hours per day), G2 (4 to 6 hours per day), G3 (6 to 8 hours per day), and G4 (8 hours or more per day). In the subsequent analysis, a DST of less than 4 hours per day was used as the reference.18
UL
The definition of UL came from the Questionnaire Data in the Kidney Conditions – Urology (KIQ) survey. When asked “How often have urinary leakage? (Question number: KIQ005)”, participants who answer “never” are considered not to have UL. Other responses are classified as having UL and are grouped based on their answers (UL1: Less than once a month. UL2: A few times a month. UL3: A few times a week. UL4: Every day and/or night).
NLR
NLR is a blood indicator used to assess the body’s inflammatory status and immune response. It can be obtained from the Laboratory Data in the Complete Blood Count (CBC). The formula for calculation is: NLR = neutrophil (LBDNENO)/lymphocyte (LBDLYMNO).
DII
Extracted data from the NHANES database using the 24-hour dietary recall questionnaire included 28 parameters to calculate the DII, such as total fat, saturated fat, carbohydrates, protein, alcohol, monounsaturated fat, fiber, cholesterol, n-3 fatty acids, polyunsaturated fat, vitamin B12, vitamin E, n-6 fatty acids, niacin, vitamin A, thiamine (vitamin B1), beta-carotene, folic acid, riboflavin (vitamin B2), vitamin B6, vitamin C, vitamin D, selenium, iron, magnesium, zinc, caffeine, and energy.19 Dietary intake data were energy-adjusted using the nutrient density method (per 1,000 kcal). To handle extreme values, nutrient intake was winsorized before calculating the z-scores.
LTPA
Extract the Physical Activity (PAQ) data from the NHANES database Questionnaire Data. Collect PAD660 – Minutes of vigorous recreational activities and PAD675 – Minutes of moderate recreational activities. Calculate LTPA using the formula from the literature: the total time spent on LTPA was calculated as minutes of moderate-intensity recreational activities plus twice the minutes of vigorous-intensity recreational activities. According to the 2018 Physical Activity Guidelines for Americans: individuals with no LTPA, those with LTPA greater than 0 but less than 150 minutes/week, and those with LTPA greater than or equal to 150 minutes/week are classified as inactive, insufficiently active, and sufficiently active, respectively.20
Other Covariates
BMI is defined as: Examination data includes BMI – Body Mass Index (kg/m2). Classification criteria: (under/normal weight: <25 kg/m2, overweight: 25 to 30 kg/m2, obesity: >30 kg/m2). Additionally, some covariates from the NHANES database were used, including age, race, education level, poverty-income ratio, and smoking.
Statistical Analysis
All statistical analyses were conducted following the guidelines provided by the Centers for Disease Control and Prevention (CDC), and appropriate sampling weights were applied for participant recruitment. Baseline characteristics of the included population were described and grouped by different DST. Continuous variables were summarized using mean (SD), while categorical variables were presented as percentages.
To analyze the association between DST and UL, we employed a crude model and adjusted models in logistic regression analysis: Model 1 without adjustments; Model 2 was additionally adjusted for age, gender, race, education level, poverty, and smoking status; Model 3 was further adjusted for BMI, NLR, and DII. The strength of associations was estimated using odds ratios (ORs) and their corresponding 95% confidence intervals (CIs).
Mediation analysis was performed using the mediation package in R software. Through mediation analysis, we can calculate how much of an effect needs to be mediated. This is an ideal strategy to elucidate pathways and provide statistical evidence for mechanistic analysis. In this study, the direct effect represented the correlation between DST, LTPA, and UL; the indirect effect, which was mediated by inflammatory indicators, represented the correlation between DST, LTPA, and UL; the mediation proportion represented the percentage of mediation effect. All analyses were performed using the R software (version 4.2.0, http://www.R-project.org, The R Foundation). P < 0.05 indicated statistically significant differences.
Results
Population Characteristics
From 2007 to 2020, a total of 66,148 individuals were initially recruited for the survey. After excluding those with missing data on age, education level, DST, UL and other factors, 20,168 participants were included in our study (Figure 1). Statistical analysis of these baseline characteristics revealed that increased DST was significantly associated with higher levels of inflammation markers, compared to group G1, groups G2, G3, and G4 showed significantly higher Systemic Inflammation Index (SII), Neutrophil-to-Lymphocyte Ratio (NLR), as well as elevated white blood cell (WBC) count and neutrophils (Ne) values, indicating a state of chronic inflammation. Besides, the overall incidence of UL was 29.19%. Compared to the group with G1 (26.02%), groups G2, G3, and G4 showed higher incidence and severity of UL. As DST increased, the DII gradually decreased, while the proportion below zero significantly rose (all P < 0.01). Detailed data can be found in Table 1.
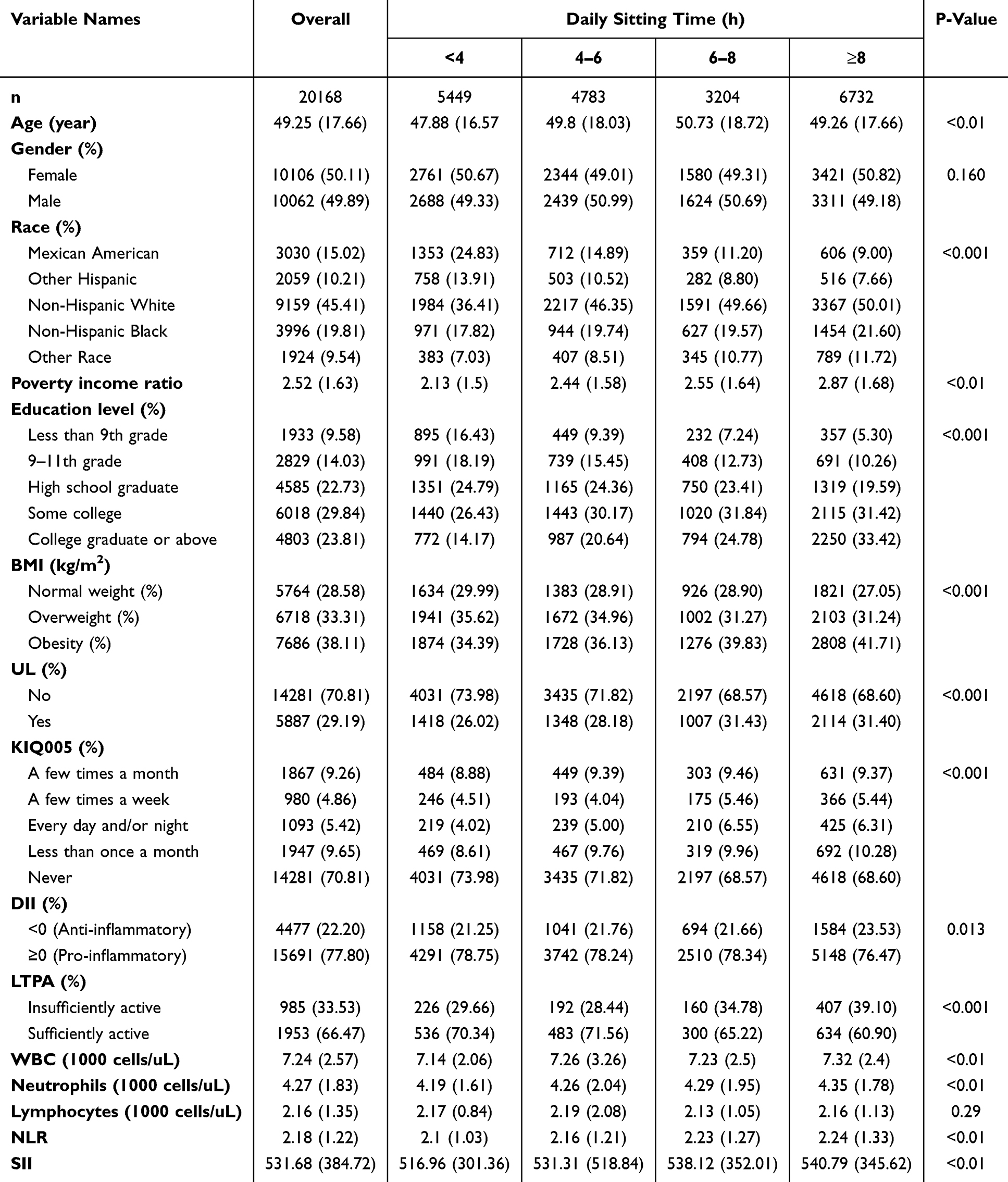 |
Table 1 Characteristics of Participants Classified by DST: NHANES 2007–2020 |
The Relationship Between DST and UL
According to the data presented in Table 2, all three models indicated a statistically significant positive correlation between DST and the risk of UL. The table listed the P-values, odds ratios (OR), and 95% confidence intervals (CI) for the three multivariable logistic regression models. In the unadjusted model (Model 1), compared to group G1, group G2 had a 12.0% increased risk of UL (OR = 1.12, 95% CI: 1.02–1.22, P = 0.014), group G3 had a 30% increased risk (OR = 1.30, 95% CI: 1.18–1.43, P < 0.001), and group G4 also face a 30% increased risk (OR = 1.30, 95% CI: 1.20–1.41, P < 0.001). In the fully adjusted model (Model 3), the association between DST and UL was not statistically significant in the 4–6 hour group (OR = 1.03, P = 0.494). However, longer sedentary durations (6–8 hours and ≥8 hours) remained significantly associated with an increased risk of UL.
 |
Table 2 Multivariable-Adjust ORs and 95% CI of DST and UL |
The Double Mediation Effects of DII-BMI-NLR
To evaluate the association of inflammation between DST and UL risk, restricted cubic spline (RCS) analysis and mediation analysis were performed. After adjusting for age, gender, race, education, poverty, and smoking status, there was a nonlinear positive correlation between NLR and the risk of UL caused by DST (P = 0) by RCS analysis. As NLR increased, the risk of UL due to DST also increased (Figure 2A). Furthermore, parallel mediation analysis revealed NLR had significant mediated effects on the association of DST with UL risk, and the proportion of mediation was 3.92% (P = 0.002) (Supplementary Figure 1). Similarly, there was a non-linear positive correlation between DII and the risk of UL caused by DST (P = 0.04). As DII increases, it further increased the risk of UL due to DST (Figure 2B). However, RCS analysis indicated that BMI showed a linear positive correlation with the risk of UL due to DST, but no nonlinear relationship was found (Supplementary Figure 2). Subsequently, we conducted a dual mediation effect analysis, significant parallel dual mediation effects were observed for DII-BMI (Summary indirect effect = 0.0042, P = 0.0000, Figure 3A) and BMI-NLR (Summary indirect effect = 0.0056, P = 0.0000, Figure 3B), whereas DII-NLR (Summary indirect effect = 0.0001, P = 0.6475, Figure 3C) did not show such effects. It is speculated that DII-BMI-NLR might jointly mediate the risk of UL due to prolonged sitting.
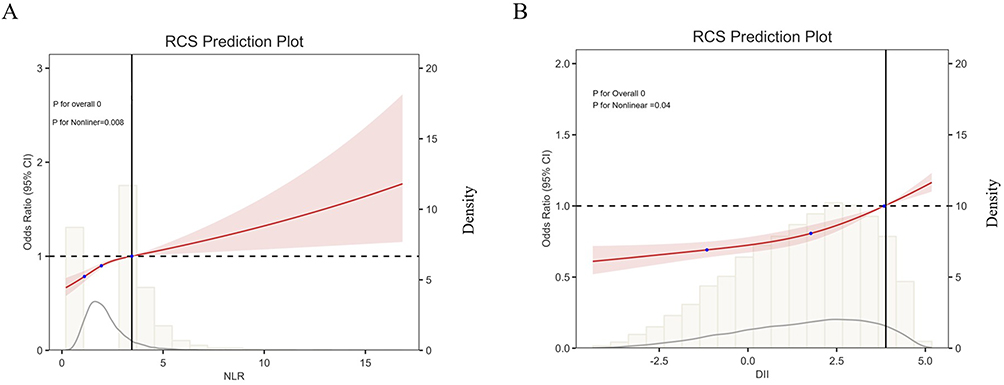 |
Figure 2 RCS revealed the association between NLR, DII, and the risk of UL caused by sedentary behavior. (A) The non-linear association between Neutrophil-to-Lymphocyte Ratio (NLR) and the risk of UL caused by sedentary behavior. (B) The non-linear association between Dietary Inflammatory Index (DII) and the risk of UL caused by sedentary behavior. In both panels, the solid red line represents the estimated Odds Ratio (OR), and the shaded area indicates the 95% Confidence Interval (CI). The horizontal dashed line represents the reference risk (OR = 1.0). The blue dots/histograms in the background represent the distribution density of the participants (referenced by the secondary y-axis). |
 |
Figure 3 Path diagram of the double mediation analysis of DII, BMI and NLR on the relationship between DST and UL. (A–C) The graphs represented the mediating role of DII-BMI, BMI-NLR and DII-NLR, respectively. The arrows indicate the direction of the hypothesized causal paths. The numbers adjacent to the arrows represent the standardized effect estimates (coefficients) and their statistical significance (P-values). |
LTPA Improved the Risk of UL Caused by Prolonged Sitting Through BMI
Current studies have shown the effectiveness of exercise interventions on UI and pelvic organ prolapse in pregnant and postpartum women.21 In our study, LTPA was also found to have had a linear negative correlation with the risk of UL caused by prolonged DST, but no non-linear relationship existed (Figure 4A). A double mediation analysis revealed that the LTPA-BMI had a significant parallel double mediation effect, suggesting that moderate LTPA might have reduced the risk of UL caused by prolonged DST by improving BMI (Figure 4B).
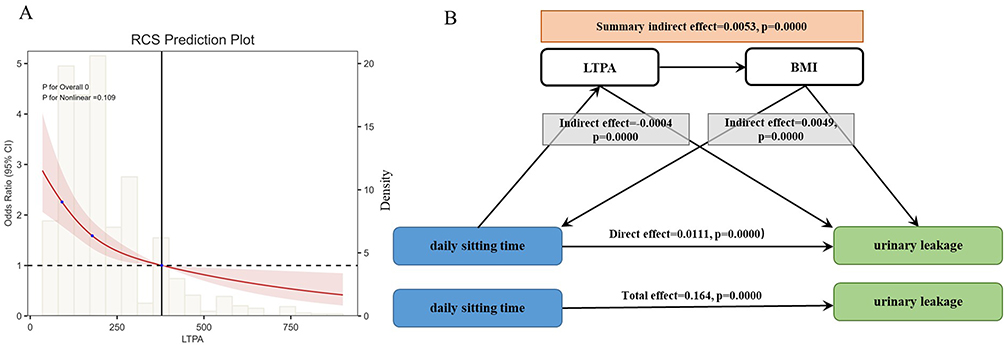 |
Figure 4 The association between LTPA and UL (A) RCS revealed the association between LTPA and the risk of UL caused by sedentary behavior. The solid red line represents the OR, the shaded area indicates the 95% CI, and the background elements represent the data density. (B) The mediating role of LTPA-BMI. The arrows indicate the mediation pathways, and the values represent the effect sizes of the direct and indirect effects. |
Discussion
This research utilized data from the NHANES to investigate the association between DST and UL and revealed meaningful and practical results. First, we observed a significant positive correlation between DST and UL, and found that inflammatory markers played a certain role in this association through their double mediation effect. Specifically, our study revealed the mediating effects of DII-BMI and BMI-NLR in the relationship between DST and UL for the first time, providing a deeper perspective on the complex mechanisms underlying this association.
Consistent with previous studies, our research demonstrated a significant association between DST and increased risk of UL, even after adjusting for confounding factors such as age, sex, race, education level, poverty, and smoking. For instance, a systematic review conducted by Faleiro et al showed that a sedentary lifestyle and less than 150 minutes of physical activity per week are at risk of developing UI. Walking (at least 30 minutes) and physical activities (600–1,500 and 600 METs per minute per week) can prevent UI.22 Furthermore, prolonged sitting can lead to the accumulation of abdominal fat, increasing intra-abdominal pressure, and subsequently increasing the pressure on the bladder and pelvic muscles, further increasing the risk of UI.23
Further analysis revealed that inflammatory factors play a mediating role in the relationship between DST and UL risk. NLR and DII as inflammatory markers showed a non-linear positive correlation with DST, even after adjusting for confounding factors. This suggests that inflammatory reactions may be an important bridge connecting DST and UL risk. The possible mechanism is that prolonged sitting leads to chronic low-grade inflammation, characterized by elevated levels of inflammatory factors such as C-reactive protein (CRP) and tumor necrosis factor-alpha (TNF-α).24 These inflammatory factors can affect the pelvic muscle tissue, leading to muscle damage and subsequently increasing the risk of UL.25 It is worth noting that in our baseline characteristics (Table 1), individuals with longer sitting times tended to have lower DII scores (indicating a more anti-inflammatory diet). This observation may be attributed to socioeconomic disparities. As shown in Table 1, participants in the highest sitting time group (≥8 h/day) had significantly higher education levels (College graduate: 33.42% vs 14.17% in the lowest sitting group). Higher socioeconomic status is often associated with sedentary white-collar occupations but also with higher health literacy and better access to high-quality nutrition, resulting in lower DII scores despite prolonged sitting.
Additionally, this study found that BMI was linearly positively correlated with the risk of UL caused by prolonged sitting and observed a parallel double mediation effect of DII-BMI and BMI-NLR. LTPA can reduce the risk of UL caused by prolonged sitting. DII reflects the long-term impact of dietary intake on the body’s inflammatory state, with high DII diets, such as high-sugar and high-saturated fat diets, promoting the production of more inflammatory factors and exacerbating inflammatory reactions.26 BMI reflects the overall fat level of the body, particularly abdominal fat, which is closely related to chronic low-grade inflammation and increases intra-abdominal pressure, putting more pressure on the pelvic muscles.27 This suggests that improving dietary structure, controlling weight, and engaging in appropriate physical activity may be effective strategies to reduce the risk of UL in individuals with prolonged sitting.
However, there are also some limitations. First, the cross-sectional design limits the ability to establish temporality or causality. Consequently, the mediation analyses presented in this study should be interpreted as statistical associations rather than confirmed causal pathways. Second, this study only included a limited number of inflammatory markers, and future studies should comprehensively evaluate the role of inflammation in the relationship between DST and UL risk. Third, the definition of UL was based on self-reported questionnaire data that did not distinguish between specific subtypes (eg, stress, urge, or mixed incontinence), which may introduce potential bias in interpreting the specific pathological mechanisms. Additionally, the study sample was sourced from the NHANES database, which may have selection bias and information bias. Therefore, more diverse data sources are needed to support our conclusions. In summary, the study findings demonstrate a significant association between prolonged sitting time and increased UL risk, and inflammatory reactions may be a key mechanism. Future prospective studies are needed to verify these findings and explore potential intervention measures, such as randomized controlled trials, to evaluate the effectiveness of reducing sitting time, improving dietary structure, and controlling weight in reducing UL risk.
Conclusion
Our research has revealed a strong link between prolonged sitting and an increased risk of UL. This association appears to be associated with inflammatory biomarkers, with the “dual mediation effect” highlighting the potential role of inflammation in this process. Encouragingly, our findings suggest that engaging in regular LTPA can help mitigate the risk of UL associated with prolonged sitting. Therefore, adopting a holistic approach that includes a balanced diet, weight management, and adequate physical activity may be key to reducing the risk of UL. These findings offer valuable insights for preventing UL and provide a foundation for future research to confirm these findings and investigate potential interventions.
Data Sharing Statement
Publicly available datasets were analyzed in this study. This data can be found here: https://www.cdc.gov/nchs/nhanes/index.htm. The analytic datasets generated during the current study are available from the corresponding author (Xia Li) upon reasonable request.
Ethics Approval and Consent to Participate
The NHANES protocols were approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board, and written informed consent was obtained from all participants. Furthermore, as this study involves the secondary analysis of publicly available, de-identified data, it is exempt from local ethical review requirements in accordance with Item 1 and Item 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (2023) in China.
Acknowledgments
This paper has been uploaded to medRxiv as a preprint: https://www.medrxiv.org/content/10.1101/2025.04.22.25326195v1.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Clinical Research Project of Changzhou Medical Center, Nanjing Medical University (CMCC202315), Nanjing Medical University Science and Technology Development Foundation Project (NMUB20250167), Changzhou City Science and Technology Bureau (CJ20245040) and Changzhou City Health Commission (ZD202446).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Irwin GM. Urinary Incontinence. Primary Care. 2019;46(2):233–10. doi:10.1016/j.pop.2019.02.004
2. Sun H, Huang J, Tang H, Wei B. Association between weight-adjusted-waist index and urge urinary incontinence: a cross-sectional study from NHANES 2013 to 2018. Sci Rep. 2024;14(1):478. doi:10.1038/s41598-024-51216-2
3. Li Z, Lu X, Zhang K, et al. U-shaped association between serum 25-hydroxyvitamin D concentrations and urinary leakage among adult females aged 45 years and over in the United States: a cross-sectional study. BMC Women’s Health. 2024;24(1):58. doi:10.1186/s12905-024-02906-6
4. Balducci S, D’Errico V, Haxhi J, et al. Effect of a Behavioral Intervention Strategy on Sustained Change in Physical Activity and Sedentary Behavior in Patients With Type 2 Diabetes: the IDES_2 Randomized Clinical Trial. JAMA. 2019;321(9):880–890. doi:10.1001/jama.2019.0922
5. Silva JC, Soler ZA, DominguesWysocki A. Associated factors to urinary incontinence in women undergoing urodynamic testing. Revista da Escola de Enfermagem da U S P. 2017;51:e03209. doi:10.1590/s1980-220x2016140903209
6. Cao C, Friedenreich CM, Yang L. Association of Daily Sitting Time and Leisure-Time Physical Activity With Survival Among US Cancer Survivors. JAMA Oncol. 2022;8(3):395–403. doi:10.1001/jamaoncol.2021.6590
7. Jerez-Roig J, Booth J, Skelton DA, Giné-Garriga M, Chastin SFM, Hagen S. Is urinary incontinence associated with sedentary behaviour in older women? Analysis of data from the National Health and Nutrition Examination Survey. PLoS One. 2020;15(2):e0227195. doi:10.1371/journal.pone.0227195
8. Cristi-Montero C, Rodríguez FR. The paradox of being physically active but sedentary or sedentary but physically active. Revista medica de Chile. 2014;142(1):72–78. doi:10.4067/S0034-98872014000100011
9. Yates T, Khunti K, Wilmot EG, et al. Self-reported sitting time and markers of inflammation, insulin resistance, and adiposity. Am J Preventive Med. 2012;42(1):1–7. doi:10.1016/j.amepre.2011.09.022
10. de Rezende LF, Rey-López JP, Matsudo VK, Do carmo luiz O. Sedentary behavior and health outcomes among older adults: a systematic review. BMC Public Health. 2014;14:333. doi:10.1186/1471-2458-14-333
11. León-Latre M, Moreno-Franco B, Andrés-Esteban EM, et al. Sedentary lifestyle and its relation to cardiovascular risk factors, insulin resistance and inflammatory profile. Revista Espanola Cardiologia. 2014;67(6):449–455. doi:10.1016/j.recesp.2013.10.017
12. Yildirim Z, Sanlier N. The Relationship of Certain Diseases and Dietary Inflammatory Index in Older Adults: a Narrative Review. Curr Nutrit Rep. 2024;13(4):768–785. doi:10.1007/s13668-024-00566-4
13. Shivappa N, Steck SE, Hurley TG, Hussey JR, Hébert JR. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014;17(8):1689–1696. doi:10.1017/S1368980013002115
14. Hobbs M, Pearson N, Foster PJ, Biddle SJ. Sedentary behaviour and diet across the lifespan: an updated systematic review. Br J Sports Med. 2015;49(18):1179–1188. doi:10.1136/bjsports-2014-093754
15. Zhang S, Bian H, Qiu S, et al. Associations between the dietary inflammatory index and urinary incontinence among women younger than 65 years. Sci Rep. 2021;11(1):9340. doi:10.1038/s41598-021-88833-0
16. Wei B, Zhao Y, Lin P, et al. The association between overactive bladder and systemic immunity-inflammation index: a cross-sectional study of NHANES 2005 to 2018. Sci Rep. 2024;14(1):12579. doi:10.1038/s41598-024-63448-3
17. Arouca AB, Santaliestra-Pasías AM, Moreno LA, et al. Diet as a moderator in the association of sedentary behaviors with inflammatory biomarkers among adolescents in the HELENA study. Eur J Nutr. 2019;58(5):2051–2065. doi:10.1007/s00394-018-1764-4
18. Li Y, Di X, Liu M, Wei J, Li T, Liao B. Association between daily sitting time and kidney stones based on the National Health and Nutrition Examination Survey (NHANES) 2007–2016: a cross-sectional study. Int J Surg. 2024;110(8):4624–4632. doi:10.1097/JS9.0000000000001560
19. Zeng Y, Piao Y. Association Analysis of Dietary Inflammatory Index and Gestational Diabetes Mellitus: based on National Health and Nutrition Examination Survey Database. Exp Clin Endocrinol Diabetes. 2024;132(8):453–462. doi:10.1055/a-2293-7983
20. Liao J, Hu M, Imm K, et al. Association of daily sitting time and leisure-time physical activity with body fat among U.S. adults. J Sport Health Sci. 2024;13(2):195–203. doi:10.1016/j.jshs.2022.10.001
21. Ryhtä I, Axelin A, Parisod H, Holopainen A, Hamari L. Effectiveness of exercise interventions on urinary incontinence and pelvic organ prolapse in pregnant and postpartum women: umbrella review and clinical guideline development. JBI Evid Implement. 2023;21(4):394–408. doi:10.1097/XEB.0000000000000391
22. Faleiro DJA, Menezes EC, Capeletto E, Fank F, Porto RM, Mazo GZ. Association of Physical Activity With Urinary Incontinence in Older Women: a Systematic Review. J Aging Pys Activity. 2019;27(4):906–913. doi:10.1123/japa.2018-0313
23. Moreno-Vecino B, Arija-Blázquez A, Pedrero-Chamizo R, et al. Associations between obesity, physical fitness, and urinary incontinence in non-institutionalized postmenopausal women: the elderly EXERNET multi-center study. Maturitas. 2015;82(2):208–214. doi:10.1016/j.maturitas.2015.07.008
24. Kim M, Lee S, Kim HS, Kwon MY, Yoo J, Kim MJ. Microbiome alterations in women with pelvic organ prolapse and after anatomical restorative interventions. Sci Rep. 2023;13(1):17547. doi:10.1038/s41598-023-44988-6
25. Gao Q, Wang M, Zhang J, et al. Pelvic floor dysfunction in postpartum women: a cross-sectional study. PLoS One. 2024;19(10):e0308563. doi:10.1371/journal.pone.0308563
26. Hariharan R, Odjidja EN, Scott D, et al. The dietary inflammatory index, obesity, type 2 diabetes, and cardiovascular risk factors and diseases. Obesity Rev. 2022;23(1):e13349. doi:10.1111/obr.13349
27. Lee UJ, Kerkhof MH, van Leijsen SA, Heesakkers JP. Obesity and pelvic organ prolapse. Cur Opin Urol. 2017;27(5):428–434. doi:10.1097/MOU.0000000000000428
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Neutrophil to Lymphocyte Ratio/Serum Albumin Ratio and Chronic Obstructive Pulmonary Disease: Results from NHANES 1999-2018
Li C, Ao T, Huang Y, Ding L, Zhen P, Hu M, Wang J
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3951-3964
Published Date: 5 December 2025