Back to Journals » Advances in Medical Education and Practice » Volume 12
Assessment of the Knowledge and Attitude Towards Dementia Among Undergraduate University Students in Uganda
Authors Musoke P ![]() , Olum R
, Olum R ![]() , Kembabazi S
, Kembabazi S ![]() , Nantaayi B
, Nantaayi B ![]() , Bongomin F
, Bongomin F ![]() , Kaddumukasa M
, Kaddumukasa M ![]()
Received 5 March 2021
Accepted for publication 25 May 2021
Published 14 June 2021 Volume 2021:12 Pages 635—646
DOI https://doi.org/10.2147/AMEP.S301445
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Phillip Musoke,1 Ronald Olum,1 Shallon Kembabazi,1 Brandy Nantaayi,1 Felix Bongomin,2 Mark Kaddumukasa3
1School of Medicine, College of Health Sciences, Makerere University, Kampala, Uganda; 2Department of Medical Microbiology and Immunology, Faculty of Medicine, Gulu University, Gulu, Uganda; 3Department of Medicine, School of Medicine, College of Health Sciences, Makerere University, Kampala, Uganda
Correspondence: Phillip Musoke
School of Medicine, College of Health Sciences, Makerere University, Kampala, Uganda
Email [email protected]
Background: Dementia remains a public health concern and a leading cause of disability and dependency among older people worldwide. However, the knowledge and attitudes towards dementia among university students remain unknown. This study assessed the knowledge and attitude towards dementia among university students in Uganda.
Methods: An online descriptive, cross-sectional study was undertaken from August to November 2020, among undergraduate students from 11 Ugandan universities. A validated study questionnaire was used to collect data on socio-demographic characteristics, knowledge, and attitudes of dementia. A score < 60% was considered poor knowledge while ≥ 80% good knowledge and more than 80% reflected positive attitudes.
Results: Overall, 1005 participants with a median age of 23 (interquartile range: 18 to 35) years participated in the study. The majority of the students were male (56.5%, n=568) and nearly half were pursuing human sciences/medicine-related programs. The mean knowledge score was 65.5% (SD± 18.5). Thirty-two percent of the study participants had poor knowledge and only 26.8% (n=269) had good knowledge of dementia. More than half of the study participants believed that dementia is a normal part of aging and that memory loss happens to all people as they age. Attitudes towards patients with dementia were positive with a mean score of 81.9% (SD± 19.6) and 65.2% of the study participants had positive dementia attitudes. Those aged more than 24 years were significantly associated with positive attitudes (adjusted odds ratio (AOR): 1.5, 95% CI: 1.1– 2.0, p=0.019). There was a weak correlation between knowledge and attitude scores (ρ=0.341, p< 0.001).
Conclusion: Whereas the majority of university students have positive attitudes towards patients with dementia, a significant number still have poor knowledge of the same. Continuous health education is suggested to improve knowledge of dementia in this population. Further studies to understand the perception in the general population are recommended.
Keywords: dementia, Alzheimer’s disease, knowledge, attitude, Uganda
Introduction
Dementia is a public health concern and a leading cause of disability and dependency among people of old age worldwide.1 Globally, about 10 million people develop dementia each year, and nearly 60% of these estimates reside in low- and middle-income countries (LMICs).2 About 2.13 million people are estimated to be living with dementia in Sub-Saharan Africa (SSA), with the majority contributed by Alzheimer’s disease (AD). Dementia in SSA is projected to surpass 3.48 million by 2030.3 The elderly population in Uganda is projected to reach 5,420,000 by 2050.4 Therefore, the increasing elderly population coupled with the high prevalence of dementia at 20% justifies studies to understand the attitudes and knowledge within the general population.5
Dementia can be overwhelming, not only for the patients but also their caregivers and immediate families. Often, there is a lack of awareness and limited understanding of dementia, resulting in stigmatization, discrimination, social exclusion, barriers to diagnosis and care with the associated physical, psychological, social, and economic burden on caregivers, family, and society.1,6
Studies have found poor knowledge and understanding of dementia amongst the general population as well as the caregivers of individuals with dementia7,8 especially within SSA.9 The poor knowledge and attitudes towards dementia may be leading to delayed health-seeking behaviors and lifestyle changes that might impact the condition progression.
Presently, no study in Uganda has assessed the knowledge and attitude of the general population towards dementia. University students form part of the general population and play an important role in information dissemination and provision of care to dementia patients within communities. Therefore, this study set out to determine the knowledge and attitudes of university students towards dementia in Uganda.
Methods and Materials
Study Design and Area
An online descriptive, cross-sectional study, was undertaken from August to November 2020. Undergraduate students from 11 universities, both private and public universities were included;
Public universities: Makerere University, Mbarara University of Science and Technology, Kyambogo University, Gulu University, and Busitema University.
Private universities: Kampala International University (KIU), Uganda Christian University (UCU), Islamic University in Uganda (IUIU), St. Augustine (King Caesar) International University, and Ndejje University. There are currently, 32 universities in Uganda all accounting for a student population of about 110,000, turning out over 30,000 graduates annually. Makerere University alone accounts for over 30% of this total and the majority of these come from all over the country. (https://www.ubos.org/wp-content/uploads/publications/11-2020).
Selection Criteria
Students aged 18 years and above, enrolled in one of the above universities were included in the study after informed electronic consent.
Sample Size and Sampling
The sample size was calculated using Epi Info StatCalc for population surveys. With an estimated population size of university students in Uganda at 60,000, expected average knowledge at 53.4% according to the study in South Africa,10 3% acceptable margin of error and design effect of 1, the estimated sample size at 95% confidence interval was therefore, 1044 students.
Data Collection Procedure
Students identified through the guild presidents of the different universities, student federations, student associations, and class WhatsApp groups received a link to a detailed study Google form questionnaire containing 40 questions and a consent form. This was shared via social media platforms (WhatsApp Messenger and Facebook Inc. California, USA).
Questionnaire Development
The study questionnaire was adapted from a pre-existing validated questionnaire which was used in South Africa, Khayelitsha for isiXhosa-speaking people.10 The questionnaire consisted of closed and open-ended questions and was divided into 4 sections: socio-demographics-age, sex, region of origin, religion, tribe, marital status, university-affiliated to, program and year of study, if they have heard or know someone who has dementia, knowledge of dementia, a self-rated knowledge scale, and attitudes towards dementia.
Assessments
Knowledge of Dementia
Sixteen (16) items obtained from Khonje et al, were used to assess dementia knowledge.10 The total knowledge score was calculated by adding the correct responses to produce a score that ranges from 0 to 16; (1 mark was awarded for every correct response and zero marks were given for incorrect response). The total knowledge score for each participant out of 16 was calculated, which was then converted to a percentage. The Cronbach alpha score for the 16 items was 0.70, implying acceptable internal reliability of the scale. Furthermore, respondents were asked to self-rate their level of knowledge of dementia based on a scale of 0 to 10 (score of 0 if “I know nothing at all” to 10, if “I am very knowledgeable”).
Attitude Toward Patients with Dementia
Eight (8) questions acquired from Khonje et al, were used to assess dementia attitude.10 The total attitude score was calculated by adding the positive responses to produce a score that ranges from 0 to 8 (1 mark was awarded for every positive response and zero marks were given for negative response). The attitude score was then converted to percentages. For the attitude scale, the Cronbach alpha score was 0.71 indicating acceptable internal reliability.
Data Analysis and Management
Fully completed questionnaires were extracted from the google form and exported to a Microsoft Excel 2016 for cleaning and coding. The cleaned data was exported to STATA 16 (StataCorp LLC, College Station, Texas, USA) for analysis. Numerical data were then summarized as means and standard deviations or median and range as appropriate for parametric or non-parametric conditions as assessed using the Shapiro–Wilk test. Categorical data were summarized as frequencies and proportions. Bloom’s cut-off of 80% was used to determine sufficient knowledge (≥80%) and positive attitude (≥4).11 Associations between independent variables (age, education details, tribe, ethnicity, sex, course of study, year of study, and sources of information on dementia) and dependent variables (level of knowledge and attitude towards dementia) were assessed at bivariate analysis using chi-square or Fisher’s Exact test. Variables with a P<0.2 were fitted into a multivariable logistic regression model to adjust for confounders. A P<0.05 was considered statistically significant for all hypothesis testing.
Covid-19 Safety Precautions
The study was conducted following the Ministry of health and the national covid-19 task force guidelines of Uganda. All the study team meetings, training, recruitment, data collection, and manuscript drafting were conducted online.
Results
Characteristics of Participants
A total of 1008 students responded to the survey (response rate = 97%). After removing 3 incomplete responses, data of 1005 students were analyzed. The median age of the respondents was 23 (interquartile range: 18 to 38) years. About 56.5% were males and only 5% (n=60) were in their fifth year of study. Over 90% of the students were single and were Christians (84.1%). Nearly half of the respondents were pursuing human sciences or medicine-related programs (46.8%, n=470) and nearly half (49.3%, n=495) were from Makerere University, the largest public tertiary institution in Uganda. Table 1 summarizes the socio-demographic characteristics of the participants.
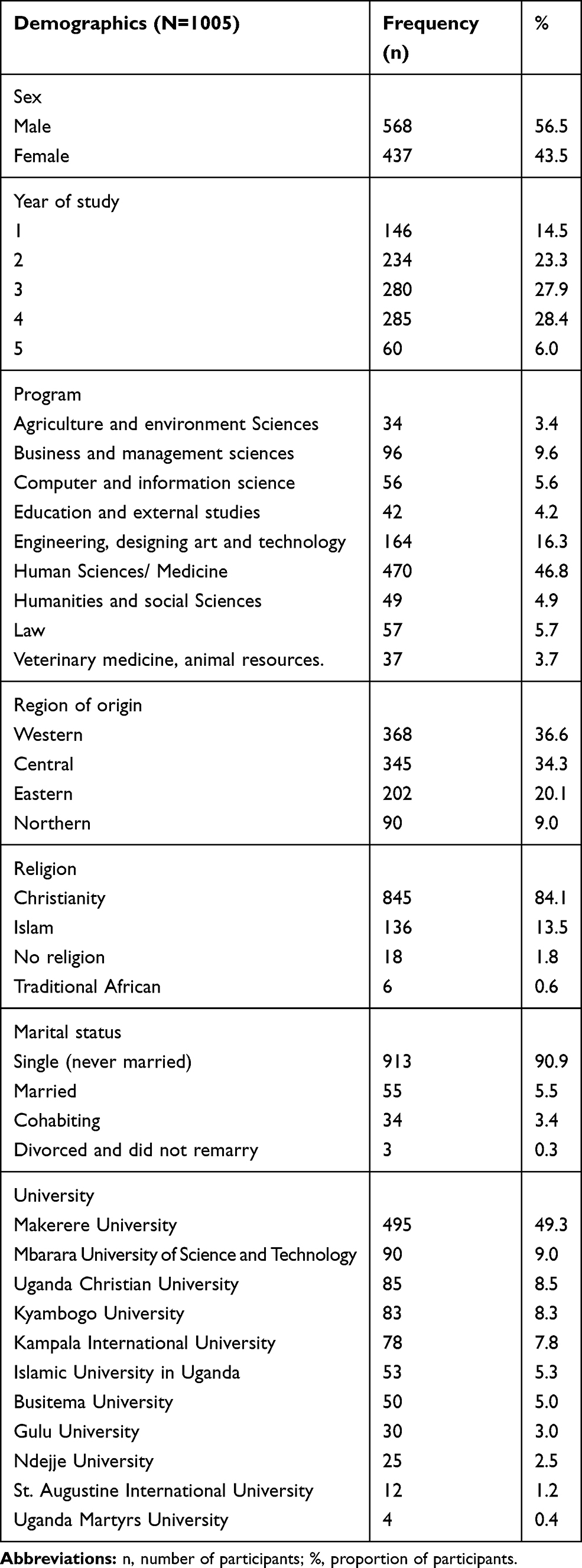 |
Table 1 Social and Demographic Characteristics of Participants |
Awareness and Knowledge of Dementia
About 78% (n=785) of the participants had heard about dementia or Alzheimer’s disease. Table 2 summarizes the responses of participants to questions on knowledge. Up to 53.4% believed that memory loss happened to all people as they age. However, the majority disagreed that forgetting family members (72%), names of objects (63%), and having trouble with speaking or understanding (53%) were normal parts of aging in humans. Remarkably, 60.2% of the participants were able to identify that the above symptoms were for dementia. Only 2.0% and 1.3% thought dementia was a punishment from God or ancestors, respectively. About 15.8% of the participants believed dementia affects only elderly people. Overall, nearly half had moderate knowledge (n=410, 41%) on dementia with only 26.8% having good knowledge and 32% had poor knowledge (Figure 1). This correlated with self-rated knowledge scale (no knowledge=5%, poor knowledge =40%, moderate knowledge =43%, very knowledgeable= 13%).
 |
Table 2 Responses of Participants to Questions About Knowledge on Alzheimer’s Disease and Dementia |
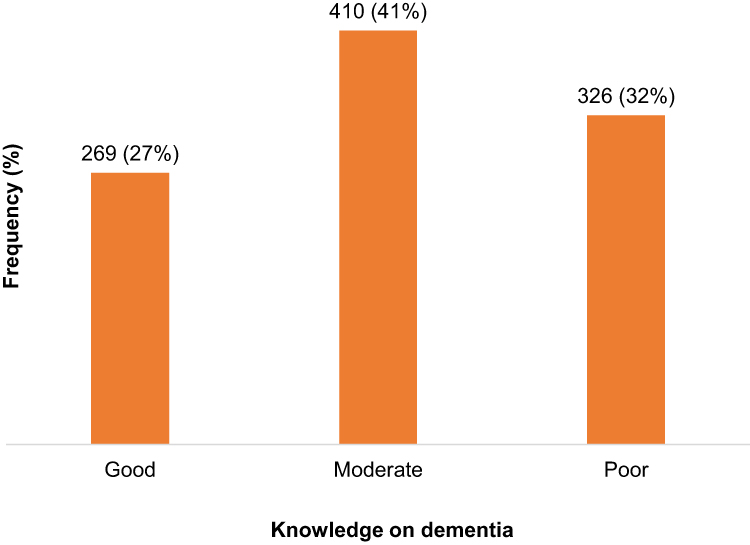 |
Figure 1 Categories of knowledge on dementia among Ugandan university students. |
At bivariate analysis (Table 3), good knowledge was associated with age (p=0.009), year of study (p<0.0001), academic program (p<0.0001), region of origin (p<0.0001) and university (p<0.0001). At multivariable logistic regression (Table 4), third - (AOR: 1.8, 95% CI: 1.0–3.2, p=0.035), fourth- (AOR: 3.1, 95% CI: 1.7–5.4, p<0.0001), and fifth-year students (AOR: 4.3, 95% CI: 2.0–9.4, p<0.0001) significantly had higher knowledge of dementia. Students pursuing human science or medicine-related programs were thrice more likely to have good knowledge of dementia (AOR: 3.1, 95% CI: 1.2–8.0, p=0.017). Also, students from eastern (AOR: 0.5, 95% CI: 0.3–0.8, p=0.002), northern (AOR: 0.3, 95% CI: 0.1–0.5, p<0.0001) and western Uganda (AOR: 0.5, 95% CI: 0.4–0.8, p=0.001) were less likely to have good knowledge of dementia compared to those in central Uganda.
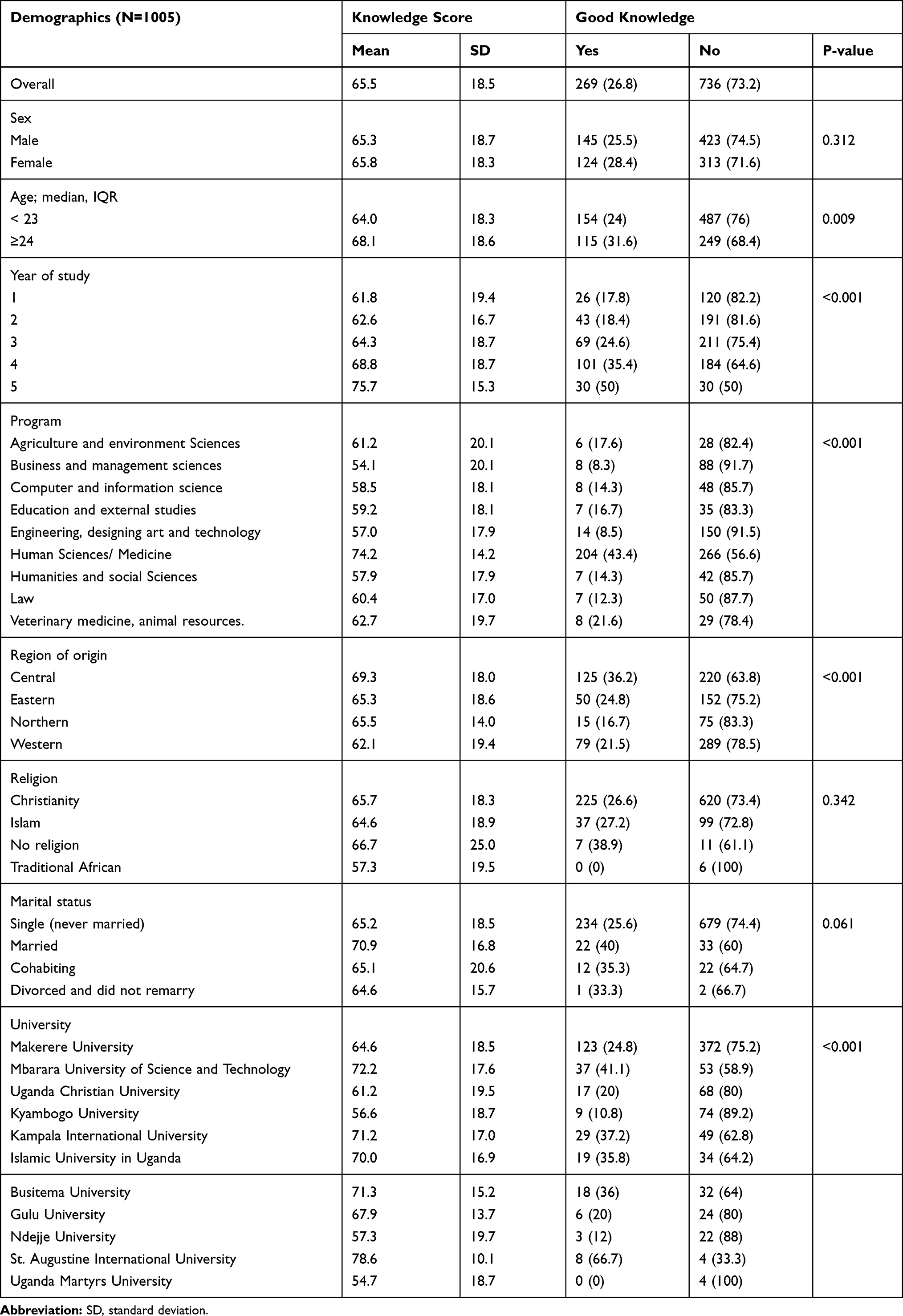 |
Table 3 Factors Associated with Good Knowledge of Dementia Among Ugandan University Students |
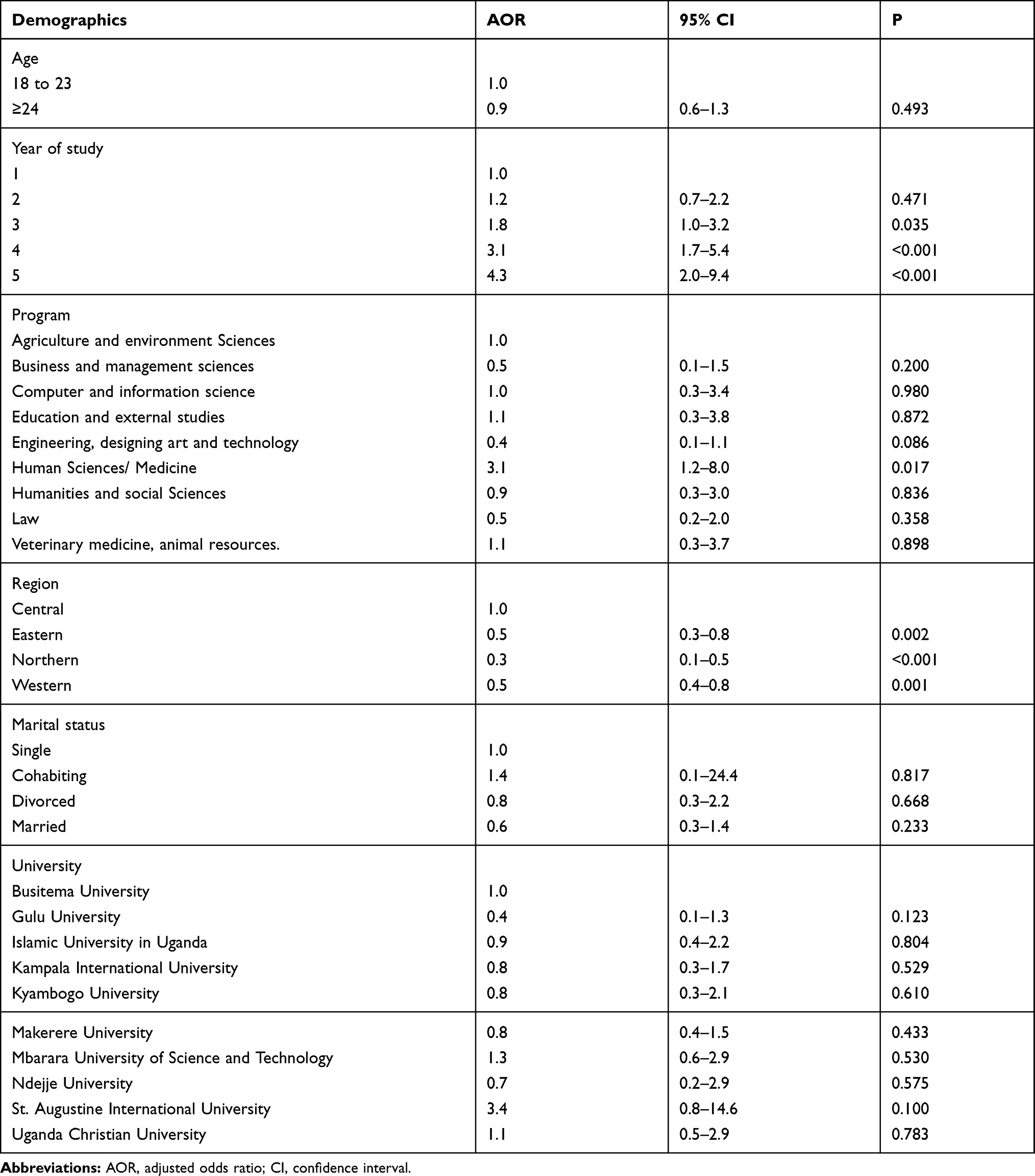 |
Table 4 Multivariable Logistic Regression Showing Factors Associated with Good Knowledge of Dementia |
Attitudes Toward Dementia
Table 5 describes the attitudes of university students towards patients with dementia. The vast majority of the participants were not scared to have as a neighbor (86.8%) as well sharing a house (88.5%) with a person with dementia. Only a few participants believed that persons with dementia were responsible for the condition (5.6%) and are dangerous people who should be avoided (7.2%). Overall, about two-thirds (65%, n=655) of the students had a positive attitude towards persons with dementia (Figure 2). At bivariate analysis, age (p<0.0001), year of study (p=0.041), and academic program (p=0.006) were associated with a positive attitude towards persons with dementia (Table 6).
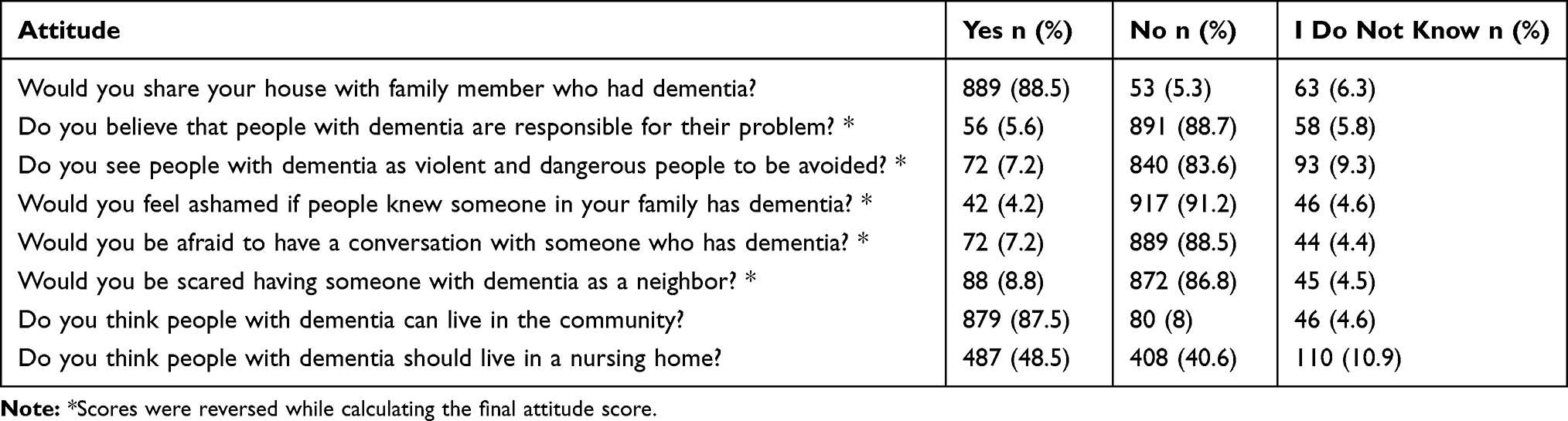 |
Table 5 Attitudes of Ugandan University Students Towards Dementia |
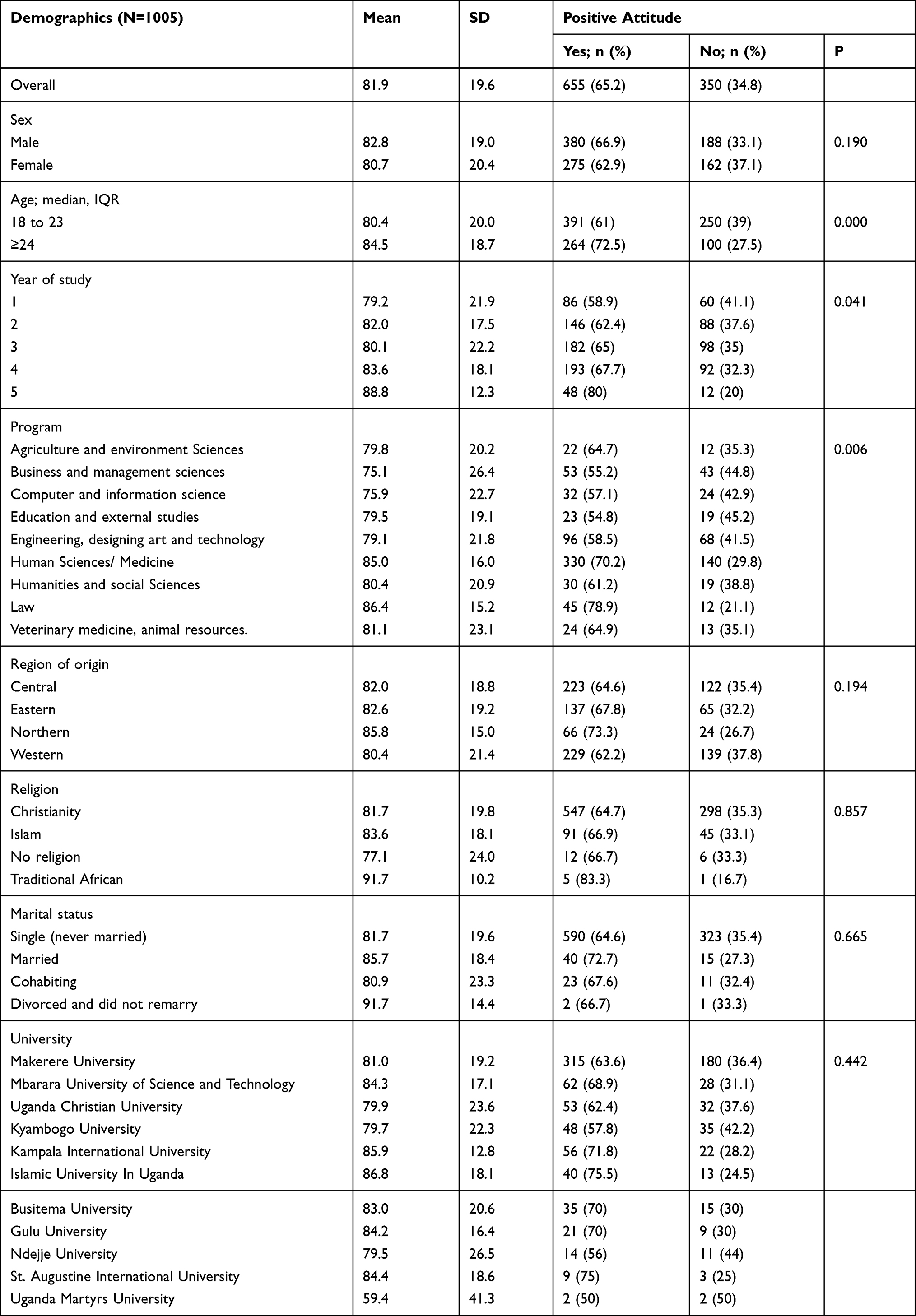 |
Table 6 Factors Associated with Positive Attitudes Towards Patients with Dementia |
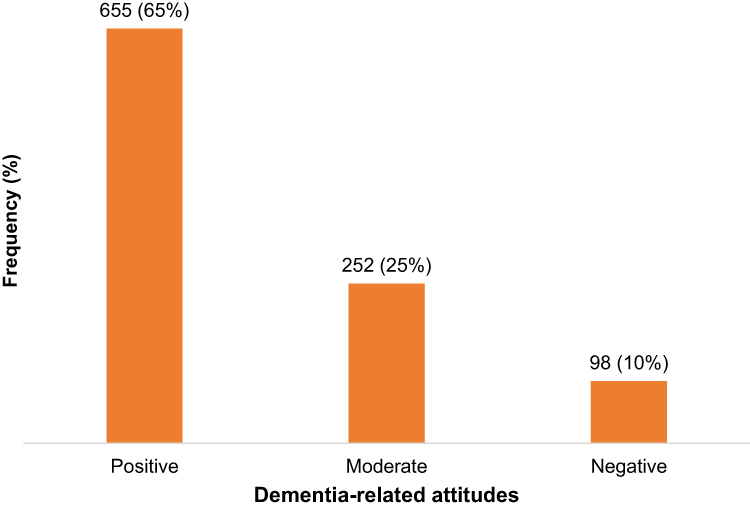 |
Figure 2 Attitudes towards dementia among Ugandan university students. |
University students aged 24 years and above were 1.5 times more likely to have a positive attitude towards persons with dementia at multivariable logistic regression (AOR: 1.5, 95% CI: 1.1–2.0, p=0.019, Table 7).
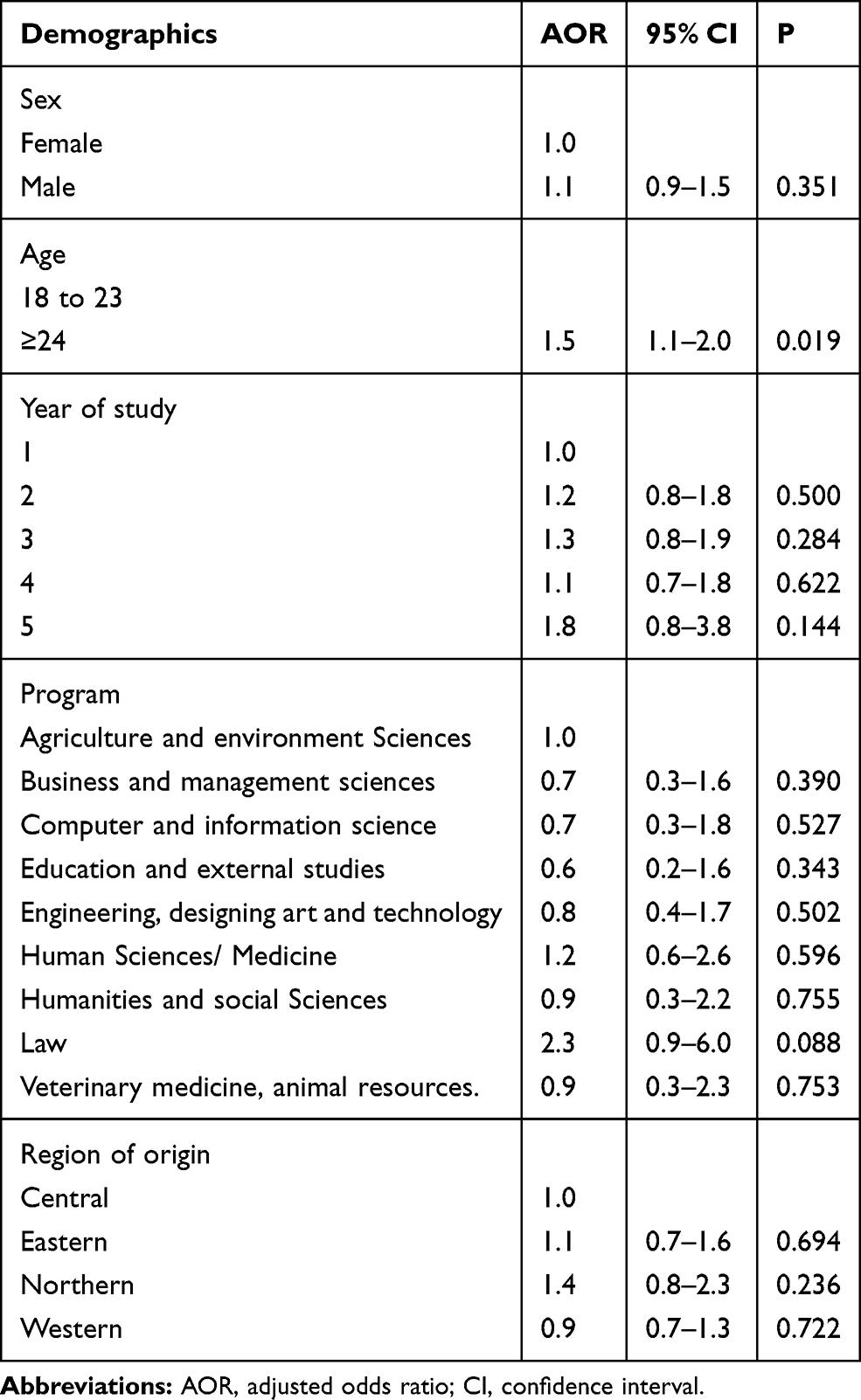 |
Table 7 Multivariable Logistic Regression Showing Factors Associated with Positive Attitudes Towards Dementia Among Ugandan University Students |
When pairwise correlation was performed, there was a weak correlation between knowledge and attitude scores (ρ=0.341, P<0.001).
Discussion
In this study, we administered an online questionnaire to undergraduate students to determine their attitudes and knowledge of dementia. The present study contributes information that would help refocus curricula for both medical and non-medical undergraduate students as well as guide targeted interventions to raise awareness of dementia in the general population. This study found that only 26.8% of the study participants had good knowledge regarding dementia and two-thirds had a good attitude regarding dementia.
Overall, the mean knowledge score on dementia of 65.5% was higher compared to that of the Norwegian undergraduate health and social care students of 23.51%12 and the undergraduate students of the University of Kathmandu who had 51.5% score.13 This may be due to fact that we used a different study questionnaire and scoring tool to what was used in these studies in Norway and Kathmandu, Nepal. This might explain the difference in scores. We adapted a pre-existing validated questionnaire that was used among the Xhosa-speaking people in South Africa while the other studies utilized the validated version of the Alzheimer’s disease Knowledge Scale (ADKS).
Furthermore, the mean knowledge score obtained in this study was higher compared to 53.44% found among the Urban Xhosa-Speaking Community in South Africa.10 The South African study was the closest we could compare our study with, due to the lack of similar studies in Sub-Saharan Africa and Africa in general. The two studies, however, were conducted in different target populations; undergraduate students versus the Urban Xhosa-Speaking people. Our study population included students undertaking various health programs hence more likely to have interfaced/interacted with a dementia patient/family. Also, campaigns to increase dementia knowledge within the general population are ongoing within Uganda.
Students undertaking health-related programs or were in the senior classes (years three, four, and five) were more likely to have good knowledge of dementia compared to non-medical students. This was consistent with one study where health care students had satisfactory knowledge compared to non-health students.14 The possible reason for this difference in knowledge among medical and non-medical may be that dementia education is included in the curricula of health-related programs or interface during the clinical teaching for health-related students as compared to those in non-health related programs.
In this study, the majority of the participants believed that dementia is a normal part of aging and that memory loss happened to all people as they age. This is the most common misconception in the general public and there is usually a lack of clarity about at which point normal age-related memory loss problems become severe enough to indicate dementia.15
About two-thirds of the study respondents had positive attitudes towards people with dementia. This finding is congruent with a greater number of studies reported from Changsha, China, Nigeria, and South Africa.10,16,17 Similarly, in our study just like in a cross-sectional study in Changsha,16 positive attitudes towards persons with dementia were generally influenced by age. We found a weak correlation between the knowledge and attitude scores although in the vast majority of the studies the attitude score does not correlate with the knowledge score.10,18–20
Students play an important role in the dissemination of information to the general public and provide care to patients with dementia. Therefore, efforts to boost the knowledge about the condition among the population should consider students with high regard. This can be done by integrating dementia lectures into the undergraduate academic curricula in the different institutions of learning to improve their knowledge. Additionally, the burden of dementia needs to be better understood in Uganda and other LMICs to enable the allocation of appropriate support and interventions. Consequently, integrating dementia into the academic curriculum along with research done about the condition will increase and maintain knowledge and skills among students and other health professionals. More so, integrating dementia programs into medical and nursing students’ curriculum is recommended as nursing research has shown that previous experience of dementia improves students’ compassion and care for people affected by dementia.21
Undergraduate medical students are the future workforce for patients with dementia, and understanding their attitude and compassion towards dementia patients is important.21 Live-model simulations which focus on dementia can help students to become more knowledgeable and have better attitudes about dementia and older adults.22
Limitations
Several limitations were taken into consideration as we interpreted these results. First, the study employed a non-random sample. Participation in the study was voluntary and no information was available about the characteristics of those who did not participate. Secondly, the cross-sectional design of our study does not allow for a causal interpretation of the results. Thirdly, due to the COVID 19 pandemic control measures, all Ugandan universities were temporarily closed, the data collection was only possible via online methods hence missing out on the population that did not own smartphones, poor connectivity to the internet or could not meet the data costs for participating in this study. This could lead to selection bias as students within rural areas might have been missed, this limits the generalization of these findings.
Fourthly, since the questionnaire was self-administered, there was a possibility of obtaining correct answers without a full understanding of dementia, recall bias and students may have interpreted the questions differently. We also used arbitrary knowledge and attitude scores which might not accurately reflect the knowledge and attitudes of the participants. However, despite these limitations, this is the first study assessing the knowledge and attitude of university students towards dementia in Uganda and SSA.
Conclusion
Whereas the majority of university students have positive attitudes towards patients with dementia, a significant number still have poor knowledge of dementia. Health education to improve knowledge is encouraged, including incorporation into the academic curriculum dementia sessions. Continuous awareness using the available media is encouraged to improve knowledge not only in this population but also in the general population. Further research into dementia prevalence, causes, and risk factors as well as care-burden and beliefs in Uganda to broaden the understanding of dementia is also urged to enable appropriate support and interventions to be introduced.
Data Sharing Statement
The data used to support the results of the research are available from the corresponding author upon request.
Ethics Approval and Informed Consent
Approval for the study was obtained from Mulago Hospital Research and Ethics Committee Reference Number; MHREC-1905. The study was conducted according to the Declaration of Helsinki. All participants were recruited only after informed electronic consent.
Acknowledgments
The authors appreciate Ms Evelyn Bakengesa, Ms Rhoda, and Ms Regina from HEPI-SHSSU for their support towards funding acquisition. The authors would also like to acknowledge all the University students who responded to the study and the research assistants from different Universities. Makerere University; Edward Tutu, Linda Atulinda, Alvin Akansasira, Lourita Nakyagaba, Arinda Deborah, Angelique Iradukunda. Mbarara University of Science and Technology; Solomon Muwanguzi, Ritah Atukwatsa, Patience Kemigisha. Kyambogo University; Joyce Nakalema, Ivan Kaijuka, Tracy Nalwanga. Gulu university; Simon Kimera, Brian Arube. Busitema University; Rossette Kyarikunda, Kenneth Wandera. Kampala International University (KIU); Obua Jonathan, Wannyana Babrah Iwakuba. Uganda Christian University (UCU); Andrew Okwi, Eria Kalemba, Cajo Delight M.Salamula, Dennis Sengooba Nyanzi, Reagan Muyinda, Tracy Wagonza. Islamic University in Uganda (IUIU); Khadijah Omar, Ndawula Kato Rodney. St. Augustine (King Caesar) International University; Paul Mulyamboga, Dennis Kwizera, and Ndejje University; Ivan Ssempijja, Dorah Namukasa, Amos Tumwesigye.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, took part in drafting the article or revising it critically for important intellectual content, agreed to submit to the current journal, gave final approval to the version to be published, and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Fogarty International Center of the National Institutes of Health, US Department of State’s Office of the US Global AIDS Coordinator and Health Diplomacy (S/GAC), and President’s Emergency Plan for AIDS Relief (PEPFAR) under Award Number 1R25TW011213. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
Dr Mark Kaddumukasa reports grants from FIC/NINDS; NIH, outside the submitted work. The authors declare no other potential conflicts of interest for this work.
References
1. World Health Organization. Dementia. 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/dementia.
2. International D. World Alzheimer report 2019: attitudes to dementia; world Alzheimer report 2019: attitudes to dementia. 2019. Available from: www.daviddesigns.co.uk.
3. Guerchet M et al. Dementia in sub-Saharan Africa: challenges and opportunities; Dementia in sub-Saharan Africa: challenges and opportunities. 2017. Available from: www.leahbeach.com.
4. UNFPA. Population ageing and development 2012. 2012. Available from: https://www.unfpa.org/resources/population-ageing-and-development-2012.
5. Mubangizi V, Maling S, Obua C, Tsai AC. Prevalence and correlates of alzheimer’s disease and related dementias in rural Uganda: cross-sectional, population-based study. BMC Geriatr. 2020;20:48. doi:10.1186/s12877-020-1461-z
6. Audu IA, Idris SH, Olisah VO, Sheikh TL. Stigmatization of people with mental illness among inhabitants of a rural community in northern Nigeria. Int J Soc Psychiatry. 2013;59:55–60. doi:10.1177/0020764011423180
7. Arai Y, Arai A, Zarit SH. What do we know about dementia?: a survey on knowledge about dementia in the general public of Japan. Int J Geriatr Psychiatry. 2008;23:433–438. doi:10.1002/gps.1977
8. Garvey G, Simmonds D, Clements V, et al. Making sense of dementia: understanding amongst indigenous Australians. Int J Geriatr Psychiatry. 2011;26:649–656. doi:10.1002/gps.2578
9. La Fontaine J, Ahuja J, Bradbury NM, Phillips S, Oyebode JR. Understanding dementia amongst people in minority ethnic and cultural groups. J Adv Nurs. 2007;60:605–614. doi:10.1111/j.1365-2648.2007.04444.x
10. Khonje V, Milligan C, Yako Y, et al. Knowledge, attitudes and beliefs about dementia in an urban xhosa-speaking community in South Africa. Adv Alzheimers Dis. 2015;4(2):21–36. doi:10.4236/aad.2015.42004
11. Kaliyaperumal K. Guideline for conducting a knowledge, attitude and practice (KAP) study. AECS Illum. 2004;4:7–9.
12. Kada S. Knowledge of alzheimer’s disease among Norwegian undergraduate health and social care students: a Survey Study. Educ Gerontol. 2015;41:428–439. doi:10.1080/03601277.2014.982009
13. Baral K, Dahal M, Pradhan S. Knowledge regarding alzheimer’s disease among college students of Kathmandu, Nepal. Int J Alzheimers Dis. 2020;2020:1–6. doi:10.1155/2020/6173217
14. Rawlins J. Attitude towards alzheimer’s disease among undergraduate students of university of the West Indies, Trinidad and Tobago. J Clin Diagn Res. 2015. doi:10.7860/JCDR/2015/10170.6571
15. Cahill S, Pierce M, Werner P, Darley A, Bobersky A. A systematic review of the public’s knowledge and understanding of alzheimer’s disease and dementia. Alzheimer Dis Assoc Disord. 2015;29:255–275. doi:10.1097/WAD.0000000000000102
16. Wang Y, Xiao LD, Luo Y, et al. Community health professionals’ dementia knowledge, attitudes and care approach: a cross-sectional survey in Changsha, China. BMC Geriatr. 2018;18(1):122. doi:10.1186/s12877-018-0821-4
17. Afolabi AO, Eboiyehi FA, Afolabi KA. Gender analysis of nurses’ attitude towards care of the elderly with dementia in Obafemi Awolowo University teaching hospitals complex, ile-ife, Osun State, Nigeria. J Women Aging. 2020;32:203–219. doi:10.1080/08952841.2019.1682488
18. Chertkow H, Feldman HH, Jacova C, Massoud F. Definitions of dementia and predementia states in alzheimer’s disease and vascular cognitive impairment: consensus from the Canadian conference on diagnosis of dementia. Alzheimers Res Ther. 2013;5:S2. doi:10.1186/alzrt198
19. Sheehan B. Assessment scales in dementia. Ther Adv Neurol Disord. 2012;5:349–358. doi:10.1177/1756285612455733
20. Sharma R, Sharma SC, Pradhan SN, Chalise P, Paudel L. Knowledge of alzheimer’s disease among medical students of a medical college. J Nepal Med Assoc. 2018;56:666–669. doi:10.31729/jnma.3622
21. Bickford B, Daley S, Sleater G, Hebditch M, Banerjee S. Understanding compassion for people with dementia in medical and nursing students. BMC Med Educ. 2019;19(35). doi:10.1186/s12909-019-1460-y
22. Maharaj T. Live-model simulation: improving nursing students’ attitudes and knowledge of alzheimer’s disease. Clin Simul Nurs. 2017;13:446–451. doi:10.1016/j.ecns.2017.05.002
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.