Back to Journals » Journal of Pain Research » Volume 18
Association Between Chronic Neck Pain and Increased Risk of Chronic Respiratory Diseases in Middle-Aged and Elderly Chinese Adults: A Cohort Study Based on CHARLS
Authors Yi M, Zhang Z, Li H, Sai J, Li W, Wang Z
Received 31 August 2025
Accepted for publication 18 December 2025
Published 30 December 2025 Volume 2025:18 Pages 7275—7286
DOI https://doi.org/10.2147/JPR.S564354
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Mingyang Yi,1,2 Zhen Zhang,1,2 Haixia Li,1– 3 Junting Sai,1,2 Weike Li,1– 3 Zhiwan Wang1– 3
1Department of Respiratory Medicine, The First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, Henan, People’s Republic of China; 2The First Clinical Medical College, Henan University of Chinese Medicine, Zhengzhou, Henan, People’s Republic of China; 3Collaborative Innovation Center for Chinese Medicine and Respiratory Diseases Co-Constructed by Henan Province & Ministry of Education of P.R. China, Henan University of Chinese Medicine, Zhengzhou, Henan, People’s Republic of China
Correspondence: Zhiwan Wang, Email [email protected]
Background: Chronic neck pain (CNP) and chronic respiratory diseases (CRD) have been shown to be associated, though such findings remain inconclusive.
Objective: This study aims to investigate the association between CNP and CRD in middle-aged and elderly Chinese populations using nationally representative longitudinal data.
Methods: This study utilized 7-year longitudinal data (2011– 2018) from the China Health and Retirement Longitudinal Study (CHARLS). The study population comprised respondents who reported chronic neck pain (CNP) without comorbid chronic respiratory diseases (CRDs) in the 2011 survey. Pain sites were assessed via self-reported questionnaires, and CRDs were confirmed based on self-reported prior diagnoses. Logistic regression was employed to analyze the association between CNP and CRDs.
Results: A total of 6864 participants were included, with 650 developing CRD during the follow-up. After adjusting for confounding factors such as gender, age, and other chronic diseases, CNP was significantly associated with incident CRD (OR = 2.25, 95% CI: 1.77– 2.86, P < 0.0001). Gender-stratified analyses revealed that the positive association between CNP and CRD risk remained significant in both males (OR = 3.08, 95% CI: 2.11– 4.48, P < 0.0001) and females (OR = 1.87, 95% CI: 1.37– 2.57, P < 0.0001), with a stronger magnitude observed in males.
Conclusion: Among Chinese CNP patients aged ≥ 45 years, the risk of developing CRD is increased by 2.25-fold, with evident gender differences. In clinical and community practice, conducting respiratory health assessment and screening for middle-aged and elderly patients with CNP (chronic neck pain), and initiating rehabilitation training as early as possible, is of vital importance for reducing their risk of developing chronic respiratory diseases.
Keywords: chronic neck pain, chronic respiratory diseases, cohort study, CHARLS
Introduction
China’s Seventh National Population Census indicates that the country’s elderly population aged 65 and above currently stands at approximately 190 million, with projections indicating an increase to 480 million by 2050, accounting for 37.8% of the total population.1 With advancing age, physiological functions in the elderly exhibit a declining trend, manifesting as multisystem dysfunction. The number of older adults with chronic conditions continues to rise, often presenting with multiple chronic comorbidities. The Report on the Development of Pain Medicine in China indicates that China currently has over 300 million chronic pain patients, with an annual growth rate of 10–20 million. Middle-aged and elderly individuals constitute a high-risk group for chronic pain.2 With population aging, this trend is projected to persist. The proportion of chronic pain patients among middle-aged and elderly populations will continue to rise and is highly prone to trigger the onset and progression of other chronic diseases. Chronic respiratory diseases (CRDs) such as chronic obstructive pulmonary disease (COPD), asthma, etc, are classified by the World Health Organization as one of the four major chronic non-communicable diseases and represent common diseases among the elderly population. In China, the prevalence of COPD among individuals aged 40 and above is 13.6%, with an estimated total of nearly 100 million affected individuals.3 Epidemiological data indicate that asthma prevalence among elderly individuals over 65 years ranges from 4% to 15%.4 Multiple studies demonstrate that the incidence of chronic pain is significantly higher in CRD patients compared to the general population. A clinical investigation revealed that the prevalence of chronic pain in patients with COPD was 41%, which was significantly higher than that in healthy controls.5 A cross-sectional multicenter study further demonstrated that 85% of COPD patients reported chronic pain, with predominant involvement of the neck, shoulders, upper back, and chest. This pain distribution pattern differed markedly from healthy controls, where lower back pain was the most common presentation.6 A randomized controlled trial revealed that asthma patients exhibit significantly lower pressure pain thresholds compared to healthy control groups, particularly in areas such as the trapezius muscle.7 These studies suggest a potential association between chronic pain and CRD.
Chronic neck pain (CNP), a prevalent musculoskeletal disorder affecting approximately 30–50% of the global population, demonstrates a stable age-standardized prevalence rate. Females exhibit higher susceptibility than males, with peak prevalence occurring between ages 45–74. Projections indicate that by 2050, global CNP cases will reach 269 million, primarily driven by population aging.8 A large-scale cross-sectional survey study on CNP prevalence among Chinese middle-aged and elderly adults revealed an 18.93% CNP prevalence rate in individuals aged 45 and above in China, with females exhibiting significantly higher prevalence than males.9 CNP patients typically present with localized hyperalgesia, restricted range of motion, and reduced muscle strength. Studies indicate that in CNP patients, accessory respiratory muscles including the sternocleidomastoid muscle, anterior scalene muscles, and trapezius muscle often demonstrate functional decline in strength, endurance, and motor control due to pain, accompanied by varying degrees of reduction in pulmonary function indicators.10,11 A meta-analysis revealed that CNP patients exhibited significant differences in maximal inspiratory and expiratory pressures compared to asymptomatic respondents, suggesting possible functional pulmonary impairment.12 A cross-sectional survey found that 68% of 320 COPD patients experienced neck pain, significantly higher than the healthy control group, with pain intensity scores positively correlating with COPD severity6. These findings indicate that CNP may lead to varying degrees of respiratory dysfunction, potentially inducing CRD development and revealing a potential association between the two conditions. The relationship between CNP and CRD has not yet been clearly established. Since most existing data come from cross-sectional studies that cannot demonstrate temporal associations, we plan to utilize longitudinal data from a nationally representative large-scale prospective cohort study to investigate the correlation between CNP and the risk of developing CRD.
Methods
Study Design
Through a longitudinal cohort study design, we addressed the following questions: Is CNP associated with the incidence of CRD in middle-aged and older adults? Is there an interaction between the two?
Study Population
CHARLS aims to collect social, economic, and health information from nationally representative samples of Chinese adults aged 45 years and older. The study population covers 450 villages across 150 counties in 28 Chinese provinces. Using probability-proportionate-to-size (PPS) sampling technique, the study involves 17,708 respondents. Since 2011, follow-up surveys have been conducted every 2–3 years, with data collection waves in 2011, 2013, 2015, 2018, and 2020.13 All respondents were interviewed using standardized questionnaires by systematically trained interviewers and provided written informed consent (IRB 00001052–11,014). To date, CHARLS has released data from 2011 to 2018. Using 2011 demographic data as baseline, we conducted longitudinal observations through 2018 after excluding respondents diagnosed with CRD at baseline or lacking CRD information during follow-up. Among 17,708 respondents, we excluded those: under 45 years old at baseline (n=404), diagnosed with CRD (n=933), missing CNP data (n=4555), having incomplete CRD information in 2011 and 2018 (n=3068), and lacking covariate information (n=1884). The final analysis included 6864 respondents, comprising 6268 non-CNP respondents and 596 CNP patients. The participant enrollment process is illustrated in Figure 1. The CHARLS study received approval from the Biomedical Ethics Committee of Peking University. This investigation adheres to the STROBE guidelines for reporting observational studies in epidemiology.14
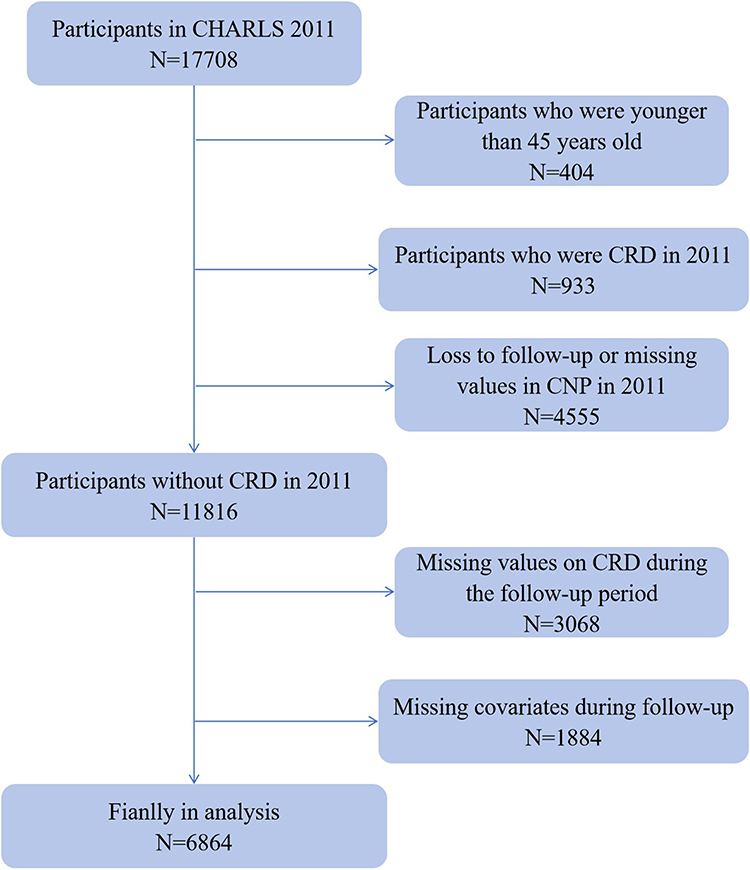 |
Figure 1 Flowchart of the study sample selection process. Abbreviations: CHARLS, China health and retirement longitudinal study; CRD, chronic respiratory disease; CNP, chronic neck pain. |
Assessment of CNP
The determination of CNP was conducted using the health status module questionnaire from the CHARLS, specifically assessed through the questions: “Have you often been troubled by pain?” and “Have you often been bothered by any bodily pain? Please list all affected areas”. The pain severity assessment options included: not at all, a little, somewhat, quite a bit, very much. The pain location assessment options included: head and shoulders, arms, wrists, fingers, chest, abdomen, back, lower back, hips, legs, knees, ankles, toes, neck, and other areas (please specify). Respondents who selected “shoulders” as one of the options were considered part of the CNP population. A series of studies have shown that the CHARLS questionnaire is commonly used to assess chronic pain.15–19
Assessment of CRD
CRD served as the primary variable in this study, encompassing COPD and asthma. This information was derived from CHARLS self-reported questionnaires. COPD assessment was based on the question: “Have you ever been diagnosed by a physician with chronic lung diseases such as chronic bronchitis or emphysema (excluding tumors or cancer)?” Asthma assessment was determined by the question: “Have you ever been diagnosed with asthma by a physician?” Respondents answering “yes” to any of these questions were classified as having CRD.
Covariates
Based on previous studies,20,21 this research controlled for potential confounding factors. Socio-demographic characteristics included age, gender (male / female), education level (illiterate / primary school / middle school / high school or above), place of residence (rural / urban), and marital status (married and cohabiting / other). Health-related factors encompassed smoking status (current / former / never smoked), alcohol consumption (current / former / never drank), body mass index (BMI, continuous variable), and nighttime sleep duration (continuous variable). Chronic conditions included hypertension and diabetes. BMI is calculated as weight (kg) divided by the square of height (m). Participants were categorized into four BMI groups according to WHO criteria: underweight (BMI < 18.5 kg/m2), normal weight (BMI 18.5–24.9 kg/m2), overweight (BMI 25.0–29.9 kg/m2), and obese (BMI ≥ 30.0 kg/m2). Hypertension was defined as self-reported physician-diagnosed hypertension, or a systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg. Diabetes was defined as self-reported physician-diagnosed diabetes, or a fasting blood glucose level ≥ 126 mg/dl, non-fasting blood glucose level ≥ 200 mg/dl, or glycated hemoglobin ≥ 6.5%.
Statistical Analysis
Categorical variables in the dataset were described as frequencies (percentages). Normally distributed continuous variables were presented as mean (standard deviation), while non-normally distributed continuous variables were described as median (interquartile range), with comparisons made using χ2-tests and analysis of variance. We employed logistic regression analysis to examine the prospective association between baseline CNP and CRD, expressed as odds ratios (OR) with 95% confidence intervals (CI). To mitigate the influence of confounding factors, we constructed multivariable-adjusted models. Specifically, the crude model was a single regression model without adjustment for confounders. Model 1 adjusted for age, education level, marital status, residence; Model 2 further adjusted for alcohol consumption status, smoking status, sleep duration, and BMI based on Model 1. Model 3 further adjusted for chronic disease history (including hypertension and hyperglycemia) based on Model 2. Additionally, we conducted subgroup analyses to assess potential interactions among variables. Specifically, we explored potential interactions across the following factors: gender, age, education level, marital status, residence, BMI, sleep duration, smoking status, alcohol consumption status, and chronic disease history (hypertension and diabetes). This study employed R version 4.5.0 for statistical analysis, with statistical significance defined as P <0.05.
Results
Characteristics of the Study Population
The study included 6864 respondents with a mean age of 57.88 years (SD 8.73). Among them, 3277 were male (47.74%), and 3587 were female (52.26%). At baseline, 9.51% of respondents reported CNP. Compared to those without CNP, respondents with CNP showed significant differences: they had shorter sleep duration, higher proportion of females, lower proportion of married individuals, and higher proportion of rural residents. Significant differences were also observed in education levels and risk behaviors between the two groups: Compared with respondents without CNP, CNP patients exhibited lower education levels and lower rates of smoking and alcohol consumption. All P <0.05, indicating statistical significance. Detailed population characteristics are presented in Table 1.
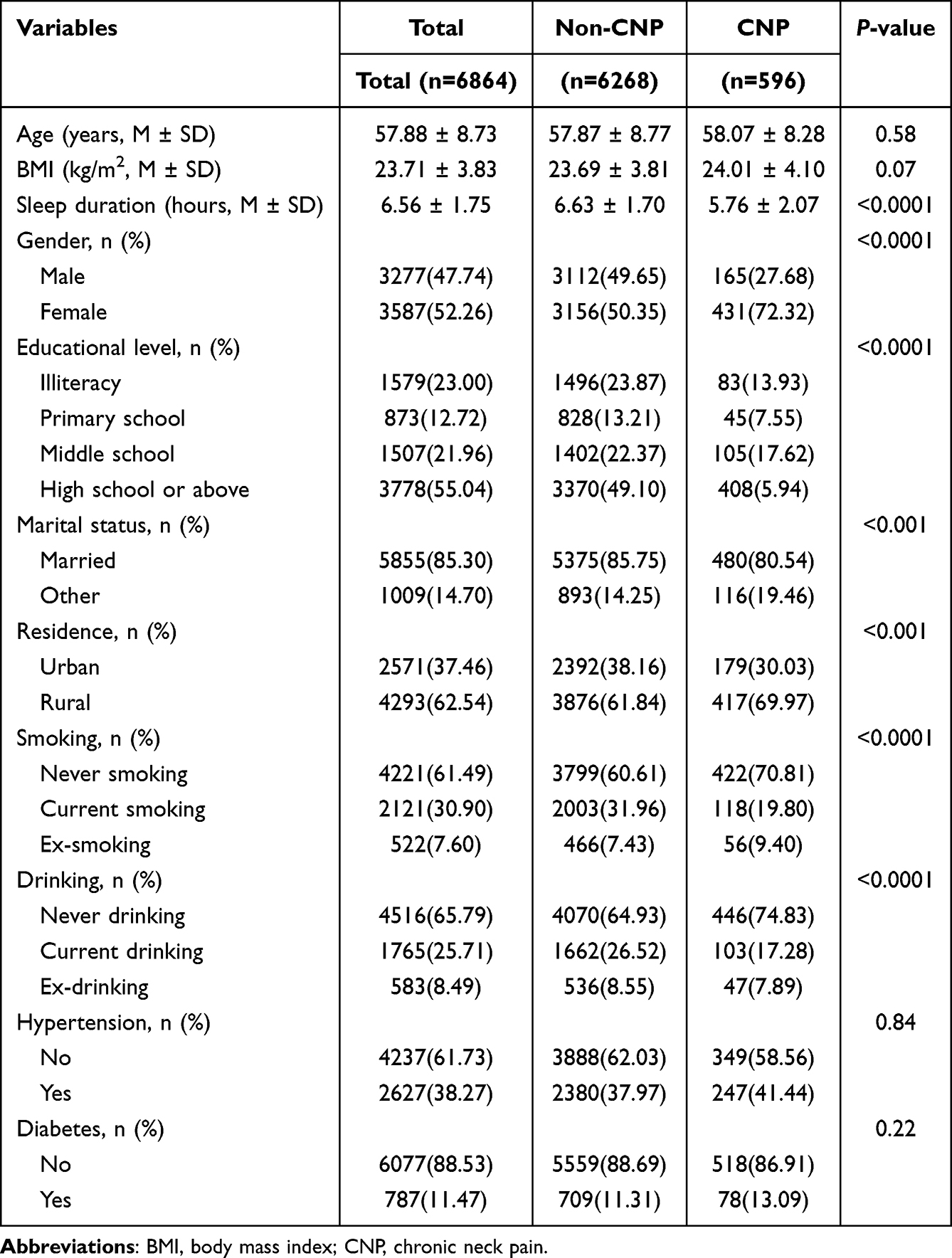 |
Table 1 Baseline Characteristics of Study Population in 2011 |
Longitudinal Association Between CNP and CRD
Over the 7-year follow-up period, a total of 650 participants developed CRD. As presented in Table 2, in the adjusted model, CNP remained significantly associated with the incidence of CRD, with an OR of 2.25 (95% CI: 1.77–2.86, P < 0.0001). Additionally, stratified analyses demonstrated that in male participants, CNP was significantly correlated with the occurrence of CRD (OR = 3.08, 95% CI: 2.11–4.48, P < 0.0001); the association between the two conditions was also significant in female participants (OR = 1.87, 95% CI: 1.37–2.57, P < 0.0001). These findings indicate that after adjusting for confounding factors such as age, educational level, marital status, residence, sleep duration, BMI, alcohol consumption, and smoking status, CNP remains significantly associated with the incidence of CRD. Gender-stratified analyses revealed that this association is relatively stronger in the male population.
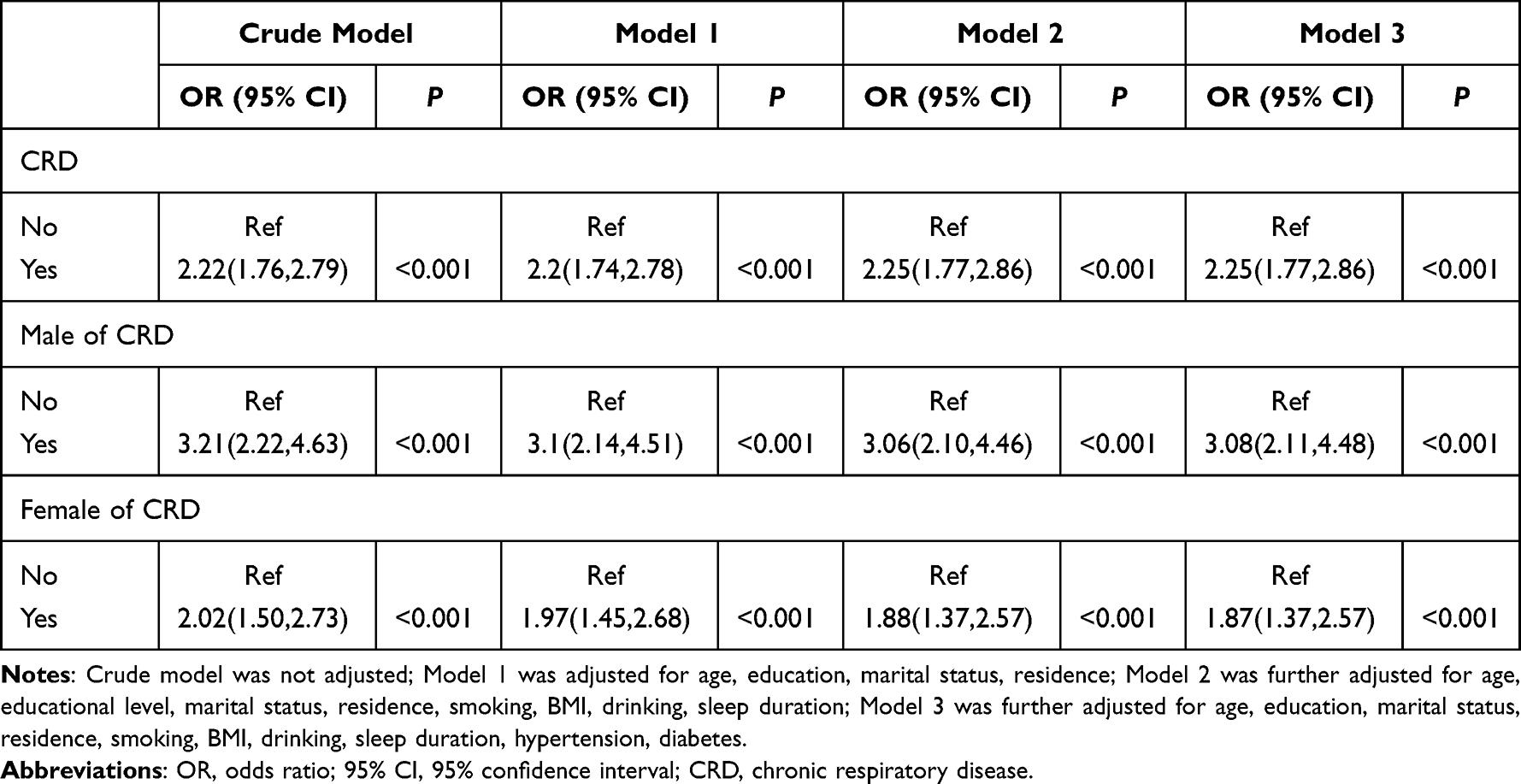 |
Table 2 Longitudinal Association of CNP and CRD, 2011~2018 |
Subgroup Analysis
To further validate the robustness of the association between CNP and CRD risk, participants were stratified into various subgroups. After adjusting for covariates, forest plots demonstrated that both the direction and magnitude of the association between CNP and CRD risk remained stable, with no reversal or significant deviation of associations observed due to subgroup stratification. Moreover, interaction tests revealed no statistically significant differences in association strength across subgroups (all interaction P > 0.05), indicating that the effect of CNP on CRD risk did not vary significantly based on subgroup characteristics. These findings support the robustness of the observed association (Figure 2).
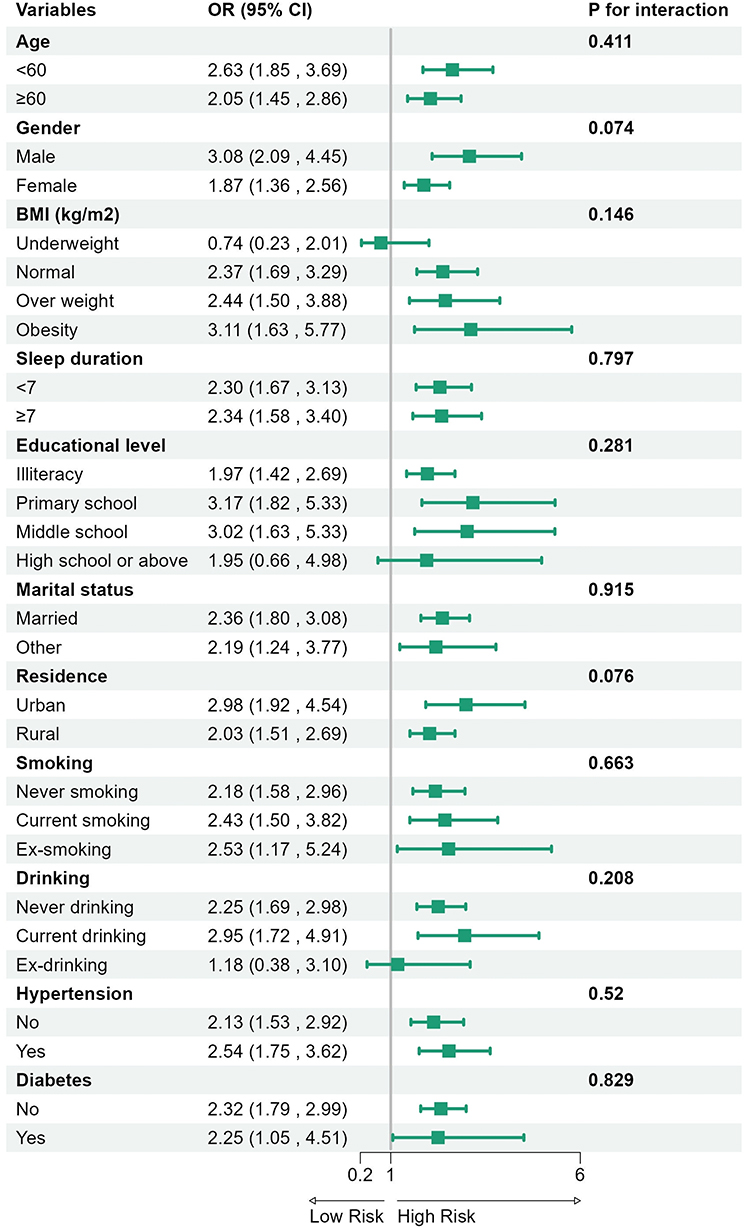 |
Figure 2 Forest plot of CNP and CRD. Abbreviations: OR, odds ratio; 95% CI, 95% confidence interval; BMI, body mass index. |
Discussion
This study is the first large-scale cohort investigation to explore the longitudinal relationship between CNP and CRD among Chinese middle-aged and elderly adults, revealing a significant association. During the 7-year follow-up period, we identified 650 newly developed CRD cases. After adjusting for confounding factors including gender, age, and education level, a significant association remained between CNP and CRD occurrence (OR=2.25, 95% CI: 1.77–2.86). Subgroup analysis results remained stable These findings hold significant implications for clinical practice. When treating CNP, incorporating exercise therapy, rehabilitation training, or other interventions to improve respiratory function may mitigate the negative impact of CNP on CRD development.
Utilizing CHARLS longitudinal data, this study demonstrates a positive association between CNP and elevated CRD risk among middle-aged and elderly adults, aligning with multiple existing research findings. Studies have demonstrated that transcutaneous carbon dioxide partial pressure (PtCO2) is significantly decreased in patients with CNP, with some individuals developing hypocapnia, which severely compromises respiratory function.22 A UK pilot study revealed that CNP patients exhibited abnormal pulmonary function indices due to weakened respiratory muscle strength, with marked reductions in maximal voluntary ventilation (MVV), maximal inspiratory pressure (Pimax), and maximal expiratory pressure (Pemax).23 A meta-analysis incorporating 11 relevant studies with 929 respondents demonstrated significantly reduced respiratory muscle strength and pulmonary function in CNP patients compared to asymptomatic individuals, with some patients exhibiting respiratory dysfunction.24 An observational study from South Korea demonstrated that compared to non-CNP patients, 48 CNP patients exhibited reduced chest mobility and weakened respiratory strength.25 These studies indicate that CNP leads to a decline in respiratory muscle strength, subsequently impairing pulmonary function and causing varying degrees of lung damage. However, these studies did not directly establish the longitudinal relationship between CNP and CRD occurrence. Therefore, we conducted cohort-based research to explore the longitudinal association between CNP and CRD.
Our study confirms that CNP is a significant factor increasing the risk of CRD in middle-aged and elderly adults. One underlying mechanism involves alterations in the musculoskeletal status of the neck. CNP leads to reduced endurance and limited mobility of accessory respiratory muscles in the neck region, including the scalene muscles, sternocleidomastoid muscle, and trapezius muscle. Sports rehabilitation research indicates that patients with neck pain exhibit energy metabolism disorders and lactate accumulation in the sternocleidomastoid muscle, anterior scalene muscles, and upper trapezius muscle.26 Prolonged hyperactivation and fatigue cause changes in their tension and force curves, while restricted cervicothoracic joint mobility contributes to incorrect breathing patterns. These factors collectively impair respiratory function during resting states. Numerous studies indicate that CNP patients often exhibit insufficient activation of local stabilizers.26,27 When neck muscles become fatigued due to pain, their stabilizing function diminishes, leading to cervicothoracic imbalance. This subsequently affects thoracic cage movement, with inadequate thoracic expansion being a significant contributor to respiratory dysfunction.25 Furthermore, according to the muscle tension-length curve, insufficient thoracic expansion causes respiratory muscles to work inefficiently. This promotes long-term shallow breathing patterns that result in inadequate pulmonary gas exchange, potentially increasing the incidence of chronic bronchitis or pulmonary infections.28
Pain is the primary clinical manifestation in CNP patients, exerting a significant adverse impact on the development of CRD. CNP patients often exhibit localized pain hypersensitivity. Through spinal reflex arcs, pain activates nociceptors, triggering transmission of pain signals to the central nervous system. This subsequently inhibits the contractile function of accessory respiratory muscles in the neck and upper thoracic region via γ-motor neurons.29 Concurrently, pain can induce spasms in the scalene and sternocleidomastoid muscles, reducing thoracic expansion during inspiration and decreasing tidal volume. Human respiratory function is coordinately regulated by the medullary respiratory center, phrenic nerve, intercostal nerves, and sensory feedback. Nociceptive signals from neck pain are transmitted to the spinal dorsal horn via the posterior branches of cervical nerves, where they form synaptic connections with respiratory-related neurons. This process releases inhibitory neurotransmitters that suppress the excitability of the respiratory center, ultimately leading to reduced respiratory drive.30 Clinical studies revealed a positive correlation between cervical spondylosis severity and diaphragmatic dysfunction in 334 patients, with patients exhibiting ipsilateral diaphragmatic paralysis demonstrating more severe cervical degeneration on the affected side.31 Diaphragmatic weakness can lead to insufficient lung expansion during inspiration, causing structural remodeling of lung tissue due to chronic under-stretching: reduced elastic fibers in alveolar walls, collagen fiber proliferation, and decreased pulmonary elastic recoil. These pathological alterations resemble early-stage COPD features.32 The neck region contains abundant vagus nerve branches, such as the recurrent laryngeal nerve. Pain stimuli are transmitted via the vagus nerve to the nucleus tractus solitarius in the medulla oblongata, activating cardiopulmonary reflexes that may cause respiratory rhythm disturbances and even trigger bronchospasm, thereby increasing asthma risk.33
CNP is often accompanied by localized chronic inflammation. Inflammatory mediators may affect respiratory function through systemic circulation. Firstly, inflammatory factors directly damage respiratory muscles. Local inflammation releases TNF-α, IL-6, prostaglandin E2, and other mediators into the bloodstream. These substances act on respiratory muscles by inhibiting Ca2+ release from the sarcoplasmic reticulum and reducing intracellular Ca2+ concentrations required for muscle contraction.34 Secondly, pro-inflammatory factors such as TNF-α and IL-6 reach lung tissue via the bloodstream, stimulating airway epithelial cells to release TGF-β. This promotes airway smooth muscle cell proliferation and collagen deposition, leading to airway wall thickening and increased airway resistance.35 Studies have found that serum IL-6 levels in CNP patients are 2–3 times higher than in healthy individuals, showing a negative correlation with forced expiratory volume in one second (FEV1). This suggests that inflammation factor release induced by pain may contribute to reduced pulmonary function.11 Concurrently, when neck pain signals are transmitted to the central nervous system via cervical nerves, they activate the neurogenic inflammatory pathway in the spinal dorsal horn, releasing substance P and calcitonin gene-related peptide. These substances reach lung tissue through blood circulation or axon reflexes, stimulating airway nerve endings and triggering airway smooth muscle contraction, increased vascular permeability, and mucus secretion. Consequently, patients become prone to recurrent symptoms including cough, sputum production, wheezing, and chest tightness.36
Depression and anxiety constitute significant risk factors for the development of CRD.37 Concurrently, CNP patients often experience negative emotions such as anxiety and depression due to impairment in daily activities, sleep quality deterioration, and social function deficits. Such anxiety and depression triggered by CNP may conversely elevate patients’ risk of developing CRD. A prospective cohort study demonstrated that individuals with anxiety and depression face a significantly increased risk of developing CRD compared to healthy subjects.38 Relevant studies indicate that anxiety and depression constitute risk factors for COPD onset and suboptimal asthma control.39,40 The mechanisms linking anxiety and depression symptoms to CRD primarily involve the following pathways: First, as psychological stress reactions, anxiety and depression persistently activate the body’s neuro-endocrine-immune axis. Consequently, adrenal cortisol secretion remains chronically dysregulated, suppressing immune cell function in respiratory mucosa and impairing mucosal pathogen clearance. Simultaneously, elevated release of pro-inflammatory factors directly damages the airway epithelial barrier, promotes excessive mucus secretion and airway remodeling, ultimately leading to CRD development.41,42 Secondly, anxiety and depression indirectly contribute to respiratory system damage through behavioral pattern alterations. Patients with anxiety and depression commonly exhibit unhealthy lifestyles such as smoking, alcohol consumption, and physical inactivity. Smoking directly damages airway epithelial cells and impairs ciliary motility, while alcohol consumption depresses the respiratory center, thereby worsening respiratory depression and hypoxia. These adverse behaviors collectively cause varying degrees of airway damage and immune function decline, consequently increasing the risk of CRD43. This indicates that anxiety and depression in CNP patients significantly increase the risk of CRD among middle-aged and elderly adults.
Based on the above findings, middle-aged and elderly CNP patients exhibit elevated CRD risk. This discovery holds significant implications for early prevention, diagnosis, intervention, and prognostic management of CRD. For CNP patients, attention should be given to respiratory symptoms such as cough, sputum production, chest tightness, and shortness of breath. Patients with pronounced symptoms should undergo pulmonary function tests and chest computed tomography (CT), to assess pulmonary status, enabling early disease diagnosis. Studies indicate that respiratory training can alleviate pain severity and improve the range of motion in CNP patients.44 Concurrently, therapeutic approaches such as cervical traction, manual release, and transcutaneous electrical stimulation not only relieve neck pain but also strengthen accessory respiratory muscles and diaphragm function while correcting poor breathing postures, thereby effectively enhancing patients’ respiratory function.45 Clinically, some CRD patients present with neck pain and anxiety-depression despite no history of smoking or air pollution exposure. When identifying relevant etiologies, clinicians should consider the adverse impact of neck pain on CRD progression. In primary health care management, respiratory health education can be implemented for CNP patients. Middle-aged and elderly patients are recommended to practice exercises such as Tai Chi and Baduanjin, which simultaneously alleviate neck pain and regulate respiratory function.
This study, based on a nationally representative CHARLS longitudinal cohort, offers several strengths: First, the large sample size and comprehensive epidemiological survey data ensure relatively high generalizability of the findings. Second, multiple confounding variables were adjusted during the research process to ensure result reliability. Concurrently, this study is the first to investigate the longitudinal relationship between CNP and CRD through a prospective cohort design. It not only provides substantive evidence for selecting treatment approaches for CNP patients but also holds significant implications for early prevention and intervention of CRD. Nevertheless, this study still has certain limitations. First, the diagnosis of CRD was not confirmed through objective examinations such as pulmonary function tests or chest CT, but relied on patient self-reports, which may introduce recall bias. Second, this study only examined the association between CNP at baseline and the subsequent occurrence of CRD during follow-up. There was a lack of quantification regarding the duration and severity of CNP, which limits the ability to further clarify whether the intensity or duration of CNP influences the incidence or severity of CRD. Third, although multiple confounding factors were adjusted for in the study, some unmeasured or substantially missing factors—such as economic status, prior health conditions, and medication history—remain unaccounted for. Fourth, as this study exclusively sampled middle-aged and elderly populations in China, caution should be exercised when extrapolating the findings to populations in other regions. Based on these findings, future studies should expand sample sizes and employ diverse methodologies—including cross-sectional studies and prospective cohort studies—to validate this association; concurrently, laboratory investigations should elucidate the underlying biological mechanisms.
Conclusion
This study is the first to untangle the risk of CRD among middle-aged and elderly Chinese patients with CNP. These findings underscore the importance of respiratory health assessment in this population, which holds significant implications for early disease prevention and diagnosis. Additionally, this study provides a basis for lifestyle modifications or other interventions aimed at reducing the incidence of CRD.
Data Sharing Statement
Data in the study are from the CHARLS database. Researchers can obtain these data by registering and logging into the official CHARLS website to submit an application. (http://charls.pku.edu.cn/pages/data/111/en.html).
Ethics Approval and Consent to Participate
This study is a secondary analysis based on anonymized information data from the publicly available CHARLS database, obtained legally. According to Article 32, Items 1 and 2, of the “Ethical Review Measures for Life Science and Medical Research Involving Human Subjects in China” (February 18, 2023), this research is exempt from ethical approval under the national legislative guidelines. And the ethical approval of CHARLS is provided by the Institutional Review Board (IRB) of Peking University (IRB00001052-11015), which is updated annually. All participants provided informed consent before joining the survey. We confirm that all methods were conducted in accordance with relevant guidelines and regulations.
Acknowledgments
We are very grateful to the China Health and Retirement Longitudinal Study project team for the access to the datasets and the guidelines for using data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by Noncommunicable Chronic Diseases-National Science and Technology Major Project (2023ZD0506700, 2023ZD0506701), and National Natural Science Foundation of China’s General Program (81973791).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Du P, Li L. Long-term trends projection of China’s population aging in the new era. J Renmin Univ China. 2021;35(1):96–109. doi:10.3969/j.issn.1000-5420.2021.01.010
2. Fan BF. Report on the development of pain medicine in China. Beijing: Tsinghua University Press, 2020.
3. Wang C, Xu J, Yang L, et al; China Pulmonary Health Study Group. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9.
4. Gibson PG, McDonald VM, Marks GB. Asthma in older adults. Lancet. 2010;376(9743):803–813. doi:10.1016/S0140-6736(10)61087-2
5. Lee AL, Goldstein RS, Brooks D. Chronic pain in people with chronic obstructive pulmonary disease: prevalence, clinical and psychological implications. Chronic Obstr Pulm Dis. 2017;4(3):194–203. doi:10.15326/jcopdf.4.3.2016.0172
6. Tanaka T, Okita M, Jenkins S, Kozu R. Clinical and psychological impact of chronic pain in people with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2022;17:893–903. doi:10.2147/COPD.S359223
7. Rodríguez-Torres J, López-López L, Cabrera-Martos I, et al. Symptom severity is associated with signs of central sensitization in patients with asthma. Clin Respir J. 2021;15(11):1219–1226. doi:10.1111/crj.13429
8. GBD 2021 Neck Pain Collaborators. Global, regional, and national burden of neck pain, 1990-2020, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Rheumatol. 2024;6(3):e142–e155. doi:10.1016/S2665-9913(23)00321-1.
9. Bai YW, Wang YC, Jiang X, et al. Prevalence and risk factors of neck pain among middle-aged and older adults in China: a cross-sectional study from the CHARLS cohort. Eur J Phys Rehabil Med. 2025;61(3):509–519. doi:10.23736/S1973-9087.25.08492-8
10. Dimitriadis Z, Kapreli E, Strimpakos N, Oldham J. Respiratory weakness in patients with chronic neck pain. Man Ther. 2013;18(3):248–253. doi:10.1016/j.math.2012.10.014
11. Dağ F, Taş S, Çimen ÖB. Pulmonary functions in patients with chronic neck pain: a case-control study. J Manipulative Physiol Ther. 2022;45(4):290–297. doi:10.1016/j.jmpt.2022.07.002
12. Kahlaee AH, Ghamkhar L, Arab AM. The association between neck pain and pulmonary function: a systematic review. Am J Phys Med Rehabil. 2017;96(3):203–210. doi:10.1097/PHM.0000000000000608
13. Zhao Y, Hu Y, Smith JP, et al. Cohort profile: the China health and retirement longitudinal study (CHARLS). Int J Epidemiol. 2014;43(1):61–68. doi:10.1093/ije/dys203
14. Von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
15. Wang G, Huang S, Sun N, et al. Depression and its influencing factors among older adults with chronic pain in China: an empirical analysis based on CHARLS data. Front Public Health. 2025;13:1547860. doi:10.3389/fpubh.2025.1547860
16. Ai Z, Tang C, Peng P, et al. Prevalence and influencing factors of chronic pain in middle-aged and older adults in China: results of a nationally representative survey. Front Public Health. 2023;11:1110216. doi:10.3389/fpubh.2023.1110216
17. Teng TQ, Liu J, Wang MM, Yu HC. Synergistic effects of chronic pain and diabetes on cardiovascular disease risk: findings from a nationwide cohort study. BMC Public Health. 2025;25(1):2085. doi:10.1186/s12889-025-23376-x
18. Luo X, Li H, Hou X, et al. The gender difference in the comorbidity of chronic pain and depression, a longitudinal study. J Affect Disord. 2026;392:120109. doi:10.1016/j.jad.2025.120109
19. Miao E, Wu Q, Cai Y. Mediating effect of depressive symptoms on the relationship of chronic pain and cardiovascular diseases among Chinese population: evidence from the CHARLS. J Psychosom Res. 2024;180:111639. doi:10.1016/j.jpsychores.2024.111639
20. Li C, Luo C, Zhu J, et A. The impact of ADL disability in middle-aged and older adults on the incidence of Hip fractures and the mediating role of depression: a longitudinal evidence from CHARLS. Front Med Lausanne. 2025;12:1604729. doi:10.3389/fmed.2025.1604729
21. Guo D, Huang K, Guan X, et A. Association between chronic respiratory diseases and frailty in Chinese elderly: a population-based longitudinal study. BMJ Open Respir Res. 2025;12(1):e002171. doi:10.1136/bmjresp-2023-002171
22. Dimitriadis Z, Kapreli E, Strimpakos N, Oldham J. Pulmonary function of patients with chronic neck pain: a spirometry study. Respir Care. 2014;59(4):543–549. doi:10.4187/respcare.01828
23. Kapreli E, Vourazanis E, Billis E, et A. Respiratory dysfunction in chronic neck pain patients. A pilot study. Cephalalgia. 2009;29(7):701–710. doi:10.1111/j.1468-2982.2008.01787.x
24. López-de-Uralde-Villanueva I, Del Corral T, Salvador-Sánchez R, et al. Respiratory dysfunction in patients with chronic neck pain: systematic review and meta-analysis. Disabil Rehabil. 2023;45(15):2422–2433. doi:10.1080/09638288.2022.2096126
25. Cheon JH, Lim NN, Lee GS, et A. Differences of spinal curvature, thoracic mobility, and respiratory strength between chronic neck pain patients and people without cervical pain. Ann Rehabil Med. 2020;44(1):58–68. doi:10.5535/arm.2020.44.1.58
26. Wirth B, Amstalden M, Perk M, et al. Respiratory dysfunction in patients with chronic neck pain - influence of thoracic spine and chest mobility. Man Ther. 2014;19(5):440–444. doi:10.1016/j.math.2014.04.011
27. Chand VH. Effect of diaphragmatic breathing, respiratory muscle stretch gymnastics and conventional physiotherapy on chest expansion, pulmonary function and pain in patients with mechanical neck pain: a single group pretest-posttest quasi-experimental pilot study. J Bodyw Mov Ther. 2023;36:148–152. doi:10.1016/j.jbmt.2023.07.004
28. López-de-Uralde-Villanueva I, Sollano-Vallez E, Del Corral T. Reduction of cervical and respiratory muscle strength in patients with chronic nonspecific neck pain and having moderate to severe disability. Disabil Rehabil. 2018;40(21):2495–2504. doi:10.1080/09638288.2017.1337239
29. Bordoni B, Jozsa F, Varacallo MA. Anatomy, Head and Neck, Scalenus Muscle. In: StatPearls. Treasure Island (FL): StatPearls Publishing, 2025
30. Kaplan CM, Kelleher E, Irani A, et al. Deciphering nociplastic pain: clinical features, risk factors and potential mechanisms. Nat Rev Neurol. 2024;20(6):347–363. doi:10.1038/s41582-024-00966-8
31. O’Beirne SL, Chazen JL, Cornman-Homonoff J, et al. Association between diaphragmatic paralysis and ipsilateral cervical spondylosis on MRI. Lung. 2019;197(6):727–733. doi:10.1007/s00408-019-00271-y
32. Rocha T, Souza H, Brandão DC, et A. The Manual Diaphragm Release Technique improves diaphragmatic mobility, inspiratory capacity and exercise capacity in people with chronic obstructive pulmonary disease: a randomised trial. J Physiother. 2015;61(4):182–189. doi:10.1016/j.jphys.2015.08.009
33. Canning BJ. Reflex regulation of airway smooth muscle tone. J Appl Physiol. 2006;101(3):971–985. doi:10.1152/japplphysiol.00313.2006
34. Dalle S, Koppo K. Is inflammatory signaling involved in disease-related muscle wasting? Evidence from osteoarthritis, chronic obstructive pulmonary disease and type II diabetes. Exp Gerontol. 2020;137:110964. doi:10.1016/j.exger.2020.110964
35. Perez-Garcia J, Cardenas A, Lorenzo-Diaz F, Pino-Yanes M. Precision medicine for asthma treatment: unlocking the potential of the epigenome and microbiome. J Allergy Clin Immunol. 2025;155(2):298–315. doi:10.1016/j.jaci.2024.06.010
36. Ye Q, Bankova LG. Brush cells fine-tune neurogenic inflammation in the airways. J Clin Invest. 2022;132(13):e161439. doi:10.1172/JCI161439
37. Yohannes AM. Anxiety and post-traumatic stress disorders in patients with chronic respiratory diseases. Curr Opin Support Palliat Care. 2023;17(4):290–295. doi:10.1097/SPC.0000000000000670
38. Xie Z, Wu Z, Sun W, et A. Association between depression and multimorbidity in Chinese middle-aged and older adults: a prospective cohort study. J Affect Disord. 2025;385:119445. doi:10.1016/j.jad.2025.119445
39. Rahi MS, Thilagar B, Balaji S, et al. The impact of anxiety and depression in chronic obstructive pulmonary disease. Adv Respir Med. 2023;91(2):123–134. doi:10.3390/arm91020011
40. Ciprandi G, Schiavetti I, Rindone E, Ricciardolo FL. The impact of anxiety and depression on outpatients with asthma. Ann Allergy Asthma Immunol. 2015;115(5):408–414. doi:10.1016/j.anai.2015.08.007
41. Pumar MI, Gray CR, Walsh JR, et al. Anxiety and depression-Important psychological comorbidities of COPD. J Thorac Dis. 2014;6(11):1615–1631. doi:10.3978/j.issn.2072-1439.2014.09.28
42. Lu Y, Feng L, Feng L, et al. Systemic inflammation, depression and obstructive pulmonary function: a population-based study. Respir Res. 2013;14(1):53. doi:10.1186/1465-9921-14-53
43. Ng R, Sutradhar R, Yao Z, et al. Smoking, drinking, diet and physical activity-modifiable lifestyle risk factors and their associations with age to first chronic disease. Int J Epidemiol. 2020;49(1):113–130. doi:10.1093/ije/dyz078
44. Yeampattanaporn O, Mekhora K, Jalayondeja W, Wongsathikun J. Immediate effects of breathing re-education on respiratory function and range of motion in chronic neck pain. J Med Assoc Thai. 2014;97(Suppl 7):S55–9.
45. Dareh-Deh HR, Hadadnezhad M, Letafatkar A, Peolsson A. Therapeutic routine with respiratory exercises improves posture, muscle activity, and respiratory pattern of patients with neck pain: a randomized controlled trial. Sci Rep. 2022;12(1):4149. doi:10.1038/s41598-022-08128-w
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.