")
Back to Journals » International Journal of General Medicine » Volume 17
Assessment of the Effectiveness of Ultrasound-Guided Needle Aspiration of Lactating Breast Abscesses
Authors Tran AT, Nguyen DM , Tran QH , Nguyen QH, Nguyen Thi TH , Tran Thi DQ, Luu HN, Do Thi YM
Received 12 November 2023
Accepted for publication 30 January 2024
Published 13 February 2024 Volume 2024:17 Pages 553—557
DOI https://doi.org/10.2147/IJGM.S449432
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Anh Tuan Tran,1– 3,* Dinh Minh Nguyen,4,* Quang Hien Tran,5,6 Quang Hung Nguyen,7 Thu Ha Nguyen Thi,1 Do Quyen Tran Thi,1 Hong Nhung Luu,1 Yen Mai Do Thi1
1Radiology Center, Bach Mai Hospital, Hanoi, Vietnam; 2Radiology Department, University of Medicine and Pharmacy, Hanoi National University, Hanoi, Vietnam; 3Stroke and Brain Vascular Disease Department, University of Medicine and Pharmacy, Hanoi National University, Hanoi, Vietnam; 4Radiology Department, Viet Duc Hospital, Hanoi, Vietnam; 5An Giang Department of Health, An Giang, Vietnam; 6Obstetrics and Gynecology, an Giang Women’s and Children’s Hospital, An Giang, Vietnam; 7Oncology and Nuclear Medicine Center, Bach Mai Hospital, Hanoi, Vietnam
*These authors contributed equally to this work
Correspondence: Quang Hien Tran, An Giang Department of Health, Obstetrics and Gynecology, an Giang Women’s and Children’s hospital, 15 Le Trieu Kiet Street, Long Xuyen City, An Giang, Vietnam, Tel +84913104293, Email [email protected]
Objective: To evaluate the effectiveness of ultrasound-guided needle aspiration in treating lactating breast abscesses.
Methods: This study was conducted in Bach Mai Hospital, from 6/2020 to 7/2021. Lactating patients with breast abscesses underwent ultrasound-guided aspiration followed by antibiotics therapy.
Results: There were 59 lactating patients with 82 breast abscesses. Most of the abscesses had heterogeneous echogenicity, no capsule, and a size smaller than 5cm. Bacterial culture results showed that 85.4% of cases were Methicillin-resistant Staphylococcus aureus. The number of aspirations was from 1 to 5. The cure rate was 91.5%, and 5.3% of these cases had a complication associated with galactocele after treatment.
Conclusion: Ultrasound-guided needle aspiration is a minimally invasive treatment option for lactating breast abscesses with a high complete cure rate and good cosmetic results.
Keywords: breast abscess, ultrasound-guided needle aspiration
Introduction
Breast abscess is a localized collection of pus within breast parenchyma and is mostly a complication of mastitis.1 This disease is popular in women 18–50 years old and is divided into lactating and non-lactating abscesses, of which lactating breast abscess accounts for 0.4–11% of all puerperal women.2 Nutritional problems, maternal hygiene, low living standards, and late and ineffective use of antibiotics are the main reasons for severe breast abscesses, especially in developing countries.3
Treatment of breast abscess is a challenge, not only with the aim of cure but also preserving breast function. Incision and drainage abscess are the traditional treatment methods. However, this method has some disadvantages, such as general anesthesia, prolonged healing time, recurrent infection, and scars with poor cosmetic outcomes after treatment.4 Incision and drainage combined with antibiotic therapy have a recurrence rate of about 10–38%.5 Ultrasound guide-needle aspiration is a minimally invasive procedure that has been applied since the 90s, and currently, there have been a lot of studies demonstrating its effectiveness in treatment with some advantages, such as safety, good cosmetic outcome, and low-cost method.6,7 Therefore, we conducted a study with the aim of assessing the effectiveness of ultrasound-guided needle aspiration of lactating breast abscess.
Subjects and Methods
The prospective and descriptive study with a convenience sample was conducted at Radiology Center in Bach Mai Hospital from June 2020 to July 2021.
All lactating patients admitted to the hospital with suspected breast abscesses underwent breast ultrasound to detect abscesses. The exclusive criteria included recurrent or chronic abscess and necrosis skin overlying the abscess. The procedure was performed by a radiologist with more than five years of interventional experience, an assistant radiologist, and a nurse in the intervention room.
Disinfect and local anesthetic the needle puncture site with Lidocaine 2%. Insert a needle through the skin into the abscess and suction the abscess under ultrasound guidance, absorbing the maximum amount of fluid possible. The size of the needle was 18 gauge to 14 gauge, depending on the feature of the pus of the abscess. If the abscess had a capsule, irrigating the abscess cavity with saline was performed several times until the suction fluid returned clear. Suction pus was sent for culture and testing for sensitivity to antibiotics. Antibiotics were also used to combine with aspiration during the patient’s treatment.
After the first time of aspiration, the patients were re-examined clinically and by ultrasound every 4–5 days. If there was residual breast abscess on ultrasound, aspirations were repeated until no fluid was visible in the abscess cavity. The cure was defined that the clinical symptoms (including swelling, pain, redness, and fever) were obtained with complete resolution and no residual abscess on ultrasound. The treatment failure was determined that inflammation did not improve in clinical and laboratory tests, the abscess had not resolved after three to five aspirations, or the skin overlying abscess was necrotic. In these cases, the patients were converted to incision and drainage.
Data collection and statistical analysis: data was collected using a research medical record. Statistical analysis was done using SPSS 20 software. Categorical data were summarized into percentages. Ultrasound image characteristics are divided into size, echogenic, capsule and septa. Homogeneous or heterogeneous echo of the abscess indicates the degree of complete or incomplete fluidization of the abscess, helping to choose the needle size. Complications are divided into 4 categories: hematoma, galactocele, recurrent abscess, milk fistula.
Results
A total of 82 breast abscesses were diagnosed in 59 patients. Seventy-five abscesses were complete resolution while 7 patients were converted to incision and drainage after 5 times of aspirations.
The long axis diameter of the abscesses ranged from 1 to 14 cm. The rate of abscess sizes smaller than 3cm, 3–5cm, and over 5cm was 51.2%, 30.5%, and 18.3%, respectively. Almost all breast abscesses were heterogeneous echogenic, with no capsules and no septa (Table 1). Staphylococcus aureus accounted for 74 breast abscesses (90.3%), with 85.4% of Methicillin-resistant S. aureus. One patient had growth of Staphylococcus argenteus (1.2%). Seven patients had negative pus cultures (Table 2). Most of the patients resolved after 1–3 aspirations, including 42.7% with one aspiration, 26.7% with two aspirations, and 21.3% with three aspirations. Two patients (2.7%) had complete resolution after five aspirations (Table 3). The success rate of ultrasound-guided needle aspiration of lactating breast abscesses was 91.5% (75 of 82 patients). The cure rate was 100% in all patients with small abscess sizes less than 5cm. There were also seven patients converted to incision and drainage, and all had abscess sizes larger than 5cm (Table 4). Galactocele was the only complication in that group of patients (5.3%) (Table 5). In the group of patients resolved with ultrasound-guided needle aspiration, there were no scars, and the patients were satisfied with good cosmetic outcomes; 88.5% of patients continued breastfeeding following treatment, and six patients (11.5%) stopped breastfeeding.
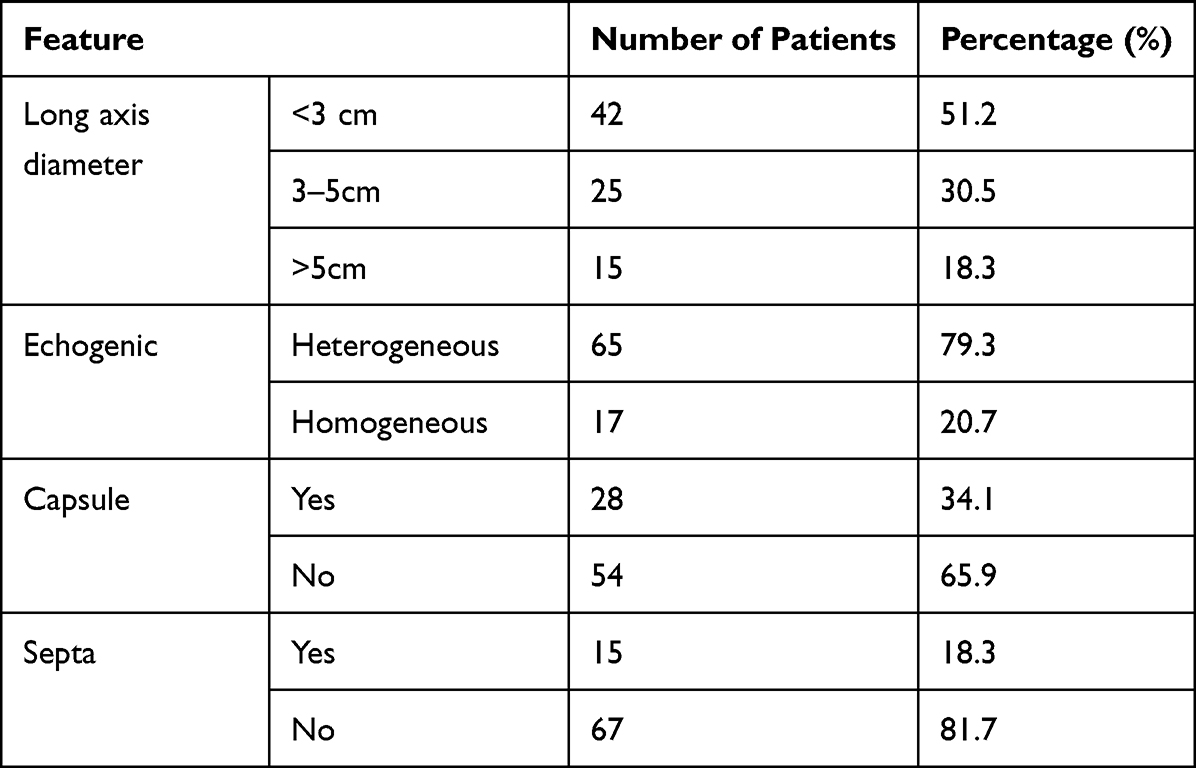 |
Table 1 Ultrasound Features of Breast Abscesses (n=82) |
 |
Table 2 Pus Culture Results (n=82) |
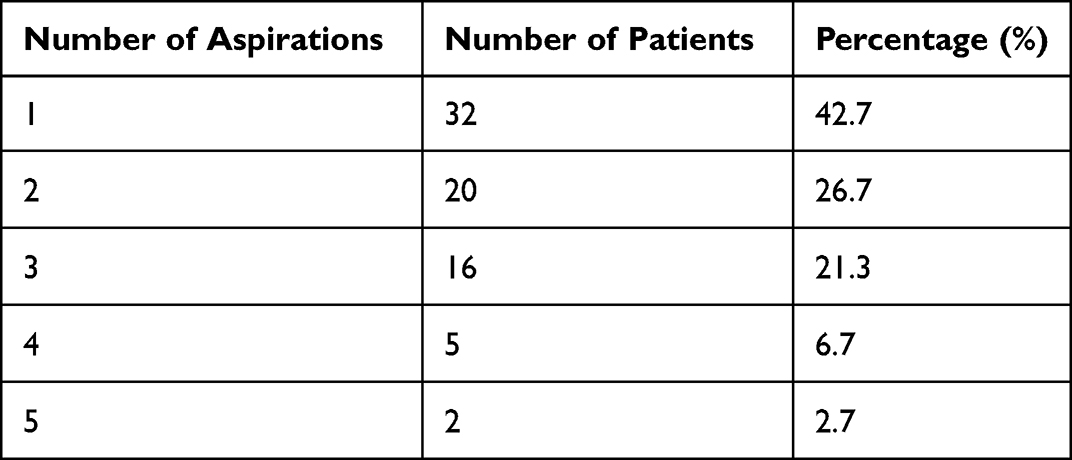 |
Table 3 Aspirations Required for Complete Resolution (n=75) |
 |
Table 4 The Association Between Abscess Size and Success Rate |
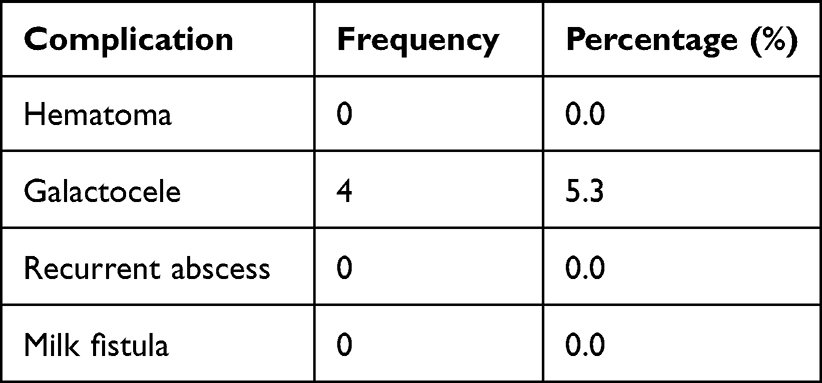 |
Table 5 Aspiration’s Complications After Complete Resolution (n=75) |
Discussion
Overall, our study had 59 lactating patients with 82 breast abscesses. Currently, most studies indicate ultrasound-under guided needle aspiration for breast abscesses smaller than 3cm or 5cm.8,9 However, in our study, we did not limit the abscess size. Most abscesses in this study had heterogeneous echogenic, no capsule or septa. These features demonstrate the ability to treat abscesses at early stage of the method.
The bacteria culture showed that the rate of Staphylococcus aureus and negative results was 90.3% and 8.5%, respectively, of which Methicillin-resistant S. aureus accounted for 85.4%. The results were close to those of Chen et al who reported 88% of Staphylococcus aureus and 75% of Methicillin-resistant S. aureus with lactating abscesses.10 The cause of breast abscess was mainly Staphylococcus aureus and the prevalence of Methicillin-resistant Staphylococcus aureus was increasing. This recommended the appropriate choice of antibiotics for the treatment of mastitis and breast abscess.
The healing rate in our study was 91.5%. The healing rate of abscesses smaller than 3cm, 3 to 5cm, and over 5cm was 100%, 100%, and 53.3%, respectively. The number of aspirations was 1–5, of which most patients healed after 1–3 times of aspiration, accounting for 90.7%, as in Figure 1. Elagili et al reported 50% of patients resolved completely with one aspiration, 23.3% with two aspirations, 10% with three aspirations, and the success rate was 83.3%.11 Dahiphale et al reported a 90% cure rate of 30 patients with breast abscesses smaller than 7cm.12
 |
Figure 1 Illustration for a lactating breast abscess in early stage, obtained resolution after one aspiration. (a) at admission, ultrasound shows a fluid collection with capsule and peripheral edema. (b) Seven days post-aspiration, ultrasound shows a hypoechoic area corresponding to inflammatory tissue, with no remaining fluid collection and (c) 14 days post-aspiration, the hypoechoic area decreases significantly in size. |
The complication rate is 5.3%, including four patients with galactocele. Most studies did not report galactocele complications due to the limitation of the size of the breast abscess and the number of aspirations. Chandika et al reported that if the abscess persisted on day 14, it was considered treatment failure and converted to the traditional incision and drainage.13
Milk drainage has an important role in mastitis treatment and is required to be performed with other methods to resolve infection and relieve discomfort. In cases where the patient is taking antibiotics that are not contraindicated to breastfeeding, the patient should be encouraged to continue breastfeeding following breast infection. If the abscess near the nipple causes pain and inability to breastfeed, milk fistula, or the abscess does not reduce in size after aspiration, the use of medication to stop breastfeeding should be considered.14 In the group of patients resolved with ultrasound-guided needle aspiration of our study, six patients stopped breastfeeding including two patients with pain and four patients with abscesses that did not improve after from 2 to 3 times of aspiration.
Conclusion
Aspiration ultrasound-guided breast abscess is a minimally invasive, effective, and safe procedure with advantages. Our study recommends aspiration ultrasound-guided should be the first choice in lactating breast abscesses with normal overlying skin.
Ethics Approval and Informed Consent
All procedures were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Our study protocol was approved by the Ethics Committee of Bach Mai Hospital (Hanoi, Vietnam). We obtained verbal consent from the participants instead of written consent, and this procedure was approved by the Ethics Committee.
Disclosure
Anh Tuan Tran and Dinh Minh Nguyen are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Rizzo M, Peng L, Frisch A, Jurado M, Umpierrez G. Breast abscesses in nonlactating women with diabetes: clinical features and outcome. Am J Med Sci. 2009;338(2):123–126. doi:10.1097/MAJ.0b013e3181a9d0d3
2. Dener C, Inan A. Breast abscesses in lactating women. World J Surg. 2003;27(2):130–133. doi:10.1007/s00268-002-6563-6
3. Trop I, Dugas A, David J, et al. Breast abscesses: evidence-based algorithms for diagnosis, management, and follow-up. Radiographics. 2011;31(6):1683–1699. doi:10.1148/rg.316115521
4. Benson EA. Management of breast abscesses. World J Surg. 1989;13(6):753–756. doi:10.1007/BF01658428
5. Watt-Boolsen S, Rasmussen NR, Blichert-Toft M. Primary periareolar abscess in the nonlactating breast: risk of recurrence. Am J Surg. 1987;153(6):571–573. doi:10.1016/0002-9610(87)90158-9
6. Strauss A, Middendorf K, Müller-Egloff S, Heer I, Untch M, Bauerfeind I. Sonographisch gesteuerte Mammaabszesspunktion als minimal-invasive Alternative zur chirurgischen Inzision. Ultraschall Med. 2003;24(6):393–398. doi:10.1055/s-2003-45217
7. Zhou F, Li Z, Liu L, et al. The effectiveness of needle aspiration versus traditional incision and drainage in the treatment of breast abscess: a meta-analysis. Ann Med. 2023;55(1):2224045. doi:10.1080/07853890.2023.2224045
8. Eryilmaz R, Sahin M, Hakan Tekelioglu M, Daldal E. Management of lactational breast abscesses. Breast. 2005;14(5):375–379. doi:10.1016/j.breast.2004.12.001
9. Ulitzsch D, Nyman MK, Carlson RA. Breast abscess in lactating women: US-guided treatment. Radiology. 2004;232(3):904–909. doi:10.1148/radiol.2323030582
10. Chen CY, Anderson BO, Lo SS, Lin CH, Chen HM. Methicillin-resistant Staphylococcus aureus infections may not impede the success of ultrasound-guided drainage of puerperal breast abscesses. J Am Coll Surg. 2010;210(2):148–154. doi:10.1016/j.jamcollsurg.2009.11.003
11. Elagili F, Abdullah N, Fong L, Pei T. Aspiration of breast abscess under ultrasound guidance: outcome obtained and factors affecting success. Asian J Surg. 2007;30(1):40–44. doi:10.1016/S1015-9584(09)60126-3
12. Dahiphale A, Kandi A, Titare P, Kaginalkar V, Jadhav S. Ultrasound-guided Percutaneous Aspiration of Breast Abscesses: an Outpatient Procedure. Int J Sci Stud. 2016;4(2):169–172.
13. Chandika AB, Gakwaya AM, Kiguli-Malwadde E, Chalya PL. Ultrasound Guided Needle Aspiration versus Surgical Drainage in the management of breast abscesses: a Ugandan experience. BMC Res Notes. 2012;5(1):12. doi:10.1186/1756-0500-5-12
14. Spencer JP. Management of mastitis in breastfeeding women. Am Fam Physician. 2008;78(6):727–731.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.