Back to Journals » ClinicoEconomics and Outcomes Research » Volume 14
Assessment of Primary Health Care Specialized Reference Clinics in Riyadh First Health Cluster: Outcome, Cost-Effectiveness and Patient Satisfaction
Authors Alshowair A ![]() , Altamimi S, Alruhaimi F, Tolba A, Almeshari A, Almubrick R
, Altamimi S, Alruhaimi F, Tolba A, Almeshari A, Almubrick R ![]() , Abdel-Azeem A
, Abdel-Azeem A ![]()
Received 30 December 2021
Accepted for publication 8 April 2022
Published 5 May 2022 Volume 2022:14 Pages 371—381
DOI https://doi.org/10.2147/CEOR.S355507
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Abdulmajeed Alshowair,1 Saleh Altamimi,1 Faisal Alruhaimi,1 Ali Tolba,1 Alhanouf Almeshari,2 Rehab Almubrick,3 Amro Abdel-Azeem3,4
1Community Health Excellence, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia; 2Public Health Administration, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia; 3Population Health Management, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia; 4Department of Community, Environmental and Occupational Medicine, Faculty of Medicine Zagazig University, Zagazig, Egypt
Correspondence: Amro Abdel-Azeem, Population Health Management, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia, Tel +966 547135224, Email [email protected]
Purpose: The objectives of the study are to assess the outcome and cost-effectiveness of specialized reference clinics (SRCs) in primary health care centers (PHCCs) of Riyadh First Health Cluster (RFHC), then to estimate the patient satisfaction among clients utilizing such SRCs.
Patients and Methods: This facility-based study was conducted in Riyadh city, Saudi Arabia among six PHCCs in RFHC that contain SRCs. Records of all patients utilizing SRCs and their referral information were studied along two years. An in-depth interview was conducted with health care providers in SRCs. Cost analysis was calculated by the financial support group within RFHC. Also, a randomly selected 400 subjects utilizing SRCs were asked to fill patient satisfaction questionnaire.
Results: Over two years, a total number of 55,084 patients utilized SRCs among different specialties. Most of these patients (86.7%) had full medical service within PHC-SRCs with no need for referral to hospitals. SRCs are significantly effective in decreasing the burden on hospitals in most specialties (p < 0.001). This effectiveness is significantly increased during the 2nd year of service. The time spent until appointment is significantly reduced from an average of six weeks in hospitals to an average of one week in SRCs. SRCs are very cost-effective as they reduced referrals to hospitals by 86.7% among 55,084 patients who utilized SRCs over two years, saving total costs of about 14.08 million Saudi Riyals (3.75 million US dollars). Most of the specialties are cost-effective except for urology and general surgery clinics, which are not cost-effective. Patient satisfaction is high regarding all service domains. The overall patient satisfaction score increased from 71.4% in the 1st year up to 73.2% in the second year.
Conclusion: PHC-SRCs are cost-effective health services and their creation is reasonable and beneficial in terms of reducing costs of health care delivery, reducing the burden on hospitals, and improving patient satisfaction.
Keywords: specialized reference clinics, outcome, cost-effectiveness, patient satisfaction, primary health care
Introduction
World health organization (WHO) defines referral as:
a process in which a health worker at one level of the health system having insufficient resources (drugs, equipment, skills) to manage a clinical condition seeks the assistance of a better or differently resourced facility at the same or higher level to assist in or take over the management of the client’s case.1
There are two types of referrals primary care physicians’ (PCPs’) specialty referrals and patients self-requested referrals.2 The main reasons for patients’ referral are looking for expert opinion, specific treatment, lack of specific specialties and the need for further management, additional assessment of patients, diagnosis of complicated cases, and unsure diagnosis or inadequate facilities and services for treatment that exist in primary health care centers.3–6 Some chronic and acute medical conditions, emergency, surgical and delivery cases may deserve referrals. To avoid hospitals being overcrowded and waste of time and resources, some cases can be treated and managed in the primary health care centers with no need to be referred to a tertiary hospital.7
A survey was done by the Practice Management Committee of the Pediatric Orthopedic Society of North America shows that most of the new referrals were for patients that could have been managed by PCPs.8 Also the lack of communication between PCPs and specialists in hospitals affects negatively on the referral system.9,10 Incomplete referral also is considered a problem that may be related to several factors such as chronic conditions and health care of surgical specialty clinic type, long time until the appointment and frequent appointment rescheduling.11 In addition, each year over 19 million clinically inappropriate physician referrals occur because of poor physician networks and the lack of secure and reliable communication channels between practices. For these reasons, it is important to establish specialized clinics in primary health care centers to treat and control patients with adequate resources and services to reduce the pressure on the tertiary hospitals and save time and costs.12 Under optimum conditions, about 85% of patients can be treated at the primary level,13,14 On the other hand Simba et al find that up to 72.5% of patients at the hospital were self-referral.15 The role of the PCPs in limiting access to secondary care is considered a strength of the national health service. In some parts of the world where health provision is largely state-funded and organized, self-referral is rare. Nevertheless, some patients have clear views of their need for referral and exert pressure upon their PCPs.16
Bypassing the lower levels of health care service increases the pressure of primary care on hospital facilities distorting health program development at the community level. Also, it makes patients have delayed appointments and spend longer waiting time to consult specialized medical workers in hospitals. This is not only a waste of time but also a misapplication of the highly trained health workers’ time. This is why a number of governments are interested in converting PHCCs to specialized clinics.7,17 Moreover, patients’ satisfaction (PS) with provided health services has emerged as a very important parameter in the evaluation of healthcare services to improve quality and accessibility while controlling cost.18,19 Low PS is associated with decreased trust in caregivers and low-perceived quality of care leading to underutilization of services, poor compliance with treatment, and neglecting follow-up.20,21
With the advent of higher health care costs in the past decade, an increasing number of companies are developing specialized clinics.22 Poor adherence to referral guidelines is associated with increased costs.23 In response to these findings, In July 2019, we developed an integrated Primary Health Care Reference Specialty Clinics and began seeing patients at six PHCCs located in Riyadh First Health Cluster. The clinic is the new home for the PHC referral cases and will provide affordable, comprehensive, confidential specialty services to clients in the Riyadh First Health Cluster catchment area.
These Reference Specialty Clinics require a shift in financial investments, and reallocation in costs and funding.24 Consequently, economic evaluation of health services is essential for hospital management, society, and decision-makers.25 Accordingly, our objectives in this study were to assess the outcome and the cost-effectiveness of SRCs in the Riyadh First Health Cluster and to estimate the level of patient satisfaction among clients utilizing such SRCs.
Materials and Methods
Study Design and Setting
This study was conducted as a facility-based study in Riyadh city, which is located in the central province of Saudi Arabia. The study was carried out among the six primary health care centers in Riyadh First Health Cluster (RFHC), which contains Specialized Reference Clinics. In our study, we used both a retrospective and prospective design. Records of all patients utilizing SRCs and those referred to tertiary care from SRCs were studied retrospectively and prospectively along the period from July 2019 to June 2021 (2 years of study). An in-depth interview was conducted with HCPs working at SRCs. Also, a cross-section of randomly selected 400 subjects utilizing SRCs was interviewed and asked to fill patient satisfaction questionnaire. Cost-effectiveness analysis was done depending on the cost analysis data calculated by the financial support group within RFHC.
Data Collection
The data was collected using four instruments including 1) The records of SRCs; 2) In-depth interviews with HCPs; 3) Patient satisfaction questionnaire; 4) Cost analysis data sheet stated by the financial support group within RFHC.
Measuring the Outcome
Records of SRCs in RFHC were studied retrospectively and prospectively. The total number of patients, who utilized SRCs over a period of two years from July 2019 to June 2021, was calculated. Also, we determined the total number of patients referred from our SRCs to tertiary hospitals in RFHC. Then, the actual reduction in referral to tertiary hospitals was calculated and expressed as a percentage of referral reduction (Reduced burden on tertiary hospitals). The percentage of referral reduction was calculated by subtracting both numbers and multiplying the result by one hundred as seen in the following equation (The total number of patients utilized SRCs – The total number of patients referred from SRCs to tertiary hospitals) X 100. This equation was used many times, first for measuring the total reduction in referrals from all patients attending our SRCs and then calculated for each specialty alone to determine the most efficient specialties regarding both high utilization rate and high referral reduction percentage.
Characteristics of referred cases were collected from SRCs’ records and from In-depth interviews with HCPs working at SRCs (Each interview takes an average of 30 min). The collected patient referral information included type of referral (self-requested, doctors’ decision), type of referred case (acute, chronic), reasons of referral to the tertiary hospital (Barriers and challenges for PHC-SRCs), and time spent in the process at various stages (time spent until appointment in specialized reference clinic, time spent until appointment in tertiary hospital).
Cost Analysis
Cost analysis sheets, stated with the financial support group within RFHC, were obtained and analyzed. The financial support group calculated the average cost for patient service both in SRCs and in tertiary hospitals. The average cost for patient service in SRCs was estimated to be 295 Saudi Riyal (SR), while the average cost for patient service in the tertiary hospital was estimated to be 590 SR (double cost). So, for every patient serviced in SRCs rather than a tertiary hospital, we save about 295 SR. The total reduction in costs was calculated by multiplying the total number of reduction in referrals to tertiary hospitals by 295 SR, as shown in the following equation (Total number of cases serviced in SRCs without referral to tertiary hospital X 295 SR). Also, the reduction in costs per specialty was calculated to identify the most efficient specialties.
Measuring Patient Satisfaction Level
A patient satisfaction survey was conducted among a cross-section of randomly selected 400 subjects utilizing SRCs. The sample size is estimated to be 384, at a significance level of 95% and power of 80% using OpenEPI statistical software. We included 400 subjects to overcome participants’ non-response or any incomplete data. Two hundred subjects were interviewed within the 1st year of SRCs’ service and the other Two hundred subjects were interviewed within the 2nd year of SRCs’ service to evaluate the change in patient satisfaction along the two years of service. Participants were interviewed during their visit to SRCs and asked to fill out a pre-constructed, self-administered patient satisfaction questionnaire. The questionnaire is based on previously published literature after some modifications, “patient satisfaction survey” provided by the American Academy of Family Physicians (AAFP) and the Medical Group Management Association (MGMA).26
The questionnaire contains a total of fourteen closed-ended questions for evaluating patient satisfaction with PHC-SRCs, based on 5 points Likert scale ranging from 1 (poor) up to 5 (excellent). The questionnaire is divided into five domains: 1) Four questions to assess patient satisfaction with his appointment and communication process in PHC-SRCs; 2) Three questions to assess patient satisfaction with SRCs’ staff (The professionalism of our physicians, nurses, and technicians); 3) Two questions to assess patient satisfaction about the medical services in PHC-SRCs; 4) Three questions to assess patient satisfaction about our PHC-SRCs facility and 5) Two questions to assess the overall patient satisfaction about the SRCs.
To ensure the reliability of the questionnaire, a pilot study was conducted at the beginning on 30 subjects and the questionnaire results were analyzed using Cronbach‘s alpha coefficient (>0.7). Then items with low scale were re-examined and modified as needed. The questionnaire had taken an average of 10 min for filling.
Statistical Analysis
The collected data was analyzed by Statistical Package for the Social Sciences (SPSS) software version 21 and it has been summarized as frequencies and percentages for qualitative variables and mean ± SD for quantitative variables. For ordinal scale and non-parametric data, median and range were used for summarization. Regarding the scoring of the patient satisfaction questionnaire, the total satisfaction score was calculated for each domain (mean ± SD) and then expressed as a percentage of one hundred. Statistical difference between proportions was tested using Chi-square test, while comparison between means was done using t-test. For ordinal scale and non-parametric data, Mann–Whitney Utest was used to test the difference. Reliability was tested using Cronbach’s alpha coefficient. Results will be considered significant if (p ≤ 0.05).
Results
Assessment of the Outcome
In July 2019, Reference Specialty Clinics were established and began serving patients at six PHC centers located in Riyadh First Health Cluster. By June 2021, a total number of 55,084 patients utilized SRCs among all its different specialties. Most of these patients (86.7%) had full medical service within PHC-SRCs with no need for further referral to tertiary hospitals. While only 7340 patients (13.3%) are referred to tertiary hospitals for further investigation or advanced management. PHC-SRCs are very effective in reducing referrals to hospitals by 86.7% leading to decrease the burden on tertiary hospitals and that is statistically significant (p < 0.001). The effectiveness of PHC-SRCs in reducing referrals is significantly increased during the 2nd year of service than that during the 1st year as regards all specialties (p < 0.001) as demonstrated in Table 1.
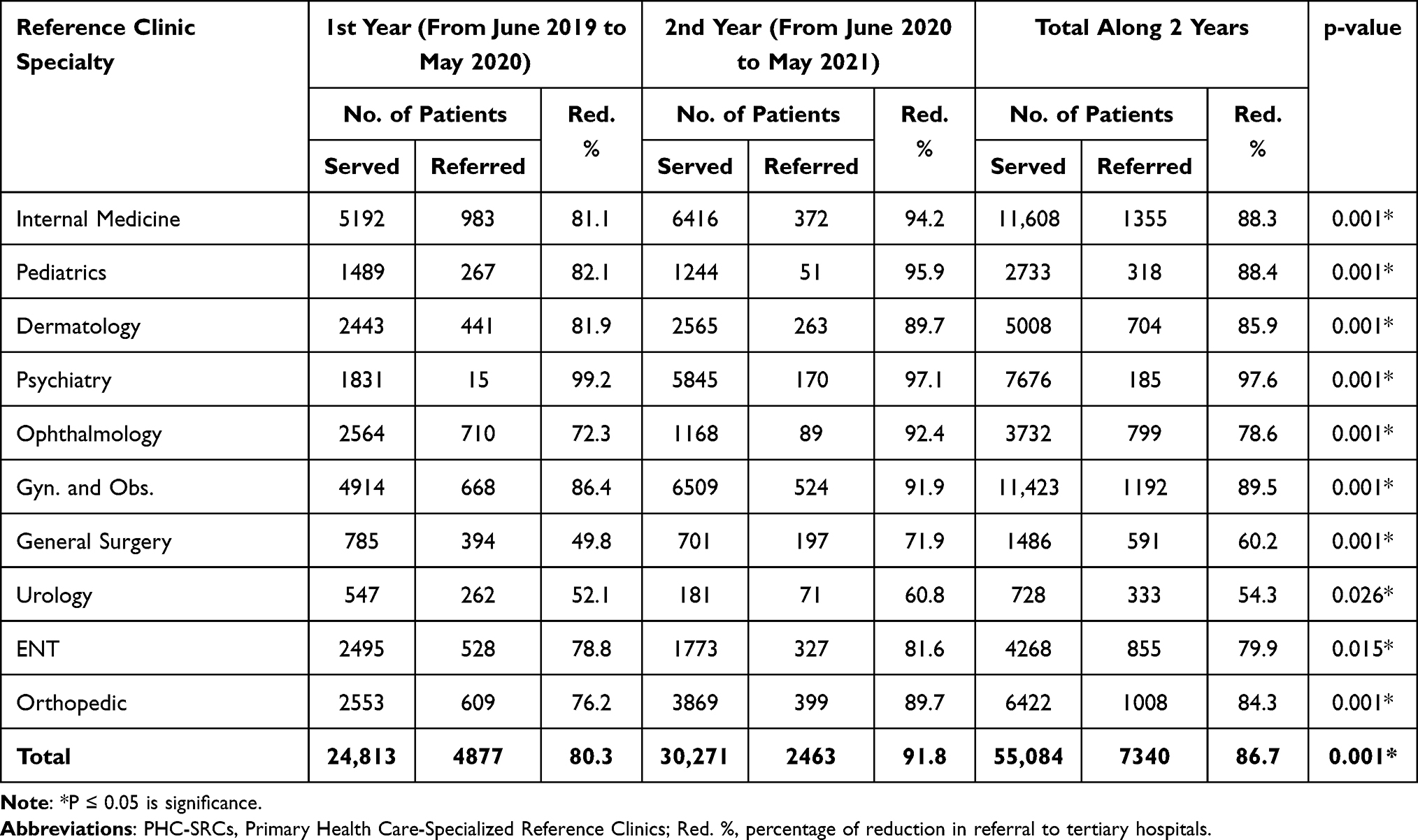 |
Table 1 Total Patients Served in PHC-SRCs and Those Who Were Referred to Tertiary Hospitals |
The highest utilization was noticed among Internal Medicine, Gynecology & Obstetrics, Psychiatry and Orthopedic clinics (11,608, 11,423, 7676 and 6422 patients) respectively, with a high reduction in referrals exceeding 84%. While, Urology and General Surgery clinics showed the lowest utilization (728 and 1486 patients) respectively, and also showed the lowest reduction in referrals (less than 60%) as demonstrated in Table 1 and Figure 1.
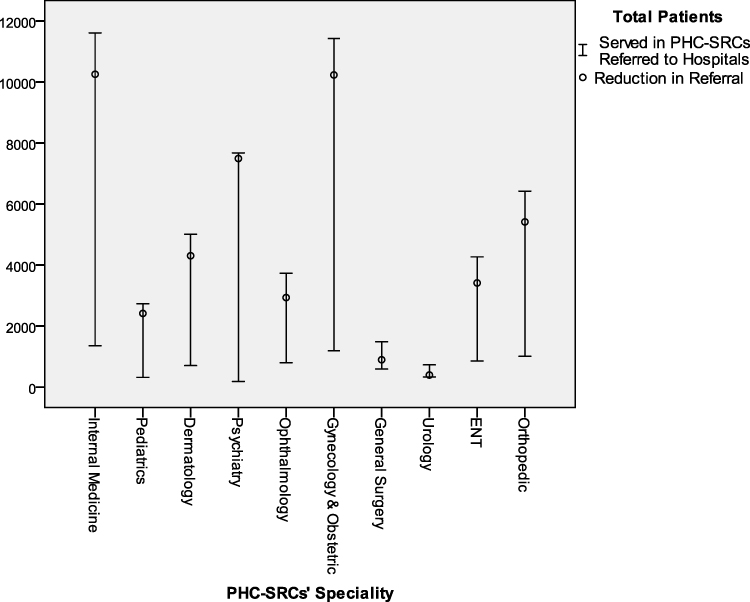 |
Figure 1 Total patients served in PHC-SRCs and those who were referred to tertiary hospitals. |
As shown in Table 2, most of the patients referred from SRCs to tertiary hospitals were chronic cases that are persistent or otherwise long-lasting in their effects (about 75%) and their referral was the doctors’ decision in about 80% of cases. Although there is a statistically significant reduction in time spent until appointment from about six weeks in hospitals to about one week in SRCs, some cases still need a referral to hospitals. The need for sophisticated management and lack of some investigations in PHC appeared as the main reasons for referral to tertiary hospitals (45% and 20%) respectively.
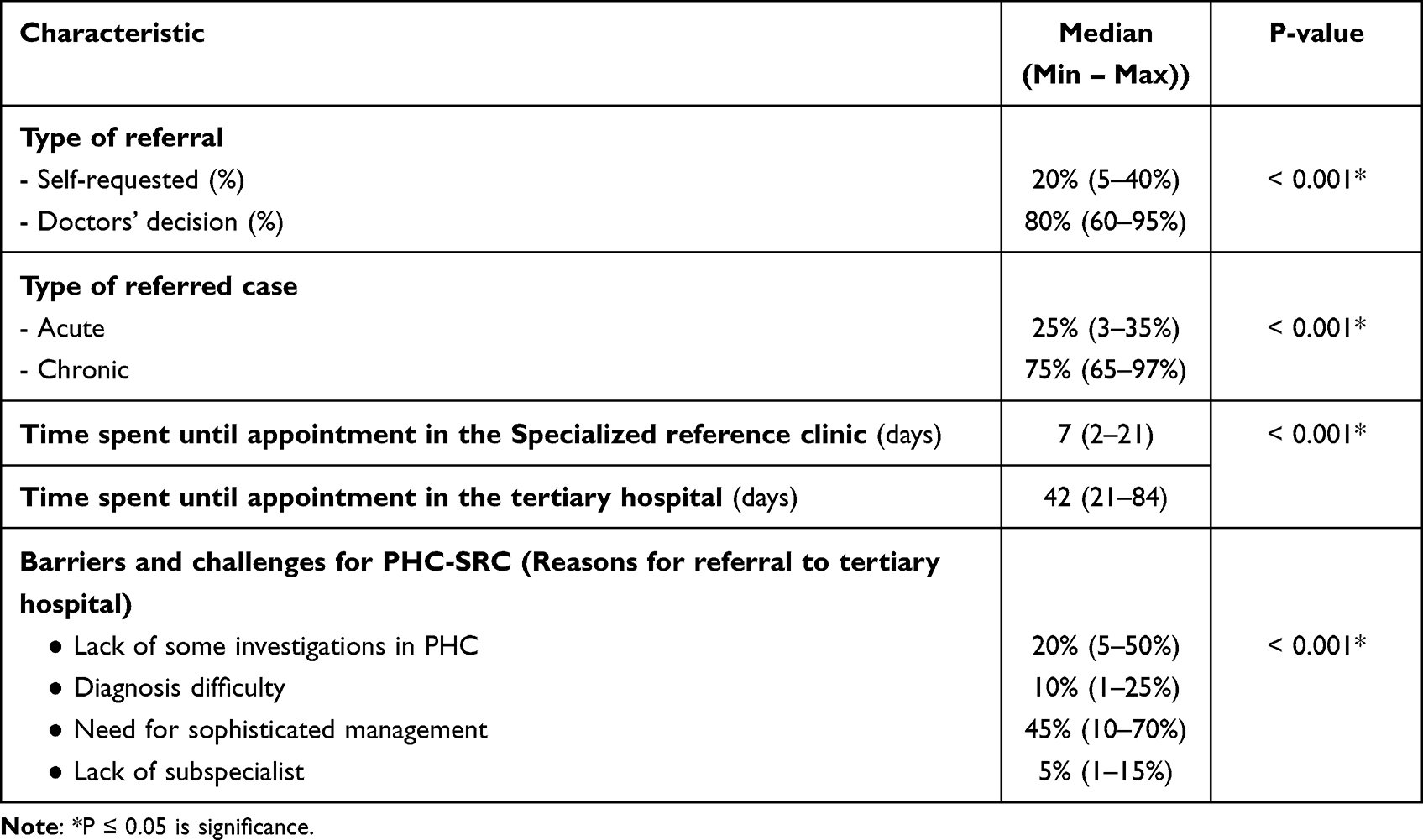 |
Table 2 Reasons for Referral to Tertiary Hospital and Characteristics of Referred Cases |
Cost-Effectiveness Analysis
Specialized reference clinics are very cost-effective as they reduced the need for referral to hospitals by 86.7%. Among 55,084 patients who utilized SRCs along two years, 47,744 patients received their medical care without referral to the hospital, saving total costs of about 14.08 million Saudi Riyals (3.75 million US dollars). The most cost-effective specialties are Internal Medicine, Gynecology & Obstetrics, Psychiatry, and Orthopedic clinics (saving 3.02, 3.01, 2.21, and 1.56 million Saudi Riyals) respectively. On the other hand, Urology and General Surgery clinics are not cost-effective as a large proportion of the patients, examined in either of them, are referred again to tertiary hospitals, and that can be explained by the need for sophisticated management and interventions that cannot be done in PHC-SRCs in these specialties (Table 3).
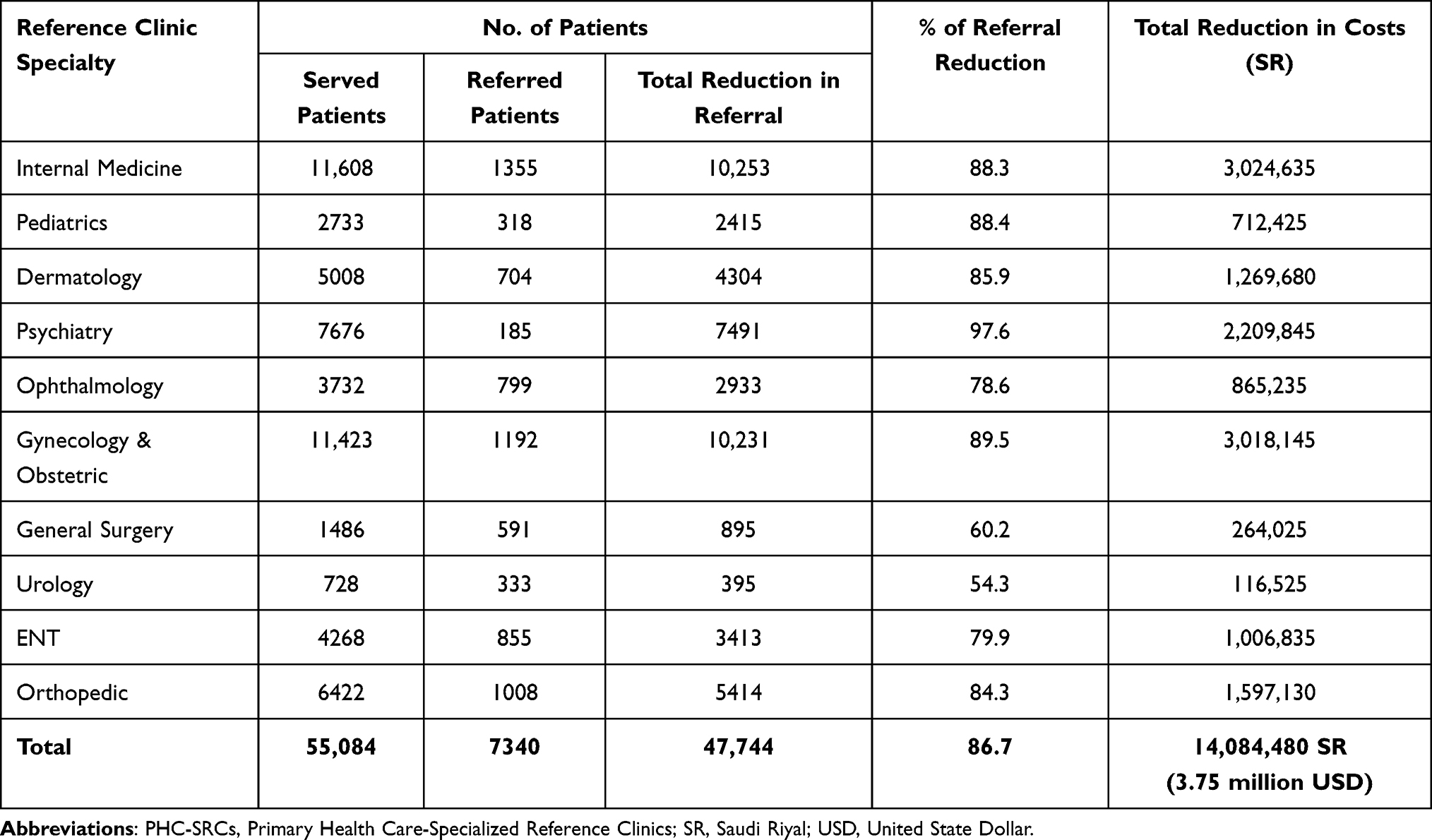 |
Table 3 Cost-Effectiveness and Total Reduction in Costs Associated with PHC-SRCs Services |
Assessment of Patient Satisfaction
Among 200 patients interviewed in the 1st year of service and another 200 patients interviewed in the 2nd year of service, the results of the patient satisfaction survey revealed that patients utilizing PHC-SRCs expressed a significant high satisfaction level in both years regarding all service domains, especially their satisfaction about medical services and their appointment in SRCs. The overall satisfaction score increased from 71.4% (mean score of 3.57 points out of 5) in the 1st year up to 73.2% (mean score of 3.66 points out of 5) in the second year. The patient satisfaction regarding most service domains has increased in the 2nd year more than that in the 1st year. However, their satisfaction about the appointment in SRCs was decreased in the 2nd year, which can be explained by increased utilization leading to more delays in appointments (Table 4).
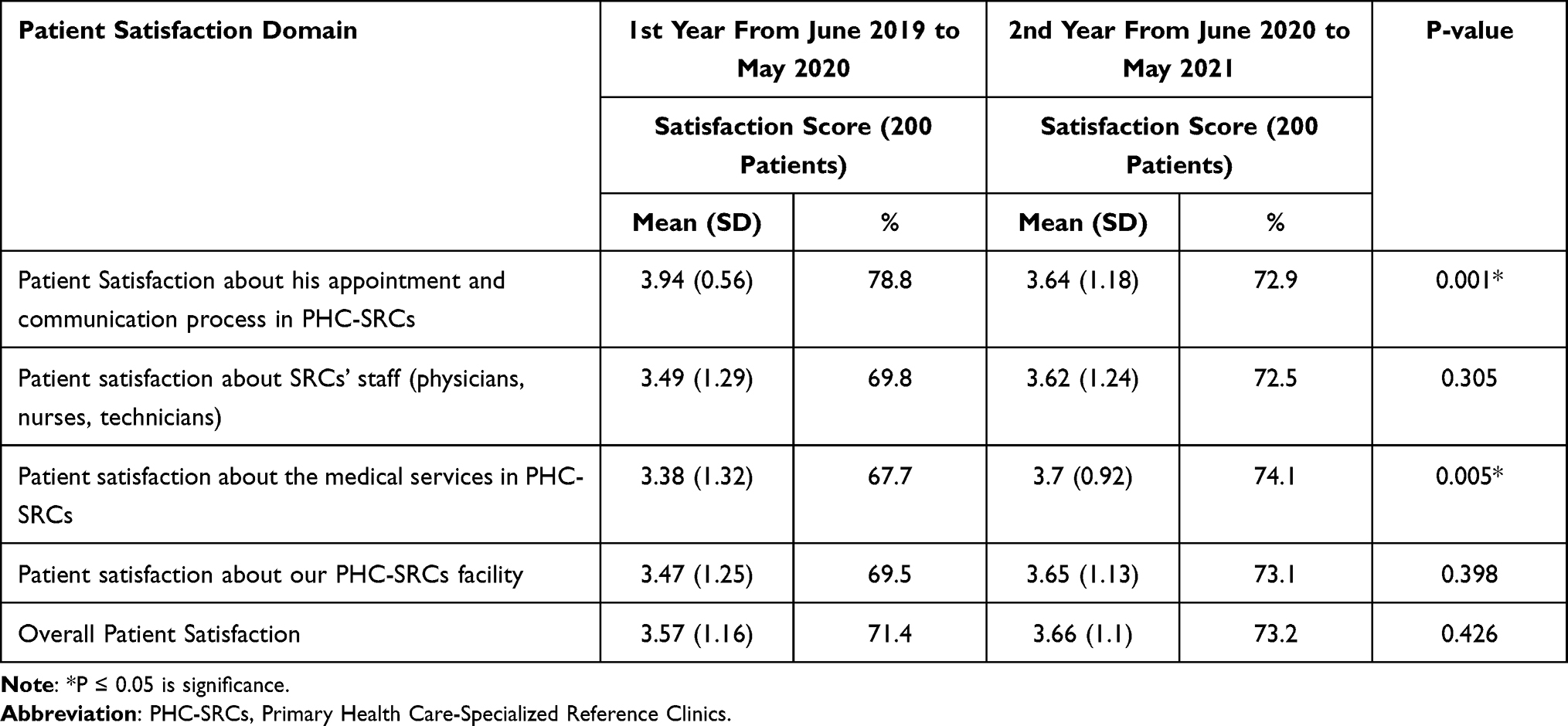 |
Table 4 Level of Patient Satisfaction Regarding the Services of PHC-SRCs |
Discussion
Referral from primary care to hospitals is a very important daily activity and physicians in PHCCs should follow clear guidelines about the need and reasons for patient referral.27 Ideally, PHCCs should be the point of first contact for patients from which patients may be referred to the secondary and tertiary levels if needed.28
Effective referral systems from PHCCs to hospitals represent a cornerstone in addressing patients’ health needs efficiently in several respects.4 From the patient’s point of view, a timely referral and appropriate medical care is the key to effective treatment. While, as a matter of healthcare economics, a well-functioning alternation between the different levels of healthcare delivery indicates that the available resources have been used efficiently.5,28
Reference Specialty Clinics were established in July 2019 at six PHCCs in Riyadh First Health Cluster. They started serving patients in many specialties in order to provide a timely referral, reduce the burden on hospitals, improve patient satisfaction and reduce the costs of healthcare delivery.
As revealed from our study, most of the patients served within PHC-SRCs had full medical service with no need for further referral to hospitals. While only 13.3% of patients are referred to hospitals for further investigation or advanced management. The finding illustrates the extreme reduction in the burden on tertiary hospitals (86.7%).
The overall referral rate observed in our study is nearly similar to the finding of Ringberg et al in Norway, as the mean referral rate to secondary care was 13.7%.29 While, referral rate in our study is lower than that reported in a study conducted in KSA by Khattab et al where a rate of 39.2% referrals was reported in Abha and a rate of 35.4% referrals was reported in Riyadh.30 On the other hand, our referral rate is high when compared with some other studies, where the referral rate ranged between 1.6 and 6.6 per 100 patient visits.5,31,32 Eighty-seven percent of patients in this study availed themselves of the referral in PHC-SRCs. These results were similar to the reports of Prathinidhi et al33 and the reports of Anton et al in India.6
As estimated from our study, the highest utilization rate and highest reduction in the need for referral to hospitals were noticed among Internal Medicine, Gynecology & Obstetrics, Psychiatry, and Orthopedic clinics respectively. While Urology and General Surgery showed the lowest utilization rate and the lowest reduction in referrals. That may be due to the more need for advanced investigations and sophisticated management for surgical-related specialty cases.
In this study, most of the referrals were made for chronic conditions (75%). However, Anton et al in their study in India noticed that almost equal numbers of referrals were made for acute conditions (51%) as for chronic ones (49%). Although many studies highlighted issues surrounding referral of acute conditions, only, few literatures discussed referrals of chronic cases.6
About eighty percent of referrals from SRCs to hospitals in this study were the physician’s decision, whether due to the need for sophisticated management or lack of some investigations in PHCCs. While only twenty percent of referrals in our study were self-requested. This was in agreement with the proportion estimated in the study of Forrest et al.2 However, Shabila et al, in their study in Iraqi, found that 38.4% of referrals were self-requested and they mentioned that lack of specific specialties in Iraqi PHCCs and the need for further management were the main reasons for further referral.4 Also, Tadesse in his study in Ethiopia stated that about one-third of the reasons for referrals were due to lack of skilled personnel and shortage of supplies.3
The starting point for the referral decision is that the physician must decide if diagnosis and management of the patient’s health problems are available within their scope of service.2 In practice the majority of patient needs can be met in primary health care. If the patient’s health problem cannot be managed, the physician should be the one who decides to refer the patient to the hospital.4 Also, the support by the specialist team in scenarios where a treatment decision is required that does not necessarily merit a formal specialist appointment, can significantly reduce the referral rate.34 Self-requested referrals to hospitals through exerting pressure on the physician may lead to system inefficiency.35
Moreover, the time factor is very essential in the treatment of all medical conditions but much more so in emergency cases.3 The objective of establishing PHC-SRCs is to provide the best specialized medical care by a skilled person at the appropriate time and accessible referral facilities. This study showed that the time spent until appointment is significantly reduced in almost all served patients from about six weeks in hospitals to about one week in PHC-SRCs. Ensuring access to appropriate management within a shorter time makes a difference to the final outcome as the prognosis will get worse as time elapses.
This study revealed that PHC-SRCs are very cost-effective as it reduced the need for referral to hospitals by 86.7% and saved total costs of about 14.08 million Saudi Riyals (3.75 million US dollars) over two years of service. The majority of SRCs are cost-effective and reduce the total costs of services to nearly half. However, surgical-related specialty clinics are not cost-effective as a large proportion of their patients needed a further referral to tertiary hospitals for more sophisticated management and interventions that cannot be done in PHC-SRCs.
These results are supported by the findings of many studies. Harindra et al 2010, concluded that specialized multidisciplinary heart clinics in Ontario, Canada, were cost-effective compared to the traditional willingness despite the apparent increase in long-term hospitalizations and their associated costs. They were associated with a 29% reduction in all-cause mortality. The 12-year cumulative cost per patient in the specialized clinic group was $66,532 versus $53,638 in the standard care group.36
Also in the study of Chenoweth and Judy Garrett (2006), the total off-site costs of care were $338,444 and that was nearly twice as high as actual on-site operational costs ($171,332). Overall, it appears that on-site clinics provide health care services 2 to 3 times more cost-effectively than do off-site healthcare services.22
Another study was conducted in Spain by de Liano et al to assess the cost-effectiveness of specialized asthma clinics. The number of patients managed in the specialized clinics increased from 41% to 86%. All cost variables, including management and diagnostic tests, were significantly reduced, giving an annual saving per patient of 338 €.24
Patient satisfaction has become a very important issue in recent decades and has been used as a research outcome of the quality of healthcare delivery. Furthermore, identifying unsatisfied patients and exploring their views on health care is essential for improving the health care quality. Accessibility of health care, organization of its services, treatment length, clinic structure, and competence of physicians are the main factors related to patient satisfaction.37
In the current study, the overall patients’ satisfaction with the provided services in our SRCs is 71.4% in the 1st year of service and has been increased up to 73.2% in the second year. Patient satisfaction has increased in the 2nd year regarding most SRCs’ service domains except for their satisfaction about appointments in SRCs, which was decreased in the 2nd year. That may be explained by the increased utilization rate of SRCs leading to more delays in appointments. These are very important results, as no previous study was done in KSA to evaluate SRCs and this will help in pushing the implementation of SRCs forward.
Our results are supported by the study of Saeed et al in Riyadh who found that clients’ satisfaction with provided services in PHCs is 75% and this satisfaction rate is close to our result.19 On the other hand, the levels of patient satisfaction reported in our study are higher than that in many other studies. Abutiheen et al in their study in Karbala revealed that the majority of clients (64.7%) were satisfied,13 AlTawil et al in Iraqi found a satisfaction rate of 69.3%,38 while in the study of Greenhow et al in Tunbridge, Kent, the satisfaction rate was 65.3%.16 Also, Afsar and Younus (2004) in their study in Pakistan, the satisfaction rate was 68.4%.39
Furthermore, previous studies in Saudi Arabia and some neighboring countries reported satisfaction rates ranging from 60% to 90%. (9–14) Satisfaction with physicians’ services in our study was (72.5%) which is better compared to studies in Jeddah City in Saudi Arabia (46.2%) and Kuwait City in Kuwait (44.2%).40,41
It is not always necessary to satisfy all patient’s wishes. Ordering investigations, referral to the hospital, and giving an appointment are all professional decisions and should be fulfilled by physicians if needed. Patients should be educated on this issue and that complying with all their wishes can have negative consequences on their own health in addition to wasting valuable resources.19
The Limitations of the Study
The first limitation of this study is that the cost-analysis was performed based on PHC centers and hospital perspectives. Therefore, indirect costs were not included in the analysis. The generalization of our results on other countries should be done with caution as cost-effectiveness results may vary from one country to another and from one specialty to another according to patient characteristics, disease epidemiology, and the costs of investigation and management.42 A second limitation is that our cost-analysis assumed the same average cost per patient irrespective of the clinic specialty, which is not actually true. Moreover, another limitation is that our estimates for the outcome of PHC-SRCs are limited to the reduction in referral rate to hospitals and the level of patient satisfaction.
Conclusion
The present study concluded that the creation of PHC-SRCs is both reasonable and beneficial in terms of reducing costs of health care delivery and improving patient outcomes. PHC-SRCs reduced the burden on hospitals, reduced the time needed for referral, have improved patient satisfaction, and saved costs in most medical specialties. Therefore PHC-SRCs is a highly cost-effective health service for patients in need of specialized care, except for surgical related specialties that were not founded to be cost-effective. The effectiveness of PHC-SRCs has been increased in the second year of service than that in the first year due to increased patient satisfaction and increased utilization rate. Our findings can inform decision-makers about the valuable benefits of implementing PHC-SRCs and suggest the need for excluding surgical related specialties to provide more cost-effective PHC-SRCs.
Abbreviations
AAFP, American Academy of Family Physicians; MGMA, Medical Group Management Association; PCPs Primary Care Physicians; PHCCs, Primary Health Care Centers; PHC-SRCs, Primary Health Care-Specialized Reference Clinics; PS, Patients’ Satisfaction; RFHC, Riyadh First Health Cluster; SRCs, SD, Standard Deviation; SPSS, Statistical Package for the Social Sciences; SR, Saudi Riyal; SRCs, Specialized Reference Clinics; WHO, World health organization.
Ethics Approval and Informed Consent
Before collecting data, ethical approval on research conduction was obtained from the Institutional Research Board of King Saud Medical City (IRB-KSMC) in Riyadh First Health Cluster (H1RE-17-Sep20-02). Also, an informed verbal consent, as approved by IRB-KSMC, was obtained from the selected subjects and documented in their records after explanation of the aim of the study and that their participation is voluntary, and were assured that collected data will be used only for the purpose of the study. We waive written consent, as the research has no risk of harm to subjects and the research involves no procedures or interventions for which written consent is normally required. We confirm that all procedures of the research comply with the Declaration of Helsinki.43
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work. No funds were received for this study from any funding organization.
References
1. World Health Organization. Referral systems - a summary of key processes to guide health services managers. WHO; [cited November 21, 2020]: 1–4. Available from: https://www.who.int/management/Referralnotes.doc.
2. Forrest CB, Nutting PA, von Schrader S, Rohde C, Starfield B. Primary care physician specialty referral decision making: patient, physician, and health care system determinants. Med Decis Making. 2006;26(1):76–85. doi:10.1177/0272989X05284110
3. Kitilla T. Reasons for referrals and time spent from referring sites to arrival at TikurAnbessa hospital in emergency obstetric: a prospective study. Ethiop J Health Dev. 2001;15(1):17–23.
4. Shabila N, Al-Tawil NG, Al-Hadithi T, Sondorp E. Assessment of the Iraqi primary care referral system: reporting a high self-requested referral rate. Middle East J Fam Medicine. 2012;10(3):4–10.
5. AlGhamdi OM, AL-Malki BM, Nahhas AE, AL-Malki AD. Rate of referral from primary health care to secondary health care among governmental hospitals in Taif governorate, KSA. Int J Med Sci Public Health. 2015;4(10):1457–1463. doi:10.5455/ijmsph.2015.19062015302
6. Anton NI, Noel V, Cyriac AP, Geoiphy GP, Christopher L. Outcome of referrals from a primary health institution in rural Karnataka. Pak J Med Sci. 2008;24(1):157–160.
7. Akande TM. Referral system in Nigeria: study of a tertiary health facility. Ann Afr Med. 2004;3(3):130–133.
8. Eric YH, Richard MS, Leamon RNJ. How many referrals to a pediatric orthopaedic hospital specialty clinic are primary care problems? J Pediatr Orthop. 2012;32(7):727–731. doi:10.1097/BPO.0b013e31826994a4
9. Stille CJ, McLaughlin TJ, Primack WA, Mazor KM, Wasserman RC. Determinants and impact of generalist–specialist communication about pediatric outpatient referrals. Am Acad Pediatr. 2006;118(4):1341–1349.
10. Zuchowski JL, Rose DE, Hamilton AB, et al. Challenges in referral communication between VHA primary care and specialty care. J Gen Intern Med. 2014;30(3):305–311.
11. Zuckerman KE, Cai X, Perrin JM, Donelan K. Incomplete specialty referral among children in community health centers. J Pediatr. 2010;158(1):3–4.
12. Nancy H. 3 reasons why a referral process goes incomplete [internet]. HealthviewX Publisher; 2018 [cited November 29, 2020]. Available from: https://www.healthviewx.com/3-reasons-referral-process-goes-incomplete.
13. Abutiheen AK. Clients’ satisfaction with referral system in Karbala. Am J Appl Sci. 2014;11(2):216–222. doi:10.3844/ajassp.2014.216.222
14. Gorgen HT, Kirsch-Woik T, Schmidt-Ehry B. The District Health System: Experiences and Prospects in Africa. Manual for Public Health Practitioners.
15. Simba DO, Mbembati NA, Museru LM, Lema LE. Referral pattern of patients received at the national referral hospital: challenges in low-income countries. East African J Public Health. 2008;5(1):6–9. doi:10.4314/eajph.v5i1.38969
16. Greenhow DE, Howitt AJ, Kinnersley PA. Patient satisfaction with referral to hospital: relationship to expectations, involvement, and information-giving in the consultation. Br J Gen Pract. 1998;48(426):911–912.
17. Osibogun A. The role of health center in the rational use of health resources.
18. Ahmad I, Nawaz A, Khan S, Khan H, Rashid MA. Predictors of patient satisfaction. Gomal J Med Sci. 2011;9(2):183–188.
19. Saeed AA, Mohammed BA, Magzoub ME, Al-Doghaither AH. Satisfaction and correlates of patients’ satisfaction with physicians’ services in primary health care centers. Saudi Med J. 2001;22(3):262–267.
20. Sohrabi MR, Albalushi RM. Clients’ satisfaction with primary health care in Tehran: a cross-sectional study on Iranian health centers. J Res Med Sci. 2011;16(6):756–762.
21. Hansen PM, Peters DH, Viswanathan K, Rao KD, Mashkoor A, Burnham G. Client perceptions of the quality of primary care services in Afghanistan. Int J Q Health Care. 2008;20(6):384–391. doi:10.1093/intqhc/mzn040
22. Chenoweth DH, Garrett J. Cost-effectiveness analysis of a worksite clinic: is it worth the cost? Aaohn J. 2006;54(2):84–91. doi:10.1177/216507990605400206
23. de Llano LA, Villoro R, Merino M, Neira MD, Muñiz C, Hidalgo Á. Cost effectiveness of outpatient asthma clinics. Arch Bronconeumol. 2016;52(4):196–203. doi:10.1016/j.arbr.2016.02.009
24. de Bakker DH, Struijs JN, Baan CB, et al. Early results from adoption of bundled payment for diabetes care in the Netherlands show improvement in care coordination. Health Aff. 2012;31(2):426–4 33. doi:10.1377/hlthaff.2011.0912
25. Hendriks J, Tomini F, Van Asselt T, Crijns H, Vrijhoef H. Cost-effectiveness of a specialized atrial fibrillation clinic vs. usual care in patients with atrial fibrillation. Europace. 2013;15(8):1128–1135. doi:10.1093/europace/eut055
26. White B. Measuring patient satisfaction: how to do it and why to bother. Fam Pract Manag. 1999;6(1):40.
27. Jarallah JS. Referral from primary care to hospitals in Saudi Arabia: 1) quality of referral letters and feedback reports. J Family Community Med. 1998;5(2):15.
28. Kvamme OJ, Olesen F, Samuelson M. Improving the interface between primary and secondary care: a statement from the European working party on quality in family practice (EQuiP). BMJ Qual Saf. 2001;10(1):33–39.
29. Ringberg U, Fleten N, Deraas TS, Hasvold T, Førde O. High referral rates to secondary care by general practitioners in Norway are associated with GPs’ gender and specialist qualifications in family medicine, a study of 4350 consultations. BMC Health Serv Res. 2013;13(1):1–10. doi:10.1186/1472-6963-13-147
30. Khattab MS, Abolfotouh MA, Al-Khaldi YM, Khan MY. Studying the referral system in one family practice center in Saudi Arabia. Ann Saudi Med. 1999;19(2):167–170. doi:10.5144/0256-4947.1999.167
31. Baghdadi L, Baghdadi R. Referral system from PHC to hospital in Holy Makkah, Umm Al-Qura University, faculty of medicine, Mecca, Saudi Arabia; 2007.Mahfouz AA, Abolfotouth MA, Al-Khozayem AA, Al-Erian RA. Referral system in the Asir Region, Saudi Arabia: a study on hospitals’ referral coordination offices. Saudi Med J. 1993;14:237–239.
32. Mahfouz AA, Abolfotouth MA, Al-Khozayem AA, Al-Erian RA. Referral system in the Asir Region, Saudi Arabia: a study on hospitals’ referral coordination offices. Saudi Med J. 1993;14(3):237–239.
33. Prathinidhi AK, Talwalkar MV, Gupte AM. A profile of referrals from primary health centres. Indian J of Community Medicine. 993;18(4):172–176.
34. Heald AH, Anderson SG, Khan A, et al. Success rates in a diabetes specialist nurse-led education programme: re-setting the glucostat. Exp Clin Endocrinol Diabetes. 2017;125(5):297–300. doi:10.1055/s-0042-108055
35. Rasoulynejad SA. Study of self-referral factors in the three-level health care delivery system. Kashan, Iran, 2000. Rural Remote Health. 2004;4(4):1–11.
36. Wijeysundera HC, Machado M, Wang X, et al. Cost-effectiveness of specialized multidisciplinary heart failure clinics in Ontario, Canada. Value in Health. 2010;13(8):915–921. doi:10.1111/j.1524-4733.2010.00797.x
37. Al-windi A. Predictors of satisfaction with health care: a primary healthcare-based study. Qual Prim Care. 2005;13(2):67–74.
38. Al-Tawil NG, Wahab M, Shabila N. Assessment of the primary care referral system in Iraqi Kurdistan.
39. Afsar HA, Younus M. Patient referral at the grass-roots level in Pakistan. Nat Sci. 2004;2:18–27.
40. Al-Doghaither A, Saeed A. Consumers’ satisfaction with primary health services in the city of Jeddah, Saudi Arabia. Saudi Med J. 2000;21(5):447–454.
41. Al-Doghaither AH, Abdelrhman BM, Saeed AA. healthcare centres in Kuwait City. JRSH. 2000;120:170–174. doi:10.1177/146642400012000306
42. Goeree R, Burke N, O’Reilly D, Manca A, Blackhouse G, Tarride JE. Transferability of economic evaluations: approaches and factors to consider when using results from one geographic area for another. Curr Med Res Opin. 2007;23(4):671–682. doi:10.1185/030079906X167327
43. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. J Am Med Assoc. 2013;310:2191. doi:10.1001/jama.2013.281053
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.